Back to Journals » Journal of Inflammation Research » Volume 19
Preoperative C–Reactive Protein–Albumin–Lymphocyte (CALLY) Score and the Risk of Acute Kidney Injury Following Cardiac Surgery: A Retrospective Cohort Study
Authors Zhou L, Wang Q, Ahmad H, Shi T, Wang Z, Zhang M, Li Y, Zheng Q
Received 20 April 2026
Accepted for publication 23 June 2026
Published 9 July 2026 Volume 2026:19 618256
DOI https://doi.org/10.2147/JIR.S618256
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Qing Lin
Lei Zhou,1 Qian Wang,1 Hasnat Ahmad,2 Tingting Shi,3 Zan Wang,1 Man Zhang,1 Yuanhai Li,1,* Qiang Zheng1,*
1Department of Anesthesiology (High-Tech Branch), The First Affiliated Hospital of Anhui Medical University, Hefei, 230022, People’s Republic of China; 2Menzies Institute for Medical Research, University of Tasmania, Hobart, Tasmania, 7000, Australia; 3Department of Central Operation Room (High-Tech Branch), The First Affiliated Hospital of Anhui Medical University, Hefei, 230022, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Qiang Zheng, Department of Anesthesiology (High-Tech Branch), The First Affiliated Hospital of Anhui Medical University, Hefei, 230022, People’s Republic of China, Email [email protected] Yuanhai Li, Department of Anesthesiology (High-Tech Branch), The First Affiliated Hospital of Anhui Medical University, Hefei, 230022, People’s Republic of China, Email [email protected]
Purpose: The C–reactive protein–albumin–lymphocyte (CALLY) score integrates inflammation, nutrition, and immune status. Its association with acute kidney injury (AKI) following cardiac surgery remains unclear.
Patients and Methods: This retrospective cohort study included 1,302 patients (mean age 60.4 ± 10.7 years; 56.4% male) who underwent major cardiac surgery at a tertiary hospital between October 2017 and October 2023. Multivariable Poisson regression with robust standard errors was used to estimate the association between preoperative CALLY score and postoperative AKI. Restricted cubic spline analysis with three knots was employed to assess potential nonlinearity in the dose–response relationship.
Results: Postoperative AKI occurred in 487 (37.4%;95% CI: 34.8%– 40.1%) patients. Patients were categorized into quartiles: Q1 (0.1 ≤ CALLY ≤ 1.1), Q2 (1.1 < CALLY ≤ 3.7), Q3 (3.7 < CALLY ≤ 7.5), and Q4 (7.5 < CALLY ≤ 35). Compared with the Q4, the adjusted incidence rate ratios for AKI were 1.45 (95% CI: 1.17– 1.80) for Q1, 1.31 (95% CI: 1.05– 1.63) for Q2, and 1.38 (95% CI: 1.11– 1.72) for Q3. A nonlinear association was observed (P for nonlinearity = 0.004), with AKI risk decreasing steeply at lower CALLY values and stabilizing beyond the reference value of 7.5.
Conclusion: Preoperative CALLY score was independently associated with postoperative AKI in a nonlinear, dose‑dependent manner. Although this association suggests the score may be useful for preoperative risk stratification, further prospective studies are needed to determine whether it has clinical utility in guiding preventive interventions.
Keywords: acute kidney injury, cardiac surgery, C–reactive protein–albumin–lymphocyte, risk factor
Introduction
Acute kidney injury (AKI) commonly occurs among patients undergoing cardiac surgery. Preoperatively, 10–30% of cardiac surgery patients have pre‑existing chronic kidney disease, which markedly increases their vulnerability to postoperative kidney injury.1,2 Postoperatively, AKI develops in 20–40% of these patients.3,4 Other common complications following cardiac surgery include postoperative atrial fibrillation (20–40%), stroke (1–5%), pulmonary complications (up to 40%), re‑exploration for bleeding (2–5%), and delirium (25–50%).5,6 Common causes of death following cardiac surgery include multiorgan failure (often triggered by AKI),7,8 stroke,6 sepsis,9 and refractory heart failure.10
Given that AKI is a major contributor to postoperative morbidity and mortality, elucidating its underlying mechanisms and risk factors is clinically important. The pathophysiology of AKI following is multifactorial. Key mechanisms might include ischemia‑reperfusion injury, systemic inflammatory activation, oxidative stress, and hemolysis‑induced cell‑free hemoglobin toxicity.11–13 Several preoperative (such as older age, diabetes mellitus, hypertension, chronic kidney disease, and heart failure), intraoperative (such as prolonged cardiopulmonary bypass time, aortic cross-clamp time, and intra-aortic balloon pump use), and postoperative (such as low cardiac output syndrome, infection, and emergency reoperation) risk factors for AKI have already been established.14
Beyond these established risk factors, identifying reliable preoperative biomarkers that capture a patient’s overall physiological reserve may further improve risk assessment. Unlike common AKI biomarkers (such as kidney injury molecule‑1, tissue inhibitor of metalloproteinase-2, and IGF-binding protein 7)15 that reflect isolated aspects of renal injury, the C‑reactive protein‑albumin‑lymphocyte (CALLY) score16 captures systemic inflammation, nutritional status, and immune function in a single composite score, offering a broader preoperative assessment of physiological reserve. The CALLY score has been used extensively in gastrointestinal cancer research since proposed in 2022.17,18 More recently, researchers have applied the CALLY score to non‑cancer diseases, including acute ischemic stroke.19 However, little is known about the link between preoperative CALLY score and postoperative AKI, especially in the high-risk population of patients undergoing cardiac surgery. Therefore, the aim of this study was to explore the association of preoperative CALLY score with the risk of AKI.
