Back to Journals » International Journal of General Medicine » Volume 16
Prevalence and Factors Associated with Depression in Patients with Diabetes Mellitus and Pulmonary Tuberculosis (DM-PTB): A Hospital-Based Cross-Sectional Study
Authors Li X, Fang X, Zhou L, Mao Y
Received 26 April 2023
Accepted for publication 6 August 2023
Published 14 August 2023 Volume 2023:16 Pages 3465—3472
DOI https://doi.org/10.2147/IJGM.S412675
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Luca Testarelli
Xiucai Li,1,* Xuee Fang,2,* Ligang Zhou,1 Yanjun Mao3
1Department of Endocrinology, Shanghai Pudong Hospital, Fudan University Pudong Medical Center, Shanghai, People’s Republic of China; 2Department of Tuberculosis, Shanghai Pulmonary Hospital Affiliated to Tongji University, Shanghai, People’s Republic of China; 3Department of Nursing, Shanghai Pulmonary Hospital Affiliated to Tongji University, Shanghai, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Ligang Zhou, Department of Endocrinology, Shanghai Pudong Hospital, Fudan University Pudong Medical Center, Shanghai, People’s Republic of China, Email [email protected] Yanjun Mao, Department of Nursing, Shanghai Pulmonary Hospital Affiliated to Tongji University, Shanghai, People’s Republic of China, Email [email protected]
Background and Objectives: A high incidence of depression has been reported in patients with pulmonary tuberculosis and diabetes mellitus (DM-PTB). However, the association between depression and DM-PTB is poorly understood and requires further investigation. This study aimed to evaluate the prevalence of depression and the associated factors in patients with DM-PTB.
Methods: A cross-sectional study was conducted among DM-PTB patients at the Tuberculosis Department of Shanghai Pulmonary Hospital Affiliated to Tongji University, China, enrolled between June 2021 and October 2021. The depression status, nutritional status, and the quality of life of the patients were evaluated using Patient Health Questionnaire– 9 (PHQ-9), Nutritional Risk Screening 2002 (NRS2002), and Quality of Life Instruments for Chronic Diseases-Pulmonary Tuberculosis (QLICD-PT), respectively.
Results: A total number of 280 DM-PTB patients were screened, of whom 22 were excluded for missing data. Among the 258 DM-PTB patients subjected to analysis, 199 patients (77.13%) had PHQ-9 scores above 10. The patients with depression are more likely to have a lower monthly income, body mass index (BMI), and QLICD-PT than those without depression. The NRS2002 score and glutamic pyruvic transaminase (GPT) and glutamic oxaloacetic transaminase (GOT) levels in the depression group were more likely to be higher than those in the control group. Multivariate logistic regression analysis showed that physical function [OR = 0.798, 95% confidence interval (CI), 0.716– 0.889, P < 0.001] was a protective factor against depression, whereas NRS2002 ≥ 3 (OR = 2.299, 95% CI, 1.095– 4.825, P = 0.028), GPT (OR = 1.048, 95% CI, 1.018– 1.079, P = 0.002), and social function (OR = 1.103, 95% CI, 1.033– 1.179, P = 0.004) were risk factors of depression.
Conclusion: Depression in DM-PTB patients may be associated with monthly income, BMI, QLICD-PT scores, NRS2002 scores, GPT, and GOT levels.
Keywords: depression, pulmonary tuberculosis, diabetes mellitus, cross-sectional study
Background
Pulmonary tuberculosis (PTB) is a chronic contagious disease caused by Mycobacterium tuberculosis infection that primarily affects the lungs.1 Diabetes mellitus (DM), on the other hand, is a metabolic disease marked by abnormally high blood glucose levels, either induced by reduced insulin production or insulin resistance.2 Both PTB and DM are major health issues that affect millions of people worldwide, and the PTB and DM comorbidity (DM-PTB) has become an emerging public health challenge, since PTB and DM may collectively lead to severe sequelae and complications, poor treatment outcomes, and increased mortality.3 It has been showed that DM patients were more susceptible to PTB due to weakened immune systems.4 In addition, PTB may promote existing insulin resistance and aggravate DM management.5 As reported by the World Health Organization (WHO), DM ranked the fifth risk factor for PTB incidence and was responsible for approximately 0.4 million of the new PTB cases in 2021.6 Accordingly, there is an urgent need for resolving their clinical complications and the associated risk factors of DM-PTB.
