")
Back to Journals » International Journal of Women's Health » Volume 15
Prevalence of Hypothyroidism in Pregnancy and Its Associations with Adverse Pregnancy Outcomes Among Pregnant Women in A General Hospital: A Cross Sectional Study
Authors Abadi KK , Jama AH , Legesse AY , Gebremichael AK
Received 2 August 2023
Accepted for publication 26 September 2023
Published 3 October 2023 Volume 2023:15 Pages 1481—1490
DOI https://doi.org/10.2147/IJWH.S429611
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Elie Al-Chaer
Kidus Kebede Abadi,1 Abdikani Hassan Jama,1,2 Awol Yemane Legesse,3 Akebom Kidanemariam Gebremichael4
1Daruxannan General Hospital, Burao, Somaliland, Somalia; 2Burao University, Burao, Somaliland, Somalia; 3Department of Obstetrics and Gynecology, Mekelle University, Mekelle, Tigray, Ethiopia; 4Saint Peter’s Specialized Hospital, Addis Ababa, Ethiopia
Correspondence: Kidus Kebede Abadi, Email [email protected]
Background: Hypothyroidism affects 3– 5% of all pregnant mothers, making it the most common thyroid disorder associated with pregnancy. Furthermore, it is associated with adverse outcomes of pregnancy and newborn. Therefore, this research is aimed at determining the magnitude and pregnancy adverse outcomes associated with hypothyroidism among pregnant women having maternity services in a general hospital in Somalia.
Methods: A cross-sectional study was conducted on pregnant women who delivered in the hospital between December 2022 and May 2023. Subjects were selected through systematic sampling and data collected through an interviewer-based questionnaire. Adjusted odds ratios (AORs) of P values and 95% confidence intervals (CIs) were used to assess the correlation between variables.
Results: The prevalence of hypothyroidism was 23.6% (95% CI: [19.4– 27.8]). Overt DM (AOR=9.125, CI (3.106– 26.812)), History of Recurrent pregnancy loss (AOR=12.938, CI (4.958– 33.763), hypertension during pregnancy (AOR=6.718, CI (2.326– 19.994)) and preterm delivery (AOR=7.015, CI (3.234– 13.958)) were variables associated with hypothyroidism in pregnancy.
Conclusion: The study has shown a high prevalence of hypothyroidism during pregnancy at Daruxannan Hospital compared to previous studies around the world. This finding highlights the need for national and regional surveys to identify the prevalence and associated factors that contribute to hypothyroidism in pregnancy to set up interventions and determine policy directions.
Keywords: hypothyroidism, pregnancy outcome, Somalia
A Letter to the Editor has been published for this article.
A Response to Letter by Professor Pei has been published for this article.
Introduction
Globally, next to diabetes, thyroid disorders are the most common endocrine disorder and are relevant to public health1,2 Hypothyroidism is a prevalent thyroid disorder during pregnancy, affecting approximately 3–5% of pregnant women. However, the prevalence can vary based on factors such as diagnostic criteria, maternal iodine status and pregnancy stage. Pregnancy-related hypothyroidism has been associated with various negative outcomes for both the mother and the newborn. These include an increased risk of spontaneous abortion, anemia, pre-eclampsia, gestational hypertension and placental abruption.3–10
The prevalence of hypothyroidism in pregnancy in low- and middle-income countries has been reported to be 5–31.6%, which is higher than the prevalence in developed countries.7,11–16 Furthermore, factors such as old age, chronic medical disease, adverse maternal and newborn outcomes, and a personal and family history of thyroid dysfunction have been correlated with hypothyroidism during pregnancy.7,13,15,17,18
Moderate-to-severe iodine deficiency has been a problem in sub-Saharan Africa.19 Furthermore, Somalia has poor access to iodized salt and a high prevalence of cultural beliefs and barriers that prevent optimal consumption of micro-nutrients like iodine.19 Studies have shown that iodine deficiency is strongly associated with hypothyroidism. However, data related to hypothyroidism in pregnancy has been limited in Somalia. Furthermore, the evidence on the risk factors and correlates of adverse maternal and neonatal outcomes of pregnant women with hypothyroidisms are limited. Understanding the associated factors of hypothyroidism in pregnancy will help reduce the magnitude and associated adverse outcomes. Therefore, the current study aims to determine the magnitude and adverse pregnancy outcomes related with hypothyroidism among pregnant women seeking maternity service at Daruxannan Hospital.
Methods
Study Design, Area, and Period
A prospective hospital-based cross-sectional study was conducted at Daruxannan Hospital in Burao, Somaliland, Somalia. The data collection period was from December 2022 to May 2023. All pregnant women who were admitted to the hospital after the gestational age (GA) of 24 completed weeks to give birth during the study were the study population. Pregnant women who delivered after GA of 24 completed weeks and gave written informed consent were included. We excluded those women who had known the result of thyroid stimulating hormone (TSH) during the current pregnancy and those on treatment for thyroid disorders. Additionally, pregnant women before the GA of 24 weeks and those who had communication difficulties were excluded.
Sample Size and Sampling Procedure
Single population proportion formula was used to calculate the sample size. Since there is no available study done with similar socio-demographic characteristics in the country, we took a P value of 0.50. Using the power of 80%, the estimated sample size was 386 adding a marginal error of 5% and a contingency rate. Systematic random sampling was utilized to collect the sample size.
Data Collection Procedures
Data was collected 24 hours after delivery using interviewee administered structured questionnaires. Consistency was checked by preparing the questionnaires in English and translating it to Somali and then translated back to English. Pre-test and appropriate modification was carried out on the questionnaire. The principal investigator trained the data collectors in pre-tested checklists. Completeness, accuracy, and consistency of the collected data were checked daily by the principal investigator.
