Back to Journals » Journal of Inflammation Research » Volume 19
Predictive Value of Uric Acid-to-Albumin Ratio for Left Atrial Thrombus or Spontaneous Echo Contrast in Patients with Non-Valvular Atrial Fibrillation
Authors Meng X ![]() , Wen Y, Wang X, Hidru TH, Tang Y, Xia Y, Yang X, Gao L
, Wen Y, Wang X, Hidru TH, Tang Y, Xia Y, Yang X, Gao L
Received 11 March 2026
Accepted for publication 23 April 2026
Published 13 May 2026 Volume 2026:19 608168
DOI https://doi.org/10.2147/JIR.S608168
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Qing Lin
Xiangzhu Meng,1,* Yuhang Wen,1,* Xiangying Wang,2,* Tesfaldet Habtemariam Hidru,1 Yuqi Tang,1 Yunlong Xia,1 Xiaolei Yang,1 Lianjun Gao1
1Department of Cardiology, Institute of Cardiovascular Diseases, The First Affiliated Hospital of Dalian Medical University, Dalian, Liaoning, People’s Republic of China; 2Department of Rehabilitation, Jiangxi Province Hospital of Integrated Chinese and Western Medicine, Nanchang, Jiangxi, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Xiaolei Yang; Lianjun Gao, Email [email protected]; [email protected]
Background: The uric acid-to-albumin ratio (UAR) is a novel inflammatory marker linked to cardiovascular disease. This study aimed to evaluate the predictive value of UAR for left atrial thrombus or spontaneous echo contrast (LAT/SEC) in non-valvular atrial fibrillation (NVAF), explore its mediating mechanisms, and assess the incremental value beyond the CHA2DS2-VASc score.
Methods: This retrospective study included 514 patients with NVAF undergoing transesophageal echocardiography (TEE). Multivariable logistic regression, restricted cubic splines (RCS), generalized additive models (GAMs), receiver operating characteristic (ROC) curves, and mediation analyses were employed to evaluate the relationship between UAR and LAT/SEC. Reclassification indices assessed UAR’s incremental value beyond the CHA2DS2-VASc score.
Results: The prevalence of LAT/SEC was 17.32%. UAR was independently associated with LAT/SEC (OR: 1.43, 95% CI: 1.25– 1.66; P < 0.001) in a nonlinear manner (P for non-linearity = 0.031). A threshold effect was identified at 12.11, below which the risk increased more significantly (OR: 1.61, 95% CI: 1.36– 1.92; P < 0.001). UAR showed better predictive performance (AUC=0.712) than UA (0.684) and albumin (0.612). Incorporating UAR into the CHA2DS2-VASc model improved risk stratification. Mediation analysis indicated that left atrial diameter (LAD) and left ventricular ejection fraction (LVEF) accounted for 8.26% and 9.75% of the association, respectively.
Conclusion: UAR is an independent predictor of LAT/SEC in patients with NVAF, outperforming its individual components and providing significant incremental value beyond the CHA2DS2-VASc score. It may serve as a readily accessible biomarker for optimizing risk stratification and clinical anticoagulation decisions. Image A is an infographic with three sections: Study Population, Exposure and Outcome, linked by arrows. Study Population features a heart icon, ECG trace and five person icons, indicating 514 NVAF cases from 2019.1 to 2022.6. Exposure shows an arm with a blood draw and a marker icon, labeled UAR (uric acid/albumin). Outcome displays a heart icon, ECG trace and five person icons, noting 89 LAT/SEC cases in NVAF patients during admission. Image B is a dose-response graph with UAR on the X-axis and Odds ratio (95% CI) on the Y-axis. The curve rises with UAR and the 95% CI band widens at higher UAR. Text indicates P for overall < 0.001 and P for nonlinear = 0.031. Image C is a decision curve analysis graph with High Risk Threshold on the X-axis and Net Benefit on the Y-axis. The legend includes UAR + CHA2DS2-VASc, CHA2DS2-VASc, All and None. The UAR + CHA2DS2-VASc curve is generally above the CHA2DS2-VASc curve, both nearing zero at higher thresholds.A three-part infographic on NVAF: UAR exposure, LAT/SEC outcome and odds and decision-curve graphs.