Besides the direct physiological and pathological impacts of chronic diseases (such as PTB and DM), accumulating evidence suggests a higher risk of depression in patients with chronic diseases.7 A previous study revealed that the prevalence of depression in PTB patients was higher than that of healthy populations.8 Human immunodeficiency virus (HIV) infection, poor social support, and perceived stigma being were found to be major risk factors for this condition.9–11 Moreover, depression in PTB patients is often associated with insufficient health care and poor treatment compliance, leading to increased drug resistance, morbidity, and mortality,4 thus negatively affecting their health-related quality of life (QOL).5,6 Consequently, understanding the essential relationships between depression and DM-PTB is urgently needed. Although the association between depression and PTB has been extensively investigated,7–9 little is known about the prevalence and risk factors of depression in DM-PTB patients. Therefore, this hospital-based cross-sectional study aimed to evaluate the prevalence of depression and the associated factors in DM-PTB patients.
Methods
Study Design and Subjects
This hospital-based cross-sectional study was conducted from June 1st to October 30th 2021 in Shanghai Pudong Hospital. Young adult participants with DM-PTB were recruited through convenience sampling. The following inclusion criteria were applied: (1) patients with DM-PTB;10 (2) age of ≥18 and ≤44 years; (3) signed an informed consent form. The exclusion criteria were as follows: (1) incomplete medical history; (2) diagnosed with extrapulmonary TB. This study was approved by the Ethics Committee of Shanghai Pulmonary Hospital Affiliated to Tongji University (No. K19-146).
Data Collection
Structured questionnaires were used to collect the enrolled participants’ information before the start of anti-TB drug treatment. All patients were interviewed by nurses who had received systematic and standardized training. The interviews lasted approximately 15–20 min for each patient. Demographic data, including age, educational level, occupation, marital status, body mass index (BMI), and income were collected. The height and weight of the patients were measured under the same conditions on the first post-admission day. BMI was used to assess the patients’ nutritional status.11 Patients with BMI below 18.5 kg/m2 were considered underweight or with malnutrition.12 Basic medical data, including comorbidities, treatment duration, hemoglobin (Hb), albumin (ALB), liver function (indicated by glutamic-pyruvic transaminase, GPT, and glutamic oxaloacetic transaminase, GOT), and medical cost origin were also collected from medical records.
The Nutritional Risk Screening 2002 (NRS2002) guidelines were used for evaluating the nutritional status of the recruited patients.13 The NRS2002 score was defined as the sum of the nutritional score, the severity of disease score, and the age adjustment score. The total NRS2002 score ranged within 0–7. Patients with total scores < 3 were considered with no nutritional risk, whereas those with scores ≥ 3 were considered to have nutritional risks.
The depression status of the patients was assessed by the Patient Health Questionnaire-9 (PHQ-9),14 consisting of nine items. Each item was scored as 0 (not at all), 1 (several days), 2 (more than half of the days), or 3 (nearly every day). The total score of the PHQ-9 ranged between 0 and 27. Since patients with PHQ-9 scores over 10 are considered more prone to depression,15 we divided the PTB patients into a depression group (score ≥ 10) and a control group (score < 10).
The patients’ quality of life (QoL) was assessed by the Quality of Life Instruments for Chronic Diseases-Pulmonary Tuberculosis (QLICD-PT),16 which included three domains as well as one specific model: Physiological function (essential physiological function, independence, energy, and discomfort), psychological function (cognition, emotion, will, and personality), social function (interpersonal interaction, social support, and social role), plus a specific module (respiratory symptoms, systemic symptoms, drug side effects, and particular psychology).
Statistical Analysis
Data analysis was conducted using the SPSS software version 21.0 (IBM, USA). The patients’ demographic and disease characteristics were analyzed with independent t-tests and Pearson’s correlation coefficient tests where appropriate. P < 0.1 in univariate analysis were entered into the multivariate logistic regression and analyzed using the forward mode. P < 0.05 was considered to indicate statistically significant differences.
