")
Back to Journals » Patient Related Outcome Measures » Volume 13
Predictors of Non-Spontaneous Vaginal Delivery Among Mothers Who Gave Birth in Wachemo University Specialized Hospital, Hossana, Ethiopia, 2021
Received 11 October 2021
Accepted for publication 11 January 2022
Published 21 January 2022 Volume 2022:13 Pages 9—19
DOI https://doi.org/10.2147/PROM.S343866
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Robert Howland
Temesgen Tamirat, Lonsako Abute
Public Health Department, College of Medicine and Health Sciences, Wachemo University, Hossana, Ethiopia
Correspondence: Temesgen Tamirat, Email [email protected]
Introduction: Non-spontaneous vaginal delivery, such as cesarean delivery and operative vaginal deliveries, provides births other than regular vaginal pregnancy. In taking effective steps to minimize the caesarean section rate and the issues associated with it, it would be useful to examine the determinants of instrumental deliveries and their key indications. Therefore, this study aimed to determine magnitude and related factors of non-spontaneous vaginal delivery.
Methods: Facility-based analytical cross-sectional study design was used. A total sample size of 383 was used. All mothers who gave birth during data collection period and fulfill inclusion criteria were included in the study. Interviewer-administered data collection method was used. Data were entered in Epi-data and exported to SPSS to analyze both descriptive and advanced analysis.
Results: About 24.4% of mothers’ mode of delivery was non-spontaneous vaginal delivery. Those mothers whose occupation was housewives were 2.8 times more likely to give birth through non-spontaneous vaginal delivery than mothers whose occupation was teachers (AOR = 2.8 95% CI 1.103– 7.261). Mothers with grand multipara were less likely to give birth through non-spontaneous vaginal delivery than nulliparous (AOR = 0.10 95% CI 0.022– 0.468) and primipara (AOR = 0.17 95% CI 0.041– 0.671). Mothers with complications during pregnancy were 3 times more likely to give birth via non-spontaneous vaginal delivery than mothers without complications during pregnancy. Mothers with non-macrosomic neonates and female neonatal sex were less likely experiencing to give birth through non-spontaneous vaginal delivery as compared to their respective reference groups.
Conclusion: Magnitude of non-spontaneous vaginal delivery was high in this study. Being a housewife, having complications during pregnancy, nullipara and primipara, macrosomic fetus and male neonate were associated with outcome variable. Attention should be given for the housewives, experiencing complication during pregnancy, a fetus with big weight and male neonatal sex in order to minimize risks of non-spontaneous delivery.
Keywords: non-spontaneous vaginal delivery, Wachemo University, delivery, South Ethiopia
Introduction
Non-spontaneous vaginal delivery, such as Cesarean delivery, Episiotomy and Operative vaginal deliveries, provides birth rather than regular vaginal birth. The most common abdominal surgery performed by pregnant women is cesarean section delivery globally. Approximately 20 million cesarean section deliveries are expected to occur per year, with continuous rapid growth in low-, middle- and high-income countries.1–3 A study conducted between 2002 and 2012 found that the cesarean section rate increased from 18.2% in 2002 to 30.3% in 2012, with the lack of a clear indication being the most common explanation.4,5 Caesarean delivery dramatically increased the risk of pregnancy-related death of a woman (35.9/100,000) compared to a woman who delivered vaginally (9.2/100,000) fatalities, according to the American College of Obstetricians and Gynecologists (ACOG) study.6 After cesarean section, rates of pelvic pain, deep dyspareunia, and profuse bleeding requiring laparotomic hysterectomy, accidental transvesical caesarean section requiring bladder repair, female postpartum sexual dysfunction, and spontaneous miscarriage were also usual.7–11
Vaginal deliveries conducted with the use of a vacuum system or forceps are operative vaginal deliveries. It can be safely done if it is technically feasible. In any situation that affects the mother or fetus, termination of the second stage of labor by operative vaginal delivery is suggested. While surgical vaginal delivery may be carried out as infrequently as 1.5% of deliveries in some countries, in other countries it may be as high as 15%. In the United Kingdom, instrumental vaginal delivery rates range from 10% to 15%; these rates have remained reasonably stable, although the preference for the instrument has shifted.3 But studies currently indicate that the trend of instrumental deliveries is declining and is a major concern in the health care system worldwide. In taking effective steps to minimize the caesarean section rate and the problems associated with it, it would be useful to analyze the patterns of instrumental deliveries and their key indications. A five-year retrospective study conducted at a tertiary teaching hospital in Puducherry, India, on trends in instrumental deliveries found that 7.7% were instrumental vaginal deliveries among a total of 5445 deliveries that occurred during the study period. The year-wise rate of instrumental deliveries varies from 6.1% to 9.8%. A decreasing trend for instrumental deliveries was observed during the study period (except during 2011).12
