")
Back to Journals » OncoTargets and Therapy » Volume 13
Predictors of Neoadjuvant Chemotherapy Response in Breast Cancer: A Review
Authors Xu W, Chen X, Deng F, Zhang J, Zhang W , Tang J
Received 9 March 2020
Accepted for publication 18 May 2020
Published 22 June 2020 Volume 2020:13 Pages 5887—5899
DOI https://doi.org/10.2147/OTT.S253056
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Leo Jen-Liang Su
Weilin Xu,* Xiu Chen,* Fei Deng, Jian Zhang, Wei Zhang, Jinhai Tang
Department of General Surgery, The First Affiliated Hospital of Nanjing Medical University, Nanjing 210029, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Jinhai Tang
Department of General Surgery, The First Affiliated Hospital of Nanjing Medical University, Nanjing 210029, People’s Republic of China
Tel +86 13705163889
Email [email protected]
Abstract: Neoadjuvant chemotherapy (NAC) largely increases operative chances and improves prognosis of the local advanced breast cancer patients. However, no specific means have been invented to predict the therapy responses of patients receiving NAC. Therefore, we focus on the alterations of tumor tissue-related microenvironments such as stromal tumor-infiltrating lymphocytes status, cyclin-dependent kinase expression, non-coding RNA transcription or other small molecular changes, in order to detect potentially predicted biomarkers which reflect the therapeutic efficacy of NAC in different subtypes of breast cancer. Further, possible mechanisms are also discussed to discover feasible treatment targets. Thus, these findings will be helpful to promote the prognosis of breast cancer patients who received NAC and summarized in this review.
Keywords: breast cancer, neoadjuvant, chemotherapy, response, predictor
Introduction
Breast cancer is the most prevalently diagnosed cancer and the leading cause of cancer deaths for females.1 Apart from the traditional surgical plus adjuvant therapies, neoadjuvant chemotherapy (NAC) has been increasingly applied. Patients, especially the cohort of triple negative breast cancer ones who have undergone NAC turn out to have incredibly well pathologic complete response (pCR) rates. But those who reach to chemoresistance after NAC could suffer from a much harder time for survival, particularly in the first 3 years.2
In order to assess early responses to NAC of primary breast cancers, quantitative ultrasound (QUS), texture and molecular features alter in the first place, which are hopefully used to guide the treatment planning of refractory patients.3 Several studies indicated that the presence of tumor after NAC drawing support from histopathological examination of the tumor bed could be the golden standard as well as pCR rate. Further surrogate biomarkers could be applied for evaluating the outcomes defined by Chevallier’s system following neoadjuvant settings.4
Fine-needle aspiration cytology is considered as an accurate technique performed by experienced cytologists to assess the existence of breast cancer.5 The core breast biopsy used to be a traditional examination technique to identify the initial diagnosis of breast lumps. Fortunately, this critical technique is able to accurately predict pathologic responses after NAC.6
In previous studies, biomarker changes before and after NAC were claimed to have great clinical relevance to age or grade impacts.7 For example, ER and Ki-67 status were reported to possess obvious changes after NAC treatments in breast cancer patients. CYP1B1 was reported to be associated with taxane hypersensitivity.8 In locally advanced breast cancer, carbonic anhydrase IX (CAIX) significantly reacted to the paclitaxel plus sunitinib therapy.9
However, there was a report noted that the expression of βIII-tubulin protein, MDR1 protein, TACC3 and CAPG gene, multigene models (20- and 26-gene),and mRNA were not predictive markers for differentiating treatment benefits between ixabepilone and paclitaxel in early-stage breast cancer.10 Few circulatory molecules were found to be probable biomarkers to forecast the effects and efficacy of NAC systemically.11 Therefore, we focus on the alterations of tumor tissue-related to microenvironments such as stromal tumor-infiltrating lymphocytes status, cyclin-dependent kinase expression, non-coding RNAs transcription or other small molecular changes, to detect potentially predicted biomarkers reflecting the therapeutic activities of NAC in different subtypes of breast cancer (Table 1).
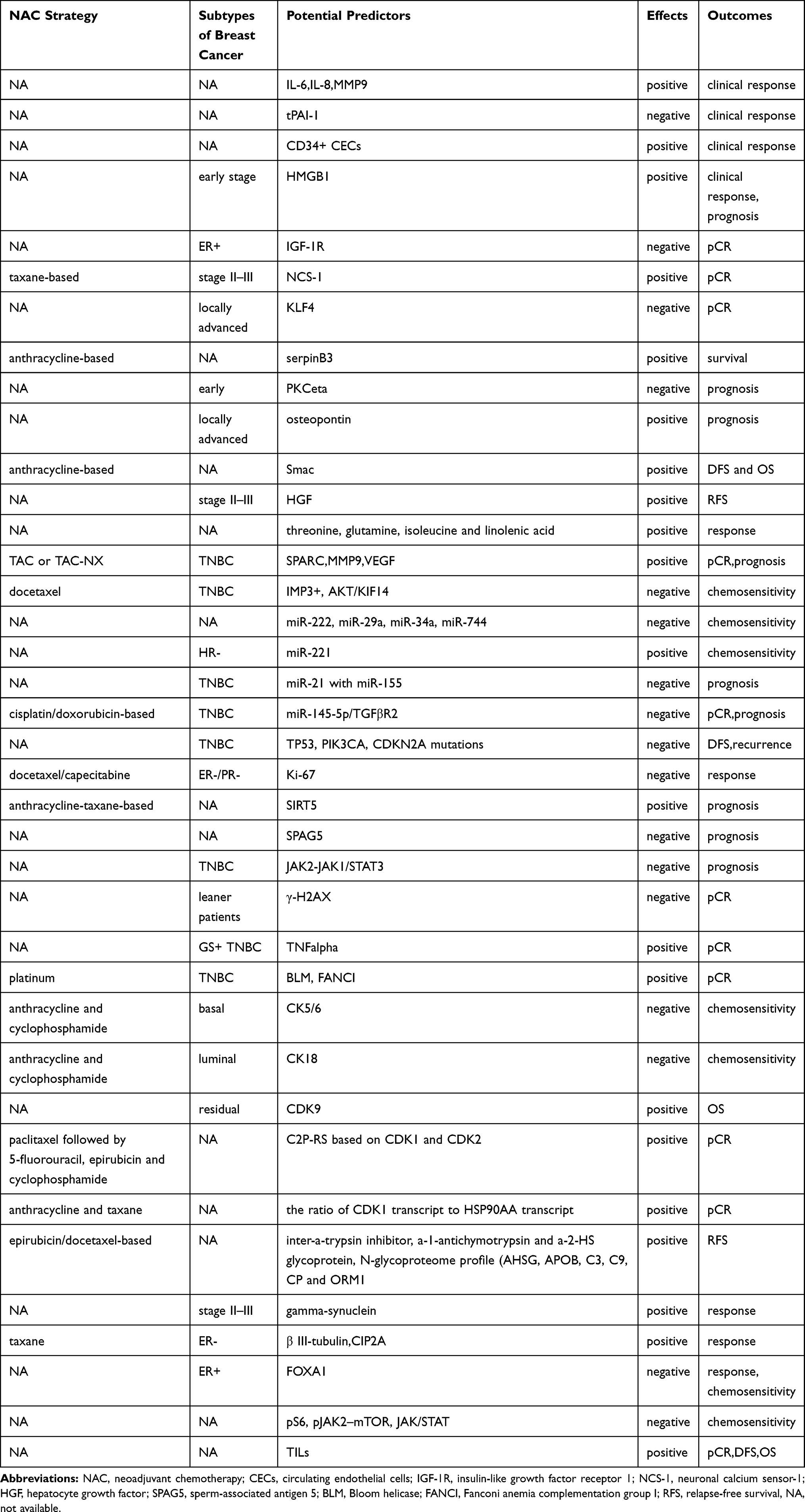 |
Table 1 Potential Predictors of Neoadjuvant Chemotherapy Response for Breast Cancer Patients |
Imaging Examination as One of the Criteria for Evaluating Treatment Outcomes
Previous evidences investigated the accuracy of MRI in evaluating residual tumor sizes in breast cancer patients after NAC, and the results supported the use of MRI to guide the following surgical planning, especially in HR- subtype of breast cancers.12,13
It is obvious that after NAC, the inner microenvironment of breast cancer patients will develop several changes which could be seen by traditional anatomical imaging or the newly improved MRI method. Besides, assessments of responses to NAC in breast cancer patients is helpful to early identification of non-responders,14 thus providing alternative treatment options to those patients suffering from poorer prognosis.15
Dynamic Contrast Enhanced MRI (DCE-MRI)
The breast DCE-MRI, with its high sensitivity and specificity, shows greater values in mammography than ultrasound. The principle of this approach is that the feature of having an enhancing curve, together with being morphologic, helps to differentiate malignant lesions from the benign ones.16 Vignati and al., applied breast DCE-MRI to 24 breast cancer patients receiving NAC (8 responders and 16 non-responders) and discovered that the vascular volume of breast cancer had significant differences between the situations before and after NAC for responders (median=1.71cc) and non-responders (median=0.41cc) by calculation from automatic vascular maps (P=0.003).17 Meanwhile, a study of 38 breast cancer patients with NAC demonstrated that tumor heterogeneity changes measured by quantitative DCE-MRI had potentials to predict pathologic responses of breast tissues to NAC.18
Diffusion-Weighted MRI