For the thyroid hormone parameter, venous blood was collected from the recruited mothers at the time of admission for delivery and the TSH values were analysed. For the abnormal range of TSH values, we checked the free levels of T3 and T4. The American Thyroid Association Guidelines 2011 was used to evaluate the results of thyroid hormone values taking a reference range of 0.3–3.0 m IU/L for third trimester.8 According to the same guideline, patients were classified as subclinical hypothyroidism if the TSH levels were elevated and a normal serum free T3 and T4 levels; high TSH levels and low levels of free T3 and T4 were classified as overt hypothyroidism. After diagnosis, the patient was referred to the treating physician for further investigation and treatment.
Hypothyroidism (TSH above 3.0 miu/l) was the dependent variable. Independent variables were sociodemographic characteristics (age, educational status, place of residency, and marital status), reproductive history (gravidity, parity, abortion, singleton versus multiple gestation and mode of conception), and risk factors (Personal/family history of thyroid dysfunction, thyroid surgery, prior adverse pregnancy outcome, chronic medical illness, history of infertility, use of iodised salt) and pregnancy outcomes (mode of delivery, GA at delivery, neonatal birth weight, maternal and newborn complications).
Data Management and Analysis
Each questionnaire was visually checked for completeness after data collection and code was given. Epi-info version 3.5.1 was used for data entry, and Statistical Package for Social Science (SPSS) version 25 software packages was used for analysis. Additionally, cross checking, data cleaning, and necessary corrections were performed by the principal investigator before data analysis. Descriptive statistics was used for sociodemographic characteristics, reproductive history, and risk factors for hypothyroidism in pregnancy. Independent factors