Back to Journals » Journal of Hepatocellular Carcinoma » Volume 10
Pretreatment Non-Invasive Biomarkers as Predictors to Estimate Portal Vein Tumor Thrombosis (PVTT) Risk and Long-Term Survival in HBV-Related Hepatocellular Carcinoma Patients Without PVTT
Authors Liu B ![]() , Liu J, Mei X, Zhang ZQ, Fang J, Zhou LL
, Liu J, Mei X, Zhang ZQ, Fang J, Zhou LL ![]() , Zheng JL
, Zheng JL ![]() , Lin HY, Zhu XL, Li DL
, Lin HY, Zhu XL, Li DL ![]()
Received 28 September 2023
Accepted for publication 19 December 2023
Published 28 December 2023 Volume 2023:10 Pages 2367—2382
DOI https://doi.org/10.2147/JHC.S442487
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr David Gerber
Bang Liu,1,2,* Jia Liu,3,* Xuan Mei,1,* Zhi-Qiang Zhang,1,2 Jian Fang,4 Li-Li Zhou,2 Jiao-Long Zheng,2 Hai-Yan Lin,2 Xiu-Ling Zhu,2 Dong-Liang Li1,2
1Fuzong Clinical Medical College of Fujian Medical University, Fuzhou, 350025, People’s Republic of China; 2Department of Hepatobiliary Disease, 900TH Hospital of Joint Logistics Support Force, Fuzhou, 350025, People’s Republic of China; 3Department of Hepatobiliary Surgery, The Fifth Medical Center of Chinese PLA General Hospital, Beijing, 100039, People’s Republic of China; 4Department of Hepatobiliary Medicine, The Third Affiliated People’s Hospital of Fujian University of Traditional Chinese Medicine, Fuzhou, 350108, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Dong-Liang Li, Department of Hepatobiliary Disease, Fuzong Clinical Medical College of Fujian Medical University & 900TH Hospital of Joint Logistics Support Force, Fuzhou, 350025, People’s Republic of China, Email [email protected]
Background: PVTT is a hallmark of advanced hepatocellular carcinoma (HCC). We aim to explore the influence of non-invasive biomarkers on the occurrence of PVTT and develop and validate models for predicting prognosis in HBV-related HCC patients without PVTT.
Methods: A total of 1026 HBV-related HCC patients without PVTT were enrolled, with 515 in the training cohort, 216 in the internal validation cohort, and 295 in the external validation cohort. We conducted Cox regression analyses to discern the independent risk factors associated with PVTT events, PFS, and OS, then constructed and validated predictive models. The predictive and discriminatory capabilities of models were assessed using the calibration, time-dependent ROC, and DCA curves.
Results: In our study, 136 patients (13.3%) experienced PVTT events during the follow-up period. The Cox regression analysis unveiled that male gender, AAPR ≤ 0.49, APRI > 0.48, extrahepatic metastasis, and multiple tumors were independent risk factors for PVTT. In the training cohort, non-invasive biomarkers (AAR and APRI), AFP, ascites, and tumor-related characteristics (extrahepatic metastasis, tumor diameter, tumor number, and PVTT event) were independent risk factors for both OS and PFS, whereas age and ALBI grade independently correlated with OS. The C-indexes of OS and PFS nomogram models were 0.795 and 0.733 in the training cohort, 0.765 and 0.716 in the internal validation cohort, and 0.780 and 0.722 in the external validation cohort, respectively. Our models demonstrated strong predictive and discriminative abilities in all cohorts and yielded a greater net benefit compared to three traditional staging systems.
Conclusion: Non-invasive biomarkers are expected to be reliable predictors for assessing PVTT risk and predicting prognosis among HBV-related HCC patients without PVTT.
Keywords: non-invasive biomarker, portal vein tumor thrombosis, HBV-related HCC, nomogram, prognosis
Introduction
In 2020, liver cancer stood as the third leading cause of cancer-related fatalities and the sixth most prevalent cancer globally, and hepatocellular carcinoma (HCC) accounts for approximately 90% of liver cancer cases.1,2 The number of new cases and deaths is expected to increase by more than 55% by the year 2040.3 China has a heavy burden of liver cancer, with more than 45% of global new cases and deaths occurring in this region, and about 84.4% of liver cancer patients are afflicted with hepatitis B virus (HBV) infection.1,4 Despite the increasing coverage of hepatitis B vaccination and a steady rise in the diagnosis and treatment rates for chronic hepatitis B in China, HCC remains a persistent challenge, primarily due to the vast number of HBV-infected individuals in the population.5,6
Portal vein tumor thrombosis (PVTT) represents a frequent clinical manifestation of HCC and serves as a hallmark of advanced HCC. Regrettably, PVTT is observed in 44–62.2% of HCC patients, what is even more concerning is that untreated patients face a median survival time of just 2.7 to 4 months.7 PVTT gives rise to hepatic hypofunction, portal hypertension, and ascites, often culminating in disease progression and fatality.8 Although treatments such as surgical resection, transcatheter arterial chemoembolization (TACE), and systemic treatment offer the potential for improved survival outcomes, options are limited once PVTT has developed, and overall survival rates remain low.7,9 Moreover, it is worth noting that HBV infection and replication significantly contribute to the formation of PVTT.10 Hence, it is important to identify risk factors for PVTT events in HBV-related HCC patients who have not yet developed PVTT. Early identification of these risk factors is crucial for timely intervention and better patient outcomes.
Presently, the Barcelona Clinic Liver Cancer (BCLC) staging system, the Cancer of the Liver Italian Program (CLIP) staging system, and the Okuda staging system are extensively employed for treatment guidance and prognosis assessment in HCC. However, owing to the inherent tumor heterogeneity and individual variability, the prognosis can significantly differ among HCC patients with the same clinical stage.11,12 Recent studies have illuminated the potential of inexpensive and readily accessible non-invasive biomarkers like albumin (ALB)-to-alkaline phosphatase (ALP) ratio (AAPR), aspartate aminotransferase (AST)-to-alanine aminotransferase (ALT) ratio (AAR), AST-to-platelet ratio index (APRI), and fibrosis-4 index (FIB-4) as valuable prognostic indicators for predicting disease progression and long-term survival in HCC patients.13–18
The nomogram, a straightforward visualization tool, is constructed by integration and quantization of numerous independent risk factors, which can be used to accurately and individually identify high-risk patients and predict prognosis, and its application can enhance the clinical management and prognosis assessment for HCC patients.19,20 However, the relationship between non-invasive biomarkers and PVTT events remains elusive, and few nomogram models are available for predicting the prognosis of HBV-related HCC patients without PVTT. Hence, this study aims to investigate the impact of non-invasive biomarkers on PVTT events and the prognostic value of non-invasive biomarkers, and constructed and validated two nomogram models to predict the overall survival (OS) and progression-free survival (PFS) of HBV-related HCC patients without PVTT, respectively.
Materials and Methods
Study Population
We conducted a retrospective analysis of clinical data involving consecutive patients newly diagnosed with HBV-related HCC without PVTT, who were admitted to the 900TH Hospital of Joint Logistics Support Force between April 2016 and February 2022. The inclusion criteria were as follows: (a) diagnosis of HCC based on radiological imaging or histopathological evidence, following the guidelines for the diagnosis and treatment of hepatocellular carcinoma (2019 Edition); (b) presence of positive HBV surface antigen (HBsAg) for at least 6 months and/or HBV-DNA viral load >500 IU/mL; (c) no previous anticancer treatment; (d) age between 18 and 85 years. Exclusion criteria encompassed: (a) PVTT was present before enrollment based on the Chinese Expert Consensus on Multidisciplinary Diagnosis and Treatment of Hepatocellular Carcinoma with Portal Vein Tumor Thrombus (2018 Edition); (b) presence of etiology other than HBV; (c) coexistence of other malignancies; (d) severe organ dysfunction (eg, heart, lung, kidney, etc.); (e) human immunodeficiency virus (HIV) infection, hematological diseases, or autoimmune diseases; (f) incomplete clinical and laboratory data or loss to follow-up. Following these inclusion and exclusion criteria, a total of 1026 HBV-related HCC patients without PVTT were included in our study. Among them, 731 patients from our center were randomly assigned to the training cohort (n=515) and the internal validation cohort (n=216) using a 7:3 ratio. An additional 295 patients from the Fifth Medical Center of Chinese PLA General Hospital (from July 2016 to August 2021) constituted the external validation cohort.