Vacuum-assisted vaginal delivery was 3.6% in the United States, 11% Australia’s Royal College of Obstetricians and Gynecologists and 17.3% in Ethiopia’s Tikur Anbessa Specialist Hospital.13–15 Magnitude of caesarian section was 41.63% in Bosnian16 and 47.6% in Uganda.17 But magnitude of caesarian section in Ethiopia was 32.5% in Gurage zone Southern Ethiopia,18 38.3% in the hospitals of Addis Ababa19 and 19.2% in demographic and health survey of Addis Ababa.20
Even though there were limited studies were done in different settings of Ethiopia to determine magnitude of the caesarian section and assisted-vaginal delivery. So, this study aimed to determine magnitude of non-spontaneous vaginal delivery including both caesarian section and instrumental delivery and the associated factors related with it in Wachemo University specialized hospital, Hosanna, southern Ethiopia.
Methods and Materials
Study Area and Period
The study was conducted in Wachemo university specialized hospital from April 12th to June 1st 2021. Wachemo University is among the public universities in Ethiopia. It is located in Hossana town Hadiya zone, Southern Ethiopia and is 232 km away from the capital of Ethiopia, Addis Ababa. This specialized hospital provides both preventive and curative health care services including maternal and child care for more than 2 million populations of its catchment and its surroundings.
Study design: Facility based analytical cross-sectional study design was employed.
Population
All mothers who gave birth in Wachemo University specialized Hospital were used as source population. Those mothers who fulfilled inclusion criteria and available during data collection period were included in the study. But, those who were not willing to participate in the study were excluded.
Inclusion and Exclusion Criteria
Those mothers who gave birth during data collection period, were willing to participate in the study were included. But, those mothers who were critically ill during data collection period, unable to communicate and not willing to participate were excluded from the study.
Sample Size Determination and Sampling Procedure
The sample size was determined by using a single population proportion formula as follows:
The estimated proportion of non-spontaneous vaginal delivery among mothers who gave birth was assumed to be 50%; the margin of error is 5% and 95% CI, and final sample size was 384.
Consecutive sampling technique was used to include participants for the study. Those mothers who came and were giving birth in the hospital during data collection period were included until expected sample size was obtained.
Operational Definitions
Non-spontaneous vaginal delivery: a cesarean section or operative vaginal delivery takes place during delivery.
Vaginal surgical delivery: is a vaginal delivery carried out with the use of a vacuum system or forceps.
Instruments and Measurements
In the above study, the questionnaire was adapted from other research with an internal accuracy of @=0.87.12,13 The questionnaire was prepared in English and then translated by another person to (local language and back translated into English language) to verify its semantic equivalence. It was also pre-tested at the General Hospital in Durame. In addition to the socio-demographic data, obstetrics and outcome variable items were included in the questionnaire.
Data Collection Methods
The data were collected by interviewer-administered questionnaire that was adopted after reviewing relevant literature. It was first developed in English then translated into Amharic and translated back into English for appropriateness and easiness in approaching study participants.
The questionnaire aimed to assess mothers: socio-demographic characteristics, obstetric factors, fetal factors and others that may affect non-spontaneous vaginal delivery.
Data were collected by trained midwiferies and supervised by senior nurses. Training aim was to enhance understanding of questionnaires, data collection methods and the way they handle challenges. The training was also supposed to deal with maintaining privacy and confidentiality.
Variables: Variables dependent:-Non-spontaneous vaginal delivery.
Independent variables: Maternal factors such as age, education, home, wages, marital status, obstetric variables, fetal factors.
