Back to Journals » Infection and Drug Resistance » Volume 19
Preoperative Aggregate Index of Systemic Inflammation is Associated with 30-Day Postoperative Pneumonia After Minimally Invasive Esophagectomy for Esophageal Squamous Cell Carcinoma: A Retrospective Cohort Study
Authors Gao M, Sun H, Chen Y, Xu D, Tang D, Ji J, Zang B, Wu Q, Xu Z, Zhao J, Xu Z ![]()
Received 5 March 2026
Accepted for publication 15 June 2026
Published 25 June 2026 Volume 2026:19 602079
DOI https://doi.org/10.2147/IDR.S602079
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Sandip Patil
Manman Gao,1 Haijun Sun,2 Yunyun Chen,1 Dafu Xu,1 Derong Tang,1 Jian Ji,1 Bao Zang,1 Qingquan Wu,1 Zhiwei Xu,1 Jianqiang Zhao,1 Zhiyun Xu1
1Department of Thoracic Surgery, The Affiliated Huai’an No. 1 People’s Hospital of Nanjing Medical University, Huai’an, Jiangsu, People’s Republic of China; 2Department of Thoracic Surgery, The First People’s Hospital of Lianyungang City, Nanjing Medical University Affiliated Lianyungang Clinical College, Lianyungang, Jiangsu, People’s Republic of China
Correspondence: Zhiyun Xu, Email [email protected] Jianqiang Zhao, Email [email protected]
Background: Postoperative pneumonia remains a frequent complication after esophagectomy for esophageal squamous cell carcinoma (ESCC). Simple preoperative inflammatory markers may help identify patients at higher perioperative risk.
Methods: This retrospective cohort study included patients undergoing curative minimally invasive esophagectomy for ESCC from January 2023 to December 2025. The primary outcome was 30-day postoperative pneumonia or pneumonia during the index hospitalization, whichever occurred first. The aggregate index of systemic inflammation (AISI) was calculated from preoperative blood counts. Discriminatory performance was assessed using receiver operating characteristic (ROC) analysis and compared with neutrophil-to-lymphocyte ratio (NLR) and platelet-to-lymphocyte ratio (PLR). Associations were evaluated using hierarchical multivariable logistic regression.
Results: Among 446 eligible patients, 140 developed postoperative pneumonia, with an incidence of 31.4%. AISI showed good discriminatory performance for postoperative pneumonia (AUC, 0.795; 95% CI, 0.753– 0.837) and had a higher AUC than NLR and PLR. In the fully adjusted model, higher AISI remained independently associated with postoperative pneumonia (per 100-unit increase: adjusted OR, 1.416; 95% CI, 1.301– 1.576; P < 0.001).
Conclusion: Preoperative AISI was independently associated with 30-day postoperative pneumonia after minimally invasive esophagectomy for ESCC and showed good discriminatory performance. AISI may serve as a simple preoperative risk-stratification marker, but external validation and prospective evaluation are needed before clinical use.
Keywords: aggregate index of systemic inflammation, AISI, esophageal squamous cell carcinoma, minimally invasive esophagectomy, postoperative pneumonia, retrospective cohort
Introduction
Postoperative pneumonia is a common and clinically important complication after esophagectomy for esophageal cancer. It is associated with delayed recovery, prolonged hospitalization, and poorer postoperative outcomes.1–3 Although enhanced recovery pathways and advances in perioperative care have improved surgical outcomes,4,5 pulmonary complications remain frequent after esophagectomy. Therefore, simple and accessible markers that can help identify patients at higher risk before surgery may be useful for perioperative assessment.
Current risk assessment for post-esophagectomy pneumonia is mainly based on clinical characteristics, pulmonary function, comorbidities, and perioperative factors. Previous studies have reported associations between impaired pulmonary function and postoperative pneumonia,6,7 and several risk models or nomograms have been proposed.8–11 However, these tools vary in candidate predictors, outcome definitions, and model performance, which may limit their use across different clinical settings. Additional markers that are routinely available and easy to interpret may help complement existing clinical assessment.12,13
Systemic inflammation may contribute to postoperative infectious complications by reflecting host immune status and perioperative vulnerability. Blood count-derived indices, such as the neutrophil-to-lymphocyte ratio (NLR) and platelet-to-lymphocyte ratio (PLR), have been investigated as simple inflammatory markers in surgical patients, including those undergoing esophageal cancer surgery.14–16 Compared with single-ratio indices, composite inflammatory markers may capture a broader immune-inflammatory profile.17,18
The aggregate index of systemic inflammation (AISI), calculated from neutrophil, platelet, monocyte, and lymphocyte counts, has been studied in several inflammatory and infection-related conditions.19–24 However, its association with postoperative pneumonia after minimally invasive esophagectomy remains insufficiently defined. In this retrospective cohort study, we examined the association between preoperative AISI and 30-day postoperative pneumonia after minimally invasive esophagectomy for esophageal squamous cell carcinoma (ESCC). We also compared the discriminatory performance of AISI with that of NLR and PLR, and explored potential non-linear associations and decision-analytic performance. We hypothesized that higher preoperative AISI would be associated with an increased risk of postoperative pneumonia.
Methods
Study Design and Participants
This retrospective cohort study evaluated the association between the aggregate index of systemic inflammation (AISI) and postoperative pneumonia among patients undergoing curative minimally invasive esophagectomy for esophageal squamous cell carcinoma (ESCC) between January 2023 and December 2025. A total of 517 consecutive patients were screened. After excluding 71 patients due to missing preoperative blood counts required for AISI calculation (n = 28), missing postoperative pneumonia documentation or incomplete follow-up (n = 17), receipt of neoadjuvant therapy (n = 14), emergency or non-elective surgery (n = 5), preoperative infection within 2 weeks (n = 4), and hematologic disease or immunosuppressive therapy (n = 3), 446 patients were included in the final analysis (Figure 1). This study was approved by the Institutional Review Board of the Affiliated Huai’an No. 1 People’s Hospital of Nanjing Medical University (Approval No. KY-2026-072-01). Owing to the retrospective design and the use of de-identified data, the requirement for informed consent was waived.