associated with hypothyroidism in pregnancy were identified using bivariate and multivariate logistic regression. First, the crude association between independent and outcome variables was observed after bivariate analysis was carried out. Then, a multivariate model was used for variables with a P value <0.2 in bivariate analysis. Hosmer-Lemeshow goodness-of-fit was used to evaluate the goodness-of-fit of the logistic regression model. Finally, using the odds ratio with a 95% confidence interval and a P value of <0.05 statistically significant variables in the multivariate regression model was identified.
Ethical Consideration
The Declaration of Helsinki served as the guide for conducting the current investigation. The Burao University Institutional Review Board (IRB) granted ethical approval, and subjects under the age of 18 were required to provide informed written consent by their legal guardian or parents. The hospital administration gave the study’s administrators permission to carry it out. After describing the study’s goals to each participant, their informed consent was obtained. We did not gather or keep any identifying information about participants in order to protect their privacy. The manuscript includes all of the data sets that were used and/or examined throughout the current study.
Results
During the study period, a total of 386 patients participated, with 91 participants having hypothyroidism. This indicates the prevalence of hypothyroidism at 23.6% (95% CI: [19.4–27.8]). Out of the 91 participants with hypothyroidism, 31 individuals (8%) had overt hypothyroidism and the remaining ten (15.6%) had subclinical hypothyroidism. Ten (2.6%) participants had hyperthyroidism, among which two (0.5%) had subclinical hyperthyroidism and eight (2.1%) had overt hyperthyroidism.
Socio-Demographic Characteristics
