Back to Journals » Drug Design, Development and Therapy » Volume 20
Preoperative Stellate Ganglion Block for Postoperative Sore Throat in Patients Undergoing Double-Lumen Endotracheal Intubation: A Randomized Clinical Trial
Authors Cong P ![]() , Tan Y
, Tan Y ![]() , Li H, Zhang H, Zhang L, Jin Y, Shan L, Zhao Y, Jin Y
, Li H, Zhang H, Zhang L, Jin Y, Shan L, Zhao Y, Jin Y ![]() , Wu Q, Chen Z
, Wu Q, Chen Z ![]() , Li N
, Li N
Received 20 March 2026
Accepted for publication 14 May 2026
Published 27 May 2026 Volume 2026:20 610843
DOI https://doi.org/10.2147/DDDT.S610843
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Tin Wui Wong
Peilin Cong,1,* Yawen Tan,2,* Huiyin Li,2 He Zhang,2 Le Zhang,2 Yuelong Jin,3 Lei Shan,4 Yunpeng Zhao,4 Yanwu Jin,5 Qianqian Wu,1 Zheping Chen,1 Ning Li2
1Shanghai Key Laboratory of Anesthesiology and Brain Functional Modulation, Translational Research Institute of Brain and Brain-Like Intelligence, Clinical Research Center for Anesthesiology and Perioperative Medicine, Department of Anesthesiology and Perioperative Medicine, Shanghai Fourth People’s Hospital, School of Medicine, Tongji University, Shanghai, People’s Republic of China; 2Department of Anesthesiology, The Second Qilu Hospital, Cheeloo College of Medicine, Shandong University, Jinan, People’s Republic of China; 3Department of Epidemiology and Biostatistics, School of Public Health, Wannan Medical University/ Institute of Chronic Disease Prevention and Control, Wuhu, People’s Republic of China; 4Department of Thoracic Surgery, The Second Qilu Hospital, Cheeloo College of Medicine, Shandong University, Jinan, People’s Republic of China; 5Department of Anesthesiology and Perioperative Medicine, Shandong Public Health Clinical Center, Shandong University, Jinan, Shandong, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Zheping Chen, Shanghai Key Laboratory of Anesthesiology and Brain Functional Modulation, Translational Research Institute of Brain and Brain-Like Intelligence, Clinical Research Center for Anesthesiology and Perioperative Medicine, Department of Anesthesiology and Perioperative Medicine, Shanghai Fourth People’s Hospital, School of Medicine, Tongji University, 1279 Sanmen Road, Hongkou District, Shanghai, 200434, People’s Republic of China, Email [email protected] Ning Li, Department of Anesthesiology, The Second Qilu Hospital, Cheeloo College of Medicine, Shandong University, 247 Bei Yuan Street, Jinan, Shandong, 250033, People’s Republic of China, Email [email protected]
Background: As a common complication of double-lumen endobronchial tube (DLT) intubation during thoracic surgery, postoperative sore throat (POST) brings adverse impacts on patient recovery. Although stellate ganglion block (SGB) can modulate sympathetic tone and inflammatory reactions, its efficacy in preventing DLT-related POST is still inconclusive. This trial aimed to determine whether SGB reduces the incidence of POST at 6 h after surgery in patients undergoing DLT intubation.
Methods: In this single-center prospective randomized controlled trial, 124 patients undergoing elective thoracic surgery with left-sided DLT intubation were randomized 1:1 to two groups: the intervention group received preoperative ultrasound-guided right-sided SGB (5 mL of 0.5% ropivacaine), and the control group received standard care (ultrasound scanning without injection plus 1% tetracaine gel lubrication). The primary endpoint was the incidence of POST at 6 h after surgery.
Results: Of the 124 randomized patients, 111 eligible subjects were finally included in the full analysis. The incidence of POST at 6 h after surgery, was significantly decreased in the ultrasound-guided SGB intervention group compared with the standard care control group (14.3% vs 38.2%; RR = 0.37; 95% CI: 0.18– 0.77; P = 0.008). This significant protective effect of SGB against POST was consistently observed at the early postoperative time point of 2 h (P = 0.017) and sustained up to 24 h after surgery (P = 0.036). SGB also significantly reduced POST severity at all time points, lowered sleep disturbance rate and improved anxiety/depression scores at 24 h after surgery (all P < 0.05). No between-group differences were observed in the incidence or severity of hoarseness or in other outcomes, and no notable complications occurred.
Conclusion: Preoperative ropivacaine-based SGB could reduce the incidence and severity of POST in patients for DLTs in thoracic surgery, with this protective effect persisting for at least 24 h after surgery. These preliminary results require validation in larger multicenter studies.
Clinical Trial Registration: Chinese Clinical Trial Registry, ChiCTR2400092313.
Keywords: postoperative sore throat, stellate ganglion block, anxiety, double-lumen endobronchial tube, thoracic surgery
Introduction
Postoperative sore throat (POST) is widely recognized as one of the most frequent and patient-distressing perioperative complications secondary to general anesthesia (GA), and existing published literature has documented that the incidence of this complication varies from 12.1% to 70% depending on patient population, type of tracheal tube, intubation technique, and the timing and definition of POST assessment.1,2 Although POST is typically self-limiting, it significantly impairs patient satisfaction and the quality of postoperative recovery, and has garnered considerable attention from anesthesiologists in recent years.3–13
Patients undergoing video-assisted thoracic surgery requiring double-lumen endobronchial tube (DLT) intubation represent an extremely high-risk population for POST.14,15 DLTs are routinely utilized to establish one-lung ventilation (OLV) during thoracic surgical procedures, as they facilitate lung collapse and precise exposure of the operative site, thereby providing an optimal surgical field for thoracic interventions.14,16,17 A prominent limitation of DLT use, however, is its larger outer diameter and greater rigidity; additionally, optimal tube positioning often necessitates repeated adjustments with a fiberoptic bronchoscope (FB) following intubation.14,18 These factors collectively cause pronounced mechanical trauma to the pharyngeal mucosa, vocal cords, and tracheal mucosa, triggering a local inflammatory cascade and neurogenic inflammation driven by sympathetic overactivation, thereby contributing to both the high incidence and the prolonged duration of POST. Existing clinical studies have demonstrated that 41.5% to 70% of patients report moderate to severe POST within 6 hours after DLT intubation, and a considerable proportion of these patients experience persistent POST symptoms for more than 24 hours.19–21
Several prophylactic strategies have been developed to mitigate DLT-associated POST, including pharmacological interventions (eg, preoperative dexamethasone,22 licorice gargle,23 esketamine gargle,24 magnesium sulfate5), non-pharmacological and technical modifications (eg, video DLTs,25 two-handed jaw thrust,26 fibreoptic-guided advance DLTs,27 180° rotation technique,20 thermal softening of DLTs21), and our previously reported preoperative ultrasound-guided block of the internal branch of the superior laryngeal nerve (SLNB).28 While these approaches have demonstrated varying degrees of clinical efficacy, they all harbor inherent limitations. For instance, SLNB only achieves sensory denervation of supraglottic structures, leaving the subglottic airway—innervated by the recurrent laryngeal nerve—unprotected; additionally, its prophylactic effect against POST over extended postoperative timeframes (eg, 24 h) is limited due to the intrinsic pharmacodynamic properties of local anesthetics (LA). Furthermore, none of these interventions directly target the sympathetic overactivation and neurogenic inflammation triggered by DLT‑induced mechanical trauma. This trauma initiates robust sympathetic drive, which promotes the release of proinflammatory mediators, amplifies nociceptive signaling, and prolongs pain sensitization. This sympathetic‑mediated cascade represents a core mechanism sustaining POST persistence, yet it remains unaddressed by current prophylactic strategies, particularly for DLTs.
