Back to Journals » Cancer Management and Research » Volume 14
Prevalence, Distribution, and Histopathological Features of Malignant Tumors Reported at Tertiary Level in Afghanistan: A 3-Year Study
Authors Malakzai HA ![]() , Haidary AM
, Haidary AM ![]() , Gulzar S, Haidari M
, Gulzar S, Haidari M ![]() , Ibrahimkhil AS, Saadaat R, Hakimi A, Sadat Hofiani SM, Rahmani S, Abdul-Ghafar J
, Ibrahimkhil AS, Saadaat R, Hakimi A, Sadat Hofiani SM, Rahmani S, Abdul-Ghafar J ![]()
Received 14 June 2022
Accepted for publication 23 August 2022
Published 30 August 2022 Volume 2022:14 Pages 2569—2582
DOI https://doi.org/10.2147/CMAR.S377710
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Harikrishna Nakshatri
Haider Ali Malakzai,1 Ahmed Maseh Haidary,1 Saleema Gulzar,2 Mujtaba Haidari,1 Abdul Sami Ibrahimkhil,3 Ramin Saadaat,1 Ahmadullah Hakimi,1 Sayed Murtaza Sadat Hofiani,4 Soma Rahmani,5 Jamshid Abdul-Ghafar1
1Department of Pathology and Clinical Laboratory, French Medical Institute for Mothers and Children (FMIC), Kabul, Afghanistan; 2School of Nursing and Midwifery, Aga Khan University (AKU), Karachi, Pakistan; 3Central Public Health Laboratories (CPHL), Kabul, Afghanistan; 4Department of Academics and Research, Postgraduate Medical Education (PGME), French Medical Institute for Mothers and Children (FMIC), Kabul, Afghanistan; 5World Health Organization (WHO), United Nations Office for the Coordination of Humanitarian and Economic Assistance Programmes Relating to Afghanistan (UNOCA) Compound, Kabul, Afghanistan
Correspondence: Jamshid Abdul-Ghafar, Tel +93 792827287, Email [email protected]
Purpose: Cancer is one of the leading causes of mortality and morbidity, and therefore, tremendous research work is continuously being done around the world with consideration of etiopathogenesis as well as identification of therapeutic targets. Decades of continuous war in Afghanistan has left the medical infrastructure of the country in a miserable situation. There is a serious deficiency in research work in the fields of pathology and oncology at the moment with minimal data available to elaborate about the demographic characteristics of various malignant disorders in the country, which would be indispensable to pave the way for further research and development.
Patients and Methods: A descriptive cross-sectional study was conducted to describe the prevalence, distribution, and important histopathological features of malignant tumors reported at tertiary level in Afghanistan.
Results: Out of 2328 consecutive cases of solid malignant tumors included in our study, 93.8% were primary and 6.2% were metastatic. Breast was the most common site of origin for primary malignancy (29.5%) in females; however, in males, esophagus was the leading site for primary malignant tumors (16.3%). Invasive ductal carcinoma was the most common histologic type of malignancy in females (87.9%). However, in both genders, squamous cell carcinoma of esophagus and skin, osteosarcoma of bone and soft tissue, and glioblastoma of central nervous system were the most common histologic types of malignancies diagnosed. Small intestine was a frequently involved site affected by extranodal non-Hodgkin lymphomas. Overall, the majority of the cancers were diagnosed in stage-II.
Conclusion: Findings in our study were somewhat similar to data presented elsewhere in the world, with some significant differences that could be related to the local factors. Our study revealed that most of the malignant tumors were diagnosed in later stages of the disease, attributable to scarcity of specialized oncology institutions and public awareness.
Keywords: cancer, prevalence, lymphoma, sarcoma, Afghanistan
Introduction
Cancer is one of the leading causes of mortality and morbidity around the globe.1 Among non-communicable diseases (NCDs), malignant tumors constitute the second leading cause of death worldwide, following cardiovascular diseases (CVDs).1,2 According to the global mortality data (2019), for every ten persons dying of NCDs, three premature deaths occur due to cancer.2 It was responsible for 9.43 million deaths in year 2016, followed by an estimated 9.6 million deaths in 2018, globally.3,4 Recently, this number has risen to 10.0 million deaths according to an estimation in the year 2020, of which, 5.5 million deaths occurred in male and 4.4 million deaths in female population with an incidence of 19.3 million new cases worldwide.5
According to the Global Cancer Observatory (GLOBOCAN) cancer statistics for the year 2020, the leading ten most common cancers in male population globally were lung malignancies (14.3%), prostate cancers (14.1%), non-melanoma skin cancers (7.2%), stomach cancer (7.1%), liver cancer (6.3%), colon cancer (6.0%), bladder cancer (4.4%), cancer of the rectum (4.4%), esophageal cancer (4.2) and non-Hodgkin lymphoma (3.0%), while in females, it included malignancies of the breast (24.5%), lung (8.4%), uterine cervix (6.5%), colon (5.9%), non-melanoma cancers of skin (5.2%), thyroid (4.9%), uterine corpus (4.5%), stomach (4.0%), ovary (3.4%), and rectum (3.1%).5
According to the World Health Organization (WHO), most of the people with cancer live in low and middle income countries, and the overall cancer survival rates in the developed countries are higher than in the developing countries, such as Afghanistan.6 In 1968, Leslie H. Sobin was the first person to carry-out a cross-sectional descriptive study entitled “Cancers in Afghanistan”, based on the country’s tumor registry, that included 895 histologically diagnosed benign and malignant neoplasms.7 The aim of the study was to determine the relative frequency of these neoplasms in Afghanistan, and to compare them with the then-published data from Iran, Pakistan, and Sweden.7 The study found that the majority of cancers in Afghans at accessible sites of the body were skin, hemolymphoid, soft tissues, eye, breast and testis, while at the deeper sites, the most frequent cancers were in stomach, esophagus and ovary.7 The results showed that mouth and uterine cervix cancers were of relatively low frequency.7 According to the investigator, this was an important finding and stated that certain conditions exist in Afghanistan which are usually associated with higher tumor frequencies.7 Considering the malignant neoplasms, the study revealed that in males, skin cancer was the most frequently diagnosed malignancy (17.4%), followed by lymphoma (12.3%), eye cancer (7.2%), soft tissue cancer (7.2%) and stomach cancer (5.9%).7 In female population, breast cancer (15.2%) was the commonest malignant tumor, followed by skin cancer (14.1%), soft tissue cancer (9.6%), ovarian cancer (6.8%) and lymphoma (6.2%).7
For more than 4 decades of continued war in the country, Afghanistan’s health infrastructure has been severely devastated which has led to the lack of advanced diagnostic and therapeutic facilities for malignant disorders, thus, the majority of Afghans go to the neighboring countries for treatment.8 In addition to that, Afghanistan is ranked 41st on the list of the world’s most populous countries and “middle-age” of Afghans is estimated 18.4 years, which reveals the elevated growth rate of the population is about 2.32%.9 Correspondingly, the data also show an elevated birth rate of about 38.57/1000 population, and death rate of an estimated 13.89 deaths/100,000 population.9 Contribution of these factors together lead to decreased life expectancy rate of 51 years among Afghans.9 The gross domestic product spent on the health care system in the country is about 8.5%, which does not meet the criteria for actual welfare.9 In addition to that, the density of physicians in Afghanistan is about 0.27 physicians/1000 population and the availability of 0.5 hospital beds/1000 population, that is very much different compared to the United States’ statistics of physician density and hospital beds density, which comprise 2.45 physicians/1000 population and 2.9 beds/1000 population, respectively.9 Beside these factors, the main causes leading to increased cancer incidence and mortality in Afghanistan are the lack of public awareness of preventive measures and the deficiency of cancer policies and registries at national level.9
Materials and Methods
A cross-sectional descriptive study was conducted with the aim to achieve the study goal and objectives at Histopathology section, Department of Pathology and Clinical Laboratory, French Medical Institute for Mothers and Children (FMIC). All histologically diagnosed cases of solid malignant tumors via routine Hematoxylin and Eosin (H&E) staining and a limited number of immunohistochemical (IHC) staining at this center were included in the study, in a time span of three years (beginning of 2018 to the end of 2020). The data were collected from patients’ records in the Integrated Laboratory Management System (ILMS) database of the FMIC. Statistical Package for Social Sciences (SPSS) application, version 25, was used for data analysis. Considering the type of data, frequencies and proportions were used for calculating categorical variables, while mean and median were used to describe continuous variables. The study was approved by the Ethical Research Committee (ERC) of FMIC (91-FMIC-ER-20).