Among different age groups, the rate of hypothyroidism was comparable. Furthermore, comparable rates of hypothyroidism were observed among housewives and employed participants. Participants who were unable to read and write had more hypothyroidism (P=0.000). Furthermore, those who lived outside of the city of Burao had a higher rate of hypothyroidism (P=0.002) (Table 1).
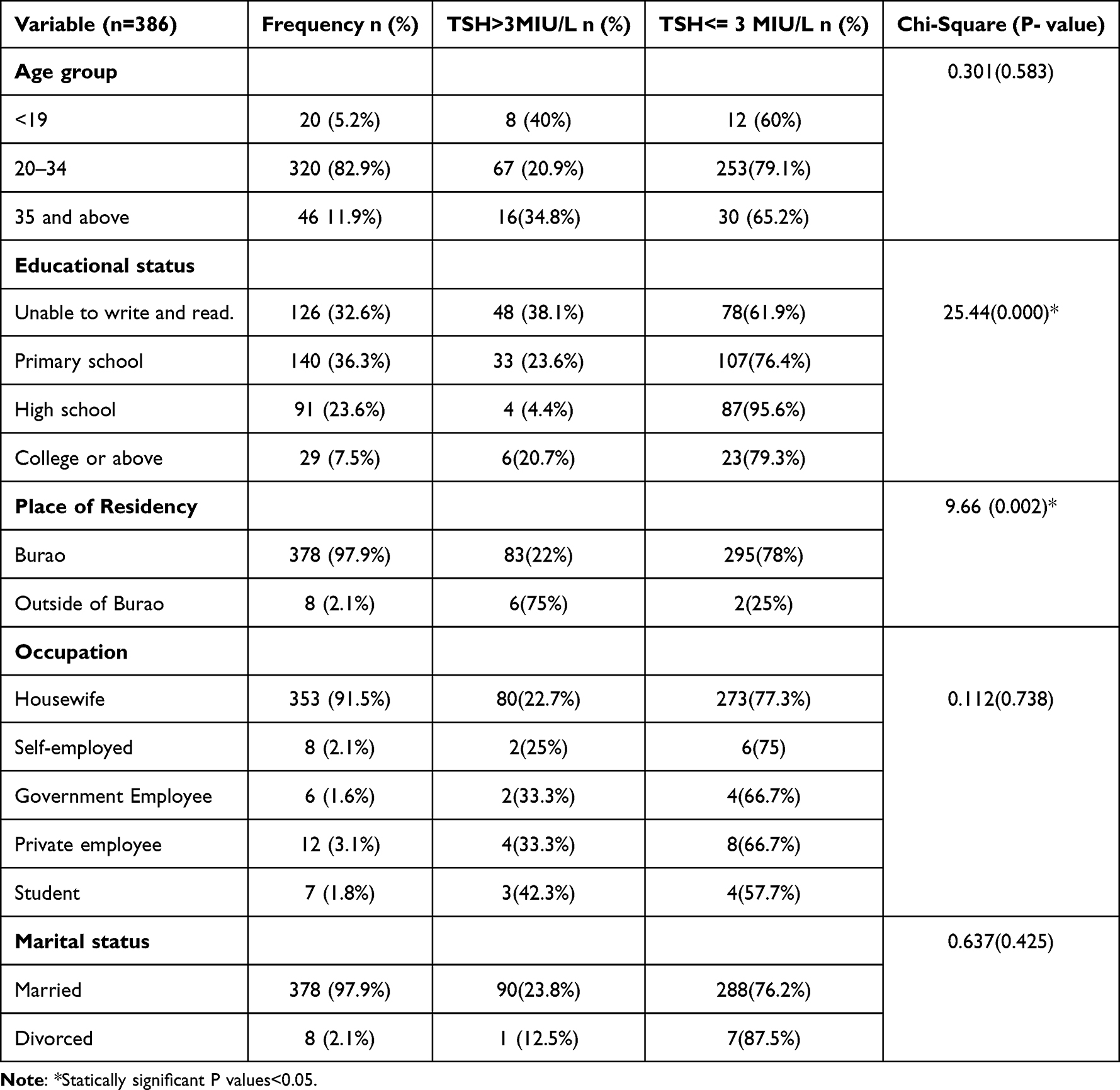 |
Table 1 Distribution of the Pregnant Women According to Their Socio-Demographic Characteristics with or Without Hypothyroidism |
Reproductive Characteristics and Risk Factors
A comparable rate of hypothyroidism was observed between different gravidities. Similarly, the prevalence of hypothyroidism among women with multiple pregnancies was comparable to those with a singleton pregnancy. However, those with a personal or family history of thyroid dysfunction had a higher prevalence than those with no self- or family history (P=0.001 and P=0.026 respectively). Similarly, the participants with chronic hypertension (P=0.000), overt DM (P=0.000), and a history of RPL (P=0.000) had a higher percentage of hypothyroidism. However, the rate of hypothyroidism was similar among those who had used iodised salt in their diet and those who had not (Table 2 and Table 3).
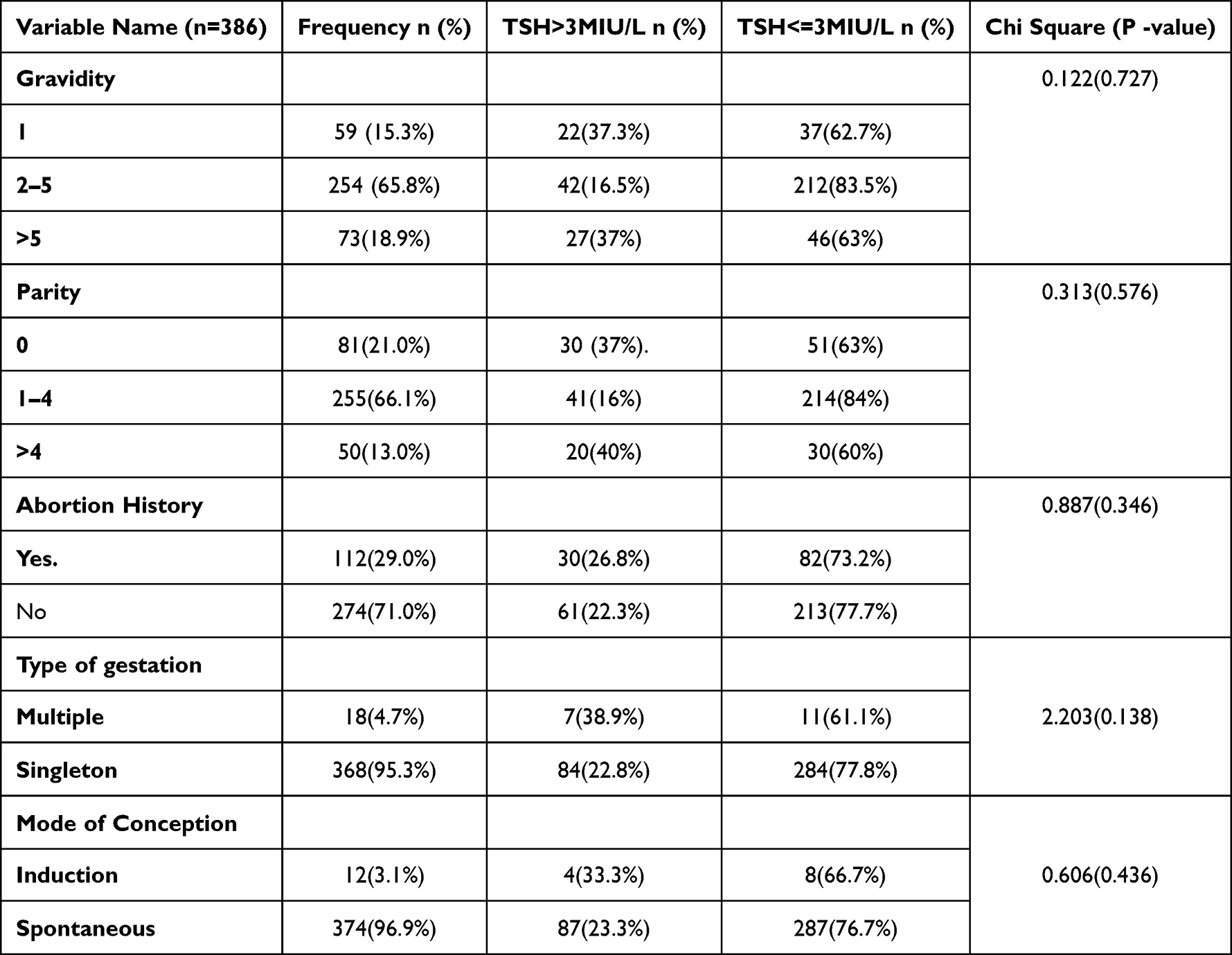 |
Table 2 Analysis of the Reproductive Characteristics of the Pregnant Women with or Without Hypothyroidism |
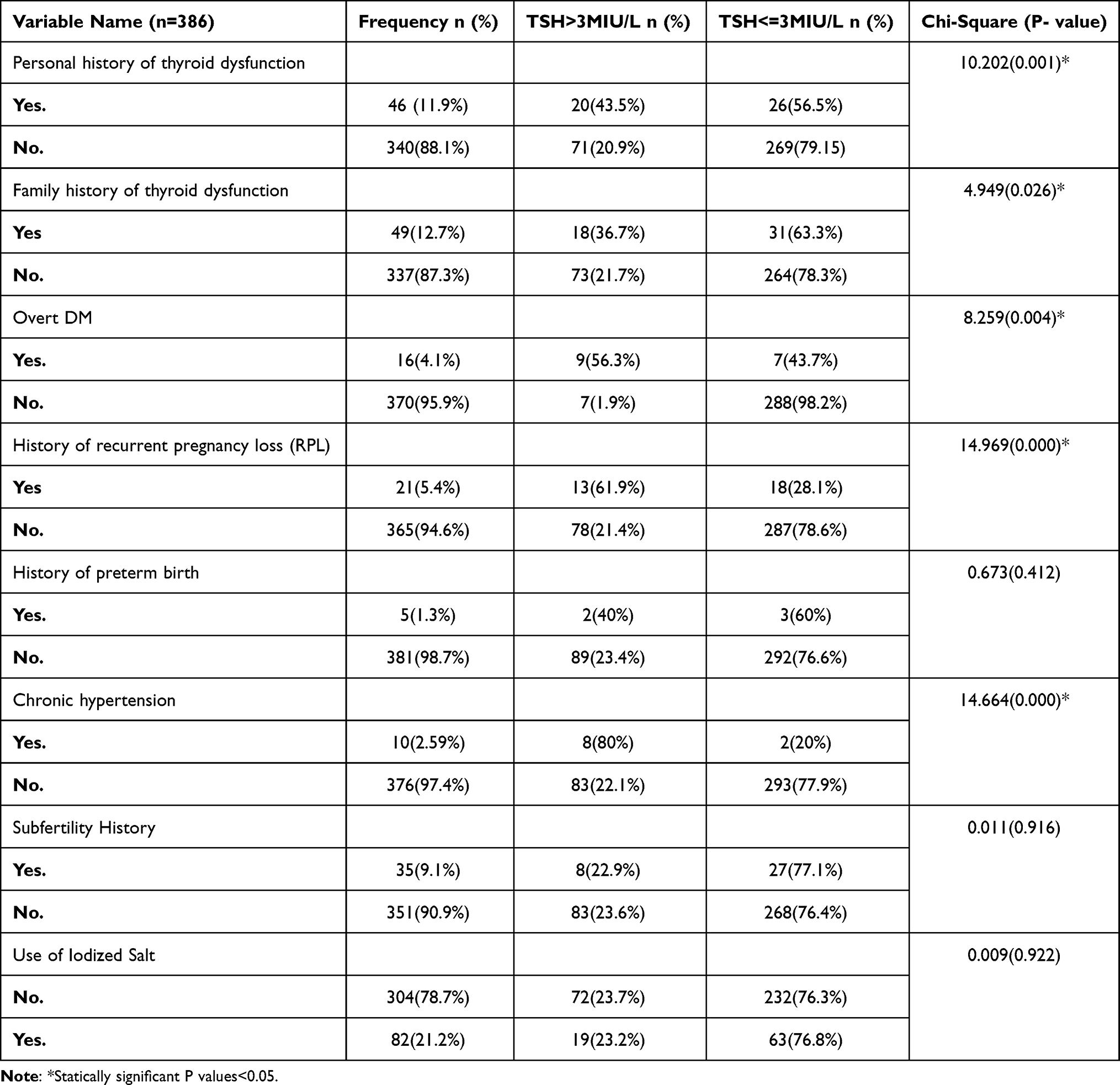 |
Table 3 Distribution of Pregnant Women According to the Risk Factors with or Without Hypothyroidism |
Pregnancy Outcomes
Pregnant women who delivered before GA of 37 completed weeks had a higher prevalence of hypothyroidism (P=0.002). Likewise, those with maternal complications of hypertension during pregnancy, Ante-Partum Hemorrhage (APH), and Post-Partum Hemorrhage (PPH) had more hypothyroidism (P=0.000). Moreover, hypothyroidism was more noted among participants with newborn complications of APGAR score less than seven, still birth and Congenital anomaly (P=0.013) (Table 4).
