")
Back to Journals » Journal of Pain Research » Volume 16
Prevalence and Associated Factors of Ankle-Foot Pain Among Nurses Working in Surgical Units of Comprehensive Specialized Hospitals in Amhara Regional State, Northwest Ethiopia, 2022
Authors Tamir Tsehay Y , Lamesgin Endalew H, Dessalegn Bogale A, Walle TA
Received 22 February 2023
Accepted for publication 27 July 2023
Published 2 August 2023 Volume 2023:16 Pages 2685—2696
DOI https://doi.org/10.2147/JPR.S405417
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Alaa Abd-Elsayed
Video abstract of "Ankle-foot pain among nurses" [ID 405417].
Views: 32
Yeshimebet Tamir Tsehay,1 Helen Lamesgin Endalew,2 Alemwork Dessalegn Bogale,1 Tarkie Abebe Walle2
1Department of Surgical Nursing, School of Health Science, College of Medicine and Health Science, Bahir Dar University, Bahir Dar, Ethiopia; 2Department of Surgical Nursing, School of Nursing, College of Medicine and Health Science, University of Gondar, Gondar, Ethiopia
Correspondence: Yeshimebet Tamir Tsehay, Department of Surgical Nursing, School of Health Science, College of Medicine and Health Science, Bahir Dar University, PO Box 79, Bahir Dar, Ethiopia, Tel +251943526569, Email [email protected]
Background: Ankle-foot pain is a serious public health concern among nurses and has a significant impact on the quality of the health care service delivery system. However, little is known about the prevalence and factors associated with ankle-foot pain among nurses working in surgical units in Ethiopia.
Purpose: The study aimed to assess the prevalence and associated factors of ankle-foot pain among nurses working in surgical units of comprehensive specialized hospitals in Amhara regional state, Northwest Ethiopia, 2022.
Participants and Methods: An institution-based cross-sectional study was conducted among 409 nurses working in surgical units of comprehensive specialized hospitals, from May 15 to June 7, 2022. A simple random sampling technique was employed. Data were collected by five BSc nurses using a structured self-administered questionnaire. The collected data were entered into Epi-data version 4.6 and exported to SPSS version 23 for analysis. The descriptive statistics and bivariable and multivariable logistic regression analyses were computed. Finally, variables were declared as statistically significant at P < 0.05 using the odds ratio and 95% CI.
Results: The prevalence of ankle-foot pain among nurses working in surgical units was 51.8% (95% CI = 46.9– 57.5). More than 10 years of working experience [AOR = 3.48, 95% CI = 1.35– 8.92], working 48 or more hours per week [AOR = 2.69, 95% CI = 1.27– 6.00], prolonged standing [AOR = 5.72, 95% CI = 3.20– 10.25], high physical job demand [AOR = 2.41, 95% CI = 1.53– 3.80], and low job control [AOR = 2.34, 95% CI = 1.47– 3.71] had statistically significant association with ankle-foot pain.
Conclusion: This study found that ankle-foot pain was common among nurses working in surgical units. Having more years of work experience, working more hours per week, prolonged standing, high physical job demand, and low job control were statistically associated with ankle-foot pain.
Keywords: ankle-foot discomfort, ankle-foot pain, Northwest Ethiopia, nurses
Introduction
Ankle-foot pain is an unpleasant sensory and emotional experience that occurs when any tissue at the distal end of the tibia or fibula, such as bones, ligaments, joints, muscles, tendons, fascia, nerves, skin, and nails sustains an injury.1 Ankle-foot pain can be caused by fracture,2,3 dislocation,4,5 neurovascular compromise, tendon rupture, and other inflammatory disorders such as fasciitis, tendonitis, and synovitis and degenerative disorders: possible consequences of aging or repetitive use or combination of these; such as degenerative arthritis and chronic tendonitis, tenosynovitis, or tendinosis.6 According to the WHO report, work-related musculoskeletal disorders affect 1.71 billion individuals worldwide, as a result, musculoskeletal illnesses severely limit physical mobility and dexterity, resulting in early retirement from work, lower well-being, and a reduced ability to participate in society.7 Based on the American Physical Therapy Association, the most common foot problem is plantar fasciitis, which is a disorder characterized by inflammation and pain to the arched ligament that crosses the lower foot and connects the heel with the base of the toes, and it affects over 2 million Americans per year and up to 10% of the population over their lifetime.8
Nursing is a physically and psychologically demanding job that is responsible for providing different healthcare services to patients.9 Nurses are the healthcare workers vulnerable to ankle-foot pain.10 Ankle-foot pain is common among operating room personnel because they are required to stand in a static position for long surgical procedures.11 Nurses had a high risk of ankle-foot pain as compared to physicians and the general population because nurses are most often remaining in prolonged standing, and walking, and have been exposed to excessive physical activities like lifting and lowering heavy loads.12,13 More than 70,000 hospital nurses in Australia have experienced ankle-foot pain and 25–30,000 hospital nurses have been restricted in their activity due to ankle-foot pain during the last 12 months.14
Nearly two-thirds of nurses working in hospitals in the United States had ankle-foot pain, with 24.8% of them reporting that it interferes with their daily activities.15 A cross-sectional study conducted in south Brazil among nurses working in the orthopedic setting showed that the prevalence of ankle-foot pain was 55.2%.16 Ankle-foot pain was the most common work-related musculoskeletal disorder for surgical workers in Europe, causing 2.4% of nurses to miss work, 1.4% to require hospitalization, 52.9% to have their daily work life negatively impacted, 2.9% to change the workplace, and more than half of nurses to use medication as a result of the problem.17–19 The prevalence of ankle-foot pain among nurses in South Asia over the previous 12 months was 7.6%20 in India and 47.2%21 in Pakistan. Studies conducted in South East Asia indicated that the annual prevalence of ankle-foot pain among nurses was 86.7%,10 47.2%22 in Malaysia, 8.7%23 in Vietnam, and 35.1%24 in Thailand.
