Back to Journals » Infection and Drug Resistance » Volume 16
Prevalence, Antimicrobial Susceptibility Pattern and Associated Factors of Group B Streptococcus Among Pregnant Women Attending Antenatal Care at Bule Hora University Teaching Hospital, Southern Ethiopia
Authors Husen O, Kannaiyan Abbai M, Aliyo A ![]() , Daka D
, Daka D ![]() , Gemechu T
, Gemechu T ![]() , Tilahun D
, Tilahun D ![]() , Dedecha W
, Dedecha W
Received 20 April 2023
Accepted for publication 28 June 2023
Published 6 July 2023 Volume 2023:16 Pages 4421—4433
DOI https://doi.org/10.2147/IDR.S415414
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Prof. Dr. Héctor Mora-Montes
Oliyad Husen,1 Moorthy Kannaiyan Abbai,1 Alqeer Aliyo,1 Deresse Daka,2 Tibeso Gemechu,1 Dagnamyelew Tilahun,1 Wako Dedecha1
1Department of Medical Laboratory Science, Institute of Health, Bule Hora University, Bule Hora, Ethiopia; 2Department of Medical Laboratory Science, College of Medicine and Health Sciences, Hawassa University, Hawassa, Ethiopia
Correspondence: Alqeer Aliyo, P.O. Box 144, Tel +251968467458, Email [email protected]
Background: In many parts of the world, Group B Streptococcus (GBS) is a major cause of maternal and neonatal illness and mortality. It has a negative impact on neonatal and pregnancy outcomes. A worrisome problem in Ethiopia is the unknown rate of antibiotic resistance and the risk factors connected to GBS infections.
Objective: This study was to determine the prevalence, antibiotic susceptibility pattern, and related variables of Group B Streptococcus among pregnant women receiving prenatal treatment conducted at Bule Hora University Teaching Hospital, Southern Ethiopia, between June 1 and August 30, 2022.
Methods: An institutional-based cross-sectional study was conducted among 213 pregnant women attending antenatal care at Bule Hora University Teaching Hospital. Data on sociodemographic and related factors were gathered using structured questionnaires. The study’s participants were selected using the consecutive sampling method. The lower vaginal/rectum area was brushed with a sterile cotton swab to capture the vaginal/rectum swab sample, which was then examined using microbiological techniques. The Kirby-Bauer disc diffusion method was used to assess antibiotic susceptibility in GBS isolates. Logistic regression analysis was performed on the data using SPSS version 26. It was deemed statistically significant when the p-value was 0.05 with a 95% confidence interval (CI).
Results: The overall prevalence of GBS was 16.9% (CI: 0.12– 0.23). A history of prematurity of the membrane (AOR: 3.35, 95% CI: 1.19– 9.45), a history of stillbirth (AOR: 2.88, 95% CI: 1.07– 7.71), and preterm delivery history (AOR: 3.41, 95% CI: 1.31– 8.89) (p 0.05) were independent predictors of GBS infection. Cefepime had the highest resistance at 58.3%. Most GBS isolates showed high susceptibility to vancomycin (97.2%) and ampicillin (91.7%). Multidrug resistance was 13.9%.
Conclusion: The prevalence of GBS was considerably high among pregnant women in this study. This finding emphasises the need for routine screening and testing of antimicrobial susceptibility to provide antibiotic prophylaxis and minimise newborn infection and comorbidity.
Keywords: Group B Streptococcus, antimicrobial susceptibility pattern, pregnant women
Introduction
Invasive infections of the mother and fetus are brought on by Group B Streptococcus (GBS), a component of the common flora of gram-positive streptococci.1 The common GBS reservoirs are the vaginal and perianal areas, and colonization of these areas increases the risk of subsequent infection in both pregnant women and neonates.2 GBS colonization may be transient, sporadic, or persistent.3 Early membrane rupture, chorioamnionitis, preterm birth, stillbirth, advanced abortion, and a number of unfavourable pregnancy outcomes in both mothers and their unborn children are all frequently caused by GBS.4 The most important risk factors for GBS vaginal colonization are a history of premature rupture of the membranes, increased maternal age, low vitamin D intake, poor personal hygiene, sexual intercourse, health care occupation, and gastrointestinal GBS colonization.5,6
According to studies, 10–30% of expectant mothers have GBS in their vagina or rectum, and about 50% of them vertically transmit the infection to their newborns during labour or delivery.7 According to a study, GBS infection caused one-fourth of puerperal fever with or without bacteremia and was the cause of 61.5% of newborn bacterial meningitis, with a death rate of 44.06%.8 Despite its pathogenicity, GBS remains one of the organisms for which no vaccine is available.9
The prevalence rate of GBS colonization during pregnancy varies according to research conducted in various nations.10 The global prevalence of GBS among expectant women is estimated to be 18%, with regional variations of 11–35%,11 20–35% in the USA,12 7.8–13.65% in Asia,13–15 and the highest prevalence rates documented in Africa (7.2–48.2%).16–18 Evidence about maternal colonization prevalence in Africa is still lacking,19 particularly in Ethiopia, where a small number of studies have revealed that maternal colonization rates range from 7.2%18 to 25.5%.20 Ethiopia has a high incidence of newborn mortality and GBS illness.21
Universal screening is recommended for the prevention of perinatal GBS disease among pregnant women between the 35th and 37th gestational weeks, according to the guidelines issued by the Centres for Disease Control and Prevention (CDC). GBS-colonised women must take antimicrobials during labour, and penicillin G crystalline is the drug of choice.1 Studies have shown that the rise in GBS infection among pregnant women and babies, which is challenging to treat and poses a serious health hazard, is a result of the global expansion of antibiotic resistance. One reason that raises this issue is the increased use of antimicrobials for prophylaxis without adequate bacteriological screening.22 However, in several African nations, like Ethiopia, there is no well-defined plan for the prevention of GBS, including routine screening practices and the provision of intrapartum antibiotic prophylaxis (IAP).23,24
GBS causes the most serious disease in pregnant women, although little is known about its epidemiology and risk factors in countries with poor resources, like Ethiopia.25 Therefore, the purpose of this study was to determine the prevalence, antimicrobial susceptibility pattern, and associated factors of GBS among pregnant women attending antenatal care at Bule Hora University Teaching Hospital.
Methods
Study Area, Design, and Period
The investigation was carried out at the Bule Hora University Teaching Hospital in the southern Ethiopian region of Oromia. The distance between Bule Hora Town and Ethiopia’s capital city, Addis Ababa, is 475 kilometres. In each of the town’s eight kebeles, there is a government hospital, a health centre, and eight health posts. In 1990, E.C., BHUTH was established. With a catchment population of nearly 1.3 million, the hospital is the largest in the West Guji Zone. It functions as a centre for clinical services, instruction, and training. A cross-sectional institutional study was carried out between June 1 and August 30, 2022, at Bule Hora University Teaching Hospital.
