Back to Journals » Patient Related Outcome Measures » Volume 15
Prevalence, Clinical Characteristics and Determinants of Unsuccessful Treatment Outcomes Among Pulmonary Tuberculosis Patients: A 5-Year Registry-Based Retrospective Cohort Study
Authors AlOsaimi HM, Alshammari MK ![]() , Almijlad GK, Alotaibi NM, Alqahtani DA, Alshamrani MM, Shutur TA, Alhazmi MF, Hurubi MA, ALShammari KS, Alzahrani KM, Aldaghriri HM, Alshammari AA, Alatawi OS, Alharbi RA
, Almijlad GK, Alotaibi NM, Alqahtani DA, Alshamrani MM, Shutur TA, Alhazmi MF, Hurubi MA, ALShammari KS, Alzahrani KM, Aldaghriri HM, Alshammari AA, Alatawi OS, Alharbi RA ![]()
Received 13 March 2024
Accepted for publication 14 May 2024
Published 23 May 2024 Volume 2024:15 Pages 187—198
DOI https://doi.org/10.2147/PROM.S463396
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Robert Howland
Hind M AlOsaimi,1 Mohammed K Alshammari,2 Ghadah K Almijlad,3 Nawaf M Alotaibi,3 Dhafer A Alqahtani,4 Mohammed M Alshamrani,5 Tariq A Shutur,6 Mansior F Alhazmi,6 Mohammed A Hurubi,6 Kutayd S ALShammari,6 Khalid M Alzahrani,7 Hadeel M Aldaghriri,7 Anood A Alshammari,8 Oudah S Alatawi,8 Reema A Alharbi9
1Department of Pharmacy Services Administration, King Fahad Medical City, Riyadh, Kingdom of Saudi Arabia; 2Department of Clinical Pharmacy, King Fahad Medical City, Riyadh, Kingdom of Saudi Arabia; 3Department of Clinical Pharmacy, Northern Border University, Rafha, Kingdom of Saudi Arabia; 4Department of Pharmacy, Security Forces Hospital, Riyadh, Kingdom of Saudi Arabia; 5Department of Respiratory Care, Northern Armed Area Forced Hospital, Hafar al Batin, Kingdom of Saudi Arabia; 6Department of Supply and Logistics, Northern Armed Area Forced Hospital, Hafar Al Batin, Kingdom of Saudi Arabia; 7Department of Radiology, Northern Armed Area Forced Hospital, Hafar Al Batin, Kingdom of Saudi Arabia; 8Pharmaceutical Services Department, Northern Area Armed Forces Hospital, King Khalid Military, Hafr Al Batin, Kingdom of Saudi Arabia; 9Department of Medicine, University of Tabuk, Tabuk, Saudi Arabia
Correspondence: Mohammed K Alshammari, Department of Clinical Pharmacy, King Fahad Medical City, Riyadh, Kingdom of Saudi Arabia, Email [email protected]
Purpose: Despite the existence of effective medications, pulmonary tuberculosis (PTB) remains a significant global public health concern, The evaluation and feedback of national TB control programs are crucial, requiring diligent monitoring of TB treatment outcomes and analysis of the factors influencing these outcomes. This study aims to provide valuable insights into the challenges faced by TB patients, which can inform better strategies for treatment and management in the future.
Patients and Methods: We conducted a study in King Fahad Medical City, Riyadh, Kingdom of Saudi Arabia (KSA), from January 1, 2018 to December 31, 2023. The study was a registry-based retrospective cohort study. Patients’ data were sourced from the National Tuberculosis Registry database of Saudi Arabia. Treatment outcomes were determined as either success or failure, considering clinical evaluation, changes in chest X-rays, and the results of subsequent sputum examinations during follow-up. To evaluate the data, SPSS version 28.0 was used.
Results: A total of 427 PTB patients participated in the study. The results show successful treatment outcomes among 88.5% of patients. Among the patients, males exhibited a higher likelihood of treatment failure as compared to females (aOR 1.3; 95%Cl 1.2– 1.5, p < 0.001). Patients with positive sputum smear (aOR 1.3; 95%Cl 1.1– 1.3 p < 0.00) and the presence of cough were associated with an increased risk of treatment failure (aOR1.5; 95%Cl 1.1– 1.4, p < 0.001).
Conclusion: This study shows that the percentage of unsuccessful treatment outcomes is high, ie, 11.5%, due to patients’ deaths and loss to follow-up. Enhanced supervision and treatment monitoring for tuberculosis patients at high risk of treatment failure can lead to improved treatment success rates in Saudi Arabia.