Materials and Methods
Study Design
This study drew on information from a retrospective cohort at a Chinese hospital, covering six years from October 2017 to October 2023.3,20 This work is a component of the “Hospital outcomes after Cardiac Surgery Project”, and full project details are published elsewhere.3,20 This report follows the Reporting of Observational Studies in Epidemiology statement.3,20,21
Participants
We excluded patients younger than 18 years, those with advanced kidney disease,22 and individuals with incomplete laboratory data needed to compute the CALLY score.
Exposure Measures
Preoperative CALLY score was measured based on the following formula:16,23,24

CRP (by immunoturbidimetry), albumin (by the bromocresol green method), and lymphocyte count (by an automated hematology analyzer) were measured in the hospital’s central clinical laboratory following standard procedures, and the data were extracted from preoperative blood tests performed within six weeks before surgery.25 Although preoperative blood tests were permitted up to six weeks before surgery, more than 95% of patients had these tests completed within one week prior to the operation. Generally, higher CALLY values reflect more favourable immunological and nutritional status, whereas lower values indicate an integrated state of hyperinflammation, malnutrition, and immunodepletion.23,26 The exposure of interest was a low preoperative CALLY score (quartiles Q1–Q3, representing the lower 75% of the distribution), with the highest quartile (Q4) serving as the reference.
Outcome Measures
AKI was defined, encompassing any of the following: an increase in serum creatinine of 26.5 μmol/L or more within two days, a creatinine rise to at least 1.5 times the baseline value within seven days, or a urine output below 0.5 mL/kg per hour for six consecutive hours.3,20,27
Covariates
Covariates were abstracted from structured medical records and included age, gender, smoking history, marital status, education status, employment, body mass index (BMI), the specific surgical procedure performed, and the time of surgical procedure.3,20 We employed the Charlson Comorbidity Index (CCI) to capture the spectrum and severity of coexisting conditions.28
Statistical Analyses
Baseline characteristics were summarized based on CALLY quartiles. To compare continuous variables across quartiles, we used one‑way analysis of variance and reported the results as means ± standard deviations. Pairwise comparisons were performed using pwmean with Bonferroni correction. For categorical variables, we used counts and percentages, and applied the chi‑square test to evaluate group differences. Pairwise chi‑square tests were performed using tabi with Bonferroni correction. A threshold of P < 0.0083 (0.05/6) was used for all pairwise comparisons to account for multiple testing.
The association between preoperative CALLY score and AKI was examined using Poisson regression with robust standard errors.29 Estimates were derived from both univariable and multivariable models controlling for age, sex, baseline estimated Glomerular Filtration Rate (eGFR), BMI, comorbidity burden, and surgical procedure category. We used a Poisson regression model with restricted cubic splines to test for nonlinearity. The knots were located at the 5th, 50th, and 95th percentiles of the CALLY score distribution. We used incidence rate ratios (IRRs) with their 95% confidence intervals (CIs) to quantify the effect size.
We performed sensitivity analyses using an alternative CALLY cutoff value determined based on the methodology of Youden index.30 Furthermore, statistical power was deemed sufficient, as the 487 observed AKI events satisfied the conventional 10–15 events per variable (EPV) threshold for reliable multivariable modeling.31 All statistical calculations were carried out using Stata SE 17.0. A two‑tailed p‑value no greater than 0.05 was regarded as statistically significant.
Results
Study Population
Of the 2,396 patients (Figure 1), 1,094 were excluded (41 for age <18 years, 37 for advanced CKD, 22 due to missing AKI data, 994 with missing preoperative CALLY score). Consequently, the study cohort consisted of 1,302 patients.
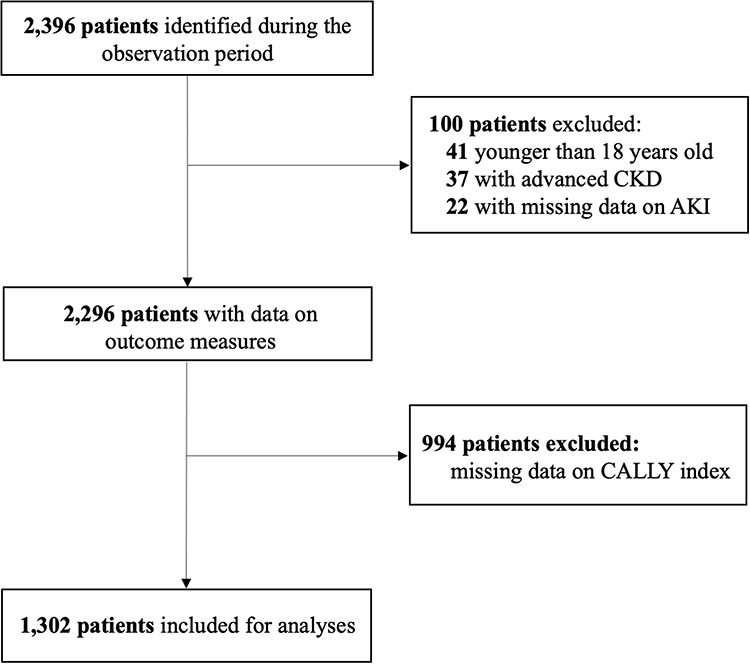 |
Figure 1 Flow chart for selection of patients. Abbreviations: AKI, Acute Kidney Injury; CALLY, C–reactive protein–albumin–lymphocyte; CKD, Chronic Kidney Disease. |
Participant Characteristics
Compared to included patients, excluded patients had higher BMI, greater comorbidity, and more CABG but fewer valve surgeries (all P < 0.01), with no other significant differences (Table S1). As shown in Table 1, the study included 1,302 patients (mean age 60.4 ± 10.7 years; 56.4% male), categorized into quartiles: Q1 (0.1 ≤ CALLY ≤ 1.1), Q2 (1.1 < CALLY ≤ 3.7), Q3 (3.7 < CALLY ≤ 7.5), and Q4 (7.5 < CALLY ≤ 35). Patients in the Q4 were younger (P < 0.001), underwent heart valve surgery more frequently (P = 0.002), and had lower BMI (P = 0.001) than those in the lower quartiles. Pairwise comparisons with Bonferroni correction confirmed that Q1, Q2, and Q3 each differed significantly from Q4 for age and surgical procedure (all P < 0.0083).
