")
Back to Journals » Diabetes, Metabolic Syndrome and Obesity » Volume 17
Prevalence and Risk Factors of Non-Alcoholic Fatty Liver Disease (NAFLD) in Non-Obese Patients with Schizophrenia: A Retrospective Study
Authors Yi W, Wu H, Fu W, Feng H, Huang J, Li H, Song Z , Chen Y, Zheng Y, She S
Received 1 December 2023
Accepted for publication 8 February 2024
Published 20 February 2024 Volume 2024:17 Pages 841—849
DOI https://doi.org/10.2147/DMSO.S437811
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Konstantinos Tziomalos
Wenying Yi,1,2 Haibo Wu,1,2 Weibin Fu,1,2 Huimei Feng,1,2 Jie Huang,1,2 Haijing Li,1,2 Zhen Song,1,2 Yuwei Chen,1,2 Yingjun Zheng,1,2 Shenglin She1,2
1Department of Psychiatry, the Affiliated Brain Hospital of Guangzhou Medical University, Guangzhou, People’s Republic of China; 2Key Laboratory of Neurogenetics and Channelopathies of Guangdong Province and the Ministry of Education of China Guangzhou Medical University, Guangzhou, People’s Republic of China
Correspondence: Shenglin She, Department of Psychiatry, the Affiliated Brain Hospital of Guangzhou MedicalUniversity, No. 36 Mingxin Road, Liwan District, Guangzhou, People’s Republic of China, Tel +86-13825154669, Fax +86-20-82068107, Email [email protected]
Background: To assess the prevalence and risk factors of NAFLD in non-obese patients with schizophrenia in a public psychiatric hospital in China.
Methods: A total of 1,305 adult inpatients with schizophrenia in 2019 were included in this retrospective study. Body mass index (BMI) ≥ 25 kg/m2 was considered obese, and BMI < 25 kg/m2 was considered non-obese. We obtained the data from electronic records of the Affiliated Brain Hospital of Guangzhou Medical University.
Results: A total of 1,045 non-obese patients and 260 obese patients were included in this study. The prevalence of NAFLD in non-obese patients was 25.0%, and it was much lower that in the obese patients (25.0% vs 64.6%, p < 0.001). Among the non-obese patients, there were significant differences in age, BMI, alanine aminotransferase (ALT), metabolic indices, and the prevalence of diabetes and hypertension between patients with NAFLD and patients without NAFLD. According to the results of binary logistic regression analysis, age, BMI, ALT, triglyceride (TG) and diabetes were significantly related to NAFLD among non-obese patients with schizophrenia. In contrast, HDL-C was was negatively associated with NAFLD among non-obese patients.
Conclusion: This study suggested that NAFLD was common in patients with schizophrenia, even in non-obese patients with schizophrenia. In non-obese patients with schizophrenia, age, BMI, ALT, TG and diabetes are significantly associated with NAFLD. Moreover, HDL-C level was an independent protective factor against NAFLD. Given the adverse outcomes of NAFLD, it is necessary to increase awareness of NAFLD in patients with schizophrenia, especially in non-obese patients with schizophrenia.
Keywords: schizophrenia, NAFLD, non-obese, obese, risk factors, China
Introduction
NAFLD is a prevalent chronic liver disease worldwide, with an estimated global prevalence at 29.8%.1 NAFLD is positively associated with the risk of extra-hepatic tumors, cardiovascular disease, diabetes and metabolic syndrome.2 Compared with patients without NAFLD, patients with NAFLD have an increased risk of all-cause mortality.3 The number of deaths caused by NAFLD has significantly increased to 168,970 in 2019 since 1990.4
Obesity is associated with a 3.5 times higher risk of NAFLD, and BMI is significantly associated the risk of developing NAFLD.5 Although NAFLD is more prevalent in obese subjects, it is also common in non-obese individuals. A meta-analysis reported that in the general population, the frequency of NAFLD ranges from 25% to higher than 50%, and approximately 40% of subjects with NAFLD worldwide can be classified as non-obese.6 Compared to obese patients with NAFLD, non-obese individuals with NAFLD had less severe metabolic profiles, while evidence found that non-obese individuals with NAFLD also had increased all-cause mortality and substantial comorbidities, including hypertension, diabetes, cardiovascular disease.6
Schizophrenia is a common and severe mental disorder. People with schizophrenia have shorter lifespans (by 15–20 years) and higher all-cause mortality rates.7 Diabetes and cardio-cerebrovascular system disorders are attributed to the higher mortality rates in schizophrenia.7 It is widely reported that patients with schizophrenia have higher risk to experience obesity and metabolic abnormalities, which are closely associated with diabetes and cardio-cerebrovascular system disorders.8 Regardless of the diagnostic criteria of metabolic syndrome, the prevalence of metabolic syndrome in patients with schizophrenia was higher than that in the health controls.9 However, only a minority of patients with schizophrenia pay attention to balanced diet and physical exercise.10 Studies have shown that obesity and metabolic syndrome are significantly associated with NAFLD in the general population.11 It could be speculated that the prevalence of NAFLD may be higher in patients with schizophrenia than that in the general population. Indeed, studies found that the prevalence of NAFLD has increased in patients with schizophrenia in the past years. A study found that only 1.5% of 6,521 patients with schizophrenia had NAFLD in 2001–2006.12 A larger sample-based observational study suggested that the prevalence of NAFLD was 22.4% among 25,503 patients with schizophrenia from 19 psychiatric hospitals between 2014 and 2018 in China.13 In Japan, a study found that 42.7% of 253 patients with schizophrenia showed NAFLD on abdominal echography from 2010 to 2020.14 A study with a smaller sample size in China reported a higher prevalence of NAFLD, which reported that the 49.5% of 202 young male patients with schizophrenia had NAFLD in 2015.15 NAFLD is also prevalent in patients with first-episode psychosis. Morlan-Coarasa et al conducted a randomized interventional study and enrolled 191 patients with first-episode non-affective psychosis from October 2005 to January 2012.16 They found that 25.1% of patients with first-episode psychosis had a fatty liver index score ≥ 60, which is associated with increased risk of developing steatosis. These studies suggested the following factors may be significantly related to NAFLD in schizophrenia: age, triglyceride (TG), BMI, medication combination, antipsychotic dosage, and negative symptom scores on the Positive and Negative Syndrome Scale.13–16
Although obesity and overweight are common in patients with schizophrenia, 6.2% of patients with schizophrenia are underweight.17 According to a recent meta-analysis, the pooled prevalence of obesity and overweight in schizophrenia patients were 25.5% and 29.8%, respectively.18 These findings suggested that nearly 40% of patients with schizophrenia had normal weight or were underweight.