Data Quality Control
One-day training was given for the data collectors and supervisors on the objective, methodology, and data collection methods. The data collection tool was translated to the local language Amharic and translated back to English. The pre-test was done on 5% of the actual sample size in Durame Hospital since it was not included in the study. Based on the result of pre-test completeness, consistency and applicability of the methods or self-administered tools/questionnaires were ensured.
Data Processing and Analysis
The data were cross-checked for completeness, then entered into Epi-Data version 3.1 software and exported to SPSS version 20.0 software for further analysis. Descriptive statistics like percentages, proportions, and mean was used. The results were presented using tables, text, and charts. For the associated factors, binary logistic regression analysis was done since the outcome variable is binary. Both bi-variable and multivariable binary logistic regression analyses were employed. Model fitness was assessed using the Hosmer–Lemeshow test. Variables with a p-value of less than 0.25 in the bi-variable logistic regression were considered for the multivariable logistic regression analysis. In the multivariable logistic regression, adjusted odds ratio (AOR) with a 95% confidence interval and p-value of less than 0.05 was used to declare the factors significantly associated with non-spontaneous vagina delivery.
Ethical Consideration
Ethical approval committees of Wachemo University have approved this study according to the relevant guidelines and regulations of the university as indicated approval number Ref. WCU/115/2021 and in accordance with the Declaration of Helsinki. A formal letter was obtained from Wachemo University and submitted to the hospital administrators. After permission was obtained, informed consent was obtained from all the subjects after clearly explaining the purpose of the study since there is no need to take a blood sample, body fluid or others, other than verbal responses. They have been told that we could withdraw from the involvement at any time without any restriction. The confidentiality of participants was also ensured throughout the research process.
Result
A total of 377 mothers participated in the study, providing a 98.2% response rate.
Socio-Demographic and Obstetric Characteristics
Out of 377, 41.9% (n = 158) were found in the 20–30 age group, 78% (n = 294) of were married. Regarding gravidity: 59.9% (n = 226) were multigravida, 33.4% (n = 126) had no antenatal care visit, 42.2% (n = 159) had term delivery (Table 1).
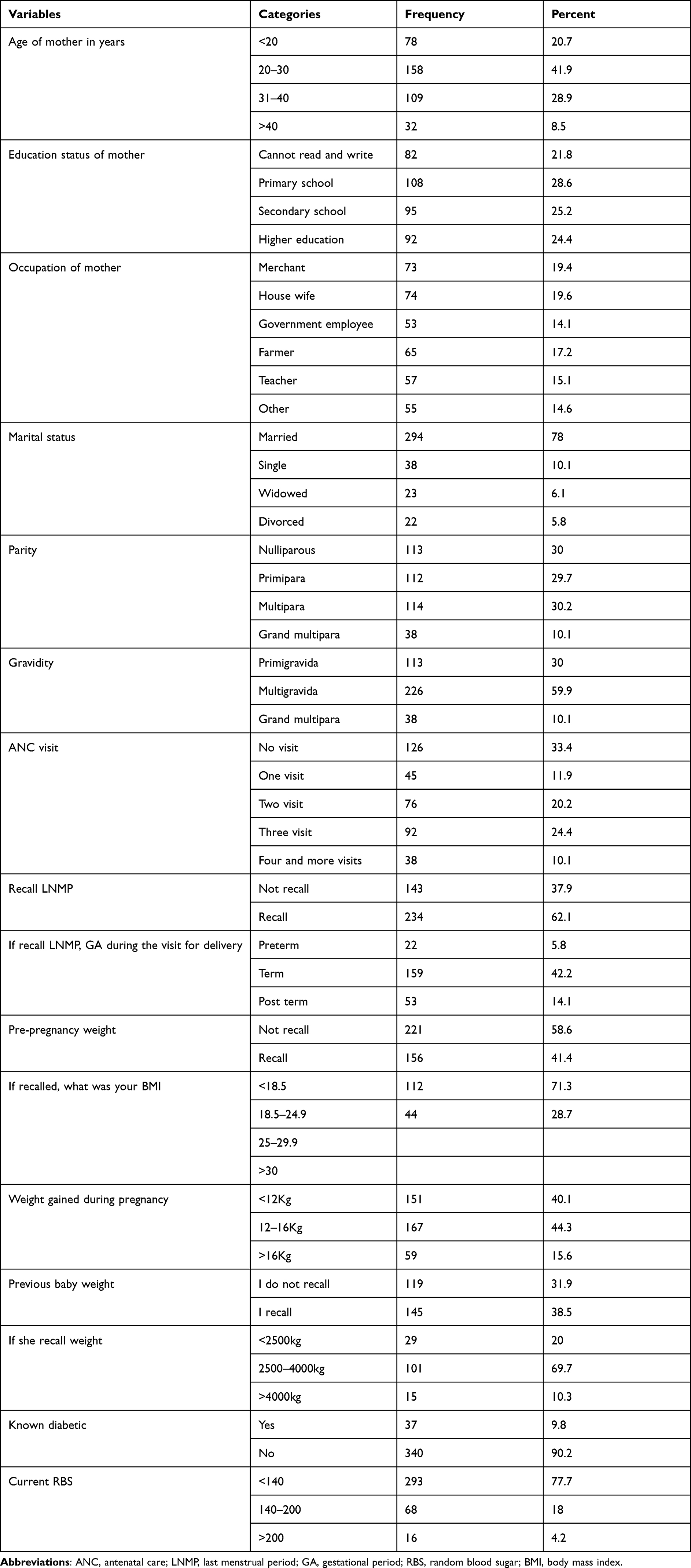 |
Table 1 Socio-Demographic Characteristics of the Mothers Who Give Birth in Wachemo University Specialized Hospital, 2021 |
Obstetric History
Out of 377: 75.6% (n = 285) gave birth through spontaneous vaginal delivery. About 6.1% (n = 23) had Macrosomia. And 27.9% (n = 105) of mothers developed complications during childbirth. The majority of neonates 68.2% (n = 257) were 2500gram-4000gram in the birth weight range (Table 2).
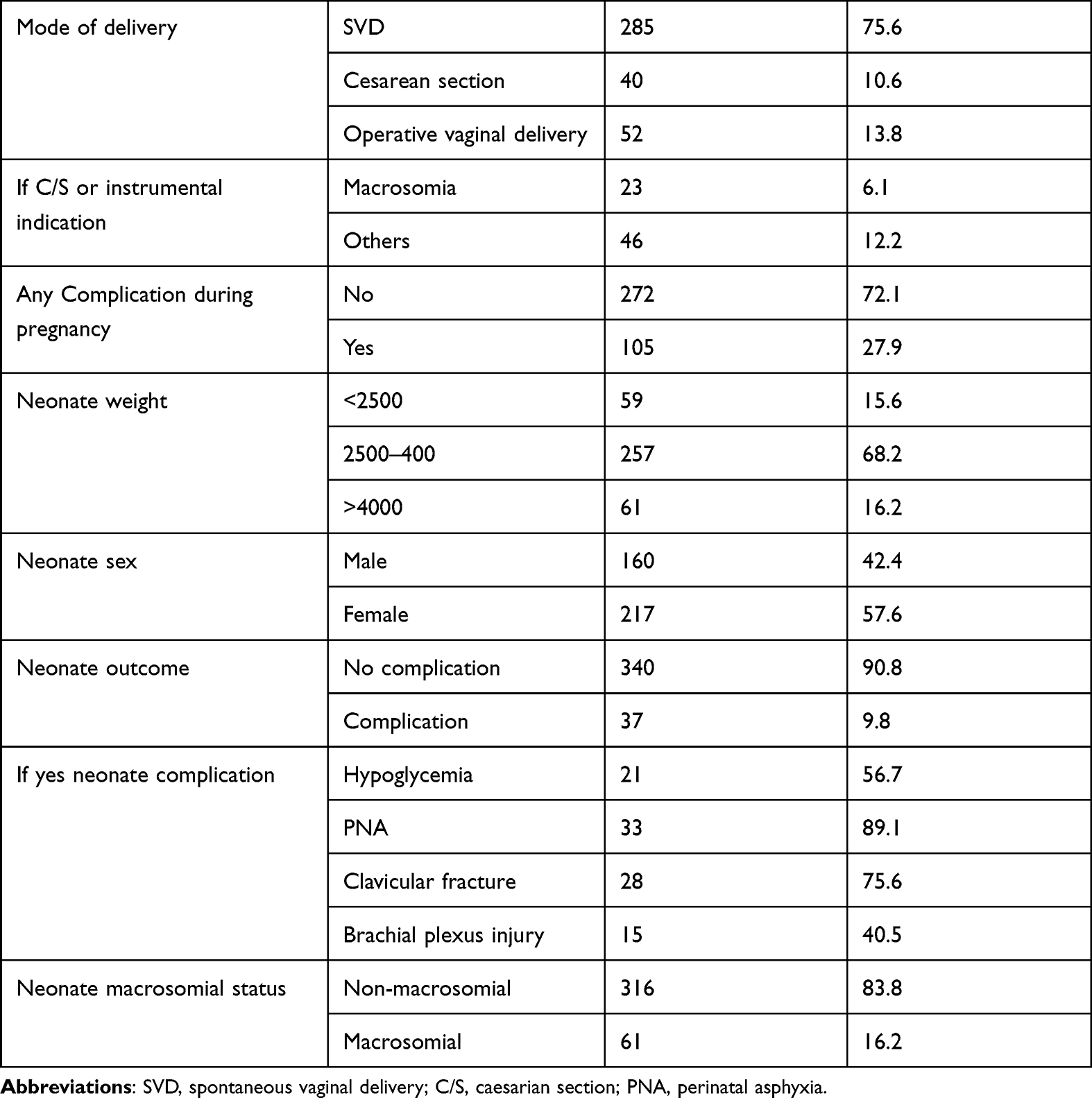 |
Table 2 Obstetric History and Neonatal Factors in Wachemo University Specialized Hospital, 2021 |
Mode of Delivery