According to a study conducted in Japan among nurses working at a university hospital, the prevalence of ankle-foot pain was 23% in the previous month.25 A systematic review and meta-analysis conducted in Iran showed that the global prevalence of ankle-foot pain among operation room personnel was 57.06%.26 Other cross-sectional studies done in South West Asia revealed that the prevalence of ankle-foot pain among operating room nurses in the last 12 months was 55.8%27 and 59%28 in Iran, and 29.7%29 in Iraq.
According to some studies conducted in Africa, the annual prevalence of ankle-foot pain among nurses was 29.7%30 in Uganda, 45.4%31 in Egypt, and 43.7%32 in Ethiopia. As reported by a single-centered study in Ethiopia, ankle-foot discomfort was the most prominent health condition for nurses, with 23.5% of those unable to perform their daily activities as a result of illness.32
Based on studies done globally, age, body mass index, gender, having multiple underlying foot conditions, working area, working hours per week, prolonged standing, working in night shift, lifting and lowering heavy loads, physical and psychological work demand, job control, job stress, and social support were major factors for nurse’s ankle-foot pain.14,15,23,25,27,32–34 So, increasing the number of staff, minimizing working hours, using safety devices to lift and lower objects, and applying ergonomic principles might be the potential interventions to alleviate ankle-foot pain.
The ankle-foot pain has various consequences such as sickness, functional limitation of daily living activities in their working area and their home, leave from work, or non-attendance for work and also affects work performance and productivity.14,16,22,25,27 Musculoskeletal disorders, particularly ankle-foot pain, become the highest among nurses working in the intensive care unit, operation room, and surgical ward,14,32,35 and the second most prevalent work-related musculoskeletal disorders among surgical workers.17
Even though other work-related musculoskeletal disorders such as low back pain among nurses have been reported previously,36 as far as the investigator search, there is limited evidence on the prevalence and associated factors of ankle-foot pain among nurses working in surgical units in Ethiopia. Especially in the study area, the problem is not well understood.
The findings of this study could help healthcare providers better understand ankle-foot pain and the factors associated with it, thus enabling them to maintain their ankle-foot health by applying preventive strategies. Furthermore, the results could be a baseline for future researchers to further investigate related topics. So, the purpose of this study was to determine the prevalence of ankle-foot pain, as well as the factors that contribute to it, among nurses working in surgical units of comprehensive specialized hospitals in Amhara regional state, Northwest Ethiopia.
Materials and Methods
Study Design and Period
An institution-based cross-sectional study was conducted from May 15-June 7, 2022.
Study Area
This study was conducted in comprehensive specialized hospitals in Amhara regional state, Northwest Ethiopia. The Amhara Region is found in the Northwestern part of Ethiopia. There are five comprehensive specialized hospitals in Amhara regional state, Northwest Ethiopia; such as Debre Markos Comprehensive Specialized Hospital (DMCSH), Tibebegion Comprehensive Specialized Hospital (TGCSH), Felege Hiwot Comprehensive Specialized Hospital (FHCSH), University of Gondar Comprehensive Specialized Hospital (UoGCSH), and Debre Tabor Comprehensive Specialized Hospital (DTCSH). These hospitals provide outpatient and inpatient services for more than a population of 22,000,000 million people living in their catchment area.
Based on the hospital administrators’ report, these hospitals have 1733 nurses. Among those 775 nurses are working in surgical units.