Results
Demographic Characteristics
A total number of 280 PTB patients were initially recruited, of whom 15 were excluded due to missing data and medical history of PTB, 5 were excluded due to missing blood nutritional indicators of PTB, and 2 were excluded due to missing QLICD-PT data. Finally, the data of a total number of 258 DM-PTB patients (92.14%) were subjected to analysis (Figure 1). The mean age of the patients was 31.00 ± 7.67 years (range 18–44 years, median 27 years). Of these included patients, 156 (60.47%) were men, 134 (51.94%) were married, 204 (79.07%) received senior primary, secondary, or above education, 147 (56.98%) were unemployed, and 116 (44.96%) had a monthly income above 5000 yuan (Table 1).
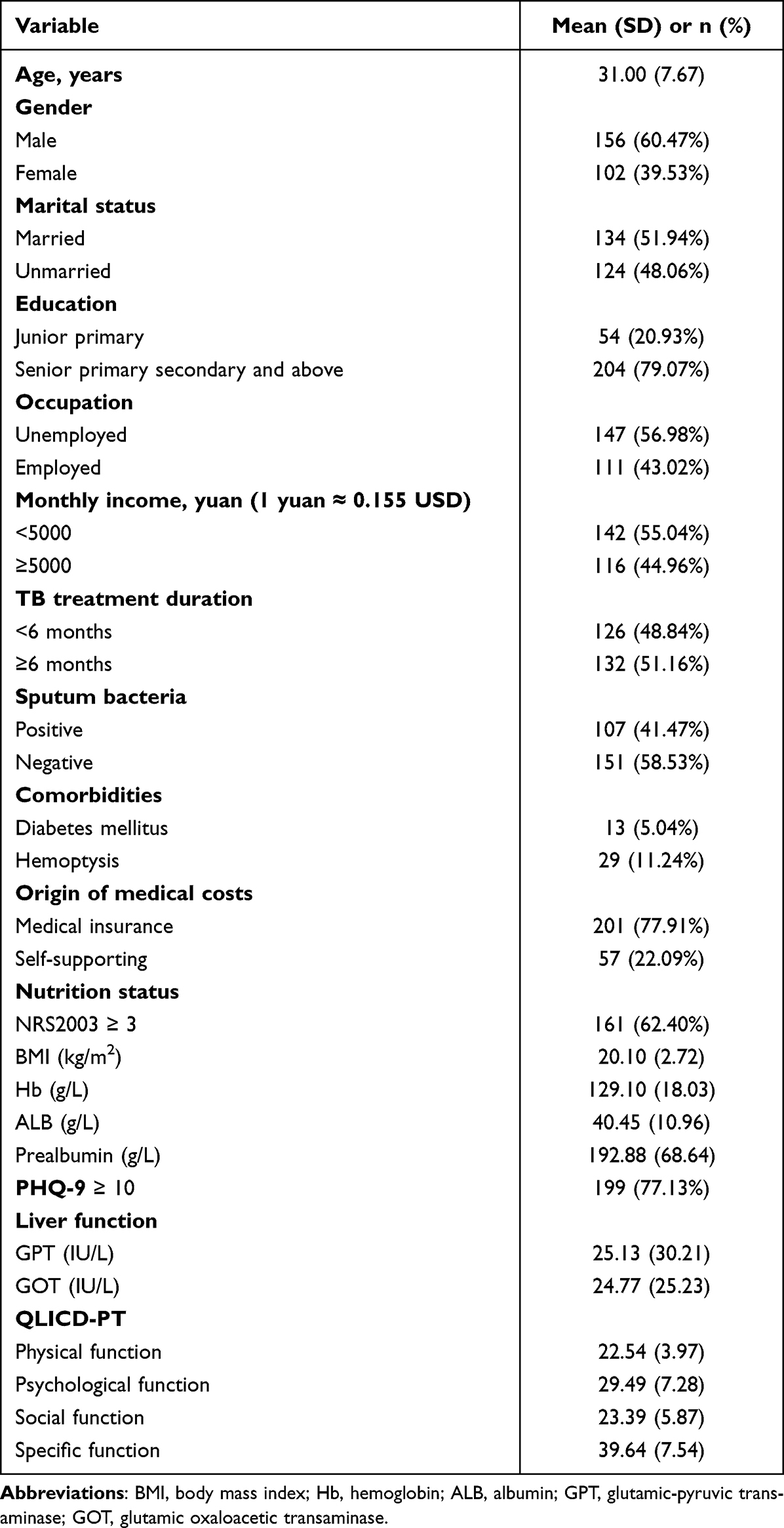 |
Table 1 Demographic Characteristics |
 |
Figure 1 Flow chart. |
Risk Factors Associated with Depression in DM-PTB Patients
With the threshold of PHQ score set to 10, the DM-PTB patients were divided into depression (n = 199, 77.13%) and control (n = 59, 22.87%) groups. There was no significant difference in age, gender, marital status, education level, occupation, TB treatment duration, sputum bacterial test results, comorbidities, and origin of medical costs between the two groups. A tendency for a lower monthly income was observed in the patients in the depression group. The BMI, overall QLICD-PT scores, and QLICD-PT scores of the physical, psychological, social, and specific functions of the depression group were significantly lower than those of the control group. Besides, a larger percentage of patients in the depression group had NRS2002 ≥ 3 than in the control group. Additionally, the GPT and GOT levels in the depression group were significantly higher than those in the control group, indicating potentially impaired liver functions (Table 2). Supplementary Table 1 displays the detailed comparison of the data the nutritional status of the DM-PTB patients, reflected by their BMI values. Overall, 29.46% of the DM-PTB patients were found to be underweight (BMI < 18.5). In the depression group, 130 (65.33%) of the patients had a BMI within the normal range, whereas 42 (71.19%) of the patients from the control group had normal nutritional status. Notably, the ratios of patients with mild (20.10%), moderate (8.54%), and severe thinness (3.52%) in the depression groups were higher than those in the control group (11.86%, 5.08%, and 3.39%, respectively).
 |
Table 2 Univariate Analysis |