Definition
The calculation formula of the non-invasive biomarkers are as follows: AAPR = ALB (g/L) / ALP (U/L); AAR = AST (U/L) / ALT (U/L); APRl = [AST (U/L) / upper limit of normal] × 100 / platelet count (PLT, 109/L); FIB-4 = [age (year) × AST (U/L)] / [PLT (109/L)×ALT (U/L)1/2]. To determine the optimal cut-off values for these non-invasive biomarkers, we conducted the time-dependent receiver operating characteristic (ROC) curve analysis within our center’s cohort. The optimal cut-off values for AAPR, AAR, APRI, and FIB-4 were 0.49 [with an area under the curve (AUC) of 5-year OS: 0.711, 95% confidence interval (CI): 0.660–0.762], 0.965 (with an AUC of 5-year OS: 0.703, 95% CI: 0.651–0.755), 0.48 (with an AUC of 5-year OS: 0.675, 95% CI: 0.620–0.731), and 1.85 (with an AUC of 5-year OS: 0.656, 95% CI: 0.602–0.710), respectively (Figure S1). The albumin-bilirubin (ALBI) score was calculated based on serum total bilirubin (TBIL) and ALB levels and categorized into three grades: grade 1 (≤ −2.60), grade 2 (> −2.60 to −1.39), and grade 3 (> −1.39).21 PVTT event was defined as the presence of an intraluminal filling defect with typical arterial enhancement in the main or branch of the portal vein, confirmed through radiologic imaging methods such as ultrasound, computed tomography (CT), and/or magnetic resonance imaging (MRI).22 The degree of ascites was classified according to the consensus of the International Ascites Club. Finally, as per the modified Response Evaluation Criteria in Solid Tumors (mRECIST), the time interval between the date of diagnosis and either death or disease progression was designated as OS and PFS, respectively.
Data Collection and Treatment
Within one week prior to treatment initiation, we gathered baseline demographic, laboratory, and imaging data for all enrolled patients. These recorded variables included age, gender, routine blood tests, biochemical tests, alpha-fetoprotein (AFP), HBV-DNA load, ascites, extrahepatic metastasis, tumor number, tumor maximum diameter, and additional pertinent factors. The management of HCC closely adhered to the China Guidelines for Diagnosis and Treatment of Primary Liver Cancer (2017 Edition to 2019 Edition). Treatment modalities included surgical resection, radiofrequency ablation, liver transplant, TACE, hepatic arterial infusion chemotherapy (HAIC), radiotherapy, systemic therapy, and best supportive care, either individually or in combination. Furthermore, all patients received antiviral therapy.
Follow-Up
Regular follow-up assessments were conducted, with intervals ranging from 1 to 3 months during the initial 12 months following treatment. Subsequently, follow-up appointments were scheduled at intervals of 3 to 6 months, continuing until May 31, 2023. These follow-up evaluations encompassed physical examinations, blood routine, biochemical tests, serum AFP level, HBV-DNA load, chest X-ray, and abdominal imaging (including ultrasound, CT, and/or MRI). Within our study, the occurrence of PVTT events was the primary endpoint, and OS and PFS were the secondary endpoints, respectively. The median follow-up time for our center and the Fifth Medical Center are 1601 days and 1538 days, respectively.
Statistics
Continuous variables were presented either as mean ± standard deviation (SD) or as median with interquartile range (IQR), and comparisons were made using appropriate statistical tests such as the Student’s t-test, one-way ANOVA, Mann–Whitney U-test, or Kruskal–Wallis test. Categorical variables were expressed as numbers and percentages and were analyzed using the Chi-square test or Yates’ correction. Univariate and multivariate Cox regression analyses were carried out to identify independent risk factors for PVTT event, OS, and PFS. Survival differences among different groups were assessed using Kaplan-Meier (KM) curves. Subsequently, nomogram models were constructed based on the multiple independent risk factors identified from the training cohort. These models were validated using both the internal and external validation cohorts. The predictive accuracy of models was evaluated using Harrell’s concordance index (C-index) and time-dependent ROC curves. Generally, a C-index or AUC value over 0.7 indicates an accurate model. The consistency of the model predicted probability and the actual probability was evaluated by a calibration curve with 800 bootstrap resamples. The closer the model’s calibration curve to the ideal line, the better the consistency and accuracy of the model was. Moreover, decision curve analysis (DCA) was employed to compare the net clinical benefits of the models against traditional staging systems. Statistical analyses and graphical visualizations were performed utilizing R software version 4.2.1 (R Foundation for Statistical Computing, Vienna, Austria), with the aid of the following R packages: ‘stats’, “survival”, “rms”, “survminer”, “timeROC”, “pROC”, and “ggplot2”. p<0.05 was considered statistically significant.
Results
Baseline Characteristics
A total of 1026 patients were enrolled in the present study. The median age of the entire cohort was 56 years (IQR: 48 to 65 years), 84.2% (n=864) were male, 59.6% (n=611) belonged to the ALBI grade 1 subgroup, 59.2% (n=607) were positive for HBV-DNA, 22.3% (n=232) had ascites, and 12.9% (n=132) had extrahepatic metastasis. According to the BCLC staging system, the distribution of patients was as follows: 108 patients (10.5%) were classified as BCLC stage 0, 416 patients (40.5%) as BCLC stage A, 296 patients (28.8%) as BCLC stage B, 173 patients (16.9%) as BCLC stage C, and 33 patients (3.2%) as BCLC stage D. In total, 136 (13.3%) patients experienced PVTT event. If we performed the analysis on the above 136 patients only, the median time of the development of PVTT would be 335 days (95% CI: 226–431). Compared to the non-PVTT group, the PVTT group had lower values of AAPR (0.35 vs 0.42, p< 0.001), but higher values of APRI (0.87 vs 0.65, p=0.002), ALBI score (−2.69 vs −2.75, p=0.034) and tumor diameter (5.95cm vs 4.7 cm, p=0.031) (Figure 1A–D), and a higher proportion of males (91.9% vs 83%, p=0.008), extrahepatic metastasis (19.1% vs 11.9%, p=0.019) and multiple tumors (55.1% vs 46%, p=0.046). The PVTT group had 136 cases (100%) of progression with a median PFS of 171 days and 126 cases (92.6%) of death with a median OS of 637.5 days, respectively. The non-PVTT group had 684 cases (76.9%) of progression with a median PFS of 374 days and 496 cases (55.7%) of death with a median OS of 1164 days, respectively. The details are shown in Table 1. The PVTT group had poorer OS [hazard ratio (HR)=1.95, 95% CI: 1.60–2.37; p<0.001] and PFS (HR=2.10, 95% CI: 1.74–2.53; p<0.001) than non-PVTT group (Figure 1E and F). Then, we divided the entire cohort into the training cohort (n=515), internal validation cohort (n=216), and external validation cohort (n=295), and details are summarized in Table 2.