However, to our knowledge, there are limited studies about NAFLD in non-obese patients with schizophrenia. Therefore, we used data from electronic records of our hospital to investigate the prevalence and risk factors of NAFLD in non-obese schizophrenia inpatients.
Methods
Design, Setting and Subjects
This retrospective study was conducted at the Affiliated Brain Hospital of Guangzhou Medical University. We reviewed the clinical records of all inpatients with schizophrenia who were discharged from psychiatric wards of the Affiliated Brain Hospital of Guangzhou Medical University during 2019. Details about all the included patients have been removed to ensure anonymity. The study included patients as follows: 1) aged 18 years or older; 2) conforming to the diagnostic criteria for schizophrenia based on the 10th revision of the International Classification of Diseases; 3) had a liver ultrasound test during hospitalization; 4) had records of BMI and laboratory tests within three days of admission to the hospital; 5) no history of alcohol abuse and other substance abuse; 6) not administered liver-protecting drugs; 7) no diseases or medicine that could cause fatty liver, such as viral hepatitis and hepatolenticular degeneration; and 8) not pregnant or breastfeeding. If a patient was admitted to the hospital more than once during the study period, only the data from the second admission were used for analysis. From January 2019 to December 2019, 1,786 schizophrenia inpatients aged 18 years or older were discharged from the psychiatric wards of our hospital. A total of 481 patients were excluded. At last, a total of 1305 adult patients with schizophrenia were included in this study. This retrospective study was proved by Institutional Review Board of the Affiliated Brain Hospital of Guangzhou Medical University. Because of the retrospective design of this study, the Institutional Review Board of the Affiliated Brain Hospital of Guangzhou Medical University exempted patient informed consent. All data analysis was performed with full patient anonymity. This study complies with the Declaration of Helsinki.
Laboratory Tests
Nurses collected blood samples between 6 and 8 am after 8–12 hours of fasting in our hospital. Laboratory tests were usually performed on the second day after admission to our hospital. All laboratory tests were performed using an automatic analyzer. The laboratory tests included alanine aminotransferase (ALT), aspartate aminotransferase (AST), total cholesterol (TC), triglyceride (TG), HDL-C and LDL-C.
Definition of NAFLD
After 8 hours of fasting, the liver ultrasound examination was conducted by a senior technician. The diagnosis of NAFLD was based on the ultrasound tests and disease history.
Definitions of Obese and Non-Obese
Obese and non-obese: Similar to our previous study in patients with schizophrenia and a study in the general population in China.17,18 Patients were grouped by BMI as follows: obesity, body mass index (BMI) ≥ 25 kg/m2; and non-obese, BMI < 25 kg/m2.
Statistical Analysis
Continuous normally distributed numerical variables are presented using the mean and standard deviation. Two-tailed Pearson χ2 test or Fisher’s exact test were used to analyze categorical variables. Student’s t-test was used to compare numerical variables. Stepwise binary logistic regression analysis was performed to examine the factors associated with NAFLD in non-obese patients. A 2-tailed p value of 0.05 was considered significant. The SPSS statistical software for Windows, version 22.0, was performed for all statistical analyses with 2-tailed p value of 0.05.
Results
Characteristics of Patients with Schizophrenia
At last, 1,305 adult patients (664 males and 641 females) with schizophrenia were included in our study. The mean age of patients was 40.88 ± 16.24 years. The mean years of education was 11.05 ± 3.24 years, ranging from 0 to 19 years. The mean duration of illness was 12.95 ± 11.85 years, ranging from 1 to 55 years. The mean inhospital stay was 54.67 ± 62.89 days, ranging from 2 to 379 days.
Comparison of the Obese Patients and Non-Obese Patients
Table 1 showed the characteristics of obese patients and non-obese patients. The distribution of BMI categories was as follows: 260 (19.9%) patients were obese, and 1,045 (80.1%) patients were non-obese. The prevalence of NAFLD in the whole study patients, obese patients and non-obese patients was 32.9%, 64.6% and 25.0%, respectively. The prevalence of NAFLD was significantly lower in the non-obese patients than in the obese patients (p < 0.001). Obese patients had higher frequency of hypertension and diabetes and longer duration of schizophrenia (p < 0.05). Significant differences were found in all the laboratory test results between the patients with obesity and the non-obese patients (p < 0.05).