Multivariate logistic regression analysis was performed to identify risk factors that independently associated with depression. As can be seen in Table 3, physical function [OR = 0.798, 95% confidence interval (CI), 0.716–0.889, P < 0.001] is a protective factor against depression, whereas NRS2002 ≥ 3 (OR = 2.299, 95% CI, 1.095–4.825, P = 0.028), GPT (OR = 1.048, 95% CI, 1.018–1.079, P = 0.002), and social function (OR = 1.103, 95% CI, 1.033–1.179, P = 0.004) are risk factors positively associated with depression.
 |
Table 3 Multivariate Logistic Regression Analysis |
Discussion
In this cross-sectional study, we found that depression in DM-PTB patients was associated with a lower monthly income, BMI, and QLICD-PT scores, as well as higher NRS2002 scores, GPT, and GOT levels. Physical function was a protective factor against depression, whereas NRS2002 ≥ 3, GPT and social function were risk factors positively associated with depression in DM-PTB patients. Understanding the occurrence and risk factors of depression in DM-PTB patients could help identify high-risk individuals, enabling early intervention and treatment to improve their QoL and prognosis.
Depression research encompasses multiple medical disciplines and requires long-term follow-up, adding complexity to the study. Despite these challenges, we prioritize addressing depression due to its potential impact on treatment outcomes, QoL, and its relatively high prevalence in DM-PTB patients. Focusing on depression allows for a comprehensive consideration of patients’ mental health, promoting overall treatment effectiveness. Most of the patients in this study were males aged between 18–44 years with relatively low incomes. The prevalence of depression in PTB patients was 41.1% in Nigeria,17 61.1% in Cameron,18 56% in Pakistan,19 54% in Ethiopia,20 16.8% in Philippines,13 and 69.6% in Liaoning Province of China.21 The percentage of depressed DM-PTB patients in this study was 77.13%, which is higher than those reported for PTB patients in the above studies. Such a difference may be attributed to the fact that we studied DM-PTB patients exclusively, who might have had a higher risk of developing depression than PTB patients due to more complications, treatment difficulties, and poor general health conditions induced by PTB and DM. The sample size, race, countries, patient populations, and depression assessment criteria might have also contributed to such differences. In addition, DM-PTB patients with a monthly income below 5000 yuan were more susceptible to depression, presumably due to the increased mental stress caused by heavy economic burdens and loss of working abilities.