Study Population and Selection Criteria
All consenting pregnant women between the gestational period of 35th and 37th weeks participated in the study, while pregnant women with a history of antibiotic use within two weeks before recruitment and emergency obstetric conditions who needed immediate intervention were excluded from the study.
Sample Size Determination
The single population ratio formula was used to get the sample size for this study. A margin of error of 5%, a confidence interval (CI), and a nonresponse rate of 5% were taken into account when the GBS proportion (15.7%) was derived from a prior study carried out in the Sidama Zone.26
Where Z is the value corresponding to a 95% level of significance, which is 1.96, P is the percentage of the prevalence of GBS in pregnant women, which is 15.7%, d is the marginal error, which is assumed to be 5%, and n = (1.96) 2 (0.157) (0.843) (0.05) 2 = 203. After adding in a nonresponse rate of 5%, which is 10, the final sample size was 213.
Sampling Techniques
All consecutively identified pregnant women who met the inclusion criteria and were between 35 and 37 weeks gestation and attending regular prenatal appointments at Bule Hora Teaching Hospital during the study period were enrolled.
Data Gathering Techniques
By employing predesigned and pretested structured questionnaires and reviewing medical records, data on sociodemographic characteristics and other pertinent information were gathered (Supplementary Material). The questionnaire was initially created in English and modified from earlier research of a similar nature. Each study participant gave informed consent after being informed of the study’s goals and methods.
Specimen Collection and Transportation
One swab from the lower vagina was taken with two distinct sterile Dacron swabs (Medical wire and equipment, USA), and the second swab was taken from the rectum (ie, by inserting the swab through the anal sphincter). Two swab samples were collected from each pregnant woman. The swabs were collected by the experienced midwife and nurses and transported immediately to the Bule Hora University microbiology laboratory for inoculation on 5% sheep blood agar (SBA) and for further analysis, with a maximum of 4–6 hours.2,4,19
GBS Isolation
The sample was inoculated directly into 5% SBA supplemented with nalidixic acid and incubated under anaerobic conditions by using a candle jar at 35°C–37°C overnight before analysis for the growth of colonies. Reincubation for an additional 24 hours was performed when there were no colonies after 24 hours before discarding the negative plates. Colony morphology, hemolytic activity on SBA, and typical streptococcal morphology on Gram staining were presumptively used to identify GBS colonies (Supplementary Material). Colonies from the screening blood agar plates were subcultured onto nutrient agar for confirmation and defined as GBS on the basis of catalase-negative reactions, bacitracin resistance tests, and the CAMP test.27 Subcultures that were negative after the first incubation were incubated again for another 24 hours and reexamined, as shown in Figure 1.
 |
Figure 1 GBS isolation colony morphology, Gram staining, GBS on the basis of catalase-negative reactions, bacitracin resistance tests, and the CAMP test. |
Antimicrobial Sensitivity Testing
Disc diffusion was used for antimicrobial susceptibility testing in accordance with Clinical and Laboratory Standard Institute guidelines (CLSI, 2014).28 About 3–5 colonies from a pure culture plate were taken out, emulsified in 3 mL of sterile physiological saline, and diluted with saline until the suspension’s turbidity matched the turbidity standard, which corresponds to 0.5 McFarland standard, before being inoculated with 5% sheep’s blood on Muller-Hinton Agar (MHA, Oxoid, England). A sterile swab was then used to evenly spread the bacteria over the surface of MHA supplemented with 5% sheep blood after the surplus suspension was removed by gently rotating the swab against the surface of the tube.
Clinical Laboratory Standard Institute (CLSI) recommendations were followed when using the following seven antibiotics and concentrations on the inoculated plates: penicillin G (PEN, 10 IU), ampicillin (AMP, 10 g), clindamycin (Da, 2 g), erythromycin (ERT, 15 g), chloramphenicol (CAP, 30 g), cefepime (FEP, 30 g), and vancomycin (VAN, 30 g). The strain used as a positive quality control was S. pneumoniae ATCC 49619. Plates were incubated for 24 hours at 35°C in 5% CO2, and rulers were used to measure the widths of the inhibitory zones. According to CLSI recommendations, the results were classified as sensitive, moderate, and resistant.29 Before usage, all isolates that were preserved were subcultured.
For multidrug resistance (MDR), the definition from Magiorakos et al was used, and GBS isolates that showed nonsusceptibility to at least one agent in three or more antibiotic categories were considered MDR.30
Data Quality Assurance
Data collectors were trained on data collection tools, study objectives, method data, and sample collection for two days.
For consistency and completeness, the obtained data were cross-checked, and on-site rectification was performed. By incubating 5% of the media overnight at 37°C without specimen inoculation, sheep blood agar (SBA) and Mullen Hinton agar (MHA) containing 5% sheep blood agar were tested for sterility.31
Control strains such as Streptococcus pneumoniae (ATCC 49619) and Staphylococcus aureus (ATCC 25923) were employed during the study period to maintain the standard of culture media and reagents.29 The selection of suitable reagents, preparations, sterility, and medium performance were all checked as part of the quality control process, following the manufacturer’s guidelines.
Data Processing and Analysis
On a PC running SPSS version 26, data analysis was done. Prevalence was calculated using the frequency distribution of the entire study population as well as separately for each group of age groups and risk variables. To describe a pertinent variable, descriptive statistics were produced and presented as texts, tables, and graphs. To compare the prevalence of GBS with other related factors, bivariable logistic regression was utilised. The strength of the link was assessed using an adjusted odds ratio (AOR). Multivariable logistic regression was used to examine a variable that had a p-value of less than 0.25 in the bivariate analysis. Statistical significance was defined as a p-value of 0.05 with a 95% confidence interval.
Operational Definition
Sensitive (S): When the inhibition zone of the isolated bacteria exceeds the inhibition zone established for the antimicrobial disc indicated in the testing panel.32
Resistant (R): When isolated bacteria’s inhibition zone is less than the inhibition zone established for the antimicrobial disc stated in the testing panel.32
Intermediate (I): When the inhibition zone of isolated bacteria is smaller than or equal to the inhibition zone established for the antimicrobial disc listed in the testing panel.32
Multidrug-resistant (MDR): Multidrug drug resistance is a laboratory-confirmed resistance to more than one agent in three or more categories of antibiotics.30
Results
Sociodemographic Characteristics of Study Participants
This study included 213 pregnant women who were attending ANC at Bule Hora University Teaching Hospital. The mean (SD) age of the study participants was 26.83 (5.360), ranging from 17 to 39 years. Seventy-two (33.8%) were between the ages of 25 and 29. The majority of the study participants (194, 91.1%) were married; 139 (65.3%) were urban dwellers; and 188 (88.3%) were unemployed. Seventy-three (32.9%) of the study participants had no formal education (Table 1).