Results
In our study, 2328 consecutive cases of solid malignant tumors were included, of which, 2183 (93.8%) tumors were primary and 145 (6.2%) were metastatic. We found that the mean and median ages of patients diagnosed with malignant tumors were 48 and 50 years, respectively. In the primary malignant tumors, breast was the most common origin for malignancy, constituting 323 (14.8%) cases, followed by esophagus 285 (13.1%), skin 237 (10.9%), bone and soft tissue 169 (7.7%) and colorectum 165 (7.5%), as shown in Table 1.
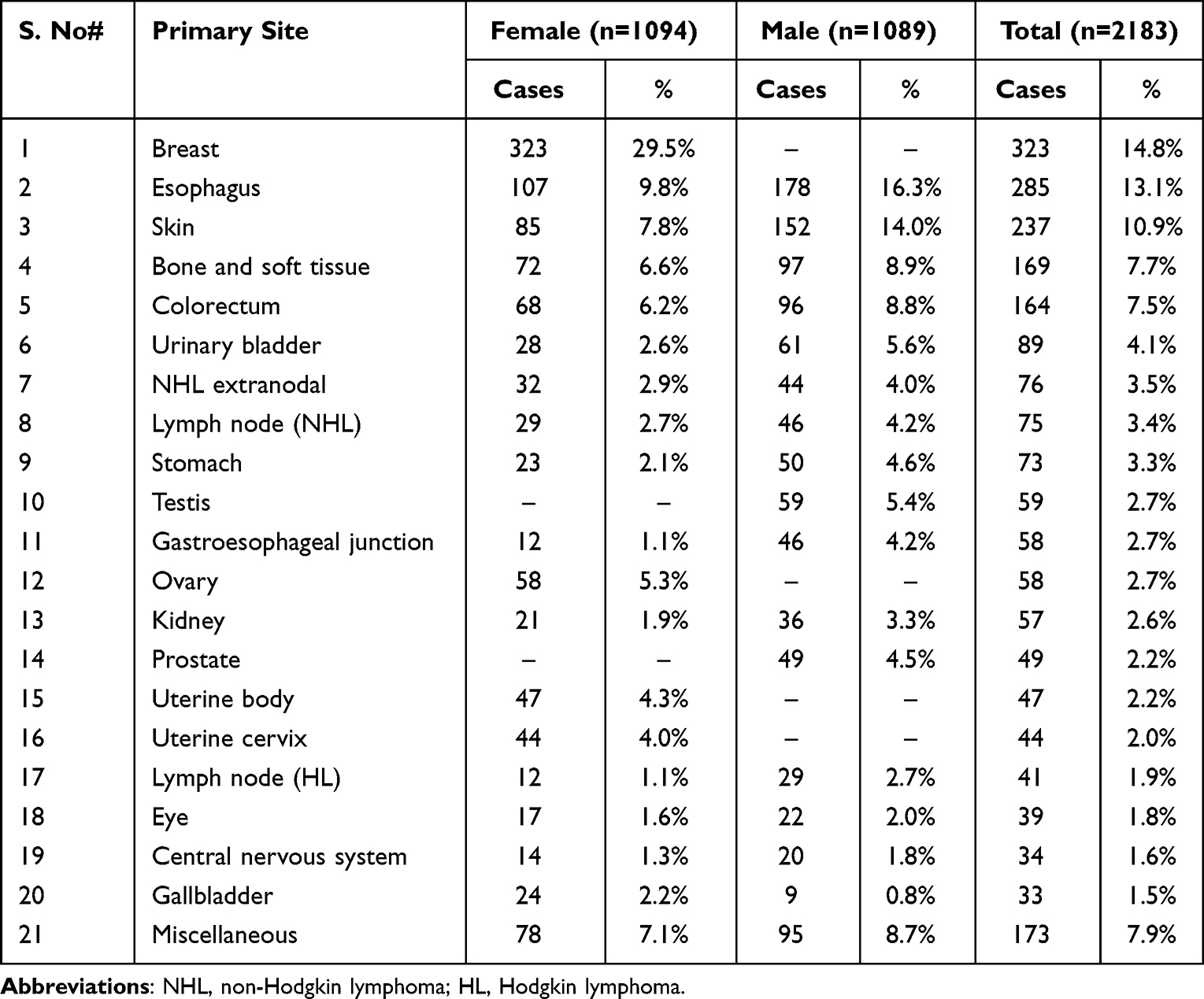 |
Table 1 Frequently Involved Primary Sites of Malignant Tumors in Both Genders (n=2183) |
In females, breast was the most frequently involved site for primary malignancy, constituting 323 (29.5%) of 1094 cases, followed by esophagus, skin, bone and soft tissue, colorectum, ovary, uterine body and uterine cervix; each constituting 107 (9.8%), 85 (7.8%), 72 (6.6%), 68 (6.2%), 58 (5.3%), 47 (4.3%) and 44 (4.0%) cases, respectively, as shown in Table 2.