 |
Table 1 Baseline Characteristics of HBV-Related HCC Patients with and without PVTT |
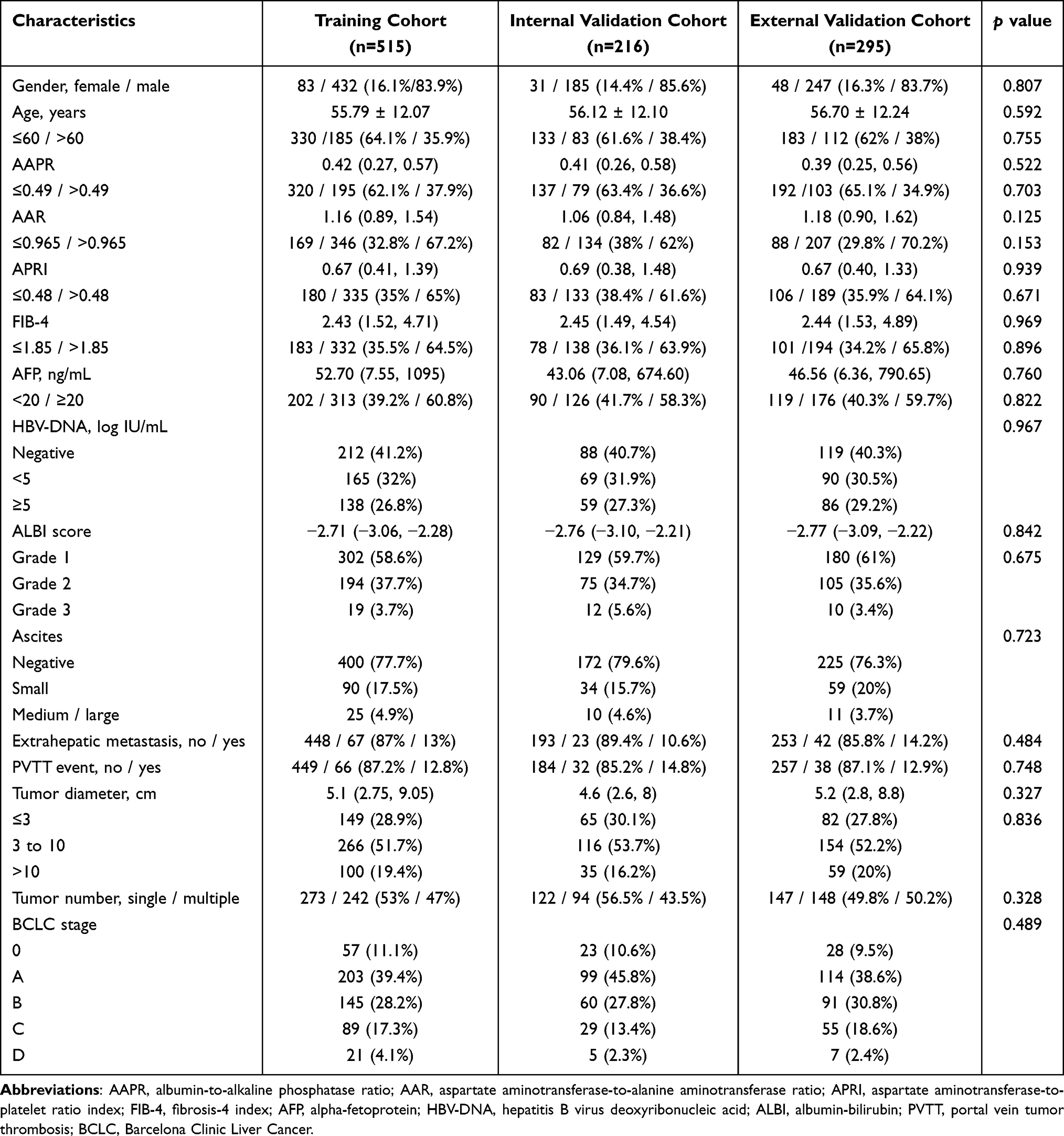 |
Table 2 Baseline Characteristics of the Three Cohorts |
 |
Figure 1 Comparison of clinical characteristics and prognosis between PVTT group and non-PVTT group. The values of AAPR (A), APRI (B), ALBI score (C), and tumor diameter (D) were marked differences between the PVTT group and the non-PVTT group. KM survival curves revealed that patients occurred PVTT events had poorer OS (E) and PFS (F) than patients without PVTT. Abbreviations: AAPR, albumin-to-alkaline phosphatase ratio; APRI, aspartate aminotransferase-to-platelet ratio index; ALBI, albumin-bilirubin; PVTT, portal vein tumor thrombosis; HR, hazard ratio. |
Cox Regression Analysis for PVTT in the Entire Cohort
Univariable and multivariable Cox regression analysis was performed to identify independent risk factors for PVTT and results are presented in Table S1. Male gender (HR: 2.171, 95% CI: 1.151–4.096), APRI >0.48 (HR: 2.644, 95% CI: 1.478–4.730), extrahepatic metastasis (HR: 3.016, 95% CI: 1.850–4.916) and multiple tumors (HR: 1.512, 95% CI: 1.040–2.199) were independently associated with higher risk of PVTT event, but AAPR >0.49 (HR: 0.428, 95% CI: 0.269–0.681) was independently related to lower risk of PVTT event (Figure 2).
 |
Figure 2 Cox regression analysis and forest plot of PVTT in the entire cohort. Abbreviations: PVTT, portal vein tumor thrombosis; HR, hazard ratio; AAPR, albumin-to-alkaline phosphatase ratio; AAR, aspartate aminotransferase-to-alanine aminotransferase ratio; APRI, aspartate aminotransferase-to-platelet ratio index; FIB-4, fibrosis-4 index; AFP, alpha-fetoprotein; HBV-DNA, hepatitis B virus DNA; ALBI, albumin-bilirubin. |
Cox Regression Analysis for OS and PFS in the Training Cohort
Multivariable Cox analysis identified 10 independent risk factors for OS and 8 independent risk factors for PFS in the training cohort (Table S2). AAR >0.965 (OS: HR =1.932, p<0.001; PFS: HR =1.662, p<0.001), APRI >0.48 (OS: HR =1.651, p=0.011; PFS: HR =1.489, p=0.014), AFP ≥20 ng/mL (OS: HR =1.382, p=0.014; PFS: HR =1.267, p=0.031), extrahepatic metastasis (OS: HR =2.669, p<0.001; PFS: HR =2.170, p<0.001), multiple tumor (OS: HR =1.848, p<0.001; PFS: HR =1.562, p<0.001), PVTT event (OS: HR =1.605, p=0.002; PFS: HR =1.946, p<0.001), ascites and tumor diameter were independent risk factors for both OS and PFS. Age >60 years (HR =1.448, p=0.005) and ALBI grade were independent risk factors of OS, but not of PFS (Figure 3). KM curves for OS and PFS of the above independent risk factors are demonstrated in Figures S2 and S3, respectively.
