")
Back to Journals » Journal of Pain Research » Volume 15
Prevalence and Predictors of Chronic Pain with Two-Year Follow-Up After Knee Arthroplasty
Authors Tian M, Li Z, Chen X, Wu Q, Shi H, Zhu Y, Shi Y
Received 1 November 2021
Accepted for publication 15 March 2022
Published 15 April 2022 Volume 2022:15 Pages 1091—1105
DOI https://doi.org/10.2147/JPR.S345496
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Houman Danesh
Meimei Tian,1,2,* Zihua Li,1,* Xujuan Chen,1 Qiting Wu,1 Huimin Shi,1 Yuchang Zhu,1 Yan Shi2
1Department of Orthopedics, Shanghai Tenth People’s Hospital, School of Medicine, Tongji University, Shanghai, 200072, People’s Republic of China; 2Department of Nursing, Shanghai Tenth People’s Hospital, School of Medicine, Tongji University, Shanghai, 200072, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Yan Shi, Tel +86 21 66307304, Fax +86 21 66307542, Email [email protected]
Background: Pain relief is the most important issue in the long-term outcome of arthroplasty surgery, with nearly one-third of patients still suffered persistent pain and caused dissatisfaction after the surgery.
Methods: A total of 713 patients underwent primary elective primary TKA and UKA were included consecutively between July 2018 and December 2019, using binary logistic method to analyze the data.
