Back to Journals » International Journal of General Medicine » Volume 15
Prevalence and Factors Associated with BRCA1/2 Gene Mutation in Chinese Populations with Breast Cancer
Authors Huang G, Lu H, Chen Q, Huang X
Received 15 June 2022
Accepted for publication 15 August 2022
Published 24 August 2022 Volume 2022:15 Pages 6783—6789
DOI https://doi.org/10.2147/IJGM.S378706
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Guoding Huang, Hongquan Lu, Qizhu Chen, Xinting Huang
Department of Oncology, The Central Hospital of Western Area of Hainan, Danzhou, Hainan, People’s Republic of China
Correspondence: Guoding Huang, Department of Oncology, The Central Hospital of Western Area of Hainan, Danzhou, Hainan, People’s Republic of China, Tel +86-898-23836851, Fax +86-898-23836853, Email [email protected]
Objective: We aimed to evaluate the prevalence of BRCA1 and BRCA2 mutations in Chinese populations with breast cancer. Factors associated with BRCA1 and BRCA2 mutations are also evaluated.
Methods: This was a cross-sectional study, and patients with breast cancer were included. Data on clinical characteristics, information of breast cancer, and BRCA1 and BRCA2 mutations were extracted. Patients were divided into the carrier and noncarrier groups.
Results: A total of 368 patients were included. Compared to the noncarrier group (n = 240), patients in the carrier group (n = 128) were younger and more likely to have breast cancer at age < 40 years. Of the overall 128 patients in the carrier groups, 58 had BRCA1 mutation and 70 had BRCA2 mutation. Among patients with early onset breast cancer, there was no difference in the prevalence of BRCA1 and BRCA2 (20.7% vs 17.1%, P = 0.35). While among patients with a family history of breast/ovarian cancer, BRCA2 mutation was more prevalent than BRCA1 mutation (54.3% vs 44.8%, P = 0.01); and among patients with triple-negative breast cancer, BRCA1 mutation was more prevalent than BRCA2 mutation (34.5% vs 28.6%, P = 0.04). After adjusting for covariates, factors associated with BRCA1 mutation included breast cancer diagnosed < 40 years, tumor size > 2 cm, and lymph node metastasis; and after adjusting for covariates, factors associated with BRCA2 mutation included age, tumor size > 2 cm, and triple-negative breast cancer.
Conclusion: The prevalence of BRCA1 and BRCA2 mutations varied according to three specific subgroups. Factors associated with BRCA1 and BRCA2 mutations were differential.
Keywords: breast cancer, prevalence, predictors, breast cancer-associated gene
Introduction
Breast cancer is the most common cancer in women globally. Several recent studies have demonstrated that breast cancer accounts for approximately 25% of the overall new-onset cancers worldwide.1–3 Furthermore, approximately 15% of cancer-related mortality were attributed to breast cancer.1–3 Germline mutation is the major risk factor for breast cancer, which accounts for 5–10% of the overall breast cancer.4,5 Prior studies from western populations have demonstrated that approximately 20–40% of inherited breast cancers are mainly due to the deleterious mutation of the breast cancer-associated gene (BRCA), namely, BRCA1 and BRCA2.6–8 A recent meta-analysis further shows that individuals with BRCA1 and BRCA2 carriers have 57–65% and 45–49% probability of developing breast cancer over lifetime, respectively.9 Therefore, it is clinically important to screen for BRCA1 and BRCA2 genes in individuals who are at a heightened risk of developing breast cancer.