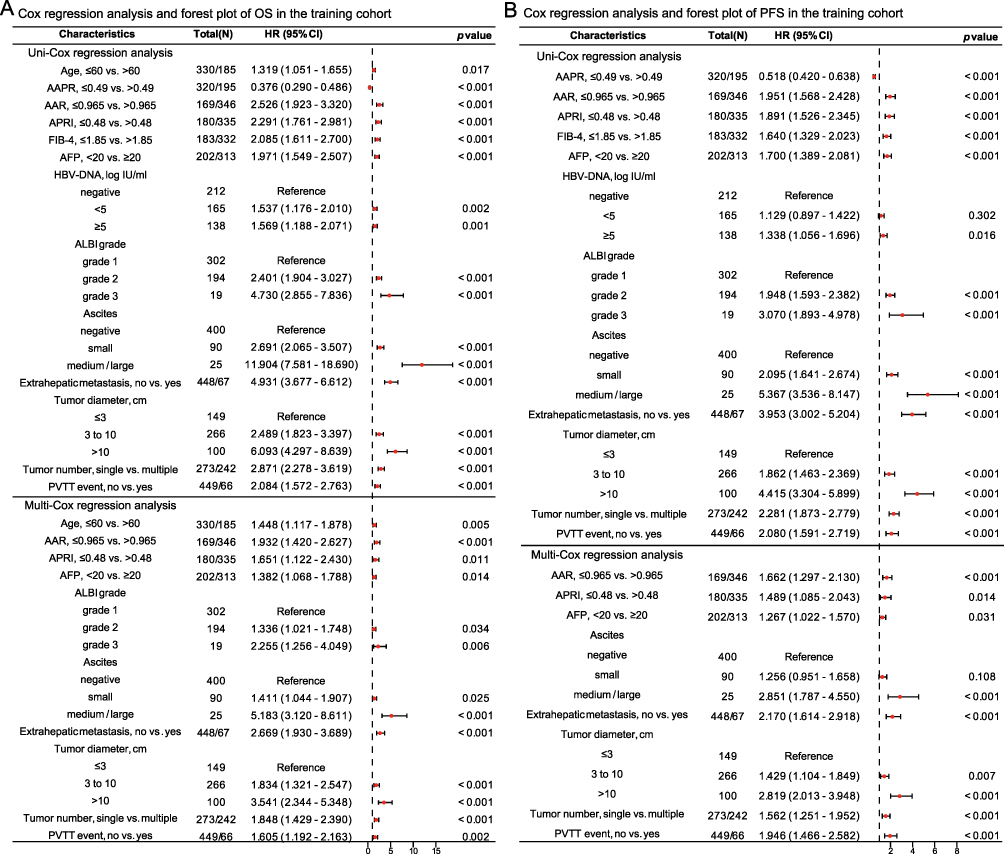 |
Figure 3 Cox regression analysis and forest plots of OS (A) and PFS (B) in the training cohort. Abbreviations: OS, overall survival; PFS, progression-free survival; HR, hazard ratio; AAPR, albumin-to-alkaline phosphatase ratio; AAR, aspartate aminotransferase-to-alanine aminotransferase ratio; APRI, aspartate aminotransferase-to-platelet ratio index; FIB-4, fibrosis-4 index; AFP, alpha-fetoprotein; HBV-DNA, hepatitis B virus DNA; ALBI, albumin-bilirubin; PVTT, portal vein tumor thrombosis. |
Construction and Validation of the OS Nomogram Model
The OS nomogram model was constructed by integrating ten independent predictors (age, AAR, APRI, AFP, ALBI grade, ascites, extrahepatic metastasis, tumor diameter, tumor number, and PVTT event) for OS in the training cohort (Figure 4A). The C-index of the OS nomogram model was 0.795 (95% CI: 0.783–0.807) for the training cohort and further validated by both the internal validation cohort (0.765, 95% CI: 0.745–0.784) and external validation cohort (0.780, 95% CI: 0.765–0.796). The calibration curves of the model for predicting 1‐, 3‐, and 5‐year OS demonstrated good agreement in the training cohort, and it performed equally well in the internal and external validation cohorts (Figure 4B–D). The time-dependent ROC curves verified the good predictive accuracy of the OS model for OS in the training cohort (1‐year AUC, 0.869; 3‐year AUC, 0.867; 5‐year AUC, 0.865), internal validation cohort (1‐year AUC, 0.885; 3‐year AUC, 0.798; 5‐year AUC, 0.826) and external validation cohort (1‐year AUC, 0.883; 3‐year AUC, 0.839; 5‐year AUC, 0.863; Figure 4E–G). DCA curves revealed that the OS nomogram model had a greater net benefit than three traditional staging systems (BCLC stage, CLIP score, and Okuda stage) at 5 years regardless of cohort (Figure 4H–J). These results showed that the OS model had good discriminating ability and clinical applicability.
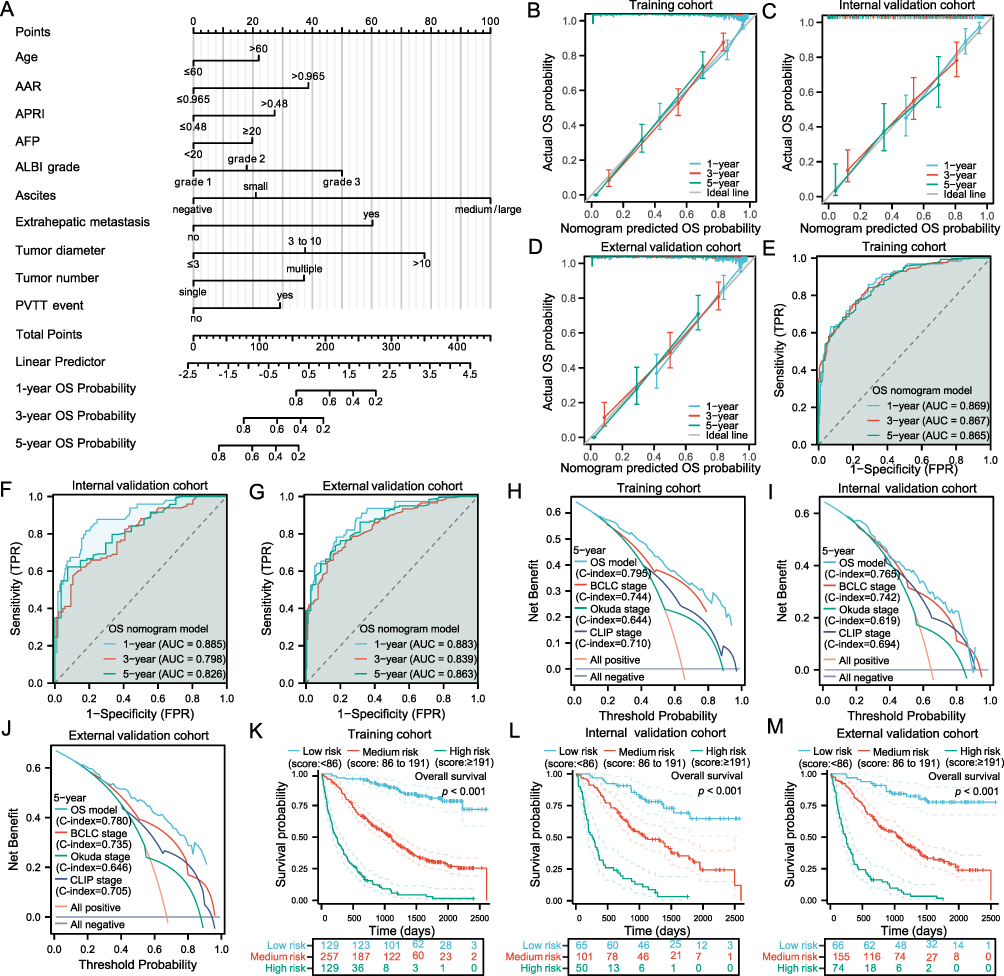 |
Figure 4 Construction and validation of the OS nomogram model. Nomogram predicting the OS for HBV-related HCC patients without PVTT (A). The calibration curves of the OS model for predicting 1‐, 3‐, and 5‐year OS in the training cohort (B), internal validation cohort (C), and external validation cohort (D). The time-dependent ROC curves of the OS model were used to evaluate the predictive ability of 1‐, 3‐, and 5‐year OS in the training cohort (E), internal validation cohort (F), and external validation cohort (G). The DCA curves of the OS model were performed to assess the clinical utility of 5‐year OS in the training cohort (H), internal validation cohort (I), and external validation cohort (J). KM survival analysis of OS among different risk groups based on the score of the OS nomogram model in the training cohort (K), internal validation cohort (L), and external validation cohort (M). Abbreviations: AAR, aspartate aminotransferase-to-alanine aminotransferase ratio; APRI, aspartate aminotransferase-to-platelet ratio index; AFP, alpha-fetoprotein; ALBI, albumin-bilirubin; PVTT, portal vein tumor thrombosis; OS, overall survival; AUC, the area under the curve; BCLC, Barcelona Clinic Liver Cancer; CLIP, Cancer of the Liver Italian Program. |
Construction and Validation of the PFS Nomogram Model
The PFS nomogram model was created by incorporating eight independent predictors (AAR, APRI, AFP, ascites, extrahepatic metastasis, tumor diameter, tumor number, and PVTT event) for PFS in the training cohort (Figure 5A). The C-index of the PFS nomogram model was 0.733 (95% CI: 0.721–0.745) for the training cohort and further supported by both the internal validation cohort (0.716, 95% CI: 0.697–0.735) and external validation cohort (0.722, 95% CI: 0.706–0.738). The calibration curves of the model for predicting 1‐, 3‐, and 5‐year PFS demonstrated good agreement in the training cohort, which performed similarly well in other cohorts (Figure 5B–D). The time-dependent ROC plots demonstrated good discriminating ability of the PFS model for PFS in the training cohort (1‐year AUC, 0.796; 3‐year AUC, 0.836; 5‐year AUC, 0.808), internal validation cohort (1‐year AUC, 0.791; 3‐year AUC, 0.810; 5‐year AUC, 0.888) and external validation cohort (1‐year AUC, 0.804; 3‐year AUC, 0.853; 5‐year AUC, 0.871; Figure 5E–G). DCA plots illustrated that the PFS nomogram model had a better net benefit than three traditional staging systems at 5 years in each cohort (Figure 5H–J). These results revealed that the PFS model has potential clinical benefits.
