Back to Journals » Clinical Interventions in Aging » Volume 21
Preoperative Frailty Screening and Risk Prediction Model in Elderly Patients Undergoing Hepatectomy: A Cross-Sectional Study
Authors Chen X ![]() , Lu L
, Lu L ![]() , Zhao T
, Zhao T ![]() , Guo Y
, Guo Y ![]() , Liu H
, Liu H ![]() , Mai J
, Mai J ![]() , Zhang L
, Zhang L ![]()
Received 5 March 2026
Accepted for publication 16 June 2026
Published 9 July 2026 Volume 2026:21 606766
DOI https://doi.org/10.2147/CIA.S606766
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Maddalena Illario
Xiaoyan Chen,1,* Laigui Lu,2,* Tianyu Zhao,1 Yunhua Guo,3 Haiyan Liu,3 Jiezhen Mai,2 Li Zhang4
1School of Nursing, Shantou University Medical College, Shantou, Guangdong, 515041, People’s Republic of China; 2Department of Hepatobiliary and Pancreatic Surgery, The First People’s Hospital of Foshan, Foshan, Guangdong, 528000, People’s Republic of China; 3Department of Nursing, Foshan Chancheng Yongan Hospital, Foshan, Guangdong, 528000, People’s Republic of China; 4Office of Retirement Administration, The First People’s Hospital of Foshan, Foshan, Guangdong, 528000, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Li Zhang, Office of Retirement Administration, The First People’s Hospital of Foshan, No. 81, Lingnan Avenue North, Chancheng District, Foshan, Guangdong, 528000, People’s Republic of China, Tel +86-18038866158, Email [email protected] Jiezhen Mai, Department of Hepatobiliary and Pancreatic Surgery, The First People’s Hospital of Foshan, No. 81, Lingnan Avenue North, Chancheng District, Foshan, Guangdong, 528000, People’s Republic of China, Tel +86-18038861061, Email [email protected]
Purpose: This study aimed to develop and evaluate a preoperative frailty screening and risk prediction model in elderly patients undergoing hepatectomy.
Patients and Methods: In this prospective observational study with a cross-sectional baseline assessment, we included 216 elderly patients aged ≥ 60 years who underwent liver resection at a tertiary hospital in Guangdong Province from January 2024 to September 2025. We collected patients’ data from their frailty assessments, preoperative clinical marker evaluations, and their demographic characteristics. Subsequently, univariate and multivariate binary logistic regression analysis was employed to identify factors associated with frailty status.
Results: Among 216 elderly patients undergoing hepatectomy, 164 (75.9%) were classified as non-frail, 40 (18.5%) as pre-frail, and 12 (5.6%) as frail, with 24.1% exhibiting frailty (FRAIL score ≥ 2). Univariate analysis identified 13 clinical indicators significantly associated with frailty status (p < 0.05). Multivariate binary logistic regression analysis demonstrated that older age, higher ASA classification, and elevated NRS-2002 score were independent risk factors for frailty, whereas higher metabolic equivalent (MET) levels and higher albumin concentrations were protective factors. The prediction model showed excellent apparent discrimination (AUC = 0.923) and good calibration; however, further validation is required before routine clinical implementation. Furthermore, frailty was significantly associated with longer postoperative and total length of stay, as well as a higher rate of unplanned reoperation.
Conclusion: Preoperative frailty status in elderly patients undergoing liver resection was associated with multiple clinical indicators. However, the proportion of patients with overt frailty among those undergoing surgery was low (5.6%), suggesting the crucial need for rigorous clinical screening. Hence, perioperative management should be prioritized for patients with pre-frailty, and an individualized treatment decision-making system should be established for those with severe frailty.
Keywords: analysis of influencing factors, elderly, frailty, hepatectomy
Introduction
The proportion of elderly individuals undergoing liver resection is increasing every year as the world’s population is aging rapidly.1 Hepatectomy is the primary treatment for liver cancers; however, the patient’s preoperative frailty state significantly impacts the procedure’s safety and recovery results.2 Frailty, a clinical syndrome characterized by diminished physiological reserves and stress response capacity, is prevalent among the elderly population. It is also recognized as an independent predictor of post-operative complications and poor prognosis.3 In recent years, preoperative frailty assessment has garnered significant attention and initiated research within geriatric surgery patients. Moreover, a strong association has been observed between preoperative frailty and increased post-operative complication rates, prolonged hospital stays, delayed functional recovery, and higher mortality.4 Because of its unique physiological impact and necessary technical demands, the patient’s preoperative physical condition is crucial for hepatectomy.5 However, large-scale studies on preoperative frailty status among elderly Chinese patients undergoing liver resection are scarce, and the factors that influence preoperative frailty have not been comprehensively evaluated.
This study collected clinical data from patients aged ≥60 years undergoing liver resection to systematically evaluate their preoperative frailty status and analyze relevant influencing factors. To address this evidence gap, this study aimed to develop and evaluate a preoperative frailty screening and risk prediction model to facilitate early identification of high-risk elderly patients undergoing hepatectomy. Thus, our findings might facilitate the identification of high-risk patients, optimize perioperative management strategies, and improve their surgical outcomes. Most existing frailty studies have focused on general surgical populations or other surgical specialties, whereas evidence specifically addressing elderly patients undergoing hepatectomy remains limited. In particular, few studies have integrated functional capacity, nutritional risk, liver-related laboratory indicators, and perioperative outcomes into a clinically applicable frailty screening model for this population.