In contrast with DCE-MR, DW-MRI is more sensitive to the changes of cell density, membrane integrity and tissue microstructure caused by the changes in water motions. Breast cancers present high signal intensity images in DW-MRI, for the inflexibility of cancer lumps with subdued signal loss from Brownian motion. Besides, a breast cancer mice model evaluated the application of DW-MRI as a reliable approach for the early measurement of response to chemotherapy.19 To further confirm the advantages of DW-MRI, Galban and al., collected 39 locally advanced breast cancer patients with NAC and proved DW-MRI to be a predictive biomarker of NAC assessments.20 MRI could be fully used to measure the shrinkage of tumor,21 therefore, in addition to distinguishing its density, DW-MRI is also an alternative choice to measure its sizes with repeatable and reproducible analysis of apparent diffusion coefficient (ADC).22 Pickels and al., emphasized the significance of DW-MRI in predicting NAC responses from data of 10 patients, and found that DW-MRI delivered obvious increases or reductions in the mean (normalized) ADC at the first cycle time (P=0.005) or the second cycle time (P=0.004) of NAC treatments.23
18F-FDG PET/CT
PET/CT may trace tumor perfusion and angiogenesis in response to chemotherapy treatments. Previous studies have investigated 46 patients and demonstrated that early changes in blood flow detected by a short dynamic 18F-FDG PET/CT could be a biomarker of prognosis of triple-negative breast cancer with NAC.24 Simultaneously, in HER2 negative breast cancer subtype, a multicenter randomized Phase II neoadjuvant trial (n=59) confirmed that the early reduction in SUVmax (63.0% in pCR group comparing to 32.9% in non-pCR group; P=0.003) on 18F-FDG PET/CT 15 days after NAC was probably a potential predictor to the pCR rate in patients.25
Other Factors
The performance of MRI in breast cancer with NAC partly depends on the molecular subtypes, which tends to be more accurate under the circumstance of more aggressive cancer types than those less aggressive ones.26 While in HER2 negative cancers, it is worse in HR positive cancers than the negative ones.27 Plenty of studies were conducted to investigate other parameters which were correlated with NAC responses. Background parenchymal enhancement (BPE) on breast MRI,28 Diffuse optical spectroscopic imaging (DOSI) parameters of MRI,29 chemical exchange saturation transfer (CEST)30 were all associated with tumor responses to NAC in breast cancer patients. Furthermore, a study of 64 patients undergoing NAC for breast cancer proved that functional tumor volume (FTV) by breast MRI was a potential assessment for recurrence-free survival (HR=8.71, 95% CI: 2.86–25.5; P≤0.00015).31 Besides, thanks to the property of the high speed of the computation, the in silico Pathway Activation Network Decomposition Analysis (iPANDA) introduced by Ozerov and al., could be a scalable and robust method for stratifying breast cancer patients based on sensitivity to NAC.32
Small Molecular Changes with the Use of NAC
Changes in Subtypes
In the process of neoadjuvant therapy, small molecule changes may provide new breakthroughs in researching how to acquire better prognosis and survival (Figure 1).
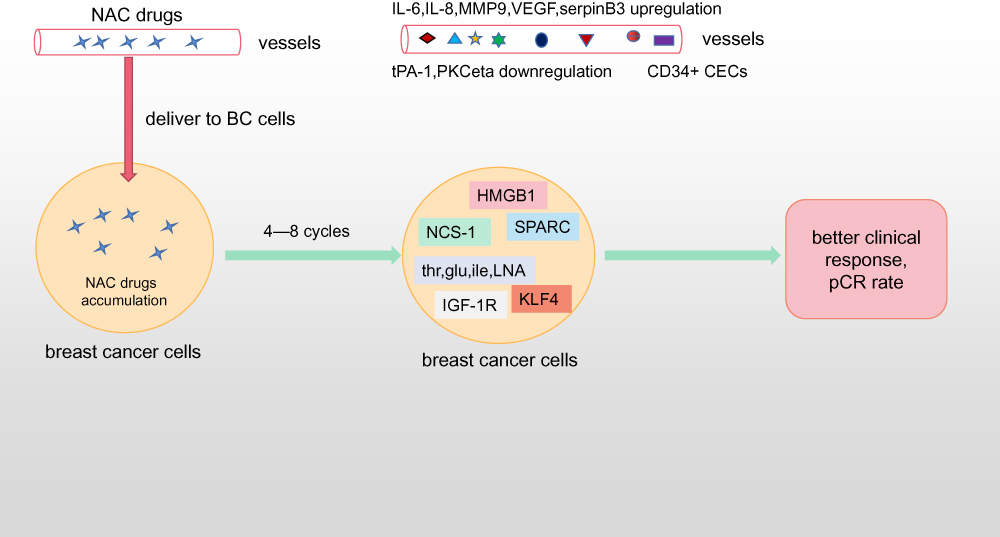 |
Figure 1 Possible responses to neoadjuvant chemotherapy in breast cancer cells and serum. After standardized NAC regiments, serum IL-6, IL-8, MMP9, VEGF, serpinB3 upregulation and tPAI-1, PKCeta downregulation with CD34+ CECs accumulation are positive predictors for better clinical responses. IGF-1R, KLF4 reduction and NCS-1, SPARC, threonine, glutamine, isoleucine and linolenic acid alteration will predict fine pCR rate. Abbreviations: NAC, neoadjuvant chemotherapy; BC, breast cancer; CEC, circulation endothelial cells; pCR, pathologic complete response. |
Nolen and al., demonstrated that elevated serum levels of IL-6, IL-8, MMP-9 (P≤0.05) and reduced serum level of tPAI-1(P≤0.05) before the initiation of NAC were associated with improved clinical response.33 The study by Ali and al., also showed that CD34+ circulating endothelial cells (CECs), in relation to tumor angiogenesis, might predict preoperative chemotherapy response in breast cancer patients.34 The chemo-induced increase HMGB1, generally considered to be released by dying cells, in plasma observed in surviving patients might be associated with a higher degree of cell death in response to therapy than in non-surviving patients. Changes of plasma HMGB1 could be a potential biomarker to predict clinical responses to NAC in breast cancer.35 Wachter and al., analyzed the association between pCR and CK5/6 or CK18 in a group of breast cancer patients undergoing NAC containing anthracycline and cyclophosphamide, and indicated that CK5/6 mainly predicted resistance to NAC in a basal subtype while CK18 predicted resistance to NAC in a luminal phenotype.36
In HR± breast cancers, a viewpoint claims that reduced insulin-like growth factor receptor 1 (IGF-1R) was related to pCR rate of NAC treatments, and thus therapies targeting IGF-1R would be an alternative choice to those who express IGF-1R.37 For stage II–III breast cancer patients, the high surviving expression was associated with pCR of NAC.38 As to the pCR of taxane-based NAC, the role of the elevated neuronal calcium sensor-1 (NCS-1) was valued.39 For locally advanced breast cancer patients, pCR rate of NAC was inhibited by an overexpression of KLF4.40
Collie and al., described that serpinB3 status might predict survival in breast cancer patients with anthracycline-based NAC.41 Studies suggested that an early increased HMGB142 or reduced PKCeta levels43 indicated better prognosis in early breast cancer patients receiving NAC. Prognosis of locally advanced breast cancer patients undergoing NAC appeared to be significantly related to osteopontin.44 Evidences also indicated that low surviving or high Smac expression in breast cancer patients treated with anthracycline-based NAC was obviously related to longer DFS and OS.45 Meanwhile, high serum hepatocyte growth factor (HGF) levels were related to longer relapse-free survival in stage II–III breast cancer receiving NAC.46
Identifying the small-molecular metabolites that are sensitive to pathological modifying by means of Metabolomics (or metabolite profiling), integration nuclear magnetic resonance spectroscopy (NMR) with liquid chromatography-mass spectrometry (LC-MS). Wei and al., observed altered metabolites of threonine, glutamine, isoleucine and linolenic acid in serum for predicting response to NAC.47
Triple negative breast cancer is not an unfavorable breast cancer because the rate of pCR after NAC is approximately 40%. This type of breast cancer has a high chemosensitivity. Regarding this subtype, the findings by Lindner and al., indicated that high expression of SPARC in the primary tumor induced a higher possibility of achieving a pCR after TAC or TAC-NX treatments.48 Moreover, IMP3+ (an oncofetal protein) along with KIF14 expression in tumors contributed to poor outcomes for the occurrence of chemoresistance to NAC in TNBC.49,50 Serum MMP-9, VEGF and secreted protein acidic and rich in cysteine (SPARC) were promising biomarkers to predict responses to NAC and prognosis of TNBC patients.51,52