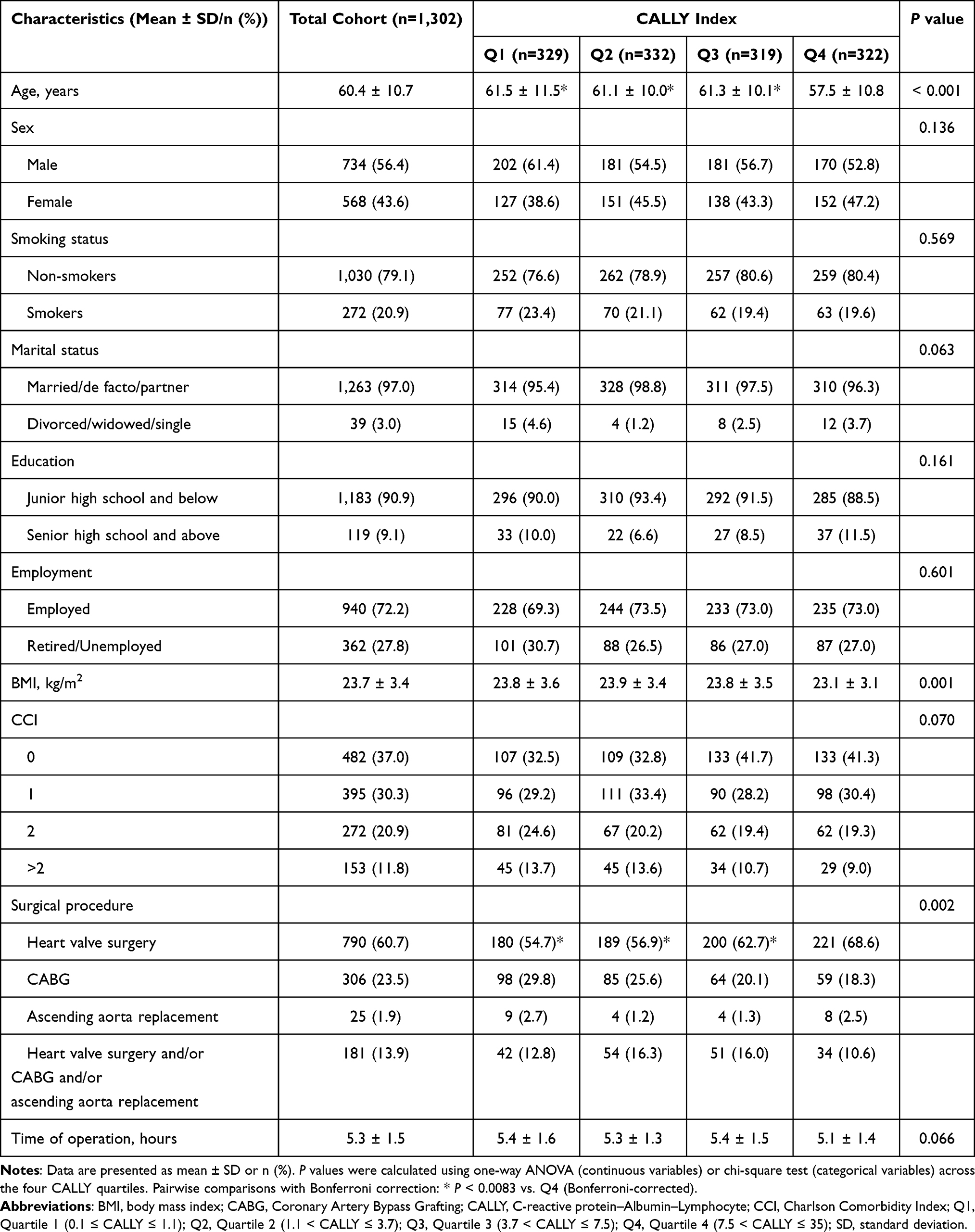 |
Table 1 Patient Demographics and Baseline Characteristics |
Incidence of Postoperative AKI
Of the 1,302 patients, 37.4% (95% CI: 34.8–40.1%) developed AKI based on both serum creatinine and urine output criteria (Table S2). Across CALLY quartiles (Figure 2), the occurrence of AKI was 42.9% (95% CI: 37.5–48.3%) in Q1, 38.3% (95% CI: 33.0–43.8%) in Q2, 41.1% (95% CI: 35.7–46.6%) in Q3, and 27.3% (95% CI: 22.5–32.5%) in Q4. A statistically significant difference was observed across quartiles (P < 0.001).