Population
All nurses who were working in surgical units of comprehensive specialized hospitals in Amhara regional state, Northwest Ethiopia, and available during the study period were included in this study. Nurses who had less than one year of work experience, recent trauma (a trauma that occurred not long ago), recent surgery (surgery that was done not long ago) due to cases other than work-related disorders, and congenital deformities in the ankle-foot region were excluded from the study.
Sample Size Determination and Sampling Technique
The sample size was determined by using a single population proportion formula with an assumption of a 95% confidence level, a 5% margin of error, and a 43.7% prevalence of ankle-foot pain.32 The sample size was


The sample size for the first objective considering a 10% non-response rate was 416. The sample size for the second objective was calculated by using Statcalc Epi Info software version 7 with an assumption of power 80%, confidence level 95%, and ratio 1 with three statistically significant variables such as: BMI, foot conditions, and working area.32,37 The maximum sample size for the second objective considering a 10% non-response rate was 68. So, the minimum adequate sample size considering a 10% non-response rate was 416.
The required sample was proportionally allocated to each comprehensive specialized hospital and then to each working area/unit. Finally, the study participants were drawn from each stratum/working area using a simple random sampling technique with a lottery method.
Operational Definition
Ankle–foot pain: Having trouble (such as ache, pain, numbness, or any discomfort) in the areas of the ankle-foot region for at least lasting one day in the last 12 months.32
Data Collection Tool and Procedure
The data were collected from nurses who have worked in surgical units of comprehensive specialized hospitals in Amhara Regional State, Northwest Ethiopia, from May 15-June 7, 2022. The data were collected using a structured self-administered questionnaire. The tool was adapted from a Standardized Nordic Questionnaire,38 and a Nationally Standardized Job Content Questionnaire,39 and also from reviewing other relevant literature.25,32
The questionnaire was prepared in the English language. The questionnaire had five parts: the first part consists of the socio-demographic characteristics of respondents with five items, the second part comprises personal factors and contains four items, the third part contains work-related factors with nine items, the fourth part contains psychosocial factors, which were assessed by Job Content Questionnaire using a 4-point Likert scale.39 This includes the psychological job demand, which consists of seven items, including “working very fast, working very hard, the job requires excessive amount of work, the job requires enough time to get the job done, conflicting demands, long periods of intense concentration on the task, and hecticness”, which were measured using the 4-point Likert scale (1–4), where 1 represents “never” and 4 represents “often”; the physical job demand with seven items, job stress with eight items, social support with eight items, job control with eight items and the fifth part consists of ankle-foot pain-related questions, which was measured by yes/no response. Five BSC nurses and three MSC nurses were selected for data collection and supervision, respectively. The purpose of the study and the input of the result were informed.
Data Quality Control
The data collectors and supervisors were trained one day before the actual data collection period regarding the purpose of the study, the nature of the data collection tool, and how to approach the study participants. Pretest was conducted on 5% of the sample size by taking 21 nurses working in surgical units at Dessie comprehensive specialized hospital. The completeness and consistency of data were ensured by the supervisors before leaving the study area. Immediately at the end of each data collection day, the data collected from each respondent was checked for completeness, clarity, and consistency by the principal investigator before the data were entered into computer software. The internal consistency of the tool used for measuring psychosocial factors by Cronbach’s alpha was 0.89. The face validity of the tool was checked.
Data Processing and Analysis
The collected data were checked, coded, and entered into Epi-data version 4.6 and exported to the IBM SPSS version 23 of statistical software for analysis. The statistical analysis was performed by the corresponding author. Data were cleaned by running the frequency of each variable and using the respondent’s ID to identify the records with missing values and to ensure completeness. Descriptive statistics were computed to determine the frequency and percentage of categorical variables and also to determine the mean with standard deviations of continuous variables.
The results of the analysis were presented with text, tables, and charts. Moreover, the chi-square test was used to determine the association between dependent and independent variables. A binary logistic regression model was computed. Further, multicollinearity was checked by the Variance Inflation Factor (VIF) (the maximum value was 2.004) and Tolerance (the minimum value was 49.9%). Model fitness was checked by the Hosmer and Lemeshow goodness-of-fit test with a p-value of 0.94. Bivariable and multivariable logistic regression analyses were computed. In multivariable logistic regression analysis with a backward stepwise variable selection method, variables were declared as statistically significant at p < 0.05 using the odds ratio and 95% CI.