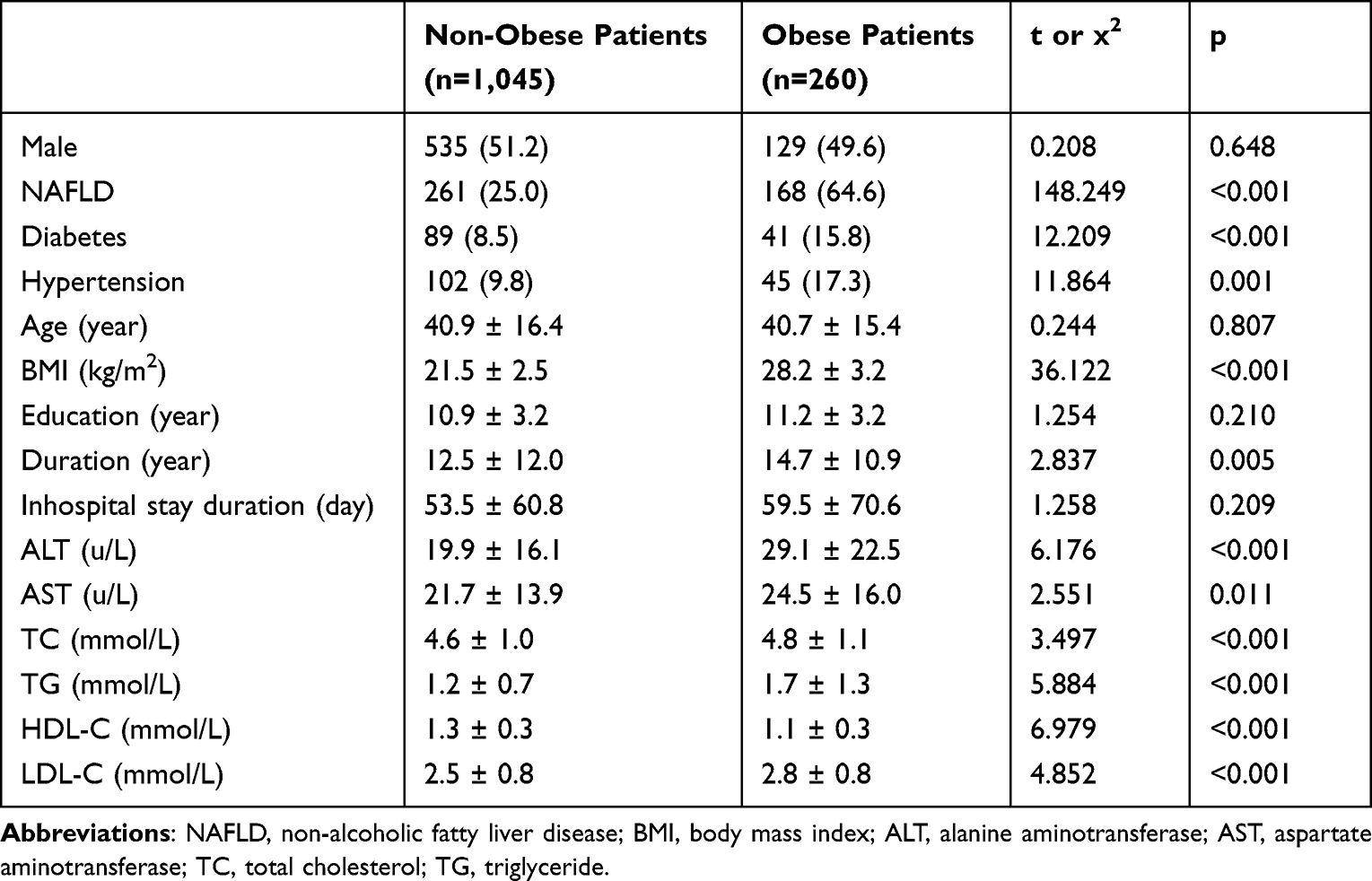 |
Table 1 Characteristics of Obese Patients and Non-Obese Patients |
Comparison of Patients with NAFLD and Patients Without NAFLD
Table 2 listed a comparison of patients with NAFLD or without NAFLD in the non-obese patients. Among the non-obese patients with schizophrenia, patients with NAFLD were older, had a higher prevalence of diabetes, had a higher prevalence of hypertension, had a higher BMI, had lower level of HDL-C, had a longer of duration, had higher level of ALT, AST, TC, TG and LDL-C than patients without NAFLD (p < 0.05).
 |
Table 2 Characteristics of Patients with NAFLD and Patients Without NAFLD in Non-Obese Patients |
Influencing Factors for NAFLD in Non-Obese Patients
Stepwise binary logistic regression analysis was performed to assess the risk factors for NAFLD among these non-obese patients with schizophrenia. As shown in Table 3, age, BMI, ALT, TG and diabetes were significantly associated with NAFLD. In contrast, HDL-C was negatively associated with NAFLD.