miRNA Alternation
MicroRNAs (miRNAs) are 20–25 nucleotides single-stranded, non-coding RNAs that involve numerous biological processes in various cancers. Hopefully, changes of miRNAs resulted from NAC treatments in breast cancer patients may play a promising role in future precisive medicine for breast cancer.53
RNA disruption is a reduction of tumor RNA integrity followed by the application of NAC in breast cancers. It has a positive relevance to elevated DFS as well.54 The study conducted by Toomey and al., investigated the use of RNA Disruption Assay (RDA) score and they found that RDA score would be a novel, early, on-treatment approach to guide subsequent system therapies after NAC, owing to its specially speculative and predictive role in pCR rates and prognosis of HER2+ breast cancer.55
Previous data presented that several chemo-resistant miRNAs including miR-222, miR-29a, miR-34a, miR-744 and so on exhibited significantly higher expressions in post-NAC breast tumor cells than pre-NAC tumors. Simultaneously, relatively high expressions of miR-222, miR-29a and other 5 miRNAs were associated with non-responders to NAC therapy.56 Moreover, for breast cancer patients receiving previous NAC with different levels of plasma miR-221, their overall response rates varied. And higher miR-221 level, as a chemosensitivity biomarker, was more frequently found in HR- patients.57 The serum miR-21 together with miR-155 which were poor prognostic predictors, endured obvious suppressions by NAC therapy especially in TNBC, thus being potential biomarkers for outcomes of patients with NAC.58,59 Besides, miR‑145‑5p was reported to discriminate between pCR and non-pCR TNBC patients with cisplatin/doxorubicin‑based NAC, and miR‑145‑5p was proven to impair cell proliferation partly by targeting TGFβR2.60
Besides, some researches explored the specific function of circulating tumor DNAs in TNBC patients with residual tumors after NAC. TP53 mutations, PIK3CA mutations, CDKN2A mutations were the three most prevalent predictors for inferior DFS and rapid recurrence in breast cancer patients.61
Ki-67
Ki-67 is a well-known proliferation marker, even reported as a continuous marker,62–64 in breast tumors or even locally advanced breast cancer.65 With the development of treatment strategies such as NAC, endocrine therapy and chemo-endocrine therapy, the Ki-67 index presents a significant reduction to estimate the decreased proliferation index of individual tumors.66,67 Interestingly, Enomoto and al., found Ki-67 suppression only in those patients who attained clinical response and who were ER positive subgroup after NAC.68 Ohno and al., observed that Ki-67 may be useful in identifying responses to preoperative docetaxel/capecitabine therapy in early-stage breast cancer.69 Also, with the help of Ki-67 status, NAC was reported to be more effective in ER-/PR- and high Ki-67 breast cancer patients.11 Therefore, reexamining the Ki-67 level after NAC might be useful to optimize the appropriate following systemic therapy and achieve better prognosis.70
Gene-proteins in the prediction to NAC response
Gene
Although with increasing effects of recent therapies, Toi and al., recognized the necessity to incorporate biomarkers, which enables researchers to further classify conventional subtypes by methods including genetic mutations and epigenetic phenotypes in order to realize better planning of treatment. It is also crucial to analyze tumor biology particularly the tumor development in the metastasis process and the clonal selection by the treatment in clinical settings.71
The researchers exhibited that the response of anthracycline-taxane-based chemotherapy may be influenced by SIRT5 through Rho pathway. SIRT5 upregulation in various degrees may be specific to certain histological subtypes, and SIRT5 mRNA in high level may imply the good prognosis.72 The findings by Abdel and al., showed that gene copy number aberration, transcript and protein on sperm-associated antigen 5 (SPAG5) were connected with poor prognosis, such as TP53 mutation, PAM50-LumB phenotype, and PAM50-HER2 phenotype. As predictive markers in breast cancer, both SPAG5 transcript and protein may be the key point for chemo-response.73
Compared to TNBC untreated with chemotherapy, the treated group showed greater frequency of amplification on JAK2. Balko and al., reported that combining JAK2-specific inhibitors with chemo-agents could delay the progression in TNBC with the aid of JAK1/STAT3-independent signaling program derived by JAK2.74 Barba and al., found that the predictive meaning of γ-H2AX might be different based on the Body Mass Index (BMI) status in TNBC. In leaner patients, γ-H2AX upregulation seems to be correlated with lower pCR rate, while, in heavier patients, the differences in pCR rates based on γ-H2AX levels did not make significant senses.75 Bardia and al., explored a TNFα-based gene expression signature associated with pCR and confirmed a biomarker-driven targeted therapy approach for selected patients with GS-positive TNBC.76
Both of the genes, which are Bloom helicase (BLM) and Fanconi anemia complementation group I (FANCI), could increase the amount of DNA and expressed in the platinum-sensitive with TNBC. Among them, BLM overexpression promoted DNA damage and upgraded sensitivity to cisplatin.77
Cyclin-Dependent-Kinase Expression
It is well known that CDK4/6 inhibitors block the phosphorylation of retinoblastoma tumor suppressor proteins, thereby preventing the progress of the cell cycle. Nowadays, there are three selective CDK4/6 inhibitors (Palbociclib, Ribociclib and Abemaciclib) approved by the FDA and EMA for the treatment of breast cancer with HR+/HER2-.78 With the help of CDK1 and CDK2 to establish the cell cycle profiling risk score (C2P-RS), Kim and al., indicated a positive association pCR and the predictive model in breast cancer patients received NAC by paclitaxel followed by 5-fluorouracil, epirubicin and cyclophosphamide (P-FEC).79 Schlafstein and al., analyzed the residual breast cancer after NAC and found that the expression of CDK9 was discovered to be a promising positive indicator to the improved 3 years OS.80 Moreover, the ratio of CDK1 transcript to HSP90AA transcript was significant in the predictor of pCR for patients receiving NAC.81 Besides, quinone oxidoreductase 1 (NQO1) was observed to rise in terms of the residual breast tumor tissues after NAC.82
Serum Proteins
The role of serum proteins pattern to predict chemo-sensibility has been extensively studied in the field of breast cancers. Prediction of the responses to NAC tends to improve effective treatment strategies of advanced breast cancer patients.