Keywords: tuberculosis, treatment outcomes, retrospective study, Saudi Arabia
Introduction
Tuberculosis presents a critical public health crisis, leading to approximately 1.5 million deaths each year.1 Pulmonary tuberculosis (PTB) (TB of the lungs) is the most common form of the disease.2 PTB symptoms include exhaustion, a chronic cough, chest pain, blood in the cough, weight loss, fever, and night sweats.3
The World Health Organization (WHO) estimates that around 10 million new cases of TB were diagnosed in 2020, and 1.4 million died from TB in 2020.4 TB is one of the leading causes of death from a single infectious agent,4 and it is particularly prevalent in low- and middle-income countries.5 In Saudi Arabia, the monitoring and reporting of TB began in 1970, where it was recorded at an incidence rate of 1298.5 cases per 100,000 people.6 Over the years, there was a consistent decrease in TB cases, dropping to 135 per 100,000 in 1980 and further to 12 per 100,000 by 1997.6 However, from 2000 to 2009, there was a stabilization in TB incidence around 15–16 cases per 100,000, despite an increase in the raw number of new cases from 3284 to 3964.6 In 2015, the TB incidence rate in Saudi Arabia stood at 12 (10–14) per 100,000 individuals, categorizing the country as having a moderate burden of TB infection.7 As per the WHO, TB has been ranked as the 11th leading cause of mortality in Saudi Arabia.8 Despite the treatability of TB in most instances, challenges persist within both patient and health system domains concerning the appropriate utilization of TB treatment, patient compliance, multi drug resistant tuberculosis (MDR-TB) and extremely drug resistant tuberculosis (XDR-TB).9
In 2014, the WHO launched the end-TB strategy, aiming to eradicate the TB epidemic by 2035.10 This strategy includes specific targets set for every five years (2020, 2025, and 2030) along with yearly objectives, such as achieving a 4–5% reduction in TB incidence compared to the preceding year.11 These targets are meant to be implemented at the national level. As a result, there has been a steady decrease in global TB incidence, declining by approximately 2% annually.12
The treatment outcome is an important indicator of the progress of TB control programs.13
Moreover, in compliance with the WHO’s appeal, the Saudi government expanded the existing national tuberculosis control program (NTCP) to adhere to the objectives and benchmarks of the end-TB strategy.4 However, despite being categorized as a “low-to-middle TB burden country”, Saudi Arabia presents unique factors that may hinder the efficacy of the strategy.6 Notably, the annual pilgrimage influx of millions and increased population mobility contribute to the heightened transmission of TB.14
Annually in Saudi Arabia, the convergence of a substantial number of immigrants in densely populated areas during the Hajj season presents a potential risk for TB transmission. Nevertheless, the TB incidence rate has not been ascertained among diverse occupational cohorts. Additionally, there is a significant lack of concrete data regarding the factors influencing the outcomes of treatment for patients with PTB. The absence of such empirical evidence poses a challenge in comprehending the intended effects of the expanded national TB service. Therefore, we conducted a study to evaluate the factors influencing the treatment outcomes of PTB patients at King Fahad Medical City, Riyadh, Kingdom of Saudi Arabia (KSA).
Materials and Methods
Study Design
A register based retrospective analysis15 was carried out to determine the factors linked with unfavorable treatment outcomes of PTB patients in King Fahad Medical City, Riyadh, Kingdom of Saudi Arabia (KSA), from 1st January 2018 to 31st December 2023. In total, 1559 patients in total had been enrolled, but 1132 of them were disqualified because they had extrapulmonary TB (EPTB). So total of 427 patients were enrolled in the study. The prevalence-based study technique was used to calculate the sample size. The flow chart for the study participants is also explained in Figure 1. The sample size was calculated based on the prevalence of TB. A minimum sample size of 385 was calculated by 95% confidence intervals and a 5% margin of error.
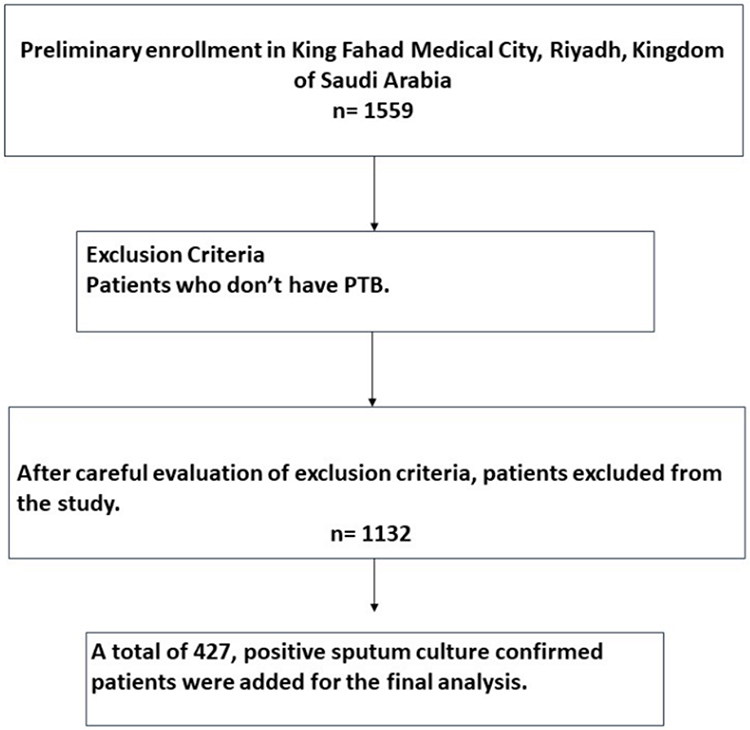 |
Figure 1 Flow chart for the study participants. |
Study Population
The study population consisted of PTB patients diagnosed between 1st January 2018 to 31st December 2023. Information regarding patients’ socio-demographics, clinical variables, and other pathological characteristics was taken from the register used throughout the treatment of the patients. The data was also verified by the doctors working in the respiratory department. According to the NTCP recommendations, “assumed TB patients” were diagnosed using the symptoms, microscopy, and chest X-ray.
Inclusion and Exclusion Criteria
Inclusion criteria: The study included data on all patients diagnosed with PTB and who started treatment.