About 24.4% (n = 92) of the mothers gave birth through non-spontaneous vaginal delivery.
Factors Associated with Non-Spontaneous Vaginal Delivery
In bivariate analysis, parity, known diabetic history, complication during pregnancy, previous neonate weight, current neonate weight and neonatal sex were identified candidates for multivariate analysis. But in multivariable logistic regression analysis: occupation, parity, complication during pregnancy, neonate sex and neonate weighing were independently and significantly associated with non-spontaneous vaginal delivery after adjustment of confounding variables.
Among socio-demographic variables, maternal occupation was associated with non-spontaneous vaginal delivery ie those mothers who were housewives by their occupation were 2.8 times more likely to give birth through non-spontaneous vaginal delivery as compared to teachers by their occupation (AOR = 2.8, 95% CI 1.103–7.261).
In this study, parity was significantly associated with non-spontaneous vaginal delivery; both nulliparous and primipara were less likely at risk of giving birth through non-spontaneous vaginal delivery as compared to grand multipara ((AOR = 0.10, 95% of CI 0.022–0.468), (AOR = 0.17 95% CI 0.041–0.671)) respectively.
Those mothers with complications during pregnancy were 3 times more likely to give birth by non-spontaneous vaginal delivery than mothers without complications during pregnancy (AOR = 3 955 CI 1.40–6.391).
Those mothers whose neonates were non-macrosomic were less likely at risk of giving birth through non-spontaneous vaginal delivery than mother whose neonates were macrosomic (AOR = 0.044 95% CI 0.012–0.119) (Table 3).