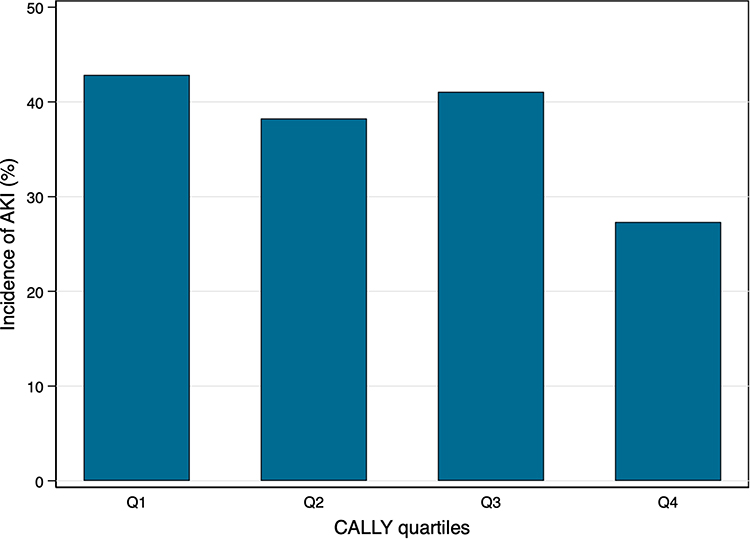 |
Figure 2 The incidence of AKI stratified by the CALLY quartiles. Abbreviations: AKI, Acute Kidney Injury; CALLY, C–reactive protein–albumin–lymphocyte; Q1, Quartile 1 (0.1–1.1); Q2, Quartile 2 (1.1–3.7); Q3, Quartile 3 (3.7–7.5); Q4, Quartile 4 (7.5–35). |
Associations of Preoperative CALLY Quartiles on AKI
Figure 3 shows that Poisson regression analyses revealed the relationship between preoperative CALLY quartiles and AKI. In the unadjusted model, patients in Q1 had an IRR of 1.57 (1.26–1.95; P < 0.001), those in Q2 had an IRR of 1.40 (1.12–1.75; P = 0.003), and those in Q3 had an IRR of 1.50 (1.20–1.88; P < 0.001), compared to those in the Q4. As for the adjusted model, the IRR for Q1was 1.45 (1.17–1.80; P = 0.001), for Q2 was 1.31 (1.05–1.64; P = 0.016), and for Q3 was 1.38 (1.11–1.72; P = 0.003), compared with Q4.
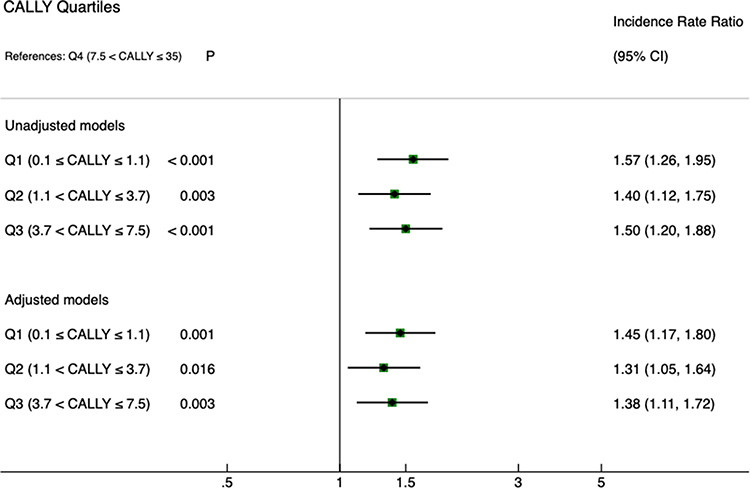 |
Figure 3 Association of preoperative CALLY score with AKI. Multivariable regression models were adjusted for age, sex, baseline estimated Glomerular Filtration Rate, BMI, CCI, and types of surgical procedures. Abbreviations: AKI, Acute Kidney Injury; BMI, Body Mass Index; CALLY, C–reactive protein–albumin–lymphocyte; CCI, Charlson Comorbidity Index; CI, Confidence Interval; IRR, Incidence Rate Ratio. |
Nonlinear Relationship Between CALLY Score and AKI
In the unadjusted model, the relationship between the CALLY score and AKI was nonlinear (P for nonlinearity = 0.0008) (Figure 4A). The risk of AKI was elevated at lower CALLY values, with a gradual decline as CALLY increased. After adjusting for age, sex, baseline eGFR, BMI, CCI, and surgical procedure type, a nonlinear inverse association remained between the CALLY score and postoperative AKI (P for nonlinearity = 0.004). Compared with the reference value of 7.5 (the third quartile cutoff), patients with a CALLY score of 1.0 had an adjusted IRR of 1.19 (1.02–1.39) (Figure 4B). Conversely, for values above 7.5, the IRR gradually declined, with a CALLY score of 15.0 yielding an IRR of 0.84 (0.72–0.98).