Keywords: uric acid-to-albumin ratio, atrial fibrillation, left atrial thrombus, spontaneous echo contrast
Introduction
Atrial fibrillation (AF) is one of the most common clinical arrhythmias, with an increasing incidence partly due to population aging.1 AF is associated with a 5-fold higher stroke risk, resulting in significant morbidity and mortality and imposing a heavy burden on public health.2 Approximately 90% of left atrial (LA) thrombi originate in the left atrial appendage (LAA), the primary thrombotic site in non-valvular atrial fibrillation (NVAF).3 Spontaneous echo contrast (SEC), a thrombotic precursor indicating blood stasis, is crucial for guiding anticoagulation.4 While the CHA2DS2-VASc score facilitates stroke risk stratification, transesophageal echocardiography (TEE) remains indispensable for the direct identification of LA thrombi prior to catheter ablation or cardioversion. Given that this invasive procedure carries potential risks such as esophageal injury, there is a clinical demand for safer, non-invasive biomarkers to predict left atrial thrombus/spontaneous echo contrast (LAT/SEC) and guide early anticoagulation for stroke prevention.
Although the underlying mechanisms of AF remain incompletely understood, inflammation and oxidative stress are known to play important roles in its initiation and maintenance.5 Emerging evidence further emphasizes the critical link between systemic inflammation and thromboembolic risk in patients with AF.6 Proinflammatory cytokines (eg, IL-2, IL-6, CRP, and TNF-α) not only reflect systemic inflammatory burden but also actively promote atrial fibrosis, endothelial dysfunction, and platelet activation—all of which contribute to a prothrombotic milieu and thrombus formation in the LAA.7
Uric acid (UA), the end product of purine metabolism, promotes oxidative stress, endothelial dysfunction, and inflammatory responses when elevated, thereby inducing a prothrombotic state.8 Accumulating evidence supports a strong association between hyperuricemia and thrombosis in AF.9,10 Conversely, albumin, the most abundant plasma protein, exerts anti-inflammatory, antioxidant, and antithrombotic effects.11 Hypoalbuminemia reflects an exacerbated inflammatory status that inherently increases thrombotic risk.12 Notably, the interplay between elevated UA and reduced albumin constitutes a pivotal inflammatory-metabolic axis. We hypothesize that this synergistic imbalance creates a highly prothrombotic state, which predisposes patients to LAT/SEC.
Given that composite inflammatory indices based on circulating biomarkers often outperform individual parameters, the uric acid-to-albumin ratio (UAR) has emerged as a novel marker of inflammation and oxidative stress. As an inexpensive and readily available indicator derived from routine blood tests, UAR has shown growing predictive utility in cardiovascular diseases.13 However, whether this inflammatory-metabolic imbalance reflected by UAR is independently associated with LAT/SEC risk in NVAF patients remains unclear. Therefore, we aimed to evaluate the association between UAR and LAT/SEC, elucidate potential mediating pathways, and determine whether UAR offers incremental predictive utility beyond the established thromboembolic risk stratification model.