Among individuals who have a family history of breast cancer, or who had breast cancer at a young age, or who had a triple-negative phenotype of breast cancer, the probability of positive test of BRCA1 and BRCA2 mutations is high.10,11 Nevertheless, most of these findings are predominantly derived from the western populations, and the data on the Chinese populations are limited. One prior study has reported the prevalence of BRCA1 and BRCA2 germline mutations in high-risk breast cancer patients of Chinese Han nationality, and the results suggest that there may be some degree of shared ancestry for the two recurrent BRCA1 mutations in Chinese.12 Deng et al evaluated the prevalence and clinical outcomes of germline mutations in BRCA1/2 genes in 2769 unselected breast cancer patients in China. The results demonstrate that BRCA1 mutation status may be associated with a worse disease progression in patients with breast cancer.13 Recently, one meta-analysis reported BRCA1 and BRCA2 mutations in Chinese patients with breast and ovarian cancer, suggesting a lower prevalence than western populations.14 Another study reported the prevalence of BRCA1 and BRCA2 mutations in Chinese Han populations with breast cancer, and these findings also suggested a lower prevalence of these gene mutations than western populations.15 It has been well documented that the genetic mutations vary significantly among different racial/ethnic groups. Therefore, it is needed to evaluate the prevalence of BRCA1 and BRCA2 mutations in Chinese populations with breast cancer, given the increased breast cancer burden in China.16,17 In addition, the factors to predict the probability of BRCA1 and BRCA2 mutations are also needed to elucidate, which can inform the strategy to screen for breast cancer and BRCA mutation.
Herein, we performed a cross-sectional study to investigate the prevalence of BRCA1 and BRCA2 mutations in individuals with documented breast cancer. In addition, the factors associated with the prevalent BRCA1 and BRCA2 mutations would also be evaluated.
Methods
Study Design and Participants
This was a cross-sectional study, which was conducted from July 2019 to July 2021. The current study was approved by the Clinical Research Ethics Committee of Central Western Hospital of Hainan (No.20190308R1). All procedures were performed in accordance with the Helsinki Declaration. Participants with documented breast cancer hospitalized in our hospital were screened for and included after written informed consent was obtained.
Data Collection
Age and menopausal status when breast cancer was diagnosed, family history of breast or ovarian cancer, risk factors and comorbidities, medical therapy, and information of the breast cancer including tumor size, lymph nodes status, grade, histological features, and estrogen receptor status were collected from the electronic health record by two independent investigators. Fasting venous blood was used to evaluate hemoglobin concentration, and renal and liver function.
BRCA1/2 Germline Mutation Assessment
Plasma was separated from blood samples collected in EDTA-treated tubes and then was transferred into fresh tubes by centrifugation to remove cell debris, aliquoted into fresh tubes, and stored at −80°C until DNA extraction. Breast cancer tissue samples were obtained by biopsy and processed into formalin-fixed paraffin-embedded cell blocks. Cell-free DNA (cfDNA) and genomic DNA were isolated from plasma and were analyzed for the mutations of BRCA1 and BRCA2 genes as previously described.18
Statistical Analysis
Continuous variables were presented as mean and standard deviation, and categorical variables were presented as number and proportion. The prevalence of BRCA1 and BRCA2 mutations was determined as the proportion of mutation-positive participants among all included participants. We compared demographic and clinical features between BRCA carriers and noncarriers with the use of Student’s t-test, Mann–Whitney test, the chi-square test, or the Fisher’s exact test as appropriate. Several subgroups (early-age onset breast cancer, family history of breast/ovarian cancer, and triple-negative breast cancer) were performed to compare the prevalence of BRCA1 and BRCA2 mutation within each subgroup. Univariate and multivariable regression analysis was performed to evaluate the factors associated with BRCA1 and BRCA2 mutations, respectively. A two-sided P-value <0.05 was considered to be statistically significant and all the analysis was performed using SPSS 22.0 software package.
Results
General Characteristics
During the study period, a total of 368 participants with breast cancer were included in the current study, and study flowchart is shown in Figure 1. General characteristics are presented in Table 1. Compared to the noncarrier group, patients in the carrier group were younger, and more likely to have breast cancer at age <40 years and prior to post-menopause. In addition, they were more likely to have a positive family history, have tumor size >2 cm, lymph node metastasis, grade III, and triple-negative breast cancer. There was no difference in histological diagnosis between these two groups.