Nutritional status is a significant risk factor for the development of depression in DM-PTB patients. The mean BMI in the depression group was significantly lower than that in the control group. Furthermore, higher percentages of DM-PTB patients in the depression group suffered from mild, moderate, or severe thinness than in the control group. The results of the present study indicate that undernutrition enhances the impact of Tuberculosis-Depression Syndemic and even exacerbates it. We found that the ratio of patients at nutritional risk (NRS2002 ≥ 3) DM-PTB within the depression group was 71.86% and that NRS2002 ≥ 3 was a risk factor for depression. While the symptoms of undernutrition and psychological distress may overlap,22 depression and undernutrition may be closely associated due to the following reasons: (1) depression and other adverse emotions may lead to loss of appetite and digestive dysfunction, resulting in decreased protein and energy intake; (2) continuous mental stimulation may lead to severe vegetative nerve dysfunction and endocrine imbalance, inhibiting the absorption of nutrients; and (3) depression itself may increase catabolism to promote protein decomposition and reduce protein synthesis, further worsening the nutritional status. These synergistic effects between depression and undernutrition may be intensified in DM-PTB patients, who are already in urgent need for nutrients for the provision of normal immune response. Hence, even worse clinical outcomes and treatment difficulties can occur. In addition, we identified that physical function is a protective factor and social function is a risk factor for depression, highlighting the need for proper physical exercise and mental health care for DM-PTB patients for depression prevention. This study also established that DM-PTB patients with high levels of GPT and GOT were more likely to develop depression. The presence of high GPT and GOT levels of in the blood may indicate liver damage, which is potentially caused by hepatoxic anti-tuberculous agents such as rifampicin and isoniazid. This liver damage may slow down the clearance of other metabolites from the blood, increasing the risk of depression development. Meanwhile, liver damage may also induce chest pain and other discomforts that increase the patients’ mental stress and thus enhance the risk of depression.23 While further studies are required to validate the potential aforementioned associations, it is clear that DM-PTB patients can easily fall into a vicious circle, in which their quality of life, economic status, mental stress, and health condition may adversely affect each other.
Certain limitations of this study are to be acknowledged. First, we included only a limited number of DM-PTB patients admitted to one hospital in a period of five months within the same year. The relatively small sample size, single-centered study design, and short data collection period might have introduced biases in our results. The effects of treatment during this period might have also been neglected. Second, a more comprehensive prospective study is thus required to validate the risk factors of depression in DM-PTB patients. Third, the monthly income and socio-economic status may be confounding factors between nutritional status and depression. In addition, limited by the nature of cross-sectional design, though we indicated that most DM-PTB patients underwent depression, the causal relationship between diabetes and depression in TB patients could not be determined. Since we only included DM-PTB patients, the comparison of patients with similarly poor nutrition with diabetes and TB combined and those with just TB could not be achieved. Moreover, we could not determine if the diabetes worsens nutrition and this is the mechanism for the worsening depression. In the future, a prospective case-control study with large sample size is needed to validate the findings in the present study.
In conclusion, depression frequently occurs in DM-PTB patients. For depression prevention, a comprehensive care plan (such as nutrition management, mental counselling, and social support) is necessary in DM-PTB patients. However, further studies are needed to validate the findings of the present study.
Abbreviations
DM-PTB, Diabetes mellitus and pulmonary tuberculosis; PHQ-9, Patient Health Questionnaire–9; NRS2002, Nutritional Risk Screening 2002; QLICD-PT, Quality of Life Instruments for Chronic Diseases-Pulmonary Tuberculosis; BMI, Body mass index; GPTL, Glutamic pyruvic transaminase; GOT, Glutamic oxaloacetic transaminase; CI, Confidence interval; PTB, Pulmonary tuberculosis; DM, Diabetes mellitus; HIV, Human immunodeficiency virus; QOL, Quality of life; Hb, Hemoglobin; ALB, Albumin.
Data Sharing Statement
The data generated in this study are available within the article and its Supplementary File.