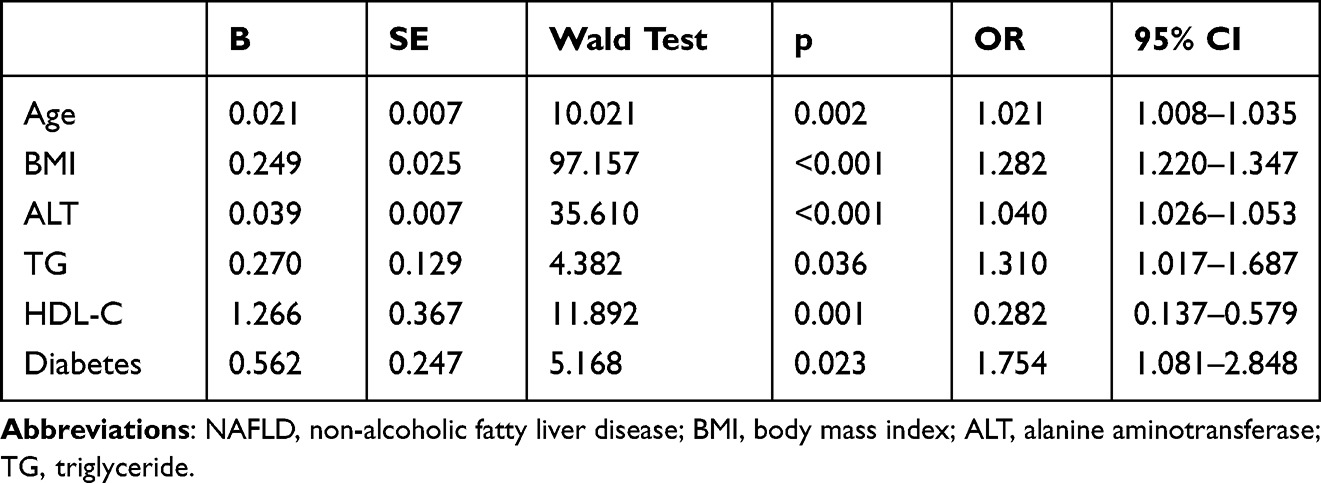 |
Table 3 Associated Factors with NAFLD in Non-Obese Patients |
Discussion
NAFLD is a public health burden, especially in China. We assessed the prevalence and risk factors of NAFLD among non-obese patients with schizophrenia in our hospital. To our knowledge, this is the first study assessing NAFLD among non-obese patients with schizophrenia in a large public hospital in China. This study suggested that the prevalence of NAFLD in all the patients, obese patients and non-obese patients was 32.9%, 64.6% and 25.0%, respectively. In the non-obese patients, those with NAFLD were older, had a higher BMI, had a higher prevalence of diabetes, had a higher prevalence of hypertension, had lower level of HDL-C, had higher level of ALT, AST, TC, TG and LDL-C than patients without NAFLD. Furthermore, age, BMI, ALT, TG and diabetes were significantly associated with NAFLD in those non-obese patients. In contrast, HDL-C was negatively associated with NAFLD in non-obese patients.
We found that the prevalence of NAFLD in all the patients with schizophrenia was 32.9%, which was higher than the prevalence of 22.4% that was observed among 25,503 inpatients with schizophrenia in a Chinese sample.13 Our study differs from that study in that we examined all the results of liver ultrasound test, and the diagnosis of NAFLD could not be ignored in this study. While the diagnosis of NAFLD was obtained from electronic health records in that study, NAFLD may be underestimated in that study. Another possible reason may be the difference in the study years between our studies. We included patients who were discharged from our hospital in 2019, and that study included patients who were admitted to 19 specialized psychiatric hospitals from 2014 to 2018, and the prevalence of NAFLD has increased over time in China. A meta-analysis reported that the prevalence of NAFLD ranged between 14.32% and 23.36% from 2000 to 2013 in Chinese general population.19 According to a recent meta-analysis, the overall prevalence of NAFLD increased to approximately 30.0% in China.20 In contrast, the prevalence of NAFLD seemed to be higher in our study than that found in Chinese general population.20 Schizophrenia patients have a higher risk of developing obesity and metabolic syndrome than healthy controls, and obesity and metabolic syndrome have been found to be closely associated with NAFLD. In addition to common influencing factors for NAFLD in the general population, such as age, obesity, dyslipidemia and metabolic syndrome, patients with schizophrenia may have unique risk factors for NAFLD, including antipsychotics use and schizophrenia symptoms.15 A study found that clozapine worsened NAFLD in mice.21 This may be due to decreased adiponectin protein levels and elevated FASN protein levels. Another study in mice reported that long-term use of risperidone may be associated with exacerbated diabetes syndrome and NAFLD.22
A meta-analysis showed that the overall prevalence and incidence of NAFLD among the non-obese general individuals were 18.3% and 24.6 per 1,000 person-years, respectively.6 A study included 1,812 biopsy-confirmed NAFLD patients from 9 countries in Asia found that more than 21.6% of patients with NAFLD were non-obese.23 Moreover, 50.5% of non-obese patients with NAFLD may develop non-alcoholic steatohepatitis (NASH) or advanced fibrosis.23 Studies have found that despite the absence of obesity, non-obese NAFLD subjects had a higher risk of death.24 Furthermore, patients with NAFLD have been found to be independently associated with an increased risk for diabetes in non-obese subjects.25 We found that NAFLD was common in non-obese patients with schizophrenia. And compared to the reported NALFD prevalence in the general population.6,26 Non-obese patients with schizophrenia had a higher prevalence of NAFLD. According to a meta-analysis, more than half of patients with schizophrenia could be defined as non-obese.18 Our findings suggested that NAFLD should be assessed and screened in adult patients with schizophrenia, even in non-obese patients.