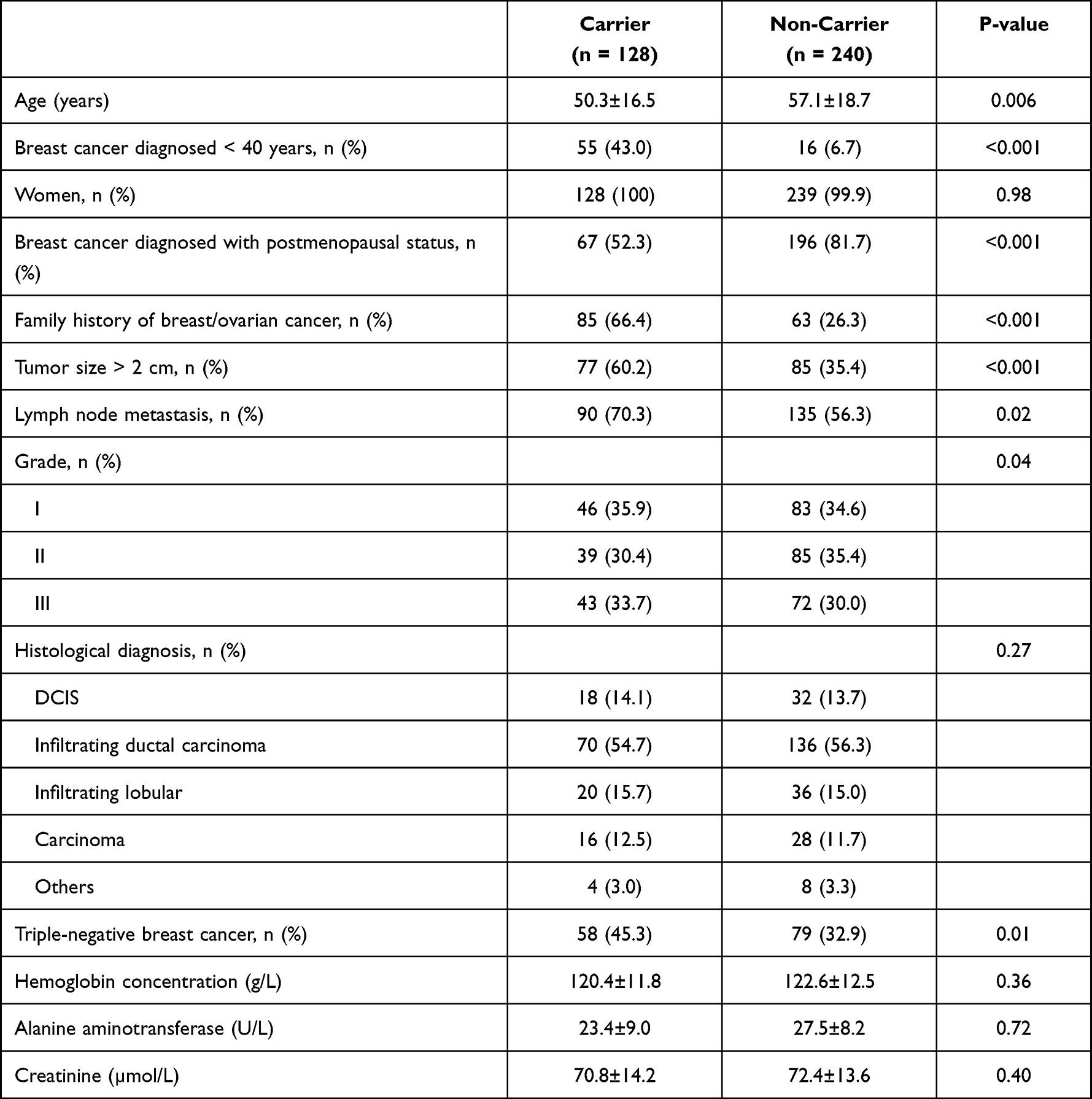 |
Table 1 General Characteristics |
 |
Figure 1 Study flowchart. |
Prevalence of BRCA1 and BRAC2 Gene Mutation in Subgroup Populations
Of the overall 128 patients in the carrier groups, 58 had BRCA1 gene mutation and 70 had BRCA2 gene mutation. In specific, among the 58 BRCA1 gene mutations, 24 (41.4%) were base substitution, 16 (27.6%) were nucleotide insertion, and 18 (31.0%) were nucleotide deletion. Among the 70 BRCA2 gene mutations, 32 (45.7%) were base substitution, 20 (28.6%) were nucleotide insertion, and 18 (25.7%) were nucleotide deletion. As shown in Figure 2, among patients with early onset breast cancer, there was no difference in the prevalence of BRCA1 and BRCA2 (20.7% vs 17.1%, P = 0.35). While among patients with a family history of breast/ovarian cancer, BRCA2 gene mutation was more prevalent than BRCA1 gene mutation (54.3% vs 44.8%, P = 0.01); and among patients with triple-negative breast cancer, BRCA1 gene mutation was more prevalent than BRCA2 gene mutation (34.5% vs 28.6%, P = 0.04).