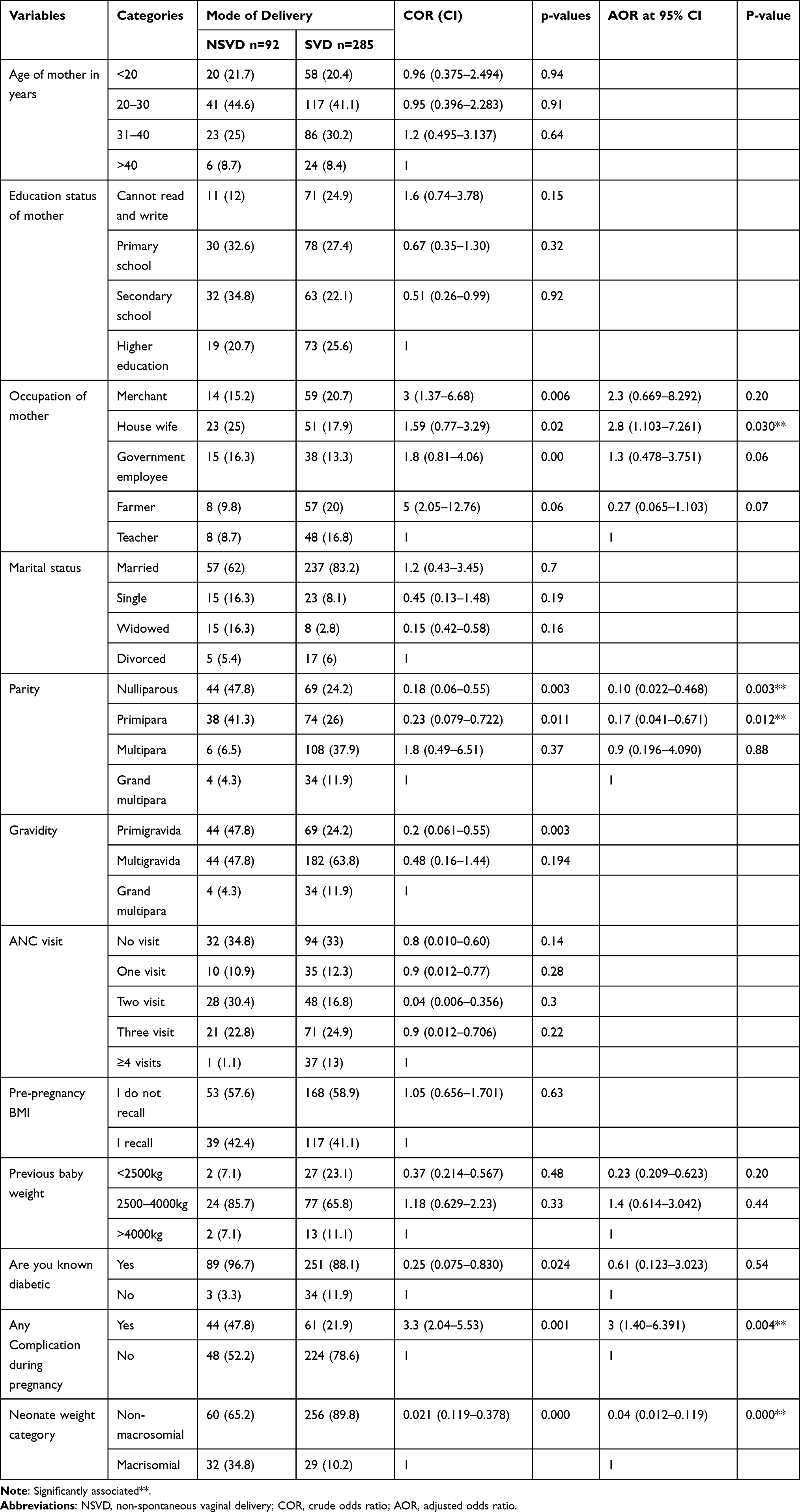 |
Table 3 Factors Associated with Non-Spontaneous Vaginal Delivery in Wachemo University Specialized Hospital, South Ethiopia 2021 |
Discussion
In this study, about 24.4% mother gave birth through non-spontaneous vaginal delivery. Of this, 13.6% was by operative vaginal delivery and 10.6% was by cesarean section. This finding of this study was higher than the studies conducted in United Kingdom, ranging from 10% to 15%; Puducherry, India (7.7%), and Jimma University (10.3%).6 But, the finding this study was lower as compared to the study done in Tuzla university clinic, Bosnian16 and Herzegovinian (41.63%) and in St. Joseph’s Hospital Kitovu, Uganda (47.6%).17 The reason behind for this difference might be varying sample size, study design, time of the study or study population.