Stellate ganglion block (SGB) has garnered increasing attention for its capacity to modulate sympathetic tone and suppress the systemic inflammatory response.29 By blocking sympathetic efferent fibers and reducing the release of proinflammatory cytokines, SGB exerts pleiotropic effects that extend beyond simple sympathetic blockade, including analgesia, post-traumatic stress disorder (PTSD) management, and improved sleep quality and cognitive function.29–32 Of note, a recent randomized controlled trial (RCT) has documented that preoperative SGB can markedly reduce both the incidence and severity of POST after tracheal intubation in patients undergoing lumbar spinal surgery.33 However, whether these beneficial effects can be extended to the high-risk population of patients undergoing thoracic surgery with DLT intubation remains elusive. Beyond its potential airway-protective properties, SGB may confer additional advantages to thoracic surgical patients, such as improvements in sleep and emotional status.
Therefore, we hypothesized that preoperative SGB would reduce the incidence and severity of POST in patients undergoing thoracic surgery with left-sided DLT intubation. Secondary objectives included exploring its effects on hoarseness, postoperative sleep quality, anxiety/depression status, and safety outcomes. This study aims to provide a novel clinical strategy and high-level evidence for the prevention of DLT-related POST.
Methods
Study Design
This single-center prospective randomized controlled trial was performed at The Second Qilu Hospital of Shandong University (Jinan, China) from December 2024 to December 2025, enrolling 124 patients undergoing thoracic surgery under GA. The full trial protocol with full methodological details has been reported in our previously published work.34
Ethical Approval
Full ethical approval for this study protocol was granted by the Institutional Review Board of the Second Qilu Hospital of Shandong University (approval number: KYLL-2024-880) on October 31, 2024. Prior to the initiation of patient recruitment, this trial was prospectively registered in the Chinese Clinical Trial Registry (registration number: ChiCTR2400092313; registration date: November 14, 2024). All study procedures were implemented in strict compliance with the ethical principles set forth in the Declaration of Helsinki. Written informed consent was acquired from every eligible participant before recruitment into the trial, and the entire research process was conducted in full adherence to the Consolidated Standards of Reporting Trials (CONSORT) 2025 guidelines.
Patients
Eligible patients were aged ≥18 years, ASA physical status I–III, scheduled for elective thoracic surgery requiring right-sided OLV via left-sided DLT intubation, consistent with the published protocol.34 Exclusion criteria included: patient refusal; contraindications to GA or SGB (coagulopathy, local/systemic infection); predicted difficult airway; preoperative sore throat/cough; upper respiratory tract infection within 2 weeks; prior oral/pharyngeal surgery; asthma/ chronic obstructive pulmonary disease (COPD); hypertension/coronary artery disease (CAD) with long-term hemodynamic medication use; cortisol-related metabolic disorders; severe hepatic/renal dysfunction; diabetes or poor glycemic control; severe bradycardia, sick sinus syndrome or high-grade atrioventricular block; and severe cognitive/language impairment.34
Randomization and Blinding
Allocation concealment was performed using sequentially numbered opaque sealed envelopes, generated with a 1:1 allocation ratio via the Sealed Envelope online randomization tool (https://www.sealedenvelope.com/simple-randomiser/v1/lists) with block sizes of 2 and 4. Envelopes were opened only by an independent research anesthesiologist immediately before the scheduled SGB procedure. This anesthesiologist had no involvement in any other study-related procedures throughout the trial. All SGB procedures were conducted by a single senior anesthesiologist with extensive experience in regional anesthesia and ultrasound-guided nerve blocks. The anesthesiologist performing DLT intubation was aware of group allocation solely due to the requirement for tracheal lubrication during DLT intubation in the control group; however, this individual had no involvement in any other trial-related procedures. All other study staff, intraoperative anesthesia providers, independent outcome assessors, and follow-up researchers remained fully blinded to group allocation for the entire study.
Interventions
Eligible participants were allocated at a 1:1 ratio via randomization to either the SGB group or the control group. For patients allocated to the SGB group, right-sided SGB was administered 30 minutes before the initiation of GA. Given that all patients underwent right‑sided thoracic surgery requiring left‑sided DLTs, right‑sided SGB was chosen for its superior perioperative safety and for its ability to deliver the block ipsilaterally to the operative side, where surgical stress and sympathetic activation are most pronounced.33,35 Patients were positioned supine with the head slightly left-rotated. A 6–13 MHz high-frequency linear ultrasound transducer was placed transversely at the cricoid cartilage level, then moved laterally to identify the C6 vertebral transverse process. The probe was moved caudally to the C7 vertebral level until the C6 anterior tubercle was no longer visible. After negative aspiration to rule out intravascular or intrathecal injection, 5 mL of 0.5% ropivacaine was injected at the surface of the longus colli muscle beneath its anterior fascia, with the full procedure performed in strict accordance with our previously published study protocol (Figure 1).34 Successful SGB was confirmed by the onset of complete Horner’s syndrome. The control group received ultrasound-guided stellate ganglion scanning without injection, plus 1% tetracaine gel lubrication before intubation as standard POST prevention care. The SGB group did not receive tetracaine gel lubrication.
 |
Figure 1 Ultrasound-guided SGB. (A) Sonographic illustration of SGB. (B) Post SGB injection. * Injection site of LA. Abbreviations: SGB, stellate ganglion block; SCM, sternocleidomastoid muscle; LCo, longus colli; LCap, longus capitis muscle; CCA, common carotid artery; IJV, internal jugular vein; LA, local anesthetics; N6, C6 nerve root. |
Perioperative Anesthesia Management
Standard intraoperative monitoring included invasive blood pressure, HR, EEG, pulse oximetry and bispectral index (BIS). GA was induced with intravenous sufentanil (0.3 μg·kg−1), propofol (1.5–3.0 mg·kg−1) and rocuronium bromide (0.7 mg·kg−1) for neuromuscular blockade, with 100% oxygen assisted ventilation during induction.
Left‑sided DLT intubation was performed by an experienced attending anesthesiologist using direct laryngoscopy with a curved Macintosh blade and a disposable left‑sided DLT, with the patient’s head supported on a headrest. The DLT size was chosen according to institutional guidelines based on patient sex and height.28 Once the bronchial tip had passed through the glottis, the stylet was removed; the DLT was then rotated 90° counterclockwise to direct the bronchial tip toward the left main bronchus and advanced to the pre‑estimated depth.28 If significant resistance was encountered at the glottis, the tube was further rotated counterclockwise up to 180° to guide the tracheal lumen anteriorly, and advancement was re‑attempted.28 Correct positioning was confirmed by fiberoptic bronchoscopy after the patient was placed in the lateral decubitus position. Only patients successfully intubated on the first attempt were included.
OLV was delivered with a tidal volume (TV) of 5–7 mL·kg−1, respiratory rate of 14–16 breaths/min, and positive end-expiratory pressure (PEEP) of 3–10 cmH2O. Anesthesia was maintained with sevoflurane (1–2% in 50% oxygen), propofol, remifentanil, and supplemental rocuronium as needed, with BIS values kept between 40 and 60. Vasoactive agents were titrated as needed to maintain hemodynamics within ± 20% of pre-induction baselines. Upon completion of surgery, the DLT was extubated once adequate spontaneous respiration was restored, defined as a tidal volume > 6 mL·kg−1, SpO2 > 95%, BIS > 90, and muscle strength recovery to ≥ grade IV.
As part of the standard perioperative analgesic protocol, all patients received an ultrasound‑guided T5–T6 thoracic paravertebral block with 10–15 mL of 0.5% ropivacaine before induction of GA. Postoperative pain was managed with patient-controlled intravenous analgesia (PCIA) containing sufentanil 100 μg, ondansetron 8 mg, and 0.9% normal saline to a total volume of 100 mL. Rescue analgesia (NSAIDs, oral analgesics, intravenous pethidine) was given as needed to maintain resting VAS pain scores < 4.