We found that obese patients with schizophrenia had a significantly higher prevalence of NAFLD than non-obese patients, which was consistent with studies in the general population.6 Obesity is strongly associated with NAFLD.5 A meta-analysis showed that among NAFLD patients, obesity may not be independently associated with the development of NASH or advanced fibrosis, but obesity may be related to a worse long-term prognosis.27 A study with 310 patients with biopsy-confirmed NAFLD found that higher BMI was a major risk factor for NAFLD/NASH in non-obese and lean individuals.28 Notably, 5% body weight loss has been reported to lead to similar NAFLD remission in both obese and lean subjects.29
Studies found that BMI is associated with risk of NAFLD in both schizophrenia patients and the general population.15 In obese children and adolescents, BMI was associated with severe liver fibrosis.11 We found that BMI was also associated with NAFLD in non-obese patients with schizophrenia, which is agreeing with studies conducted in the non-obese general population.30,31 A Japanese study with 3,271 subjects suggested that ≥10 kg of weight gain since the age of 20 years old was significantly related to the risk of NAFLD in non-obese individuals of both sexes.32 Our findings suggest that schizophrenia patients with a normal BMI also should avoid weight gain to decrease the risk for NAFLD. Moreover, a study found that plasma apelin levels were significantly higher in patients with schizophrenia than healthy controls.33 Apelin could be involved in pathological processes, such as obesity, diabetes, heart failure, and cancer.34 Higher apelin levels may be associated with obesity and NAFLD in patients with schizophrenia.
ALT is closely associated with NAFLD. A study in Japan found that ALT was most strongly associated with fibro Scan-aspartate aminotransferase scores, which could be used to stratify NAFLD severity.35 In China, a large population-based longitudinal study suggested that an elevated ALT/AST ratio was closely associated with the risk of new-onset NAFLD.36 A study found that the level of ALT was associated with interventricular septum thickness in subjects with NAFLD.37 That study also showed that ALT can be used as an alternative marker for left ventricular hypertrophy in overweight and/or obese subjects with NAFLD. A study reported that in patients with schizophrenia, patients without NAFLD had much lower levels of ALT than patients with NAFLD, but ALT was not associated with NAFLD after adjusting BMI, fasting blood glucose, TC, TG and other factors.15 However, two studies suggested that ALT was closely related to metabolic syndrome in patients with schizophrenia.12,38 Increased ALT within the normal range and metabolic syndrome were correlated in patients with schizophrenia with clozapine.12 Antipsychotics, especially olanzapine and the combination of olanzapine and divalproex, may increase the level of ALT.39–41 In our study, elevated levels of ALT were significantly related to NAFLD in non-obese patients with schizophrenia. The associations between serum ALT and liver fat accumulation and between ALT-associated hepatic insulin resistance may account for the relationship between ALT and NAFLD.42 A study revealed that the severity of the metabolic profile and the prevalence of advanced fibrosis were associated with ALT in patients with biopsy-confirmed NAFLD.43 It is noted that patients could develop NASH, even if the patients had persistent normal ALT.44
In the non-obese general population, lipid metabolism has been found to be closely associated with NAFLD. In Japan, a study with 3,271 individuals showed that triglycerides were significantly independently associated with NAFLD in non-obese patients.32 In China, a population-based cross-sectional study suggested that TG was significantly independently associated with increased risk for NAFLD in non-obese individuals.30 Moreover, a study with patients with biopsy-confirmed NAFLD found that cholesterol was an important biomarker of advanced liver disease in non-obese patients.23 A 5-year longitudinal cohort study in China suggested that LDL/HDL ratio was associated the risk of developing new-onset NAFLD in Chinese non-obese individuals with normal lipid levels.45 The present study showed that TG was associated with increased prevalence of NAFLD, and HDL-L was negatively associated with NAFLD in non-obese adult inpatients with schizophrenia, which is similar to these studies in a non-obese general population. Fortunately, in the general population, studies have suggested that improving blood lipid metabolism and statin treatment may decrease the risk of NAFLD.46,47
Increased evidence suggests that NAFLD and diabetes are directly bidirectional.48 Diabetes may accelerate liver disease progression in subjects with NAFLD, while NAFLD could increase the risk of diabetes complications.48 Liver plays an important role in the pathophysiology of diabetes and NAFLD, and it results in the development of insulin resistance, which is involved the mechanisms of NAFLD and diabetes. We found that among non-obese inpatients with schizophrenia, patients without NAFLD had a lower prevalence of diabetes than patients with NAFLD, and diabetes was associated with NAFLD. A recent systematic review and meta-analysis published in 2019 suggested that the estimated global frequency of NAFLD in patients with diabetes reached up to 55.5%, and diabetes is one of the most important risk factors for NAFLD.48 Notably, schizophrenia patients have a 2- to 5-fold higher risk of developing diabetes than healthy controls because of antipsychotics use, poor diet, and sedentary lifestyle.49 Further studies should be conducted to assess the risk of NAFLD in schizophrenia patients with diabetes.