Results: The prevalence of CPSP at rest and on movement at 2-year was 12.1% and 37.7% respectively after primary knee arthroplasty and CPSP at rest factors included: age above 80 (odds ratio [OR]= 6.72, 95% confidence interval [CI] 1.58 to 28.56), BMI above 30 (2.339, 1.02 to 5.383), and moderate to severe pain variables: preoperative pain, (1.95, 1.11 to 3.41); APSP on movement, 4.9 (2.31– 10.6); and follow-up contralateral knee pain-at-rest scores (12.6, 5.5 to 28.5). Factors associated with presence of CPSP on movement included: no smoking (2.59, 1.07 to 6.26); and moderate to severe pain variables: preoperative pain, (1.57, 1.073 to 2.30); APSP at rest, (1.85, 1.13 to 3.02); APSP on movement, 6.11 (3.82 to 9.78); and follow-up contralateral knee pain-on-movement scores, 3.22 (2.08 to 5.00). Factors to occurrence of moderate to severe CPSP on movement include: presence of COPD (12.20, 2.19 to 67.98); and moderate to severe pain variables: preoperative pain (2.36, 1.32 to 4.23); APSP on movement (4.68, 1.95 to 11.25); and follow-up contralateral knee pain-on-movement scores (2.71, 1.66 to 4.42).
Conclusion: Prevention strategies should be targeted to different types of pain, and the comorbidity of COPD undergoing knee arthroplasty should receive early identification and attention.
Keywords: chronic postsurgical pain, acute-postoperative pain, total knee arthroplasty, rest pain, movement pain
Introduction
Total knee arthroplasty (TKA) can effectively improve the function of knee and patients’ quality of life, with improvement rate reported 85% and 90% respectively.1 Reduce pain caused by knee joint degeneration is the main appeal of patients undergoing TKA surgery. Many patients state that