Among total of the 377 neonates, 9.8% of neonates’ outcome ended with complication. This finding was lower than the studies conducted in Felege Hiwot Specialist Hospital, Northwest Ethiopia, where 12.1% of the participants developed complications and 17.3% of the Jimma University Medical Center. This result, however, was higher than that of the studies carried out in the United States and England.3,12 The differences might be due to socio-cultural and study period disparity.
Hypoglycemia (56.7%), perinatal asphyxia (89.1%), clavicular fracture (75.6%) and brachial plexus injury were the main complications (40.5%). However, this result varies from the studies conducted at the Aminu Kano Teaching Hospital in Kano, Nigeria.2,10
This study’s finding indicates that those mothers who were housewives by their occupation were 3 times more likely to give birth through non-spontaneous vaginal delivery as compared to those who were teachers by their occupation. But, the study conducted in Uganda indicated that housewives were not at risk of giving birth via caesarian section.17 In this study housewives might have medical problems such as blood loss, infections, organ damage, prolonged labor or abnormal positioning. Or, those mothers who were teachers by their occupation might have got sufficient information on antenatal care follow up, birth preparedness and preparedness for complication.
This research shows that mothers with grand multipara were less likely than nulliparous and primipara to give birth through non-spontaneous vaginal delivery. This result is in line with the Felege Hiwot extensive specialized hospital research, Northwest Ethiopia shows that the mother of Primipara was around 3.5 times more likely to give via non-spontaneous vaginal delivery than the mother of multipara. There is strong reasoning that supports having high chances of giving birth through non-spontaneous vaginal delivery when the mother is nullipara or primipara than grand multipara because mother has prior experiences of regular birth giving there could be dilatation of reproductive organs and birth canals, and the possibility of giving birth through non-spontaneous vaginal delivery would be reduced.
Mothers with pregnancy complications were 3 times more likely to give birth via non-spontaneous vaginal delivery than mothers without pregnancy complications. It is believed that if a mother is suspected of developing complications during pregnancy, the risk of non-spontaneous vaginal delivery may be high relative to those mothers who may not have suspected or reported complications during pregnancy, even though the result and outcome of the pregnancy cannot be determined before birth, and other studies do not support this finding.
The prevalence of macrosomal neonates in this study was 16.2%. This result is higher than Gonder (7.54%), Hawassa (11.86%), and lower than Mekele’s research (19.1%). The disparity may be due to the difference in the study period and the difference in socio-culture. Moreover, mothers giving non-macrosomal neonates were less likely than mothers giving macrosomal neonates to give birth via non-spontaneous vaginal delivery.
Conclusion and Recommendation
In this study, magnitude of non-spontaneous vaginal delivery is higher. Being a housewife and having complications during pregnancy, being nullipara and primipara and neonates being macrosomic were significantly associated predictors of non-spontaneous vaginal delivery. Mothers who suffer complications during pregnancy, as well as housewives, should be monitored closely, and neonatal weight gain should be evaluated early in order to prepare for and manage the potential risks associated with non-spontaneous vaginal delivery.
Data Sharing Statement
The datasets of this study are available on reasonable request.
Ethics Approval and Consent to Participant
Ethical approval committees of Wachemo University have approved this study according to the relevant guidelines and regulations of the university as indicated approval number Ref.WCU/115/2021 and in accordance with the Declaration of Helsinki. A formal letter was obtained from Wachemo University and submitted to the hospital administrators. After permission was obtained, informed consent was obtained from all the subjects after clearly explaining the purpose of the study since there is no need to take a blood sample, body fluid or others, other than verbal responses. They have been told that we could withdraw from the involvement at any time without any restriction. The confidentiality of participants was also ensured throughout the research process.
Acknowledgments
The authors would like to thank Wachemo University for providing this study with ethical approval. The authors want to give data collectors, managers, and participants their sincere thanks for their willingness to participate in the research.
Disclosure
The authors report no conflicts of interest for this work.
References
1. Betrán AP, Merialdi M, Lauer JA, et al. Rates of caesarean section: analysis of global, regional and national estimates. Paediatr Perinat Epidemiol. 2007;21(2):98–113. doi:10.1111/j.1365-3016.2007.00786.x
2. Luz G, Belizán JM, Lauer JA, Betrán AP, Merialdi M, Althabe F. The global numbers and costs of additionally needed and unnecessary caesarean sections performed per year: overuse as a barrier to universal coverage. World Health Rep. 2010;30:1–31.