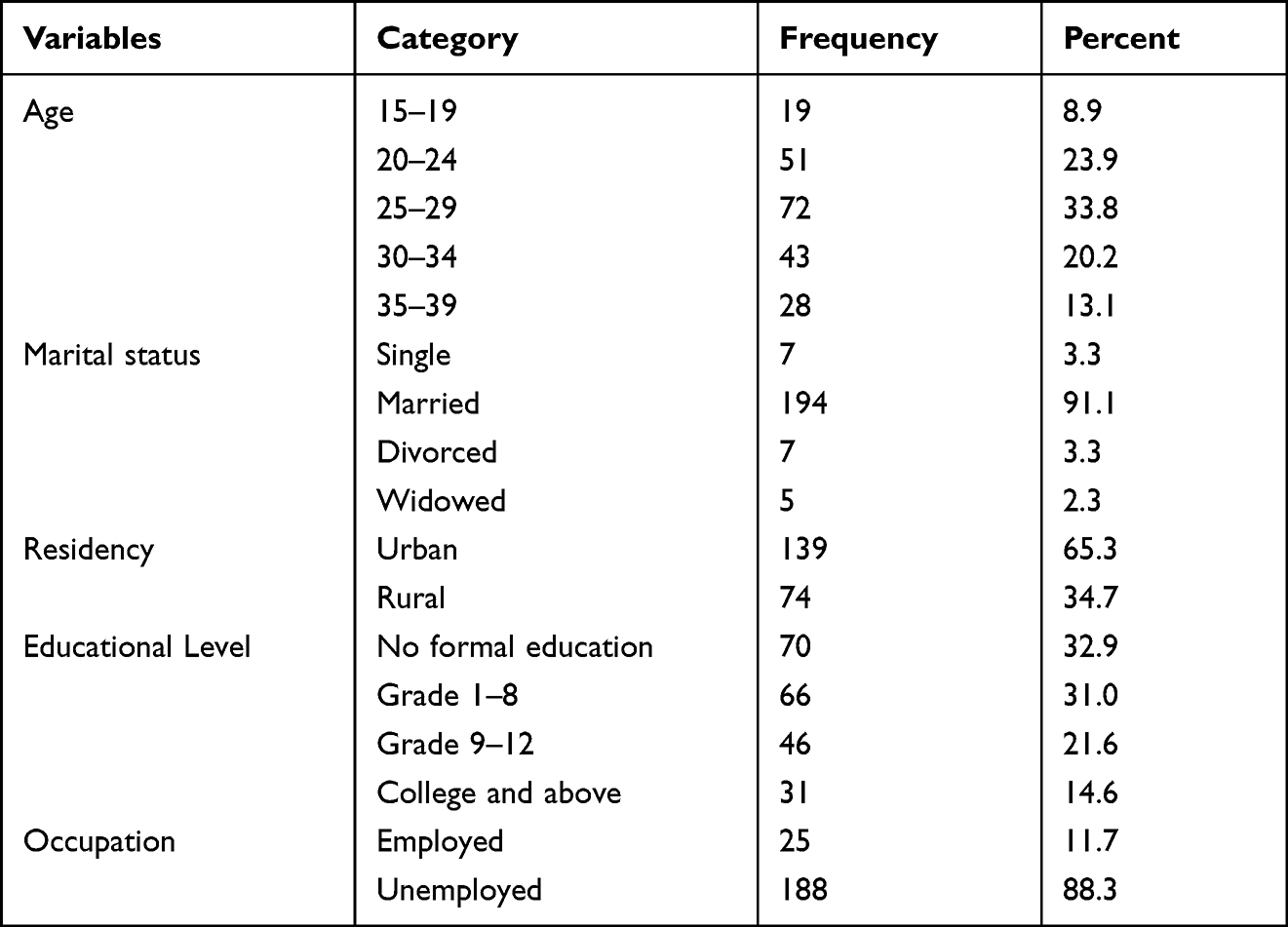 |
Table 1 Sociodemographic Features of Pregnant Women Following Antenatal Care at BHUTH from June 1 to August 30, 2022 (n = 213) |
The Prevalence of Group B Streptococcus
In the current study, the overall prevalence of Group B Streptococcus was 36/213 (16.9%) (95% CI: 0.121–0.226) among pregnant women between gestational weeks 35–37.
Antimicrobial Susceptibility Pattern of Group B Streptococcus Isolates
The susceptibility pattern of GBS isolates was checked by using seven different antibiotic discs. The ranges of nonsusceptibility for GBS isolates were from 2.8% to 58.3%. The GBS bacterium isolated in this population had the highest resistance to cefepime (21/36; 58.3%). Most GBS isolates showed high susceptibility to vancomycin (35/36; 97.2%), ampicillin (33/36; 91.7%), and penicillin (31/36; 86.1%) (Table 2).
 |
Table 2 Antimicrobial Susceptibility Profile of GBS Isolated from Pregnant Women Attending Antenatal Care at BHUTH from June 1 to August 30, 2022 |
Multidrug Resistance Pattern of Group B Streptococcus Isolates
Of all GBS isolates, only four were sensitive to all seven antibiotic discs used; 17 (47.2%) were resistant to only one drug; 10 (27.8%) were resistant to two antimicrobials, and 4 (11.1%) were resistant to three different antimicrobials. Multidrug-resistant in this study was 5 (13.9%) (Table 3).