pain can be relieved within 6 to 12 weeks (3 months) after TKA, however, there is still 8–70% chronic pain occurs after surgery,2–4 some of which need to use analgesics after surgery on a long-term basis.3,5,6 Chronic postsurgical pain (CPSP) is defined by the International Association for the Study of Pain as a persistent pain at least 2 months after the intervention, meanwhile other causes for the pain have been excluded.6,7 Chronic pain after TKA is the main predictor of dissatisfaction after TKA,2 and it is estimated that the annual volume of primary TKA procedures in the US would increase by 401%, from 680,150 in 2014 to 3416,000 by 20408 and the annual expenditure on chronic pain in the United States is up to $560 billion to $635 billion.9 Although the issue of CPSP after TKA has been extensively reported in the literatures, the predictive effects of these independent variables on CPSP have not been studied systematically. Meanwhile, the association of acute-postoperative pain (APSP) with CPSP has also been widely discussed, but the effect observed in studies is inconsistent.10 Risk factors that have been reported to be associated with CPSP following TKA2,10 include: preoperative pain, preoperative joint function, socio-economic factors, surgical technical factors, acute postoperative pain (within 1–8 days after surgery), postoperative functional level, medical comorbidity, psychological factors (preoperative or postoperative anxiety, depression, pain catastrophizing), as well as demographic factors (gender, age, race, obesity).