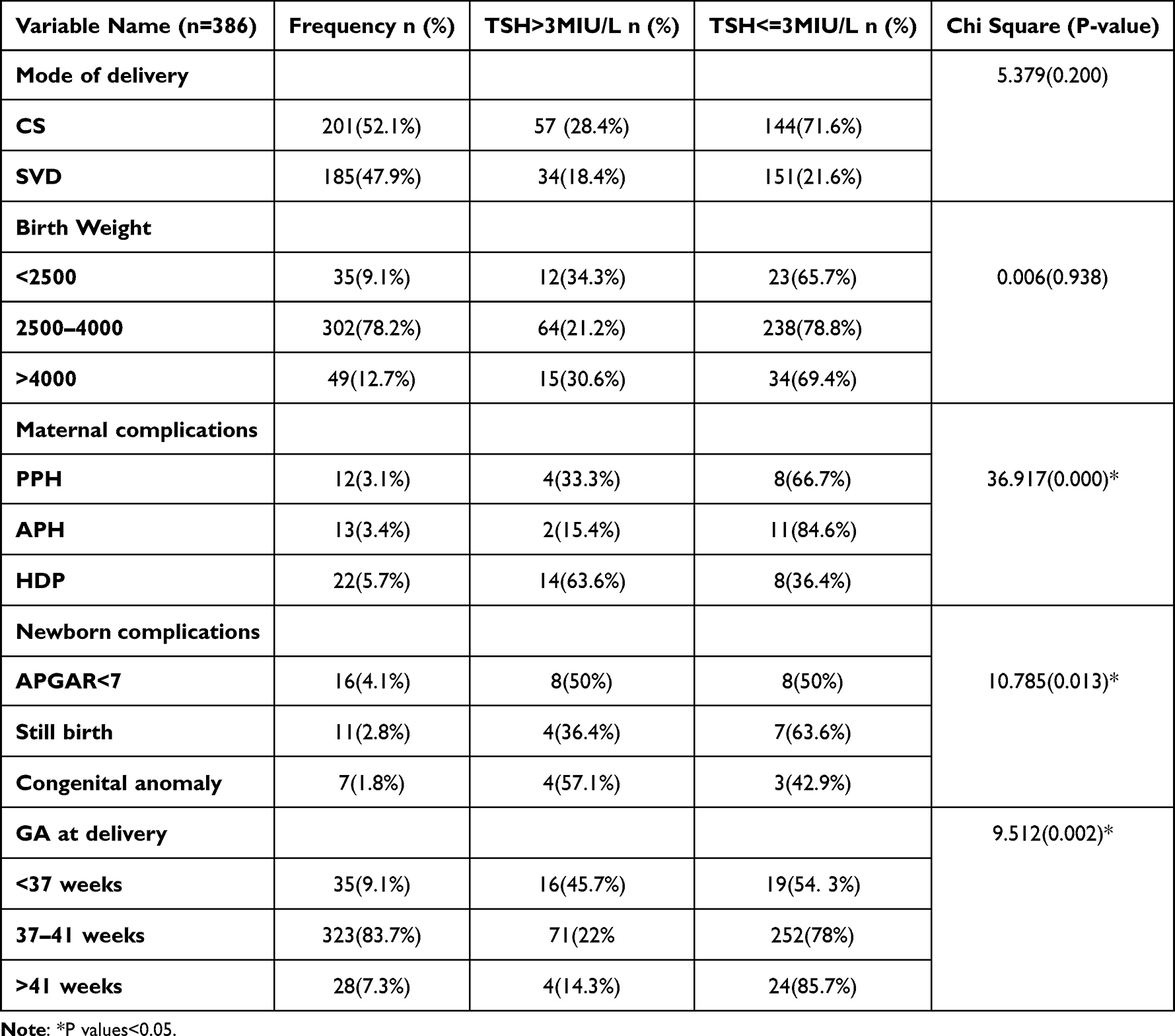 |
Table 4 Analysis of the Pregnancy Outcomes in Pregnant Women with or Without Hypothyroidism |
Adverse Pregnancy Outcomes Associated with Hypothyroidism During Pregnancy
Overt DM, a history of RPL, chronic hypertension, and multiple gestation and adverse pregnancy outcomes of hypertension during pregnancy, preterm delivery, cesarean section, and low APGAR score were found to be associated with hypothyroidism during pregnancy in bivariate analysis. Then, a multivariable logistic regression model was used for these variables. Finally, using the odds ratio with a 95% confidence interval and a P value of <0.05 statistically significant variables in the multivariate regression model was identified. Overt DM (9.125 (3.106–26.812)), History of Recurrent pregnancy loss (12.938 (4.958–33.763)), hypertension during pregnancy (6.718 (2.326–19.994)) and preterm delivery (7.015 (3.234–13.958)) were variables associated with hypothyroidism in pregnancy (Table 5).