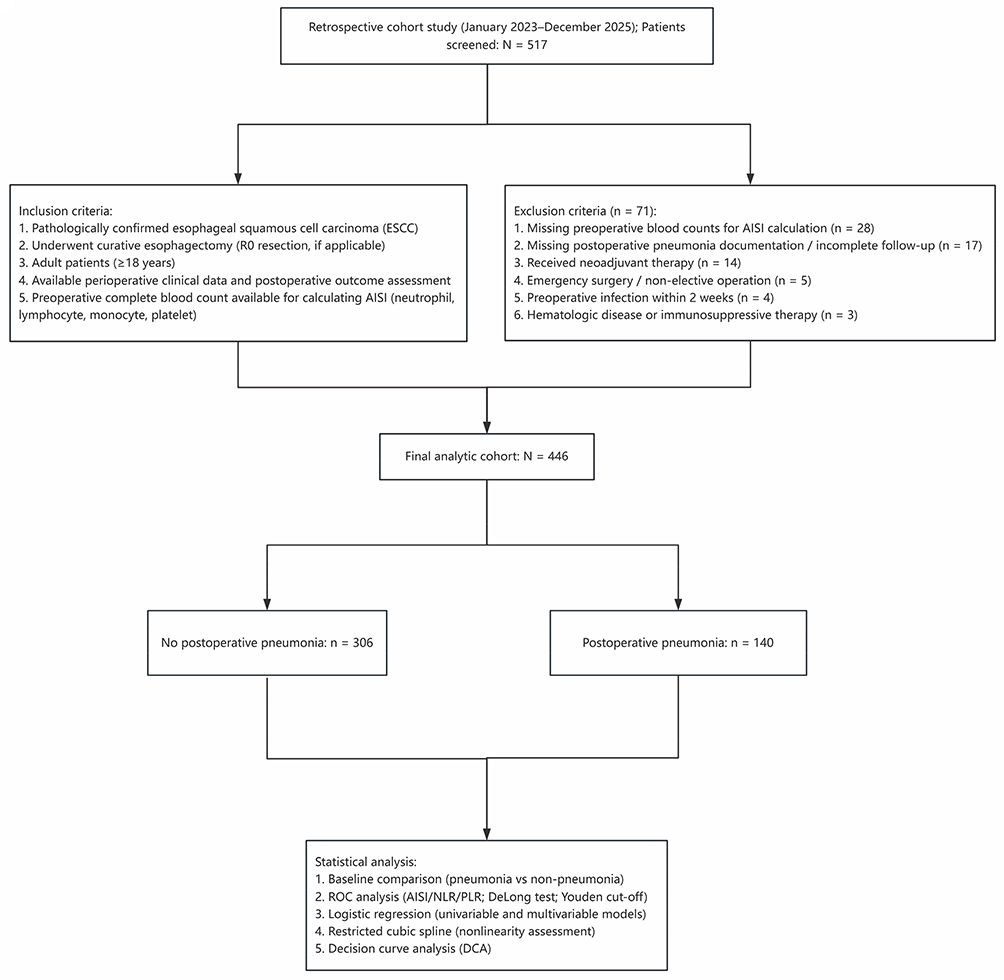 |
Figure 1 Study flow diagram. Flowchart showing patient screening, exclusion criteria, final cohort construction, postoperative pneumonia status, and planned statistical analyses. |
Baseline Data Collection and Covariates
Clinicopathological and perioperative variables were extracted from institutional medical records and standardized anesthesia and surgical documentation. Baseline characteristics included demographics (age, sex, and body mass index [BMI]), lifestyle factors (smoking and drinking), comorbidities (hypertension, diabetes mellitus, and coronary heart disease), functional and perioperative risk markers (Eastern Cooperative Oncology Group [ECOG] performance status and American Society of Anesthesiologists [ASA] physical status), cardiopulmonary function (forced expiratory volume in 1 second/forced vital capacity [FEV1/FVC] and left ventricular ejection fraction [LVEF]), perioperative factors (operative duration, single-lung ventilation time, intraoperative blood loss, and recurrent laryngeal nerve [RLN] injury), and tumor-related variables (tumor location, tumor length, differentiation, and pathological staging [pT, pN, and pTNM]). Clinical and laboratory data were extracted from institutional medical records by trained nursing staff using a predefined data-collection form. The extracted data were checked by the research team for completeness and consistency. Data extraction followed a predefined variable list based on the study protocol.
Exposure Definition: AISI and Comparator Indices
AISI was calculated from preoperative complete blood count components as follows: AISI = (neutrophil × platelet × monocyte) / lymphocyte. Two commonly used inflammatory indices were also derived for comparative analyses: neutrophil-to-lymphocyte ratio (NLR) and platelet-to-lymphocyte ratio (PLR). AISI was analyzed as both a continuous variable, scaled per 100-unit increase for regression modeling, and a dichotomized variable for sensitivity analyses using the Youden-index–derived ROC cut-off (AISI ≥ 324.4 vs < 324.4). Preoperative complete blood count values were obtained from the most recent routine test before surgery, typically within 72 hours.
Outcome Definition: Postoperative Pneumonia
The primary outcome was postoperative pneumonia within 30 days after minimally invasive esophagectomy or during the index hospitalization, whichever occurred first. Pneumonia was diagnosed when new or progressive pulmonary infiltrates or consolidation on chest imaging were present and at least two of the following criteria were documented: (1) fever (>38°C) or hypothermia (<36°C); (2) leukocytosis or leukopenia; (3) purulent sputum or respiratory secretions, or a new or worsening cough; and (4) worsening oxygenation or increased oxygen requirement.25 When available, microbiological results and initiation of antibiotic therapy for suspected pneumonia were used as supportive evidence. Alternative postoperative pulmonary conditions, including atelectasis, pulmonary edema, aspiration pneumonitis, and acute respiratory distress syndrome, were considered during outcome adjudication. Outcome adjudication was performed by two independent clinicians who were blinded to AISI values. Discrepancies were resolved by consensus or by a third senior reviewer when needed.