Results
Socio-Demographic Characteristics of Nurses Working in Surgical Units
A total of 409 nurses were included in the analysis giving a 98.3% response rate. Male respondents accounted for 59.4% of the sample and the mean (± SD) age was 32.1 (±6.2) years. Nearly two-thirds (65%) of the respondents were married and the majority (90%) of respondents had bachelor’s degrees in Nursing (Table 1).
 |
Table 1 Socio-Demographic Characteristics of Nurses Working in Surgical Units of CSHs in Amhara Regional State, Northwest Ethiopia, 2022 (n = 409) |
Prevalence of Ankle-Foot Pain Among Nurses Working in Surgical Units
The prevalence of ankle-foot pain in the preceding 12 months in this study was 51.8% (95% CI: 46.9–57.5). More than one-fourth (27.4%) of the respondents faced difficulties in performing their daily activities, 26.4% of the respondents had healthcare provider visits and around (25.5%) of nurses had taken sick leave from work due to ankle-foot pain in the last 12 months.
Personal Characteristics of Nurses Working in Surgical Units
The mean (± SD) body mass index of the respondents was 22.5 (± 3.27) kg/m2 and nearly three-fourths (72.9%) of respondents had normal body mass index (Table 2).
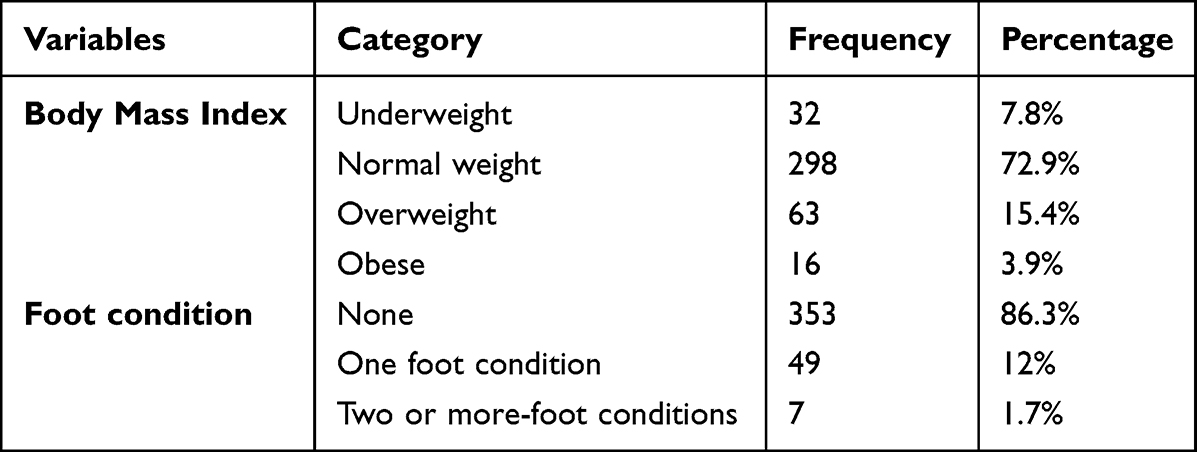 |
Table 2 Personal Characteristics of Nurses Working in Surgical Units of CSHs in Amhara Regional State, Northwest Ethiopia, 2022 (n = 409) |
Work-Related and Psychosocial Factors of Ankle-Foot Pain
Out of 409 respondents who took part in this study, more than half (54.3%) of respondents had 5–10 years of work experience and the majority (81.7%) of respondents were working more than or equal to 48 hours per week. Among the total respondents, more than three-fourths (79%) of nurses were working in night shift and nearly three-fourths (75.8%) of the respondents reported that their work involves prolonged standing. Nearly two-thirds (65.5%) of nurses were working in a static posture and 65.3% of nurses reported that their work involves lifting or lowering heavy loads. Regarding psychosocial factors, 225 (55%) and more than half (53.8%) of respondents reported that their work had high physical and psychological job demands, respectively. Two hundred and thirty-seven (57.9%) of respondents reported having high job control (Table 3).
 |
Table 3 Work-Related and Psychosocial Factors of Ankle-Foot Pain Among Nurses Working in Surgical Units of CSHs in Amhara Regional State, Northwest Ethiopia, 2022 (n = 409) |
Factors Associated with Ankle-Foot Pain Among Nurses Working in Surgical Units
In multivariable logistic regression analysis, working experience, working hours per week, prolonged standing, physical job demands, and job control were found to be independent predictors of ankle-foot pain at a p-value <0.05 (Table 4).
 |
Table 4 Bivariable and Multivariable Logistic Regression Analysis of Factors Associated with Ankle-Foot Pain Among Nurses Working in Surgical Units of CSHs in Amhara Regional State, Northwest Ethiopia, 2022 (n = 409) |
Nurses who had more than 10 years of work experience were 3.5 times [AOR = 3.48, 95% CI (1.35–8.92)] more likely to have ankle-foot pain as compared to nurses who had less than 5 years of work experience. The odds of having ankle-foot pain was 2.7 times [AOR = 2.69, 95% CI (1.27–6.00)] higher among nurses who were working 48 or more hours per week as compared to those who were working less than 40 hours per week. The odds of having ankle-foot pain were 5.7 times [AOR = 5.72, 95% CI (3.20–10.25)] higher among nurses who had prolonged standing as compared to those who did not have prolonged standing (Table 4).