Study Outcomes
The primary outcome was the incidence of POST at 6 h after surgery.26,28 POST and hoarseness were assessed using a 4-grade scale (none, mild, moderate, severe) at 2, 6, and 24 h postoperatively (Supplementary Table 1).28 Secondary outcomes included: (1) incidence of postoperative sore throat at 2 and 24 h; (2) severity of POST at 2, 6, and 24 h; (3) incidence and severity of hoarseness at 2, 6, and 24 h (Supplementary Table 1); (4) sleep disturbance assessed using the Numeric Rating Scale (NRS)-sleep and Athens Insomnia Scale (AIS) preoperatively and on postoperative day 1; (5) anxiety and depression assessed using the Hospital Anxiety and Depression Scale (HADS) preoperatively and at 24 h; and (6) intraoperative hemodynamic parameters.
Exploratory outcomes included duration of post-anesthesia care unit (PACU) stay and length of postoperative hospital stay. Safety outcomes covered perioperative adverse events, especially SGB procedure-related complications (LA systemic toxicity, hematoma, infection, pneumothorax, recurrent laryngeal or phrenic nerve block, and brachial plexus block).
Sample Size Calculation
Sample size was calculated using chi-square test based on previously published studies reporting an incidence of postoperative sore throat at 6 h after DLT intubation ranging from 41.5% to 59%, with a mean incidence of 50.25%.26,28 Based on previous publications, we hypothesized that preoperative SGB would yield an absolute risk reduction (ARR) of 30 percentage points in the incidence of POST, from 50.25% to 20.25%.28,33,36,37 Sample size calculation was performed with a two-sided α of 0.05 and 90% statistical power, requiring 49 patients per group. Considering a 20% anticipated dropout rate, 62 patients were enrolled in each group, with a total sample size of 124 participants. All calculations were completed using PASS 15.0 software (NCSS, LLC., Kaysville, UT, USA).
Statistical Analysis
Baseline balance was assessed using absolute standardized differences (ASD), with a value ≥ 0.352 ( ) defined as imbalance.38 The Kolmogorov–Smirnov test was used to test the normality of continuous variables. Normally distributed data were presented as mean ± SD and compared via independent-samples t tests; non-normally distributed data were reported as median (IQR) and compared via Mann–Whitney U-tests. Treatment effects were presented as risk/mean/median differences with 95% CIs, calculated using the Hodges–Lehmann estimator. Categorical variables were described as counts (percentages) and compared via chi-square or Fisher’s exact test, with between-group differences reported as RRs and 95% CIs. Time-to-event outcomes (postoperative hospital stay) were analyzed via Kaplan–Meier curves and Log rank test, with HRs and 95% CIs estimated by univariable Cox regression.
) defined as imbalance.38 The Kolmogorov–Smirnov test was used to test the normality of continuous variables. Normally distributed data were presented as mean ± SD and compared via independent-samples t tests; non-normally distributed data were reported as median (IQR) and compared via Mann–Whitney U-tests. Treatment effects were presented as risk/mean/median differences with 95% CIs, calculated using the Hodges–Lehmann estimator. Categorical variables were described as counts (percentages) and compared via chi-square or Fisher’s exact test, with between-group differences reported as RRs and 95% CIs. Time-to-event outcomes (postoperative hospital stay) were analyzed via Kaplan–Meier curves and Log rank test, with HRs and 95% CIs estimated by univariable Cox regression.
To evaluate the effect of SGB on POST and hoarseness, generalized estimating equations (GEEs) were used to analyze the repeated measurement data.39 For the incidence of POST and hoarseness (a binary outcome), the model was specified with a Poisson distribution, a log link function, and an exchangeable working correlation structure to directly estimate the relative risk (RR) and its 95% confidence interval. For the severity of POST and hoarseness, a cumulative logit GEE (proportional odds model) with an independent working correlation structure was employed to estimate the cumulative odds ratio (OR) and its 95% confidence interval. All models included group (SGB vs control) and time (2 h, 6 h, and 24 h, with 2 h as the reference).
Post-hoc subgroup analyses were conducted for the primary outcome (POST at 6 h) across the following clinically relevant subgroups: sex (male vs female), age (< 65 y vs ≥ 65 y), smoking status (non‑smoker vs smoker), ASA physical status (II vs III), Cormack‑Lehane grade (I vs II), duration of surgery (< 120 min vs ≥ 120 min), and DLT size (35Fr vs 37Fr). Treatment-covariate interactions were tested via logistic regression, with P < 0.10 defined as a significant interaction.40 No multiple comparison correction was performed for secondary and exploratory outcomes, and all related results should be interpreted as exploratory.
All statistical tests were two-sided, with P < 0.05 considered statistically significant. Analyses were performed using SPSS 17.0 for Windows (SPSS Inc., Chicago, IL, USA) and RStudio 4.1.0 (RStudio, Boston, MA, USA) by two blinded biostatisticians.
Results
Study Population and Baseline Characteristics
Between December 2024 and December 2025, 143 elective thoracic surgery patients were screened for eligibility. 19 were excluded pre-randomization (18 ineligible, 1 declined participation), and 124 eligible patients were randomized 1:1 to the SGB group (n = 62) and control group (n = 62). In the SGB group, 6 patients were excluded after randomization due to Cormack–Lehane grade 3 (n = 3), failed first intubation attempt (n = 2), or conversion to thoracotomy (n = 1), leaving 56 patients for final analysis. In the control group, 7 patients were excluded due to Cormack–Lehane grade 3 (n = 3), failed first intubation attempt (n = 3), or ventilator therapy with tube after surgery (n = 1), leaving 55 patients for final analysis (Figure 2). The final analysis therefore included 111 patients (56 in the SGB group and 55 in the control group).
 |
Figure 2 CONSORT flow diagram of patient enrollment, randomization, and follow-up. |
Baseline demographic and clinical characteristics were comparable between the two groups (Table 1). The median age was 60 years (IQR: 55–65) in the SGB group and 60 years (IQR: 53–67) in the control group. Female patients comprised 58.9% and 50.9% of the SGB and control groups, respectively. BMI, smoking history, baseline Athens Insomnia Scale scores, and HADS scores were comparable between groups. No significant between-group differences were observed in surgical characteristics, including surgery type, operation duration, intraoperative sufentanil equivalent, ASA status, Cormack–Lehane grade, DLT size, time to achieve intubation, and duration of intubation.