Statistical Analysis
Baseline characteristics were summarized for the overall cohort and stratified by postoperative pneumonia status. Continuous variables were presented as mean ± standard deviation (SD) when approximately normally distributed or as median (interquartile range [IQR]) otherwise. Categorical variables were presented as counts and percentages. Group comparisons were performed using Student’s t-test or the Mann–Whitney U-test for continuous variables and the chi-square test or Fisher’s exact test for categorical variables, as appropriate. Receiver operating characteristic (ROC) curves were used to evaluate the discriminatory performance of AISI, NLR, and PLR for postoperative pneumonia. The optimal AISI cut-off was determined using the Youden index. Areas under the curve (AUCs) were compared using the DeLong test. Univariable logistic regression was performed to estimate odds ratios (ORs) and 95% confidence intervals (CIs) for candidate variables. Continuous predictors were scaled by clinically meaningful increments: AISI per 100 units, PLR per 10 units, operative duration and single-lung ventilation time per 10 minutes, intraoperative blood loss per 50 mL, and other continuous variables per 1 unit. Multivariable analyses used a prespecified hierarchical adjustment strategy. The crude model included AISI only. Model 1 was adjusted for age, sex, and BMI. Model 2 was additionally adjusted for smoking, drinking, hypertension, diabetes mellitus, coronary heart disease, ECOG performance status, ASA physical status, and FEV1/FVC. Model 3 was further adjusted for operative duration, single-lung ventilation time, intraoperative blood loss, RLN injury, and pTNM stage. Sensitivity analyses repeated the multivariable models using dichotomized AISI with the same model definitions. Restricted cubic spline (RCS) models were used to explore potential non-linear associations between continuous AISI and postoperative pneumonia risk, using the covariate adjustment strategy of Model 3. Decision curve analysis (DCA) was performed to evaluate net benefit across threshold probabilities from 0.01 to 0.60, comparing the fully adjusted model, continuous AISI, and dichotomized AISI, with treat-all and treat-none strategies as references. Analyses were performed using complete-case data for each model or variable as reported in the tables. All tests were two-sided, and P < 0.05 was considered statistically significant. Statistical analyses were conducted using R software (version 4.5.1). ROC analyses and DeLong tests were performed using the pROC package, restricted cubic spline modeling was implemented using the rms package, and decision curve analysis was conducted using the rmda package. Logistic regression was fitted using generalized linear models, and data management was performed using the tidyverse suite. Knots for RCS models were placed at the 5th, 35th, 65th, and 95th percentiles of AISI. Net benefit was calculated using model-predicted probabilities.
Results
Study Population and Incidence of Postoperative Pneumonia
Among 517 screened patients undergoing curative minimally invasive esophagectomy for ESCC, 71 were excluded for prespecified reasons (Figure 1). The final analytic cohort included 446 patients, of whom 140 developed postoperative pneumonia and 306 did not, yielding an incidence of 31.4%.
Baseline Characteristics
Baseline characteristics stratified by postoperative pneumonia status are summarized in Table 1. Patients who developed postoperative pneumonia had higher preoperative inflammatory indices than those without pneumonia. Median AISI was 554.4 (IQR, 383.6–822.6) in the pneumonia group and 282.1 (IQR, 170.9–409.7) in the non-pneumonia group. NLR and PLR were also higher among patients with postoperative pneumonia, and all three inflammatory indices differed significantly between groups. Other baseline, perioperative, and tumor-related variables are shown in Table 1.
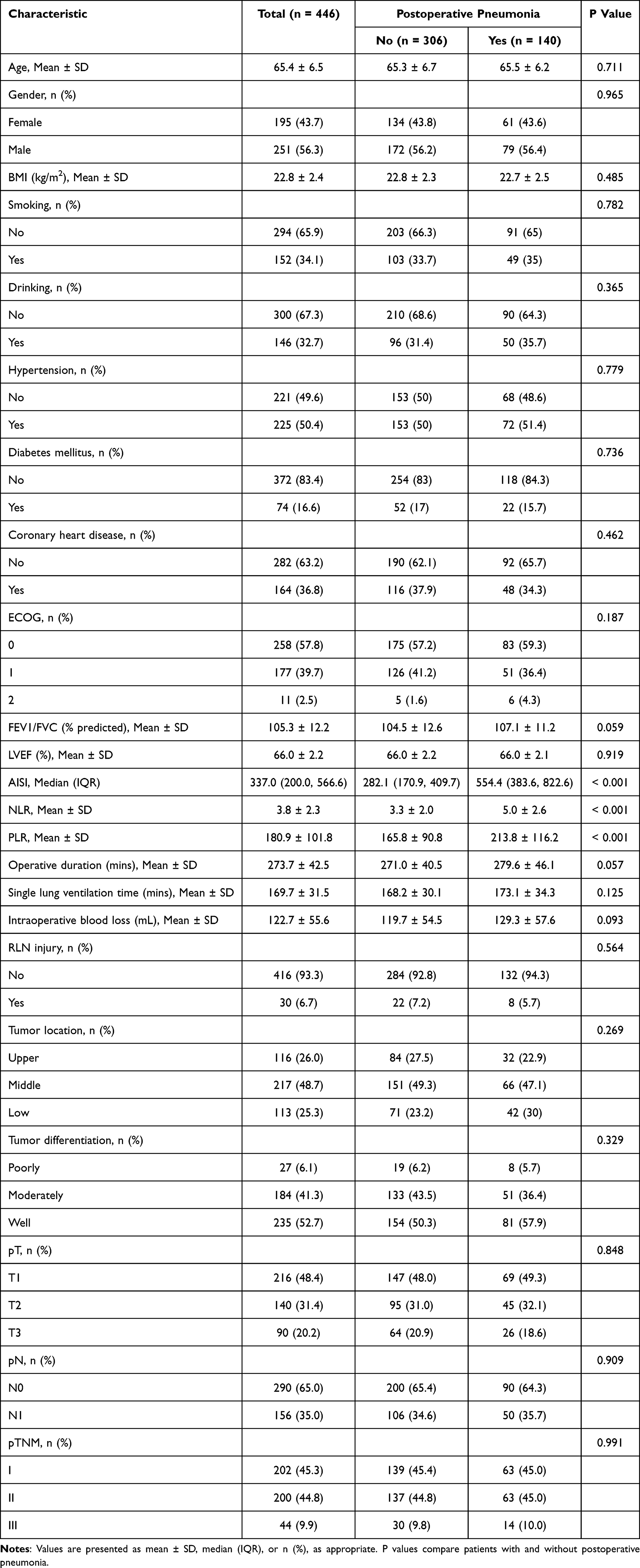 |
Table 1 Baseline Clinicopathological Characteristics of Patients Undergoing Esophagectomy for Esophageal Squamous Cell Carcinoma Stratified by Postoperative Pneumonia Status |
Discriminatory Performance of Inflammatory Indices
ROC analysis showed that AISI had good discriminatory performance for postoperative pneumonia, with an AUC of 0.795 (95% CI, 0.753–0.837) (Figure 2). The Youden-derived cut-off was 324.4, with a sensitivity of 85.7% and specificity of 63.1%. In comparative analyses, AISI showed the highest AUC among the three inflammatory indices, followed by NLR and PLR (Figure 3). Pairwise AUC comparisons using the DeLong test showed that the AUC for AISI was significantly higher than those for NLR and PLR.