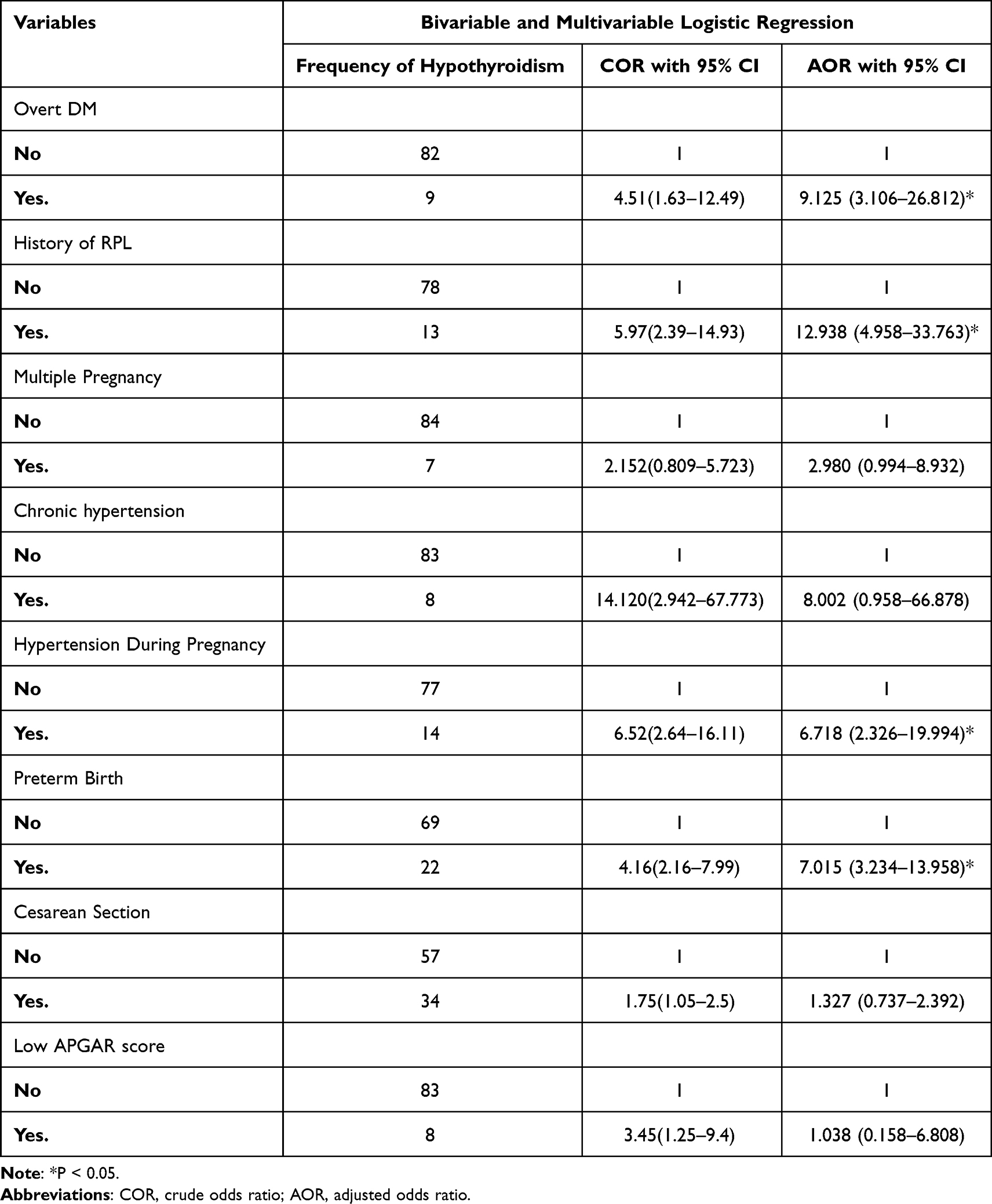 |
Table 5 The Bivariable and Multivariable Logistic Regression results on Variables Associated with Hypothyroidism in Pregnancy |
Discussion
The current research is conducted at Daruxannan General Hospital to evaluate the magnitude of hypothyroidism during pregnancy and the adverse pregnancy outcomes associated with hypothyroidism. The prevalence of hypothyroidism during pregnancy in our study is 23.6% (95% CI: [19.4–27.8]). Overt DM, history of RPL were the risk factors significantly associated with hypothyroidism in pregnancy. Furthermore, hypertension during pregnancy and preterm delivery were the adverse pregnancy outcomes associated with hypothyroidism in pregnancy.
The magnitude of hypothyroidism in pregnancy in our study is greater than the 2% to 18% prevalence reported worldwide.11,12,14,15 It is also not in line with the study done in Africa Ivory Coast and Nigeria, which reported a prevalence of 12.1% and 18%, respectively.15,16 However, a prospective observational study carried out in a tertiary care institute in Punjab, North India has shown a prevalence of 31.6% prevalence of hypothyroidism in pregnancy, which is higher than our study.7 Moderate-to-severe iodine deficiency has been a problem in sub-Saharan Africa.19 Somalia is a coastal country, and the main source of dietary iodine is groundwater.19 According to our study only 20% of the participants reported use of iodized salt in their diet. It has also been noted that there is a lack of access to iodized salt and a significant prevalence of cultural attitudes and impediments to poor consumption of micro-nutrients, especially iodine.19 The large percentage of high-risk patients in hospitals and the country’s inadequate access to health-care services may be the factor for the significant proportion of hypothyroidism among pregnant women in the current study.
In countries with different cultures and development, factors correlated to hypothyroidism in pregnancy appear similar and disproportionately associate with old age, poor socioeconomic status, chronic medical illness, and history of adverse pregnancy outcomes.18–20 Likewise, our study noted higher prevalence of hypothyroidism among pregnant women who were not able to write and read, lived outside of the city (P=0.002), maternal complications (P=0.000) and newborn complications. Additionally, chronic diseases such as diabetes mellitus are associated with hypothyroidism in pregnancy. A hospital-based cross-sectional study conducted at Bouget General Hospital, Abidjan, Ivory Coast illustrated that patients with reported type 1 diabetes mellitus had an increased risk of hypothyroidism (aOR: 12.6, 95% CI 1.9–100.8; p ≤ 0.01).15 In line with this, the current study showed a significant association of overt diabetes mellitus with hypothyroidism in pregnancy. Potential explanations include the fact that patients with diabetes mellitus could also manifest concomitant autoimmune insult to other endocrine glands, including the thyroid.21 Moreover, the high rate of both diabetes and hypothyroidism in this could line with this explanation.