It was the very first time for Michlmayr and al., to study the complement cascade alterations by NAC in breast cancer. When patients were treated by epirubicin/docetaxel-based NAC, activation of complement component C3 occurred, followed by modulations of protein spots 195 and 529 in C3, as well as inter-a-trypsin inhibitor, a-1-antichymotrypsin and a-2-HS glycoprotein.83 N-glycoproteome profile (AHSG, APOB, C3, C9, CP and ORM1) were confirmed to identify sensitive responders to DC+AC NAC in breast cancer and to predict RFS.84 In stage II to III locally advanced breast cancers, combination of gamma-synuclein and other biomarkers may speculate responses to NAC.85 At the same time, overexpression of class III β –tubulin (β III-tubulin) and CIP2A may serve as a positive prediction to responses in taxane-based NAC for ER- breast cancer patients.86,87
FOXA1 expression before NAC was correlated with poor chemo response in ER± as well as luminal A and B breast cancer patients (P=0.002, 0.001, and 0.049 respectively). There is also a significant correlation between the change in FOXA1 staining position and chemo-sensitivity after NAC (P=0.024). Thus it was decided that FOXA1 expression might independently predict chemosensitivity to NAC in ER± breast cancer patients.88
Signal Pathways
In the study of the prognosis of NAC for breast cancer, signaling pathways are a new choice and the key point for many researchers.
The phenomenon of chemo-sensitivity in patients treated with docetaxel mediated by increasingly low expression of KIF14, which might be descended with AKT activity, finally led to pro-survival pathways downgraded.50
The study by Jhaveri and al., exhibited that the increase in the expression with pS6, pJAK2, pSTAT3 and IL6 existed in IBC and IDC treated with NAC. Both pS6 and pJAK2 active status in IBC may imply dual targeting of mTOR and JAK/STAT pathways, and these findings inferred a potential mechanism following NAC.89(Figure 2)
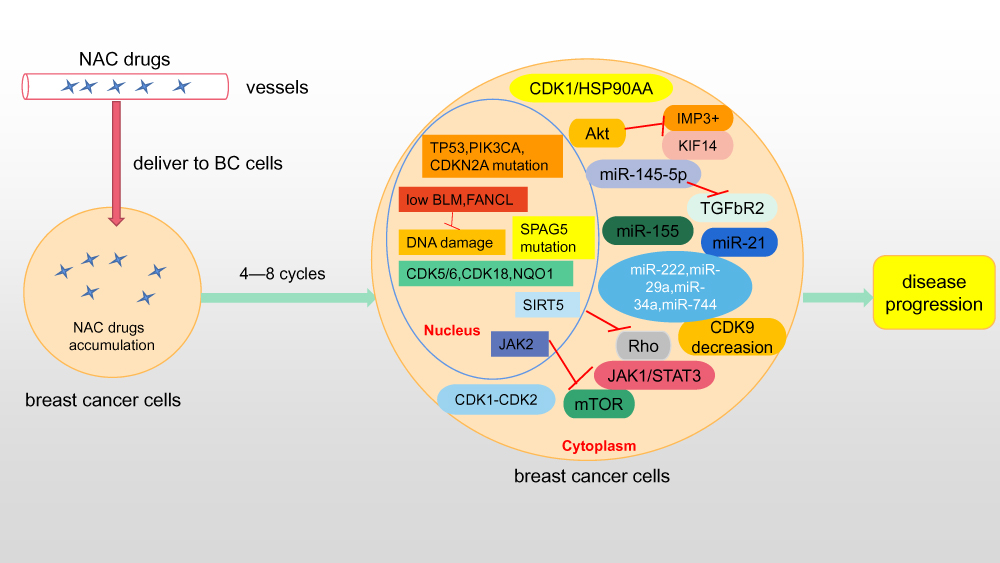 |
Figure 2 Several genetic, miRNA changes and pathways in breast cancer cells after neoadjuvant chemotherapy. Abbreviations: NAC, neoadjuvant chemotherapy; BC, breast cancer. |
Tumor-Infiltrating Lymphocytes (TILs)
The number of circulating endothelial progenitor cells is correlated with NAC response.90 In details, reports discovered that the high peripheral lymphocyte count was a positive predictor of NAC effectiveness, while low peripheral neutrophil counts might result in a favorable DFS.91
Among breast cancer patients who received NAC, immune responses like tumor-infiltrating lymphocyte (TIL) counts was associated with high-grade, ki67, and HR- breast cancer.92,93 High levels of TIL were observed in TNBC patients and were associated with pCR in ER- breast cancers.94–97
TILs can be classified into two subgroups: lymphocytes infiltrating the tumor stroma (stromal TILs) and lymphocytes infiltrating the tumor epithelial cells (intra-tumoral).98 Both of them were associated with pCR in HER2+ and TNBC breast cancers.95,99,100 The Breast International Group 02–08 trial indicated that each 10% elevation in intra-tumoral and stromal TILs was respectively related to 17% and 15% reduced relapse risk (adjusted P=0.1 and P=0.025), 27% and 17% reduced death risk (adjusted P=0.035 and P=0.023) in node-positive, ER-/HER2- breast cancer patients.101 Interestingly, sTILs alone may be an essential evaluation in the assessment of pCR rates to NAC and prognosis in HER2+ breast cancers.100,102
The majority of TILs are T lymphocytes, and B lymphocyte infiltrations are less common.103 Abundant counts of CD8+ TILs were verified to be associated with improved prognosis and prolonged survivals of less aggressive breast cancer subtypes with over 1300 cases.104 The presence of FOXP3+ sTILs, instead of the intra-tumoral FOXP3+ TILs, was reported to be able to forecast a poor prognosis, and the CD8+/FOXP3+ TIL ratio (CFR) can be invented to identify well responders to NAC in breast cancers, especially in TNBC.95,105 The increasing pCR rates and better RFS were obviously relevant to high changes of CFR in breast cancer patients with NAC,106 especially in HR+/HER2- subgroups.107
In contrast, γδ TILs were responsible for poor prognosis in another study.108 Similarly, programmed death (PD)-1+ TILs were observed to result in inferior OS in luminal B and basal-like breast cancer types.109
Therefore, lymphocyte-predominant breast cancer (LPBC) mainly had an increased pCR rates in HER2+ and TNBC cases undergoing anthracycline and taxane based NAC treatments.110,111
Besides, a profile including 7270 samples reflected that higher fraction of M0 macrophages and activated mast cells were independently associated with worse DFS (HR=1.66, 95% CI: 1.18–2.33) or OS (HR=1.71, 95% CI: 1.12–2.61) in ER+ or ER+/HER2- tumors and worse DFS (HR=5.85, 95% CI: 2.20–15.54), OS (HR=5.33, 95% CI: 2.04–13.91) in HER2+ tumors.112
Despite of the helpful role of TILs in stratifying prognostic breast cancer subgroups and in guiding future therapy decisions, a standard definition of TILs is still under confirmation. There is a lot to solve until they are applied in routine clinical practices. Therefore, TILs are emerging biomarkers mediating tumor response to NAC treatments.
Discussion
Surgery was the vital therapy for breast cancer patients in the past decades. With the development of technologies, NAC raises its significant power in the treatment of breast cancer. If breast cancer patients have one of the following conditions, neoadjuvant therapy is usually recommended: 1) the mass is larger than 5cm;2) being axillary lymph node metastasis;3)Her-2± subtype breast cancer;4) triple negative breast cancer;5) the proportion of primary tumor to breast is large but patients who wish to retain the breast. The positive lymph node after NAC was used to be considered as the predictor for the development of metastasis in breast cancer patients and for the following choices for therapy strategies.113,114 Unfortunately, no specific biomarker for predicting the clinical response to NAC has yet been defined.
Background parenchymal enhancement (BPE) on breast MRI was described as an independent marker for breast cancer risk assessment, diagnosis, and treatment. However, BPE is influenced by endogenous and exogenous hormone levels, so its application in breast cancers may be somehow limited.115 Therefore, researches tried to find that PET/CT imaging features might be potential predictors of pCR rate of NAC in locally advanced breast cancer patients,116 but the cost and inconvenience hindered its way to be used broadly. Simultaneously, an increasing number of scientists are endeavoring to find the breaking points in cancerous treatments by investigating the tumor microenvironments, such as surrounding immune cells, adipocytes, secreted small molecules and so on.117
Therefore, we summarized the alterations of microenvironments related to tumor tissue to reflect the NAC response, such as the changes in the stromal tumor-infiltrating lymphocytes status, cyclin-dependent kinase expression, non-coding RNAs transcription or other small molecular. We aim to detect potentially predicted biomarkers to reflect the therapeutic activities of NAC in different types of breast cancer. Therefore, it will be possible to promote the prognosis of breast cancer patients who received NAC by monitoring the response predictors.