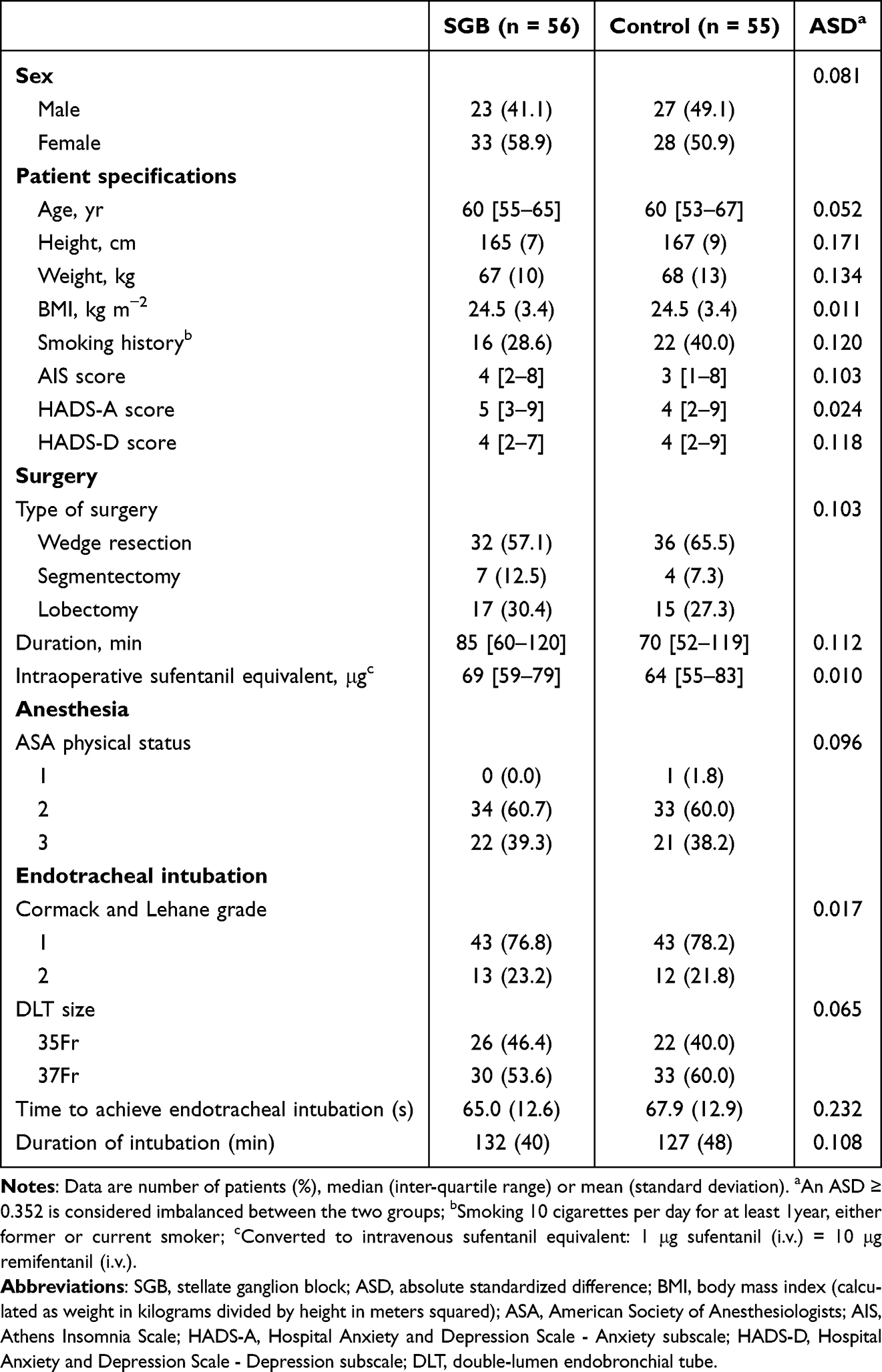 |
Table 1 Demographics and Baseline Characteristics |
Primary and Secondary Outcomes
The incidence of POST at 6 h after surgery was significantly lower in the SGB group than the control group (14.3% [8/56] vs 38.2% [21/55]; RR = 0.37; 95% CI 0.18–0.77; P = 0.008; Table 2 and Figure 3). Analysis for the severity of POST demonstrated a consistent benefit, with a cumulative OR of 0.24 (95% CI: 0.10 to 0.61; P = 0.002) for the SGB group compared with controls at 6 h postoperatively (Table 2 and Figure 3).
 |
Table 2 Efficacy Outcomes |
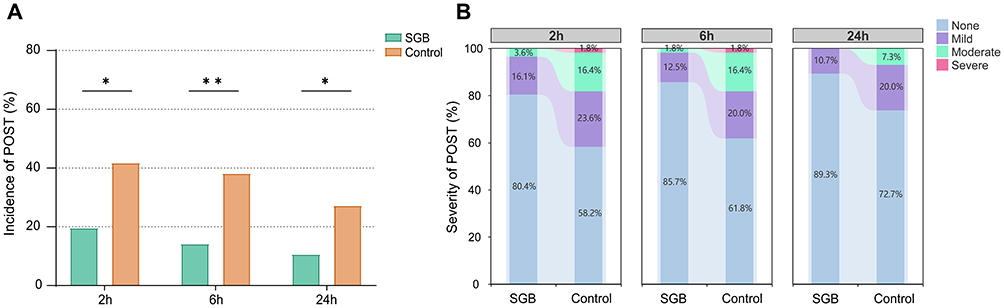 |
Figure 3 Incidence (A) and severity (B) of POST. *P < 0.05; **P < 0.01. Abbreviations: POST, postoperative sore throat; SGB, stellate ganglion block. |
The beneficial effect of SGB on POST was also observed at 2 h and 24 h after surgery. At 2 h postoperatively, 11 patients (19.6%) in the SGB group reported POST compared with 23 patients (41.8%) in the control group (RR = 0.47; 95% CI: 0.25 to 0.87; P = 0.017; Table 2). We also found a significant reduction in severity at 2 h after surgery (cumulative OR = 0.31; 95% CI: 0.14 to 0.72; P = 0.007). At 24 h postoperatively, the incidence of POST remained lower in the SGB group (6 patients, 10.7%) than in the control group (15 patients, 27.3%) (RR = 0.39; 95% CI: 0.16 to 0.94; P = 0.036), with corresponding severity analysis showing cumulative OR = 0.32 (95% CI: 0.11 to 0.89; P = 0.030) (Table 2 and Figure 3). No significant differences were observed between groups in the incidence or severity of hoarseness at any assessed time point (all P > 0.05) (Table 2).
Sleep disturbance was significantly less frequent in the SGB group at 24 h postoperatively. Twenty-two patients (39.3%) in the SGB group met criteria for sleep disturbance, compared with 35 patients (63.6%) in the control group (RR = 0.62; 95% CI: 0.42 to 0.91; P = 0.010; Table 2). Patients in the SGB group also demonstrated significantly lower HADS‑A score (median difference [MD] −2.00; 95% CI: −3.00 to 0.00; P = 0.006) and HADS‑D scores (MD −2.00; 95% CI: −3.00 to 0.00; P = 0.006) at 24 h after surgery compared with controls (Table 2). No significant differences were observed between groups in intraoperative hemodynamic parameters, including SBP, DBP and HR (all P > 0.05; Supplementary Figure 1).
Exploratory Outcomes
Duration of post-anesthesia care unit stay was comparable between groups (mean 25.7 ± 5.3 min in the SGB group vs 26.8 ± 5.0 min in the control group; MD = −1.14; 95% CI: −3.06 to 0.78; P = 0.243). Similarly, the length of postoperative hospital stay did not differ significantly between groups (median 4 days, IQR: 3–6 in the SGB group vs 4 days, IQR: 3–5 in the control group; HR = 1.26; 95% CI: 0.87 to 1.83; P = 0.128; Table 2) (Table 2 and Figure 4).
 |
Figure 4 Kaplan-Meier curve and Log rank test of the postoperative hospital stay. |
Subgroup Analysis
Subgroup analyses were performed to explore potential heterogeneity in treatment effect on the primary outcome (POST at 6 h) across clinically relevant subgroups (Figure 5). A significant treatment-by-covariate interaction was observed for duration of surgery (<120 min vs ≥120 min, P for interaction = 0.017). The protective effect of SGB was more pronounced in patients with shorter surgical duration compared with those with longer duration. No significant interactions were detected for sex (male vs female, P for interaction = 0.465), age (< 65y vs ≥ 65 y, P for interaction = 0.906), smoking status (nonsmoker vs smoker, P for interaction = 0.815), ASA classification status (II vs III, P for interaction = 0.171), Cormack–Lehane grade (I vs II, P for interaction = 0.427), or DLT size (35Fr vs 37Fr, P for interaction = 0.211).
 |
Figure 5 Subgroup analysis of incidence of POST at 6 h after surgery. Abbreviations: ASA, American Society of Anesthesiologists; DLT, double-lumen endobronchial tube; POST, postoperative sore throat; SGB, stellate ganglion block; RR, relative risk. |
Safety Outcomes
Safety outcomes were similar between groups (Table 3). Hypotension occurred in 16 patients (28.6%) in the SGB group and 14 patients (25.5%) in the control group (P = 0.712). Recurrent laryngeal nerve block occurred in 3 patients (5.4%) in the SGB group, with no cases in the control group (P = 0.177). All cases of recurrent laryngeal nerve block were transient and resolved spontaneously within 24 h without clinical sequelae. No cases of local anesthetic systemic toxicity, hematoma, puncture-related infection, pneumothorax, phrenic nerve block, or brachial plexus block were observed in either group. Hypertension, bradycardia, tachycardia, and desaturation were also comparable between groups (all P > 0.05).