Ethics Approval and Consent to Participate
This study was approved by the Ethics Committee of Shanghai Pulmonary Hospital Affiliated to Tongji University (No. K19-146). Informed consent was obtained from all patients (or subjects). This study complies with the Declaration of Helsinki.
Consent for Publication
Written informed consent to publish this information was obtained from the participant.
Acknowledgments
Xiucai Li and Xuee Fang are co-first authors for this study.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas: took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by the Project of Key Medical Discipline of Pudong Hospital of Fudan University (Zdxk2020-18011), Project of Key Medical Specialty and Treatment Center of Pudong Hospital of Fudan University (Zdzk2020-24).
Disclosure
The authors declare that they have no conflicts of interest in this work.
References
1. Luies L, Du Preez I. The echo of pulmonary tuberculosis: mechanisms of clinical symptoms and other disease-induced systemic complications. Clin Microbiol Rev. 2020;33(4):e00036–00020. doi:10.1128/CMR.00036-20
2. Tomic D, Shaw JE, Magliano DJ. The burden and risks of emerging complications of diabetes mellitus. Nat Rev Endocrinol. 2022;18(9):525–539. doi:10.1038/s41574-022-00690-7
3. Guo S, Lei S, Li J, Li L, Chen H, Chongsuvivatwong V. Gradient association between pulmonary tuberculosis and diabetes mellitus among households with a tuberculosis case: a contact tracing-based study. Sci Rep. 2022;12(1):1854. doi:10.1038/s41598-022-05417-2
4. Pachi A, Bratis D, Moussas G, Tselebis A. Psychiatric morbidity and other factors affecting treatment adherence in pulmonary tuberculosis patients. Tuberc Res Treat. 2013;2013:1–37. doi:10.1155/2013/489865
5. Dos Santos APC, Lazzari TK, Silva DR. Health-related quality of life, depression and anxiety in hospitalized patients with tuberculosis. Tuberc Respir Dis. 2017;80(1):69–76. doi:10.4046/trd.2017.80.1.69
6. Kastien-Hilka T, Rosenkranz B, Sinanovic E, Bennett B, Schwenkglenks M. Health-related quality of life in South African patients with pulmonary tuberculosis. PLoS One. 2017;12(4):e0174605. doi:10.1371/journal.pone.0174605
7. Aggarwal AN. Quality of life with tuberculosis. J Clin Tuberc Other Mycobact Dis. 2019;17:100121. doi:10.1016/j.jctube.2019.100121
8. Bauer M, Leavens A, Schwartzman K. A systematic review and meta-analysis of the impact of tuberculosis on health-related quality of life. Qual Life Res. 2013;22:2213–2235. doi:10.1007/s11136-012-0329-x
9. Shrestha SK, Joshi S, Bhattarai RB, et al. Prevalence and risk factors of depression in patients with drug-resistant tuberculosis in Nepal: a cross-sectional study. J Clin Tuberc Other Mycobact Dis. 2020;21:100200. doi:10.1016/j.jctube.2020.100200
10. Lin Y, Harries AD, Kumar AMV, et al. Tackling diabetes mellitus and tuberculosis: a new Union guide on the management of diabetes-tuberculosis. Int J Tuberc Lung Dis. 2019;23(7):771–772. doi:10.5588/ijtld.19.0119
11. Feleke BE, Feleke TE, Biadglegne F. Nutritional status of tuberculosis patients, a comparative cross-sectional study. BMC Pulm Med. 2019;19:1–9.
12. World Health Organization. Nutrition Landscape Information System (NLIS) Country Profile Indicators: Interpretation Guide. World Health Organization; 2019.