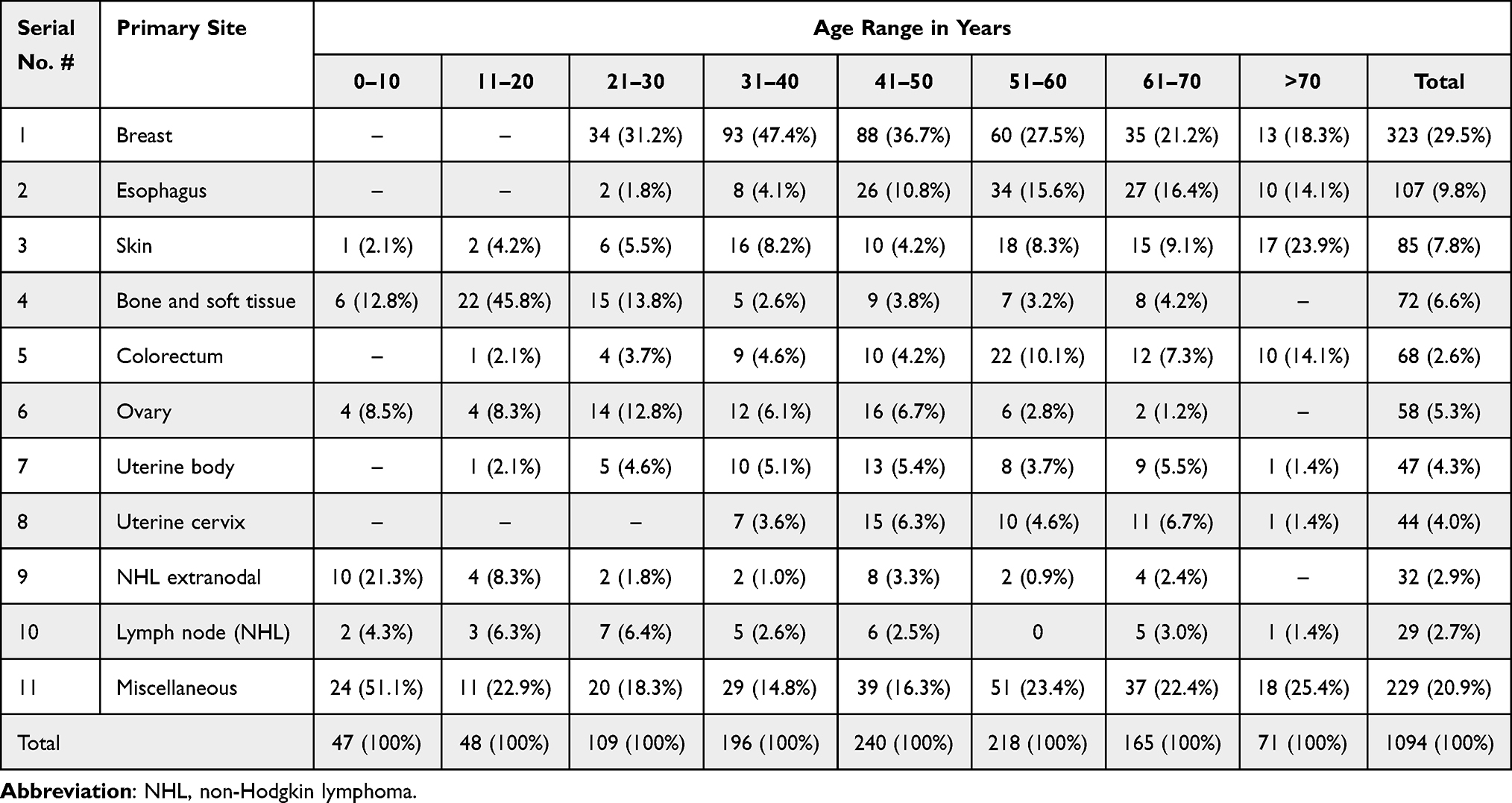 |
Table 2 Decade-Wise Age Distribution of Common Primary Malignant Tumors in Females (n=1094) |
In males, esophagus was the most common site of primary malignant tumors, constituting 178 (16.3%) of 1089 cases, followed by skin, bone and soft tissue, colorectum, urinary bladder, testis, stomach and prostate; each constituting 152 (14.0%), 97 (8.9%), 96 (8.8%), 61 (5.6%), 59 (5.4%), 50 (4.6%) and 49 (4.5%) cases, respectively, as shown in Table 3.
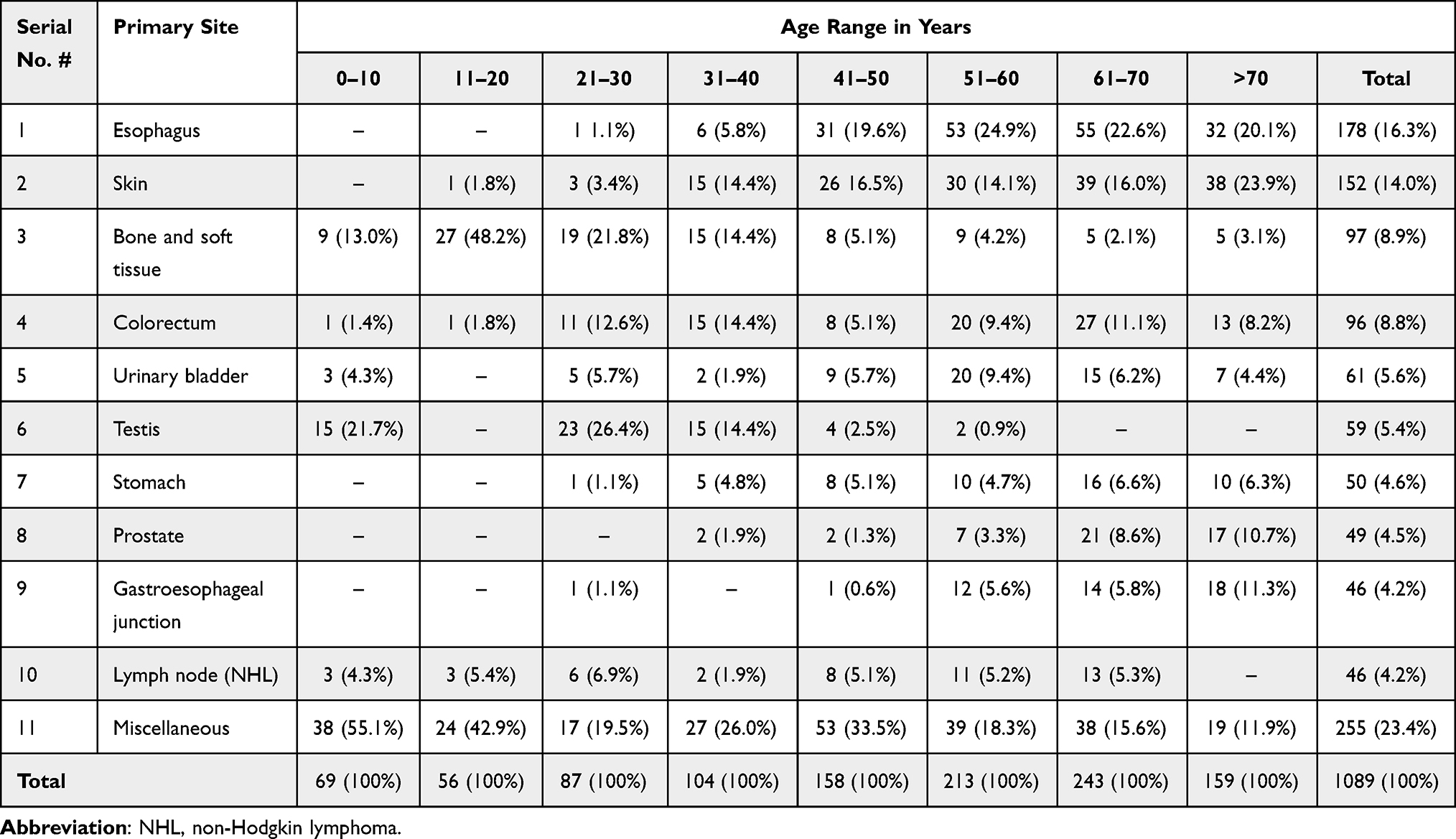 |
Table 3 Decade-Wise Age Distribution of Common Primary Malignant Tumors in Males (n=1089) |
With regards to the female gender, malignancies of the breast were common in the fourth and fifth decades of life, esophageal malignancies were common between the fifth and seventh decades, skin related malignancies were common in fourth, sixth and above seventh decades, bone and soft tissue malignancies were common in the second and third decades, colorectal malignancies were common in the sixth decade, ovarian malignancies were common in the third and fifth decades, malignancies of the uterine body were common in the fifth decade, malignancies of the uterine cervix were common in the fifth decade, extranodal involvement of NHL was common in the first and fifth decades and nodal NHL involvement was common in the third and fifth decades of life, as shown in Table 2. The mean and median ages at diagnosis of primary malignancies in female patients were 46 and 48 years, respectively.
With regards to the male gender, malignancies related to esophagus were common in the sixth and seventh decades, malignancies related to the skin were common between sixth and above seventh decades, malignancies of the bone and soft tissue were common between second and fourth decades, colorectal malignancies were common in the sixth and seventh decades, malignancies of the urinary bladder were common in the sixth and seventh decades, malignancies of the testis were common in the first, third and fourth decades, malignancies of the stomach and prostate were common in the seventh decade, malignancies of the gastroesophageal junction were common in the seventh and above seventh decades, and lymph node involvement of NHL was common in the sixth and seventh decades of life, as shown in Table 3. The mean and median ages at diagnosis of primary malignancies in male patients were 50 and 55 years, respectively.