 |
Table 1 Inclusion and Exclusion Criteria |
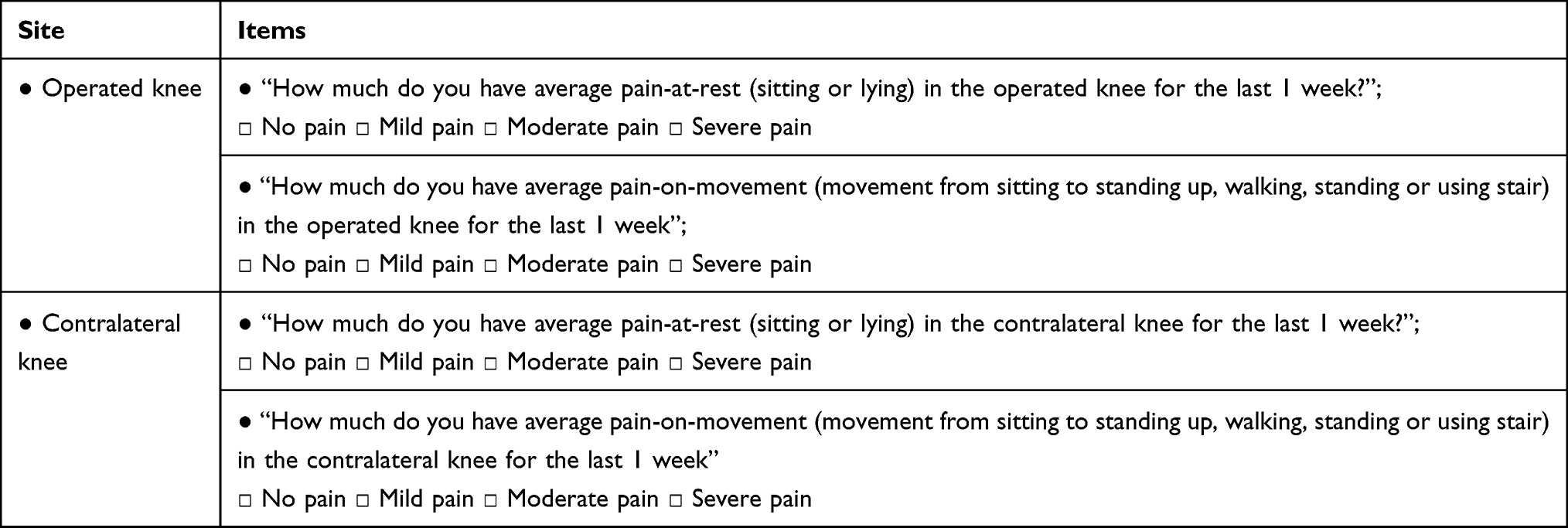 |
Table 2 Follow-Up Questions on Chronic Pain |
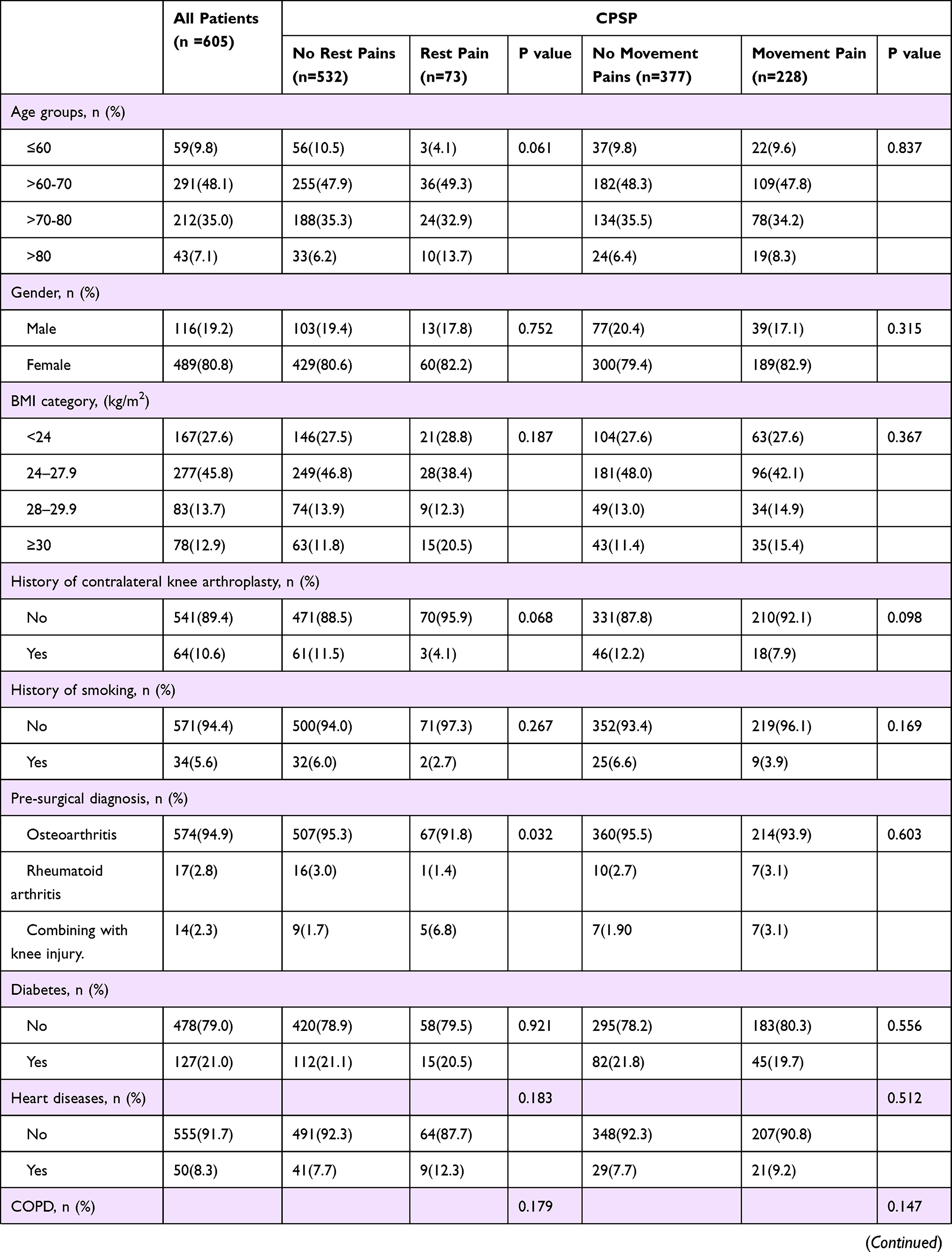 | 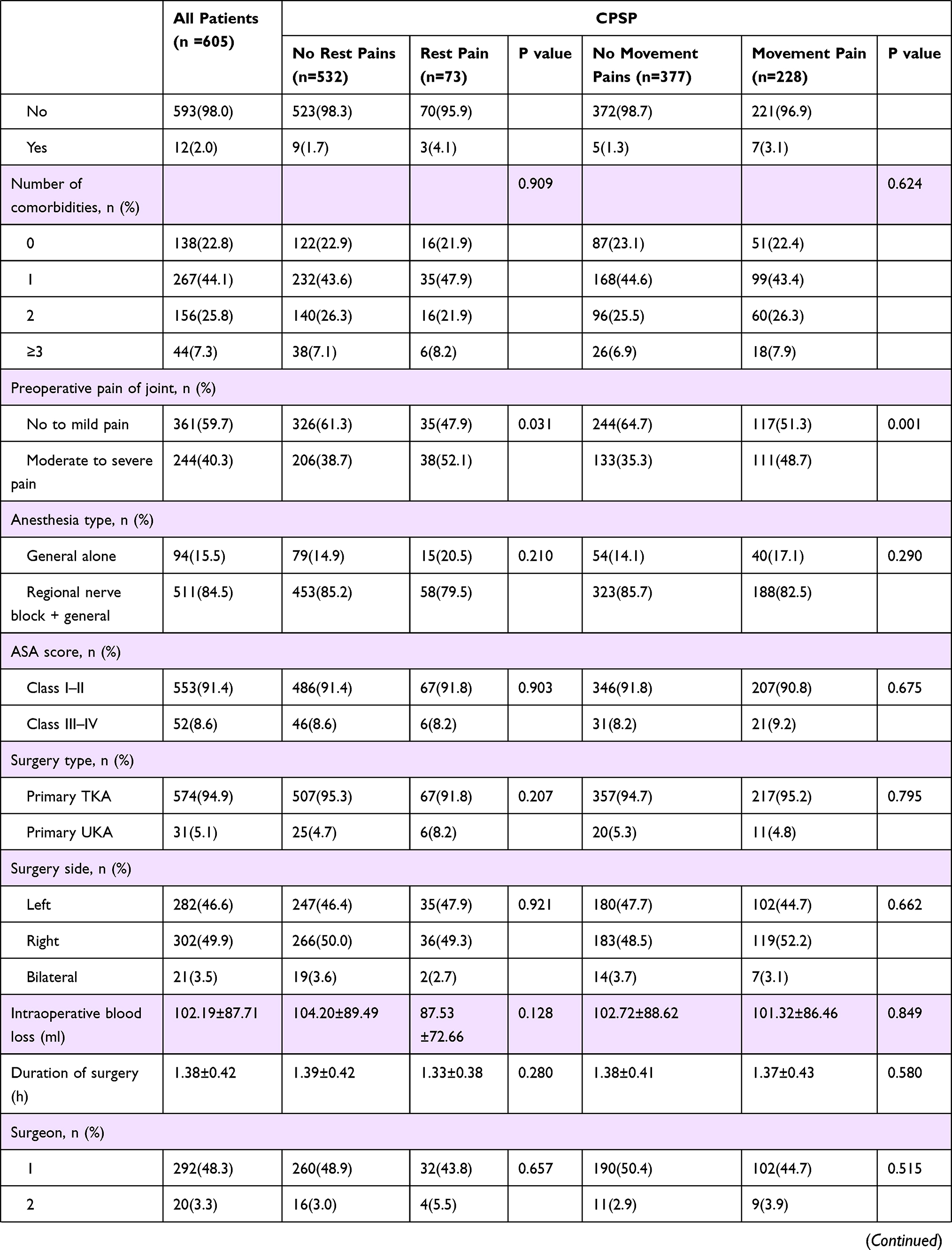 | 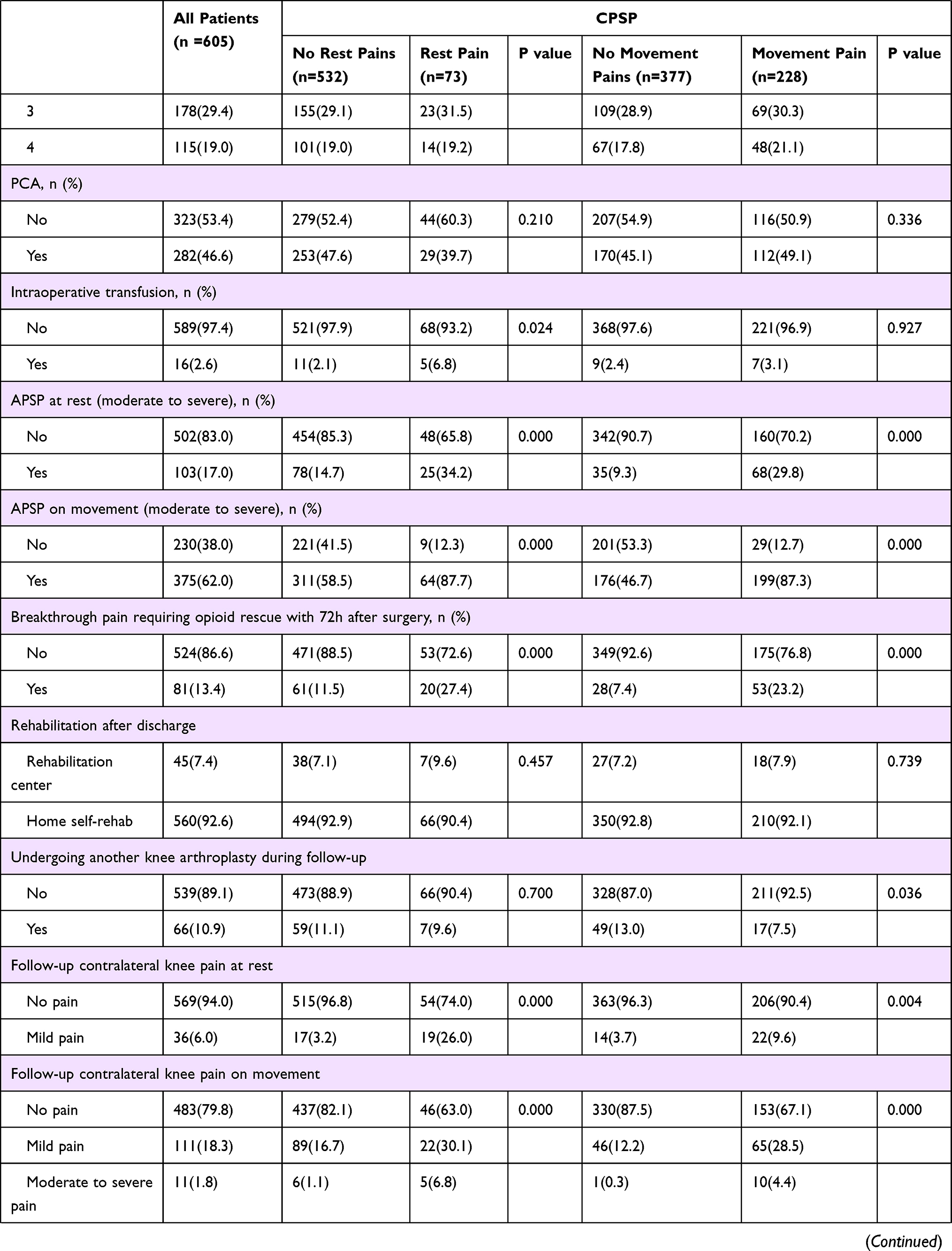 | 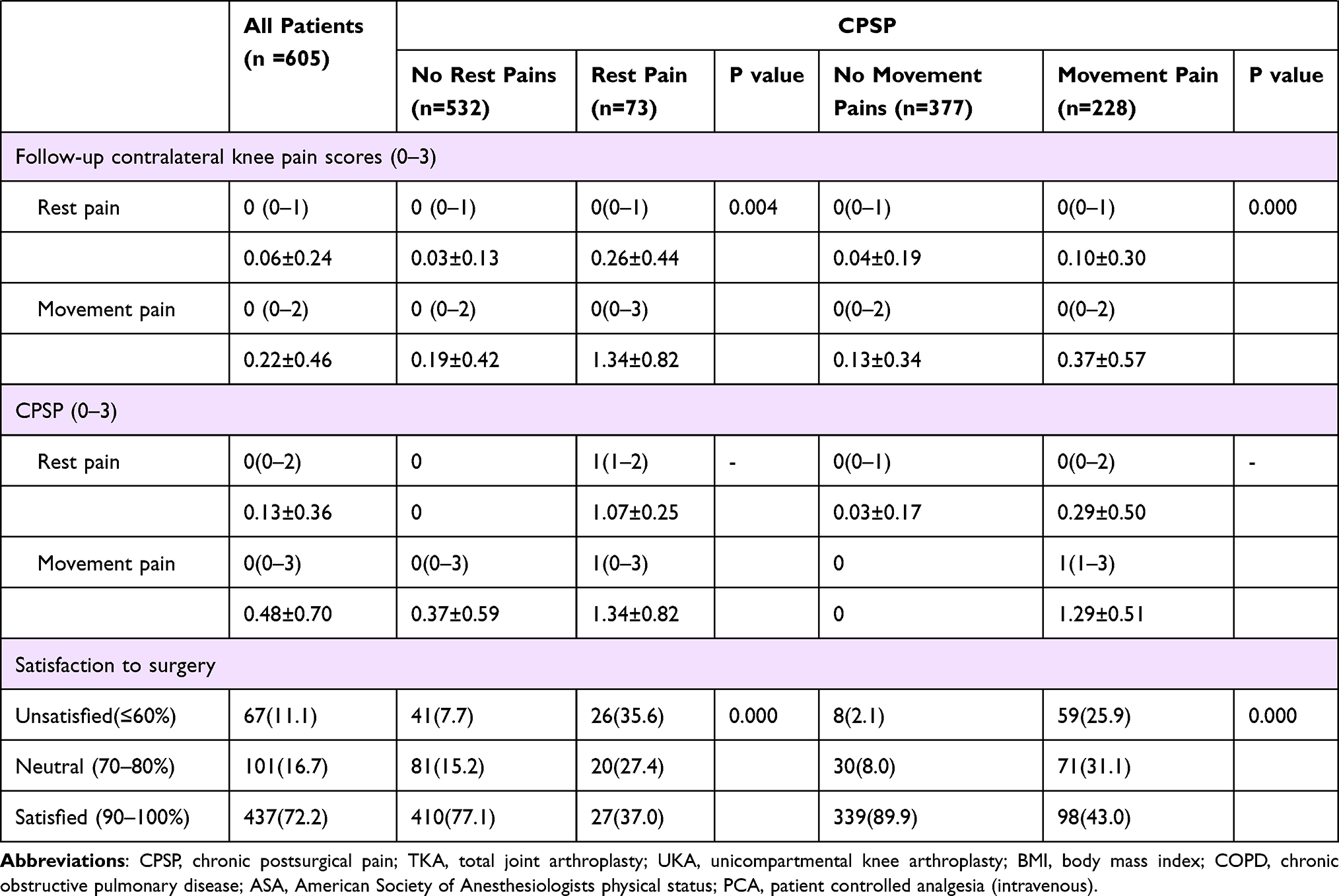
Table 3 Univariable (Unadjusted) Analysis of Independent Variable with and without CPSP |
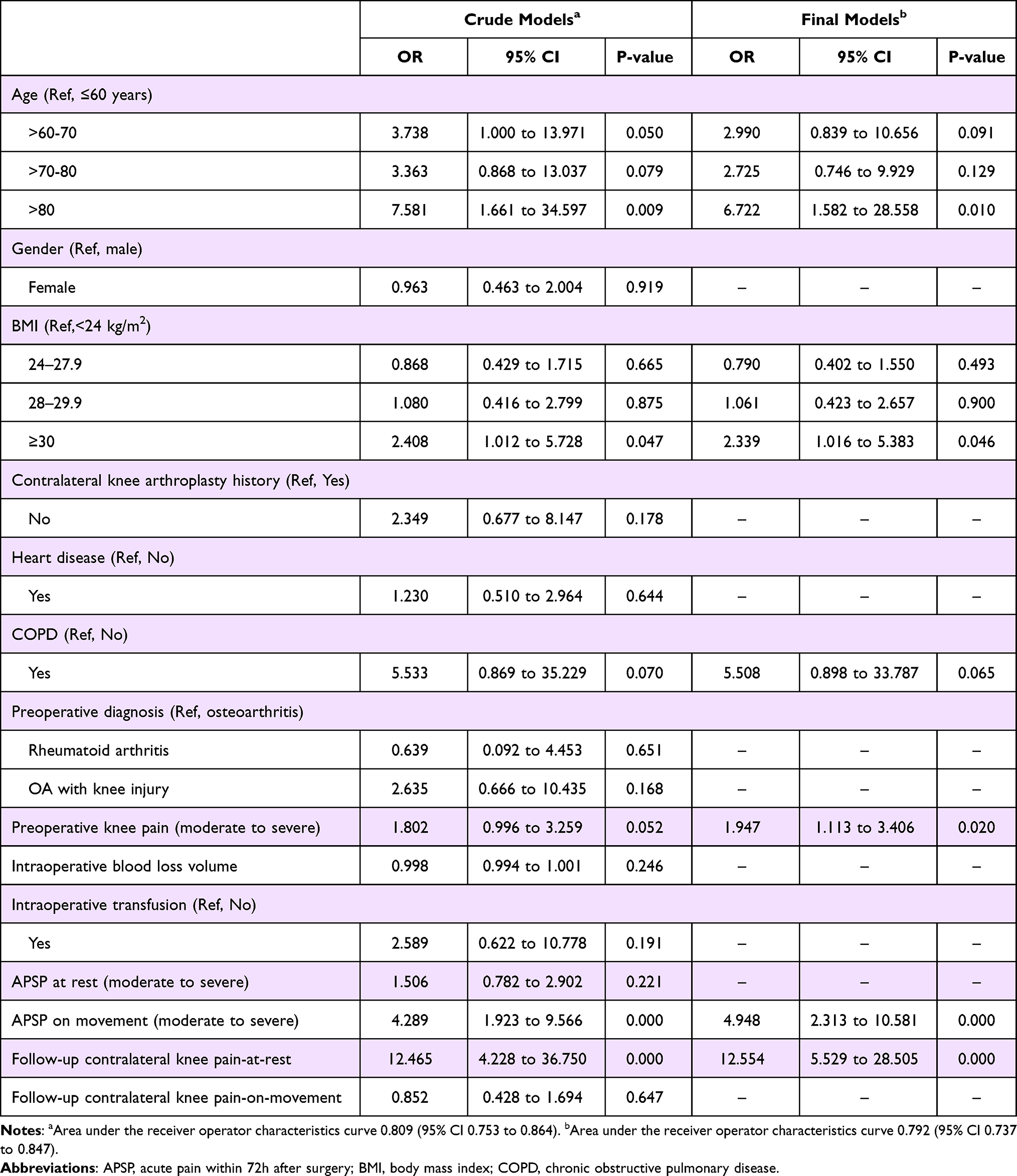 |
Table 4 Multivariable (Adjusted) Binary Logistic Regression Analysis of CPSP at Rest 2-Year Following Knee Arthroplasty (n=605) |
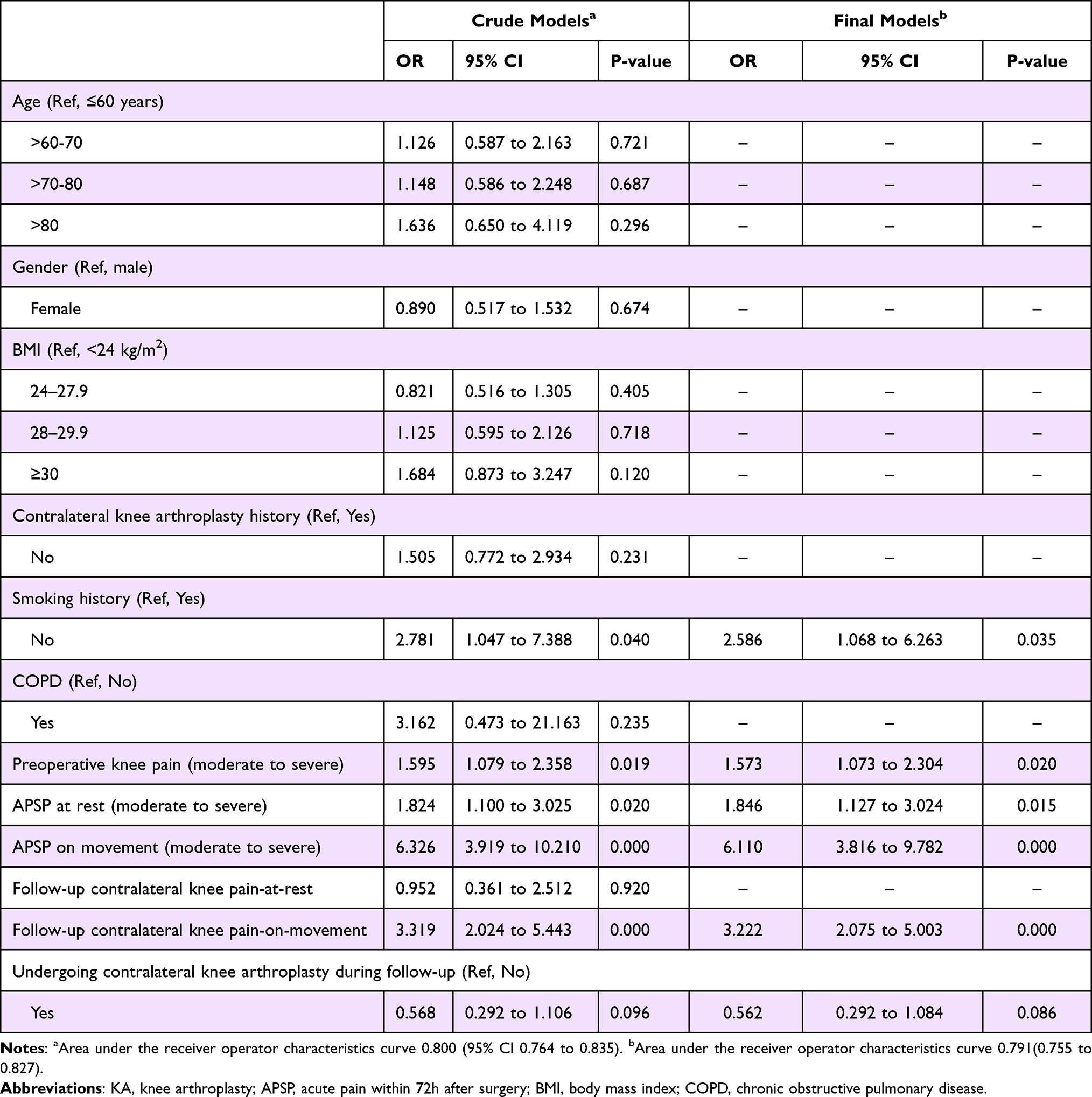 |
Table 5 Multivariable (Adjusted) Binary Logistic Regression Analysis of CPSP on Movement 2-Year Following Knee Arthroplasty (n=605) |
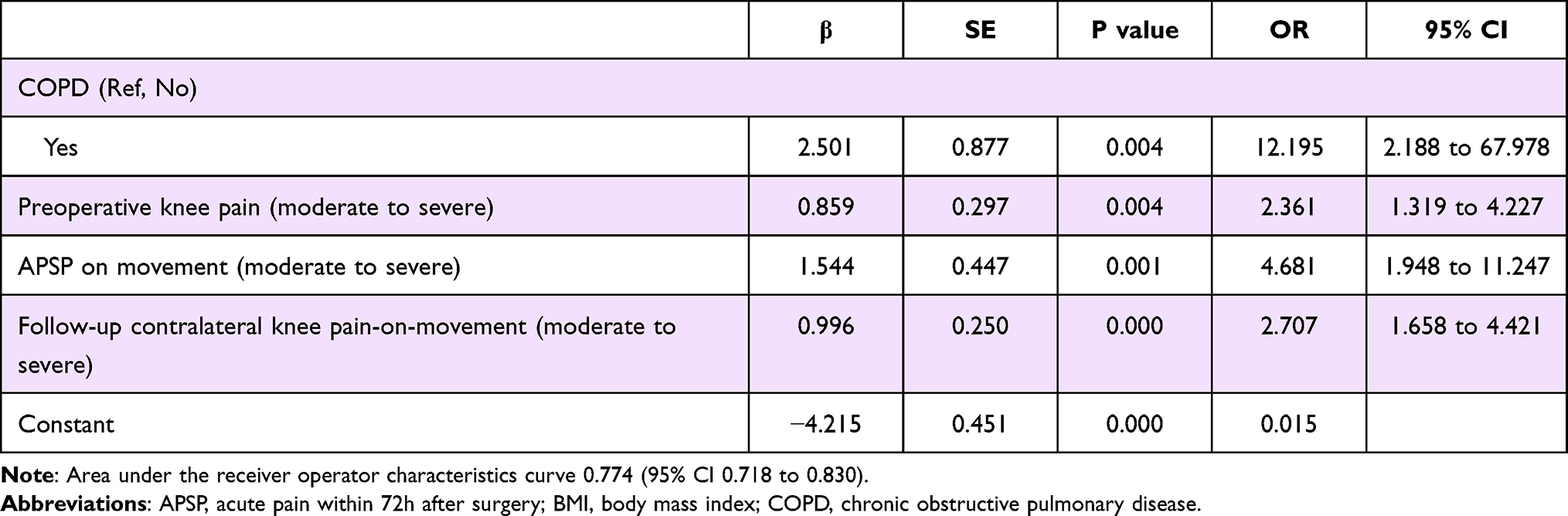 |
Table 6 Parsimonious Multivariable (Adjusted) Binary Logistic Regression Analysis of Moderate to Severe CPSP on Movement 2-Year Following Knee Arthroplasty (n=605) |
As we know, the pain of osteoarthritis (OA) and TKA can be divided into two main categories: pain on movement and pain at rest,11 and there may be different approaches and mechanisms underlying the two different types of pain.4 Most of the existing studies have focused on predictors of chronic pain on movement, further studies are needed to add to the growing body of evidence on it, meanwhile rest pain and movement pain should be discussed separately, for each of these factors can be targeted using a preventive approach.