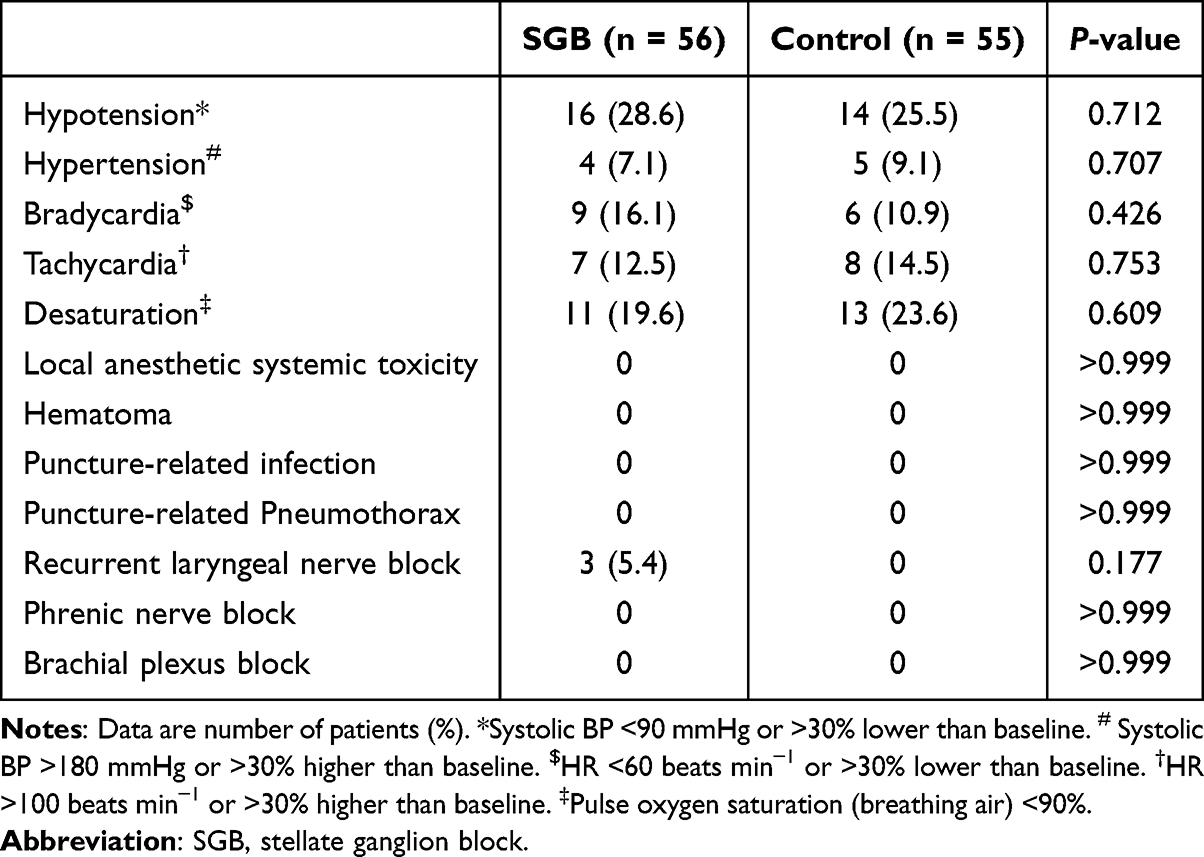 |
Table 3 Safety Outcomes Within 24 h After Surgery |
Discussion
To our knowledge, this is the first RCT assessing the preventive effect of preoperative ultrasound-guided SGB on POST in DLT intubation patients. Results demonstrated that SGB significantly reduced both the incidence and severity of POST over the first 24 postoperative hours compared with control group. Furthermore, SGB conferred clinically meaningful improvements in sleep quality and emotional well-being at 24h after surgery; however, it did not significantly affect the incidence and severity of hoarseness.
POST represents the most frequently reported patient complaint among individuals undergoing thoracic surgery with DLT placement, and it remains a highly prevalent adverse event following DLTs under GA.28 POST following DLT intubation is primarily attributable to mechanical trauma-induced local inflammation.3,41 Compared to single-lumen endotracheal tubes, DLTs possess a larger outer diameter and greater rigidity, and their placement necessitates repeated FB manipulation—collectively resulting in more pronounced mechanical injury to the pharyngeal mucosa, vocal folds, and tracheal mucosa.18,42 Current strategies to mitigate POST encompass pharmacological interventions, non-pharmacological modalities, and diverse drug delivery routes; however, many pharmacologic agents are constrained by dose-limiting adverse effects.2,3,43 Furthermore, despite various available preventive strategies, many patients still develop moderate to severe POST.21,28,44 In our prior RCT, we found preoperative SLNB demonstrated efficacy in reducing POST incidence at 6 h after surgery, yet failed to sustain this protective effect beyond that timeframe—highlighting a critical gap in prolonged POST prevention.28
The 6-hour postoperative POST incidence in the control group was 38.2%, consistent with previous studies, confirming the 6-hour time point as the critical period for POST burden after DLT intubation. Notably, preoperative SGB reduced the POST incidence at 6 h after surgery to 14.3%, a finding that is largely consistent with our prior research. In our earlier study, preoperative SLNB was shown to decrease POST incidence from 41.5% to 17.1%;28 similarly, Park et al26 reported that the two-handed jaw thrust maneuver lowered POST incidence from 59% to 26%, and Chang et al37 demonstrated that prophylactic administration of benzydamine hydrochloride reduced POST incidence from 56.5% to 23.9%. These collective data indicate that preoperative SGB yields a comparable protective effect against POST at 6 h after surgery to that of previously reported pharmacologic and nonpharmacologic prophylactic strategies. A key novel finding of the present study, however, is that SGB maintained a significant protective effect and reduced POST incidence at 24 h after surgery, which aligns with existing evidence supporting the efficacy of SGB in mitigating POST after tracheal intubation. Luo et al33 reported that preoperative SGB significantly reduced the incidence and severity of POST after single-lumen tracheal tube intubation in patients undergoing lumbar surgery, yet this effect was restricted to 6 h after surgery. A plausible explanation for this discrepancy in treatment effect is that, in addition to the difference in LA used between the two studies, airway injury induced by DLT intubation in our study is more persistent and severe compared with that caused by single-lumen endotracheal intubation. Therefore, SGB may confer sustained protective benefits for patients undergoing DLT intubation.