Considering the histological type of malignant breast tumors in females, invasive ductal carcinoma (IDC) was the most common type of malignancy, constituting 284 (87.9%) of 323 cases, followed by metaplastic carcinoma, invasive lobular carcinoma (ILC), mucinous adenocarcinoma, ductal carcinoma in-situ, sebaceous carcinoma, malignant Phyllodes tumor, angiosarcoma, micropapillary carcinoma, medullary carcinoma and fibrosarcoma, as shown in Figure 1. Based on histological grading of IDC and ILC of the breast, grade-II was the most common grade, comprising 110 (37.7%) cases, followed by grade-III: 105 (36%) cases and grade-I: 77 (26.4%) cases, as shown in Figure 2.
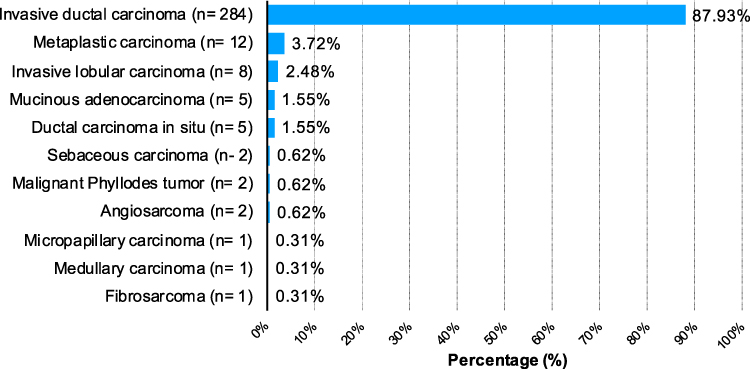 |
Figure 1 Histologic types of malignant breast tumors in females (n=323). |
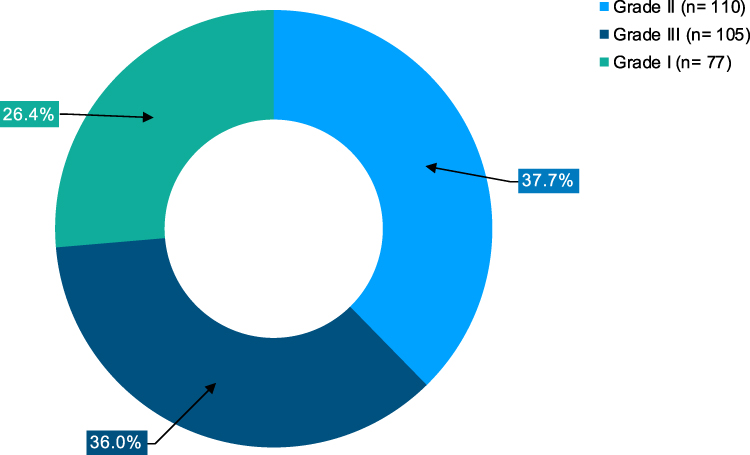 |
Figure 2 Histologic grades of invasive mammary carcinomas of female breast (n=292). |
Considering the histological type of esophageal carcinoma in both the genders, SCC was the most common type of cancer, constituting 220 (77.1%) out of 285 cases, followed by adenocarcinoma (AC), small cell carcinoma, signet ring cell carcinoma and neuroendocrine carcinomas, as shown in Figure 3.
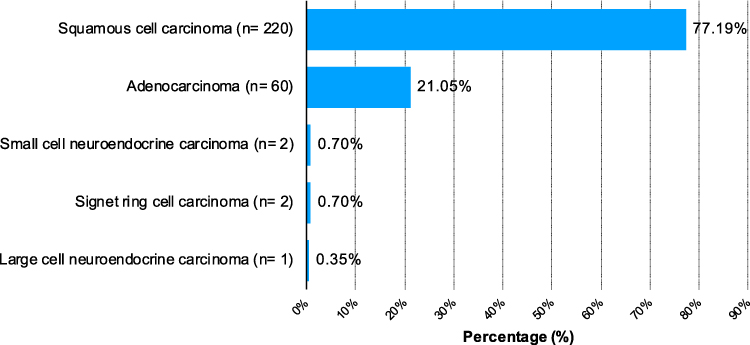 |
Figure 3 Histologic types of esophageal carcinoma in both genders (n=285). |
Similarly, with consideration of the histologic type of malignant skin tumors in both the genders, SCC was the most common type of skin cancer, constituting 132 (55.7%) of 237 cases, followed by basal cell carcinoma (BCC), melanoma, basosquamous carcinoma, dermatofibrosarcoma protuberans (DFSP), sebaceous carcinoma and mucinous adenocarcinoma, as shown in Figure 4.
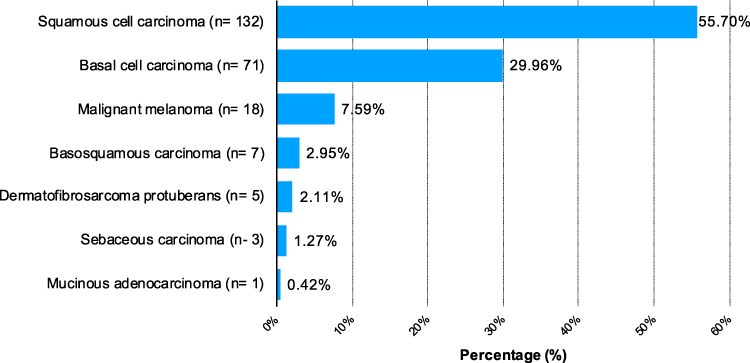 |
Figure 4 Histologic types of malignant skin tumors in both genders (n=237). |
Considering the histologic type of bone and soft tissue malignancies, in both the genders, osteosarcoma was the most common type of diagnosis, constituting 43 (25.4%) of 169 cases, followed by rhabdomyosarcoma, Ewing’s sarcoma, synovial sarcoma, chondrosarcoma, malignant peripheral nerve sheath tumor (MPNST), leiomyosarcoma, fibrosarcoma, liposarcoma, alveolar soft part sarcoma, myxofibrosarcoma, epithelioid sarcoma, angiosarcoma, Kaposi sarcoma and desmoplastic small round cell tumor (DSRCT), as shown in Figure 5.
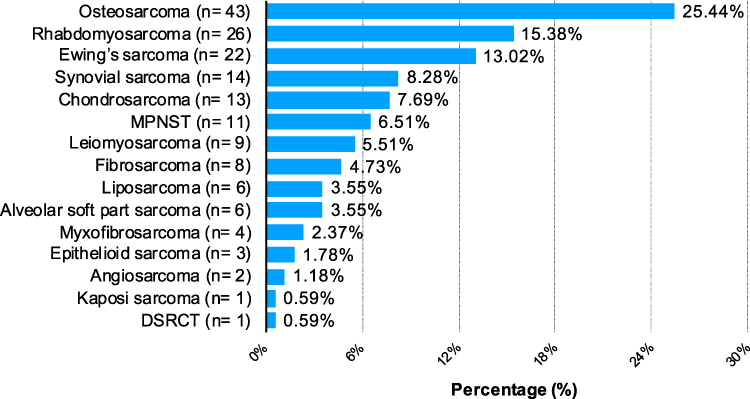 |
Figure 5 Histologic types of malignant bone and soft tissue tumors in both genders (n=169). Abbreviations: MPNST, malignant peripheral nerve sheath tumor; DSRCT, desmoplastic small round cell tumors. |
With regards to the malignant Central Nervous System (CNS) tumors in both the genders, glioblastoma (WHO grade-IV) was the most common diagnosis, constituting 20 (58.9%) cases of 34, followed by anaplastic ependymoma (WHO grade III), anaplastic oligodendroglioma (WHO Grade III), anaplastic meningioma (WHO Grade III), medulloblastoma (WHO Grade IV), anaplastic astrocytoma (WHO Grade III) and primitive neuroectodermal tumors (WHO Grade IV), as shown in Figure 6.