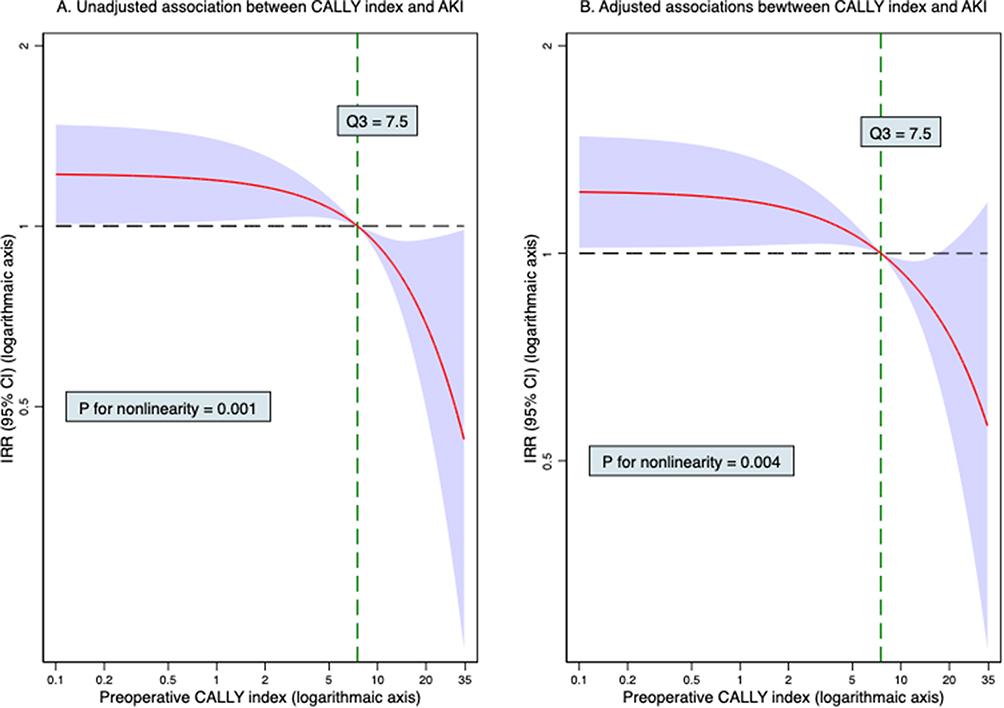 |
Figure 4 Non–linear relationship between preoperative CALLY score and AKI. (A) Unadjusted restricted cubic spline plot showing the dose‑response relationship between CALLY score and the predicted probability of postoperative AKI. (B) Adjusted restricted cubic spline plot after controlling for age, sex, baseline estimated Glomerular Filtration Rate, BMI, CCI, and type of surgical procedure. The solid line represents the IRR; shaded areas indicate 95% CI. The reference value is set at the third quartile cutoff of CALLY (7.5), indicated by the vertical dashed line. Both the X‑axis (CALLY score) and the Y‑axis (IRR) are log‑transformed to improve visual readability and maintain statistical fidelity. Abbreviations: AKI, Acute Kidney Injury; BMI, Body Mass Index; CALLY, C–reactive protein–albumin–lymphocyte; CCI, Charlson Comorbidity Index; CI, Confidence Interval; IRR, Incidence Rate Ratio; Q3, the third quartile cutoff of CALLY. |
Sensitivity Analyses
The optimal cutoff value for the CALLY score was calculated as 4.0 based on the Youden index. After multivariable adjustment for age, sex, baseline eGFR, BMI, CCI, and surgical procedure type, patients with a low CALLY score (≤ 4.0) faced a significantly increased AKI risk, with an IRR of 1.15 (1.00–1.32, P = 0.050), compared to those with a high CALLY score (> 4.0).
Discussion
This study provides the first investigation of how preoperative CALLY score relates to the risk of postoperative AKI, specifically in the cardiac surgery setting. We observed that a low CALLY score was linked to an elevated risk of postoperative AKI. A non–linear dose–response pattern between preoperative CALLY score and AKI was also detected. The risk of AKI decreased steeply as the CALLY score increased from low values, with the association attenuating and stabilizing at higher levels, compared with the reference value of 7.5 (the third quartile cutoff of CALLY score).
The overall incidence of postoperative AKI in our cohort was 37.4%, which falls within the upper range of previously reported rates (20–40%) for cardiac surgery.3,4 The relatively high incidence may be explained by the inclusion of complex procedures (eg., combined valve and CABG). Notably, AKI incidence ranged from 27.3% (Q4) to 42.9% (Q1), suggesting a graded association between poorer immunonutritional status and higher AKI risk. Although the overall trend decreased from Q1 to Q4, the quartile analysis did not show a strictly dose‑dependent pattern. Restricted cubic spline analysis further revealed a significant nonlinear inverse association (P for nonlinearity = 0.004). However, the confidence intervals widened substantially at higher CALLY scores due to sparse data, warranting cautious interpretation of the nonlinear relationship, particularly at the upper end of the CALLY distribution.
We found that patients in the lowest CALLY quartile had a 48% higher risk of AKI compared with those in the highest quartile. This was consistent with the findings of many studies demonstrating the prognostic role of the CALLY score.16,32–34 Initially developed and validated in patients undergoing hepatectomy, where low CALLY score predicted reduced overall survival,16 subsequent studies have extended its application to Sepsis,32 Asthma,33 and ST-segment elevation myocardial infarction.34
We also found a nonlinear dose–response pattern between CALLY score and AKI, with the steepest risk reduction occurring at lower CALLY values and stabilization beyond the threshold of 7.5. This pattern resembles findings from studies of other inflammatory indices (eg., the stress hyperglycaemia ratio), where risk attenuation occurs beyond certain thresholds.35 This suggests that preoperative identification of patients with low CALLY scores may enable targeted nutritional and anti-inflammatory interventions prior to surgery. However, the confidence intervals widened considerably at higher CALLY scores due to sparse data in that range, indicating reduced precision; therefore, the nonlinear relationship should be interpreted cautiously, particularly at extreme CALLY scores.