As a well-established regional anesthetic technique, SGB has been shown to exert regulatory effects on sympathetic tone and anti-inflammatory actions, which are postulated to be the underlying mechanisms mediating its analgesic and anti-inflammatory efficacy in the upper airway.45 In contrast, SLNB abrogates the conduction of pain signals rapidly by directly inhibiting sensory afferent fibers in the laryngopharyngeal mucosa, and its therapeutic effect is predominantly dependent on the pharmacodynamic duration of the LA administered.28 In the present study, the protective effect of SGB persisted up to 24 hours postoperatively, whereas the pharmacodynamic duration of 0.5% ropivacaine is only approximately 6–8 hours. This prolonged effect suggests that the therapeutic benefits of SGB may extend beyond the intrinsic pharmacokinetic duration of the local anesthetic itself. This phenomenon can be explained by the dual sympathetic-modulating and anti-inflammatory effects of SGB. Clinically, SGB has been documented to decrease postoperative levels of IL-6, C-reactive protein (CRP), and norepinephrine.31 Beyond this acute-phase suppression, preclinical evidence demonstrates that SGB also downregulates the IKK/NF-κB pathway and inhibits type 2 cytokines (IL-4, IL-5, IL-13),45 highlighting its broader airway anti-inflammatory capacity that may provide additional protection in the context of thoracic surgery. Furthermore, SGB exhibits prominent regulatory effects on the sympathetic nervous system and maintained stable autonomic nervous function.29,46
In this study, SGB significantly lowered the incidence of 24-hour postoperative sleep disturbance, with marked improvements in anxiety and depression scores, consistent with the findings of Yang et al30 in patients undergoing breast cancer surgery, suggesting that the sympathetic modulatory effects of SGB may disrupt the vicious cycle of “pain-sleep disturbance-emotional deterioration” by regulating the sleep-wake cycle and the function of the hypothalamic-pituitary-adrenal (HPA) axis.47 Although the breast cancer population differs from our thoracic surgical cohort in important respects, the underlying mechanisms through which SGB improves sleep and emotional status are likely to be generalizable rather than disease‑specific. These results indicate that SGB may confer broader perioperative benefits via central neural modulation. Preclinical studies have demonstrated that SGB can inhibit the release of norepinephrine (NE) from the locus coeruleus (LC) to key brain regions, thereby exerting a significant ameliorative effect on emotional and cognitive functions, and similar findings have been reported in several RCTs.33,48–50 Furthermore, the regulatory effect of SGB on sympathetic balance has also been explored by our team as a potential therapy for chronic insomnia in the anesthesia clinic, although its efficacy for this indication remains investigational.51
Subgroup analysis revealed a significant interaction between surgical duration and the therapeutic effect of SGB on POST, with patients undergoing surgery of less than 120 minutes deriving a more pronounced benefit from SGB. Previous studies have identified surgical duration as a significant risk factor for POST; prolonged surgery is associated with a longer indwelling time of the DLT, prolonged airway mucosal compression and a potentially higher frequency of FB adjustments, and the cumulative airway injury induced by these factors may exceed the protective capacity of SGB.52–54 However, this interaction was identified in a prespecified, exploratory subgroup analysis that employed a P < 0.10 threshold for interaction significance, involved subgroups of unbalanced size, and was not adjusted for multiplicity. It should therefore be regarded as hypothesis‑generating and requires independent validation in future studies specifically designed to test this hypothesis.55
In terms of safety outcomes, a relatively higher incidence of recurrent laryngeal nerve block was observed in the SGB group. As a known complication of SGB, recurrent laryngeal nerve block arises from the anatomical adjacency between the recurrent laryngeal nerve and the stellate ganglion: the recurrent laryngeal nerve courses along the tracheoesophageal groove and lies posterior to the carotid sheath, rendering it susceptible to infiltration by the spread of LA solution.29 The incidence of recurrent laryngeal nerve block in the present study was 5.4%, and all cases were transient, resolving spontaneously within 24 hours without any severe associated complications being observed. However, in thoracic surgery patients—who depend on effective cough and intact glottic closure for secretion clearance and aspiration prevention in the immediate postoperative period—even transient unilateral vocal cord impairment warrants attention. Although no aspiration events or respiratory complications were observed in these patients, the risk–benefit balance of SGB for POST should nevertheless be carefully evaluated by the attending anesthesiologist.
Several limitations of this prospective RCT should be acknowledged when interpreting the study findings. First, the control group received 1% tetracaine gel for DLT lubrication; therefore, our study evaluated the incremental value of SGB added to routine practice rather than efficacy against a placebo. Second, although patients were formally blinded, some in the SGB group may have perceived the needle puncture or Horner’s signs and inferred their allocation. The intubating anesthesiologist was also aware of group assignment due to the gel lubrication required in the control group, though this individual did not participate in outcome assessment. Coupled with our team’s established interest in the neuropsychological applications of SGB—which may introduce unconscious investigator bias—these factors could collectively have influenced the subjective outcomes, even though all were assessed by blinded evaluators using prespecified instruments. Third, intention-to-treat analysis (ITT) was not performed, with some patients excluded per predefined intraoperative criteria. Fourth, this single-center, single-anesthesiologist design limits generalizability to settings with varying operator experience. Fifth, no upper age limit was applied at enrolment. Although a prespecified subgroup analysis found no evidence that age modified the treatment effect, a residual influence of age on baseline POST risk cannot be excluded; these warrants dedicated investigation in geriatric cohorts. Sixth, we did not measure inflammatory mediators, leaving the mechanistic basis of SGB’s effects incompletely explored. Finally, Enhanced Recovery After Surgery (ERAS) protocol implementation led to a relatively short hospital stay, precluding assessment of the long-term prognosis of POST and its impact on patient quality of life.
Conclusion
This RCT suggests that preoperative ropivacaine-based SGB could reduce the incidence and severity of POST in thoracic surgery patients with DLT intubation, with a protective effect lasting at least 24 hours postoperatively. SGB could also improve postoperative sleep quality and emotional status. However, SGB did not significantly reduce hoarseness, and the risk of adverse effects warrant careful risk–benefit assessment. SGB may represent a new strategy for preventing POST, though these preliminary results require validation in larger multicenter studies.
Data Sharing Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Ethics Approval and Consent to Participate
The study was conducted with Institutional Review Board approval from The Second Qilu Hospital of Shandong University in China (No: KYLL-2024-880) on October 31, 2024, and the guidelines outlined in the Declaration of Helsinki followed. The study protocol was registered in the Chinese Clinical Trial Registry (No: ChiCTR2400092313; date of registration: November 14, 2024) before the first patient enrollment. Written informed consent was obtained from all study participants.
Acknowledgments
We express our gratitude to the anesthesiologists, anesthetic nurses, and surgical nurses who participated in treating our patients. We express our sincere appreciation to Prof. Yunpeng Zhao and Dr. Lei Shan for their exceptional surgical expertise.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis, and interpretation, or in all these areas; took part in drafting, revising, or critically reviewing the article; gave final approval of the version to be published; agreed on the journal to which the article has been submitted; and agreed to be accountable for all aspects of the work.
Funding
There is no funding to report.
Disclosure
No potential conflict of interest was reported by the authors.