Materials and Methods
Participants
We conducted a prospective observational study with a cross-sectional baseline frailty assessment. Consecutive patients aged ≥60 years who underwent liver resection at a tertiary hospital in Guangdong Province from January 2024 to September 2025 were enrolled. Our inclusion criteria were: (1) Those aged 60–90 years; (2) Patients with preoperative diagnosis as liver mass requiring hepatectomy; (3) Those who voluntarily participated after providing signed consent. Our exclusion criteria were: (1) Those undergoing emergency surgery; (2) Patients with incomplete clinical data, and (3) Those with mental disorders or communication barriers that might prevent assessment. This study was approved by the hospital’s ethics review board with the ethics approval number: (Ethics Review No. 25, 2025).
Research Methods
Data Collection
We employed a self-designed general information questionnaire to collect patients’ demographic, clinical, and pathological characteristics, as well as laboratory test results through the electronic medical record system. The questionnaire included the following parameters: (1) Demographic data: These included age, gender, marital and employment status, educational level, surgical history, allergy history, smoking history, alcohol consumption history, etc. (2) Clinical characteristics: Clinical data comprised Body Mass Index (BMI), comorbidities, cardiac function, Child-Pugh classification, pathological subtype, ASA physical status classification, etc. (3) Laboratory indicators: Laboratory parameters consisted of HB, ALB, TBIL, INR, etc. (4) Functional assessment indicators: These included NRS-2002, MET, ADL score, Morse Fall Risk Assessment score, etc.
Postoperative outcomes, including postoperative complications, unplanned reoperation, postoperative length of stay, and total length of stay, were extracted from the electronic medical record system.
Frailty Assessment
We employed the FRAIL Frailty Questionnaire for evaluation (Figure 1). Developed by the International Association for Nutrition, Health and Ageing in 2008, this questionnaire consists of five items across four dimensions: vitality, strength, health status, and nutritional status. To ensure objectivity, frailty assessments were performed by uniformly trained research personnel who were blinded to laboratory results, clinical classifications, and perioperative outcome data. Each item scored 1 point: 0–1 points indicated no frailty, 2 points represented pre-frailty, and 3–5 points signified significant frailty. The questionnaire demonstrated a Cronbach’s alpha coefficient of 0.826 and content validity indices ranging from 0.93 to 1.00.6
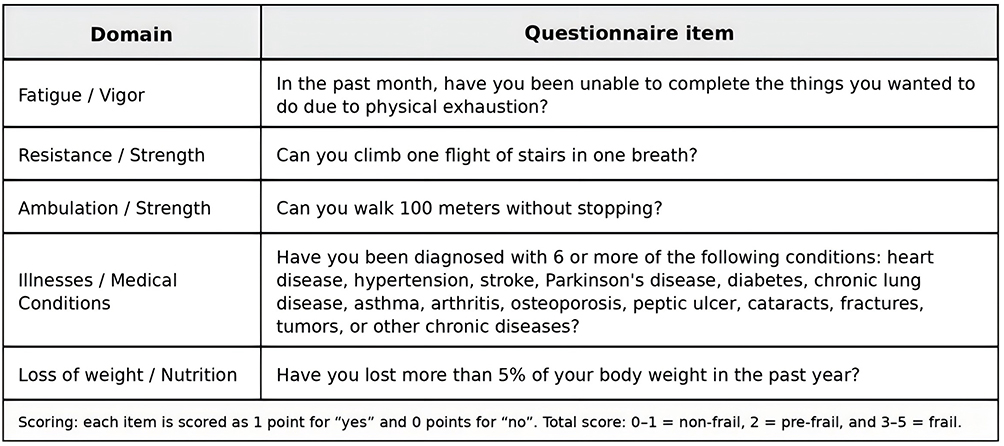 |
Figure 1 FRAIL frailty questionnaire used for preoperative frailty assessment. |
MET Assessment
Functional capacity was assessed preoperatively using a structured interview conducted by trained research personnel. Patients were asked about their ability to perform common daily activities corresponding to different metabolic equivalents (METs), such as climbing a flight of stairs, walking briskly, or carrying groceries. The estimated MET level was recorded as the patient’s functional capacity. A threshold of 4 METs is commonly used in perioperative risk stratification to indicate poor functional capacity; therefore, MET was additionally categorized as <4 versus ≥4 METs for descriptive analyses. In regression analyses, MET was entered as a continuous variable.
Statistical Analysis
Statistical analysis was performed using SPSS 26.0 software. Normally distributed quantitative data were expressed as mean ± standard deviation, and inter-group comparisons were conducted using analysis of variance (ANOVA). Non-normal data were expressed as median M (P25, P75), and inter-group comparisons were conducted using the Kruskal–Wallis H-test. Qualitative data were expressed as case numbers (%) and compared between groups using the chi-square test. Multivariate logistic regression analysis helped to identify independent factors influencing preoperative frailty. A p-value <0.05 was considered statistically significant.