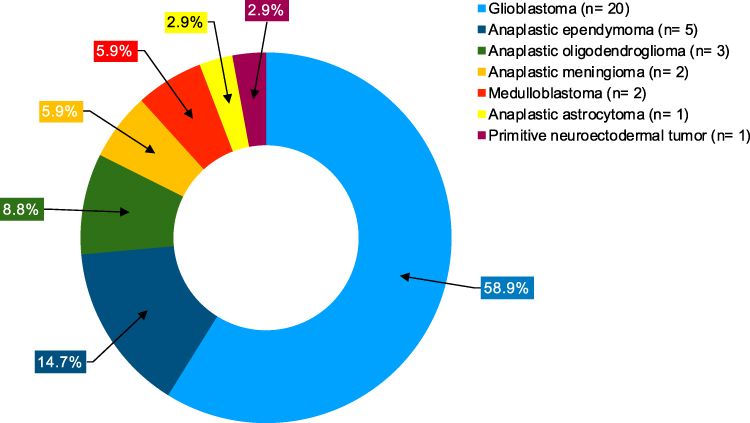 |
Figure 6 Histologic types of malignant CNS tumors in both genders (n=34). |
With consideration of extranodal involvement for NHL, in both the genders, small intestine was the most common site of involvement (36.6%), followed by skin, ovary, testis, nasopharynx, stomach and pleura, as shown in Figure 7.
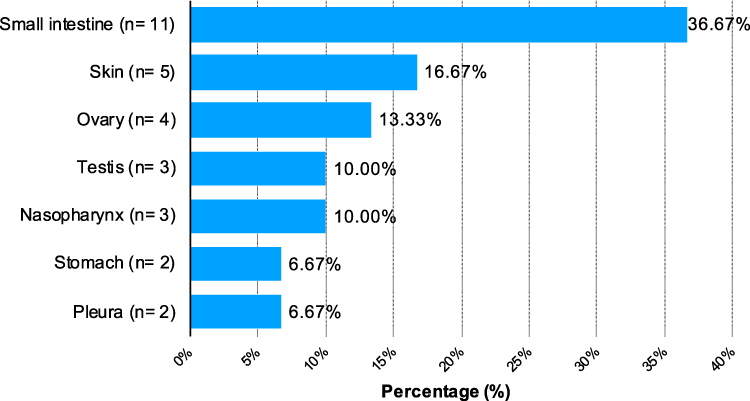 |
Figure 7 Sites involved by extranodal non-Hodgkin lymphoma in both genders (n=30). |
As shown in Figure 8, with consideration of the clinical stage of the disease at diagnosis, 357 of 2183 primary tumor cases of variable sites (gastrointestinal tract, genital tract, eye, urinary tract) with available stage calculations in both the genders were included. Most of the tumors were diagnosed in stage-II, followed by stage-III, stage-I and stage-IV; each constituting 131 (36.7%), 119 (33.3%), 56 (15.7%) and 51 (14.3%) cases, respectively. However, no T-is stage tumor was diagnosed in this period.
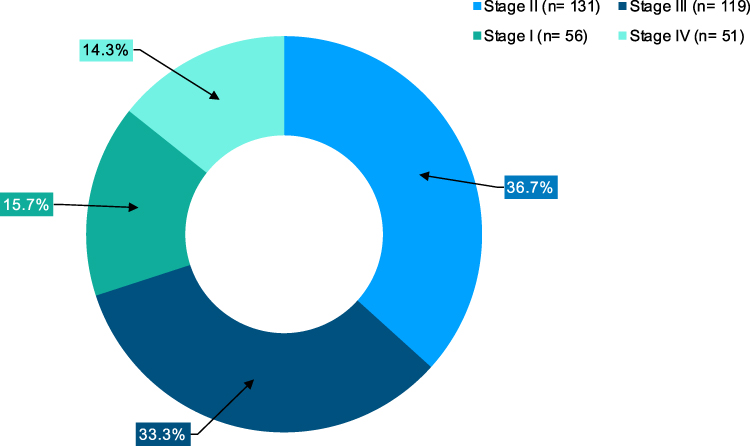 |
Figure 8 Stages of primary malignant tumors in both genders (n=357). |
With regards to the side of involvement, IDC, renal cell carcinoma (RCC) and serous cystadenocarcinoma were dominant on the left side, while seminoma was more often involving the right testis. There was no significant difference between left and right sides involvement for retinoblastoma, as shown in Table 4.
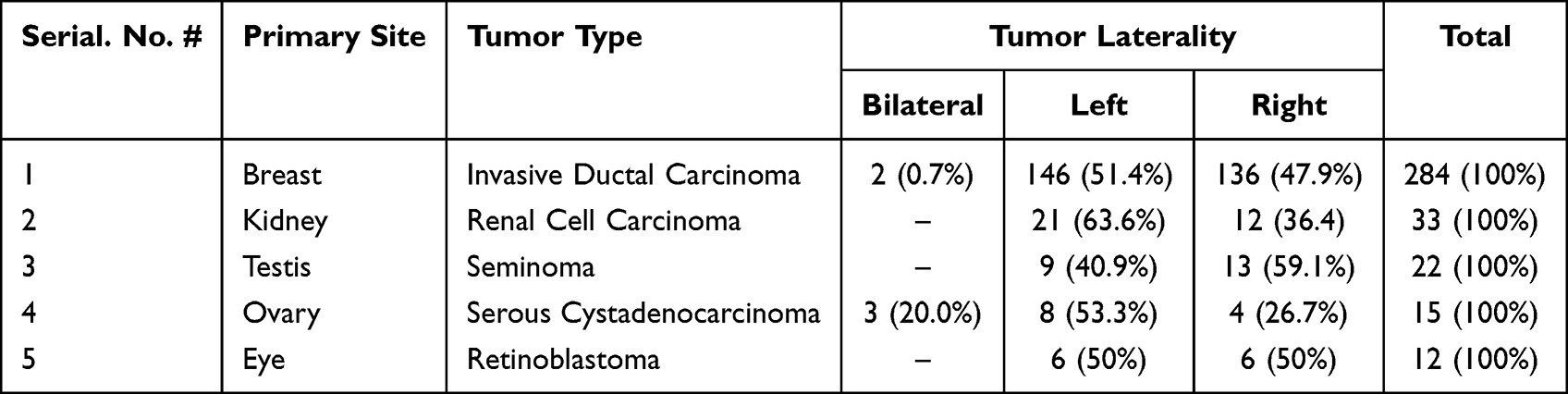 |
Table 4 Common Malignant Tumor Types with Primary Sites and Laterality (n=366) |
Excisional biopsy was the most common type of biopsy technique which was used in 797 (36.5%) of 2183 cases, followed by total organ resection, endoscopic biopsy, incisional biopsy, core needle biopsy, punch biopsy, curettage, transurethral resection of bladder tumor (TURBT) and transurethral resection of the prostate (TURP), as shown in Figure 9.