References
1. Higgins PP, Chung F, Mezei G. Postoperative sore throat after ambulatory surgery. Br J Anaesth. 2002;88(4):582–15. doi:10.1093/bja/88.4.582
2. Moulder ZJ, Mann J, Bramley P, Heinz J, Wiles MD. Postoperative sore throat: a systematic review. Anaesthesia. 2026;81(1):116–133. doi:10.1111/anae.70048
3. Chen Z, Zuo Z, Zhang L, et al. Postoperative sore throat after tracheal intubation: an updated narrative review and call for action. J Pain Res. 2025;18:2285–2306. doi:10.2147/jpr.S498933
4. Lehmann M, Monte K, Barach P, Kindler CH. Postoperative patient complaints: a prospective interview study of 12,276 patients. J Clin Anesth. 2010;22(1):13–21. doi:10.1016/j.jclinane.2009.02.015
5. Wang L, Liu Y, Li F, Qiu Q, Xiong X, Wang G. Comparison of preoperative topical magnesium sulfate spraying and magnesium sulfate gargling for the prevention of postoperative sore throat after tracheal intubation: a randomized, double-blind, non-inferiority trial. Drug Des Devel Ther. 2025;19:1741–1752. doi:10.2147/dddt.S502081
6. Li X, Wen X, Liu Y, Zeng S, Wang F. Effects of dyclonine mucilage and compound lidocaine cream as tracheal catheter lubricant on postoperative pharyngeal complications after general anesthesia. Int J Surg. 2025;111(9):6181–6190. doi:10.1097/js9.0000000000002736
7. Zhang ZQ, Yang R, Li JJ, et al. Effect of preoperative esketamine nebulized inhalation on cough reflex, sedation, and postoperative sore throat in extubation of surgical patients: a prospective, double-blind, randomized controlled trial. Drug Des Devel Ther. 2026;20:580872. doi:10.2147/dddt.S580872
8. Kuriyama A, Maeda H, Sun R, Aga M. Topical application of corticosteroids to tracheal tubes to prevent postoperative sore throat in adults undergoing tracheal intubation: a systematic review and meta-analysis. Anaesthesia. 2018;73(12):1546–1556. doi:10.1111/anae.14273
9. Kuriyama A, Aga M, Maeda H. Topical benzydamine hydrochloride for prevention of postoperative sore throat in adults undergoing tracheal intubation for elective surgery: a systematic review and meta-analysis. Anaesthesia. 2018;73(7):889–900. doi:10.1111/anae.14224
10. Wang G, Qi Y, Wu L, Jiang G. Comparative efficacy of 6 topical pharmacological agents for preventive interventions of postoperative sore throat after tracheal intubation: a systematic review and network meta-analysis. Anesth Analg. 2021;133(1):58–67. doi:10.1213/ane.0000000000005521
11. Tazeh-Kand NF, Eslami B, Mohammadian K. Inhaled fluticasone propionate reduces postoperative sore throat, cough, and hoarseness. Anesth Analg. 2010;111(4):895–898. doi:10.1213/ANE.0b013e3181c8a5a2
12. Subedi A, Tripathi M, Pokharel K, Khatiwada S. Effect of intravenous lidocaine, dexamethasone, and their combination on postoperative sore throat: a randomized controlled trial. Anesth Analg. 2019;129(1):220–225. doi:10.1213/ane.0000000000003842
13. Farhang B, Grondin L. The effect of zinc lozenge on postoperative sore throat: a prospective randomized, double-blinded, placebo-controlled study. Anesth Analg. 2018;126(1):78–83. doi:10.1213/ane.0000000000002494
14. Li H, Wang H, Wang C, et al. Comparison of clinical characteristics of different ventilation devices for one-lung ventilation in adults: a network meta-analysis. Int J Surg. 2025;111(6):3989–4001. doi:10.1097/js9.0000000000002378
15. Hao D, Saddawi-Konefka D, Low S, Alfille P, Baker K. Placement of a Double-Lumen endotracheal tube. N Engl J Med. 2021;385(16):e52. doi:10.1056/NEJMvcm2026684
16. Knoll H, Ziegeler S, Schreiber JU, et al. Airway injuries after one-lung ventilation: a comparison between double-lumen tube and endobronchial blocker: a randomized, prospective, controlled trial. Anesthesiology. 2006;105(3):471–477. doi:10.1097/00000542-200609000-00009
17. Hsu HT, Chou SH, Chen CL, et al. Left endobronchial intubation with a double-lumen tube using direct laryngoscopy or the Trachway® video stylet. Anaesthesia. 2013;68(8):851–855. doi:10.1111/anae.12340
18. Mourisse J, Liesveld J, Verhagen A, et al. Efficiency, efficacy, and safety of EZ-blocker compared with left-sided double-lumen tube for one-lung ventilation. Anesthesiology. 2013;118(3):550–561. doi:10.1097/ALN.0b013e3182834f2d
19. Bihani P, Das D, Jaju R, Misra S. Postoperative sore throat following Double-Lumen tube insertion in adults undergoing surgery: a scoping review. J Cardiothorac Vasc Anesth. 2026;40(1):355–363. doi:10.1053/j.jvca.2025.08.031
20. Seo JH, Kwon TK, Jeon Y, Hong DM, Kim HJ, Bahk JH. Comparison of techniques for double-lumen endobronchial intubation: 90° or 180° rotation during advancement through the glottis. Br J Anaesth. 2013;111(5):812–817. doi:10.1093/bja/aet203
21. Seo JH, Cho CW, Hong DM, Jeon Y, Bahk JH. The effects of thermal softening of double-lumen endobronchial tubes on postoperative sore throat, hoarseness and vocal cord injuries: a prospective double-blind randomized trial. Br J Anaesth. 2016;116(2):282–288. doi:10.1093/bja/aev414
22. Park SH, Han SH, Do SH, Kim JW, Rhee KY, Kim JH. Prophylactic dexamethasone decreases the incidence of sore throat and hoarseness after tracheal extubation with a double-lumen endobronchial tube. Anesth Analg. 2008;107(6):1814–1818. doi:10.1213/ane.0b013e318185d093
23. Ruetzler K, Fleck M, Nabecker S, et al. A randomized, double-blind comparison of licorice versus sugar-water gargle for prevention of postoperative sore throat and postextubation coughing. Anesth Analg. 2013;117(3):614–621. doi:10.1213/ANE.0b013e318299a650
24. Liang J, Liu J, Qiu Z, et al. Effect of esketamine gargle on postoperative sore throat in patients undergoing double-lumen endobronchial intubation: a randomised controlled trial. Drug Des Devel Ther. 2023;17:3139–3149. doi:10.2147/dddt.S430077
25. Shui W, Hu W, Ma W, et al. The effects of video double-lumen tubes on intubation complications in patients undergoing thoracic surgery: a randomised controlled study. Eur J Anaesthesiol. 2024;41(4):305–313. doi:10.1097/eja.0000000000001959
26. Park JJ, Huh H, Yoon SZ, et al. Two-handed jaw thrust decreases postoperative sore throat in patients undergoing double-lumen endobronchial intubation: a randomised study. Eur J Anaesthesiol. 2020;37(2):105–112. doi:10.1097/eja.0000000000001149
27. Park JW, Jo JH, Park JH, et al. Comparison of conventional and fibreoptic-guided advance of left-sided double-lumen tube during endobronchial intubation: a randomised controlled trial. Eur J Anaesthesiol. 2020;37(6):466–473. doi:10.1097/eja.0000000000001216
28. Chen Z, Jin Y, Lu G, Jin Y, Feng C, Zhao X. Preoperative ultrasound-guided internal branch block of superior laryngeal nerve reduces postoperative sore throat caused by double lumen endotracheal intubation: a randomized trial. Anesth Analg. 2023;137(6):1270–1278. doi:10.1213/ane.0000000000006534
29. Tsai EH, Nunez-Rodriguez E, Cata JP. Stellate ganglion block in perioperative practice: a narrative review. Br J Anaesth. 2026;136(1):179–196. doi:10.1016/j.bja.2025.07.095
30. Yang RZ, Li YZ, Liang M, et al. Stellate ganglion block improves postoperative sleep quality and analgesia in patients with breast cancer: a randomized controlled trial. Pain Ther. 2023;12(2):491–503. doi:10.1007/s40122-022-00473-y