 |
Figure 2 Prevalence of BRCA1 and BRCA2 gene mutation. |
Factors Associated with BRCA1 and BRCA2 Gene Mutations
As presented in Table 2, in the univariate analysis, factors associated with BRCA1 gene mutation included breast cancer diagnosed <40 years, family history of breast/ovarian cancer, tumor size >2 cm, lymph node metastasis, and triple-negative breast cancer; after adjusted for covariates, factors associated with BRCA1 gene mutation included breast cancer diagnosed <40 years, tumor size >2 cm, and lymph node metastasis. As presented in Table 3, in the univariate analysis, factors associated with BRCA2 gene mutation included age, breast cancer diagnosed <40 years, family history of breast/ovarian cancer, tumor size >2 cm, and triple-negative breast cancer; after adjusted for covariates, factors associated with BRCA2 gene mutation included age, tumor size >2 cm, and triple-negative breast cancer.
 |
Table 2 Factors Associated with BRCA1 Gene Mutation |
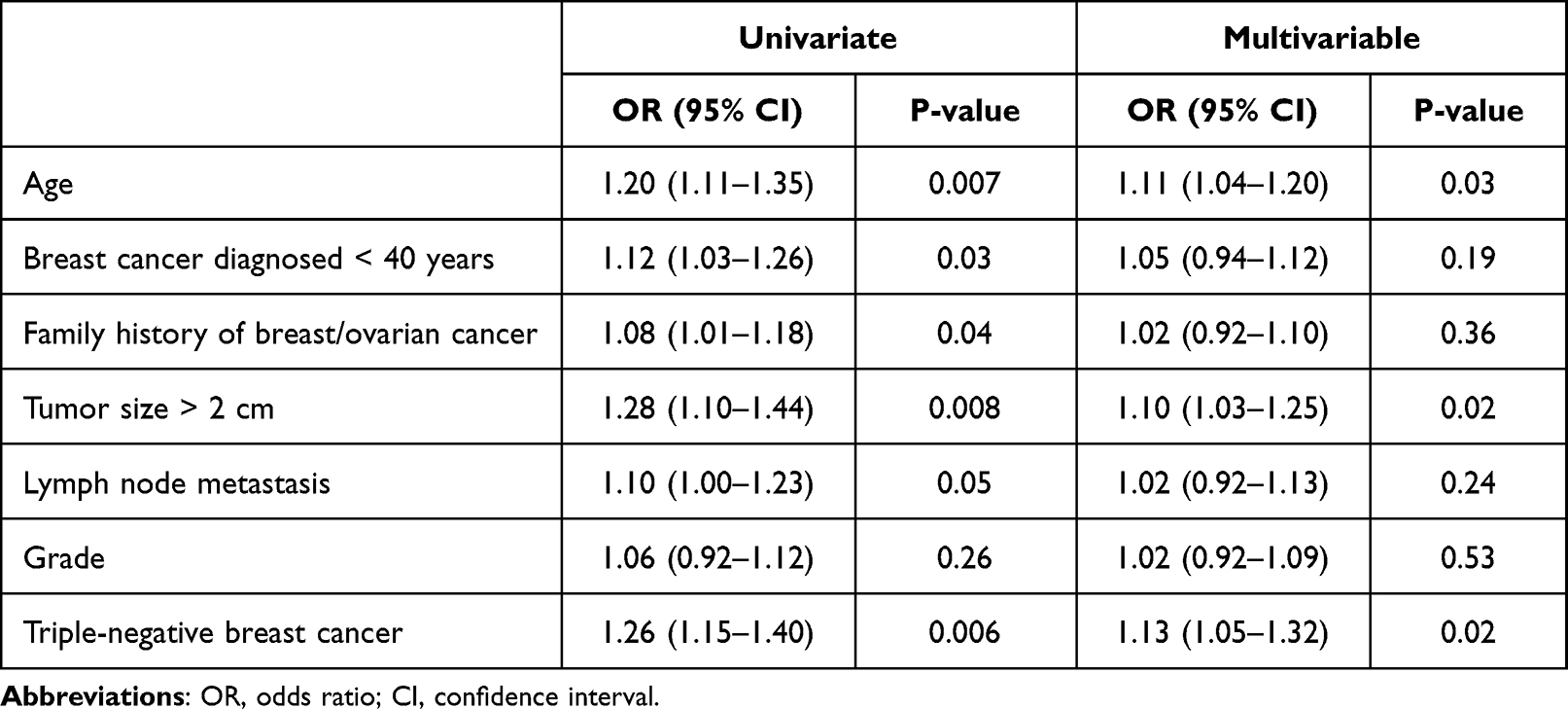 |
Table 3 Factors Associated with BRCA2 Gene Mutation |
Discussion
To the best of our knowledge, the current study should be the first few studies in evaluating the prevalence of BRCA1 and BRCA2 gene mutations among Chinese patients with breast cancer. In addition, factors associated with BRCA1 and BRCA2 gene mutations were also identified. There are three major findings. First, compared to breast cancer patients without BRCA1 and BRCA2 gene mutations, patients with these mutations have differential clinical and pathological characteristics. Second, among three specific subgroups, the prevalence of BRCA1 and BRCA2 gene mutations was significantly different. Third, factors differentially associated with BRCA1 and BRCA2 gene mutations were also identified. Their findings might provide a foundation to screen for BRCA gene mutation and guide prevention strategies for patients who are at risk for breast cancer in the future.