3. Berhan Y, Abdela A. Emergency obstetric performance with emphasis on operative delivery outcome: does it reflect the quality of care? Ethiop J Health Dev. 2004;18(2):96.
4. Strom S. Rates, Trends and Determinants of Cesarean Section Deliveries in El Salvador: 1998 to 2008. University of Washington; 2013.
5. Al Rifai R. Rising cesarean deliveries among apparently low-risk mothers at university teaching hospitals in Jordan: analysis of population survey data, 2002–2012. Glob Health Sci Pract. 2014;2(2):195–209. doi:10.9745/GHSP-D-14-00027
6. ACOG. American College of Obstetricians and Gynecologists Profile of Ob-Gyn Practice; 2013.
7. Laganà AS, Cromi A, Tozzi R, Franchi M, Lukanović D, Ghezzi F. Uterine scar healing after cesarean section: managing an old surgery in an evidence-based environment. J Investig Surg. 2018. doi:10.1080/08941939.2018.1465145
8. Franchi M, Raffaelli R, Baggio S, et al. Unintentional transvesical caesarean section: incidence, risk factors, surgical technique and post-operative management. Eur J Obstet Gynecol Reprod Biol. 2019;236:26–31. doi:10.1016/j.ejogrb.2019.02.023
9. Laganà AS, Platania A, Butticè S, et al. Comment on “Impact of mode of delivery on female postpartum sexual functioning: spontaneous vaginal delivery and operative vaginal delivery vs cesarean section”. J Sex Med. 2016;13(7):1142–1143. doi:10.1016/j.jsxm.2016.03.373
10. Laganà A, Burgio MA, Ciancimino L. Evaluation of recovery and quality of sexual activity in women during postpartum in relation to the different mode of delivery: a retrospective analysis. Minerva Ginecol. 2015;67(4):315–320.
11. Williams F, Gary Cunningham Kenneth J, Leveno Steven L, et al. Operative Vaginal Delivery.
12. Instrumental Vaginal Delivery. The Royal Australian and New Zealand College of Obstetricians and Gynecologists; 2012.
13. Royal College of Obstetricians and Gynecologists (RCOG). Operative Vaginal Delivery Guideline Number 26—Jan 2011, Clinical Green Top Guidelines. London, UK: RCOG Press; 2011.
14. Adaji SE, Shittu SO, Sule ST. Operative vaginal deliveries in Zaria, Nigeria. Ann Afr Med. 2009;8(2):95–99. doi:10.4103/1596-3519.56236
15. Kabiru WN, Jamieson D, Graves W, Lindsay M. Trends of instrumental deliveries at a tertiary care teaching hospital. Am Coll Obstet Gynecol Press. 2015;5(7):20–32.
16. Cerovac A, Gordana G, Ljuca D. Mode of delivery in preterm births - Bosnian and Herzegovinian Experience. Mater Sociomed. 2018;30(4):290–293. PMID: 30936795; PMCID: PMC6377931. doi:10.5455/msm.2018.30.290-293
17. Kizito O. Determinants of caesarean section rates in private-not-for-profit healthcare facilities: St. Joseph’s Hospital_ Kitovu, Omona Kizito. Cogent Med. 2021;8:1928939. doi:10.1080/2331205X.2021.1928939
18. Mose A, Abebe H. Magnitude and associated factors of caesarean section deliveries among women who gave birth in Southwest Ethiopia: institutional-based cross-sectional study. Arch Public Health. 2021;79:158. doi:10.1186/s13690-021-00682-5
19. Tsegaye H, Desalegne B, Wassihun B, et al. Prevalence and associated factors of caesarean section in Addis Ababa hospitals, Ethiopia. Pan Afr Med J. 2019;34:136. doi:10.11604/pamj.2019.34.136.16264
20. Tebekaw Y, Mashalla Y, Thupayagale-Tshweneagae G. Patterns of caesarean-section delivery in Addis Ababa, Ethiopia. Afr J Primary Health Care Fam Med. 2016;8:1–6. doi:10.4102/phcfm.v8i2.953
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.