However, researches on TKA pain has mostly centered on the intervention and management of postoperative acute pain, yet there is still a serious lack of research on chronic pain and its predictive factors after TKA. The aim of this study is to prospectively determine the prevalence of CPSP in patients and to identify potential factors for 2-year postoperative pain outcomes after primary total knee arthroplasty (TKA) and unicompartmental knee arthroplasty (UKA). A better knowledge of contributing factors for CPSP might help to identify its modifiable risk factors and implement stratified management for target groups, so as to reduce its incidence and ultimately improve patients’ satisfaction on knee arthroplasty.
Methods
This study was ethically approved by the Ethics Board of Shanghai Tenth Peoples’ Hospital of Tongji University, reference number SHSY-IEC-4.1/20-21/01 and 05.12.19035, in accordance with the Declaration of Helsinki Ethical Principles for Medical Research Involving Human Subjects. The report of this study adheres to the statement guideline: “Strengthening the Reporting of Observational Studies in Epidemiology” (STROBE).
Participants
The study was conducted as a prospective, observational cohort study on patients who underwent a primary tricompartmental TKA or unicompartmental UKA, excluding patellofemoral arthroplasty. The inclusion and exclusion criteria are shown in Table 1. Patients were recruited between July 2018 and December 2019, from our institution (Department of Joint Surgery, Shanghai Tenth People’s Hospital of Tongji University, China). And eligible subjects were screened and approached 1–2 days prior to surgery by researchers. Participants meeting inclusion criteria were scheduled to meet with researcher the day before surgery to conduct baseline survey complete study procedures. Beforehand, all subjects provided written, informed consent for participating study. Predictors of interest and covariates were collected via a standard questionnaire, and each patient was assigned with a code to protect privacy.
All patients received general anesthesia through endotracheal intubation or laryngeal mask, in combination with or without femoral nerve block, at the anesthesiologist’s discretion. And the cocktails (containing morphine 10mg, Betamethasone 1mL, and 0.25% ropivacaine 20mL) were diluted to a total volume of 100 mL with normal saline injected into the muscles, tendons, suprapatellar bursa, and sub patellar bursa surrounding knee joint before the last skin suture. Whether patients were intravenously given analgesic pump (analgesics and formulations were left to the discretion of the anesthetist according to gender, age, weight and comorbidity of the patient) after surgery for 48h is determined by patients’ intention during preoperative conversations.
Subsequent to the TKA surgery, the patients were transferred to the post-anesthesia care unit (PACU), and then went back orthopedic ward after recovering from anesthesia. Standard postoperative “preemptive, multimodal analgesia regimen”, which includes non-steroidal anti-inflammatory drugs and gabapentin (300 mg q8h), was used for all the patients. And pethidine 50mg was only used when patients reported severe pain. In addition, physiotherapy was performed twice (20 minutes at a time) on a daily basis.
Predictors of Interest and Covariates
(1) Demographic characteristics: age (categorized as ≤60, >60–70, >70–80, >80), gender, and BMI was categorized as underweight or normal weight (BMI< 24 kg/m2), overweight (BMI 24.0–27.9 kg/m2), obese 1 (BMI 28–29.9 kg/m2), obese 2 and above (BMI ≥30 kg/m2), according to the standards of the Working Group on Obesity in China.12
(2) Preoperative clinical variables: Preoperative clinical variables were extracted from the Hospital Information Manage System. And preoperative diagnosis was categorized as osteoarthritis, rheumatoid arthritis, or combined with knee injury (the injury aggravated knee pain, MRI showed a meniscus tear, knee ligament tear); comorbidities for each patient included the most common disease groups of interest that we hypothesized might potentially be related to CPSP were recorded, including hypertension, diabetes, chronic kidney disease, chronic liver diseases, chronic obstructive pulmonary disease (COPD), cardiovascular disease and cerebrovascular disease. The absolute number of comorbidities was used as a variable, and there was no attempt to qualify the actual contribution to CPSP from each comorbidity for each patient, except for hypertension, diabetes, cardiovascular disease and COPD. Additionally, history of contralateral knee arthroplasty was assessed by preoperative routine full-length radiographs of the lower limbs.
(3) Surgery variables: Intraoperative data collected include surgeons, American Society of Anesthesiologists (ASA) physical status, anesthesia method, operation time, surgery site, estimated intraoperative blood loss, with or without intraoperative blood transfusion, and patient-controlled analgesia after surgery.
(4) Preoperative pain: Evaluation were conducted the day before surgery, and each patient was asked about the average pain intensity over the past week, and a four-descriptor verbal rating scale (VRS) measuring pain intensity was used, with the words none, mild, moderate, and severe.
(5) Acute postsurgical pain: APSP was defined as pain within the first 72 hours postoperatively, and it was assessed by trained clinical nurses at 14:00 every day, using the instrument of VRS. Each patient answered two questions: the average pain-at-rest (sitting or lying) over the last 24 hours, the average pain-on-movement (movement from sitting to standing up, walking, standing or using stair) over the last 24 hours. Finally, the maximum value of the measurement in 3 days was set as an independent variable.
Outcome of Interest
And in present study, the independent variables include mild or above level chronic pain at rest and on movement, chronic pain-on-movement of moderate to severe level. A simple questionnaire that assesses the chronic postsurgical pain was conducted via phone call at 2-year (±3 months) time point after surgery to all patients undergone knee arthroplasty. Patients answered questions investigating their situation regarding chronic postsurgical pain (See Table 2). Their responses were also based on a four-descriptor verbal rating scale (VRS) measuring pain intensity: none, mild, moderate, and severe. In addition, another two questions were also included, one was to clarify whether the patients receive professional rehabilitation center after discharge or not; the other requires patients to rate postoperative satisfaction, from not at all satisfied (0% satisfied) to completely satisfied (100% satisfied), which takes up 11 points on the scale.
Statistical Analysis
Descriptive statistics on characteristics of independent and dependent variables comprise frequencies, measures of central tendency (means, median) and dispersion (standard deviation). The primary outcome reveals the prevalence of CPSP at 2-year (± 3months) after knee arthroplasty. The univariable (unadjusted) analysis of independent variables with and without CPSP was determined by binary logistic regression. Multivariable (full model) model of CPSP adjusting for confounding risk factors was performed, including variables with p < 0.2 in the univariable analysis for CPSP. A parsimonious model (final model) was created by binary logistic regression with likelihood ratio test from the full model, and two model building methods were applied: backward elimination and forward selection. Goodness of fit for the models were assessed based on the Hosmer-Lemeshow test, Pseudo R-Squared and the area under the receiver operating characteristics curve (AUC). Measures of effect of variables in the model are reported as adjusted odds ratios (ORs) and 95% confidence intervals (CIs). Predictive models were constructed separately for presence of CPSP-at-rest, CPSP-on-movement, and moderate to severe CPSP-on-movement, to identify specific risk factors associated with each of them. We used SPSS version 23.0 (SPSS, Armonk, NY, USA) for data analysis.