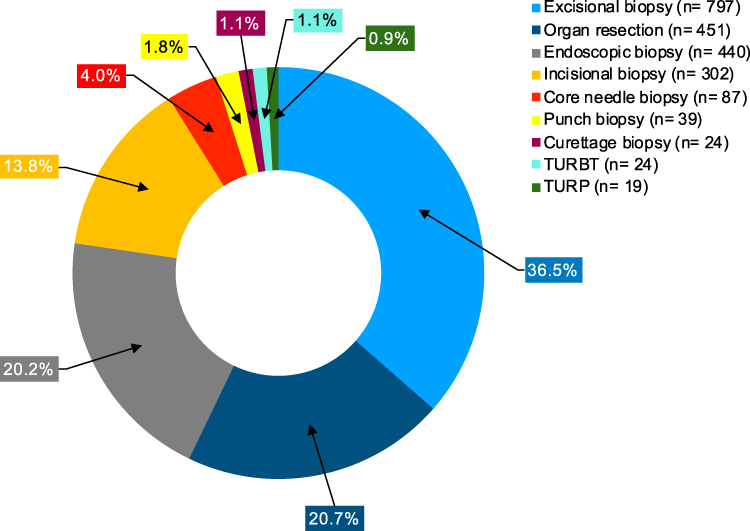 |
Figure 9 Common biopsy techniques for sampling primary malignant tumors (n=2183). Abbreviations: TURBT, transurethral resection of bladder tumor; TURP, transurethral resection of the prostate. |
Discussion
Prevalence and Gender Distribution
Our study revealed that the top 10 primary sites of malignant tumors in both males and females comprised breast, esophagus, skin, bone and soft tissue, colorectum, urinary bladder, extranodal NHL, nodal NHL, stomach and testis. In females, breast was the most frequent primary site affected by malignancy followed by esophagus, while in males, esophagus was on the top followed by skin cancers, which was similar when compared to a study conducted by Joya et al, in Kabul Afghanistan, where they also demonstrated that breast was the most common site for malignancies in females followed by esophagus, while in males, esophagus was the leading cancer site followed by stomach.6 In addition to that, a study by Ahmad Javid Safi in 2019, also revealed that breast cancer was the leading malignancy in Afghanistan followed by stomach cancer, and added that the lack of public awareness about the risk factors of such malignancies, lack of basic education and the lack of treatment facilities could be the reasons behind the existence of these tumors in large numbers in Afghanistan.9
In the majority of the international literature, breast cancer has been shown to be the most frequently diagnosed malignancy in female population, while in males, a variety in the leading sites and types of cancers have been reported by various researchers. In the neighboring country Pakistan, a study by Ahmed et al, revealed that breast carcinoma was the most frequently diagnosed cancer followed by esophageal cancer, however in males, they found that oral cavity cancers were the commonest followed by lymphomas.10 In comparison to our study, it was similar in females but very much different in males, as oral cavity cancers were not even in the top 10 cancers in male patients. The high prevalence of oral cavity cancers could be attributed to the high prevalence of consumption of “Paan” in Pakistani population, which is not practiced in Afghanistan.
The Surveillance, Epidemiology and End Results (SEER) 9 registries in 2010 also revealed that breast was the leading cancer site in females; however, prostate was the most common site in male population in the United States of America.11 In our study, prostate cancer was in 8th position in the most common cancers list in males.
Age Distribution
Our study revealed that the majority of cancers diagnosed in females were inbetween 4th and 6th decades of life, however in males, cancers were common inbetween 5th and 7th decades of life. The findings support the results that were obtained by a previous study conducted by Joya et al, in Kabul Afghanistan, showing that malignancies in female patients were frequently diagnosed in 4th and 5th decades of life, and in male patients it was the 5th, 6th and 7th decades of life in order of the high frequency for cancer diagnosis.6
In comparison, a study by Ahmad et al, in Pakistan, revealed that overall cancers were common in older ages between 4th and 7th decades of life in both genders.10 The study’s results also elaborated that in females, cancers were commonly diagnosed inbetween 4th and 6th decades of life, and in males, the frequency rose slightly higher in patients aged between 5th and 7th decades of life.10
Histologic Types and Grades of Tumors
Based on the histologic types of female breast malignancies in our study, IDC was the most frequently diagnosed histologic type comprising 284 (87.9%) cases followed by metaplastic carcinoma, ILC, mucinous adenocarcinoma and other histologic types, including primary sarcomas. These findings closely resemble the results obtained by Oluogun et al, in a study in Nigeria, which also revealed that IDC was the leading histologic type of breast cancer (88.9%), followed by ILC, medullary carcinoma and mucinous carcinoma.12 Our study’s findings were also in agreement with Ahmad et al, who found that IDC was the most commonly diagnosed histologic type of breast cancer with a slight difference in types of cancers.10 They revealed that IDC was followed by ILC and metaplastic carcinoma in order of frequency; however in our study, IDC was followed by metaplastic carcinoma in the 2nd position and ILC was in 3rd.10
In consideration of tumor grading, histologic grades of IDC and ILC were included in our study, showing that grade-II tumors were on the peak, followed by grade-III and grade-I tumors in order of frequency. These results were comparable to the findings in a study by Metzger-Filho et al, which revealed that grade-II tumors, comprising 61.3%, were the most common, followed by grade-I and grade-III. The results revealed agreement in leading grade of tumor with our study; however, the findings in their study showed that grade-I and grade-III tumors were followed by grade-II tumors in order of frequency.13
Esophageal carcinoma was the most common malignancy in males, in our study, however, it was the second leading cancer following breast malignancies in female population. In a previous study, it was demonstrated to be the 8th most common cancer around the globe and the 6th most common cause of death among cancer related deaths in the world.14 SCC often occurred in the upper and middle parts of the esophagus, while AC was frequently diagnosed in the lower third of esophagus.14 SCC was still the leading histologic type of esophageal carcinoma in the world, and it was also the histological type that was responsible for the majority of deaths occurring from esophageal cancer.14,15 However, in the western world, especially in Caucasian males, the recent incidence of AC has replaced SCC in order of frequency.14 In our study, the findings showed that SCC was the most common histologic type of esophageal cancer, followed by AC, which was different from the data of the western countries and was following the rest of the world in terms of the leading histologic types of esophageal cancer.
Skin was another important primary site for variable types of malignancies. According to the findings in our study, it was the second most common site for primary malignant tumors in males following esophagus and third most common site in female population following breast and esophagus. Cutaneous malignancies are usually classified into malignant melanoma and non-melanoma skin cancers (NMSC) categories, the latter includes the leading histologic types of skin cancers comprising SCC and BCC as major subtypes.16 In NMSC, BCC is known to be the commonest subtype that constitutes 80% of the NMSC diagnosed in the United States of America (USA) annually.17 SCC is the second most frequently occurring subtype of NMSC and despite its low frequency compared to BCC, the mortality rate of SCC is higher than that of BCC in the USA.17 Malignant melanoma is another common skin cancer which comprises 4.6% of newly diagnosed cancer in the USA that is in fifth position in males and sixth in females considering the frequency of diagnosis.17 According to our study’s results, SCC was the most common cutaneous malignancy followed by BCC and malignant melanoma, that was different from the epidemiologic findings in the USA and other western countries, where BCC is the major histologic type of skin malignancies, probably due to the skin pigmentation of individuals, inherent genetic variabilities and sociocultural differences, as BBC commonly arises in light and fair skin that is vulnerable to ultraviolet exposure.18 In contest of Asia, a study done by Laishram et al, in Manipur State of India, revealed identical findings to our study, as they showed that out of 92 histologically diagnosed skin malignancies, SCC was the most commonly diagnosed cancer type, comprising 43.6%, followed by BCC 32.6%, and malignant melanoma 14.2%.19
Down to the fourth position, malignant bone and soft tissue tumors comprised another important category of tumors in our study, accounting for 169 (7.7%) of 2183 primary malignant tumors that we diagnosed, in which, 72 (6.6%) cases were related to females and 97 (8.9%) cases to males. Osteosarcoma was the most common diagnosis among malignant bone and soft tissue tumors in our study, followed by rhabdomyosarcoma, Ewing’s sarcoma, synovial sarcoma and chondrosarcoma. Our findings were somewhat similar when compared to the findings of a study conducted by Oztürk et al, in Turkey; they also demonstrated that osteosarcoma was the leading bone malignancy followed by Ewing’s sarcoma and chondrosarcoma, however in soft tissue malignancies, they showed that liposarcoma was the commonest followed by synovial sarcoma and malignant mesenchymal tumors, which was different from our findings, as mentioned previously.20
The primary malignant tumors of central nervous system were relatively uncommon comprising only 2% of all cancers; however, despite the application of proper treatment protocols, it causes significant morbidity and mortality worldwide.21 Studies revealed that the overall incidence of primary malignant central nervous system tumors has increased recently with the incidence rate of 3.4 per 100,000 population globally.21 In agreement with that, primary malignant CNS tumors were less common compared to other cancers in our study, and were in 19th position in order of frequency. Only 34 cases of high grade primary malignant CNS tumors were included in which it was demonstrated that glioblastoma (WHO grade-IV) was the leading histologic type of malignant CNS tumor, followed by anaplastic ependymoma (WHO grade-III) and anaplastic oligodendroglioma (WHO grade-III).