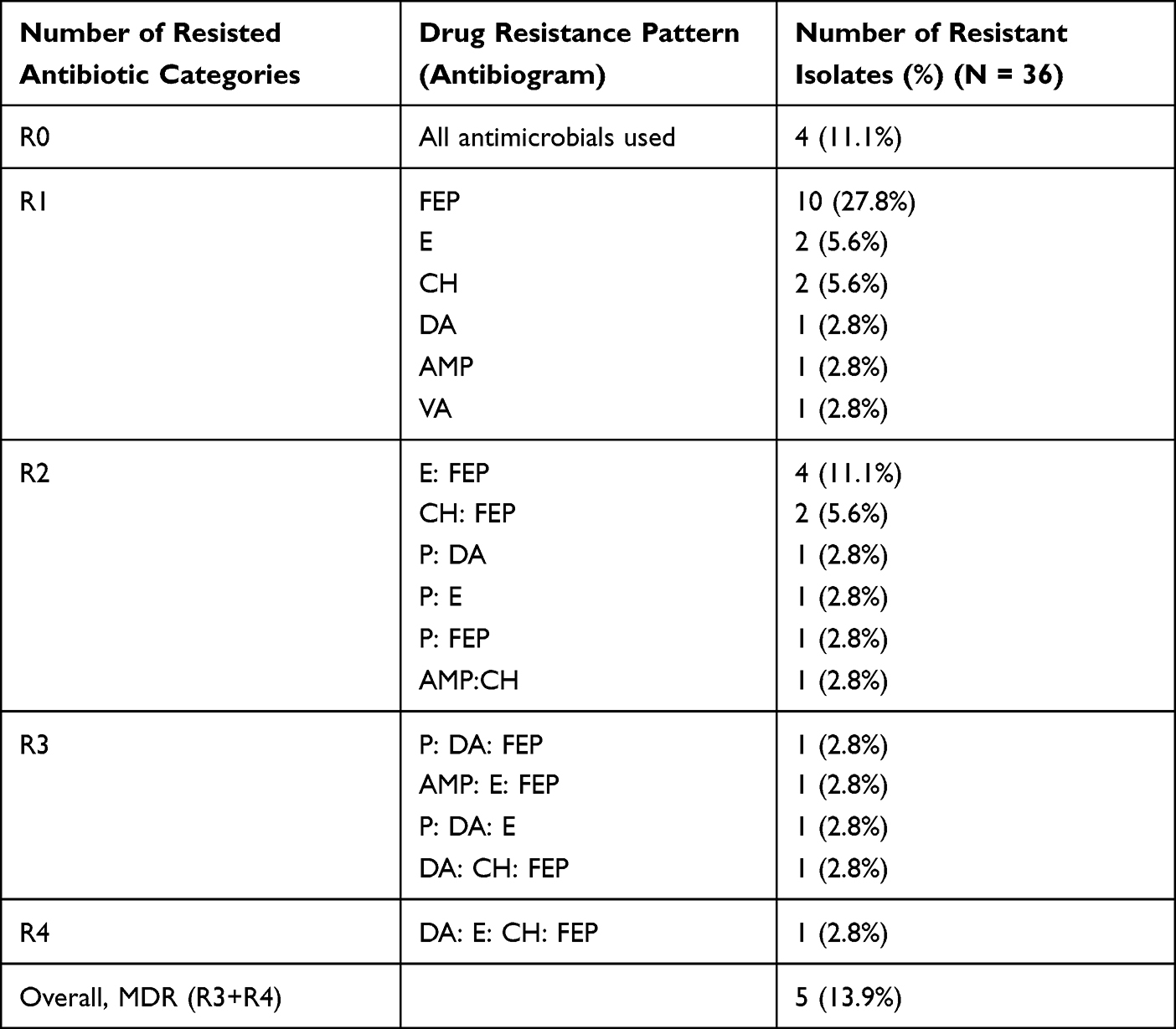 |
Table 3 Multidrug Resistance Pattern of Group B Streptococcus Isolated from Pregnant Women Attending BHUTH from June 1 to August 30, 2022 |
Factors Associated with Group B Streptococcus Colonization
In the bivariable analysis, all variables were assessed, and the variables with p-values 0.25 became candidates for multivariable analysis. Preterm birth history increased the probability of GBS colonization in pregnant women by 3 times (AOR: 3.406, 95% CI: 1.305–8.892, p-value: 0.012) compared to non-preterm birth history. Pregnant women with a history of premature rupture of the membrane (PROM) had a three times (AOR: 3.351, 95% CI: 1.189–9.449, p-value: 0.022) higher likelihood of developing GBS colonization than those without a history of PROM. Additionally, pregnant women with a history of stillbirth were twice (AOR: 2.876, 95% CI: 1.073–7.708, p = 0.036) more likely to have a stillbirth (Table 4).
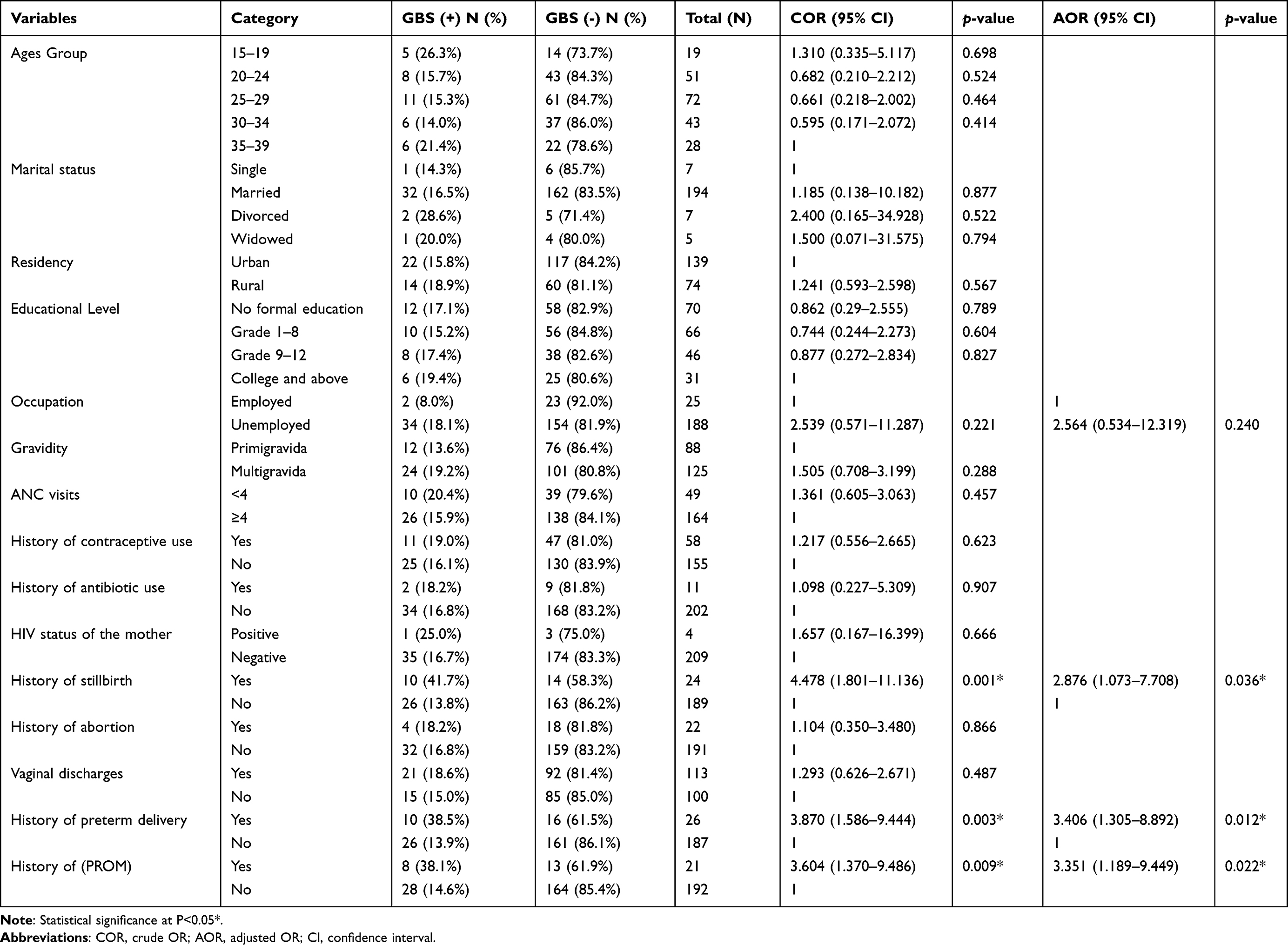 |
Table 4 Factors Associated with GBS Prevalence Among Pregnant Women Attending Antenatal Care at BHUTH from June 1 to August 2022 (n = 213) |
Discussion
For women and newborns, GBS is a major source of infection and sepsis.33 Between 114,000 and 204,000 invasive cases, 147,000 stillbirths, and infant deaths occur as a result of it each year around the world. Furthermore, infant mortality rates in rich and poor nations, which range from 10 to 15% and 40 to 58%, respectively, amply demonstrate that the vertical transmission of GBS continues to be a global issue.34–36 With regional variations of 11–35%, the global prevalence of GBS in pregnant women is estimated to be 18%,11 with Africa bearing the heaviest share of severe neonatal infections, stillbirths, and infant fatalities.34,37 Ethiopia has a high rate of newborn mortality and GBS illnesses.21,38
In this study, a total of 213 pregnant women who were between the 35th and 37th weeks participated, with an overall prevalence of 16.9% (95% CI: 0.121–0.226) of GBS colonization. The prevalence of GBS among pregnant women in the present study was comparable with GBS among pregnant women reported from Bahir Dar (18.5%), Addis Ababa (14.6%), Jigjiga (15.9%), Hawassa (15.7%), Cameroon (14%), Asia (18%), and Jordan (19.5%).2,14,26,31,39–41 In contrast to the present finding, a low prevalence of GBS was reported in Tigray (11.3%), Addis Ababa (7.3%), Cameroon (8.69%), Burkina Faso (6.05%), Iraq (6.7%), and China (3.5–8.7%).8,18,42–45 These results indicate that the prevalence of maternal GBS colonization, which is the primary risk factor for the early onset of GBS disease, differs in different countries and within the same country.11 The variation might be due to the sample size variation, the gestational period of participants, or geographical location.