Results
Post Hoc Power Analysis
A post hoc power analysis was computed for the logistic regression (one-sided z test) using the G Power software (Version 3.1.9.7, Germany).13 In this analysis, the power of all statistically significant predictors included into the final model were estimated taking into account other covariables. The preoperative knee pain was the factor with the weakest association (OR=1.573) in this study (Tables 4–6), considering the actual sample size and real findings on this predictor, the minimum power of study was calculated as 0.83 for a significance level of 0.05 (one-sided). The post hoc statistical power analysis indicated that the power of age, BMI, preoperative knee pain, APSP on movement, and contralateral knee pain-at-rest as predictors of CPSP at rest was 1, 0.98, 0.84, 0.99, 0.99, respectively, at a significance level of 5% (one-sided). Similarly, the power of smoking, APSP at rest, APSP on movement and contralateral knee pain-on-movement as predictors of CPSP on movement was 0.84, 0.87, 1, 0.99, respectively.
A total number of 605 patients who were enrolled between July 2018 and December 2019 completed survey and the results were shown in Figure 1. Approximately 12% patients still had rest pain and 38% of whom sufferred movement pain 2 years after primary knee arthroplasty. Among which, the prevalence of moderate-severe pain-on-movement was nearly 10%.
 |
Figure 1 Subject flow through study. |
The univariate associations of predictors of interest with or without CPSP are shown in Table 3. There were significant difference in the chronic pain-at-rest or pain-on-movement group including preoperative pain, APSP, follow-up contralateral knee pain, and presence of requiring opioid rescue within 72h after surgery. Pre-surgical diagnosis of patients with combined knee injury, patients with intraoperative transfusion, patients requiring opioid rescue were associated with the occurrence of chronic pain-at-rest, while patients undergoing another knee arthroplasty during follow-up was correlated with lower incidence of chronic pain-on-movement.
Age, gender, BMI, history of contralateral knee arthroplasty, heart diseases, COPD, preoperative diagnosis, preoperative pain intensity, estimated intraoperative blood loss, intraoperative transfusion, APSP at rest and with movement, requiring opioid rescue, follow-up contralateral knee pain intensity at rest and with movement were entered in a binary logistic regression model (full model) for chronic pain-at-rest. The full model had a Nagelkerke’s pseudo R2=0.285, a Homer and Lemeshow p=0.406, and an AUC of 0.809 (95% CI 0.753 to 0.864). The more accurate model included six factors were found to be independently and significantly associated with the presence of CPSP at rest (Table 4): age > 80 (OR = 6.772, 95% CI = [1.582–28.558], P = 0.01), BMI ≥ 30 (OR = 2.339, 95% CI = [1.016–5.383], P = 0.046), with moderate to severe preoperative knee pain (OR = 1.947, 95% CI = [1.113–3.406], P = 0.02), a moderate to severe APSP on movement (OR = 4.948, 95% CI = [2.313–10.581], P < 0.001), and suffering a higher contralateral knee pain-at-rest (OR = 12.554, 95% CI = [5.529–28.505], P < 0.001) (Figure 2). Further Z-test compared the areas under ROC curves, there was no significant difference between them, and their diagnostic performance was similar (Z = 0.3757, p = 0.0.707). The final model had a Nagelkerke’s pseudo R2=0.263, a Homer and Lemeshow p=0.767 and an AUC of 0.792 (95% CI 0.737 to 0.847). Binary characteristics of the final model was sensitivity 21.9% (95% CI 13.4% to 33.4%), specificity 98.7 (95% CI 97.2% to 99.4%), positive predictive value 69.6% (95% CI 47.0% to 85.9%), negative predictive value 90.2% (95% CI 87.4% to 92.4%) and a diagnostic accuracy of 89.4% (95% CI 86.6% to 91.7%).
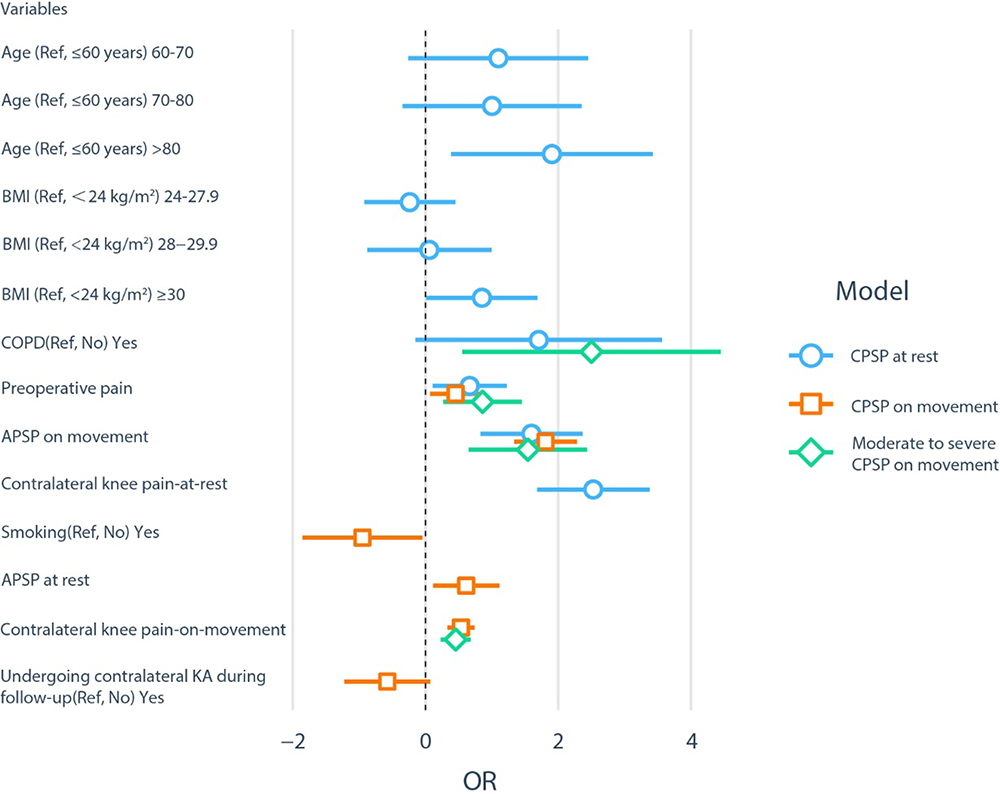 |
Figure 2 Parsimonious multivariable (adjusted) binary logistic regression of CPSP-at-rest, CPSP-on-movement and moderate to severe CPSP-on-movement. |
For chronic pain-on-movement, age, gender, BMI, history of contralateral knee arthroplasty, COPD, smoking, preoperative pain intensity, APSP at rest and with movement, requiring opioid rescue within operative 72h, follow-up contralateral knee pain intensity at rest and with movement, and undergoing another knee arthroplasty during follow-up were entered in a full model, and the full model had a Nagelkerke’s pseudo R2=0.334, a Homer and Lemeshow p=0.985, and an AUC of 0.800 (95% CI 0.764 to 0.835). Stepwise elimination identified five predictors to be independently and significantly associated with the presence of CPSP on movement in the parsimonious final model (Table 5): no smoking history (OR = 2.586, 95% CI = [1.068–6.263], P = 0.035), having moderate to severe preoperative knee pain (OR = 1.573, 95% CI = [1.073–2.304], P = 0.02), a moderate to severe APSP at rest (OR = 1.846, 95% CI = [1.127–3.024], P =0.015) and on movement (OR = 6.110, 95% CI = [3.816–9.782], P < 0.001), and suffering a higher contralateral knee pain-on-movement (OR = 3.222, 95% CI = [2.075–5.003], P < 0.001). Further Z-test compare the areas under ROC curves, there was no statistical difference between the performance of two models (Z = 0.322, p = 0.747). The final model had a Nagelkerke’s pseudo R2=0.317, a Homer and Lemeshow p = 0.941 and an AUC of 0.791 (95% CI 0.755 to 0.827). Binary characteristics s of the final model was sensitivity 66.7% (95% CI 60.1% to 72.7%), specificity 78.0 (95% CI 73.4% to 82.0%), positive predictive value 64.7% (95% CI 58.2% to 70.7%), negative predictive value 79.5% (95% CI 74.9% to 83.4%) and a diagnostic accuracy of 73.7% (95% CI 70.0% to 77.2%).