The inverse relationship between preoperative CALLY score and the risk of AKI might be attributable to the following potential biological mechanisms. The CALLY score captures three interrelated physiological dimensions, which has been independently linked to AKI pathogenesis. For example, CRP directly reflects this inflammatory burden, and elevated preoperative CRP levels have been associated with postoperative AKI in prior studies.36 Low serum albumin may compromise renal perfusion and lower the kidney’s tolerance to ischemia–reperfusion injury.37 Reduced lymphocyte counts have been shown to independently predict poor outcomes following surgery.38 Therefore, a low CALLY score may capture a combined state of high inflammation, poor nutrition, and weakened immunity. All of which may increase the kidney’s susceptibility to injury around the time of surgery. However, these proposed mechanisms are speculative, and causality cannot be inferred from this observational study.
The demonstrated association with AKI suggests that the CALLY score might complement existing risk stratification models (eg., the Cleveland Clinic Score).39 Patients identified as high-risk based on low CALLY values might benefit from perioperative optimization strategies, including nutritional support, minimization of nephrotoxic exposures, and enhanced hemodynamic monitoring. However, future prospective studies are necessary to evaluate whether preoperative optimization of the CALLY score components can mitigate AKI risk and improve postoperative health outcomes.
A key limitation is the lack of serial CRP measurements; thus, the CALLY score could only be evaluated preoperatively, precluding analysis of perioperative dynamics. Continuous measurements throughout the perioperative period might provide additional prognostic information and insight into dynamic risk trajectories. Our results might be biased by several unmeasured confounders (such as cardiac function, cardiopulmonary bypass time, intraoperative transfusion, and postoperative hemodynamic parameters) due to the retrospective observational settings. Moreover, a substantial number of patients (43.3% of the initial cohort) were excluded due to missing CALLY score components. Compared with the included patients, those excluded had higher BMI, greater comorbidity burden, and more frequent CABG but fewer valve surgeries, indicating a higher baseline risk profile. This selection bias may have led to an underestimation of the true AKI incidence in the full cardiac surgery population; therefore, our findings should be considered conservative. In addition, single centre setting in a Chinese cohort might limit the generalizability of our results to other populations. Lastly, we did not directly compare CALLY with its individual components or other inflammatory indices (eg., systemic immune‑inflammation index). Future prospective studies with larger samples are needed to determine whether CALLY score adds incremental prognostic value over markers for AKI risk stratification.
Conclusion
In this retrospective cohort study, the overall incidence of postoperative AKI was 37.4% (95% CI: 34.8%–40.1%), with marked variation across CALLY quartiles. Preoperative CALLY score was independently associated with postoperative AKI in a nonlinear, dose‑dependent manner. Although this association suggests potential utility for risk stratification, external validation and formal predictive performance analyses are needed before clinical application. Strengths of this study include the large sample size and first evaluation of CALLY in AKI, while limitations include the retrospective, single‑center design, lack of serial CALLY measurements, and absence of comparison with other inflammatory indices.
Abbreviations
AKI, acute kidney injury; BMI, body mass index; CALLY, C–reactive protein–albumin–lymphocyte; CCI, Charlson Comorbidity Index; CI, confidence interval; CRP, C‑reactive protein; eGFR, estimated Glomerular Filtration Rate; EPV, events per variable; IRR, incidence rate ratio; KDIGO, Kidney Disease, Improving Global Outcomes; RCS, restricted cubic spline; SD, standard deviation.
Data Sharing Statement
The data that support the findings of this study are not openly available due to reasons of sensitivity and are available from the corresponding author upon reasonable request.
Ethics Approval and Consent to Participate
The Institutional Review Board of the First Affiliated Hospital of Anhui Medical University approved this retrospective cohort study (reference number: PJ2024-06-85). Informed consent was waived because the study involved no more than minimal risk to participants (only existing medical records were reviewed), and it was impracticable to obtain consent from all eligible patients given the large sample size and the retrospective design spanning six years. All patient data were anonymized and de-identified prior to analysis. This study was conducted in accordance with the principles of the Declaration of Helsinki.
Acknowledgments
The authors thank all anonymous Editors and Reviewers for their valuable comments and suggestions.
Author Contributions
Lei Zhou: Investigation: lead; Validation: lead; Visualization: lead; Writing – original draft: lead.
Qian Wang: Data curation: lead; Validation: lead; Writing – review & editing: equal.
Hasnat Ahmad: Methodology: equal; Software: equal; Writing – review & editing: equal.
Tingting Shi: Data curation: equal; Writing – review & editing: equal.
Man Zhang: Data curation: equal; Writing – review & editing: equal.
Zan Wang: Data curation: equal; Writing – review & editing: equal.
Yuanhai Li: Conceptualization: equal; Project administration: equal; Supervision: equal; Writing – review & editing: equal.
Qiang Zheng: Conceptualization: lead; Formal analysis: lead; Funding acquisition: lead; Methodology: lead; Project administration: lead; Resources: lead; Software: lead; Supervision: lead; Writing – review & editing: lead.
All authors gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
No funding was received for this study.
Disclosure
The authors have no conflicts of interest to declare in relation to this work.