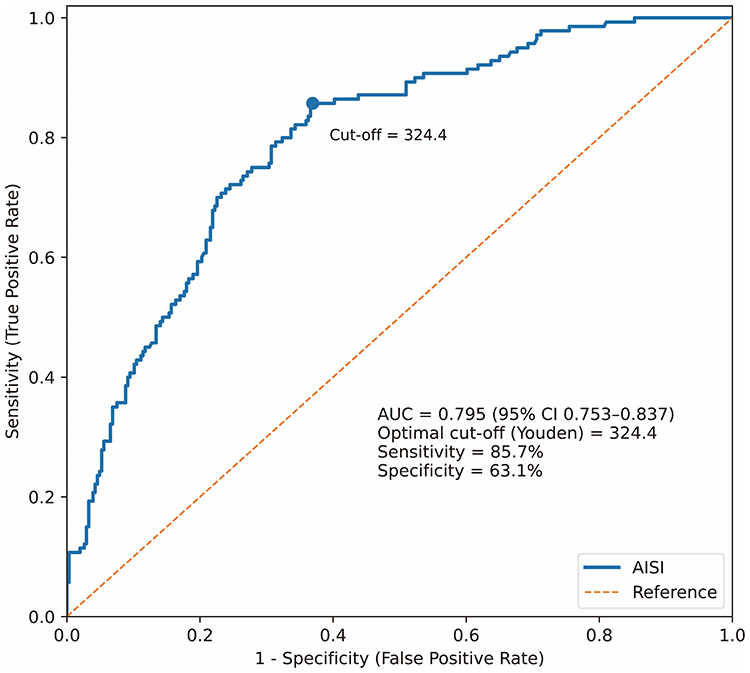 |
Figure 2 Receiver operating characteristic curve of AISI for postoperative pneumonia. The curve shows the discriminatory performance of preoperative AISI for postoperative pneumonia. The Youden-derived cut-off was 324.4, with an AUC of 0.795, sensitivity of 85.7%, and specificity of 63.1%. |
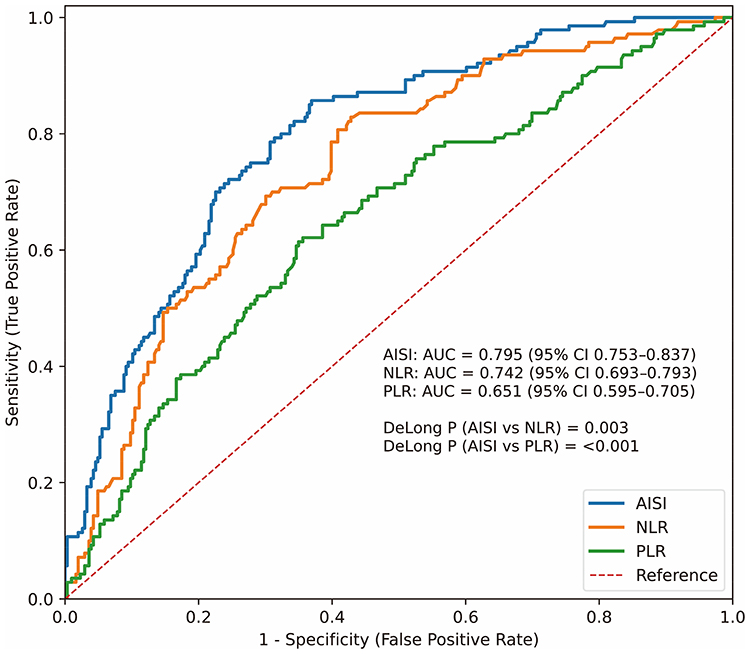 |
Figure 3 Comparison of ROC curves for AISI, NLR, and PLR. ROC curves compare the discriminatory performance of AISI, NLR, and PLR for postoperative pneumonia. AUCs and pairwise DeLong test results are shown in the figure. |
Univariable Logistic Regression Analyses
Univariable logistic regression results are presented in Table 2. AISI modeled per 100-unit increase was associated with postoperative pneumonia. NLR and PLR were also associated with postoperative pneumonia in univariable analyses. Among other candidate variables, operative duration and FEV1/FVC showed statistically significant associations.
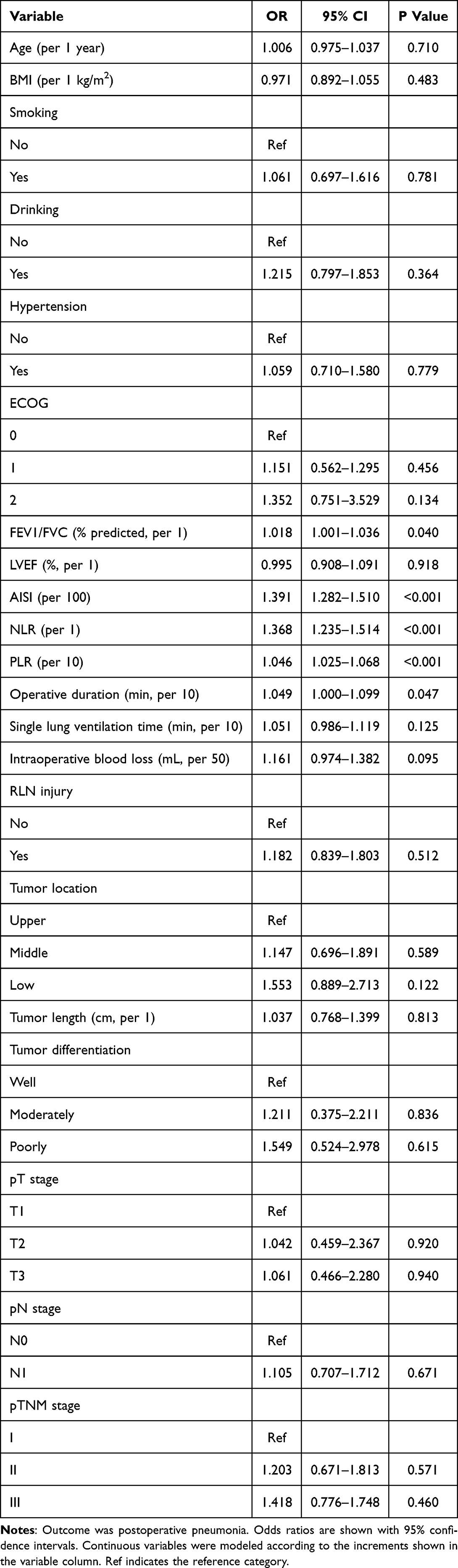 |
Table 2 Univariable Logistic Regression Analyses of Baseline Variables (Including AISI) for Postoperative Pneumonia |
Multivariable Logistic Regression and Sensitivity Analyses
In multivariable analyses, AISI remained independently associated with postoperative pneumonia across the hierarchical adjustment models (Table 3). In the fully adjusted model, each 100-unit increase in AISI was associated with higher odds of postoperative pneumonia (adjusted OR, 1.416; 95% CI, 1.301–1.576; P < 0.001). Sensitivity analyses using the Youden-derived cut-off showed consistent results (Table 4). Patients with high AISI (≥324.4) had higher odds of postoperative pneumonia than those with low AISI, and the association remained significant after full adjustment.