Exclusion criteria: Patients whose information was incomplete were excluded from the study.
TB Diagnosis
In accordance with the guidelines established by the NTCP, individuals suspected of having TB, termed as “presumptive TB cases”, are identified at the TB outdoor clinic through symptom assessment and subsequent microscopy follow-up.12 Treatment was based on the guidelines of the country with a full course of anti-TB therapy Directly Observed Treatment, Short-course (DOTs). This strategy is particularly beneficial in settings where treatment supervision and monitoring may be challenging, as it enhances patient accountability and improves treatment outcomes overall. Treatment of new TB patients consists of a 2-month intensive phase with Isoniazid, Rifampicin, Pyrazinamide and Ethambutol followed by a 4-month continuation phase with Rifampicin and Isoniazid. Outcomes were categorized as successful (cured/completed) and unsuccessful (loss to follow-up, failure and died).
Treatment Outcomes Measure Definitions
According to WHO treatment outcomes are measured through respective variables.13
Cured: A patient with bacteriologically confirmed TB at the beginning of treatment who was smear- or culture-negative in the last month of treatment and on at least one previous occasion.
Treatment completed: A TB patient who completed treatment without evidence of failure but with no record to show that sputum smear or culture results in the last month of treatment and on at least one previous occasion were negative, either because tests were not done or because results are unavailable.
Died: A TB patient who dies for any reason before starting or during treatment.
Loss to follow-up: A TB patient who did not start treatment or whose treatment was interrupted for 2 consecutive months or more.
Treatment failure: TB patient whose sputum smear or culture was positive at five months or later during TB treatment.
Not evaluated: A TB patient for whom no treatment outcome is assigned. This includes cases “transferred out”, to another treatment unit as well as cases for whom the treatment is unknown to the reporting unit.
Ethical Approval
The ethical approval was granted by the Institutional Review Board of King Fahad Medical City, Riyadh, KSA under IRB log Number: 23–525. The data was sorted from the national TB registry available in the hospital. The study followed the ethical guidelines and complies by declaration of Helsinki.
Data Collection
The health personnel of the NTCP regularly review TB data collected and submitted by regional TB programs to produce monthly, quarterly, and yearly statistical reports. For this study, we compiled data from the annual statistical reports spanning from 2018 to 2023 and integrated it into a unified database. Subsequently, the data underwent cleaning and coding processes.