Same as above, we also performed predictive analysis for moderate to severe chronic pain-on-movement. In the final model, four predictors showed independently and significantly associated with the presence of moderate to severe CPSP on movement (Table 6). Concomitant COPD was significant as a predictive factor (OR = 12.195, 95% CI = [2.188–67.978], P = 0.004), and having moderate to severe preoperative pain (OR = 2.361, 95% CI = [1.319–4.227], P = 0.004), a moderate to severe APSP with movement (OR = 4.681, 95% CI = [1.948–11.247], P = 0.001), and suffering a higher contralateral knee pain-on-movement (OR = 2.707, 95% CI = [1.658–4.421], P < 0.001). The final model had a Nagelkerke’s pseudo R2=0.192, a Homer and Lemeshow p=0.425 and an AUC of 0.774 (95% CI 0.718 to 0.830). And sensitivity, specificity, positive predictive value, negative predictive value, and diagnostic accuracy were 10% (95% CI 4.1% to 21.2%), 99.4% (95% CI 98.3% to 99.9%), 66.6% (95% CI 30.9% to 90.9%), 90.9% (95% CI 88.3% to 93.1%), 90.6% (95% CI 87.9% to 92.7%), respectively. The Hosmer-Lemeshow test gave a non-significant result (P value > 0.05), indicating an absence of fit issues for above three final model.
And, no relationship was found between whether to undertake professional rehabilitation after discharge and occurrence of chronic pain in present study. Overall satisfaction was classified as dissatisfied (0–60%), natural (70–80%) and Satisfied (90–100%), and our results revealed that 72%(n=437) of patients claimed that they were satisfied or very satisfied, 17% (n=101) of patients were neutral, while 11% (n=67) were very dissatisfied or dissatisfied, expressing their regret having surgery.
Discussion
This study showed an overall incidence of CPSP involving in pain at rest and on movement at the follow-up time (2-year postoperatively) of 12.1% and 37.7%, respectively, in which, 9.8% of patients suffered moderate to severe pain on movement. Our study has found that approximately 11% of patients are not satisfied 2-year after surgery, which was in accordance with the figures reported in western counties,14,15 and it was related to chronic pain: at rest and on movement.
Our finding suggests that BMI is probably associated with rest pain instead of pain on movement for chronic pain at rest that might related to subchondral bone pressure.11 Patients above 80 years old were more inclined to chronic pain at rest in present study, which was not in accordance with previous research.16,17 As chronic pain at rest was related to subchondral bone pressure, together with the evidence that 40% of those over the age of 80 years are sarcopenic obesity,18 it can be referred that the correlation between age > 80 year and chronic rest pain might be attributed to muscle weakness. Therefore, targeting this demographic emphasis will be on enhance the muscle strength to prevent chronic pain at rest.
Moreover, our study indicated that acute postoperative pain-at-rest was correlated to chronic pain with movement, rather than chronic pain at rest after adjusting acute postoperative pain-on-movement and the pain in the contralateral knee. Surgical trauma can lead to the release of inflammatory mediators (CRP, PGE2, and IL-6) at the site of injury, which are positively correlated with acute postoperative pain following primary TKA.19 Meanwhile chronic pain with movement is proved to be strongly correlated to inflammation, on the contrary, chronic pain at rest might related to subchondral bone pressure.11
More importantly, our empirical analysis found a strong positive correlation between acute pain-on-movement and chronic pain outcomes in final model, which was not in accordance with the results of Sayer et al4 on account of the inconsistency in assessing and calculating the variable of pain within the first 72 hours postoperatively. In present study, we assessed the pain-at-rest and pain-on-movement at 14:00 every day by asking patients’ average pain over the last 24 hours, then took the maximum value of the measurement in 3 days and the primary aim of this design was to avoid the influence of anesthetic effects, analgesic effects and rehabilitation exercise on pain, and ultimately aiming to develop a simple and feasible model to predict CPSP after knee arthroplasty for clinical practice. It is highlighted that pethidine was only used when patients reported breakthrough pain, while in the above study,4 opioids (oxycodone) were given to patients every 12 hours, and this might result in differences of APSP degree that cannot be ignored. In this research, approximately 62% of patients report moderate to severe pain-on-movement within the first 72 hours postoperatively, noticeably higher than prevalence of moderate to severe pain before TKA (40.3%), which suggests that there is still space for improvement in acute postoperative pain management. To our knowledge, central sensitization is probably an important mechanism for the development of CPSP and if patients continued to be exposured to nociception caused by surgery over time, that will further generate primary hyperalgesia and secondary hyperalgesia, leading to CPSP.21 Our founding revealed that acute pain-on-movement, and preoperative pain were independent risk factors for occurrence of CPSP. Obviously, poorly controlled acute pain-on-movement is not equivalent to preoperative pain in terms of prediction of CPSP after TKA, and each of the two factors can be targeted using a preventive approach. Therefore, compared with the preoperative pain, acute postoperative pain is more likely to be under control and optimal management to reduce the risk of CPSP for clinician. In addition, the nature in pain suggests these two factors may be mutually maintaining, being linked to shared negative pain cognitions and pain coping strategies, and pain itself may serve as traumatic stressor that induces increased emotional numb.22 In order to preventive analgesia, a cognitive-behavioral perspective are desirable on the basis of screening for both factors.
Our study data showed that after adjusting factors including patients’ characters, operative factors, preoperative pain and APSP, presence of follow-up contralateral knee pain was an independent risk factor for CPSP at 2-year after primary knee arthroplasty. The painful affected knee tended to avoid bearing weight, then contralateral knee was inevitably bearing increased load during OA disease progression and surgical recovery,23,24 such asymmetrical loadings are likely to increase subchondral bone pressure, which is more associated with pain-at-rest.11 In addition, an increased rate of loading at the knee joint has been associated with weakened quadriceps strength,25 which results in arthrogenic muscle inhibition (AMI) to impairedynamic knee-joint stability26 and narrow tibiofemoral joint-space.27 Therefore, achieving symmetry loadings on both knees and adopting promising intervention of mitigating the effects of AMI are latent important target in decreasing chronic pain-at-rest.
An unexpected discovery in our study is that smoking is the protective factor for both acute and chronic pain-on-movement, and it is a psychological factor that cannot be ignored (eg anxiety, depression), which has been proved to be correlate with the severity of pain from nociceptive stimuli.2 Additionally, there were studies of smokers have shown that nicotine can reduce anxiety and relieve stress.28 However, the association of smoking with increased levels of inflammatory markers is well documented,29 and the present study did not include the exact amount of smoking, more importantly there is no significant correlation between smoking and moderate to severe chronic pain in our study. Therefore, further researches are needed concerning the relationship between smoking and chronic pain.
In addition to the pain indicators at different time points, chronic obstructive pulmonary disease (COPD) was an independent risk factors, and to our knowledge, this is the first study to show the association between COPD and the occurrence of chronic pain after knee arthroplasty. A recent study has borne out claims that systemic inflammation is also found in patients with COPD,30 generating chronic and neuropathic pain by activating cytokines, which may be known as underlying mechanisms for chronic pain-on-movement after knee arthroplasty. In addition, chronic pain in COPD is associated with higher depression and lower physical activity, and this may aggravate chronic pain after TKA.
However, there were several strengths and limitations in our study. To our knowledge, this is the first reported large cohort of patients followed up to 2-years for chronic pain after knee arthroplasty, and the rest pain and movement pain were predicted, respectively. As a result, it allowed us to explore the meaningful predictors under the control of demography data and surgery variables confounders. The limitation of this study is no psychological variables were included, although our predictive performance is not less than previous researches included psychological variables, this might impede discovering deeper causes underlying contributing variables; and we did not measure functional status based on the accepted scale for the participants, future researches are needed to fill in the gaps.