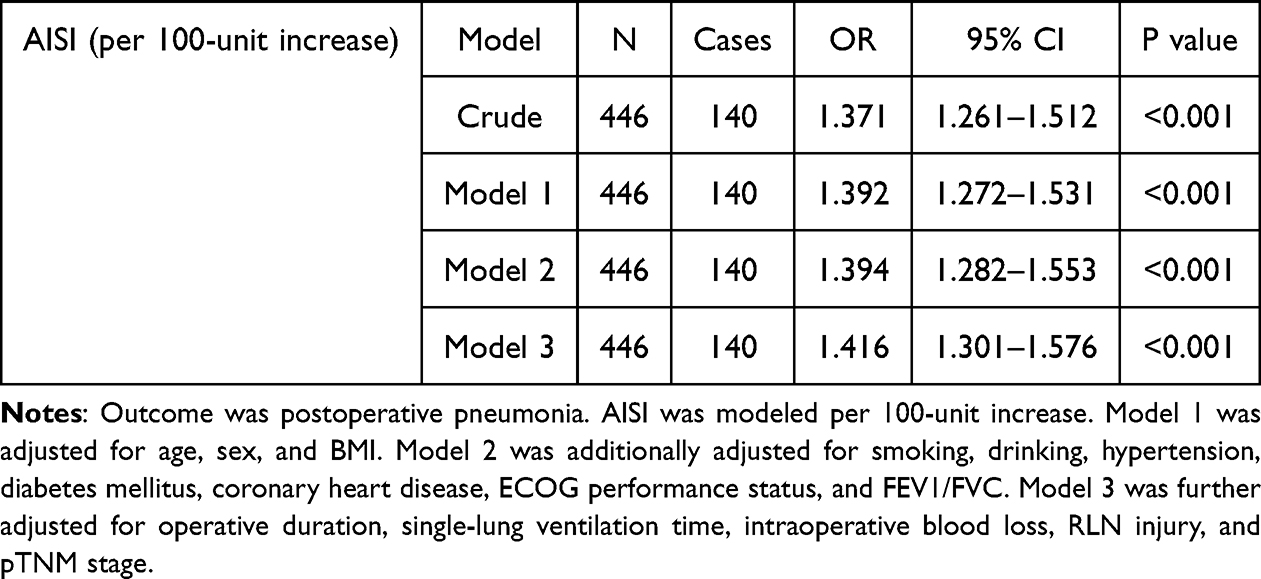 |
Table 3 Multivariable Logistic Regression Models Assessing the Association Between Continuous AISI and Postoperative Pneumonia |
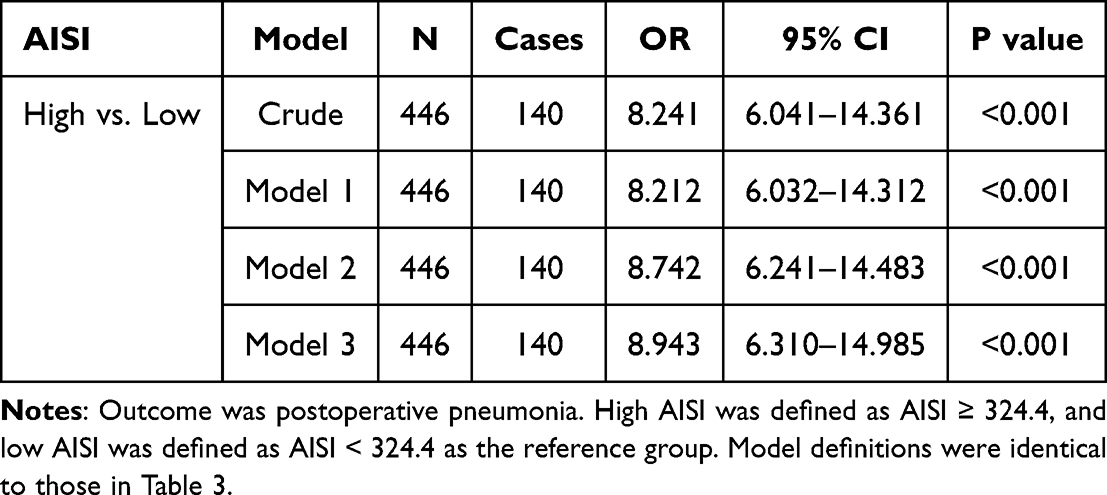 |
Table 4 Sensitivity Analysis: Multivariable Logistic Regression Models for Postoperative Pneumonia Using Dichotomized AISI |
Non-Linear Association Between AISI and Postoperative Pneumonia
Restricted cubic spline analysis suggested a non-linear association between continuous AISI and postoperative pneumonia risk (Figure 4). The overall association was statistically significant (P for overall < 0.001), with evidence of non-linearity (P for non-linearity < 0.001). The adjusted odds of postoperative pneumonia increased with higher AISI values, particularly above the reference range.