For regression modeling, frailty status was dichotomized as non-frail (FRAIL score 0–1) and frail (FRAIL score ≥2) to ensure adequate statistical power and model stability. Variables with p < 0.05 in univariate analysis and with clinical relevance were entered into a multivariate binary logistic regression model. Model discrimination was evaluated using receiver operating characteristic (ROC) curve analysis, and the area under the curve (AUC) was calculated. Model calibration was assessed using the Hosmer–Lemeshow goodness-of-fit test. Standardized regression coefficients were calculated by entering z-transformed continuous variables into the logistic regression model. Because the model was developed in a single-center cohort without an independent validation dataset, the AUC should be interpreted as apparent model performance, and further internal and external validation is needed.
Postoperative outcomes were compared between non-frail and frail groups. Categorical outcomes (any complication and unplanned reoperation) were compared using the chi-square test or Fisher’s exact test as appropriate. Continuous outcomes (postoperative length of stay and total length of stay) were compared using the Mann–Whitney U-test. Additionally, multivariable regression models adjusting for age and ASA classification were used to evaluate the independent association between frailty and length of stay. Multicollinearity among independent variables was assessed using the variance inflation factor (VIF). A VIF value >5 was considered indicative of significant multicollinearity.
Results
Preoperative Frailty Status in Elderly Patients Undergoing Hepatectomy
Of 216 patients, 152 (70.3%) and 64 (29.7%) were males and females, respectively. Their ages ranged from 60 to 85 years, with a mean age of (67.9 ± 5.69) years. The preoperative frailty assessment grouped them into 164 cases without frailty (75.9%), 40 cases with pre-frailty stage (18.5%), and 12 cases with frailty (5.6%).
Univariate Analysis of Factors Affecting Frailty
Demographic Characteristics of Geriatric Inpatients
No statistically significant differences were observed among the three groups in terms of gender, marital and employment status, educational attainment, surgical history, allergy history, smoking history, or alcohol consumption history (p>0.05, Table 1). However, increasing age was significantly associated with frailty status (p<0.05).
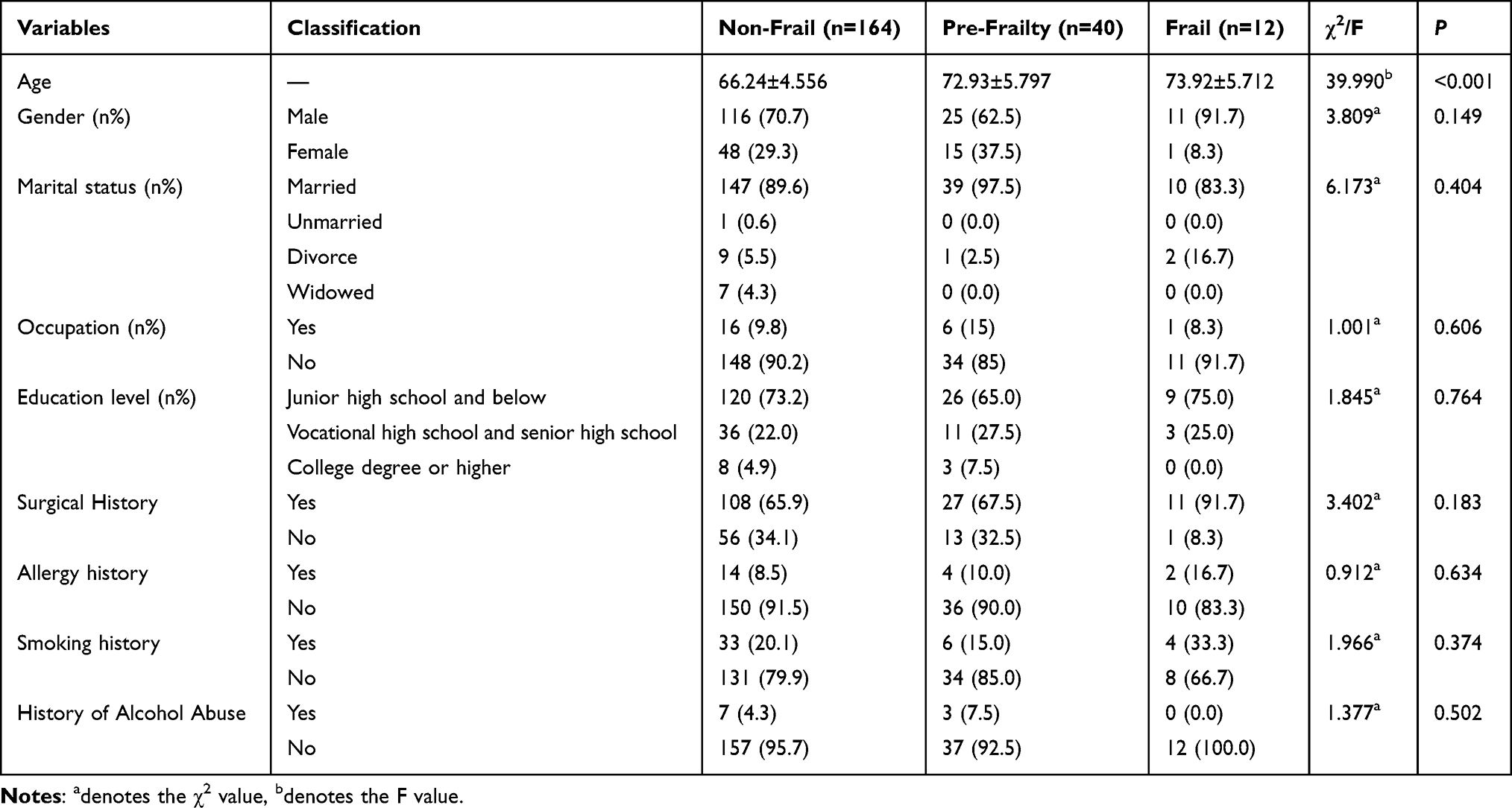 |
Table 1 Comparison of Demographic Characteristics Among Patients Undergoing Hepatic Resection with Different Degrees of Frailty (n=216) |
Comparison of Preoperative Clinical Data
A comparison of preoperative clinical data among patients with varying frailty stages revealed statistically significant differences (p<0.05) in 12 indicators. These included preoperative comorbidities, cardiac function classification, Child-Pugh classification, HB, ALB, NRS-2002 score, MET, ADL score, Morse score, INR, TBIL, and ASA classification (Table 2).