Numerous unfavorable maternal and newborn outcomes have been linked to hypothyroidism during pregnancy. A retrospective cohort study conducted in the Boston medical center in the United States (US) demonstrated that maternal serum TSH concentration >4 mIU/L during pregnancy was doubling the risks of prematurity and RDS in offspring. Elevated TSH was also associated with statistically not significant increases in the risk of fetal loss, preeclampsia/eclampsia, and low birth weight.6 Similarly, a cohort study of 41647 participants conducted in a tertiary academic medical center reported that overt hypothyroidism was related to the risk of severe PE (OR, 2.59; 95% CI, 1.05–6.37).5 Moreover, a cross-sectional study of hypertensive pregnant women in different trimesters in Warri (Pessu and Eboh Health Centers) showed that serum TSH was elevated (p < 0.035) among hypertensive pregnant women compared to non-hypertensive pregnant women.6 Our study has shown that hypothyroidism during pregnancy has a significant association with hypertension during pregnancy, including gestational hypertension, preeclampsia, and eclampsia. Although this finding is in line with previous evidence, more study with a methodology that can establish a cause-and-effect relationship may be needed. Furthermore, there is inconsistent evidence showing that the risk of recurrent pregnancy loss is associated with hypothyroidism in pregnancy. Hypothyroidism has a statistically significant relationship with recurrent pregnancy loss in the first trimester, according to a retrospective cohort study conducted in India on 163 non-pregnant women with recurrent pregnancy loss in a gestational age range up to 12 weeks that was confirmed by a pregnancy test or ultrasonography.4 The current study also showed a history of recurrent pregnancy significantly associated with hypothyroidism in pregnancy. However, the diagnosis of recurrent pregnancy loss was made by history and not confirmed with ultrasound or histology. This might have impacted the magnitude of the RPL. On the contrary, a systematic review and meta-analysis done in a university setting concluded that there is no association between RPL and subclinical hypothyroidism, although association was noted with sporadic abortion.22
Preterm birth is linked to hypothyroidism and autoimmune thyroid disorders in pregnant women.23 The relative risks of clinical hypothyroidism, subclinical hypothyroidism, and hypothyroxinemia during pregnancy on preterm birth were calculated to be 1.30 (95% CI: 1.05–1.61, p=0.013), 1.36 (95% CI: 1.09–1.68, p=0.005), and 1.31 (95% CI: 1.04–1.66, p=0.020) respectively in a systematic review and meta-analysis of 23 studies.24 The current study has shown elevated risk of preterm delivery among hypothyroid patients. However, the gestational age of the participants was estimated from ultrasound performed during admission for those without an early ultrasound scan and unknown last normal menstrual period (LNMP). This could under or overestimate the gestational age at delivery.
The study’s strengths include the prospective main data collection in a single interaction with each patient and a lower dropout rate. Additionally, the relatively lengthy period of data collection—about six months—could aid in capturing the variation over time and improve the representativeness of samples that might be used to forecast the outcome variable. The study also has limitations. The sample size calculation may not have been sufficient because it might not take into account how many variables were present. As any cross-sectional study, it could not explain the cause-and-effect relationship. Furthermore, being a single hospital-based study; the current study could have suffered from the possibility of selection bias. Moreover, limitation on accurate estimations of gestational age may limit the strength of the correlates. These factors together may limit the generalizability of the current findings.
Conclusions and Recommendations
The current study reveals a higher prevalence of hypothyroidism during pregnancy at Daruxannan Hospital compared to previous global studies. Factors such as a history of recurrent pregnancy loss and diabetes mellitus were found to be significantly associated with hypothyroidism in pregnancy. Hypertension during pregnancy and premature birth were the adverse outcomes of pregnancy associated with hypothyroidism. However, since cross-sectional studies do not establish causality, it may be necessary to conduct a case-control or cohort study to further investigate the potential adverse outcomes of hypothyroidism on newborns during pregnancy. In addition, national and regional surveys are needed to determine the prevalence of hypothyroidism during pregnancy and factors that contribute at the country level to determine policy directions and set up interventions.
Abbreviations
AOR, Adjusted Odd Ratio; CI, Confidence Interval; IRB, Institutional Review Board; LNMP, Last Normal Menstrual Period; OR, Odds Ratio; SPSS, Statistical Package for Social Science; US, United States; DM, Diabetes Mellitus; RPL, Recurrent Pregnancy Loss; HDP, Hypertension During Pregnancy; GA, Gestational Age; APH, Ante-Partum Hemorrhage; PPH, Post-Partum Hemorrhage.