Nurses who had high physical job demand were 2.4 times [AOR = 2.41, 95% CI (1.53–3.80)] more likely to develop ankle-foot pain as compared to those who had low physical job demand. Moreover, the odds of developing ankle-foot pain were 2.34 times [AOR = 2.34, 95% CI (1.47–3.71)] higher among nurses who had low job control as compared to those who had high job control (Table 4).
Discussion
This study aimed to determine the prevalence and factors associated with ankle-foot pain among nurses working in surgical units of Comprehensive Specialized Hospitals in Amhara regional state, Northwest Ethiopia.
In the current study, the prevalence of ankle-foot pain among nurses working in surgical units, during the preceding 12 months was 51.8% [95% CI (46.9–57.5)]. This finding is in line with the results from the studies conducted in Australia (55.3%),14 South Brazil (55.2%),16 England (55%),17 and Pakistan (47.2%).21 The possible reason for this might be due to similarities in study design, outcome measurement tool (Standardized Nordic Questionnaire), and operational definition of the outcome variable.
In this study, the prevalence of ankle-foot pain is higher than the findings from studies conducted in Japan (23%),25 Uganda (29.7%),30 Egypt (45.5%),31 and Ethiopia (43.7%).32 This discrepancy could be due to differences in the study population that the studies included nurses who were working in all units. This could be explained by the fact that nurses who work in surgical units are exposed to high static loads caused by standing for extended periods during surgical procedures, monitoring patients’ overall condition, and transferring patients from one location to the other put them at a high risk of developing ankle-foot pain.40
However, the finding of this study is lower than the finding of the study conducted in Malaysia (86.7%).10 This could be due to differences in the study population and sampling technique. In the current study, both female and male nurses working in surgical units were included in the study and a simple random sampling technique was used. However, according to the study conducted in Malaysia, only female nurses were included and a convenience sampling technique was employed. The possible explanation might be female nurses were more likely to be affected by ankle-foot pain than male nurses.41 Female nurses are more likely to sustain ankle-foot pain due to after-work responsibilities including parenting, handling household tasks, insufficient rest time, and lack of exercise.22
In addition, the present study result is lower than the finding of the study conducted in Iran (59%).28 This discrepancy could be due to differences in the study populations. In this study, the study population was all nurses working in all surgical units. Whereas based on the study done in Iran, the study population was nurses working only in the operation room. This could be because nurses working in the operation room are at greater risk for ankle-foot pain. After all, the operation room is recognized as a physically and psychologically demanding environment that requires prolonged standing, walking, and excessive physical activities like lifting and lowering heavy loads, thus causing loading to the lower extremity, especially in the ankle-foot region.27
In multivariable logistic regression analysis, more years of working experience, working more hours per week, prolonged standing, high physical job demand, and low job control were found to be significantly associated with ankle-foot pain.
This study showed that nurses who had more than 10 years of work experience were 3.5 times more likely to develop ankle-foot pain than those who had less than 5 years of work experience. This finding is supported by the study conducted in the USA showed that more years of nursing experience was associated with ankle-foot pain.15 The possible reason could be that nurses who have worked for a longer period have had enough exposure to risk factors, because ankle-foot pain by its nature is a repetitive strain that develops gradually as a result of overuse.
In this study, the odds of having ankle-foot pain were 2.7 times higher among nurses who were working 48 or more hours per week as compared to those who were working less than 40 hours per week. The result of this study is consistent with the study conducted in Ghana which revealed that there was a significant association between ankle-foot pain and working hours per week.34 This could be explained by the possibility that working more hours per week would result in longer exposure to job demands and hazards, or reduce the time for sleep, family, and non-work activities.42
The odds of developing ankle-foot pain were 5.7 times higher among nurses who had prolonged standing as compared to those who did not have prolonged standing. This finding is consistent with the study done in Finland.43 This can be explained by the fact that an immobilization or locking of the joints in the ankle-feet region that can occur during prolonged standing can facilitate degeneration in the tendons and ligaments, thus causing ankle-foot pain.44
In the current study, nurses who had high physical job demands were 2.4 times more likely to have ankle-foot pain as compared to those who had low physical job demands. This finding is congruent with the studies conducted in Iran and Ethiopia.27,32 The possible reason might be that high physical job demands, including prolonged standing, walking, and excessive physical activities cause strain to the lower extremities, especially on the ankle-foot region, thus leading to ankle-foot discomfort.35
In the present study, the odds of developing ankle-foot pain were 2.3 times higher among nurses who had low job control as compared to those who had high job control. This finding agreed with the study done in Japan, Panama, and Thailand.24,25,45 This might be because low job control can increase the activity of the sympathetic‐adrenal medullary system, which appears to play an important role in the development of ankle-foot pain.46
Limitations of the Study
In this study, nurses working in surgical units self-reported their ankle-foot pain experienced during the previous 12 months, which may have introduced some level of recall bias.