Dispute remains over whether gender contributes to the risk of NAFLD. For instance, a meta-analysis suggested that there was no gender difference in the prevalence of NAFLD in the general population.1 A meta-analysis of 48 studies with 356,367 subjects revealed that males had a significant higher prevalence of NAFLD than females in China.19 That meta-analysis found that 24.81% of male individuals and 13.16% of female individuals had NAFLD, with almost 2 times the prevalence of NAFLD in male individuals compared with female individuals. Moreover, Ma et al suggested that male gender was one of important risk factors for NAFLD among mental disorder patients in China.13 In contrast, a meta-analysis comprising 93 studies with 10,576,383 subjects found that among non-obese subjects, female subjects had a higher prevalence of NAFLD, but there was no significant gender difference in the prevalence of NAFLD.6 Recently, a large prospective cohort study with 3,659 non-obese adults in China suggested that there was no gender difference in the prevalence of NAFLD at baseline and at the end of the follow-up.50 We found that there was no gender difference in the prevalence of NAFLD among all the inpatients with schizophrenia and the non-obese inpatients with schizophrenia. Possible reasons for the inconsistent results regarding NAFLD prevalence in males and females include differences in study design, enrolled subjects, sample size, definition of obesity and non-obesity, races, regions, and hormonal regulation.
There were several limitations in this study. First, as a retrospective study, this study could not determine whether there is a causal relationship between the associated factors and NAFLD in non-obese patients with schizophrenia. Second, only inpatients with schizophrenia from a hospital were included. Outpatients, patients in general hospitals, and patients living in communities were not enrolled. Third, other important factors associated with NAFLD, such as diet, physical activity, antipsychotics use, smoking, family history of NAFLD and genetic factors were not investigated in this study. Fourth, this study did not enroll healthy controls with matched age and gender. Thus, there may be some possible bias when comparing our findings with the general population of other studies.
In conclusion, the findings suggests NAFLD is prevalent in Chinese patients with schizophrenia, even in those non-obese patients with schizophrenia. In non-obese patients with schizophrenia, age, BMI, ALT, TG and diabetes are significantly associated with NAFLD. In contrast, HDL-C was a protective factor against NAFLD in those non-obese patients. NAFLD results in increased unfavorable outcome. Given the adverse outcomes of NAFLD, it is necessary to increase awareness of NAFLD in patients with schizophrenia, especially in non-obese patients with schizophrenia.
Funding
This study is supported by the Planed Science and Technology Projects of Guangzhou (202201011338), Guangzhou Municipal Key Discipline in Medicine (2021-2023), Guangzhou Research-oriented Hospital, Guangzhou High-level Clinical Key Specialty, Guangzhou Research-oriented Hospital, and the Planed Science and Technology Projects of Guangzhou (2023A03J0836).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Le MH, Yeo YH, Li X, et al. 2019 global NAFLD prevalence: a systematic review and meta-analysis. Clin Gastroenterol Hepatol. 2022;20(12):2809–2817.e28. doi:10.1016/j.cgh.2021.12.002
2. Zhou F, Zhou J, Wang W, et al. Unexpected rapid increase in the burden of NAFLD in China from 2008 to 2018: a systematic review and meta-analysis. Hepatology. 2019;70(4):1119–1133. doi:10.1002/hep.30702
3. Liu Y, Zhong GC, Tan HY, Hao FB, Hu JJ. Nonalcoholic fatty liver disease and mortality from all causes, cardiovascular disease, and cancer: a meta-analysis. Sci Rep. 2019;9(1):11124. doi:10.1038/s41598-019-47687-3
4. Chen H, Zhan Y, Zhang J, et al. The global, regional, and national burden and trends of NAFLD in 204 countries and territories: an analysis from global burden of disease 2019. JMIR Public Health Surveill. 2022;8(12):e34809. doi:10.2196/34809
5. Li L, Liu DW, Yan HY, Wang ZY, Zhao SH, Wang B. Obesity is an independent risk factor for non-alcoholic fatty liver disease: evidence from a meta-analysis of 21 cohort studies. Obes Rev. 2016;17(6):510–519. doi:10.1111/obr.12407
6. Ye Q, Zou B, Yeo YH, et al. Global prevalence, incidence, and outcomes of non-obese or lean non-alcoholic fatty liver disease: a systematic review and meta-analysis. Lancet Gastroenterol Hepatol. 2020;5(8):739–752. doi:10.1016/S2468-1253(20)30077-7
7. Correll CU, Solmi M, Croatto G, et al. Mortality in people with schizophrenia: a systematic review and meta-analysis of relative risk and aggravating or attenuating factors. World Psychiatry. 2022;21(2):248–271. doi:10.1002/wps.20994
8. Mitchell AJ, Vancampfort D, De Herdt A, Yu W, De Hert M. Is the prevalence of metabolic syndrome and metabolic abnormalities increased in early schizophrenia? A comparative meta-analysis of first episode, untreated and treated patients. Schizophr Bull. 2013;39(2):295–305. doi:10.1093/schbul/sbs082