Conclusion
After overviewing relevant studies, it is concluded that cellular and molecular changes (such as stromal tumor-infiltrating lymphocytes status, cyclin-dependent kinase expression, non-coding RNAs transcription) in tumor microenvironments are potential predictors to reflect the NAC response of breast cancer patients, which will be helpful to optimize the therapeutic strategy of breast cancer patients.
Ethical Approval
This article does not contain any studies with human participants or animals performed by any of the authors.
Funding
This research was supported by the National Key Research and Development Program of China (No. 2016YFC0905900), National Natural Science Foundation of China (No. 81872365 and NO.81902987), and Jiangsu Provincial Key Research Development Program(No.BE2019731).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Siegel RL, Miller KD, Jemal A. Cancer statistics, 2020. CA Cancer J Clin. 2020;70(1):7–30. doi:10.3322/caac.21590
2. Liedtke C, Mazouni C, Hess KR, et al. Response to neoadjuvant therapy and long-term survival in patients with triple-negative breast cancer. J Clin Oncol. 2008;26(8):1275–1281. doi:10.4049/jimmunol.1201892
3. Sannachi L, Gangeh M, Tadayyon H, et al. Response monitoring of breast cancer patients receiving neoadjuvant chemotherapy using quantitative ultrasound, texture, and molecular features. PLoS One. 2018;13(1):e0189634. doi:10.1016/j.clbc.2012.01.009
4. Vasudevan D, Jayalakshmy PS, Kumar S, et al. Assessment of pathological response of breast carcinoma in modified radical mastectomy specimens after neoadjuvant chemotherapy. Int J Breast Cancer. 2015;2015:536145. doi:10.1155/2015/536145
5. Garbar C, Cure H. Fine-needle aspiration cytology can play a role in neoadjuvant chemotherapy in operable breast cancer. ISRN Oncol. 2013;2013:935796. doi:10.1155/2013/935796
6. Layman RM, Thomas DG, Griffith KA, et al. Neoadjuvant docetaxel and capecitabine and the use of thymidine phosphorylase as a predictive biomarker in breast cancer. Clin Cancer Res. 2007;13(14):4092–4097. doi:10.1158/1078-0432.CCR-07-0288
7. Xian Z, Quinones AK, Tozbikian G, et al. Breast cancer biomarkers before and after neoadjuvant chemotherapy: does repeat testing impact therapeutic management? Hum Pathol. 2017;62:215–221. doi:10.1016/j.humpath.2016.12.019
8. Rizzo R, Spaggiari F, Indelli M, et al. Association of CYP1B1 with hypersensitivity induced by taxane therapy in breast cancer patients. Breast Cancer Res Treat. 2010;124(2):593–598. doi:10.1007/s10549-010-1034-5
9. Brown-Glaberman U, Marron M, Chalasani P, et al. Circulating carbonic anhydrase IX and antiangiogenic therapy in breast cancer. Dis Markers. 2016;2016:9810383. doi:10.1155/2016/9810383
10. Horak CE, Pusztai L, Xing G, et al. Biomarker analysis of neoadjuvant doxorubicin/cyclophosphamide followed by ixabepilone or Paclitaxel in early-stage breast cancer. Clin Cancer Res. 2013;19(6):1587–1595. doi:10.1158/1078-0432.CCR-12-1359
11. Jin G, Han Y, Liu C, et al. Evaluation of biomarker changes after administration of various neoadjuvant chemotherapies in breast cancer. Int J Clin Exp Pathol. 2015;8(1):914–921.
12. Um E, Kang JW, Lee S, et al. Comparing accuracy of mammography and magnetic resonance imaging for residual calcified lesions in breast cancer patients undergoing neoadjuvant systemic therapy. Clin Breast Cancer. 2018;18(5):e1087–e91. doi:10.1016/j.clbc.2018.03.011
13. Chen JH, Bahri S, Mehta RS, et al. Impact of factors affecting the residual tumor size diagnosed by MRI following neoadjuvant chemotherapy in comparison to pathology. J Surg Oncol. 2014;109(2):158–167. doi:10.1002/jso.23470
14. Dietzel M, Kaiser C, Pinker K, et al. Automated semi-quantitative analysis of breast MRI: potential imaging biomarker for the prediction of tissue response to neoadjuvant chemotherapy. Breast Care (Basel). 2017;12(4):231–236. doi:10.1159/000480226
15. O’Flynn EA, DeSouza NM. Functional magnetic resonance: biomarkers of response in breast cancer. Breast Cancer Res. 2011;13(1):204. doi:10.1186/bcr2815
16. Warner E, Plewes DB, Shumak RS, et al. Comparison of breast magnetic resonance imaging, mammography, and ultrasound for surveillance of women at high risk for hereditary breast cancer. J Clin Oncol. 2001;19(15):3524–3531. doi:10.1200/JCO.2001.19.15.3524
17. Vignati A, Giannini V, Carbonaro LA, et al. A new algorithm for automatic vascular mapping of DCE-MRI of the breast: clinical application of a potential new biomarker. Comput Methods Programs Biomed. 2014;117(3):482–488. doi:10.1016/j.cmpb.2014.09.003
18. Thibault G, Tudorica A, Afzal A, et al. DCE-MRI texture features for early prediction of breast cancer therapy response. Tomography. 2017;3(1):23–32. doi:10.18383/j.tom.2016.00241
19. Lee KC, Moffat BA, Schott AF, et al. Prospective early response imaging biomarker for neoadjuvant breast cancer chemotherapy. Clin Cancer Res. 2007;13(2):443–450. doi:10.1158/1078-0432.CCR-06-1888
20. Galban CJ, Ma B, Malyarenko D, et al. Multi-site clinical evaluation of DW-MRI as a treatment response metric for breast cancer patients undergoing neoadjuvant chemotherapy. PLoS One. 2015;10(3):e0122151. doi:10.1093/jnci/djw192
21. Zhang Z, Zhang W, Jin Y, et al. Evaluating the response of neoadjuvant chemotherapy for treatment of breast cancer: are tumor biomarkers and dynamic contrast enhanced MR images useful predictive tools? J Thorac Dis. 2014;6(6):785–794. doi:10.3978/j.issn.2072-1439.2014.04.28
22. Newitt DC, Zhang Z, Gibbs JE, et al. Test-retest repeatability and reproducibility of ADC measures by breast DWI: results from the ACRIN 6698 trial. J Magn Reson Imaging. 2019;49(6):1617–1628. doi:10.1002/jmri.26539
23. Pickles MD, Gibbs P, Lowry M, et al. Diffusion changes precede size reduction in neoadjuvant treatment of breast cancer. Magn Reson Imaging. 2006;24(7):843–847. doi:10.1016/j.mri.2005.11.005
24. Humbert O, Riedinger JM, Vrigneaud JM, et al. 18F-FDG PET-derived tumor blood flow changes after 1 cycle of neoadjuvant chemotherapy predicts outcome in triple-negative breast cancer. J Nucl Med. 2016;57(11):1707–1712. doi:10.1158/1078-0432.CCR-06-1888
25. Connolly RM, Leal JP, Goetz MP, et al. TBCRC 008: early change in 18F-FDG uptake on PET predicts response to preoperative systemic therapy in human epidermal growth factor receptor 2-negative primary operable breast cancer. J Nucl Med. 2015;56(1):31–37. doi:10.1200/JCO.2007.14.4147
26. Chen JH, Bahri S, Mehta RS, et al. Breast cancer: evaluation of response to neoadjuvant chemotherapy with 3.0-T MR imaging. Radiology. 2011;261(3):735–743. doi:10.1148/radiol.11110814
27. Kuzucan A, Chen JH, Bahri S, et al. Diagnostic performance of magnetic resonance imaging for assessing tumor response in patients with HER2-negative breast cancer receiving neoadjuvant chemotherapy is associated with molecular biomarker profile. Clin Breast Cancer. 2012;12(2):110–118. doi:10.1371/journal.pone.0122151
28. Oh SJ, Chae EY, Cha JH, et al. Relationship between background parenchymal enhancement on breast MRI and pathological tumor response in breast cancer patients receiving neoadjuvant chemotherapy. Br J Radiol. 2018;91(1088):20170550. doi:10.1002/jmri.26539
29. O’Sullivan TD, Leproux A, Chen JH, et al. Optical imaging correlates with magnetic resonance imaging breast density and reveals composition changes during neoadjuvant chemotherapy. Breast Cancer Res. 2013;15(1):R14. doi:10.2967/jnumed.114.144741