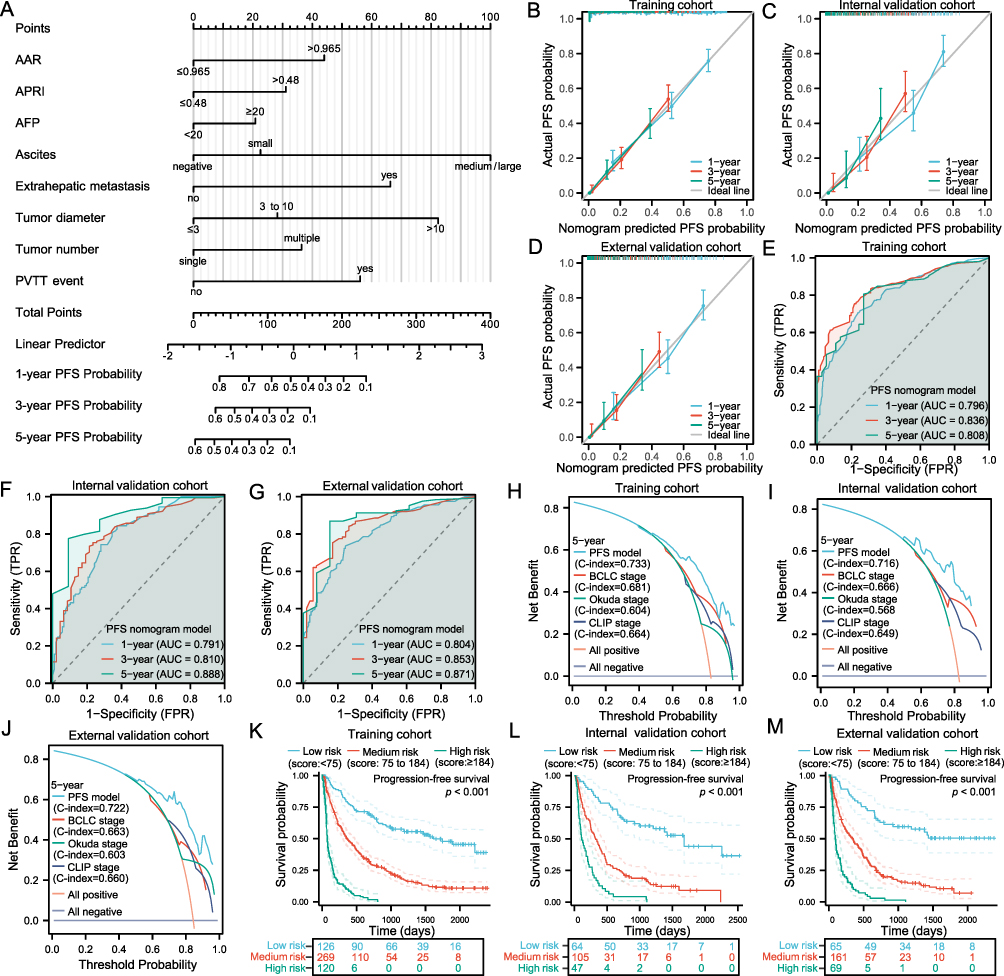 |
Figure 5 Construction and validation of the PFS nomogram model. Nomogram predicting the PFS for HBV-related HCC patients without PVTT (A). The calibration curves of the PFS model for predicting 1‐, 3‐, and 5‐year PFS in the training cohort (B), internal validation cohort (C), and external validation cohort (D). The time-dependent ROC curves of the PFS model were used to evaluate the predictive ability of 1‐, 3‐, and 5‐year PFS in the training cohort (E), internal validation cohort (F), and external validation cohort (G). The DCA curves of the PFS model were performed to assess the clinical utility of 5‐year PFS in the training cohort (H), internal validation cohort (I), and external validation cohort (J). KM survival analysis of PFS among different risk groups based on the score of the PFS nomogram model in the training cohort (K), internal validation cohort (L), and external validation cohort (M). Abbreviations: AAR, aspartate aminotransferase-to-alanine aminotransferase ratio; APRI, aspartate aminotransferase-to-platelet ratio index; AFP, alpha-fetoprotein; PVTT, portal vein tumor thrombosis; PFS, progression-free survival; AUC, the area under the curve; BCLC, Barcelona Clinic Liver Cancer; CLIP, Cancer of the Liver Italian Program. |
The Ability of Models to Discriminate the Risk of Patients
According to the score of the OS nomogram model using the 25th and 75th percentiles as the cut-off value, patients were divided into low- (score: <86), medium- (score: 86 to 191), and high- (score: ≥191) risk groups, respectively, and significant differences in OS were observed among the three groups regardless of the cohort (p<0.001 for all; Figure 4K–M). The survival analysis showed that the high-risk group (training cohort: 235 days; internal validation cohort: 263.5 days; external validation cohort: 242 days) had a significantly shorter median OS compared with the medium-risk group (training cohort: 1099 days; internal validation cohort: 1088 days; external validation cohort: 1056 days), and the median OS of the medium-risk group was exhibited shorter than the low-risk group (training cohort: not reached; internal validation cohort: not reached; external validation cohort: not reached).
Similarly, patients were stratified into low- (score: <75), medium- (score: 75 to 184), and high- (score: ≥184) risk groups based on the score of the PFS nomogram model using the 25th and 75th percentiles as the cut-off value. There were significant differences in PFS among the three groups in each cohort (p<0.001 for all; Figure 5K–M). The survival analysis of PFS revealed that the low-risk group (training cohort: 1617 days; internal validation cohort: 1679 days; external validation cohort: not reached) had the longest median PFS, the medium-risk group (training cohort: 367 days; internal validation cohort: 323 days; external validation cohort: 345 days) with the second longest, and the high-risk group (training cohort: 81 days; internal validation cohort: 112 days; external validation cohort: 98 days) with the shortest median PFS.
Subgroup Analysis of Models According to the BCLC Staging System
A subgroup analysis based on the BCLC staging system was performed to investigate the discriminatory ability of our novel models in patients with the same BCLC stages, and patients were classified into BCLC 0/A (n=524), BCLC B (n=296), and BCLC C/D groups (n=206). In BCLC stage 0/A, there were significant differences in OS and PFS between the low- and medium-risk groups (p<0.001 for both), also significant differences between the medium- and high-risk groups were observed in PFS but not in OS (Figure 6A and D). The OS and PFS differences among the three risk groups were significant in BCLC stage B patients (p<0.001 for all; Figure 6B and E). As for BCLC stage C/D patients, OS and PFS in the medium- and high-risk groups (p<0.001 for both) were all statistically different but not in the low- and medium-risk groups (Figure 6C and F). These results indicated that our models can distinguish the risk of prognostic in patients with the same BCLC stages, especially BCLC stage B.