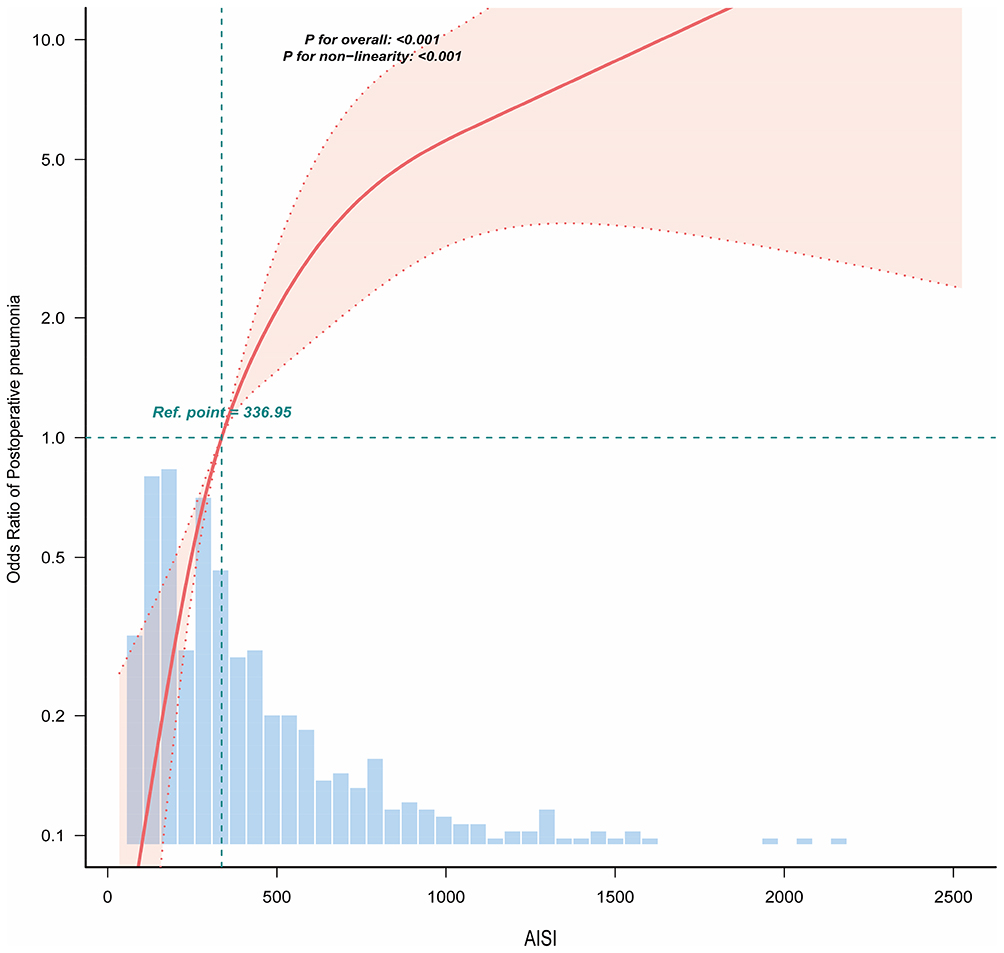 |
Figure 4 Restricted cubic spline analysis of AISI and postoperative pneumonia risk. The curve shows adjusted odds ratios for postoperative pneumonia across continuous AISI values. The reference point was AISI = 336.95, and the shaded area represents the 95% confidence interval. The histogram shows the distribution of AISI in the cohort. |
Decision Curve Analysis
Decision curve analysis compared the net benefit of the fully adjusted model, continuous AISI, dichotomized AISI, and the treat-all and treat-none strategies (Figure 5). The AISI-based models, particularly the fully adjusted model, showed higher net benefit than the reference strategies over parts of the evaluated threshold range.
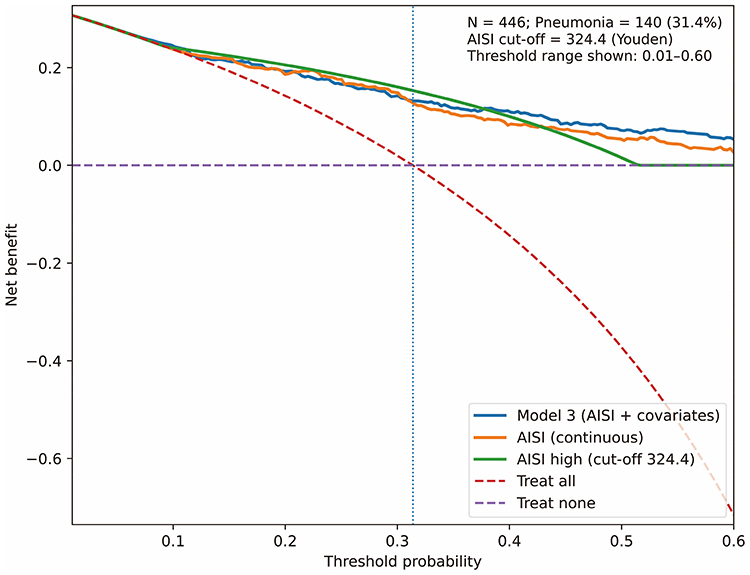 |
Figure 5 Decision curve analysis of AISI-based models. Decision curves compare the net benefit of the fully adjusted model, continuous AISI, dichotomized AISI, and the treat-all and treat-none strategies across threshold probabilities from 0.01 to 0.60. |
Discussion
In this retrospective cohort of patients undergoing minimally invasive esophagectomy for ESCC, postoperative pneumonia occurred in 31.4% of patients. Higher preoperative AISI was independently associated with 30-day postoperative pneumonia after adjustment for demographic, clinical, pulmonary function, perioperative, and pathological factors. AISI also showed better discriminatory performance than NLR and PLR in this cohort. In addition, restricted cubic spline analysis suggested a non-linear association between AISI and pneumonia risk, and decision curve analysis showed potential net benefit over selected threshold ranges. These findings suggest that AISI may be a simple preoperative marker for pneumonia risk stratification, although external validation is needed before clinical use.
Postoperative pneumonia remains one of the most important complications after esophagectomy and has been associated with delayed recovery, prolonged hospitalization, and adverse short- and long-term outcomes.1–3 Many previous studies have focused on clinical and functional risk factors, including pulmonary function, comorbidities, operative factors, and perioperative care pathways.4–7 Several risk models have been developed for postoperative pneumonia or morbidity after esophagectomy, but their generalizability may be limited by differences in patient populations, surgical approaches, candidate predictors, and outcome definitions.8–11 Therefore, routinely available biomarkers that can complement clinical assessment may be useful, particularly if they are inexpensive and easy to obtain before surgery.
Inflammation-based markers have received increasing attention in surgical risk assessment. NLR and PLR are commonly used blood count-derived indices and have been associated with postoperative complications in patients undergoing esophageal cancer surgery.14–16 AISI differs from these single-ratio markers because it integrates neutrophils, monocytes, platelets, and lymphocytes into one composite index. This may allow AISI to reflect a broader inflammatory and immune profile than NLR or PLR alone.19–24 In the present study, AISI showed higher discriminatory performance than both NLR and PLR, suggesting that this combined index may capture clinically relevant information related to postoperative pneumonia risk.
The biological interpretation of AISI is plausible but should remain cautious. A higher AISI may reflect increased neutrophil, monocyte, and platelet activity together with relative lymphopenia. This pattern may indicate an inflammatory state with reduced adaptive immune reserve before major surgery.26,27 Surgical stress, anesthesia, single-lung ventilation, tissue injury, and postoperative atelectasis can further disturb pulmonary host defense and increase susceptibility to respiratory infection.26,28–31 Therefore, elevated AISI may represent a preoperative immune-inflammatory phenotype that is more vulnerable to postoperative pulmonary infection. However, this study was not designed to determine mechanism, and these explanations should be considered hypothesis-generating.