Acknowledgments
We would like to thank the institutional review board of Burao University for the ethical clearance and the hospital administration for permission to conduct the study. Furthermore, we would like to thank all study participants for their valuable contribution.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Alexander EK, Pearce EN, Brent GA, et al. 2017 guidelines of the American thyroid association for the diagnosis and management of thyroid disease during pregnancy and postpartum. Thyroid. 2017;27(3):315–389. doi:10.1089/thy.2016.0457
2. Vanderpump MPJ. The epidemiology of thyroid disease. Br Med Bull. 2011;99:39–51. doi:10.1093/bmb/ldr030
3. Teng W, Shan Z, Patil-Sisodia K, Cooper DS. Hypothyroidism during pregnancy. Lancet Diabetes Endocrinol. 2013;1(3):228–237. doi:10.1016/S2213-8587(13)70109-8
4. Rao VRC, Lakshmi A, Sadhnani MD. Prevalence of hypothyroidism in recurrent pregnancy loss in first trimester. Indian J Med Sci. 2008;62(9):357–361. doi:10.4103/0019-5359.43122
5. Wang J, Gong XH, Peng T, Wu JN. Association of thyroid function during pregnancy with the risk of pre-eclampsia and gestational diabetes mellitus. Endocr Pract. 2021;27(8):819–825. doi:10.1016/j.eprac.2021.03.014
6. Lee SY, Cabral HJ, Aschengrau A, Pearce EN. Associations between maternal thyroid function during pregnancy and obstetric and perinatal outcomes. J Clin Endocrinol Metab. 2020;105(5):e2015–23. doi:10.1210/clinem/dgz275
7. Kumar R, Bansal R, Shergill HK, Garg P. Prevalence of thyroid dysfunction in pregnancy and its association with feto-maternal outcomes: a prospective observational study from a tertiary care institute in Northern India. Clin Epidemiol Glob Health. 2023;19:101201. doi:10.1016/j.cegh.2022.101201
8. Stagnaro-Green A, Abalovich M, Alexander E, et al. Guidelines of the American thyroid association for the diagnosis and treatment of thyroid disease during pregnancy and postpartum. Thyroid. 2011;21(10):1081–1125. doi:10.1089/thy.2011.0087
9. Nwabudike P, Emokpae MA. Thyroid dysfunction among hypertensive pregnant women in Warri, Delta State, Nigeria. Medicines. 2022;9(4). doi:10.3390/medicines9040029
10. Allan WC, Haddow JE, Palomaki GE, et al. Maternal thyroid deficiency and pregnancy complications: implications for population screening. J Med Screen. 2000;7(3):127–130. doi:10.1136/jms.7.3.127
11. Yassaee F, Farahani M, Abadi AR. Prevalence of subclinical hypothyroidism in pregnant women in Tehran-Iran. Int J Fertil Steril. 2014;8(2):163–166.
12. Gupta P, Jain M, Verma V, Gupta NK. The study of prevalence and pattern of thyroid disorder in pregnant women: a prospective study. Cureus. 2021;13(7):e16457. doi:10.7759/cureus.16457
13. Mahadik K, Choudhary P, Roy PK. Study of thyroid function in pregnancy, its feto-maternal outcome; a prospective observational study. BMC Pregnancy Childbirth. 2020;20(1):769. doi:10.1186/s12884-020-03448-z
14. LeBeau SO, Mandel SJ. Thyroid disorders during pregnancy. Endocrinol Metab Clin North Am. 2006;35(1):117. doi:10.1016/j.ecl.2005.09.009
15. Adoueni VK, Azoh AJC, Kouame E, et al. Prevalence and correlates of hypothyroidism in pregnancy: a cross-sectional study at Bouget General Hospital, Ivory Coast. Pan Afr Med J. 2022;41:37. doi:10.11604/pamj.2022.41.37.32553
16. Abdulslam K, Yahaya I. Prevalence of thyroid dysfunction in gestational hypertensive Nigerians. Sub Saharan Afr J Med. 2015;2(1):19. doi:10.4103/2384-5147.151569
17. Maraka S, Ospina NMS, O’Keeffe DT, et al. Subclinical Hypothyroidism in Pregnancy: a systematic review and meta-analysis. Thyroid. 2016;26(4):580–590. doi:10.1089/thy.2015.0418
18. Toloza FJK, Abedzadeh-Anaraki S, Maraka S. Subclinical hypothyroidism in pregnancy. Curr Opin Endocrinol Diabetes Obes. 2019;26(5):225–231. doi:10.1097/MED.0000000000000491
19. Businge CB, Longo-Mbenza B, Kengne AP. The prevalence of insufficient iodine intake during pregnancy in Africa: protocol for a systematic review and meta-analysis. Syst Rev. 2019;8(1):209. doi:10.1186/s13643-019-1092-7
20. Kassim IAR, Moloney G, Busili A, et al. Iodine intake in Somalia is excessive and is associated with the source of household drinking water. J Nutr. 2014;144(3):375–381. doi:10.3945/jn.113.176693
21. Shun CB, Donaghue KC, Phelan H, Twigg SM, Craig ME. Thyroid autoimmunity in Type 1 diabetes: systematic review and meta-analysis. Diabet Med. 2014;31(2):126–135. doi:10.1111/dme.12318
22. Dong AC, Morgan J, Kane M, Stagnaro-Green A, Stephenson MD. Subclinical hypothyroidism and thyroid autoimmunity in recurrent pregnancy loss: a systematic review and meta-analysis. Fertil Steril. 2020;113(3):587–600.e1. doi:10.1016/j.fertnstert.2019.11.003
23. Stagnaro-Green A. Maternal thyroid disease and preterm delivery. J Clin Endocrinol Metab. 2009;94(1):21–25. doi:10.1210/jc.2008-1288
24. Parizad Nasirkandy M, Badfar G, Shohani M, et al. The relation of maternal hypothyroidism and hypothyroxinemia during pregnancy on preterm birth: an updated systematic review and meta-analysis. Int J Reprod Biomed. 2017;15(9):543–552.
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.