References
1. Wang XD, Bao R, Lan Y, et al. The incidence, risk factors, and prognosis of acute kidney injury in patients after cardiac surgery. Front Cardiovasc Med. 2024;11:1396889. doi:10.3389/fcvm.2024.1396889
2. Cheruku SR, Raphael J, Neyra JA, Fox AA. Acute kidney injury after cardiac surgery: prediction, prevention, and management. Anesthesiology. 2023;139(6):880–11. doi:10.1097/aln.0000000000004734
3. Zheng Q, Wang Z, Wang H, et al. Prognostic accuracy of the kidney disease: improving global outcomes criteria for in-hospital mortality following cardiac surgery: a comparative analysis of acute kidney injury definitions. J Cardiothorac Vasc Anesth. 2026;40(4):1180–1186. doi:10.1053/j.jvca.2026.01.004
4. Ronco C, Bellomo R, Kellum JA. Acute kidney injury. Lancet. 2019;394(10212):1949–1964. doi:10.1016/S0140-6736(19)32563-2
5. Cerda LM. Common Complications in Cardiothoracic Surgery: incidence, Risk Factors, Prevention and Management. In: Whizar-Lugo VM, Barba-Pérez IS, Díaz Arizmendi DE, editors. Postoperative Care and Complications. IntechOpen; 2026.
6. Laimoud M, Alanazi MN, Machado P, et al. Acute ischemic and hemorrhagic cerebrovascular strokes after cardiac surgery: incidence, predictors, and outcomes. Crit Care Res Pract. 2025:6645363. doi:10.1155/ccrp/6645363
7. Ostermann M, Lumlertgul N, Jeong R, See E, Joannidis M, James M. Acute kidney injury. Lancet. 2025;405(10474):241–256. doi:10.1016/S0140-6736(24)02385-7
8. Regner KR. Epidemiology of acute kidney injury after cardiac surgery: an update. J Organ Dysfunct. 2007;3(4):232–239. doi:10.1080/17471060701236935
9. Michalopoulos A, Stavridis G, Geroulanos S. Severe sepsis in cardiac surgical patients. Euro J Surg. 1998;164(3):217–222. doi:10.1080/110241598750004670
10. Baldan BU, Hegeman R, Bos N, Smeenk HG, Klautz RJM, Klein P. Comparative analysis of therapeutic strategies in post-cardiotomy cardiogenic shock: insight into a high-volume cardiac surgery center. J Clin Med. 2024;13(7):2118. doi:10.3390/jcm13072118
11. Yang X, Zhu L, Pan H, Yang Y. Cardiopulmonary bypass associated acute kidney injury: better understanding and better prevention. Ren Fail. 2024;46(1):2331062. doi:10.1080/0886022x.2024.2331062
12. Schaer DJ, Schaer CA, Humar R, et al. Navigating hemolysis and the renal implications of hemoglobin toxicity in cardiac surgery. Anesthesiology. 2024;141(6):1162–1174. doi:10.1097/aln.0000000000005109
13. Greite R, Schott S, Wang L, et al. Free heme and hemopexin in acute kidney injury after cardiopulmonary bypass and transient renal ischemia. Clin Transl Sci. 2023;16(12):2729–2743. doi:10.1111/cts.13667
14. Scurt FG, Bose K, Mertens PR, Chatzikyrkou C, Herzog C. Cardiac surgery-associated acute kidney injury. Kidney360. 2024;5(6):909–926. doi:10.34067/kid.0000000000000466
15. SchmidtOtt K, Westhoff T, Budde K, Barasch J, Schrezenmeier E. Biomarkers in acute kidney injury–pathophysiological basis and clinical performance. Acta Physiol. 2017;219(3):554–572. doi:10.1111/apha.12764
16. Iida H, Tani M, Komeda K, et al. Superiority of CRP-albumin-lymphocyte index (CALLY index) as a non-invasive prognostic biomarker after hepatectomy for hepatocellular carcinoma. HPB. 2022;24(1):101–115. doi:10.1016/j.hpb.2021.06.414
17. Wu B, Liu J, Shao C, Yu D, Liao J. Integrating inflammation, nutrition, and immunity: the CALLY index as a prognostic tool in digestive system cancers - a systematic review and meta-analysis. BMC Cancer. 2025;25(1):672. doi:10.1186/s12885-025-14074-3
18. Li J, Zhang S, Hu X, Huang T, Chen M. Correlation between the C-reactive protein (CRP)-albumin-lymphocyte (CALLY) index and the prognosis of gastric cancer patients after gastrectomy: a systematic review and meta-analysis. Surg Today. 2025;55(4):483–491. doi:10.1007/s00595-024-02921-y
19. Zhu L, Jie S, Wu S, et al. Ineffective recanalization and complications in patients with acute ischemic stroke receiving endovascular treatment: predictive value of the C-reactive protein–albumin–lymphocyte (CALLY) index. J Inflamm Res. 2025;18:14649–14661. doi:10.2147/jir.S535881
20. Wang C, Lu X, Wang H, et al. The impact of functional status assessed by the barthel index on postoperative outcomes in patients undergoing cardiac surgery: a retrospective cohort study. J Cardiothorac Vasc Anesth. 2025;39(12):3411–3417. doi:10.1053/j.jvca.2025.06.044
21. von Elm E, Altman DG, Egger M, Pocock SJ, Gøtzsche PC, Vandenbroucke JP. Strengthening the reporting of observational studies in epidemiology (STROBE) statement: guidelines for reporting observational studies. BMJ. 2007;335(7624):806–808. doi:10.1136/bmj.39335.541782.AD