From a clinical perspective, AISI is attractive because it is derived from routine blood tests and can be assessed before surgery. Rather than serving as a stand-alone decision rule, AISI may help identify patients who warrant closer perioperative respiratory assessment or more careful postoperative monitoring. It may also be considered alongside established clinical factors, pulmonary function, operative risk, and institutional care pathways.32 The decision curve analysis provides preliminary support for the potential clinical value of AISI-based risk stratification, but the net benefit observed in this single-center cohort should be interpreted cautiously because threshold probabilities and preventive strategies may vary across institutions.
This study has several strengths. First, AISI was evaluated as both a continuous and dichotomized variable, and the findings were consistent across the main and sensitivity analyses. Second, the study compared AISI directly with NLR and PLR in the same cohort, allowing an internally consistent assessment of discriminatory performance. Third, the analysis included multivariable adjustment, restricted cubic spline modeling, and decision curve analysis, providing information on association, possible non-linearity, and potential clinical value.
Several limitations should also be acknowledged. First, this was a retrospective, single-center study, and residual confounding or selection bias cannot be excluded. Second, postoperative pneumonia is a clinically heterogeneous outcome, and overlap with atelectasis, aspiration, pulmonary edema, or other pulmonary complications may affect outcome classification despite structured adjudication. Third, the AISI cut-off was derived from the same cohort using the Youden index, which may lead to optimism and may not be directly transferable to other populations. Fourth, although decision curve analysis suggested potential net benefit, its interpretation depends on threshold probabilities, baseline risk, and available preventive strategies. Finally, the findings require external validation and prospective evaluation before AISI can be incorporated into routine perioperative risk assessment.
Conclusion
In this retrospective cohort of patients undergoing minimally invasive esophagectomy for ESCC, higher preoperative AISI was independently associated with 30-day postoperative pneumonia and showed good discriminatory performance compared with NLR and PLR. These findings suggest that AISI may serve as a simple preoperative risk-stratification marker. External validation and prospective evaluation are needed before its use in routine clinical practice.
Data Sharing Statement
The datasets generated and/or analyzed during the current study are not publicly available because they contain information that could compromise participant privacy and are subject to institutional restrictions. Data are available from Zhiyun Xu upon reasonable request and with permission of the relevant institution.
Ethics Approval and Consent to Participate
This study was conducted in accordance with the Declaration of Helsinki and was approved by the Ethics Committee of Nanjing Medical University (Reference No. KY-2026-072-01). Owing to the retrospective design of the study and the use of de-identified data, the requirement for written informed consent was waived by the Ethics Committee.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work. Conceptualization and study design: Jianqiang Zhao and Zhiyun Xu. Data curation: Manman Gao, Haijun Sun, Yunyun Chen, Dafu Xu, and Derong Tang. Statistical analysis: Manman Gao, Yunyun Chen, and Jian Ji. Methodology: Manman Gao, Haijun Sun, and Yunyun Chen. Manuscript drafting: Manman Gao and Haijun Sun. Manuscript review and editing: all authors. Supervision: Jianqiang Zhao and Zhiyun Xu. Funding acquisition: Jianqiang Zhao and Zhiyun Xu. All authors read and approved the final manuscript.
Funding
This work was supported by Nanjing Medical University Science and Technology Development Fund (NMUB20230112) and Jiangsu Provincial Medical Key Discipline Cultivation Unit (JSDW202233). The funders had no role in the study design, data collection, analysis, interpretation, manuscript preparation, or the decision to submit for publication.
Disclosure
The authors declare that they have no competing interests.
References
1. Tanaka K, Yamasaki M, Kobayashi T, et al. Postoperative pneumonia in the acute phase is an important prognostic factor in patients with esophageal cancer. Surgery. 2021;170(2):469–15. doi:10.1016/j.surg.2021.03.051
2. Kalata S, Singh B, Graham N, et al. Epidemiology of postoperative complications after esophagectomy: implications for management. Ann Thorac Surg. 2023;116(6):1168–1175. doi:10.1016/j.athoracsur.2023.09.004
3. Manara M, Bona D, Bonavina L, Aiolfi A. Impact of pulmonary complications following esophagectomy on long-term survival: multivariate meta-analysis and restricted mean survival time assessment. Updates Surg. 2024;76(3):757–767. doi:10.1007/s13304-024-01761-2
4. Tang Z, Lu M, Qu C, et al. Enhanced recovery after surgery improves short-term outcomes in patients undergoing esophagectomy. Ann Thorac Surg. 2022;114(4):1197–1204. doi:10.1016/j.athoracsur.2021.08.073
5. Kennelly P, Davey MG, Griniouk D, et al. Evaluating the impact of enhanced recovery after surgery protocols following oesophagectomy: a systematic review and meta-analysis of randomised clinical trials. Dis Esophagus. 2025;38(1):doae118. doi:10.1093/dote/doae118
6. Maruyama S, Okamura A, Ishizuka N, et al. Airflow limitation predicts postoperative pneumonia after esophagectomy. World J Surg. 2021;45(8):2492–2500. doi:10.1007/s00268-021-06148-7
7. Sawai S, Nakatani E, Sato S, et al. Peak expiratory flow predicts the occurrence of postoperative pneumonia after esophagectomy for esophageal cancer. Dis Esophagus. 2024;37(12):doae084. doi:10.1093/dote/doae084
8. Jin D, Yuan L, Li F, et al. A novel nomogram predicting the risk of postoperative pneumonia for esophageal cancer patients after minimally invasive esophagectomy. Surg Endosc. 2022;36(11):8144–8153. doi:10.1007/s00464-022-09249-z
9. Liu J, Wang Y, Wang Y, et al. Development and validation of an online nomogram calculator to predict postoperative pneumonia in elderly patients with esophageal cancer after transthoracic esophagectomy. J Cardiothorac Vasc Anesth. 2025;39(12):3465–3474. doi:10.1053/j.jvca.2025.07.033