Conclusion and Recommendations
The current study showed that more than half of nurses who work in surgical units had ankle-foot pain, in the preceding 12 months. More years of work experience, working more hours per week, prolonged standing, high physical job demand, and low job control had a statistically significant association with ankle-foot pain. Health system administrators were recommended to consider reducing nurses’ exposure to job demands because these are the unavoidable nature of nursing jobs. They also need to consider expanding nurses’ ability to exert their influence over their working environment. Further, nursing leaders should support workplace environments that prevent working more than the recommended hours per week. Nursing staff should prioritize wearing supportive shoes, moving around whenever possible, and elevating their feet during breaks as preventive measures to reduce ankle-foot pain. Future researchers were recommended to conduct prospective studies to provide more reliable evidence about ankle-foot pain.
Abbreviations
AOR, Adjusted odds ratio; BMI, Body mass index; CI, Confidence interval; COR, Crude odds ratio; CSH, Comprehensive Specialized Hospital; DMCSH, Debre Markos Comprehensive Specialized Hospital; DTCSH, Debre Tabor Comprehensive Specialized Hospital; ETB, Ethiopian birr; FHCSH, Felege Hiwot Comprehensive Specialized Hospital; ICU, Intensive care unit; IRB, Institution review board; JCQ, Job Content Questionnaire; OR, Operation room; RR, Recovery room; SNQ, Standardized Nordic Questionnaire; SPSS, Statistical Package for Social Science; TGCSH, Tibebegion Comprehensive Specialized Hospital; UOGCSH, University of Gondar Comprehensive Specialized Hospital; WMSD, Work-related Musculoskeletal Disorder.
Data Sharing Statement
The corresponding author can provide the data presented in this study upon request.
Ethical Approval and Consent to Participate
Ethical clearance and approval were obtained from the ethical review committee of the school of nursing on behave of the institutional review board (IRB) of the University of Gondar with reference number S/N/241/2014 to conduct the study. Permission was obtained from each hospital administrator after explaining the purpose of the study. Written informed consent was obtained after providing information to each respondent regarding the purpose, risk, and benefit of participation. Confidentiality was maintained by making the data only accessible to the investigator. The Declaration of Helsinki’s ethical standards and guidelines were followed throughout the study.
Acknowledgments
We are grateful to the University of Gondar, College of Medicine and Health Science, School of Nursing, and Bahir Dar University College of Medicine and Health Science, School of Health Science for allowing us to do this thesis work. We would like to express our deepest gratitude to the coordinators of comprehensive specialized hospitals in Amhara regional state, Northwest Ethiopia for their unreserved support. We would like to thank all data collectors, supervisors, and respondents.
Author Contributions
All authors made a significant contribution to this work; contributed to conception, study design, execution, acquisition of data, analysis and interpretation, and wrote the first draft of the manuscript; involved in drafting, and critically reviewing of the article; have agreed on the journal to which the article will be submitted, and reviewed and agreed on all versions of the article before submission and during revision; agree to take responsibility and be accountable for the contents of the article.
Disclosure
The authors declare that they have no conflicts of interest in this work.
References
1. Hawke F, Burns J. Understanding the nature and mechanism of foot pain. J Foot Ankle Res. 2009;2(1):1–11.
2. Biz C, Barison E, Ruggieri P, Iacobellis C. Radiographic and functional outcomes after displaced intra-articular calcaneal fractures: a comparative cohort study among the traditional open technique (ORIF) and percutaneous surgical procedures (PS). J Orthop Surg Res. 2016;11(1):1–11. doi:10.1186/s13018-016-0426-6
3. Biz C, Golin N, De Cicco M, et al. Long-term radiographic and clinical-functional outcomes of isolated, displaced, closed talar neck and body fractures treated by ORIF: the timing of surgical management. BMC Musculoskelet Disord. 2019;20:1–11. doi:10.1186/s12891-019-2738-2
4. Biz C, Baldin G, Cappelletto C, et al. Isolated medial subtalar joint dislocation during sports activities: a systematic review of the literature with individual participant data analysis. Osteology. 2021;1(1):48–61. doi:10.3390/osteology1010005
5. Biz C, Ruaro A, Torrent J, Papa G, Ruggieri P, Ruggieri P. Conservative management of isolated medial subtalar joint dislocations in volleyball players: a report of three cases and literature review. J Sports Med Phys Fitness. 2019;59(10):1739–1746. doi:10.23736/S0022-4707.19.09531-8
6. Kurt TH. Contributors to Ankle and Foot Disorders Guide Line. ACOEM; 2015.
7. World Health Organization. Musculoskeletal Conditions. World Health Organization; 2021.
8. Martin RL, Davenport TE, Reischl SF, et al. Heel pain—plantar fasciitis: revision 2014. J Orthop Sports Phys Ther. 2014;44(11):A1–A33. doi:10.2519/jospt.2014.0303
9. Khan AR, Nadeem T, Mazhar S, Hadi SUJRJo HS. Frequency of foot and ankle pain among nurses of hayatabad medical complex-peshawar. Rehman J Health Sci. 2022;4(1):10–13.