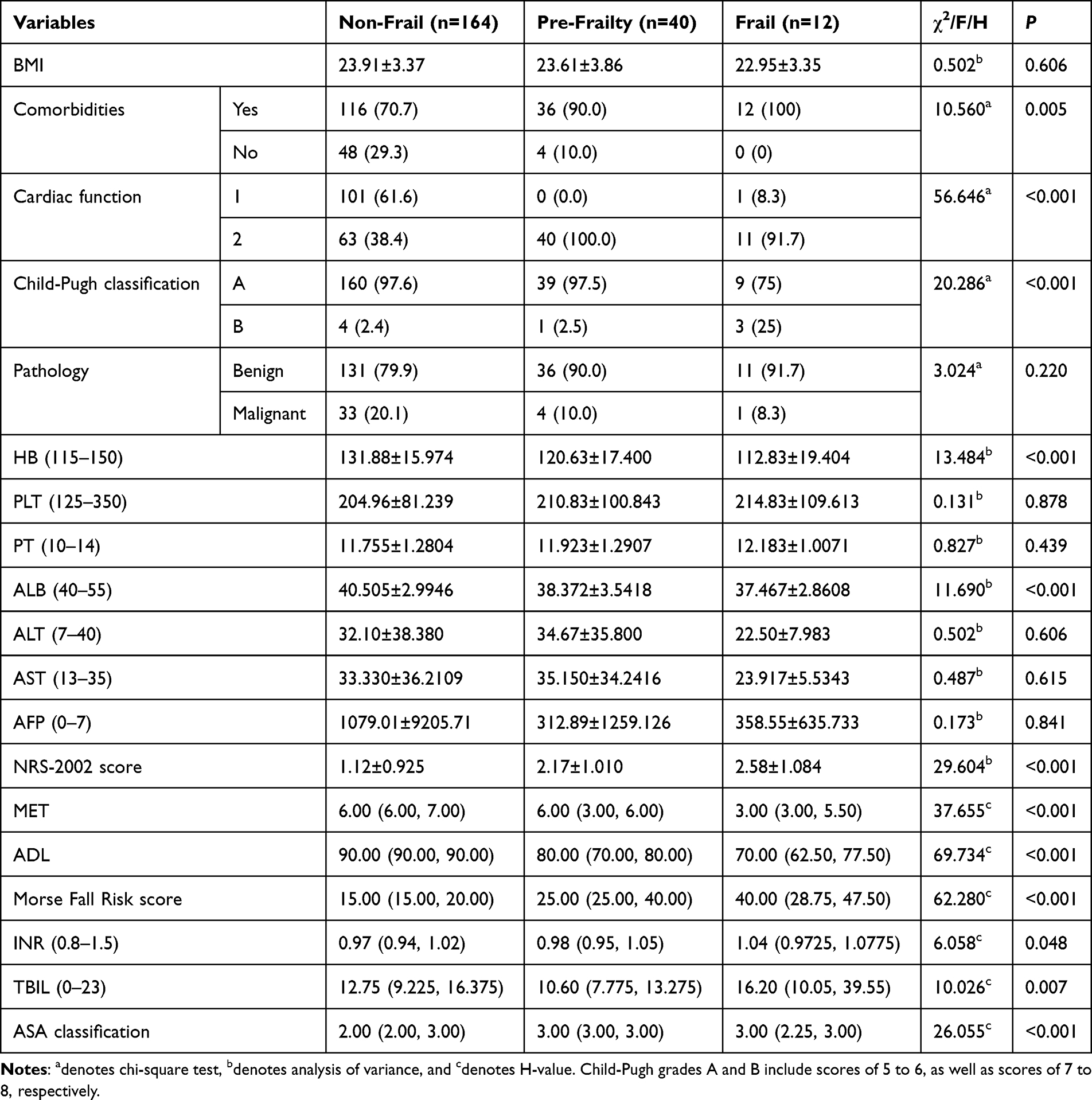 |
Table 2 Comparison of Preoperative Clinical Data Among Patients Undergoing Hepatectomy with Varying Frailty Stages (n=216) |
Multivariate Binary Logistic Regression Analysis
Multivariate binary logistic regression analysis identified age (OR=1.22, 95% CI: 1.11–1.35, p<0.001), ASA classification (OR=2.49, 95% CI: 1.00–6.22, p=0.049), NRS-2002 score (OR=1.72, 95% CI: 1.06–2.80, p=0.030) as independent risk factors for frailty. Conversely, higher MET levels (OR=0.45, 95% CI: 0.32–0.62, p<0.001) and higher albumin levels (OR=0.80, 95% CI: 0.68–0.93, p=0.004) were protective factors. The ROC curve analysis demonstrated excellent apparent discriminative ability of the model, with an AUC of 0.923 (Table 3 and Figure 2). The Hosmer–Lemeshow goodness-of-fit test indicated good model calibration (χ2 = 6.93, p = 0.545). The calibration curve demonstrated good agreement between predicted and observed probabilities (Figure 3).