 |
Figure 6 Subgroup survival analysis for the entire cohort stratified by the BCLC staging system. KM survival analysis of OS and PFS among different risk groups based on the score of the OS nomogram model and PFS nomogram model in BCLC stage 0/A patients (A and D), BCLC stage B patients (B and E), and BCLC stage C/D patients (C and F), respectively. Abbreviation: BCLC, Barcelona Clinic Liver Cancer. |
Discussion
In China, liver cancer is one of the most common tumors, claiming over 380,000 lives annually.1 Most HCC patients have chronic HBV infection, and approximately 66% of them are diagnosed at the intermediate or advanced stage.23 PVTT emergence serves as a distinctive feature of advanced HCC, which imposes a great treatment challenge for HCC, and patients with PVTT are typically classified as BCLC stage C and have a dismal prognosis. Therefore, the identification of independent risk factors for PVTT is of paramount importance, as it holds the potential to facilitate early intervention and prevention, thereby improving the clinical management of HCC, which means a lot to HBV-related HCC patients who have yet to develop PVTT. In our study, we observed that a total of 136 patients (13.3%) experienced PVTT events during the follow-up period, which was mostly in line with the results reported by Guarino et al (11.1%) and Tortora et al (14.4%).24,25
Multivariate Cox regression analysis revealed that male gender, AAPR ≤0.49, APRI >0.48, the presence of extrahepatic metastasis, and multiple tumors were independent risk factors for PVTT. We suggest that patients with a high risk of PVTT progression should be followed up regularly and closely. Once HCC progression has been detected, appropriate treatment modalities should be selected according to current HCC treatment guidelines. Notably, there is a significant gender disparity in liver cancer, with men experiencing more than twice the incidence and mortality rates compared to women.1 This gender difference may be attributed to the influence of sex hormones; estrogen exerts a protective effect against HCC in women, while testosterone promotes liver cancer cell proliferation by inhibiting adiponectin.26,27 AAPR, being an easily accessible non-invasive biomarker, may serve as an indicator of a patient’s nutritional status and liver function. Its prognostic value in HCC has been substantiated by several studies.13,14 Regrettably, due to the limited number of PVTT events in our study, we were unable to establish an ideal PVTT prediction model. The C-index of the model only reached 0.649 and 0.691 in the internal and external validation cohorts, respectively (these results are not displayed). Furthermore, multi-omics analyses (such as genomics, metabolomics, and transcriptomics) gained growing attention in the study of HCC, which can help to find the key molecules or therapeutic targets, and also contribute to elucidating the potential pathogenesis of PVTT.28 A reliable tool for assessing drugs is essential in the development of anti-HCC drugs depending on the corresponding molecules or targets.29
Currently, there is a scarcity of reliable methods or tools available for predicting the prognosis of HBV-related HCC patients who have yet to develop PVTT. In this study, we successfully identified independent risk factors for both OS and PFS within the training cohort using multivariate Cox analysis. Subsequently, we developed and validated two novel prognostic models for predicting OS and PFS in HBV-related HCC patients who do not present with PVTT (Figures 4 and 5). The C-indexes for OS and PFS prediction were 0.795 and 0.733 in the training cohort, 0.765 and 0.716 in the internal validation cohort, and 0.780 and 0.722 in the external validation cohort, respectively. This consistency between predicted and observed outcomes across different cohorts underscores the robust prediction performance of our models. Furthermore, the AUC values from time-dependent ROC analysis at 1-year, 3-year, and 5-year intervals for both OS and PFS exceeded 0.79 across all cohorts, which indicated that our models had high prediction accuracy. The DCA plots demonstrated that our models had superior net benefits in clinical applications when compared to traditional staging systems. Additionally, our models allowed for risk stratification of patients into low-, medium-, and high-risk groups based on their OS and PFS nomogram scores, as evidenced by KM curve analysis. This stratification effectively distinguished patients with distinct prognoses, with p-values <0.001 for all groups. Even in patients classified under the same BCLC stages, our models exhibited satisfactory discriminatory ability. Particularly noteworthy is the ability of our models to differentiate low-, medium-, and high-risk BCLC stage B patients, revealing significant differences in both OS and PFS (p<0.001 for all, Figure 6B and E), thereby enhancing prognostic assessment in this subgroup of patients. This finding offers valuable insights into improving prognostic stratification within the BCLC stage B category, where patients often exhibit varying outcomes despite similar treatment modalities.11,12
Indeed, hepatocarcinogenesis is a complex and multifaceted process involving various factors and stages, including sustained hepatocyte damage, necrosis, regeneration, and hepatic fibrosis. Consequently, the accurate assessment of the degree of liver injury and fibrosis is important for predicting the prognosis of HCC patients.30 Multiple studies have consistently demonstrated that non-invasive biomarkers such as the AAR, APRI, and ALBI grade can effectively evaluate liver function reserve and the extent of hepatic fibrosis. These biomarkers have shown significant associations with the prognosis of HCC patients.15–17,31,32 AAR is calculated from the serum AST and ALT levels and serves as a sensitive indicator of hepatocellular injury. ALT is predominantly located in the cytoplasm, while AST is found in both the cytoplasm and mitochondria. When cellular and mitochondrial membrane integrity is compromised, ALT and AST are released into the bloodstream, leading to elevated serum ALT and AST levels. Tumor cells, driven by their high energy demands for rapid proliferation, often exhibit increased aerobic glycolysis, which enhances glucose uptake.33 AST plays a crucial role in the malate-aspartate shuttle pathway, and its activity, as well as the AST/ALT ratio, is frequently elevated in cancer patients.34 AAR may thus reflect the metabolic state of the tumor and its connection to tumor growth, progression, and ultimately, prognosis.35 PLT can promote tumor angiogenesis by secreting various cytokines, particularly vascular endothelial growth factor (VEGF), and help tumor cells escape from immune surveillance and immune clearance by wrapping around the tumor cells, which contributes to tumor progression and metastasis.36,37 In HCC, more than 80% of patients have underlying cirrhosis or fibrosis,38 often accompanied by portal hypertension and hypersplenism, which can lead to thrombocytopenia. This condition helps explain the relatively high value of APRI in HCC patients, as PLT levels serve as the denominator in the calculation of APRI. Owing to methodological differences and patient heterogeneity, the optimal cut-off value of non-invasive biomarkers remains controversial. We propose that AAR >0.965 and APRI >0.48 are associated with poor OS and PFS, and APRI >0.48 is also related to a higher risk of PVTT event.
The ALBI grade, a simple and objective index, is calculated using serum ALB and TBIL levels. It has gained widespread acceptance for assessing liver function and predicting the prognosis of HCC patients, because of its superior discriminatory ability in prognostication compared to the Child-Pugh score and is generally applicable to patients across various BCLC stages.31,32 Our findings provide further affirmation of the ALBI grade’s prognostic predictive capability for HBV-related HCC patients without PVTT. Ascites, a parameter integral to the Child-Pugh score, serve as an important indicator of liver synthetic and reserve function. Hypoproteinemia and portal hypertension contribute to the development of ascites. Patients typically enter a stage of hepatic decompensation once ascites appear. Furthermore, the incidence of complications related to ascites increases over time, and HCC patients with ascites often face significantly higher mortality rates.39 Our study has underscored the relationship between the presence of ascites and OS and PFS in HCC patients. Previous studies found that older HCC patients had poorer prognoses than younger counterparts. This age-related difference may be attributed to younger patients having fewer underlying diseases, which allows them to tolerate and often receive more aggressive treatment regimens.17,40 Our study’s results confirm that age over 60 years is an independent risk factor for reduced OS.