A study in Pakistan by Ahmad et al, revealed glioblastoma to be the most frequently diagnosed histologic type of CNS malignancy, followed by anaplastic oligodendroglioma and medulloblastoma.10 These results were similar to the findings in our study with regards to glioblastoma being the commonest histologic type of malignant CNS tumor. Although, they revealed anaplastic oligodendroglioma to be the second most common type of CNS malignancy, which was in 3rd position in order of frequency in our study.
Sites Involved by Extranodal Non-Hodgkin Lymphomas
Our study revealed that extranodal NHL was in 7th position in order of frequency in both the genders. The most common primary site for extranodal NHL was the small intestine, comprising 36.5% of all 30 cases, followed by skin (16.6%), ovary 13.3%, testis and nasopharynx 10% each, and stomach and pleura comprising 6.6% each. These findings were very much different compared to a study conducted by Padhi et al, in India, which revealed that CNS was the most frequently involved site for primary extranodal NHL, constituting 20 (29.5%) cases out of 68, followed by gastrointestinal tract 17 (25%) and nasopharynx 8 (11.8%).22
Tumor Staging
The latest 8th edition of American Joint Committee on Cancer (AJCC) manual guidelines were used for reporting the clinical stage of the tumor, using the Tumor, Nodes and Metastasis (TNM) staging system.23 A total of 357 cases of malignant tumors arising from gastrointestinal tract and its appendages, genital tract including female breast, urinary tract and eye were included. The most frequently present tumors at diagnosis were stage-II tumors, comprising 36.7%, followed by stage-III, stage-I and stage-IV; however, no tumor with T-is stage was present in our database. We hypothesize that the rarity of stage-IV tumors was due the high mortality rate of the stage, financial problems of the patients and lack of oncosurgical facilities in the country. Moreover, the small number of stage-I tumors is probably due to the late visit of patients to the doctors and healthcare professionals for check-ups, low socioeconomical status, low level of basic education among Afghan people and the lack of self-awareness and basic information about the disease in the countryside.
Tumor Laterality
The tumor laterality in our study was considered in five paired organs and their specific malignant tumors including: IDC of female breast, RCC of kidney, seminoma of testis, serous cystadenocarcinoma of ovary, and retinoblastoma of the eye. Our study revealed that IDC, RCC and serous cystadenocarcinomas were slightly dominant on the left side, constituting 51.4%, 63.6% and 53.3%, respectively, while seminoma involved the right testis more often than the left. However, there was no significant difference in left and right sides involvement for retinoblastoma. Cheng et al also found that IDC was slightly dominant on the left side in females in their study.24
The SEER registries between 2010 and 2014 revealed that the right kidney was slightly more involved by RCC (50.6%) than the left kidney which was contradictory to our results that showed a left side dominance.25 The results of our study for seminoma were identical to a study conducted by Beigh et al, which showed that malignant germ cell tumors, including the majority of seminoma cases, were dominant in the right testis.26 Ovarian serous cystadenocarcinoma is well-known for its bilateral ovarian involvement.27 A study by Mondal et al, demonstrated that out of 109 cases, 54 (49.5%) ovarian serous cystadenocarcinomas were bilateral, which was 20% in our study.27 In case of retinoblastoma, Domingo et al supported the results of our study by demonstrating no significant difference in side involvement.28
Common Biopsy Techniques
Our study revealed that various surgical techniques and procedures were applied for tumor biopsies for diagnostic, prognostic and therapeutic purposes by doctors in Afghanistan. Studies have suggested that the effect of an excisional biopsy on patients’ survival is not significantly better than that of an incisional biopsy, despite the therapeutical preference of excisional biopsy procedure.29 However, our findings showed that the most common biopsy procedure was the total excision and total organ resection, when approaching a mass lesion, in Afghanistan. The endoscopic biopsy technique, which is a form of specialized incisional biopsy technique, was in the third position in order of frequency, following open incisional biopsy in second place. Core needle biopsy technique was the fifth most commonly applied technique, which is another specialized type of incisional biopsy technique that requires the expertise of interventional radiologists for sampling soft tissue tumors and tumors involving the internal organs using radiological guidance.30 Punch biopsy technique was concluded to be in sixth position in order of frequency in our study, and is considered to be the most commonly used technique for sampling superficial lesions. The less common biopsy techniques applied in our study were the curettage biopsy technique, TURBT and TURP.
Strengths and Limitations
To the best of our knowledge, the current study has the strength of being the largest scale study ever carried out in terms of the huge number of study participants, to investigate the prevalence and distribution of solid malignant tumors in Afghanistan, until date. Thus, it provides a good picture of the issue and clears the path for implementing future comprehensive and specialized studies regarding malignant disorders in the country.
On the other hand, although this study was conducted in one of the leading diagnostic and therapeutic private tertiary care centers in the country, the generalization of its findings over the whole population of Afghanistan is questionable as it was carried out in a single institution. In addition to that, a small number of undifferentiated and poorly differentiated tumors were excluded from the study due to the limited number of IHC stains and the lack of molecular testing for confirmative diagnosis, which might have affected the internal validity of the research.
Conclusion
Findings of our study regarding the epidemiological characteristics and histopathological features of various solid malignant tumors were more or less similar to the characteristics that have already been elaborated by various researchers and organizations, pertaining to the prevalence, distribution, types and histopathological features of solid organ malignancies diagnosed in other parts of the world. Minor differences that were noted could be explained to be related to the local, socio-economic, dietary and environmental factors, in particular considering the fact that in Afghanistan the majority of the population lives under the umbrella of poverty with minimal supply of vital nutrients in their daily diet.
In our study, breast cancer being reported as the commonest malignancy in female gender was in agreement with the reported data in the majority of international literature; however, a significant variability was seen between our study findings and the data reported from other countries about the most common site and type of cancer in males. In the current study, the most common malignancy in males was esophageal cancer, which should be further investigated in terms of etiopathogenesis and the possible linked demographic characteristics of the Afghan population to the disorder.
Another important finding in our study was the fact that due to lack of availability of specialized healthcare facilities for the majority of the people, most of the malignant tumors were diagnosed in later stages of the disease. Conducting studies to further elaborate about the etiopathogenesis of various malignant tumors and significant changes in healthcare policies to ensure availability of specialized diagnostic and therapeutic facilities for most of the people, would be the key to change the current scenario.