It has been well demonstrated that BRCA1 and BRCA2 gene mutations are independent risk factors for breast cancer. Studies of Western Europe and North American populations suggest that patients with breast cancer and BRCA gene mutations display differential clinical characteristics when compared to their counterparts without gene mutations, suggesting that BRCA1 and BRCA2 might be associated with unique clinical phenotype of breast cancer. Interestingly, in this study, we also found that compared to the non-carriers, patients in the carrier group were younger, and more likely to have breast cancer at age <40 years and before post-menopause. These findings underscore that BRCA1 and BRCA2 mutations might cause early-onset breast cancer. In addition, they were more likely to have a positive family history, have tumor size >2 cm, lymph node metastasis, grade III, and triple-negative breast cancer. These pathological findings provide important foundations to explain the early-onset breast cancer and the worst prognosis in patients with BRCA1 and BRCA2 gene mutations.
Interestingly and importantly, it is noted that among three specific subgroups, the prevalence of BRCA1 and BRCA2 gene mutations was significantly different. Specifically, among patients with early-onset breast cancer, there was no difference in the prevalence of BRCA1 and BRCA2 gene mutations. While among patients with a family history of breast/ovarian cancer, BRCA2 gene mutation was more prevalent than BRCA1 gene mutation; and among patients with triple-negative breast cancer, BRCA1 gene mutation was more prevalent than BRCA2 gene mutation, which was somewhat consistent with prior reports. These findings could have important clinical implications. First, it seems that both BRCA1 and BRCA2 gene mutations were associated with early-onset breast cancer, suggesting that screening for either mutation can be helpful to screen for those at high risk of developing breast cancer at an early age. Second, compared to BRCA1 gene mutation, BRCA2 gene mutation might be more closely related to patients with a positive family history, suggesting that it should be routinely screened for breast cancer in patients with BRCA2 gene mutation. Third, compared to BRCA2 gene mutation, BRCA1 gene mutation was more likely to be present in patients with triple-negative breast cancer. These findings highlight that BRCA1 gene mutation might exert a differential effect on the development of the triple-negative breast cancer. Further studies are needed to evaluate whether targeting BRCA1 gene mutation could provide additional benefits to these populations.