10. Krishnan KS, Raju G, Shawkataly ER. Prevalence of work-related musculoskeletal disorders: psychological and physical risk factors. Int J Environ Res Public Health. 2021;18(17):9361. doi:10.3390/ijerph18179361
11. Raake H. Decreasing musculoskeletal injuries among operating room personnel through the use of anti-fatigue mats; 2019.
12. Sung K-C, Chung J-Y, Feng I-J, et al. Plantar fasciitis in physicians and nurses: a nationwide population-based study. Ind Health. 2020;58(2):153–160. doi:10.2486/indhealth.2019-0069
13. Stolt M, Suhonen R, Kielo E, Katajisto J, Leino‐Kilpi HJIJo NP. Foot health of nurses—a cross‐sectional study. Int J Nurs Pract. 2017;23(4):e12560.
14. Reed LF, Battistutta D, Young J, Newman B. Prevalence and risk factors for foot and ankle musculoskeletal disorders experienced by nurses. BMC Musculoskelet Disord. 2014;15(1):1–7.
15. Li J, Sommerich CM, Chipps E, Lavender SA, Stasny EA. A framework for studying risk factors for lower extremity musculoskeletal discomfort in nurses. Ergonomics. 2020;63(12):1535–1550. doi:10.1080/00140139.2020.1807615
16. Santos E, Andrade RD, Lopes SGR, Valgas CJ. Prevalence of musculoskeletal pain in nursing professionals working in orthopedic setting. Revista Dor. 2017;18:298–306.
17. Anderson J, Williams AE, Nester CJIJo IE. Musculoskeletal disorders, foot health and footwear choice in occupations involving prolonged standing. Int J Ind Ergon. 2021;81:103079.
18. Ribeiro T, Serranheira F, Loureiro HJ. Work related musculoskeletal disorders in primary health care nurses. Appl Nurs Res. 2017;33:72–77. doi:10.1016/j.apnr.2016.09.003
19. Yilmaz T. Ergonomics. Musculoskeletal system disorders among surgical nurses related to the health industry in northwestern Turkey: a cross-sectional study. Int J Occup Saf Ergon. 2021;28:1–6.
20. Anap DB, Iyer C, Rao K. Work related musculoskeletal disorders among hospital nurses in rural Maharashtra, India: a multi centre survey. Int J Res Med Sci. 2013;1(2):101–107.
21. Tariq S, Farooq Islam AA, Gilani SA. Prevalence of foot and ankle musculoskeletal disorders in nurses of Lahore Pakistan. Global J Med Res. 2018;2018:1.
22. Amin NA, Nordin RB, Noah R, Oxley J, Fatt CR. Work related musculoskeletal disorders in female nursing personnel: prevalence and impact. Int J Collab Res Intern Med Public Health. 2016;8(3):294–315.
23. Luan HD, Hai NT, Xanh PT, et al. Musculoskeletal disorders: prevalence and associated factors among district hospital nurses in Haiphong, Vietnam. Biomed Res Int. 2018;2018. doi:10.1155/2018/3162564
24. Jin S, Srisaenpang S, Pinitsoontorn S, Eungpinichpong WJJo HR. Prevalence of work-related musculoskeletal disorders among registered nurses in Srinagarind hospital, Thailand. J Health Res. 2011;25(2):61–68.
25. Tojo M, Yamaguchi S, Amano N, et al. Prevalence and associated factors of foot and ankle pain among nurses at a university hospital in Japan: a cross-sectional study. J Occup Health. 2017;63:132–139.
26. Tavakkol R, Kavi E, Hassanipour S, Rabiei H, Malakoutikhah M. The global prevalence of musculoskeletal disorders among operating room personnel: a systematic review and meta-analysis. Clin Epidemiol Glob Health. 2020;8(4):1053–1061.
27. Choobineh A, Movahed M, Tabatabaie SH, Kumashiro M. Perceived demands and musculoskeletal disorders in operating room nurses of Shiraz city hospitals. Ind Health. 2010;48(1):74–84. doi:10.2486/indhealth.48.74
28. Asghari E, Dianat I, Abdollahzadeh F, et al. Musculoskeletal pain in operating room nurses: associations with quality of work life, working posture, socio-demographic and job characteristics. Int J Ind Ergon. 2019;72:330–337.