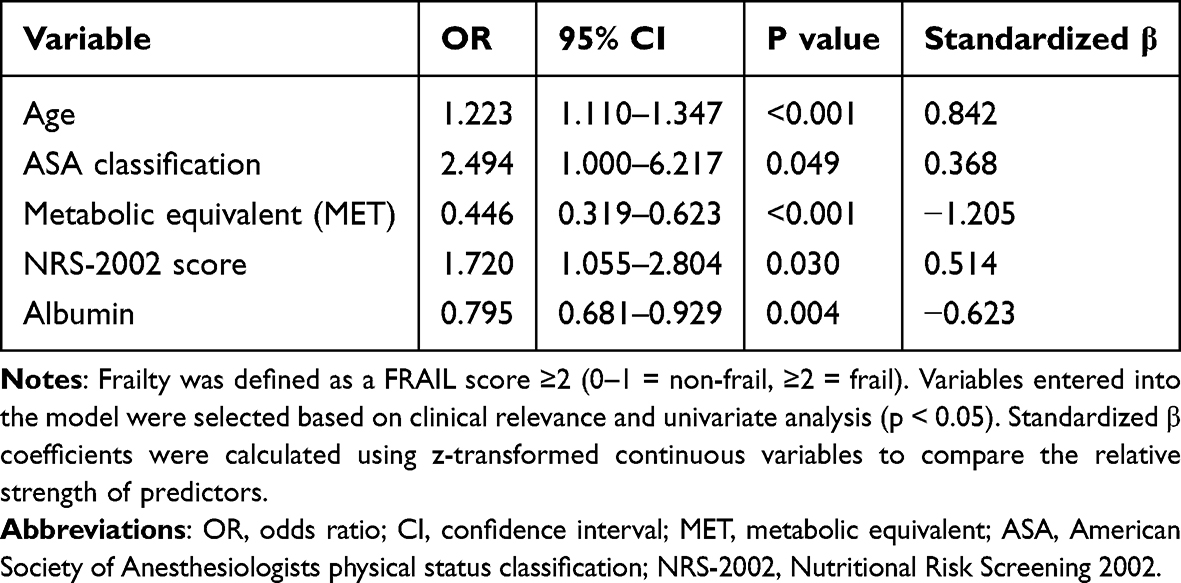 |
Table 3 Multivariate Logistic Regression Analysis of Factors Associated with Frailty |
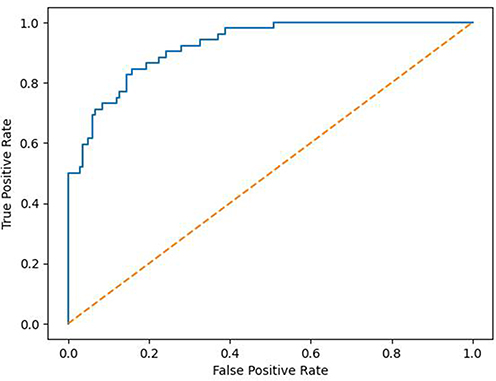 |
Figure 2 ROC curve of the multivariate model. |
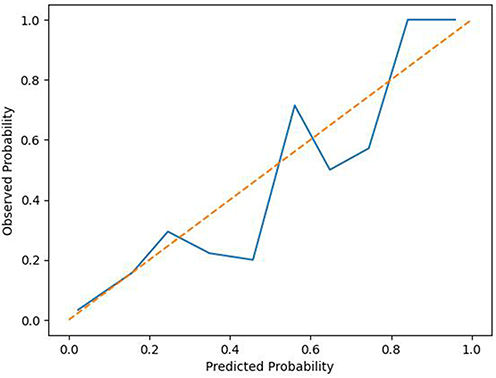 |
Figure 3 Calibration curve of the multivariate logistic regression model. The solid line represents the observed probabilities, and the dashed diagonal line represents perfect calibration. |
The adequacy of sample size for multivariate logistic regression was assessed according to the events-per-variable (EPV) rule. An EPV ≥10 is generally recommended to reduce the risk of overfitting and unstable parameter estimation. In this study, 52 events (frailty cases) were observed, and five independent variables were entered into the model, yielding an EPV of 10.4, meeting the commonly recommended EPV threshold and suggesting acceptable model stability, although the possibility of overfitting cannot be completely excluded. Among all predictors, MET showed the strongest standardized effect, followed by age and albumin.