Data Analysis
Statistical Package for Social Science (SPSS) (version 23, IBM Corp. Armonk, N.Y., United States) was used in analyzing data.16 Univariate analysis was used to assess the association between patients’ sociodemographic, microbiological, and clinical characteristics with unsuccessful treatment outcomes. To identify the ultimate predictors of unsatisfactory treatment outcomes, multiple logistic regression analysis was used to examine statistically significant factors in univariate analysis. The variables that showed a p-value <0.05 were considered to be statistically significant.
Results
Socio-Demographics of the Patients
The study indicated females comprise 25.9% (n=111) and males dominate the majority at 74.1% (n=316). Individuals aged 66 and above constitute the largest segment, accounting for 27.2% (n=116), followed by those aged 56–65 at 22.5% (n=96). The majority of participants, 68.9% (n=294), reside in urban areas. In this study, a substantial proportion, 70.5% (n=301), identified as married. The majority of participants, 90.4% (n=386), identified as current smokers. The results are explained in Table 1.
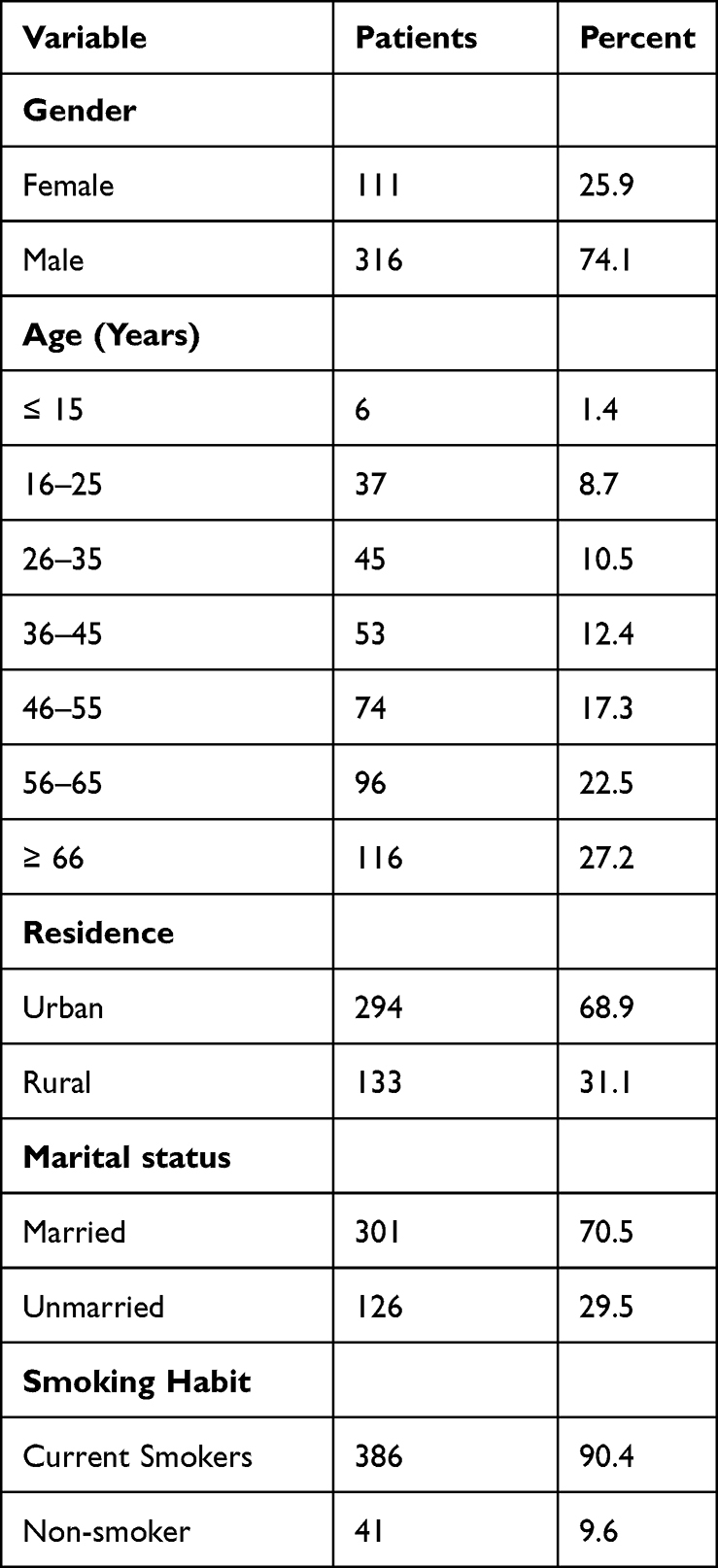 |
Table 1 Socio-Demographic Characteristics of PTB Patients |
Clinical Characteristics
The study categorized patients based on sputum smear results. The majority, 88.3% (n=377), are identified as sputum smear positive. Patients are further classified into relapse and new cases. New patients constitute the substantial majority at 96.7% (n=413), emphasizing the prevalence of newly diagnosed cases. A significant proportion, 98.6% (n=421), exhibit lesions on chest X-rays, indicative of pulmonary abnormalities. Notable findings include the prevalence of night sweats in 55.1% (n=220) of patients, cough in 87.8% (n=375), fever in 72.4% (n=118), shortness of breath in 51.1% (n=218), weight loss in 67.7% (n=289), appetite loss in 73.8% (n=315), and hemoptysis in 26.7% (n=114) of cases. Among the TB cases, 83.1% (n=355) exclusively present with PTB, while 16.9% (n=72) exhibit comorbidities. The results are described in Table 2.
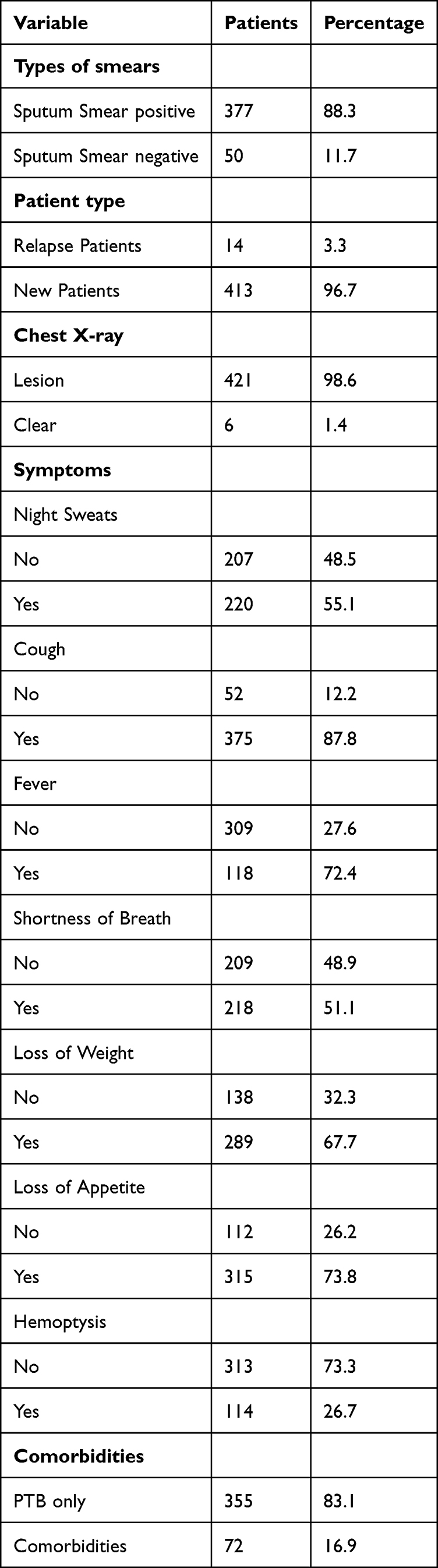 |
Table 2 Clinical Characteristics of PTB Patients |
Treatment Outcome
Figure 2 shows the percentages of patients in successful and unsuccessful treatment outcome categories. The success rate for the treatment of PTB patients was (88.5%). Of all PTB patients (4.4%) were reported as cured and 84.1% of patients completed their treatment. The rate of unsuccessfully treated patients was (11.5%), (5.6%) of patients died, (0%) of patients failed the treatment, (4.6%) of patients were lost to follow-up.