9. Sahpolat M, Ari M. Higher prevalence of metabolic syndrome and related factors in patients with first-episode psychosis and schizophrenia: a cross-sectional study inTurkey. Nord J Psychiatry. 2021;75(1):73–78. doi:10.1080/08039488.2020.1815080
10. Sugawara N, Yasui-Furukori N, Yamazaki M, et al. Attitudes toward metabolic adverse events among patients with schizophrenia in Japan. Neuropsychiatr Dis Treat. 2016;12:427–436. doi:10.2147/NDT.S98711
11. Moran-Lev H, Cohen S, Webb M, et al. Higher BMI predicts liver fibrosis among obese children and adolescents with NAFLD - an interventional pilot study. BMC Pediatr. 2021;21(1):385. doi:10.1186/s12887-021-02839-1
12. Lee NY, Roh MS, Kim SH, et al. The prevalence of metabolic syndrome and its association with alanine aminotransferase in clozapine-treated Korean patients with schizophrenia. Int Clin Psychopharmacol. 2013;28(2):71–79. doi:10.1097/YIC.0b013e32835b99bd
13. Ma Q, Yang F, Ma B, et al. Prevalence of nonalcoholic fatty liver disease in mental disorder inpatients in China: an observational study. Hepatol Int. 2021;15(1):127–136. doi:10.1007/s12072-020-10132-z
14. Koreki A, Mori H, Nozaki S, Koizumi T, Suzuki H, Onaya M. Risk of nonalcoholic fatty liver disease in patients with schizophrenia treated with antipsychotic drugs: a cross-sectional study. J Clin Psychopharmacol. 2021;41(4):474–477. doi:10.1097/JCP.0000000000001421
15. Yan J, Hou C, Liang Y. The prevalence and risk factors of young male schizophrenics with non-alcoholic fatty liver disease. Neuropsychiatr Dis Treat. 2017;13:1493–1498. doi:10.2147/NDT.S137183
16. Morlan-Coarasa MJ, Arias-Loste MT, Ortiz-Garcia de la Foz V, et al. Incidence of non-alcoholic fatty liver disease and metabolic dysfunction in first episode schizophrenia and related psychotic disorders: a 3-year prospective randomized interventional study. Psychopharmacology. 2016;233(23–24):3947–3952. doi:10.1007/s00213-016-4422-7
17. Sugawara N, Maruo K, Sugai T, et al. Prevalence of underweight in patients with schizophrenia: a meta-analysis. Schizophr Res. 2018;195:67–73. doi:10.1016/j.schres.2017.10.017
18. Afzal M, Siddiqi N, Ahmad B, et al. Prevalence of overweight and obesity in people with severe mental illness: systematic review and meta-analysis. Front Endocrinol. 2021;12:769309. doi:10.3389/fendo.2021.769309
19. Li Z, Xue J, Chen P, Chen L, Yan S, Liu L. Prevalence of nonalcoholic fatty liver disease in mainland of China: a meta-analysis of published studies. J Gastroenterol Hepatol. 2014;29(1):42–51. doi:10.1111/jgh.12428
20. Wu Y, Zheng Q, Zou B, et al. The epidemiology of NAFLD in Mainland China with analysis by adjusted gross regional domestic product: a meta-analysis. Hepatol Int. 2020;14(2):259–269. doi:10.1007/s12072-020-10023-3
21. Chang GR, Liu HY, Yang WC, et al. Clozapine worsens glucose intolerance, nonalcoholic fatty liver disease, kidney damage, and retinal injury and increases renal reactive oxygen species production and chromium loss in obese mice. Int J Mol Sci. 2021;22(13):6680.
22. Tsai HP, Hou PH, Mao FC, et al. Risperidone exacerbates glucose intolerance, nonalcoholic fatty liver disease, and renal impairment in obese mice. Int J Mol Sci. 2021;22(1):409.
23. Tan EX, Lee JW, Jumat NH, et al. Non-obese non-alcoholic fatty liver disease (NAFLD) in Asia: an international registry study. Metabolism. 2022;126:154911. doi:10.1016/j.metabol.2021.154911
24. Oladunjoye O, Oladunjoye AO, Dhital R, et al. A retrospective study of hospitalizations in the USA: proportion of hospitalizations with non-alcoholic fatty liver disease in non-obese population. Cureus. 2021;13(9):e17869. doi:10.7759/cureus.17869
25. Dai W, Zhang Z, Zhao S. The risk of type 2 diabetes and coronary artery disease in non-obese patients with non-alcoholic fatty liver disease: a cohort study. Front Cardiovasc Med. 2021;8:680664. doi:10.3389/fcvm.2021.680664
26. Zou ZY, Wong VW, Fan JG. Epidemiology of nonalcoholic fatty liver disease in non-obese populations: meta-analytic assessment of its prevalence, genetic, metabolic, and histological profiles. J Dig Dis. 2020;21(7):372–384. doi:10.1111/1751-2980.12871
27. Lu FB, Hu ED, Xu LM, et al. The relationship between obesity and the severity of non-alcoholic fatty liver disease: systematic review and meta-analysis. Expert Rev Gastroenterol Hepatol. 2018;12(5):491–502. doi:10.1080/17474124.2018.1460202
28. Eshraghian A, Nikeghbalian S, Geramizadeh B, Kazemi K, Shamsaeefar A, Malek-Hosseini SA. Characterization of biopsy proven non-alcoholic fatty liver disease in healthy non-obese and lean population of living liver donors: the impact of uric acid. Clin Res Hepatol Gastroenterol. 2020;44(4):572–578. doi:10.1016/j.clinre.2019.09.002
29. Hamurcu Varol P, Kaya E, Alphan E, Yilmaz Y. Role of intensive dietary and lifestyle interventions in the treatment of lean nonalcoholic fatty liver disease patients. Eur J Gastroenterol Hepatol. 2020;32(10):1352–1357. doi:10.1097/MEG.0000000000001656
30. Li Y, Chen Y, Tian X, Zhang S, Jiao J. Comparison of clinical characteristics between obese and non-obese patients with Nonalcoholic Fatty Liver Disease (NAFLD). Diabetes Metab Syndr Obes. 2021;14:2029–2039. doi:10.2147/DMSO.S304634
31. Oral A, Sahin T, Turker F, Kocak E. Relationship between serum uric acid levels and nonalcoholic fatty liver disease in non-obese patients. Medicina. 2019;55(9):600.