Association Between Frailty and Postoperative Outcomes
Compared with non-frail patients, frail patients (FRAIL score ≥2) had a higher rate of postoperative complications (25.0% vs 15.2%), although the difference was not statistically significant (p = 0.213). Frail patients showed a significantly higher rate of unplanned reoperation (5.8% vs 0.6%, Fisher’s exact p = 0.049). Frail patients also had longer postoperative length of stay (median 10 [8–13] vs 8 [7–12] days, p = 0.018) and longer total length of stay (median 19.5 [16.25–24] vs 17 [13–21] days, p = 0.001). After adjustment for age and ASA classification, frailty remained independently associated with longer postoperative and total length of stay (both p < 0.05) (Table 4). No significant multicollinearity was observed among the included variables. VIF values ranged from 1.13 to 4.68, indicating acceptable collinearity.
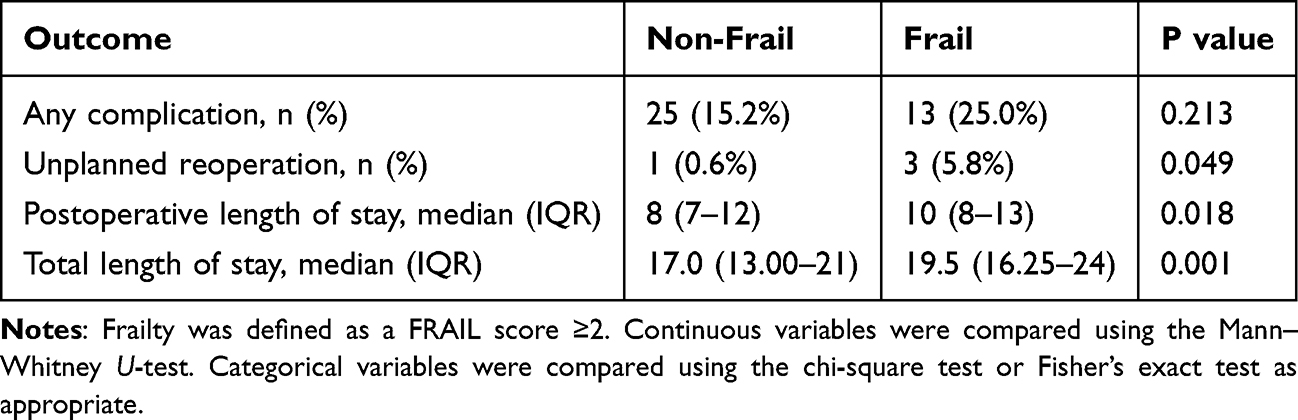 |
Table 4 Association Between Frailty Status and Postoperative Outcomes in Elderly Patients Undergoing Hepatectomy |
Discussion
Preoperative Frailty Characteristics and Clinical Implications in Elderly Hepatic Resection Patients
This phenomenon might be related to a selection effect associated with the preoperative evaluation process for hepatectomy. As a highly invasive and physiologically demanding procedure, hepatectomy requires careful preoperative assessment of cardiopulmonary function, nutritional status, and overall physiological reserve.7 Patients with pronounced frailty may be less likely to be scheduled for elective hepatectomy or may receive alternative, less invasive treatments. Consequently, the cohort undergoing surgery may represent a selected subgroup with relatively preserved physiological reserve, which could partly explain the lower observed prevalence of overt frailty.8 However, because data on patients who were excluded from surgery were not available, this explanation should be interpreted as a hypothesis rather than a definitive conclusion.9 Another international study has also revealed significant variations in preoperative frailty rates among elderly patients across different surgical subspecialties like cardiac surgery, orthopedics, and general surgery.10 These disparities are directly linked to differing inclusion criteria and risk prediction models for each procedure.7,11
Clinical Significance and Pathway Analysis of Factors Associated with Frailty
In this study, we developed and evaluated a preoperative frailty risk prediction model in elderly patients undergoing hepatectomy. The model demonstrated excellent discriminative performance and identified key clinical predictors associated with frailty. Our univariate analysis revealed that 13 indicators encompassing multiple dimensions like physiological function, nutritional status, coagulation mechanisms, ADL status, and clinical comprehensive assessment were significantly correlated with preoperative frailty status. Our findings indicate that age, ASA classification, and nutritional risk were independent predictors of frailty, whereas higher functional capacity and better nutritional status (albumin level) were protective. The predictive model demonstrated excellent apparent discrimination (AUC = 0.923) and good calibration, suggesting potential clinical utility in preoperative screening; nevertheless, this finding should be interpreted cautiously until the model is validated in larger independent cohorts.12,13
A key indicator of individual physical fitness and cardiopulmonary function, MET reflects diminished physical activity capacity and endurance through lower scores—a core feature of frailty. In the present model, MET showed the strongest standardized effect among all predictors, and higher MET levels were independently associated with a lower likelihood of frailty status defined as FRAIL score ≥2 (OR=0.446). This association is clinically plausible because MET integrates cardiopulmonary reserve, skeletal muscle function, and the ability to tolerate daily physical activity. Therefore, simple preoperative questions regarding stair climbing, brisk walking, or carrying groceries may provide practical information for identifying elderly patients at risk of frailty before hepatectomy. This aligns with findings from another international study, which explicitly identified self-reported functional capacity below 4 METs as an independent risk factor for post-operative mortality and major complications in such elderly patients.8,14 As a nutritional risk screening tool, an enhanced NRS-2002 score indicates significant malnutrition risk. A higher NRS-2002 score was independently associated with frailty, highlighting the critical role of nutritional risk. Liver disease patients often face malnutrition risks due to impaired liver function, digestive absorption disorders, and metabolic abnormalities. Additionally, malnutrition may exacerbate muscle loss and functional decline, thereby contributing to a vicious cycle of nutritional deterioration and frailty progression. A systematic review on perioperative nutritional management in hepatectomy patients emphasized that nutritional risk is an intervenable predictor of post-operative outcomes. Thus, preoperative nutritional support may improve clinical results in selected high-risk patients.9,15