22. Pérez-Fernández X, Ulsamer A, Cámara-Rosell M, et al. Extracorporeal blood purification and acute kidney injury in cardiac surgery: the SIRAKI02 randomized clinical trial. JAMA. 2024;332:1446. doi:10.1001/jama.2024.20630
23. Süygün H, Turinay Ertop ZS, Polat M, et al. Prognostic value of the C-reactive protein–albumin–lymphocyte (CALLY) index for 1-year mortality after transcatheter aortic valve implantation. J Cardiovasc Dev Dis. 2026;13(2). doi:10.3390/jcdd13020083
24. Wen SH, Tang T, Ye ZR. BMI mediates the association of CALLY index with liver steatosis and fibrosis. Sci Rep. 2025;15(1):33189. doi:10.1038/s41598-025-18919-6
25. Qi L, Chen Q, Li Y, Guo Y. Association between the C-reactive protein–albumin–lymphocyte (CALLY) index and osteoarthritis prevalence: a cross-sectional study of American adults based on NHANES. Front Nutr. 2025;12:1710682. doi:10.3389/fnut.2025.1710682
26. Cetin HK, Demir T. Importance of CALLY scores in predicting coronary artery bypass grafting outcomes. Ann Thorac Cardiovasc Surg. 2025;31(1). doi:10.5761/atcs.oa.25-00156
27. Kellum JA, Lameire N. Diagnosis, evaluation, and management of acute kidney injury: a KDIGO summary (Part 1). Crit Care. 2013;17(1):204. doi:10.1186/cc11454
28. Charlson ME, Pompei P, Ales KL, MacKenzie CR. A new method of classifying prognostic comorbidity in longitudinal studies: development and validation. J Chronic Dis. 1987;40(5):373–383. doi:10.1016/0021-9681(87)90171-8
29. Chen W, Qian L, Shi J, Franklin M. Comparing performance between log-binomial and robust Poisson regression models for estimating risk ratios under model misspecification. BMC Med Res Methodol. 2018;18(1):63. doi:10.1186/s12874-018-0519-5
30. Hassanzad M, Hajian-Tilaki K. Methods of determining optimal cut-point of diagnostic biomarkers with application of clinical data in ROC analysis: an update review. BMC Med Res Methodol. 2024;24(1):84. doi:10.1186/s12874-024-02198-2
31. Peduzzi P, Concato J, Kemper E, Holford TR, Feinstein AR. A simulation study of the number of events per variable in logistic regression analysis. J Clin Epidemiol. 1996;49(12):1373–1379. doi:10.1016/s0895-4356(96)00236-3
32. Patro S, Pattnaik SS, Arora P, et al. C-reactive protein–albumin–lymphocyte (CALLY) index in patients with sepsis: an observational study. Cureus. 2026;18(2):e103423. doi:10.7759/cureus.103423
33. Luo W, Yu Z, Zhang Y, Lin D, Wang W, Wang C. The C-reactive protein–albumin–lymphocyte (CALLY) index and all-cause mortality in adults with Asthma: a cohort study using NHANES 1999–2010. Respir Med. 2026;253:108706. doi:10.1016/j.rmed.2026.108706
34. Xu D, Liu Y, Ye J, et al. Evaluating the predictive value of the CALLY index for MACE events in STEMI patients: a comparative analysis across admission and discharge time points. J Cardiothorac Surg. 2025;21(1):4. doi:10.1186/s13019-025-03763-6
35. Yan F, Chen X, Quan X, Wang L, Wei X, Zhu J. Association between the stress hyperglycemia ratio and 28-day all-cause mortality in critically ill patients with sepsis: a retrospective cohort study and predictive model establishment based on machine learning. Cardiovasc Diabetol. 2024;23(1):163. doi:10.1186/s12933-024-02265-4
36. Verwijmeren L, Bosma M, Vernooij LM, et al. Associations between preoperative biomarkers and cardiac surgery-associated acute kidney injury in elderly patients: a cohort study. Anesth Analg. 2021;133(3):570–577. doi:10.1213/ane.0000000000005650
37. Yoon HJ, Kim TH, Ko DE, Song JW, Min N, Ham SY. Postoperative hypoalbuminemia as a predictor of acute kidney injury after open repair of ruptured abdominal aortic aneurysm. World J Surg. 2023;47(12):3382–3393. doi:10.1007/s00268-023-07178-z
38. Manzoli TF, Delgado AF, Troster EJ, et al. Lymphocyte count as a sign of immunoparalysis and its correlation with nutritional status in pediatric intensive care patients with sepsis: a pilot study. Clinics. 2016;71(11):644–649. doi:10.6061/clinics/2016(11)05
39. Vives M, Candela A, Monedero P, et al. Improving the performance of the cleveland clinic score for predicting acute kidney injury after cardiac surgery: a prospective multicenter cohort study. Minerva Anestesiol. 2024;90(4):245–253. doi:10.23736/s0375-9393.23.17596-1
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Long-Term Consequences of Increased Activity of Urine Enzymes After Cardiac Surgery – A Prospective Observational Study
Biernawska J, Kotfis K, Szymańska-Pasternak J, Bogacka A, Bober J
Therapeutics and Clinical Risk Management 2022, 18:867-877
Published Date: 26 August 2022
An Explainable Machine Learning Model to Predict Acute Kidney Injury After Cardiac Surgery: A Retrospective Cohort Study
Gao Y, Wang C, Dong W, Li B, Wang J, Li J, Tian Y, Liu J, Wang Y
Clinical Epidemiology 2023, 15:1145-1157
Published Date: 4 December 2023