13. Masumoto S, Yamamoto T, Ohkado A, Yoshimatsu S, Querri AG, Kamiya Y. Prevalence and associated factors of depressive state among pulmonary tuberculosis patients in Manila, The Philippines. Int J Tuberc Lung Dis. 2014;18(2):174–179. doi:10.5588/ijtld.13.0335
14. Arrieta J, Aguerrebere M, Raviola G, et al. Validity and utility of the Patient Health Questionnaire (PHQ)‐2 and PHQ‐9 for screening and diagnosis of depression in rural Chiapas, Mexico: a cross‐sectional study. J Clin Psychol. 2017;73(9):1076–1090. doi:10.1002/jclp.22390
15. Kroenke K, Spitzer RL, Williams JB. The PHQ‐9: validity of a brief depression severity measure. J Gen Intern Med. 2001;16(9):606–613. doi:10.1046/j.1525-1497.2001.016009606.x
16. Sun Y, Yang Z, Wan C, et al. Development and validation of the pulmonary tuberculosis scale of the system of Quality of Life Instruments for Chronic Diseases (QLICD-PT). Health Qual Life Outcomes. 2018;16:1–10. doi:10.1186/s12955-018-0960-5
17. Ige OM, Lasebikan VO. Prevalence of depression in tuberculosis patients in comparison with non-tuberculosis family contacts visiting the DOTS clinic in a Nigerian tertiary care hospital and its correlation with disease pattern. Ment Health Fam Med. 2011;8(4):235.
18. Kehbila J, Ekabe CJ, Aminde LN, Noubiap JJN, Fon PN, Monekosso GL. Prevalence and correlates of depressive symptoms in adult patients with pulmonary tuberculosis in the Southwest Region of Cameroon. Infect Dis Poverty. 2016;5(1):1–8. doi:10.1186/s40249-016-0145-6
19. Rizvi N, Rizvi N. Frequency of depression and anxiety among tuberculosis patients. J Tuberc Res. 2016;4(04):183. doi:10.4236/jtr.2016.44021
20. Dasa TT, Roba AA, Weldegebreal F, et al. Prevalence and associated factors of depression among tuberculosis patients in Eastern Ethiopia. BMC Psychiatry. 2019;19:1–7. doi:10.1186/s12888-019-2042-6
21. Wang X-B, X-l L, Zhang Q, et al. A survey of anxiety and depressive symptoms in pulmonary tuberculosis patients with and without tracheobronchial tuberculosis. Front Psychiatry. 2018;9:308. doi:10.3389/fpsyt.2018.00308
22. Ma L, Poulin P, Feldstain A, Chasen M. The association between malnutrition and psychological distress in patients with advanced head-and-neck cancer. Current Oncol. 2013;20(6):554–560. doi:10.3747/co.20.1651
23. Chang R-Y, SH-H H, Tsai H-L, Koo M. Association of anxiety and depression with chronic liver diseases in patients with noncardiac chest pain: a cross-sectional study. Medicine. 2022;101(31):e29620. doi:10.1097/MD.0000000000029620
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Depression, Diabetes Mellitus and Mortality in Older Adults: A National Cohort Study in Taiwan
Chen VCH, Wang TN, Hsieh MC, Chou SY, Lee MC, McIntyre RS, Lu ML, Liao YT, Yeh CJ
Neuropsychiatric Disease and Treatment 2022, 18:2639-2648
Published Date: 10 November 2022
Influencing Factors of Treatment Outcomes Among Patients with Pulmonary Tuberculosis: A Structural Equation Model Approach
Liu K, Zhang M, Luo D, Zheng Y, Shen Z, Chen B, Jiang J
Psychology Research and Behavior Management 2023, 16:2989-2999
Published Date: 4 August 2023
Anxiety and Depression in People with Eczema or Psoriasis: A Comparison of Associations in UK Biobank and Linked Primary Care Data
Matthewman J, Mansfield KE, Hayes JF, Adesanya EI, Smith CH, Roberts A, Langan SM, Henderson AD
Clinical Epidemiology 2023, 15:891-899
Published Date: 7 August 2023
Prevalence and Determinants of Anxiety and Depression Among Healthcare Workers in Liaoning Province, China
Lu J, Dou X, Yi Y, Yu Y, Zhou L
Risk Management and Healthcare Policy 2024, 17:983-993
Published Date: 23 April 2024
Prevalence of Depression Among Women Using Hormonal Contraceptives in Mogadishu, Somalia: A Cross-Sectional Study
Yusuf AM, Warsame MO, Gedi S, Abdullahi NA, Ahmed DI
Open Access Journal of Contraception 2024, 15:89-98
Published Date: 19 June 2024