Materials and Methods
Study Design and Population
This single-center, retrospective cohort study was conducted at the First Affiliated Hospital of Dalian Medical University. We consecutively enrolled 514 hospitalized patients with NVAF who underwent TEE prior to catheter ablation or direct current cardioversion between January 2019 and June 2022. Exclusion criteria were as follows: (1) age < 18 years; (2) congenital or severe valvular heart disease; (3) moderate-to-severe hepatic or renal dysfunction; (4) malignancy, active infection, chronic inflammatory disease, or autoimmune disease; (5) prior left atrial appendage closure (LAAC); (6) gout, thyroid disorders, or use of medications affecting serum uric acid levels; (7) acute myocardial infarction or acute heart failure; and (8) missing essential baseline data. This study was approved by the Ethics Committee of the First Affiliated Hospital of Dalian Medical University (No. PJ-KS-KY-2026-122) and conducted in accordance with the Declaration of Helsinki. Written informed consent was obtained from all participants, and all data were anonymized to ensure confidentiality. This study was reported in accordance with the REporting of studies Conducted using Observational Routinely-collected health Data (RECORD) guidelines to ensure methodological rigor and transparency.14
Clinical Definitions
Two experienced echocardiographers, who were blinded to clinical data, independently evaluated the presence of LAT/SEC via TEE. Inter-observer reliability was assessed using Cohen’s kappa coefficient, which showed excellent agreement between the two specialists (κ = 0.902, 95% CI: 0.853–0.951; P < 0.001). Discrepancies were resolved by consensus or consultation with a third senior expert. LAT was defined as a well-demarcated echogenic mass distinct from adjacent myocardium and visible in multiple views.15 SEC was defined as swirling, smoke-like echogenic signals persisting under optimal gain.16 According to the Fatkin classification, SEC grades 3 and 4 were considered dense. The CHA2DS2-VASc score was calculated as follows: 1 point each for congestive heart failure, hypertension, female sex, age 65–74 years, diabetes mellitus, or vascular disease (comprising peripheral artery disease or myocardial infarction), and 2 points each for age ≥75 years or prior stroke/transient ischemic attack (TIA).1
Data Collection
Baseline clinical data extracted from electronic medical records included demographics (age, gender, smoking status, and alcohol consumption), and AF type. Comorbidities were defined as follows: hypertension (systolic blood pressure ≥140 mmHg and/or diastolic blood pressure ≥90 mmHg, a self-reported history of hypertension, or current antihypertensive medication use) and diabetes mellitus (use of hypoglycemic agents/insulin, fasting serum glucose ≥7.0 mmol/L, and/or random blood glucose ≥11.1 mmol/L). Echocardiographic parameters included: left atrial diameter (LAD), left ventricular ejection fraction (LVEF), left ventricular end-diastolic diameter (LVEDD), and E-wave deceleration time (EDT). Laboratory parameters comprised white blood cells (WBC), red blood cells (RBC), platelets (PLT), neutrophils, lymphocytes, monocytes, hemoglobin (Hb), D-dimer, albumin, creatinine, aspartate aminotransferase (AST), alanine aminotransferase (ALT), uric acid (UA), triglycerides (TG), total cholesterol (TC), low-density lipoprotein cholesterol (LDL-C), high-density lipoprotein cholesterol (HDL-C), and fasting plasma glucose (FPG). The UAR was calculated using the formula: UAR = uric acid (μmol/L) / albumin (g/L).
Statistical Analysis
Sample size was calculated using G*Power (Version 3.1.9.7) based on the Hsieh method for multivariable logistic regression.17 To detect a minimal clinically important effect, the expected odds ratio (OR) was set at 1.50 per standard deviation (SD) increase in UAR, assuming a standard normal distribution (mean=0, SD=1). While our previous cohort showed a 21.2% LAT/SEC incidence,18 we conservatively estimated a 15% baseline probability to account for reduced rates with widespread direct oral anticoagulant (DOAC) use and improved AF management. With an R2 of 0.15 for covariates, a two-tailed α = 0.05, and 80% power, a minimum of 445 participants was required. Statistical analyses were performed using IBM SPSS Statistics (Version 31.0), R (Version 4.5.2), and Zstats (Version 1.0; www.zstats.net). Patients were stratified into tertiles based on UAR levels. Continuous variables, assessed for normality using the Kolmogorov–Smirnov test, were expressed as mean ± SD or median (interquartile range [IQR]) and compared using one-way analysis of variance (ANOVA) or the Kruskal–Wallis test, respectively. Categorical variables were presented as counts (percentages) and analyzed using the chi-squared test. Variables with >10% missing data were excluded, while multiple imputation was applied to those with <10% missingness.
Multivariable logistic regression was performed to evaluate the associations of UAR (both as a continuous variable and in tertiles) with LAT/SEC, reporting odds ratios (ORs) and 95% confidence intervals (CIs). Potential risk factors identified in univariate analysis (Supplementary Table 1) and other clinically relevant variables were incorporated into the multivariable analysis. Variables with a variance inflation factor (VIF) < 5 and tolerance > 0.2 were retained, as they demonstrated no significant multicollinearity (Supplementary Table 2). Four sequentially adjusted models were constructed: Model 1 (unadjusted); Model 2 (adjusted for age, gender, body mass index [BMI], and smoking status); Model 3 (Model 2 covariates + hypertension, diabetes mellitus [DM], heart failure [HF], coronary heart disease [CHD], stroke/TIA, paroxysmal AF, anticoagulants, and antiplatelets); and Model 4 (Model 3 covariates + WBC, PLT, D-dimer, ALT, AST, creatinine, HDL-C, LDL-C, LAD, and LVEF).