Tumor-related features, including extrahepatic metastasis, PVTT event, tumor diameter, tumor number, and AFP levels, hold a vital position in both of the prognostic models developed in this study. Extrahepatic metastasis is a sign of advanced tumor-node-metastasis (TNM) stage in HCC and is associated with an unfavorable prognosis. It is estimated to occur in approximately 10% of newly diagnosed HCC patients,41 and our study’s findings (12.9%) align with these statistics. To some extent, extrahepatic metastasis, along with PVTT events, can serve as indicators of the degree of malignancy and invasive potential of HCC. Larger tumor diameters indicate an increased likelihood of capsule invasion, microvascular invasion (MVI), and the occurrence of satellite nodules.42 The higher number of the tumor might imply that the micrometastatic nodule has already been present which was too small to be detected on imaging examination. AFP, a widely used tumor marker for diagnosis and treatment efficacy evaluation, plays an important role in the formation, growth, and proliferation of HCC.43 However, approximately 30–40% of HCC patients are AFP-negative, the percentage was even higher in early-stage patients with a smaller tumor diameter, limiting its diagnostic and prognostic applicability.44,45 Nevertheless, the prognostic value of AFP has been supported by our study. Furthermore, the prognostic value of HBV-DNA load was not observed in this study, this may be attributed to the fact that all patients received anti-HBV treatment. It is worth mentioning that Hu et al suggested that the prognosis of HBV-related HCC patients with elevated baseline HBV loads could potentially improve after receiving anti-HBV treatment.46
Despite models demonstrating satisfactory discriminatory ability and prognostic value, our study still has several limitations. Firstly, it is important to note that our study was a retrospective study, which introduces the possibility of selective bias. Secondly, the two nomogram models were developed based on data from HBV-related HCC patients, and it remains unknown whether these models would apply to other non-HBV-infected HCC patients. Additionally, a prospective, large-sample, and multicenter study is needed to validate the two novel nomogram models in the future.
Conclusion
Pretreatment non-invasive biomarkers were independent risk factors for PVTT event, OS, and PFS in HBV-related HCC patients without PVTT. In our study, approximately 13.3% of patients experienced PVTT events, and patients with PVTT had poorer OS and PFS than those without PVTT. We successfully developed two nomogram models to predict both PFS and OS for HBV-related HCC patients without PVTT. Models have good prediction performance, and superior net benefit in clinical applications than traditional staging systems, which have been internally and externally validated. They can distinguish patients with different prognoses, and their discriminatory ability remained consistently satisfactory even among patients within the same BCLC stages.
Data Sharing Statement
The data presented in this study are available from the corresponding author upon reasonable request.
Ethics Approval and Informed Consent
This study strictly followed the principles outlined in the Declaration of Helsinki and adhered to current ethical guidelines. The study was approved by the Ethics Committee of 900TH Hospital of Joint Logistics Support Force, with the assigned Ethics Approval Number: 2022-014. Due to the retrospective nature of the study and the analysis being conducted anonymously, informed consent was exempted from the participants.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work. Bang Liu, Jia Liu, and Xuan Mei contributed the same to the manuscript.
Funding
This study was supported by Guiding Projects of Social Development of Fujian Province (Grant number: 2021Y0062) and 900TH Hospital of Joint Logistics Support Force Fund (Grant number: 2020Q02, 2020L25, 2021MS12, and 2021MS22).
Disclosure
The authors have no conflicts of interest to disclose.
References
1. Sung H, Ferlay J, Siegel RL, et al. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. Ca a Cancer J Clinicians. 2021;71(3):209–249. doi:10.3322/caac.21660
2. Llovet JM, Kelley RK, Villanueva A, et al. Hepatocellular carcinoma. Nature Reviews Disease Primers. 2021;7(1):6. doi:10.1038/s41572-020-00240-3
3. Rumgay H, Arnold M, Ferlay J, et al. Global burden of primary liver cancer in 2020 and predictions to 2040. J Hepatol. 2022;77(6):1598–1606. doi:10.1016/j.jhep.2022.08.021
4. Lin J, Zhang H, Yu H, et al. Epidemiological characteristics of primary liver cancer in mainland china from 2003 to 2020: a representative multicenter study. Front Oncol. 2022;12:906778. doi:10.3389/fonc.2022.906778
5. Cui F, Blach S, Manzengo Mingiedi C, et al. Global reporting of progress towards elimination of hepatitis B and hepatitis C. Lancet Gastroenterol Hepatol. 2023;8(4):332–342. doi:10.1016/S2468-1253(22)00386-7
6. Hou JL, Zhao W, Lee C, et al. Outcomes of long-term treatment of chronic HBV infection with entecavir or other agents from a randomized trial in 24 countries. Clin Gastroenterol Hepatol. 2020;18(2):457–467.e421. doi:10.1016/j.cgh.2019.07.010
7. Lu J, Zhang XP, Zhong BY, et al. Management of patients with hepatocellular carcinoma and portal vein tumour thrombosis: comparing east and west. Lancet Gastroenterol Hepatol. 2019;4(9):721–730. doi:10.1016/S2468-1253(19)30178-5
8. Liu PH, Huo TI, Miksad RA. Hepatocellular carcinoma with portal vein tumor involvement: best management strategies. Semin Liver Disease. 2018;38(3):242–251. doi:10.1055/s-0038-1666805
9. Wang JC, Xia AL, Xu Y, Lu XJ. Comprehensive treatments for hepatocellular carcinoma with portal vein tumor thrombosis. J Cell Physiol. 2019;234(2):1062–1070. doi:10.1002/jcp.27324
10. Wei X, Li N, Li S, et al. Hepatitis B virus infection and active replication promote the formation of vascular invasion in hepatocellular carcinoma. BMC Cancer. 2017;17(1):304. doi:10.1186/s12885-017-3293-6
11. Zhong JH, Ke Y, Gong WF, et al. Hepatic resection associated with good survival for selected patients with intermediate and advanced-stage hepatocellular carcinoma. Ann Surg. 2014;260(2):329–340. doi:10.1097/SLA.0000000000000236
12. Zhaohui Z, Shunli S, Bin C, et al. Hepatic resection provides survival benefit for selected intermediate-stage (BCLC-B) hepatocellular carcinoma patients. Cancer Res Treat. 2019;51(1):65–72. doi:10.4143/crt.2018.038
13. Chen ZH, Zhang XP, Cai XR, et al. The predictive value of albumin-to-alkaline phosphatase ratio for overall survival of hepatocellular carcinoma patients treated with trans-catheter arterial chemoembolization therapy. J Cancer. 2018;9(19):3467–3478. doi:10.7150/jca.26120
14. Li Q, Lyu Z, Wang L, Li F, Yang Z, Ren W. Albumin-to-alkaline phosphatase ratio associates with good prognosis of hepatitis B virus-positive HCC patients. Onco Targets Ther. 2020;13:2377–2384. doi:10.2147/OTT.S242034
15. Zhang LX, Lv Y, Xu AM, Wang HZ. The prognostic significance of serum gamma-glutamyltransferase levels and AST/ALT in primary hepatic carcinoma. BMC Cancer. 2019;19(1):841. doi:10.1186/s12885-019-6011-8
16. Zhang Y, Zhang X. Prognostic value of aspartate aminotransferase to platelet ratio index as a noninvasive biomarker in patients with hepatocellular carcinoma: a meta-analysis. Cancer Manage Res. 2018;10:3023–3032. doi:10.2147/CMAR.S174095
17. Kuo YH, Huang TH, Yen YH, et al. Nomogram to predict the long-term overall survival of early-stage hepatocellular carcinoma after radiofrequency ablation. Cancers. 2023;15(12). doi:10.3390/cancers15123156