Extending prior studies, we also explored factors associated with BRCA1 and BRCA2 gene mutations. The findings suggest that there were differential associations between factors associated with BRCA1 and BRCA2 gene mutations. Specifically, after multivariable analysis, factors associated with BRCA1 gene mutation included breast cancer diagnosed <40 years, tumor size >2 cm, and lymph node metastasis, while factors associated with BRCA2 gene mutation included age, tumor size >2 cm, and triple-negative breast cancer. These findings once again support the concept that patients with BRCA1 and BRCA2 gene mutation might present with differential clinical phenotypes. In addition, these findings also suggest that among breast cancer patients with these factors might be more likely to have BRCA1 and BRCA2 gene mutations, respectively.
There are some limitations of this study. First, we only included the Chinese patients, and these findings might not be extrapolated to other racial/ethnic groups. Second, this was a cross-sectional study and whether the presence of BRCA1 and BRCA2 gene mutations was associated with worse clinical outcomes was unknown. Third, although we have adjusted for covariates, other factors which might also be associated with BRCA1 and BRCA2 gene mutations could also exist. Last but not the least, we did not follow-up on the outcome of these patients, and therefore we cannot evaluate the prognostic implication of BRCA1 and BRCA2 gene mutations in Chinese patients with breast cancer.
Conclusion
In conclusion, this study suggests that patients with BRCA1 and BRCA2 gene mutations have differential clinical and pathological characteristics, and the prevalence of BRCA1 and BRCA2 gene mutations varied according to the three specific subgroups. Furthermore, factors associated with BRCA1 and BRCA2 gene mutations were differential. Their findings provide a foundation to screen for BRCA gene mutation and guide prevention strategies for patients who are at risk for breast cancer in the future.
Acknowledgment
We appreciate the staff that supported this study very much.
Funding
This study was supported by the Hainan Medical Research Grant (No. 2005320672A2001).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Katsura C, Ogunmwonyi I, Kankam HK, Saha S. Breast cancer: presentation, investigation and management. Br J Hosp Med. 2022;83:1–7. doi:10.12968/hmed.2021.0459
2. Green VL. Breast cancer risk assessment and management of the high-risk patient. Obstet Gynecol Clin North Am. 2022;49:87–116. doi:10.1016/j.ogc.2021.11.009
3. Nassif AB, Talib MA, Nasir Q, Afadar Y, Elgendy O. Breast cancer detection using artificial intelligence techniques: a systematic literature review. Artif Intell Med. 2022;127:102276. doi:10.1016/j.artmed.2022.102276
4. Mavaddat N, Dorling L, Carvalho S, et al. Pathology of tumors associated with pathogenic germline variants in 9 breast cancer susceptibility genes. JAMA Oncol. 2022;8:e216744. doi:10.1001/jamaoncol.2021.6744
5. Kashyap D, Pal D, Sharma R, et al. Global increase in breast cancer incidence: risk factors and preventive measures. Biomed Res Int. 2022;2022:9605439. doi:10.1155/2022/9605439
6. Filippini SE, Vega A. Breast cancer genes: beyond BRCA1 and BRCA2. Front Biosci. 2013;18:1358–1372. doi:10.2741/4185
7. Saleem M, Ghazali MB, Wahab M, et al. The BRCA1 and BRCA2 genes in early-onset breast cancer patients. Adv Exp Med Biol. 2020;1292:1–12. doi:10.1007/5584_2018_147
8. Chen B, Zhang G, Li X, et al. Comparison of BRCA versus non-BRCA germline mutations and associated somatic mutation profiles in patients with unselected breast cancer. Aging. 2020;12:3140–3155.