Moreover, a higher prevalence of GBS was reported in Gondar (25.5%),20 Addis Ababa (23.6%),46 South Africa (30.9%),47 Nigeria (29.4%),48 Trinidad and Tobago (29%),49 and Italy (25.5%)50 compared to the current findings. The possible reason could be due to variations in sample size, method employed, and culture media used. Similarly, the difference in prevalence could be explained by the laboratory method used in the identification of GBS.11 This study used blood agar plates, which have a lower ability to isolate GBS compared to selective media such as colistin and nalidixic acid agar and Todd-Hewitt broth used in other studies.
Vancomycin is recommended for GBS-colonised mothers with a high risk of anaphylaxis to penicillin and if the isolates are resistant to clindamycin.51 In the present study, the percentage of susceptibility to vancomycin was 97.2%, which was in line with the study reported by Bahir Dar (96.3%),31 Jigjiga (96.6%),2 and Addis Ababa (93.3%).46 The study conducted in Burkina Faso reported no GBS isolates resistant to vancomycin.8 However, it is higher than the study conducted in Palestine (45.7%).52 The possible reason for this difference in susceptibility might be due to the infrequent use of this antibiotic, as it is an alternative drug for patients at high anaphylaxis risk to penicillin and is used only when GBS is resistant to clindamycin and erythromycin drugs or when susceptibility is unknown.53
The percentage of susceptibility to penicillin (86.1%) was comparable with previous reports from Bahir Dar (88.9%),31 Jigjiga (86.2%),2 and Italy (87.93%).50 However, a study conducted in Namibia reported the absence of GBS isolate resistance to penicillin.54 Moreover, the susceptibility to penicillin reported in this study is higher than that in a previous study conducted in Addis Ababa (penicillin 42.3%).46 This did not match the CDC’s 2010 guidelines study, which did not find any resistance to penicillin. The expanded use of beta-lactam antimicrobials in the treatment of several infective clinical syndromes, the non-restrictive availability of these drugs in different areas at lower prices, and the free accessibility of purchases over the counter might be the causes of the emergence of GBS-resistant strains in this environment. This reduced susceptibility could also be due to acquired mutations in the penicillin-binding protein domain and penicillin-binding protein alterations in noninvasive GBS isolates.55,56
The percentage of susceptibility to ampicillin (91.7%) was in agreement with previous findings from Gondar (90.8%),20 Bahir Dar (90.7%),31 and Jigjiga (93.1%).2 In contrast, the study conducted in Namibia and Burkina Faso reported that all GBS isolates were susceptible to ampicillin (100%).8,54 This implies that this drug is still good as a first choice to manage pregnant women colonised with GBS.
The Centres for Disease Control (CDC) guidelines recommend testing GBS isolates for susceptibility to clindamycin and erythromycin, as they are the drugs of choice for penicillin-allergic women at high risk for anaphylaxis.51 The percentage of susceptibility to clindamycin was 83.3%, which was consistent with studies reported from Ethiopia (86.4%)46 and Asia (84%).57 However, it is higher than the study reported from Bahir Dar city (66.7%),31 Palestine (70.8%),52 and Italy (56.25%).50 Since clindamycin is another alternative antibiotic recommended by the CDC for pregnant women who are allergic to penicillin, the resistance level underlines the need to carry out a susceptibility test. This might be due to the widespread use of antibiotics.
The percentage of nonsusceptibility to erythromycin (27.8%) was correlated with studies conducted in Gondar (26.5%),20 South America (31.6%),49 Palestine (25%)52 and Korea (28%).57 The current CDC advice that an antibiotic susceptibility test should be carried out if erythromycin medication is required to prevent neonatal GBS infection is highly supported by the rate of erythromycin resistance in the GBS isolates. Erythromycin is used frequently when beta-lactams have run their course, not just in cases of allergy.
In the present study, the percentage of nonsusceptibility to chloramphenicol was 19.4%. This finding was comparable with a study from Ethiopia (20.4%).46 This finding is higher compared to the study reported from Jigjiga (3.4%).2 The possible reason for this difference could be inappropriate use and empirical prescription of this drug from the local pharmacy. Cefepime had the highest level of resistance in the current study (58.3%). This result was in line with the Addis Ababa study’s findings (cefepime 59.4%).46 This can be caused by the extensive use of these medicines, the simplicity of obtaining antibiotics, or the careless use of antimicrobial medications in this region. Due to the fact that this antibiotic is advised for use with all Streptococcus, the level of resistance highlights the necessity of doing a susceptibility test.
Of the independent variables that were assessed, history of premature birth, history of preterm delivery, and history of premature rupture of the membrane were statistically significantly associated with the prevalence of GBS. In the present study, a history of stillbirth was statistically significantly associated with the prevalence of GBS, which was in agreement with the studies reported from Cameroon43 and Ethiopia.31 Several findings indicate that GBS infection during pregnancy can result in issues such as premature membrane rupture, stillbirth, and preterm delivery. GBS is possibly a significant and curable cause of stillbirth, particularly in nations with inadequate resources like Ethiopia.58
According to research done in Bahir Dar,31 Jigjiga,2 and Palestine,52 a history of preterm delivery was substantially related to the prevalence of GBS. Preterm births are more prevalent in women who were colonized with GBS than in women who were not.59 The other variable that was significantly associated with the prevalence of GBS was a history of premature rupture of the membrane, which was similar to the study reported from Ethiopia.2,42 GBS is the most common bacterium that causes premature rupture of membranes due to an infection in the vagina, cervix, and uterus, and this infection can be detrimental to pregnant women and their neonates. Therefore, GBS might be an important component that should be ruled out in this case.6
Limitations of the Study
It was not possible to perform serotypes due to the absence of laboratory reagents. The unavailability of selective media such as colistin, nalidixic acid agar, and Todd-Hewitt broth Besides, double confirmation of resistant strains was not performed due to the limitations of the E-strip method or microbroth dilution to identify the minimum inhibitory concentration. Penicillin nonsusceptibility in the current study was interestingly high, and it needs further investigation as its resistance in GBS is an alarming issue.