Non-linear relationships between UAR and LAT/SEC risk were analyzed using restricted cubic splines (RCS) with 3 knots, smooth curve fitting, and generalized additive models (GAMs). Segmented regression was applied to identify potential threshold effects and inflection points. The predictive accuracy of UAR, UA, and albumin was assessed using receiver operating characteristic (ROC) curves and the area under the curve (AUC). The incremental predictive value of adding UAR to the CHA2DS2-VASc score was quantified using Harrell’s C-index, net reclassification improvement (NRI), and integrated discrimination improvement (IDI). A bootstrapped mediation analysis (with 1000 resamples) was performed to explore the mediating role of UAR between relevant clinical factors and LAT/SEC. Sensitivity analyses were conducted to assess the robustness of the findings. All tests were two-tailed, with P < 0.05 considered statistically significant.
Results
Baseline Characteristics of Participants
Of 815 initially screened patients with NVAF, 301 were excluded per predefined criteria (detailed in Supplementary Figure 1), yielding a final cohort of 514 participants. Patients were stratified into UAR tertiles: T1 (3.68–7.63), T2 (7.64–9.68), and T3 (9.69–16.51). As summarized in Table 1, the cohort was predominantly male (63.42%) and aged ≥ 60 years (72.18%). Compared with lower tertiles, patients in T3 had significantly higher rates of paroxysmal AF and alcohol consumption. Baseline comorbidities (hypertension, DM, CHD, HF, stroke/TIA) and medication use (antiplatelets, anticoagulants, statins, β-blockers) did not differ significantly across groups (all P > 0.05). Regarding laboratory findings, increasing UAR was associated with significantly elevated RBC, neutrophils, Hb, TG, creatinine, and UA, as well as reduced albumin and HDL-C. Echocardiographic assessment revealed progressive increases in LAD and LVEDD, accompanied by a corresponding decrease in LVEF from T1 to T3 (all P < 0.001). Notably, the prevalence of LAT/SEC increased markedly across UAR tertiles, from 6.98% in T1 to 29.24% in T3 (P < 0.001).
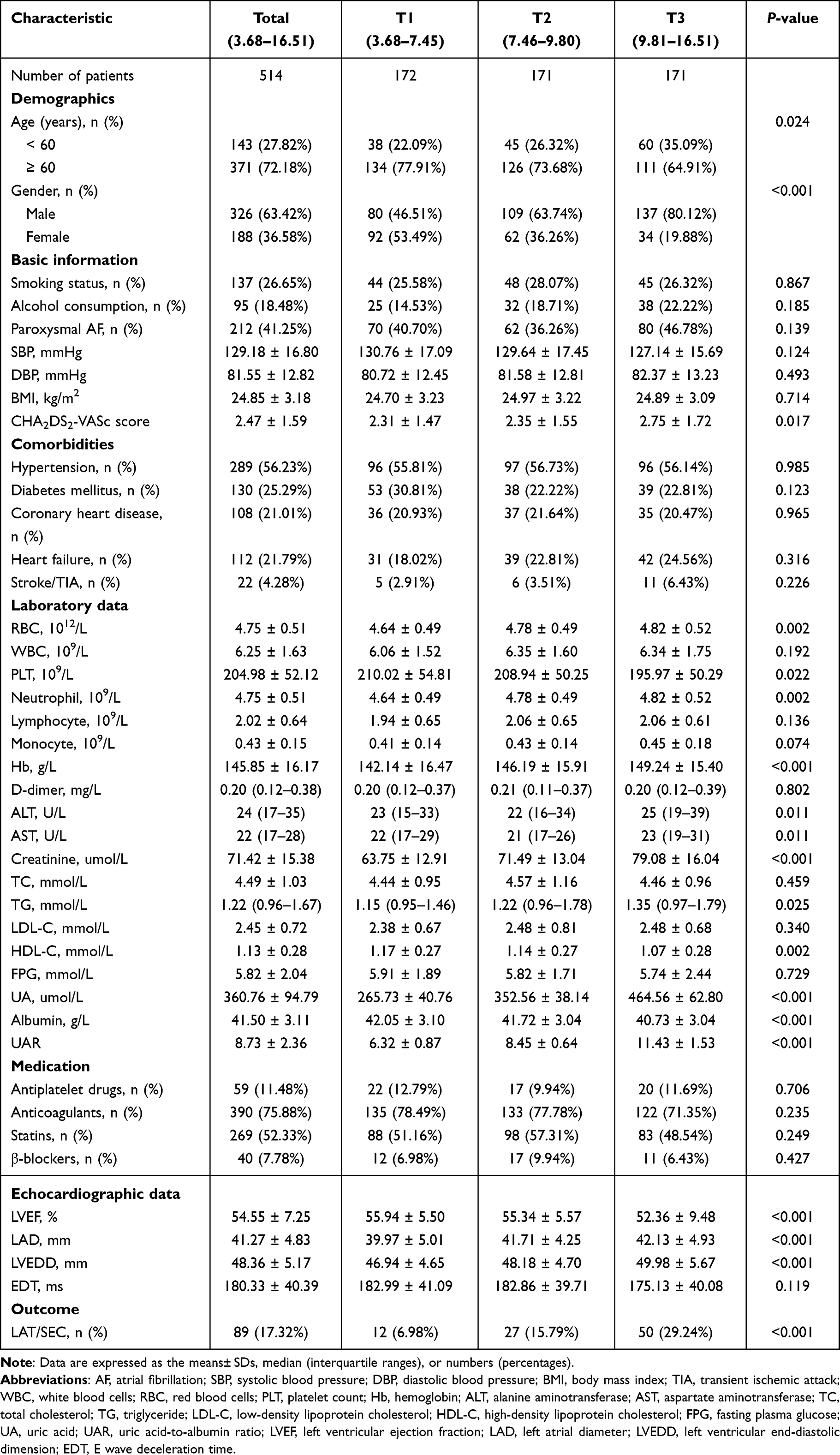 |