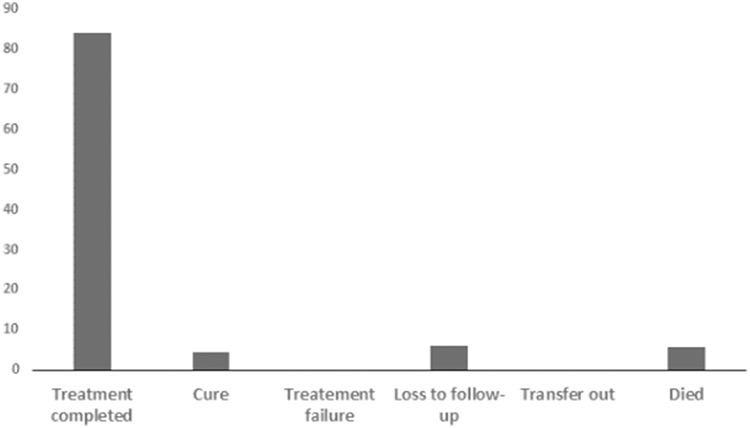 |
Figure 2 Treatment outcomes among PTB patients. |
Factors Associated with Unsuccessful Treatment Outcomes
Table 3 depicts the results of the multivariable logistic regression analysis revealing that the males exhibited a higher likelihood of treatment failure compared to females AOR = 1.3 (95% CI: 1.2–1.5), p < 0.001. Urban residence was associated with an increased risk of treatment failure, AOR = 1.21 (95% CI: 1.1–1.2), p <0.01. Married individuals demonstrated a higher risk of treatment failure, AOR = 1.9 (95% CI: 1.0–1.7), p < 0.001. Patients with positive sputum smears had an elevated risk of treatment failure, AOR = 1.3 (95% CI: 1.1–1.3), p < 0.001. The presence of cough was associated with an increased risk of treatment failure, AOR = 1.5 (95% CI: 1.1–1.4), p < 0.001. The presence of comorbidities significantly increased the risk of treatment failure, AOR = 1.7 (95% CI: 1.1–1.6), p < 0.001.
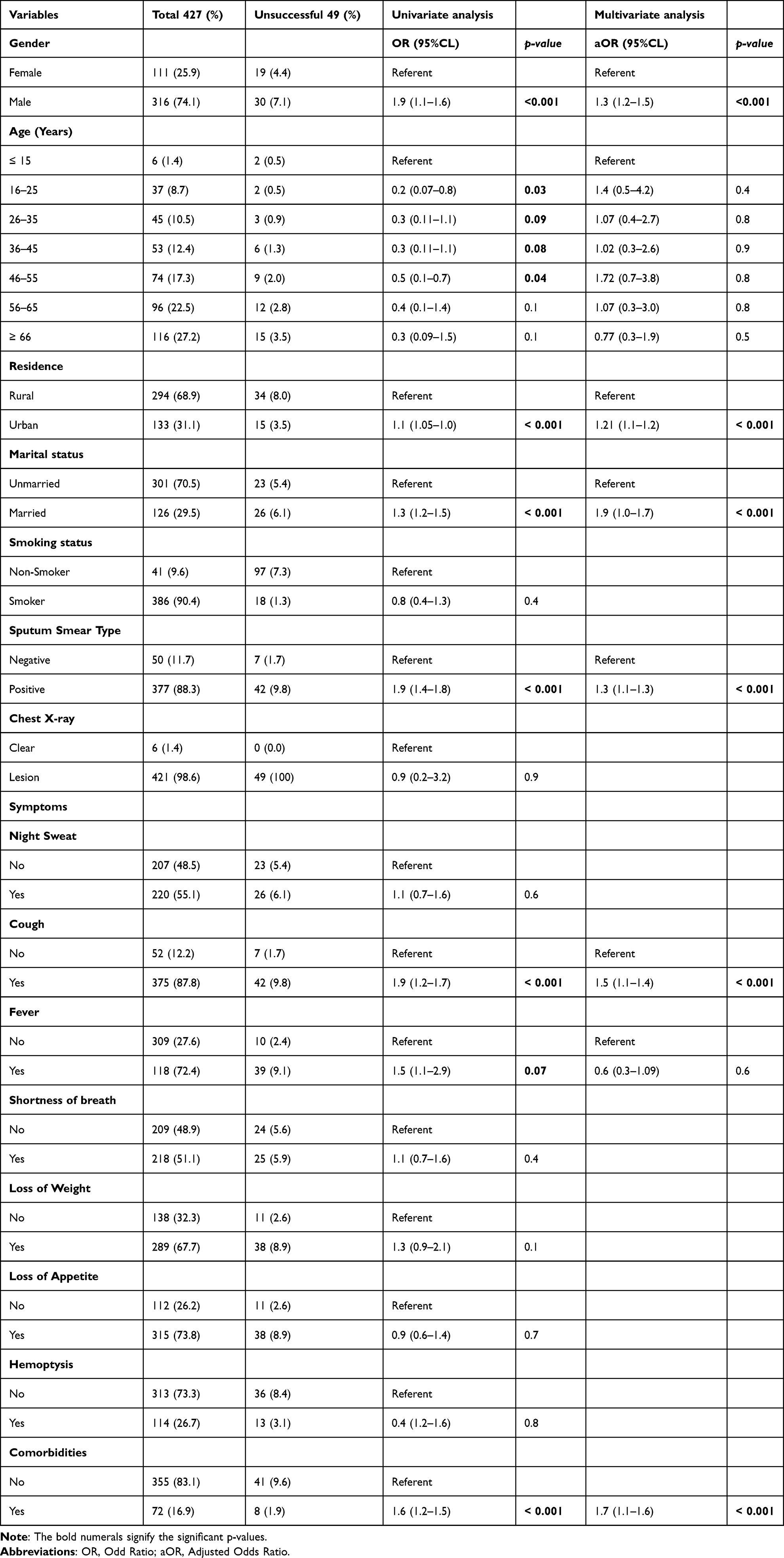 |
Table 3 Factors Associated with Unsuccessful Treatment Outcome |
Discussion
The aim of this study was to evaluate the prevalence, clinical characteristics and unsuccessful treatment outcomes among PTB patients receiving care at King Fahad Hospital in Riyadh, Saudi Arabia. This study not only evaluated treatment outcomes in new smear-positive PTB patients but also identified risk factors associated with unsuccessful treatment outcomes. Over 2/3rd of patients (88.5%) of patients have successful treatment outcomes, which is higher than treatment success rate in India (74%),17 Brazil (71%)18 and Pakistan (69%).19 The successful treatment outcomes recorded in our study could be attributed to the introduction of effective policies by the NTP and WHO for the eradication of TB in Saudi Arabia.9,20 But it is still less than the WHO target of 90%.21 The NTCP was expanded to conform with the worldwide objective of achieving a TB-free world by 2035.11 The success rate can be improved by raising more awareness regarding TB in Saudi Arabia.