30. Krikken E, Khlebnikov V, Zaiss M, et al. Amide chemical exchange saturation transfer at 7 T: a possible biomarker for detecting early response to neoadjuvant chemotherapy in breast cancer patients. Breast Cancer Res. 2018;20(1):51. doi:10.1186/s13058-018-0982-2
31. Jafri NF, Newitt DC, Kornak J, et al. Optimized breast MRI functional tumor volume as a biomarker of recurrence-free survival following neoadjuvant chemotherapy. J Magn Reson Imaging. 2014;40(2):476–482. doi:10.1186/s13058-018-0982-2
32. Ozerov IV, Lezhnina KV, Izumchenko E, et al. In silico Pathway Activation Network Decomposition Analysis (iPANDA) as a method for biomarker development. Nat Commun. 2016;7(1):13427. doi:10.1038/ncomms13427
33. Nolen BM, Marks JR, Ta’san S, et al. Serum biomarker profiles and response to neoadjuvant chemotherapy for locally advanced breast cancer. Breast Cancer Res. 2008;10(3):R45. doi:10.1186/bcr2096
34. Ali AM, Ueno T, Tanaka S, et al. Determining circulating endothelial cells using cellsearch system during preoperative systemic chemotherapy in breast cancer patients. Eur J Cancer. 2011;47(15):2265–2272. doi:10.1016/j.ejca.2011.06.015
35. Arnold T, Michlmayr A, Baumann S, et al. Plasma HMGB-1 after the initial dose of epirubicin/docetaxel in cancer. Eur J Clin Invest. 2013;43(3):286–291. doi:10.1111/eci.12043
36. Wachter DL, Fasching PA, Haeberle L, et al. Prognostic molecular markers and neoadjuvant therapy response in anthracycline-treated breast cancer patients. Arch Gynecol Obstet. 2013;287(2):337–344. doi:10.1007/s00404-012-2534-9
37. Bhargava R, Beriwal S, McManus K, et al. Insulin-like growth factor receptor-1 (IGF-1R) expression in normal breast, proliferative breast lesions, and breast carcinoma. Appl Immunohistochem Mol Morphol. 2011;19(3):218–225. doi:10.1097/PAI.0b013e3181ffc58c
38. Petrarca CR, Brunetto AT, Duval V, et al. Survivin as a predictive biomarker of complete pathologic response to neoadjuvant chemotherapy in patients with stage II and stage III breast cancer. Clin Breast Cancer. 2011;11(2):129–134. doi:10.1016/j.clbc.2011.03.002
39. Moore LM, Wilkinson R, Altan M, et al. An assessment of neuronal calcium sensor-1 and response to neoadjuvant chemotherapy in breast cancer patients. NPJ Breast Cancer. 2018;4(1):6. doi:10.1038/s41523-018-0057-7
40. Dong MJ, Wang LB, Jiang ZN, et al. The transcription factor KLF4 as an independent predictive marker for pathologic complete remission in breast cancer neoadjuvant chemotherapy: a case-control study. Oncol Targets Ther. 2014;7:1963–1969. doi:10.2147/OTT.S68340
41. Collie-Duguid ES, Sweeney K, Stewart KN, et al. SerpinB3, a new prognostic tool in breast cancer patients treated with neoadjuvant chemotherapy. Breast Cancer Res Treat. 2012;132(3):807–818. doi:10.1007/s10549-011-1625-9
42. Exner R, Sachet M, Arnold T, et al. Prognostic value of HMGB1 in early breast cancer patients under neoadjuvant chemotherapy. Cancer Med. 2016;5(9):2350–2358. doi:10.1002/cam4.827
43. Zurgil U, Ben-Ari A, Rotem-Dai N, et al. PKCη is an anti-apoptotic kinase that predicts poor prognosis in breast and lung cancer. Biochem Soc Trans. 2014;42(6):1519–1523. doi:10.1042/BST20140182
44. Anborgh PH, Caria LB, Chambers AF, et al. Role of plasma osteopontin as a biomarker in locally advanced breast cancer. Am J Transl Res. 2015;7(4):723–732.
45. Zhao YC, Wang Y, Ni XJ, et al. Clinical significance of Smac and survivin expression in breast cancer patients treated with anthracycline-based neoadjuvant chemotherapy. Mol Med Rep. 2014;9(2):614–620. doi:10.3892/mmr.2013.1842
46. Kim H, Youk J, Yang Y, et al. Prognostic implication of serum hepatocyte growth factor in stage II/III breast cancer patients who received neoadjuvant chemotherapy. J Cancer Res Clin Oncol. 2016;142(3):707–714. doi:10.1007/s00432-015-2072-5
47. Wei S, Liu L, Zhang J, et al. Metabolomics approach for predicting response to neoadjuvant chemotherapy for breast cancer. Mol Oncol. 2013;7(3):297–307. doi:10.1002/cam4.827
48. Lindner JL, Loibl S, Denkert C, et al. Expression of secreted protein acidic and rich in cysteine (SPARC) in breast cancer and response to neoadjuvant chemotherapy. Ann Oncol. 2015;26(1):95–100. doi:10.1093/annonc/mdu487
49. Ohashi R, Sangen M, Namimatsu S, et al. Prognostic value of IMP3 expression as a determinant of chemosensitivity in triple-negative breast cancer. Pathol Res Pract. 2017;213(9):1160–1165. doi:10.1016/j.prp.2017.07.002
50. Singel SM, Cornelius C, Zaganjor E, et al. KIF14 promotes AKT phosphorylation and contributes to chemoresistance in triple-negative breast cancer. Neoplasia. 2014;16(3):247–56, 56 e2. doi:10.1016/j.neo.2014.03.008
51. Wang RX, Chen S, Huang L, et al. Predictive and prognostic value of Matrix metalloproteinase (MMP) - 9 in neoadjuvant chemotherapy for triple-negative breast cancer patients. BMC Cancer. 2018;18(1):909. doi:10.1186/s12885-018-4822-7
52. Wang RX, Chen S, Huang L, et al. Monitoring serum VEGF in neoadjuvant chemotherapy for patients with triple-negative breast cancer: a new strategy for early prediction of treatment response and patient survival. Oncologist. 2018. doi:10.1634/theoncologist.2017-0602
53. Ambros V. The functions of animal microRNAs. Nature. 2004;431(7006):350–355. doi:10.1038/nature02871
54. Parissenti AM, Guo B, Pritzker LB, et al. Tumor RNA disruption predicts survival benefit from breast cancer chemotherapy. Breast Cancer Res Treat. 2015;153(1):135–144. doi:10.1007/s10549-015-3498-9
55. Toomey S, Eustace AJ, Pritzker LB, et al. RE: RNA disruption assay as a biomarker of pathological complete response in neoadjuvant trastuzumab-treated human epidermal growth factor receptor 2-positive breast cancer. J Natl Cancer Inst. 2016;108(8):djw111. doi:10.1093/jnci/djw111
56. Chen X, Lu P, Wang DD, et al. The role of miRNAs in drug resistance and prognosis of breast cancer formalin-fixed paraffin-embedded tissues. Gene. 2016;595(2):221–226. doi:10.1016/j.gene.2016.10.015
57. Zhao R, Wu J, Jia W, et al. Plasma miR-221 as a predictive biomarker for chemoresistance in breast cancer patients who previously received neoadjuvant chemotherapy. Onkologie. 2011;34(12):675–680. doi:10.1159/000334552
58. Chernyy V, Pustylnyak V, Kozlov V, et al. Increased expression of miR-155 and miR-222 is associated with lymph node positive status. J Cancer. 2018;9(1):135–140. doi:10.7150/jca.22181
59. Yadav P, Mirza M, Nandi K, et al. Serum microRNA-21 expression as a prognostic and therapeutic biomarker for breast cancer patients. Tumour Biol. 2016;37(11):15275–15282. doi:10.1007/s13277-016-5361-y
60. Garcia-Garcia F, Salinas-Vera YM, Garcia-Vazquez R, et al. miR1455p is associated with pathological complete response to neoadjuvant chemotherapy and impairs cell proliferation by targeting TGFbetaR2 in breast cancer. Oncol Rep. 2019;41(6):3527–3534. doi:10.3892/or.2019.7102
61. Chen YH, Hancock BA, Solzak JP, et al. Next-generation sequencing of circulating tumor DNA to predict recurrence in triple-negative breast cancer patients with residual disease after neoadjuvant chemotherapy. NPJ Breast Cancer. 2017;3(1):24. doi:10.1038/s41523-017-0028-4
62. Gandini S, Guerrieri-Gonzaga A, Pruneri G, et al. Association of molecular subtypes with Ki-67 changes in untreated breast cancer patients undergoing pre-surgical trials. Ann Oncol. 2014;25(3):618–623. doi:10.1093/annonc/mdt528
63. Denkert C, Loibl S, Muller BM, et al. Ki67 levels as predictive and prognostic parameters in pretherapeutic breast cancer core biopsies: a translational investigation in the neoadjuvant GeparTrio trial. Ann Oncol. 2013;24(11):2786–2793. doi:10.1093/annonc/mdt350