Data Sharing Statement
The raw data used to support the findings of this study have not been made publicly accessible because of patient’ confidentiality and privacy rules; however, it can be shared by the corresponding author upon reasonable request.
Acknowledgments
We would like to acknowledge the role played by Agha Khan Development Network (AKDN), for establishing the country’s first state of the art Pathology department.
Disclosure
All the authors report no conflicts of interest in this work.
References
1. Sung H, Ferlay J, Siegel RL, et al. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 Countries. Ca Cancer J Clin. 2021;71(3):41. doi:10.3322/caac.21660
2. Bray F, Laversanne M, Weiderpass E, Soerjomataram I. The ever‐increasing importance of cancer as a leading cause of premature death worldwide. Cancer. 2021;127(16):3029–3030. doi:10.1002/cncr.33587
3. Mattiuzzi C, Lippi G. Current cancer epidemiology. J Epidemiol Glob Health. 2019;9:217. doi:10.2991/jegh.k.191008.001
4. The Global Cancer Observatory. Cancer fact sheet. World Health Organ; 2019. Available from: https://gco.iarc.fr/today/fact-sheets-cancers.
5. Ferlay J, Colombet M, Soerjomataram I, et al. Cancer statistics for the year 2020: an overview. Int J Cancer. 2021;149(4):778–789. doi:10.1002/ijc.33588
6. Joya M, Stanikzai Z, Akbarzadeh I, Babaloui S, Bradley David A, Jafari SM. Prevalence of cancers diagnosed in Jamhuriyat Hospital, Kabul, Afghanistan. Heliyon. 2020;6(3):e03603. doi:10.1016/j.heliyon.2020.e03603
7. Sobin LH. Cancer in Afghanistan. Cancer. 1969;23(3):678–688. doi:10.1002/1097-0142(196903)23:3<678::AID-CNCR2820230322>3.0.CO;2-4
8. Yusuf MA, Hussain F, Sultan F, Badar F, Sullivan R. Cancer care in times of conflict: cross border care in Pakistan of patients from Afghanistan. ecancermedicalscience. 2020;14. doi:10.3332/ecancer.2020.1018
9. Safi AJ. The Leading Cancer Types in Afghanistan. J Cancer Ther. 2019;10(11):877–881. doi:10.4236/jct.2019.1011074
10. Ahmad Z, Idrees R, Fatima S, et al. Commonest cancers in Pakistan - findings and histopathological perspective from a premier surgical pathology center in Pakistan. Asian Pac J Cancer Prev. 2016;17(3):1061–1075. doi:10.7314/APJCP.2016.17.3.1061
11. Zhang AS, Ostrom QT, Kruchko C, Rogers L, Peereboom DM, Barnholtz-Sloan JS. Complete prevalence of malignant primary brain tumors registry data in the United States compared with other common cancers, 2010. Neuro-Oncol. 2016;now252. doi:10.1093/neuonc/now252
12. Oluogun WA, Adedokun KA, Oyenike MA, Adeyeba OA. Histological classification, grading, staging, and prognostic indexing of female breast cancer in an African population: a 10-year retrospective study. Int J Health Sci. 2019;13(4):7.
13. Metzger-Filho O, Ferreira AR, Jeselsohn R, et al. Mixed invasive ductal and lobular carcinoma of the breast: prognosis and the importance of histologic grade. Oncologist. 2019;24(7):e441–e449. doi:10.1634/theoncologist.2018-0363
14. Abbas G, Krasna M. Overview of esophageal cancer. Ann Cardiothorac Surg. 2017;6(2):131–136. doi:10.21037/acs.2017.03.03
15. Zhang H. Epidemiological investigation of esophageal carcinoma. World J Gastroenterol. 2004;10(12):1834. doi:10.3748/wjg.v10.i12.1834
16. Gordon R. Skin cancer: an overview of epidemiology and risk factors. Semin Oncol Nurs. 2013;29(3):160–169. doi:10.1016/j.soncn.2013.06.002
17. Gandhi SA, Kampp J. Skin cancer epidemiology, detection, and management. Med Clin North Am. 2015;99(6):1323–1335. doi:10.1016/j.mcna.2015.06.002
18. Kim GK, Rosso JQD, Bellew S. Skin cancer in asians: part 1: nonmelanoma skin cancer. J Clin Aesthet Dermatol. 2009;2(8):4.
19. Laishram RS, Banerjee A, Punyabati P, Chandra LD. Pattern of skin malignancies in Manipur, India: a 5-year histopathological review. J Pak Associa Dermatol. 2010;20(3):128–132.
20. Öztürk R, Şm A, Bulut EK, Kekeç AF, Çelebi F, Güngör BŞ. Distribution and evaluation of bone and soft tissue tumors operated in a tertiary care center. Acta Orthop Traumatol Turc. 2019;53(3):189–194. doi:10.1016/j.aott.2019.03.008
21. Tamimi AF, Tamimi I, Abdelaziz M, et al. Epidemiology of Malignant and Non-Malignant Primary Brain Tumors in Jordan. Neuroepidemiology. 2015;45(2):100–108. doi:10.1159/000438926
22. Padhi S, Paul TR, Challa S, et al. Primary extra nodal non Hodgkin lymphoma: a 5 year retrospective analysis. Asian Pac J Cancer Prev. 2012;13(10):4889–4895. doi:10.7314/APJCP.2012.13.10.4889
23. Amin MB, Greene FL, Edge SB, et al. The Eighth Edition AJCC cancer staging manual: continuing to build a bridge from a population-based to a more “personalized” approach to cancer staging: the eighth edition AJCC cancer staging manual. CA Cancer J Clin. 2017;67(2):93–99. doi:10.3322/caac.21388
24. Cheng SA, Liang LZ, Liang QL, et al. Breast cancer laterality and molecular subtype likely share a common risk factor. Cancer Manag Res. 2018;10:6549–6554. doi:10.2147/CMAR.S182254
25. Guo S, Yao K, He X, et al. Prognostic significance of laterality in renal cell carcinoma: a population‐based study from the surveillance, epidemiology, and end results (SEER) database. Cancer Med. 2019;8(12):5629–5637. doi:10.1002/cam4.2484
26. Beigh A, Junaid S, Beg A, Farooq S, Wani LA, Manzoor F. Clinicopathological study of testicular tumors: an experience in a tertiary care hospital in Kashmir valley, Jammu and Kashmir, India. Int J Res Med Sci. 2017;5(6):2741. doi:10.18203/2320-6012.ijrms20172480
27. Mondal S, Nag D, Mondal P, Banyopadhyay R, Roychowdhury S, Sinha S. Histologic pattern, bilaterality and clinical evaluation of 957 ovarian neoplasms: a 10-year study in a tertiary hospital of eastern India. J Cancer Res Ther. 2011;7(4):433. doi:10.4103/0973-1482.92011
28. Domingo R, Manganip L, Castro R. Tumors of the eye and ocular adnexa at the Philippine Eye Research Institute: a 10-year review. Clin Ophthalmol. 2015;1239. doi:10.2147/OPTH.S87308
29. Shinohara S, Takebayashi S, Kikuchi M, et al. Prognostic impact of incisional or excisional biopsy of cervical lymph node metastases of solid tumors. Jpn J Clin Oncol. 2018;48(6):529–534. doi:10.1093/jjco/hyy056
30. Birgin E, Yang C, Hetjens S, Reissfelder C, Hohenberger P, Rahbari NN. Core needle biopsy versus incisional biopsy for differentiation of soft‐tissue sarcomas: a systematic review and meta‐analysis. Cancer. 2020;126(9):1917–1928. doi:10.1002/cncr.32735
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.