In this study, the rate of unsuccessful treatment is 11.5%. This could be attributed to patients’ deaths, and patients who were lost to follow-up. Studies conducted in Libya and Ethiopia have reported similar findings regarding loss to follow-up among PTB patients.22,23 At the local level, patient loss to follow-up may be exacerbated by the necessity to purchase medications to manage the side effects of TB drugs, particularly for those with limited financial resources.24 Literature12,25 also indicates that constraints on patients’ time, long distances to TB clinics, and societal stigma towards their illness may contribute to treatment non-compliance. Another significant factor affecting lower treatment success rates is the higher mortality rate among patients in our study, it is consistent with previous research in Singapore26 and the United States.27 The elevated mortality rate in our study may be attributed to the study setting.
To have a higher chance of successful treatment, people with PTB should be diagnosed and treated promptly, should take their medication as prescribed, and should receive support to help them adhere to their treatment regimen.28 The rate of unsuccessful treatment outcomes could be reduced through effective health policies and surveillance.
Unsuccessful treatment outcomes may be associated with clinical characteristics.29 The characteristics included in the study were microbiological smear examinations, radiograph chest x-ray examinations, and investigations regarding the symptoms of PTB. The majority of PTB patients who died were smear-positive patients and showed lesions in the lung cavity on Chest X-rays. In light of this, individuals with smear-positive PTB are considered to have failed treatment if a positive smear result is discovered after two months or five months of treatment.30 Studies from India and South Africa also revealed consistent results regarding loss of follow-up among PTB patients who had smear-positive results.31,32
Our study demonstrated that gender, marital status, residential status, coughing, and comorbidity were the independent predictors of unsuccessful treatment outcomes among PTB patients in the multiple logistic regression analysis. Poor treatment outcomes among PTB cases have been documented in studies which are consistent with our findings.23,33 Married PTB patients showed a significant association with unsuccessful treatment outcomes. The reason for this could be higher levels of professional stress, as well as higher smoking and alcohol consumption. Self-neglect, bad food habits, and sedentary living conditions may also contribute to unsuccessful PTB treatment outcomes.34
Cough was associated with unsuccessful treatment outcomes. Previous studies showed mixed results in clinical presentation among PTB patients.35,36 It has been shown that patients with comorbidities had a higher chance of poor outcomes and mortality.37 According to the WHO’s “Framework for Collaborative Action on Tuberculosis and Comorbidities”, our findings advocate for a holistic approach to care that prioritizes the integration of TB and comorbidities, focusing on early identification and treatment of concurrent conditions, suitable TB treatment plans, and vigilant monitoring of patients with comorbidities.38
These findings imply that TB programs should focus on identifying high-risk groups for TB-related disease and then developing suitable treatments to improve treatment outcomes. Examining treatment outcomes in PTB patients is crucial as they serve as significant benchmarks for evaluating the performance of the NTCP.
Strength and Limitations
This study is one of its types to be conducted in Saudi Arabia. The study highlights the problem caused by the delayed diagnosis and the factors associated with the treatment failure. The findings of this retrospective descriptive study will help healthcare professionals and policymakers to better understand the problems causing unsuccessful treatment outcomes. The factors indicate that the success rate can be improved due to various factors, including the practical and holistic approach of NTCP and the WHO End TB strategy in Saudi Arabia, as well as more awareness regarding TB in Saudi Arabia. The study fills the gap of information regarding treatment outcomes and variables associated with unsuccessful outcomes among PTB patients from Saudi Arabia.
The only limitation is that the study is a single center study. The study should be conducted at a larger scale to observe much better results. A specific concern is the substantial amount of missing data related to TB. To address these limitations and improve data quality, we recommend the implementation of more rigorous data management strategies aimed at standardizing these practices.