64. Denkert C, Budczies J, von Minckwitz G, et al. Strategies for developing Ki67 as a useful biomarker in breast cancer. Breast. 2015;24(Suppl 2):S67–72. doi:10.1016/j.breast.2015.07.017
65. Prihantono P, Hatta M, Binekada C, et al. Ki-67 expression by immunohistochemistry and quantitative real-time polymerase chain reaction as predictor of clinical response to neoadjuvant chemotherapy in locally advanced breast cancer. J Oncol. 2017;2017:6209849. doi:10.1155/2017/6209849
66. Dawood S, Gonzalez-Angulo AM. Biomarker discordance pre and post neoadjuvant chemotherapy in breast cancer. Cancer Biomark. 2012;12(6):241–250. doi:10.3233/CBM-130315
67. Kanjer K, Tatic S, Neskovic-Konstantinovic Z, et al. Treatment response to preoperative anthracycline-based chemotherapy in locally advanced breast cancer: the relevance of proliferation and apoptosis rates. Pathol Oncol Res. 2013;19(3):577–588. doi:10.1007/s12253-013-9621-5
68. Enomoto Y, Morimoto T, Nishimukai A, et al. Impact of biomarker changes during neoadjuvant chemotherapy for clinical response in patients with residual breast cancers. Int J Clin Oncol. 2016;21(2):254–261. doi:10.1007/s10147-015-0897-1
69. Ohno S, Chow LW, Sato N, et al. Randomized trial of preoperative docetaxel with or without capecitabine after 4 cycles of 5-fluorouracil- epirubicin-cyclophosphamide (FEC) in early-stage breast cancer: exploratory analyses identify Ki67 as a predictive biomarker for response to neoadjuvant chemotherapy. Breast Cancer Res Treat. 2013;142(1):69–80. doi:10.1007/s10549-013-2691-y
70. Wu YT, Li X, Lu LJ, et al. Effect of neoadjuvant chemotherapy on the expression of hormone receptors and Ki-67 in Chinese breast cancer patients: a retrospective study of 525 patients. J Biomed Res. 2017. doi:10.7555/JBR.32.20170059
71. Toi M, Masuda N, Ishiguro H, et al. Development of breast cancer therapy: biomarker-driven and response-guided approaches in a neoadjuvant setting. Int J Biol Markers. 2015;30(2):e252–3. doi:10.5301/jbm.5000136
72. Xu L, Che X, Wu Y, et al. SIRT5 as a biomarker for response to anthracycline-taxane-based neoadjuvant chemotherapy in triple-negative breast cancer. Oncol Rep. 2018;39(5):2315–2323. doi:10.3892/or.2018.6319
73. Abdel-Fatah TMA, Agarwal D, Liu DX, et al. SPAG5 as a prognostic biomarker and chemotherapy sensitivity predictor in breast cancer: a retrospective, integrated genomic, transcriptomic, and protein analysis. Lancet Oncol. 2016;17(7):1004–1018. doi:10.1016/S1470-2045(16)00174-1
74. Balko JM, Schwarz LJ, Luo N, et al. Triple-negative breast cancers with amplification of JAK2 at the 9p24 locus demonstrate JAK2-specific dependence. Sci Transl Med. 2016;8(334):334ra53. doi:10.1126/scitranslmed.aad3001
75. Barba M, Vici P, Pizzuti L, et al. Body mass index modifies the relationship between γ-H2AX, a DNA damage biomarker, and pathological complete response in triple-negative breast cancer. BMC Cancer. 2017;17(1):101. doi:10.1186/s12885-016-3045-z
76. Bardia A, Parton M, Kummel S, et al. Paclitaxel with inhibitor of apoptosis antagonist, LCL161, for localized triple-negative breast cancer, prospectively stratified by gene signature in a biomarker-driven neoadjuvant trial. J Clin Oncol. 2018:JCO2017748392. doi:10.1200/JCO.2017.74.8392.
77. Birkbak NJ, Li Y, Pathania S, et al. Overexpression of BLM promotes DNA damage and increased sensitivity to platinum salts in triple-negative breast and serous ovarian cancers. Ann Oncol. 2018;29(4):903–909. doi:10.1093/annonc/mdy049
78. Chen X, Xu D, Li X, et al. Latest overview of the cyclin-dependent kinases 4/6 inhibitors in breast cancer: the past, the present and the future. J Cancer. 2019;10(26):6608–6617. doi:10.7150/jca.33079
79. Kim SJ, Nakayama S, Shimazu K, et al. Recurrence risk score based on the specific activity of CDK1 and CDK2 predicts response to neoadjuvant paclitaxel followed by 5-fluorouracil, epirubicin and cyclophosphamide in breast cancers. Ann Oncol. 2012;23(4):891–897. doi:10.1093/annonc/mdr340
80. Schlafstein AJ, Withers AE, Rudra S, et al. CDK9 expression shows role as a potential prognostic biomarker in breast cancer patients who fail to achieve pathologic complete response after neoadjuvant chemotherapy. Int J Breast Cancer. 2018;2018:6945129. doi:10.1155/2018/6945129
81. Jarzab M, Kowal M, Bal W, et al. Ratio of proliferation markers and HSP90 gene expression as a predictor of pathological complete response in breast cancer neoadjuvant chemotherapy. Folia Histochem Cytobiol. 2016;54(4):202–209. doi:10.5603/FHC.a2016.0026
82. Grim J, Jandik P, Slanska I, et al. Low expression of NQO1 predicts pathological complete response to neoadjuvant chemotherapy in breast cancer patients treated with TAC regimen. Folia Biologica. 2012;58(5):185–192.
83. Michlmayr A, Bachleitner-Hofmann T, Baumann S, et al. Modulation of plasma complement by the initial dose of epirubicin/docetaxel therapy in breast cancer and its predictive value. Br J Cancer. 2010;103(8):1201–1208. doi:10.1038/sj.bjc.6605909
84. Hyung SW, Lee MY, Yu JH, et al. A serum protein profile predictive of the resistance to neoadjuvant chemotherapy in advanced breast cancers. Mol Cell Proteomics. 2011;10(10):M111 011023. doi:10.1074/mcp.M111.011023
85. Wan F, Dong L, Zhang F, et al. Clinical study of the relationship between γ-synuclein and the response of neoadjuvant chemotherapy in breast cancer. J Int Med Res. 2013;41(3):743–753. doi:10.1177/0300060513484434
86. Wang Y, Sparano JA, Fineberg S, et al. High expression of class III beta-tubulin predicts good response to neoadjuvant taxane and doxorubicin/cyclophosphamide-based chemotherapy in estrogen receptor-negative breast cancer. Clin Breast Cancer. 2013;13(2):103–108. doi:10.3892/or.2019.7102
87. Yu G, Liu G, Dong J, et al. Clinical implications of CIP2A protein expression in breast cancer. Med Oncol. 2013;30(2):524. doi:10.1007/s12032-013-0524-9
88. Xu C, Wei Q, Guo J, et al. FOXA1 expression significantly predict response to chemotherapy in estrogen receptor-positive breast cancer patients. Ann Surg Oncol. 2015;22(6):2034–2039. doi:10.1245/s10434-014-4313-2
89. Jhaveri K, Teplinsky E, Silvera D, et al. Hyperactivated mTOR and JAK2/STAT3 pathways: molecular drivers and potential therapeutic targets of inflammatory and invasive ductal breast cancers after neoadjuvant chemotherapy. Clin Breast Cancer. 2016;16(2):113–22e1. doi:10.1007/s10549-013-2691-y
90. Tanaka S, Ueno T, Ishiguro H, et al. The lack of increases in circulating endothelial progenitor cell as a negative predictor for pathological response to neoadjuvant chemotherapy in breast cancer patients. NPJ Precis Oncol. 2017;1(1):6. doi:10.1038/s41698-017-0006-1
91. Qian Y, Tao J, Li X, et al. Peripheral inflammation/immune indicators of chemosensitivity and prognosis in breast cancer patients treated with neoadjuvant chemotherapy. Onco Targets Ther. 2018;11:1423–1432. doi:10.2147/OTT.S148496
92. Issa-Nummer Y, Loibl S, von Minckwitz G, et al. Tumor-infiltrating lymphocytes in breast cancer: a new predictor for responses to therapy. Oncoimmunology. 2014;3(3):e27926. doi:10.4161/onci.27926
93. Melichar B, Studentova H, Kalabova H, et al. Predictive and prognostic significance of tumor-infiltrating lymphocytes in patients with breast cancer treated with neoadjuvant systemic therapy. Anticancer Res. 2014;34(3):1115–1125.