In addition to identifying predictors of frailty, we further demonstrated that frailty was associated with worse postoperative utilization outcomes, including longer postoperative and total length of stay, and a higher risk of unplanned reoperation. These findings support the clinical value of routine frailty screening in elderly patients undergoing hepatectomy to optimize perioperative management and resource allocation.
Research Limitations and Future Directions
This study has several limitations. First, pre-frail and frail patients were combined into a single frailty-risk group for binary logistic regression because the number of overtly frail patients was small. Although this approach improved model stability, it may have obscured clinically meaningful differences between pre-frailty and established frailty. Future studies with larger samples should examine frailty as an ordinal outcome and explore whether different predictors are associated with pre-frailty and overt frailty. Second, this study did not assess inter-rater reliability of the FRAIL scale, as frailty assessment was performed by trained research personnel without duplicate independent evaluation. Although standardized training was provided, potential measurement bias cannot be completely excluded. Third, selection bias should be considered when interpreting our findings. Emergency surgical cases were excluded from this study, and patients with severe frailty who were deemed unsuitable for elective surgery were unlikely to be scheduled for hepatectomy. Therefore, the study population represents a relatively selected cohort of elderly patients with preserved physiological reserve. This selection process may have led to an underestimation of the true prevalence of frailty and may limit the generalizability of our findings to all elderly patients with liver disease. Fourth, the model was developed in a single-center cohort and has not yet undergone independent external validation; therefore, the high AUC may partly reflect optimism or overfitting. Future multicenter studies should perform internal resampling validation and external validation before the model is used for routine clinical decision-making. Moreover, our study model did not incorporate all potential driving factors, and our results might be influenced by unmeasured confounders, such as specific comorbidities, socioeconomic factors, cognitive function, inflammatory markers, sarcopenia, or detailed tumor burden. Thus, future studies should expand their sample sizes, adopt multicenter designs, and incorporate objective functional assessment measures to validate our findings. Concurrently, interventional studies are also needed to evaluate the efficacy of preoperative rehabilitation interventions in improving frailty status and surgical outcomes.
Conclusion
We systematically evaluated preoperative frailty status in elderly patients undergoing hepatectomy and found that approximately 24.1% exhibited pre-frailty or frailty. The relatively low proportion of overt frailty (5.6%) may reflect the stringent preoperative selection process in surgical candidates. Based on these findings, we developed an exploratory preoperative frailty risk prediction model incorporating age, ASA classification, functional capacity, nutritional risk, and albumin level. The model demonstrated good apparent discriminative performance and may assist clinicians in the early identification of vulnerable patients, but further validation is required. Our results further support the implementation of routine preoperative frailty screening for elderly patients undergoing liver resection. We recommend adopting the FRAIL scale as an efficient and rapid screening tool, integrated with ASA classification, MET assessment, and nutritional evaluation to establish a comprehensive multidimensional assessment framework. Pre-frailty may represent an important window for early intervention, whereas patients identified as frail or at high risk should receive individualized perioperative management and multidisciplinary evaluation to optimize surgical decision-making and improve clinical outcomes.
Data Sharing Statement
The raw data supporting this study are available from the corresponding author (Li Zhang, [email protected]) upon reasonable request. Ethical approval restrictions apply to participant-level data.
Ethics Approval
The study was approved by the Ethics Committee of First People’s Hospital of Foshan (Ethics Review No. 25, 2025) and was conducted in accordance with the Declaration of Helsinki.
Statement of Informed Consent
Informed consent was obtained from all individual participants included in the study.