Conclusion
This study reveals that the rate of unsuccessful treatment outcomes is relatively higher than anticipated. The level of treatment completed and cured patient is high which is encouraging ie, 88.5%. The study showed that males, patients with positive sputum smear test, patients with cough and comorbidities were significantly related to the unsuccessful treatment outcomes. Loss to follow-up, and mortality were the main reasons for unsuccessful treatment results. A large number of patients were lost to follow-up and passed away during therapy, which raised serious issues and call for quick action. Developing and implementing effective tracing methods for patients who have been lost to follow-up is essential to reduce treatment interruptions. Additionally, patients at higher risk of experiencing unsuccessful treatment outcomes should receive enhanced supervision and treatment monitoring to improve their overall outcomes.
Informed Consent
This is a retrospective study but informed consent was obtained from the study participants before study commencement. The patients who were below 18 years, the consent was taken from the parents.
Acknowledgments
The authors would like to thank the research center at King Fahad Medical City, Riyadh Second Health Cluster, for the technical support provided for the manuscript. This research received no external funding.
Author Contributions
All authors made a significant contribution to the work reported, whether in the conception, study design, execution, acquisition of data, analysis and interpretation, or in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed to be accountable on the journal to which the article has been submitted.
Disclosure
The authors report no conflicts of interest in this work.
References
1. World Health Organization. Global tuberculosis report 2020. Glob Tuberc Rep. 2020;2020:1.
2. Park HY, Kang D, Shin SH, et al. Pulmonary tuberculosis and the incidence of lung cancer among patients with chronic obstructive pulmonary disease. Ann Am Thoracic Soc. 2022;19(4):640–648. doi:10.1513/AnnalsATS.202010-1240OC
3. John S, Abdulkarim S, Usman S, Rahman MT, Creswell J. Comparing tuberculosis symptom screening to chest X-ray with artificial intelligence in an active case finding campaign in Northeast Nigeria. BMC Global and Public Health. 2023;1(1):17. doi:10.1186/s44263-023-00017-2
4. Chakaya J, Petersen E, Nantanda R, et al. The WHO Global Tuberculosis 2021 Report–not so good news and turning the tide back to End TB. Inter J Infect Dis. 2022;124:S26–S29.
5. Foo CD, Shrestha P, Wang L, et al. Integrating tuberculosis and noncommunicable diseases care in low-and middle-income countries (LMICs): a systematic review. PLoS Med. 2022;19(1):e1003899. doi:10.1371/journal.pmed.1003899
6. Alawi MM, Alserehi HA, Ali AO, et al. Epidemiology of tuberculosis in Saudi Arabia following the implementation of end tuberculosis strategy: analysis of the surveillance data 2015-2019. Saudi Medical J. 2024;45(1):60. doi:10.15537/smj.2024.45.1.20230424
7. Semilan HM, Abugad HA, Mashat HM, Abdel Wahab MM. Epidemiology of tuberculosis among different occupational groups in Makkah region, Saudi Arabia. Sci Rep. 2021;11(1):12764. doi:10.1038/s41598-021-91879-9
8. Al-Orainey I, Alhedaithy MA, Alanazi AR, Barry MA, Almajid FM. Tuberculosis incidence trends in Saudi Arabia over 20 years: 1991-2010. Anna Thorac Med. 2013;8(3):148–152. doi:10.4103/1817-1737.114303
9. Saati AA, Khurram M, Faidah H, Haseeb A, Iriti M. A Saudi Arabian public health perspective of tuberculosis. Int J Environ Res Public Health. 2021;18(19):10042. doi:10.3390/ijerph181910042
10. Khanna A, Saha R, Ahmad N. National TB elimination programme-what has changed. Indian J Med Microbiol. 2023;42:103–107. doi:10.1016/j.ijmmb.2022.10.008
11. Uplekar M, Raviglione M. WHO’s End TB Strategy: from stopping to ending the global TB epidemic. Indian J Tuberculosis. 2015;62(4):196–199. doi:10.1016/j.ijtb.2015.11.001
12. Ledesma JR, Ma J, Vongpradith A, et al. Global, regional, and national sex differences in the global burden of tuberculosis by HIV status, 1990–2019: results from the global burden of disease study 2019. Lancet Infect Dis. 2022;22(2):222–241. doi:10.1016/S1473-3099(21)00449-7
13. Heyckendorf J, Georghiou SB, Frahm N, et al. Tuberculosis treatment monitoring and outcome measures: new interest and new strategies. Clin Microbiol Rev. 2022;35(3):e00227–21. doi:10.1128/cmr.00227-21
14. Yezli S, Memish ZA. Tuberculosis in Saudi Arabia: prevalence and antimicrobial resistance. J Chemother. 2012;24(1):1–5. doi:10.1179/1120009X12Z.0000000001
15. Beyene N, Fanta K, Tatiparthi R. Pharmacotherapy pattern and treatment outcomes of stroke patients admitted to Jimma University Medical Center, Ethiopia. Pat Relat Outcome Meas. 2021;Volume 12:267–275. doi:10.2147/PROM.S307291