10. Li S, Fang C, Tao Z, Zhu J, Ma H. A nomogram for postoperative pulmonary infections in esophageal cancer patients: a two-center retrospective clinical study. BMC Surg. 2025;25(1):70. doi:10.1186/s12893-025-02794-z
11. van Nieuw Amerongen MP, de Grooth HJ, Veerman GL, et al. Prediction of morbidity and mortality after esophagectomy: a systematic review. Ann Surg Oncol. 2024;31(5):3459–3470. doi:10.1245/s10434-024-14997-4
12. Kaneta A, Sato T, Nakano H, et al. Preoperative bacterial culture can predict severe pneumonia in patients receiving esophagectomy. Fukushima J Med Sci. 2022;68(2):109–116. doi:10.5387/fms.2022-09
13. Jogiat U, Kirkland M, Verhoeff K, Bedard ELR, Kung JY, Turner SR. Oral care reduces incidence of pneumonia after esophagectomy: systematic review and meta-analysis. Langenbecks Arch Surg. 2023;408(1):209. doi:10.1007/s00423-023-02936-y
14. Shi BW, Xu L, Gong CX, et al. Preoperative neutrophil to lymphocyte ratio predicts complications after esophageal resection that can be used as inclusion criteria for enhanced recovery after surgery. Front Surg. 2022;9:897716. doi:10.3389/fsurg.2022.897716
15. Shi J, Tang S, Shen C, Xu D, Tian WZ, Xu Z. The role of nutritional and inflammatory markers in predicting postoperative complications after esophagectomy for esophageal squamous cell carcinoma: mechanisms, clinical applications, and future perspectives. Front Surg. 2025;12:1671783. doi:10.3389/fsurg.2025.1671783
16. Kato T, Oshikiri T, Goto H, et al. Preoperative neutrophil-to-lymphocyte ratio predicts the prognosis of esophageal squamous cell cancer patients undergoing minimally invasive esophagectomy after neoadjuvant chemotherapy. J Surg Oncol. 2021;124(7):1022–1030. doi:10.1002/jso.26611
17. Jiao Y, Zhang X, Liu M, et al. Systemic immune-inflammation index within the first postoperative hour as a predictor of severe postoperative complications in upper abdominal surgery: a retrospective single-center study. BMC Gastroenterol. 2022;22(1):403. doi:10.1186/s12876-022-02482-9
18. Xiaowei M, Wei Z, Qiang W, et al. Assessment of systemic immune-inflammation index in predicting postoperative pulmonary complications in patients undergoing lung cancer resection. Surgery. 2022;172(1):365–370. doi:10.1016/j.surg.2021.12.023
19. Wang HK, Wei Q, Yang YL, Lu TY, Yan Y, Wang F. Clinical usefulness of the lymphocyte-to-monocyte ratio and aggregate index of systemic inflammation in patients with esophageal cancer: a retrospective cohort study. Cancer Cell Int. 2023;23(1):13. doi:10.1186/s12935-023-02856-3
20. Zinellu A, Paliogiannis P, Mangoni AA. Aggregate index of systemic inflammation (AISI), disease severity, and mortality in COVID-19: a systematic review and meta-analysis. J Clin Med. 2023;12(14):4584. doi:10.3390/jcm12144584
21. Hosseninia S, Ghobadi H, Garjani K, et al. Aggregate index of systemic inflammation (AISI) in admission as a reliable predictor of mortality in COPD patients with COVID-19. BMC Pulm Med. 2023;23(1):107. doi:10.1186/s12890-023-02397-5
22. Ghobadi H, Mohammadshahi J, Javaheri N, et al. Role of leukocytes and systemic inflammation indexes (NLR, PLR, MLP, dNLR, NLPR, AISI, SIR-I, and SII) on admission predicts in-hospital mortality in non-elderly and elderly COVID-19 patients. Front Med. 2022;9:916453. doi:10.3389/fmed.2022.916453
23. Huang YW, Zhang Y, Li ZP, Yin XS. Association between a four-parameter inflammatory index and all-cause mortality in critical ill patients with non-traumatic subarachnoid hemorrhage: a retrospective analysis of the MIMIC-IV database (2012-2019). Front Immunol. 2023;14:1235266. doi:10.3389/fimmu.2023.1235266
24. Zinellu A, Collu C, Nasser M, et al. The aggregate index of systemic inflammation (AISI): a novel prognostic biomarker in idiopathic pulmonary fibrosis. J Clin Med. 2021;10(18):4134. doi:10.3390/jcm10184134
25. Abbott TEF, Fowler AJ, Pelosi P, et al. A systematic review and consensus definitions for standardised end-points in perioperative medicine: pulmonary complications. Br J Anaesth. 2018;120(5):1066–1079. doi:10.1016/j.bja.2018.02.007
26. Bezu L, Akcal Oksuz D, Bell M, et al. Perioperative immunosuppressive factors during cancer surgery: an updated review. Cancers. 2024;16(13):2304. doi:10.3390/cancers16132304
27. Schroth J, Weber V, Jones TF, et al. Preoperative lymphopaenia, mortality, and morbidity after elective surgery: systematic review and meta-analysis. Br J Anaesth. 2021;127(1):32–40. doi:10.1016/j.bja.2021.02.023
28. van der Poll T, Shankar-Hari M, Wiersinga WJ. The immunology of sepsis. Immunity. 2021;54(11):2450–2464. doi:10.1016/j.immuni.2021.10.012
29. Scozzi D, Liao F, Krupnick AS, Kreisel D, Gelman AE. The role of neutrophil extracellular traps in acute lung injury. Front Immunol. 2022;13:953195. doi:10.3389/fimmu.2022.953195
30. Burkard P, Schonhart C, Vogtle T, et al. A key role for platelet GPVI in neutrophil recruitment, migration, and NETosis in the early stages of acute lung injury. Blood. 2023;142(17):1463–1477. doi:10.1182/blood.2023019940
31. Ko E, Yoo KY, Lim CH, et al. Is atelectasis related to the development of postoperative pneumonia? a retrospective single center study. BMC Anesthesiol. 2023;23(1):77. doi:10.1186/s12871-023-02020-4
32. Odor PM, Bampoe S, Gilhooly D, et al. Perioperative interventions for prevention of postoperative pulmonary complications: systematic review and meta-analysis. BMJ. 2020;368:m540. doi:10.1136/bmj.m540
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Comparison of Neoadjuvant Immunotherapy Plus Chemotherapy versus Neoadjuvant Chemoradiotherapy for Patients with Esophageal Squamous Cell Carcinoma: A Propensity Score Matching Study
Zhao J, Hao S, Tian J, Li Y, Han D
Journal of Inflammation Research 2023, 16:3351-3363
Published Date: 8 August 2023
The CALLY Index as a Predictive Tool for Postoperative Pneumonia in Esophageal Squamous Cell Carcinoma: A Retrospective Cohort Study
Xu Z, Chen C, Zhao J, Li C, Zang B, Xiong X
Journal of Inflammation Research 2025, 18:5463-5475
Published Date: 23 April 2025
Predicting Postoperative Pneumonia in ESCC After Neoadjuvant Chemo-Immunotherapy: Combined Use of ARISCAT Score and Inflammatory Biomarkers
Ding J, Zhao J, Qin T, Liu C, Yang Y, Xu D, Chen Y, Xu Z
Journal of Inflammation Research 2025, 18:12855-12868
Published Date: 16 September 2025