Conclusion and Recommendations
In the present study, the overall prevalence of Group B Streptococcus was 16.9% among pregnant women attending antenatal care at Bule Hora University Teaching Hospital. The highest percentage of GBS susceptibility was to vancomycin, while the least susceptibility was to erythromycin. The highest resistance was recorded for cefepime. GBS colonization was found to be independently associated with a history of premature rupture of the membrane, a history of stillbirth, and a history of preterm delivery.
To assist in determining the best IAP, stakeholders should take routine culture-based bacteriological screening of pregnant women into consideration. The fight against antimicrobial resistance needs to be stepped up. More extensive research should be done to determine the prevalence of GBS in newborns and possible treatments. We also recommend further investigations for penicillin nonsusceptibility, as it was interestingly high in the current study. Future research should be done to determine the serotype distributions of GBS in this population since it is important to keep track of regional variations in serotype distribution in order to create and administer a successful GBS vaccine. A general awareness campaign and ongoing health education for pregnant mothers attending antenatal clinics were advised to teach them about their health, prevent hazardous behaviours, and address the risk of GBS during their pregnancy.
Abbreviations
ANC, Antenatal Care; AST, Antimicrobial Susceptibility Test; BHUTH, Bule Hora University Teaching Hospital; CDC, Center for disease prevention and control; CLSI, Clinical and laboratory standard institute guidelines; GBS, Group B Streptococcus; HIV, Human immunodeficiency virus; IAP, Intrapartum antibiotic prophylaxis; IHRERC, Institutional health research ethics review committee; SE, Standard error; SBA, Sheep blood agar; SOP, Standard operating procedure; STI, Sexually transmitted infection; UTI, Urinary tract infection; WHO, World Health Organization.
Data Sharing Statement
Data for this research are available for this work and can be accessed from the corresponding author.
Ethical Approval and Consent to Participate
The Institutional Health Research Ethics Review Committee of Bulehora University (IHRERC/2022) examined and approved the study protocol. Bule Hora University Teaching Hospital received a formal letter of support. All procedures were carried out per the necessary standards and laws (Declarations of Helsinki). All subjects, and/or their parent, husband, or legal guardian for those under the age of 18, provided informed, voluntary, written, and signed consent throughout the study. Every participant received information on the study, including its goals, methods, potential risks, and advantages. Participants in the study were made aware of their right to decline or leave the study at any time. The study participants were unaffected by their decision to decline participation. By omitting names and other identifiers from the questionnaire, participants’ data were kept secret. Women who tested positive for GBS were connected to their doctors and given the recommended treatments.
Acknowledgments
First of all, we want to express our gratitude to Bule Hora University for providing us with the opportunity to develop a research project. We also like to thank the medical laboratory science staff for their help and thoughtful approach. Last but not least, we want to convey our sincere gratitude to the study participants who had ANC at Bule Hora University Teaching Hospital.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The authors declare no potential conflicts of interest concerning the research, authorship, and publication of this paper.
References
1. Schrag SJ, Verani JR. Intrapartum antibiotic prophylaxis for the prevention of perinatal group B streptococcal disease: experience in the United States and implications for a potential group B streptococcal vaccine. Vaccine. 2013;31:D20–D6. doi:10.1016/j.vaccine.2012.11.056
2. Tesfaye A, Melese A, Derbie A, Falkinham J. Antimicrobial resistance profile and associated factors of group B Streptococci colonization among pregnant women attending antenatal clinics in Jigjiga, Southeast Ethiopia. Int J Microbiol. 2022;2022:1–8. doi:10.1155/2022/9910842
3. CDC R. Prevention of Perinatal Group B Streptococcal Disease. Atlanta: MMWR Series; 2010.
4. Shiferawu S, Mekonen M, Baza D, Lera T. Prevalence of Group B Streptococcus, its associated factors and antimicrobial susceptibility pattern among pregnant women attending antenatal care at Arbaminch Hospital, South Ethiopia. Am J Health Res. 2019;7(6):104–115. doi:10.11648/j.ajhr.20190706.12
5. Alp F, Findik D, Dagi HT, Arslan U, Pekin AT, Yilmaz SA. Screening and genotyping of group B streptococcus in pregnant and non-pregnant women in Turkey. J Infect Dev Ctries. 2016;10(03):222–226. doi:10.3855/jidc.6190
6. Akoh CC, Pressman EK, Cooper E, Queenan RA, Pillittere J, O’Brien KO. Prevalence and risk factors for infections in a pregnant adolescent population. J Pediatr Adolesc Gynecol. 2017;30(1):71–75. doi:10.1016/j.jpag.2016.08.001
7. Tanno D, Saito K, Ohashi K, Toyokawa M, Yamadera Y, Shimura H. Matrix-assisted laser desorption ionization–time-of-flight mass spectrometry with time-of-flight peak analysis for rapid and accurate detection of group b streptococcus in pregnant women. Microbiol Spectr. 2022;10(3):e01732–21. doi:10.1128/spectrum.01732-21
8. Ouédraogo A-S, Sawadogo Y, Somé DA, et al. Prevalence of Group B Streptococcus among pregnant women in bobo-dioulasso (Burkina Faso). Open J Med Microbiol. 2019;9(3):63–76. doi:10.4236/ojmm.2019.93008
9. Lin SM, Zhi Y, Ahn KB, Lim S, Seo HS. Status of group B streptococcal vaccine development. Clin Exp Vaccine Res. 2018;7(1):76–81. doi:10.7774/cevr.2018.7.1.76
10. Kwatra G, Cunnington MC, Merrall E, et al. Prevalence of maternal colonisation with group B streptococcus: a systematic review and meta-analysis. Lancet Infect Dis. 2016;16(9):1076–1084. doi:10.1016/S1473-3099(16)30055-X