16. G/Mariam B, Tilahun T, Merdassa E, Tesema D. Indications, Outcome and risk factors of cesarean delivery among pregnant women utilizing delivery services at selected Public Health Institutions, Oromia Region, South West Ethiopia. Pat Relat Outcome Meas. 2021;227–236. doi:10.2147/PROM.S304672
17. Khumsri J, Hiransuthikul N, Hanvoravongchai P, Chuchottaworn C. Effectiveness of tuberculosis screening technology in the initiation of correct diagnosis of pulmonary tuberculosis at a tertiary care hospital in Thailand: comparative analysis of Xpert MTB/RIF versus sputum AFB smear. Asia Pac J Public Health. 2018;30(6):542–550. doi:10.1177/1010539518800336
18. Abe RY, Maestrini HA, Guedes GB, et al. Real-world data from selective laser trabeculoplasty in Brazil. Sci Rep. 2022;12(1):1923. doi:10.1038/s41598-022-05699-6
19. Ali MK, Karanja S, Karama M. Factors associated with tuberculosis treatment outcomes among tuberculosis patients attending tuberculosis treatment centres in 2016-2017 in Mogadishu, Somalia. Pan Afr Med J. 2017;28(1). doi:10.11604/pamj.2017.28.197.13439
20. Al-Janabi AHK. Outcome and determinants of directly observed short-course treatment for tuberculosis patients. South Asian J Soc Sci Humanit. 2023;4(6):63–77. doi:10.48165/sajssh.2023.4604
21. Chakaya JM, Harries AD, Marks GB. Ending tuberculosis by 2030—pipe dream or reality? Inter J Infect Dis. 2020;92:S51–S54. doi:10.1016/j.ijid.2020.02.021
22. Gebrezgabiher G, Romha G, Ejeta E, Asebe G, Zemene E, Ameni G. Treatment outcome of tuberculosis patients under directly observed treatment short course and factors affecting outcome in southern Ethiopia: a five-year retrospective study. PLoS One. 2016;11(2):e0150560. doi:10.1371/journal.pone.0150560
23. Solliman MA, Hassali MA, Al-Haddad MS, Sulaiman SAS, Atif M, Saleem F. Treatment outcomes of new smear positive pulmonary tuberculosis patients in north east Libya. Latin Am J Pharm. 2012;2012:31.
24. Shaweno T, Getnet M, Fikru C. Does time to loss to follow-up differ among adult tuberculosis patients initiated on tuberculosis treatment and care between general hospital and health centers? A retrospective cohort study. Trop Med Int Health. 2020;48(1):1–11. doi:10.1186/s41182-020-00198-8
25. Soedarsono S, Mertaniasih NM, Kusmiati T, et al. Determinant factors for loss to follow-up in drug-resistant tuberculosis patients: the importance of psycho-social and economic aspects. BMC Pulm Med. 2021;21(1):1–8. doi:10.1186/s12890-021-01735-9
26. Low S, Ang L, Cutter J, et al. Mortality among tuberculosis patients on treatment in Singapore. Int J Tuberc Lung Dis. 2009;13(3):328–334.
27. Horne DJ, Hubbard R, Narita M, Exarchos A, Park DR, Goss CH. Factors associated with mortality in patients with tuberculosis. BMC Infect Dis. 2010;10(1):1–8. doi:10.1186/1471-2334-10-258
28. Thomas BE, Suresh C, Lavanya J, et al. Understanding pretreatment loss to follow-up of tuberculosis patients: an explanatory qualitative study in Chennai, India. BMJ Global Health. 2020;5(2):e001974. doi:10.1136/bmjgh-2019-001974
29. Tok PSK, Liew SM, Wong LP, et al. Determinants of unsuccessful treatment outcomes and mortality among tuberculosis patients in Malaysia: a registry-based cohort study. PLoS One. 2020;15(4):e0231986. doi:10.1371/journal.pone.0231986
30. Galamay LC, Chee CBE, Mar KWK, Lau BQ, Wang YT. Smear-positive pulmonary tuberculosis patients with previously abnormal chest radiographs: missed opportunities for early diagnosis. Singapore Med J. 2021;62(6):296. doi:10.11622/smedj.2020027
31. Mlotshwa M, Abraham N, Beery M, et al. Risk factors for tuberculosis smear non-conversion in Eden district, Western Cape, South Africa, 2007–2013: a retrospective cohort study. BMC Infect Dis. 2016;16(1):1–12. doi:10.1186/s12879-016-1712-y
32. Singla R, Bharty SK, Gupta UA, et al. Sputum smear positivity at two months in previously untreated pulmonary tuberculosis patients. Int J Mycobacteriol. 2013;2(4):199–205. doi:10.1016/j.ijmyco.2013.08.002
33. Loudon RG, Spohn SK. Cough frequency and infectivity in patients with pulmonary tuberculosis. Amer Rev Respir Dis. 1969;99(1):109–111. doi:10.1164/arrd.1969.99.1.109
34. Jaggarajamma K, Ramachandran R, Charles N, Chandrasekaran V, Muniyandi M, Ganapathy S. Psycho-social dysfunction: perceived and enacted stigma among tuberculosis patients registered under revised national tuberculosis control programme. Indian J Tuberculosis. 2008;55(4):179–187.
35. Turner RD, Bothamley GH. Cough and the transmission of tuberculosis. J Infect Dis. 2015;211(9):1367–1372. doi:10.1093/infdis/jiu625
36. Jittimanee S, Ngamtrairai N, White M, Jittimanee S. A prevalence survey for smear-positive tuberculosis in Thai prisons. Int J Tuberc Lung Dis. 2007;11(5):556–561.
37. Alavi-Naini R, Moghtaderi A, Metanat M, Mohammadi M, Zabetian M. Factors associated with mortality in tuberculosis patients. J Res Med Sci. 2013;18(1):52.
38. World Health Organization. Framework for collaborative action on tuberculosis and comorbidities. Framework for Collaborative Action on Tuberculosis and Comorbidities. 2022.
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.