32. Nishioji K, Sumida Y, Kamaguchi M, et al. Prevalence of and risk factors for non-alcoholic fatty liver disease in a non-obese Japanese population, 2011–2012. J Gastroenterol. 2015;50(1):95–108. doi:10.1007/s00535-014-0948-9
33. Sahpolat M, Ari M, Kokacya MH. Plasma apelin, visfatin and resistin levels in patients with first episode psychosis and chronic schizophrenia. Clin Psychopharmacol Neurosci. 2020;18(1):109–115. doi:10.9758/cpn.2020.18.1.109
34. Wysocka MB, Pietraszek-Gremplewicz K, Nowak D. The role of apelin in cardiovascular diseases, obesity and cancer. Front Physiol. 2018;9:557. doi:10.3389/fphys.2018.00557
35. Fujii H, Fukumoto S, Enomoto M, et al. The FibroScan-aspartate aminotransferase score can stratify the disease severity in a Japanese cohort with fatty liver diseases. Sci Rep. 2021;11(1):13844. doi:10.1038/s41598-021-93435-x
36. Zou Y, Zhong L, Hu C, Sheng G. Association between the alanine aminotransferase/aspartate aminotransferase ratio and new-onset non-alcoholic fatty liver disease in a nonobese Chinese population: a population-based longitudinal study. Lipids Health Dis. 2020;19(1):245. doi:10.1186/s12944-020-01419-z
37. Ybarra J, Fernandez S, Sanchez-Hernandez J, et al. Serum alanine aminotransferase predicts interventricular septum thickness and left ventricular mass in patients with nonalcoholic fatty liver disease. Eur J Gastroenterol Hepatol. 2014;26(6):654–660. doi:10.1097/MEG.0000000000000086
38. Kim EY, Kim SH, Lee NY, et al. Aminotransferase levels as a prospective predictor for the development of metabolic syndrome in patients with schizophrenia. Psychopharmacology. 2014;231(23):4479–4487. doi:10.1007/s00213-014-3601-7
39. Pae CU, Lim HK, Kim TS, et al. Naturalistic observation on the hepatic enzyme changes in patients treated with either risperidone or olanzapine alone. Int Clin Psychopharmacol. 2005;20(3):173–176. doi:10.1097/00004850-200505000-00009
40. Gonzalez-Heydrich J, Raches D, Wilens TE, Leichtner A, Mezzacappa E. Retrospective study of hepatic enzyme elevations in children treated with olanzapine, divalproex, and their combination. J Am Acad Child Adolesc Psychiatry. 2003;42(10):1227–1233. doi:10.1097/00004583-200310000-00014
41. Gaertner I, Altendorf K, Batra A, Gaertner HJ. Relevance of liver enzyme elevations with four different neuroleptics: a retrospective review of 7263 treatment courses. J Clin Psychopharmacol. 2001;21(2):215–222. doi:10.1097/00004714-200104000-00014
42. Oh HJ, Kim TH, Sohn YW, et al. Association of serum alanine aminotransferase and gamma-glutamyltransferase levels within the reference range with metabolic syndrome and nonalcoholic fatty liver disease. Korean J Hepatol. 2011;17(1):27–36. doi:10.3350/kjhep.2011.17.1.27
43. Ulasoglu C, Enc FY, Kaya E, Yilmaz Y. Characterization of patients with biopsy-proven non-alcoholic fatty liver disease and normal aminotransferase levels. J Gastrointestin Liver Dis. 2019;28(4):427–431. doi:10.15403/jgld-293
44. Zheng KI, Liu WY, Pan XY, et al. Combined and sequential non-invasive approach to diagnosing non-alcoholic steatohepatitis in patients with non-alcoholic fatty liver disease and persistently normal alanine aminotransferase levels. BMJ Open Diabetes Res Care. 2020;8(1):e001174.
45. Zou Y, Zhong L, Hu C, Zhong M, Peng N, Sheng G. LDL/HDL cholesterol ratio is associated with new-onset NAFLD in Chinese non-obese people with normal lipids: a 5-year longitudinal cohort study. Lipids Health Dis. 2021;20(1):28. doi:10.1186/s12944-021-01457-1
46. van den Berg EH, Wolters AAB, Dullaart RPF, et al. Prescription of statins in suspected non-alcoholic fatty liver disease and high cardiovascular risk, a population-based study. Liver Int. 2019;39(7):1343–1354. doi:10.1111/liv.14116
47. Lee JI, Lee HW, Lee KS, Lee HS, Park JY. Effects of statin use on the development and progression of nonalcoholic fatty liver disease: a nationwide nested case-control study. Am J Gastroenterol. 2021;116(1):116–124. doi:10.14309/ajg.0000000000000845
48. Younossi ZM, Golabi P, de Avila L, et al. The global epidemiology of NAFLD and NASH in patients with type 2 diabetes: a systematic review and meta-analysis. J Hepatol. 2019;71(4):793–801. doi:10.1016/j.jhep.2019.06.021
49. Suvisaari J, Keinanen J, Eskelinen S, Mantere O. Diabetes and Schizophrenia. Curr Diab Rep. 2016;16(2):16. doi:10.1007/s11892-015-0704-4
50. Ji L, Cai X, Bai Y, Li T. Application of a novel prediction model for predicting 2-year risk of non-alcoholic fatty liver disease in the non-obese population with normal blood lipid levels: a large prospective cohort study from China. Int J Gen Med. 2021;14:2909–2922. doi:10.2147/IJGM.S319759
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.