In conclusion, our result showed that the prevalence of CPSP at rest and with movement at 2-year and that age >80 years and BMI ≥30 are risk factors for CPSP at rest following TKA/UKA; and follow-up contralateral knee pain-at-rest is a risk factor for CPSP at rest, while contralateral kne pain-on-movement is a risk factor for CPSP on movement. Additionally, patients with COPD has higher risk for developing moderate to severe CPSP after surgery. However, nonresponse bias and single study center limits the generalizability of study findings and further research is needed to investigate the different predictors behind CPSP at rest and on movement after knee arthroplasty using robust research designs.
Ethical Approval
This study was ethically approved by the Ethics Board of Shanghai Tenth Peoples’ Hospital of Tongji University. Ethical approval number: SHSY-IEC-4.1/20-21/01 and 05.12.19035.
Disclosure
The authors report no conflicts of interest for this work.
References
1. Lange JK, Lee YY, Spiro SK, Haas SB. Satisfaction rates and quality of life changes following total knee arthroplasty in age-differentiated cohorts. J Arthroplasty. 2018;33(5):1373–1378. doi:10.1016/j.arth.2017.12.031
2. Kim DH, Pearson-Chauhan KM, McCarthy RJ, Buvanendran A. Predictive factors for developing chronic pain after total knee arthroplasty. J Arthroplasty. 2018;33(11):3372–3378. doi:10.1016/j.arth.2018.07.028
3. Sugiyama Y, Iida H, Amaya F, et al. Prevalence of chronic postsurgical pain after thoracotomy and total knee arthroplasty: a retrospective multicenter study in Japan (Japanese Study Group of Subacute Postoperative Pain). J Anesth. 2018;32(3):434–438. doi:10.1007/s00540-018-2481-0
4. Sayers A, Wylde V, Lenguerrand E, et al. Rest pain and movement-evoked pain as unique constructs in hip and knee replacements. Arthritis Care Res (Hoboken). 2016;68(2):237–245. doi:10.1002/acr.22656
5. Grosu I, Thienpont E, De Kock M, Scholtes JL, Lavand’homme P. Dynamic view of postoperative pain evolution after total knee arthroplasty: a prospective observational study. Minerva Anestesiol. 2016;82(3):274–283.
6. Thomazeau J, Rouquette A, Martinez V, et al. Predictive factors of chronic post-surgical pain at 6 months following knee replacement: influence of postoperative pain trajectory and genetics. Pain Physician. 2016;19(5):E729–41.
7. Macrae W, Davies HT. Chronic postsurgical pain. In: Epidemiology of Pain. IASP Press; 1999:18.
8. Singh JA, Yu S, Chen L, Cleveland JD. Rates of total joint replacement in the United States: future projections to 2020-2040 using the national inpatient sample. J Rheumatol. 2019;46(9):1134–1140. doi:10.3899/jrheum.170990
9. Gaskin DJ, Richard P. The economic costs of pain in the United States. J Pain. 2012;13(8):715–724. doi:10.1016/j.jpain.2012.03.009
10. Wylde V, Beswick AD, Dennis J, Gooberman-Hill R. Post-operative patient-related risk factors for chronic pain after total knee replacement: a systematic review. BMJ Open. 2017;7(11):e018105. doi:10.1136/bmjopen-2017-018105
11. Creamer P. Current perspectives on the clinical presentation of joint pain in human OA. Novartis Found Symp. 2004;260:
12. China CM-aGotWGoOi. Predictive values of body mass index and waist circumference torisk factors of related diseases in Chinese adult population. Chin J Epidemiol. 2002;23(1):6. doi:10.3760/j.issn:0254-6450.2002.01.003
13. Faul F, Erdfelder E, Lang AG, Buchner A. G*Power 3: a flexible statistical power analysis program for the social, behavioral, and biomedical sciences. Behav Res Methods. 2007;39(2):175–191. doi:10.3758/BF03193146
14. Baker PN, van der Meulen JH, Lewsey J, Gregg PJ; National Joint Registry for E, Wales. The role of pain and function in determining patient satisfaction after total knee replacement. Data from the National Joint Registry for England and Wales. J Bone Joint Surg Br. 2007;89(7):893–900. doi:10.1302/0301-620X.89B7.19091
15. Bourne RB, Chesworth BM, Davis AM, Mahomed NN, Charron KD. Patient satisfaction after total knee arthroplasty: who is satisfied and who is not? Clin Orthop Relat Res. 2010;468(1):57–63. doi:10.1007/s11999-009-1119-9
16. Singh JA, Gabriel SE, Lewallen DG. Higher body mass index is not associated with worse pain outcomes after primary or revision total knee arthroplasty. J Arthroplasty. 2011;26(3):366–374 e1. doi:10.1016/j.arth.2010.02.006
17. Namba RS, Singh A, Paxton EW, Inacio MCS. Patient factors associated with prolonged postoperative opioid use after total knee arthroplasty. J Arthroplasty. 2018;33(8):2449–2454. doi:10.1016/j.arth.2018.03.068
18. Hiona A, Leeuwenburgh C. The role of mitochondrial DNA mutations in aging and sarcopenia: implications for the mitochondrial vicious cycle theory of aging. Exp Gerontol. 2008;43(1):24–33. doi:10.1016/j.exger.2007.10.001
19. Si HB, Yang TM, Zeng Y, et al. Correlations between inflammatory cytokines, muscle damage markers and acute postoperative pain following primary total knee arthroplasty. BMC Musculoskelet Disord. 2017;18(1):265. doi:10.1186/s12891-017-1597-y
20. Reddi D, Curran N. Chronic pain after surgery: pathophysiology, risk factors and prevention. Postgrad Med J. 2014;90(1062):
21. Grosu I, de Kock M. New concepts in acute pain management: strategies to prevent chronic postsurgical pain, opioid-induced hyperalgesia, and outcome measures. Anesthesiol Clin. 2011;29(2):311–327. doi:10.1016/j.anclin.2011.04.001
22. Katz J, Asmundson GJ, McRae K, Halket E. Emotional numbing and pain intensity predict the development of pain disability up to one year after lateral thoracotomy. Eur J Pain. 2009;13(8):870–878. doi:10.1016/j.ejpain.2008.10.003
23. Van Onsem S, Verstraete M, Zwaenepoel B, Dhont S, Van der Straeten C, Victor J. An evaluation of the influence of force- and weight bearing (a)symmetry on patient reported outcomes after total knee arthroplasty. Acta Orthop Belg. 2020;86(2):294–302.
24. Maxwell J, Niu J, Singh JA, Nevitt MC, Law LF, Felson D. The influence of the contralateral knee prior to knee arthroplasty on post-arthroplasty function: the multicenter osteoarthritis study. J Bone Joint Surg Am. 2013;95(11):989–993. doi:10.2106/JBJS.L.00267
25. Mikesky AE, Meyer A, Thompson KL. Relationship between quadriceps strength and rate of loading during gait in women. J Orthop Res. 2000;18(2):171–175. doi:10.1002/jor.1100180202
26. Felson DT, Niu J, McClennan C, et al. Knee buckling: prevalence, risk factors, and associated limitations in function. Ann Intern Med. 2007;147(8):534–540. doi:10.7326/0003-4819-147-8-200710160-00005
27. Segal NA, Glass NA, Torner J, et al. Quadriceps weakness predicts risk for knee joint space narrowing in women in the MOST cohort. Osteoarthritis Cartilage. 2010;18(6):769–775. doi:10.1016/j.joca.2010.02.002
28. Picciotto MR, Brunzell DH, Caldarone BJ. Effect of nicotine and nicotinic receptors on anxiety and depression. Neuroreport. 2002;13(9):1097–1106. doi:10.1097/00001756-200207020-00006
29. Bakhru A, Erlinger TP. Smoking cessation and cardiovascular disease risk factors: results from the Third National Health and Nutrition Examination Survey. PLoS Med. 2005;2(6):e160–e160. doi:10.1371/journal.pmed.0020160
30. Ovsyannikov ES, Avdeev SN, Budnevsky AV. [Systemic inflammation in patients with chronic obstructive pulmonary disease and obesity]. Ter Arkh. 2020;92(3):13–18. Russian. doi:10.26442/00403660.2020.03.000265
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.