29. Khudhir KM, Mahmood KA, Saleh KK, Adulah SR. Psychosocial factors in relation to musculoskeletal disorders among nursing professionals in Raparin Administration.
30. Mutanda T, Mwaka E, Sekimpi P, Ntuulo J. Occupation-related musculoskeletal disorders among nurses at the National Referral Hospital, Mulago in Uganda. Occup Med Health Aff. 2017;5(3):1–5.
31. Zayed HA, Saied SM, El-Sallamy R, Shehata WMJTEJo CM. Work-related musculoskeletal disorders among nursing staff of Tanta University Hospitals: pattern, risk factors, and coping strategies. Occup Med Health Aff. 2019;37(4):51–61.
32. Getie K, Kahsay G, Kassaw A, Gomera G, Alamer A, Hailu TJJo PR. Ankle and foot pain and associated factors among nurses at ayder comprehensive specialized hospital, Mekelle, Ethiopia: cross-sectional study. J Pain Res. 2021;14:83. doi:10.2147/JPR.S283580
33. Attar SM. Frequency and risk factors of musculoskeletal pain in nurses at a tertiary centre in Jeddah, Saudi Arabia: a cross sectional study. BMC Res Notes. 2014;7(1):1–6.
34. Abla Kofi-Bediako W, Sama G, Yarfi C, Ed-Bansah D, Appah Acquah A. Work-related musculoskeletal disorders among nurses at the ho teaching Hospital, Ghana.
35. Stolt M, Miikkola M, Suhonen R, Leino-Kilpi H. Nurses’ perceptions of their foot health: implications for occupational health care. Workplace Health Saf. 2018;66(3):136–143. doi:10.1177/2165079917727011
36. Tefera BZ, Zeleke H, Abate A, Abebe H, Mekonnen Z, Sewale Y. Magnitude and associated factors of low back pain among nurses working at intensive care unit of public hospitals in Amhara region, Ethiopia. PLoS One. 2021;16(12):e0260361. doi:10.1371/journal.pone.0260361
37. Reed LF. An Investigation of Foot and Ankle Problems Experienced by Nurses. Queensland University of Technology; 2007.
38. Kuorinka I, Jonsson B, Kilbom A, et al. Standardised Nordic questionnaires for the analysis of musculoskeletal symptoms. Appl Ergon. 1987;18(3):233–237. doi:10.1016/0003-6870(87)90010-x
39. Karasek R, Brisson C, Kawakami N, Houtman I, Bongers P, Amick BJ. The Job Content Questionnaire (JCQ): an instrument for internationally comparative assessments of psychosocial job characteristics. J Occup Health Psychol. 1998;3(4):322. doi:10.1037//1076-8998.3.4.322
40. Rypicz Ł, Karniej P, Witczak I, Kołcz A. Evaluation of the occurrence of work‐related musculoskeletal pain among anesthesiology, intensive care, and surgical nurses: an observational and descriptive study. Nurs Health Sc. 2020;22(4):1056–1064. doi:10.1111/nhs.12767
41. Bernardes RA, Caldeira S, Parreira P, et al. Foot and Ankle disorders in nurses exposed to prolonged standing environments: a scoping review. Workplace Health Saf. 2023;2023:21650799221137646.
42. Garza JL, Ferguson JM, Dugan AG, et al. Investigating the relationship between working time characteristics on musculoskeletal symptoms: a cross sectional study. Arch Environ Occup Health. 2022;77(2):141–148. doi:10.1080/19338244.2020.1860878
43. STOlT M, Virolainen P, Leino-Kilpi H. Lower extremity musculoskeletal disorders in nurses: a narrative literature review. Scand J Public Health. 2016;44(1):106–115.
44. Hughes NL, Nelson A, Matz MW, Lloyd JJ. AORN Ergonomic Tool 4: solutions for prolonged standing in perioperative settings. AORN J. 2011;93(6):767–774. doi:10.1016/j.aorn.2010.08.029
45. Bernal D, Campos-Serna J, Tobias A, Vargas-Prada S, Benavides FG, Serra CJ. Work-related psychosocial risk factors and musculoskeletal disorders in hospital nurses and nursing aides: a systematic review and meta-analysis. Int J Nurs Stud. 2015;52(2):635–648. doi:10.1016/j.ijnurstu.2014.11.003
46. Lee J, Kim H-R, Lee D-W, Kang M. Interaction between occupational physical burdens and low job control on musculoskeletal pain: analysis of the 5th Korean Working Environment Survey. J Occup Health. 2021;63(1):e12244. doi:10.1002/1348-9585.12244
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.