18. Toyoda H, Kumada T, Tada T, Kaneoka Y, Maeda A. A laboratory marker, FIB-4 index, as a predictor for long-term outcomes of hepatocellular carcinoma patients after curative hepatic resection. Surgery. 2015;157(4):699–707. doi:10.1016/j.surg.2014.10.022
19. Berardi G, Morise Z, Sposito C, et al. Development of a nomogram to predict outcome after liver resection for hepatocellular carcinoma in Child-Pugh B cirrhosis. J Hepatol. 2020;72(1):75–84. doi:10.1016/j.jhep.2019.08.032
20. Serenari M, Han KH, Ravaioli F, et al. A nomogram based on liver stiffness predicts postoperative complications in patients with hepatocellular carcinoma. J Hepatol. 2020;73(4):855–862. doi:10.1016/j.jhep.2020.04.032
21. Johnson PJ, Berhane S, Kagebayashi C, et al. Assessment of liver function in patients with hepatocellular carcinoma: a new evidence-based approach-The ALBI grade. J Clin Oncol. 2015;33(6):550–558. doi:10.1200/JCO.2014.57.9151
22. Cheng S, Chen M, Cai J, et al. Chinese expert consensus on multidisciplinary diagnosis and treatment of hepatocellular carcinoma with portal vein tumor thrombus (2018 Edition). Liver Cancer. 2020;9(1):28–40. doi:10.1159/000503685
23. Park JW, Chen M, Colombo M, et al. Global patterns of hepatocellular carcinoma management from diagnosis to death: the BRIDGE Study. Liver Internat. 2015;35(9):2155–2166. doi:10.1111/liv.12818
24. Guarino M, Cucchetti A, Pontillo G, et al. Pattern of macrovascular invasion in hepatocellular carcinoma. Eur J Clin Invest. 2021;51(7):e13542. doi:10.1111/eci.13542
25. Tortora R, Farella N, Morisco F, et al. Development of a risk score to predict portal vein tumor thrombosis in patients with hepatocellular carcinoma. Eur J Gastroenterol Hepatol. 2023;35(7):734–741. doi:10.1097/MEG.0000000000002549
26. Yu MW, Chang HC, Chang SC, et al. Role of reproductive factors in hepatocellular carcinoma: impact on hepatitis B- and C-related risk. Hepatology. 2003;38(6):1393–1400. doi:10.1016/j.hep.2003.09.041
27. Manieri E, Herrera-Melle L, Mora A, et al. Adiponectin accounts for gender differences in hepatocellular carcinoma incidence. J Exp Med. 2019;216(5):1108–1119. doi:10.1084/jem.20181288
28. Triozzi PL, Stirling ER, Song Q, et al. Circulating immune bioenergetic, metabolic, and genetic signatures predict melanoma patients’ response to Anti-PD-1 immune checkpoint blockade. Clin Can Res. 2022;28(6):1192–1202. doi:10.1158/1078-0432.CCR-21-3114
29. Lu Z, Priya Rajan SA, Song Q, et al. 3D scaffold-free microlivers with drug metabolic function generated by lineage-reprogrammed hepatocytes from human fibroblasts. Biomaterials. 2021;269:120668. doi:10.1016/j.biomaterials.2021.120668
30. Zhang DY, Friedman SL. Fibrosis-dependent mechanisms of hepatocarcinogenesis. Hepatology. 2012;56(2):769–775. doi:10.1002/hep.25670
31. Hiraoka A, Kumada T, Michitaka K, Kudo M. Newly proposed ALBI Grade and ALBI-T score as tools for assessment of hepatic function and prognosis in hepatocellular carcinoma patients. Liver Cancer. 2019;8(5):312–325. doi:10.1159/000494844
32. Pinato DJ, Sharma R, Allara E, et al. The ALBI grade provides objective hepatic reserve estimation across each BCLC stage of hepatocellular carcinoma. J Hepatol. 2017;66(2):338–346. doi:10.1016/j.jhep.2016.09.008
33. Vander Heiden MG, Cantley LC, Thompson CB. Understanding the Warburg effect: the metabolic requirements of cell proliferation. Science. 2009;324(5930):1029–1033. doi:10.1126/science.1160809
34. Greenhouse WV, Lehninger AL. Occurrence of the malate-aspartate shuttle in various tumor types. Cancer Res. 1976;36(4):1392–1396.
35. Wu J, Chen L, Wang Y, Tan W, Huang Z. Prognostic value of aspartate transaminase to alanine transaminase (De Ritis) ratio in solid tumors: a pooled analysis of 9400 patients. Onco Targets Ther. 2019;12:5201–5213. doi:10.2147/OTT.S204403
36. Franco AT, Corken A, Ware J. Platelets at the interface of thrombosis, inflammation, and cancer. Blood. 2015;126(5):582–588. doi:10.1182/blood-2014-08-531582
37. Schlesinger M. Role of platelets and platelet receptors in cancer metastasis. J Hematol Oncol. 2018;11(1):125. doi:10.1186/s13045-018-0669-2
38. Singal AG, Llovet JM, Yarchoan M, et al. AASLD practice guidance on prevention, diagnosis, and treatment of hepatocellular carcinoma. Hepatology. 2023;2023:1.
39. Ndow G, Vo-Quang E, Shimakawa Y, et al. Clinical characteristics and outcomes of patients with cirrhosis and hepatocellular carcinoma in The Gambia, West Africa: a prospective cohort study. Lancet Glob Health. 2023;11(9):e1383–e1392. doi:10.1016/S2214-109X(23)00263-2
40. Xu XS, Chen W, Miao RC, et al. Survival analysis of hepatocellular carcinoma: a comparison between young patients and aged patients. Chinese Med J. 2015;128(13):1793–1800. doi:10.4103/0366-6999.159356
41. Hsu CY, Liu PH, Ho SY, et al. Metastasis in patients with hepatocellular carcinoma: prevalence, determinants, prognostic impact and ability to improve the Barcelona clinic liver cancer system. Liver Internat. 2018;38(10):1803–1811. doi:10.1111/liv.13748
42. Pawlik TM, Delman KA, Vauthey JN, et al. Tumor size predicts vascular invasion and histologic grade: implications for selection of surgical treatment for hepatocellular carcinoma. Liver Transplant. 2005;11(9):1086–1092. doi:10.1002/lt.20472
43. Mizejewski GJ. Does alpha-fetoprotein contribute to the mortality and morbidity of human hepatocellular carcinoma? A commentary. J Hepatocell Carcinoma. 2016;3:37–40. doi:10.2147/JHC.S114198
44. Farinati F, Marino D, De Giorgio M, et al. Diagnostic and prognostic role of alpha-fetoprotein in hepatocellular carcinoma: both or neither? Am J Gastroenterol. 2006;101(3):524–532. doi:10.1111/j.1572-0241.2006.00443.x
45. Giannini EG, Marenco S, Borgonovo G, et al. Alpha-fetoprotein has no prognostic role in small hepatocellular carcinoma identified during surveillance in compensated cirrhosis. Hepatology. 2012;56(4):1371–1379. doi:10.1002/hep.25814
46. Hu Z, Sun X, Mei J, et al. Antiviral treatments eliminate the adverse impacts of high baseline HBV loads on the survival of HBV-Related HCC patients. J Hepatocell Carcinoma. 2022;9:315–325. doi:10.2147/JHC.S363123
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Histological Severity of Cirrhosis Influences Surgical Outcomes of Hepatocellular Carcinoma After Curative Hepatectomy
Liang BY, Gu J, Xiong M, Zhang EL, Zhang ZY, Lau WY, Wang SF, Guan Y, Chen XP, Huang ZY
Journal of Hepatocellular Carcinoma 2022, 9:633-647
Published Date: 23 July 2022
A Nomogram Based on SEER Database for Predicting Prognosis in Patients with Mucinous Ovarian Cancer: A Real-World Study
Zhang K, Feng S, Ge Y, Ding B, Shen Y
International Journal of Women's Health 2022, 14:931-943
Published Date: 26 July 2022
Nomogram for the Preoperative Prediction of the Macrotrabecular-Massive Subtype of Hepatocellular Carcinoma
Shan Y, Yu X, Yang Y, Sun J, Wu S, Mao S, Lu C
Journal of Hepatocellular Carcinoma 2022, 9:717-728
Published Date: 10 August 2022
Establishment and Validation of a Model for Disease-Free Survival Rate Prediction Using the Combination of microRNA-381 and Clinical Indicators in Patients with Breast Cancer
Shen J, Wang M, Li F, Yan H, Wang R, Zhou J
Breast Cancer: Targets and Therapy 2022, 14:375-389
Published Date: 30 November 2022
Development and Validation of a Novel Nomogram Integrated with Hypoxic and Lactate Metabolic Characteristics for Prognosis Prediction in Hepatocellular Carcinoma
Qiu X, Dong L, Wang K, Zhong X, Xu H, Xu S, Guo H, Wei X, Chen W, Xu X
Journal of Hepatocellular Carcinoma 2024, 11:241-255
Published Date: 2 February 2024