9. Petrucelli N, Daly MB, Pal T. BRCA1- and BRCA2-associated hereditary breast and ovarian cancer. In: Adam MP, Mirzaa GM, Pagon RA, et al., editors. GeneReviews(®). Seattle: University of Washington, Seattle Copyright © 1993–2022, University of Washington, Seattle; GeneReviews is a registered trademark of the University of Washington, Seattle. All rights reserved. 1993.
10. Lang GT, Shi JX, Hu X, et al. The spectrum of BRCA mutations and characteristics of BRCA-associated breast cancers in China: screening of 2991 patients and 1043 controls by next-generation sequencing. Int J Cancer. 2017;141:129–142. doi:10.1002/ijc.30692
11. Warner E. Screening BRCA1 and BRCA2 mutation carriers for breast cancer. Cancers. 2018;10. doi:10.3390/cancers10120477
12. Li WF, Hu Z, Rao NY, et al. The prevalence of BRCA1 and BRCA2 germline mutations in high-risk breast cancer patients of Chinese Han nationality: two recurrent mutations were identified. Breast Cancer Res Treat. 2008;110:99–109. doi:10.1007/s10549-007-9708-3
13. Deng M, Chen HH, Zhu X, et al. Prevalence and clinical outcomes of germline mutations in BRCA1/2 and PALB2 genes in 2769 unselected breast cancer patients in China. Int J Cancer. 2019;145:1517–1528. doi:10.1002/ijc.32184
14. Gao X, Nan X, Liu Y, et al. Comprehensive profiling of BRCA1 and BRCA2 variants in breast and ovarian cancer in Chinese patients. Hum Mutat. 2020;41:696–708. doi:10.1002/humu.23965
15. Dong H, Chandratre K, Qin Y, et al. Prevalence of BRCA1/BRCA2 pathogenic variation in Chinese Han population. J Med Genet. 2021;58:565–569. doi:10.1136/jmedgenet-2020-106970
16. Fan L, Strasser-Weippl K, Li JJ, et al. Breast cancer in China. Lancet Oncol. 2014;15:e279–89. doi:10.1016/S1470-2045(13)70567-9
17. Li T, Mello-Thoms C, Brennan PC. Descriptive epidemiology of breast cancer in China: incidence, mortality, survival and prevalence. Breast Cancer Res Treat. 2016;159:395–406. doi:10.1007/s10549-016-3947-0
18. Kim EK, Park SY, Kim SW. Clinicopathological characteristics of BRCA-associated breast cancer in Asian patients. J Pathol Transl Med. 2020;54:265–275. doi:10.4132/jptm.2020.04.07
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Breast Cancer Awareness Among Medical Students, University of Bisha, Saudi Arabia
Miskeen E, Al-Shahrani AM
Breast Cancer: Targets and Therapy 2023, 15:271-279
Published Date: 17 April 2023
Predictors of Tuberculosis and Non-Communicable Disease Comorbidities Among Newly Enrolled Tuberculosis Patients, Southern Ethiopia
Nunemo MH, Gidebo KD, Woticha EW, Lemu YK
Integrated Blood Pressure Control 2023, 16:95-109
Published Date: 22 November 2023
Predictive Models of Psychological Distress, Quality of Life, and Adherence to Medication in Breast Cancer Patients: A Scoping Review
Pezzolato M, Spada GE, Fragale E, Cutica I, Masiero M, Marzorati C, Pravettoni G
Patient Preference and Adherence 2023, 17:3461-3473
Published Date: 19 December 2023
Analysis of Cardiotoxicity and Risk Factors of Breast Cancer Chemotherapy Drugs: A Five-Year Single-Centre Retrospective Study in Early Breast Cancer
Ju F, Gu H, Yu L, Zhao G, Liu Y, Yin D, Niu J, Xue T, Yin C, Jiao L, Li C, Wu J, Ji Y
Drug Design, Development and Therapy 2025, 19:6505-6517
Published Date: 30 July 2025