11. Russell NJ, Seale AC, O’Driscoll M, et al. Maternal colonization with group B Streptococcus and serotype distribution worldwide: systematic review and meta-analyses. Clin Infect Dis. 2017;65(suppl_2):S100–S11. doi:10.1093/cid/cix658
12. Kum-Nji P, Meloy L, Pierce J, Ritter A, Wheeler R, Spradley FT. Group B streptococcal colonization: prevalence and impact of smoking in women delivering term or near term neonates in a large tertiary care hospital in the southern United States. PLoS One. 2020;15(9):e0239294. doi:10.1371/journal.pone.0239294
13. YektaKooshali MH, Hamidi M, Tousi SMTR, Nikokar I. Prevalence of group B streptococcus colonization in Iranian pregnant women: a systematic review and meta-analysis. Int J Reprod BioMed. 2018;16(12). doi:10.18502/ijrm.v16i12.3679
14. Clouse K, Shehabi A, Suleimat AM, et al. High prevalence of Group B Streptococcus colonization among pregnant women in Amman, Jordan. BMC Pregnancy Childbirth. 2019;19(1):1–8. doi:10.1186/s12884-019-2317-4
15. Buca D, Winberg P, Rizzo G, et al. Prenatal risk factors for urgent atrial septostomy at birth in fetuses with transposition of the great arteries: a systematic review and meta-analysis. J Mater Fetal Neonatal Med. 2022;35(3):598–606. doi:10.1080/14767058.2020.1725883
16. Lekala LM, Mavenyengwa RT, Moyo SR, et al. Risk factors associated with group B streptococcus colonization and their effect on pregnancy outcome. J Gynecol Obstet. 2015;3(6):121–128. doi:10.11648/j.jgo.20150306.14
17. Gizachew M, Tiruneh M, Moges F, Tessema B. Streptococcus agalactiae maternal colonization, antibiotic resistance and serotype profiles in Africa: a meta-analysis. Ann Clin Microbiol Antimicrob. 2019;18(1):1–14. doi:10.1186/s12941-019-0313-1
18. Woldu ZL, Teklehaimanot TG, Waji ST, Gebremariam MY. The prevalence of Group B Streptococus recto-vaginal colonization and antimicrobial susceptibility pattern in pregnant mothers at two hospitals of Addis Ababa, Ethiopia. Reprod Health. 2014;11(1):1–4. doi:10.1186/1742-4755-11-80
19. Verani JR, McGee L, Schrag SJ. Prevention of Perinatal Group B Streptococcal Disease: Revised Guidelines from CDC, 2010. Department of Health and Human Services, Centers for Disease Control and …; 2010.
20. Gizachew M, Tiruneh M, Moges F, Adefris M, Tigabu Z, Tessema B. Streptococcus agalactiae from Ethiopian pregnant women; prevalence, associated factors and antimicrobial resistance: alarming for prophylaxis. Ann Clin Microbiol Antimicrob. 2019;18(1):1–9. doi:10.1186/s12941-019-0303-3
21. Ali MM, Mulate YW, Woldetsadik DA, et al. Group B streptococci carriage rate and serotype distribution among mother newborn dyads attending Tikur Anbesa Specialized Hospital, Ethiopia. Ethiop Med J. 2020;58(2):1–7.
22. Moraleda C, Benmessaoud R, Esteban J, et al. Prevalence, antimicrobial resistance and serotype distribution of Group B Streptococcus isolated among pregnant women and newborns in Rabat, Morocco. J Med Microbiol. 2018;67(5):652–661. doi:10.1099/jmm.0.000720
23. Gizachew M, Tiruneh M, Moges F, Adefris M, Tigabu Z, Tessema B. Proportion of Streptococcus agalactiae vertical transmission and associated risk factors among Ethiopian mother-newborn dyads, Northwest Ethiopia. Sci Rep. 2020;10(1):3477. doi:10.1038/s41598-020-60447-y
24. Mengist A, Kannan H, Abdissa A. Prevalence and antimicrobial susceptibility pattern of anorectal and vaginal group B Streptococci isolates among pregnant women in Jimma, Ethiopia. BMC Res Notes. 2016;9(1):1–5. doi:10.1186/s13104-016-2158-4
25. Gizachew M, Tiruneh M, Moges F, Adefris M, Tigabu Z, Tessema B. Newborn colonization and antibiotic susceptibility patterns of Streptococcus agalactiae at the University of Gondar Referral Hospital, Northwest Ethiopia. BMC Pediatr. 2018;18(1):1–11. doi:10.1186/s12887-018-1350-1
26. Ali MM, Woldeamanuel Y, Woldetsadik DA, et al. Prevalence of group B streptococcus among pregnant women and newborns at Hawassa University comprehensive specialized hospital, Hawassa, Ethiopia. BMC Infect Dis. 2019;19(1):1–9. doi:10.1186/s12879-019-3859-9
27. Rahbar M, Hajia M, Mohammadzadeh M. Urinary Tract Infections caused by Group B Streptococcus in adult women: survey of 11800 urine culture results. Iranian J Pathol. 2012;7(1):32–37.
28. Afhami S, Borumand MA, Bazzaz NE, et al. Antimicrobial resistance pattern of Acinetobacter; a multicenter study, comparing European Committee on Antimicrobial Susceptibility Testing (EUCAST) and the Clinical and Laboratory Standards Institute (CLSI); evaluation of susceptibility testing methods for polymyxin. Immunopathol Persa. 2020;7(1):e04–e.
29. Tague AJ, Putsathit P, Hammer KA, et al. Cationic biaryl 1, 2, 3-triazolyl peptidomimetic amphiphiles: synthesis, antibacterial evaluation and preliminary mechanism of action studies. Eur J Med Chem. 2019;168:386–404. doi:10.1016/j.ejmech.2019.02.013
30. Magiorakos A-P, Srinivasan A, Carey RB, et al. Multidrug-resistant, extensively drug-resistant and pandrug-resistant bacteria: an international expert proposal for interim standard definitions for acquired resistance. Clin Microbiol Infect. 2012;18(3):268–281. doi:10.1111/j.1469-0691.2011.03570.x
31. Leykun Y, Genet C, Mulu W. Group B streptococci vaginal-recto colonization, vertical transmission to newborns, antimicrobial susceptibility profile and associated factors in selected health facilities of Bahir Dar city: a cross-sectional study. Infect Drug Resist. 2021;14:5457–5472. doi:10.2147/IDR.S343429
32. Humphries R, Bobenchik AM, Hindler JA, Schuetz AN, McAdam AJ. Overview of changes to the clinical and laboratory standards institute performance standards for antimicrobial susceptibility testing, M100. J Clin Microbiol. 2021;59(12):e00213–e00221. doi:10.1128/JCM.00213-21
33. Alfouzan W, Gaddar N, Dhar R, Rabaan AA. A study of group B streptococcus in pregnant women in Lebanon: prevalence, risk factors, vaginal flora and antimicrobial susceptibility. Sepsis. 2021;4:7.