31. Zhou W, Yu Y, Tian S, et al. Preemptive left stellate ganglion block reduces the incidence and severity of cardiac surgery-associated acute kidney injury: a randomized clinical trial. Int J Surg. 2025;111(11):8070–8078. doi:10.1097/js9.0000000000002913
32. Rae Olmsted KL, Bartoszek M, Mulvaney S, et al. Effect of stellate ganglion block treatment on posttraumatic stress disorder symptoms: a randomized clinical trial. JAMA Psychiatry. 2020;77(2):130–138. doi:10.1001/jamapsychiatry.2019.3474
33. Luo D, Su Y, Pang Y. Effects of ultrasound-guided stellate ganglion block on postoperative sore throat and postoperative sleep disturbance after lumbar spine surgery: a randomized controlled trial. BMC Anesthesiol. 2023;23(1):343. doi:10.1186/s12871-023-02301-y
34. Chen Z, Tan Y, Cong P, Jin Y, Jin Y, Li N. Effects of preoperative stellate ganglion block on postoperative sore throat and hoarseness in patients undergoing double-lumen endobronchial intubation: protocol for a prospective randomized controlled trial. J Pain Res. 2026;19:11. doi:10.2147/jpr.S573249
35. Song JG, Hwang GS, Lee EH, et al. Effects of bilateral stellate ganglion block on autonomic cardiovascular regulation. Circulation J. 2009;73(10):1909–1913. doi:10.1253/circj.cj-09-0244
36. Yan W, Cai J, Zhu C, et al. Effect of thermal softening of double-lumen endobronchial tubes on postoperative sore throat in patients with prior SARS-CoV-2 infection: a randomized controlled trial. BMC Anesthesiol. 2023;23(1):403. doi:10.1186/s12871-023-02363-y
37. Chang JE, Min SW, Kim CS, Han SH, Kwon YS, Hwang JY. Effect of prophylactic benzydamine hydrochloride on postoperative sore throat and hoarseness after tracheal intubation using a double-lumen endobronchial tube: a randomized controlled trial. Canad J Anaesthes. 2015;62(10):1097–1103. doi:10.1007/s12630-015-0432-x
38. Austin PC. Balance diagnostics for comparing the distribution of baseline covariates between treatment groups in propensity-score matched samples. Stat Med. 2009;28(25):3083–3107. doi:10.1002/sim.3697
39. Ma Y, Mazumdar M, Memtsoudis SG. Beyond repeated-measures analysis of variance: advanced statistical methods for the analysis of longitudinal data in anesthesia research. Reg Anesth Pain Med. 2012;37(1):99–105. doi:10.1097/AAP.0b013e31823ebc74
40. Tan Y, Chen Z, Ji W, et al. Effect of non-intubated anesthesia video-assisted thoracoscopic surgery on postoperative diaphragm function and pulmonary complications in patients undergoing lung surgery: a randomized clinical trial. Int J Surg. 2026;112(2):3213–3222. doi:10.1097/js9.0000000000003842
41. McHardy FE, Chung F. Postoperative sore throat: cause, prevention and treatment. Anaesthesia. 1999;54(5):444–453. doi:10.1046/j.1365-2044.1999.00780.x
42. Brodsky JB, Lemmens HJ. Tracheal width and left double-lumen tube size: a formula to estimate left-bronchial width. J Clin Anesth. 2005;17(4):267–270. doi:10.1016/j.jclinane.2004.07.008
43. Murugaiyan A, Sahoo AK, Rao PB, Misra S. Effect of 5% EMLA cream on postoperative sore throat in adults following general endotracheal anesthesia: a randomized placebo-controlled study. Anesth Analg. 2023;136(2):338–345. doi:10.1213/ane.0000000000006269
44. Shan T, Zhang H, Zhou X, et al. Effect of different head position during tracheal intubation on postoperative sore throat: a randomized clinical trial. Ann Med. 2025;57(1):2464943. doi:10.1080/07853890.2025.2464943
45. Duan Q, Zhang H, Zhao K, Hu H, Zhou Y, Yang D. Stellate ganglia block reduces airway hyperresponsiveness with modulates the IKK/NF-κB/IL-4/IL-5/IL-13 pathway. Respir Res. 2025;26(1):65. doi:10.1186/s12931-025-03131-x
46. Chen Y, Xie Y, Xue Y, Wang B, Jin X. Effects of ultrasound-guided stellate ganglion block on autonomic nervous function during CO2-pneumoperitoneum: a randomized double-blind control trial. J Clin Anesth. 2016;32:255–261. doi:10.1016/j.jclinane.2016.03.019
47. O’Gara BP, Gao L, Marcantonio ER, Subramaniam B. Sleep, pain, and cognition: modifiable targets for optimal perioperative brain health. Anesthesiology. 2021;135(6):1132–1152. doi:10.1097/aln.0000000000004046
48. Wang Z, Liu Z, Yu Y, et al. Stellate ganglion block diminishes consolidation of conditioned fear memory in mice by inhibiting the locus coeruleus to the basolateral amygdala neural circuit. Transl Psychiatry. 2025;15(1):172. doi:10.1038/s41398-025-03383-7
49. Lipov EG, Joshi JR, Sanders S, et al. Effects of stellate-ganglion block on hot flushes and night awakenings in survivors of breast cancer: a pilot study. Lancet Oncol. 2008;9(6):523–532. doi:10.1016/s1470-2045(08)70131-1
50. Hanling SR, Hickey A, Lesnik I, et al. Stellate ganglion block for the treatment of posttraumatic stress disorder: a randomized, double-blind, controlled trial. Reg Anesth Pain Med. 2016;41(4):494–500. doi:10.1097/aap.0000000000000402
51. Li Z, Wang L, Cong P, et al. Ultrasound-guided stellate ganglion block with cervicotemporal myofascial trigger point acupuncture for insomnia with comorbid anxiety and depression: a retrospective observational study. Nat Sci Sleep. 2025;17:2131–2143. doi:10.2147/nss.S551748
52. Bekele Z, Melese Z. Incidence and risk factors for postoperative sore throat after general anesthesia with endotracheal intubation: prospective cohort study. Ann Med Surg Lond. 2023;85(6):2356–2361. doi:10.1097/ms9.0000000000000786
53. Brodsky MB, Akst LM, Jedlanek E, et al. Laryngeal injury and upper airway symptoms after endotracheal intubation during surgery: a systematic review and meta-analysis. Anesth Analg. 2021;132(4):1023–1032. doi:10.1213/ane.0000000000005276
54. Biro P, Seifert B, Pasch T. Complaints of sore throat after tracheal intubation: a prospective evaluation. Eur J Anaesthesiol. 2005;22(4):307–311. doi:10.1017/s0265021505000529
55. Wang R, Lagakos SW, Ware JH, Hunter DJ, Drazen JM. Statistics in medicine--reporting of subgroup analyses in clinical trials. New Engl J Med. 2007;357(21):2189–2194. doi:10.1056/NEJMsr077003
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Ultrasound-Guided Stellate Ganglion Block with Cervicotemporal Myofascial Trigger Point Acupuncture for Insomnia with Comorbid Anxiety and Depression: A Retrospective Observational Study
Li Z, Wang L, Cong P, Chen S, Wang J, Zhang H, Zhao J, Li G, Jiao F, Li L, Wang R, Wu Q, Gong M, Chen Z, Wang Y
Nature and Science of Sleep 2025, 17:2131-2143
Published Date: 5 September 2025
Effects of Preoperative Stellate Ganglion Block on Postoperative Sore Throat and Hoarseness in Patients Undergoing Double-Lumen Endobronchial Intubation: Protocol for a Prospective Randomized Controlled Trial
Chen Z, Tan Y, Cong P, Jin Y, Jin Y, Li N
Journal of Pain Research 2026, 19:573249
Published Date: 30 January 2026
Preoperative Ultrasound-Guided Stellate Ganglion Block for Prevention of Postoperative Sore Throat After Thoracic Surgery: Study Protocol for a Randomized Controlled Trial
Wang L, Yan X, Jiang J, Wu A
Journal of Pain Research 2026, 19:612817
Published Date: 9 July 2026