Acknowledgments
We thank all participants and researchers for their contributions to this study. We thank Editeg Inc. for its assistance in the preparation of this manuscript.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was funded by Foshan Municipal Self-funded Scientific and Technological Innovation Projects (Grant Nos. 2420001004064).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Zheng R, Qu C, Zhang S, et al. Liver cancer incidence and mortality in China: temporal trends and projections to 2030. Chin J Cancer Res. 2018;30(6):571–10. doi:10.21147/j.issn.1000-9604.2018.06.01
2. Notarnicola M, Felli E, Roselli S, et al. Laparoscopic liver resection in elderly patients: systematic review and meta-analysis. Surg Endosc. 2019;33(9):2763–2773. doi:10.1007/s00464-019-06840-9
3. Yang JP, Shi ZY, Zhou YF, et al. Evidence summary of preoperative evaluation and management of older patients with frailty. J Nurs. 2016;26:34–39.
4. Burg ML, Clifford TG, Bazargani ST, et al. Frailty as a predictor of complications after radical cystectomy: a prospective study of various preoperative assessments. Urologic Oncol. 2019;37(1):40–47. doi:10.1016/j.urolonc.2018.10.002
5. Merath K, Tiwari A, Court C, et al. Post-operative liver failure: definitions, risk factors, prediction models and prevention strategies. J Gastrointestinal Surg. 2023;27(11):2640–2649. doi:10.1007/s11605-023-05834-2
6. Wei Y, Cao YP, Yang XL, et al. Frailty syndrome in hospitalized geriatric patients and its risk factors. Fudan Univers J Med Sci. 2018;45:496–502.
7. Lin HS, Watts JN, Peel NM, et al. Frailty and post-operative outcomes in older surgical patients: a systematic review. BMC Geriatr. 2016;16(1):157. doi:10.1186/s12877-016-0329-8
8. Wijeysundera DN, Pearse RM, Shulman MA, et al. Assessment of functional capacity before major non-cardiac surgery: an international, prospective cohort study. Lancet. 2018;391(10140):2631–2640. doi:10.1016/S0140-6736(18)31131-0
9. Hayakawa T, Kawaguchi Y, Ito K, et al. Integrating surgical complexity and nutritional parameters to enhance prediction of post-operative complications in liver resection. Surgery. 2024;176(6):1645–1652. doi:10.1016/j.surg.2024.08.021
10. Cao T, Quan Y, Zhang J, et al. Analysis of preoperative frailty and its influencing factors in elderly patients undergoing elective abdominal surgery. Chin General Pract. 2019;22:1730.
11. Revenig LM, Canter DJ, Taylor MD, et al. Too frail for surgery? Initial results of a large multidisciplinary prospective study examining preoperative variables predictive of poor surgical outcomes. J Am College Surg. 2013;217(4):665–670. doi:10.1016/j.jamcollsurg.2013.06.012
12. Battistella S, D’Arcangelo F, Grasso M, et al. Liver transplantation for non-alcoholic fatty liver disease: indications and post-transplant management. Clin Mol Hepatol. 2023;29(Suppl):S286–S301. doi:10.3350/cmh.2022.0392
13. Aloisi A, Tseng J, Kuhn T, et al. Robotic surgery in the frail elderly: analysis of perioperative outcomes. Ann Surg Oncol. 2020;27(10):3772–3780. doi:10.1245/s10434-020-08475-w
14. McIsaac DI, Harris EP, Hladkowicz E, et al. Prospective comparison of preoperative predictive performance between 3 leading frailty instruments. Anesthesia Analg. 2020;131(1):263–272. doi:10.1213/ANE.0000000000004475
15. Zhang Y, Zhang X, Qi P, et al. Preoperative frailty tendency predicts delirium occurrence in older people undergoing spinal surgery. BMC Geriatr. 2024;24(1):856. doi:10.1186/s12877-024-05476-2
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Study on the Association Between Dietary Habits, Patterns and Frailty of the Elderly: A Cross-Sectional Survey from Communities in China
Yang J, Wang A, Shang L, Sun C, Jia X, Hou L, Xu R, Wang X
Clinical Interventions in Aging 2022, 17:1527-1538
Published Date: 13 October 2022
Relationship of Frailty with Kidney Function in Adults More Than 60-Years-Old: Effect of Using Different Formulas to Estimate Glomerular Filtration Rate
Shi X, Wang S, Hu J, Chen F, Zhang H, Yang Y, Li X, Ma Q
Clinical Interventions in Aging 2023, 18:999-1007
Published Date: 27 June 2023
Factors Affecting Mortality in Elderly Hypertensive Hospitalized Patients with COVID-19: A Retrospective Study
Xu Q, Li F, Chen X
Clinical Interventions in Aging 2023, 18:1905-1921
Published Date: 20 November 2023
Effects of Anticoagulant Therapy and Frailty in the Elderly Patients with Atrial Fibrillation
Ding J, Sun Y, Zhang K, Huang W, Tang M, Zhang D, Xing Y
Clinical Interventions in Aging 2024, 19:247-254
Published Date: 14 February 2024
Effect of Continuous Positive Airway Pressure on Incident Frailty in Elderly Patients with Obstructive Sleep Apnea: A Study Based on Propensity Score Matching
Xue X, Zhao LB, Zhao Z, Xu WH, Cai WM, Chen SH, Li TJ, Nie TY, Rui D, Qian XS, Liu L
Clinical Interventions in Aging 2024, 19:255-263
Published Date: 16 February 2024