94. Asano Y, Kashiwagi S, Goto W, et al. Prediction of treatment response to neoadjuvant chemotherapy in breast cancer by subtype using tumor-infiltrating lymphocytes. Anticancer Res. 2018;38(4):2311–2321. doi:10.1007/s12032-013-0524-9
95. Ahn SG, Jeong J, Hong S, et al. Current issues and clinical evidence in tumor-infiltrating lymphocytes in breast cancer. J Pathol Transl Med. 2015;49(5):355–363. doi:10.4132/jptm.2015.07.29
96. Siregar KB, Pane J, Siburian R. Correlation between tumor-infiltrating lymphocytes and pathological response in locally advanced breast cancer patients who received neoadjuvant chemotherapy in H. Adam Malik General Hospital. Case Rep Oncol. 2017;10(2):699–705. doi:10.1159/000477799
97. West NR, Milne K, Truong PT, et al. Tumor-infiltrating lymphocytes predict response to anthracycline-based chemotherapy in estrogen receptor-negative breast cancer. Breast Cancer Res. 2011;13(6):R126. doi:10.1186/bcr3072
98. Hornychova H, Melichar B, Tomsova M, et al. Tumor-infiltrating lymphocytes predict response to neoadjuvant chemotherapy in patients with breast carcinoma. Cancer Invest. 2008;26(10):1024–1031. doi:10.1080/07357900802098165
99. O’Loughlin M, Andreu X, Bianchi S, et al. Reproducibility and predictive value of scoring stromal tumour infiltrating lymphocytes in triple-negative breast cancer: a multi-institutional study. Breast Cancer Res Treat. 2018;171(1):1–9. doi:10.1007/s10549-018-4825-8
100. Yang X, Rao J, Yang W, et al. Evaluation of the predictive and prognostic values of stromal tumor-infiltrating lymphocytes in HER2-positive breast cancers treated with neoadjuvant chemotherapy. Target Oncol. 2018;13(6):757–767. doi:10.1007/s11523-018-0602-1
101. Loi S, Sirtaine N, Piette F, et al. Prognostic and predictive value of tumor-infiltrating lymphocytes in a Phase III randomized adjuvant breast cancer trial in node-positive breast cancer comparing the addition of docetaxel to doxorubicin with doxorubicin-based chemotherapy: BIG 02-98. J Clin Oncol. 2013;31(7):860–867. doi:10.1200/JCO.2011.41.0902
102. Li XB, Krishnamurti U, Bhattarai S, et al. Biomarkers predicting pathologic complete response to neoadjuvant chemotherapy in breast cancer. Am J Clin Pathol. 2016;145(6):871–878. doi:10.1093/ajcp/aqw045
103. Cimino-Mathews A, Ye X, Meeker A, et al. Metastatic triple-negative breast cancers at first relapse have fewer tumor-infiltrating lymphocytes than their matched primary breast tumors: a pilot study. Hum Pathol. 2013;44(10):2055–2063. doi:10.1016/j.humpath.2013.03.010
104. Mahmoud SM, Paish EC, Powe DG, et al. Tumor-infiltrating CD8+ lymphocytes predict clinical outcome in breast cancer. J Clin Oncol. 2011;29(15):1949–1955. doi:10.1200/JCO.2010.30.5037
105. Asano Y, Kashiwagi S, Goto W, et al. Tumour-infiltrating CD8 to FOXP3 lymphocyte ratio in predicting treatment responses to neoadjuvant chemotherapy of aggressive breast cancer. Br J Surg. 2016;103(7):845–854. doi:10.1002/bjs.10127
106. Goto W, Kashiwagi S, Asano Y, et al. Predictive value of improvement in the immune tumour microenvironment in patients with breast cancer treated with neoadjuvant chemotherapy. ESMO Open. 2018;3(6):e000305. doi:10.1136/esmoopen-2017-000305
107. Matikas A, Lovrot J, Ramberg A, et al. Dynamic evaluation of the immune infiltrate and immune function genes as predictive markers for neoadjuvant chemotherapy in hormone receptor positive, HER2 negative breast cancer. Oncoimmunology. 2018;7(9):e1466017. doi:10.1080/2162402X.2018.1466017
108. Ma C, Zhang Q, Ye J, et al. Tumor-infiltrating gammadelta T lymphocytes predict clinical outcome in human breast cancer. The Journal of Immunology. 2012;189(10):5029–5036. doi:10.4049/jimmunol.1201892
109. Muenst S, Soysal SD, Gao F, et al. The presence of programmed death 1 (PD-1)-positive tumor-infiltrating lymphocytes is associated with poor prognosis in human breast cancer. Breast Cancer Res Treat. 2013;139(3):667–676. doi:10.1007/s10549-013-2581-3
110. Ingold Heppner B, Untch M, Denkert C, et al. Tumor-infiltrating lymphocytes: a predictive and prognostic biomarker in neoadjuvant-treated HER2-positive breast cancer. Clin Cancer Res. 2016;22(23):5747–5754. doi:10.1158/1078-0432.CCR-15-2338
111. Herrero-Vicent C, Guerrero A, Gavila J, et al. Predictive and prognostic impact of tumour-infiltrating lymphocytes in triple-negative breast cancer treated with neoadjuvant chemotherapy. Ecancermedicalscience. 2017;11:759. doi:10.3332/ecancer.2017.759
112. Bense RD, Sotiriou C, Piccart-Gebhart MJ, et al. Relevance of tumor-infiltrating immune cell composition and functionality for disease outcome in breast cancer. J Natl Cancer Inst. 2017;109(1):djw192. doi:10.1093/jnci/djw192
113. Gabani P, Weiner AA, Hernandez-Aya LF, et al. Treatment response as predictor for brain metastasis in triple negative breast cancer: a score-based model. Breast J. 2019;25(3):363–372. doi:10.1111/tbj.13230
114. Lim GH, Teo SY, Allen JC, et al. Determining whether high nodal burden in early breast cancer patients can be predicted preoperatively to avoid sentinel lymph node biopsy. J Breast Cancer. 2019;22(1):67–76. doi:10.4048/jbc.2019.22.e8
115. Liao GJ, Henze Bancroft LC, Strigel RM, et al. Background parenchymal enhancement on breast MRI: a comprehensive review. J Magn Reson Imaging. 2019. doi:10.1002/jmri.26762
116. Antunovic L, De Sanctis R, Cozzi L, et al. PET/CT radiomics in breast cancer: promising tool for prediction of pathological response to neoadjuvant chemotherapy. Eur J Nucl Med Mol Imaging. 2019;46(7):1468–1477. doi:10.1007/s00259-019-04313-8
117. Azizi E, Carr AJ, Plitas G, et al. Single-cell map of diverse immune phenotypes in the breast tumor microenvironment. Cell. 2018;174(5):1293–308 e36. doi:10.1016/j.cell.2018.05.060
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.