34. Seale AC, Bianchi-Jassir F, Russell NJ, et al. Estimates of the burden of group B streptococcal disease worldwide for pregnant women, stillbirths, and children. Clin Infect Dis. 2017;65(suppl_2):S200–S19. doi:10.1093/cid/cix664
35. Ku LC, Boggess KA, Cohen-Wolkowiez M. Bacterial meningitis in infants. Clin Perinatol. 2015;42(1):29–45. doi:10.1016/j.clp.2014.10.004
36. Oordt-Speets AM, Bolijn R, van Hoorn RC, Bhavsar A, Kyaw MH, Borrow R. Global etiology of bacterial meningitis: a systematic review and meta-analysis. PLoS One. 2018;13(6):e0198772. doi:10.1371/journal.pone.0198772
37. Sinha A, Russell LB, Tomczyk S, et al. Disease burden of group B Streptococcus among infants in sub-Saharan Africa: a systematic literature review and meta-analysis. Pediatr Infect Dis J. 2016;35(9):933. doi:10.1097/INF.0000000000001233
38. Debelew GT, Afework MF, Yalew AW, Weitkamp J-H. Determinants and causes of neonatal mortality in Jimma zone, southwest Ethiopia: a multilevel analysis of prospective follow up study. PLoS One. 2014;9(9):e107184. doi:10.1371/journal.pone.0107184
39. Assefa S, Desta K, Lema T. Group B streptococci vaginal colonization and drug susceptibility pattern among pregnant women attending in selected public antenatal care centers in Addis Ababa, Ethiopia. BMC Pregnancy Childbirth. 2018;18(1):1–9. doi:10.1186/s12884-018-1791-4
40. Dilrukshi G, Kottahachchi J, Dissanayake D, et al. Group B Streptococcus colonisation and their antimicrobial susceptibility among pregnant women attending antenatal clinics in tertiary care hospitals in the Western Province of Sri Lanka. J Obstet Gynaecol. 2021;41(1):1–6. doi:10.1080/01443615.2020.1716313
41. Nkembe NM, Kamga HG, Baiye WA, Chafa AB, Njotang PN. Streptococcus agalactiae prevalence and antimicrobial susceptibility pattern in vaginal and anorectal swabs of pregnant women at a tertiary hospital in Cameroon. BMC Res Notes. 2018;11(1):1–6. doi:10.1186/s13104-018-3589-x
42. Gebremeskel TK, Zeleke TA, Mihret A, Tikue MD. Prevalence and antibiotic susceptibility pattern of Streptococcus agalactiae among pregnant women at Adigrat Zonal Hospital and Adigrat Health Center, Tigray, Ethiopia. J Gynecol Obstet. 2015;3(2):29–35. doi:10.11648/j.jgo.20150302.13
43. Sama LF, Noubom M, Kenne C, et al. Group B Streptococcus colonisation, prevalence, associated risk factors and antimicrobial susceptibility pattern among pregnant women attending antenatal care at Dschang District Hospital, West Region of Cameroon: a hospital‐based cross‐sectional study. Int J Clin Pract. 2021;75(10):e14683. doi:10.1111/ijcp.14683
44. Majeed HT, Aljanaby AAJ. Antibiotic susceptibility patterns and prevalence of some extended spectrum beta-lactamases genes in gram-negative bacteria isolated from patients infected with urinary tract infections in Al-Najaf City, Iraq. Avicenna J Med Biotechnol. 2019;11(2):192.
45. Ge Y, Pan F, Bai R, et al. Prevalence of group B streptococcus colonization in pregnant women in Jiangsu, East China. BMC Infect Dis. 2021;21(1):1–5. doi:10.1186/s12879-021-06186-5
46. Fantahun Y, Sebre S, Seman A, Kumbi S. Magnitude of maternal vaginal colonization of Group B Streptococcus and neonatal transmission in pregnant women during labor and delivery at Tikur Anbessa Specialized Hospital, Addis Ababa, Ethiopia. Ethiop Med J. 2020;58:1–9.
47. Bolukaoto JY, Monyama CM, Chukwu MO, et al. Antibiotic resistance of Streptococcus agalactiae isolated from pregnant women in Garankuwa, South Africa. BMC Res Notes. 2015;8(1):1–7. doi:10.1186/s13104-015-1328-0
48. Akinlolu J, Omololu-Aso J, Owolabi A, Omololu-Aso O. Molecular epidemiological status of Group B Streptococcus in Ile Ife South Western Nigeria. Arch Med. 2018;10(3):4.
49. Akpaka PE, Henry K, Thompson R, Unakal C. Colonization of Streptococcus agalactiae among pregnant patients in Trinidad and Tobago. IJID Reg. 2022;3:96–100. doi:10.1016/j.ijregi.2022.03.010
50. Matani C, Trezzi M, Matteini A, Catalani C, Messeri D, Catalani C. Streptococcus agalactiae: prevalence of antimicrobial resistance in vaginal and rectal swabs in Italian pregnant women. Infez Med. 2016;24(3):217–221.
51. Nanduri SA, Petit S, Smelser C, et al. Epidemiology of invasive early-onset and late-onset group B streptococcal disease in the United States, 2006 to 2015: multistate laboratory and population-based surveillance. JAMA Pediatr. 2019;173(3):224–233. doi:10.1001/jamapediatrics.2018.4826
52. Qadi M, AbuTaha A, Al-Shehab R, et al. Prevalence and risk factors of Group B Streptococcus Colonization in pregnant women: a pilot study in Palestine. Can J Infect Dis Med Microbiol. 2021;2021:1–8. doi:10.1155/2021/8686550
53. Apgar BS, Greenberg GM, Yen G. Prevention of group B streptococcal disease in the newborn. Am Fam Physician. 2005;71(5):903–910.
54. Haimbodi EL, Mukesi M, Moyo SR. Prevalence and molecular characterization of group B streptococcus in pregnant women from hospitals in Ohangwena and Oshikoto regions of Namibia. BMC Microbiol. 2021;21(1):1–9. doi:10.1186/s12866-021-02283-2
55. Dahesh S, Hensler ME, Van Sorge NM, et al. Point mutation in the group B streptococcal pbp2x gene conferring decreased susceptibility to β-lactam antibiotics. Antimicrob Agents Chemother. 2008;52(8):2915–2918. doi:10.1128/AAC.00461-08
56. Nagano N, Nagano Y, Toyama M, et al. Nosocomial spread of multidrug-resistant group B streptococci with reduced penicillin susceptibility belonging to clonal complex 1. J Antimicrob Chemother. 2012;67(4):849–856. doi:10.1093/jac/dkr546
57. Choi SJ, Kang J, Uh Y. Recent epidemiological changes in group B streptococcus among pregnant Korean women. Ann Lab Med. 2021;41(4):380–385. doi:10.3343/alm.2021.41.4.380
58. Seale AC, Blencowe H, Bianchi-Jassir F, et al. Stillbirth with group B Streptococcus disease worldwide: systematic review and meta-analyses. Clin Infect Dis. 2017;65(suppl_2):S125–S32. doi:10.1093/cid/cix585
59. Feikin DR, Thorsen P, Zywicki S, Arpi M, Westergaard JG, Schuchat A. Association between colonization with group B streptococci during pregnancy and preterm delivery among Danish women. Am J Obstet Gynecol. 2001;184(3):427–433. doi:10.1067/mob.2001.109936
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.