Table 1 Baseline Characteristics According to Tertiles of the UAR Levels |
Spearman Correlation Analysis
As shown in Supplementary Figure 2, Spearman correlation analysis revealed positive associations between UAR and WBC, neutrophils, and monocytes, consistent with its role as a marker of inflammation and oxidative stress. UAR also correlated positively with the CHA2DS2-VASc score; of note, multiple comorbidities incorporated into this score (eg, HF, hypertension, DM) are linked to chronic inflammation. Regarding cardiac metrics, UAR correlated negatively with LVEF and positively with LVEDD and LAD, suggesting that an inflammatory and oxidative milieu may contribute to adverse cardiac structural and functional remodeling. Additionally, its positive association with TG and inverse relationship with HDL-C suggest a potential link between systemic inflammation, oxidative stress, and lipid metabolism.
Link Between UAR and LAT/SEC
Patients with LAT/SEC had significantly higher UAR levels than those without (10.21 vs. 8.42; P < 0.001) (Figure 1A), and the density curve showed a rising proportion of LAT/SEC cases across increasing UAR tertiles (Figure 1B). Multivariable logistic regression (Table 2) confirmed UAR as a robust independent predictor of LAT/SEC. When analyzed as a continuous variable, each one-unit increase in UAR was associated with an increased risk of LAT/SEC in the unadjusted model (OR: 1.36, 95% CI: 1.23–1.50; P < 0.001) and the fully adjusted Model 4 (OR: 1.43, 95% CI: 1.25–1.66; P < 0.001). When stratified by tertiles, patients in T3 exhibited a substantially higher risk compared with those in T1 (unadjusted OR: 5.51, 95% CI: 2.90–11.30; fully adjusted OR: 7.04, 95% CI: 3.18–16.60; both P < 0.001). A significant dose-response relationship was observed across all models (P for trend < 0.001).
 |
Table 2 Logistic Regression Models for the Association Between UAR and LAT/SEC |
 |
Figure 1 Raincloud plot comparing the UAR between the LAT/SEC and the Non-LAT/SEC groups (A), and density curves of the UAR and LAT/SEC in NVAF patients (B). Abbreviations: UAR, uric acid-to-albumin ratio; LAT/SEC, left atrial thrombus or spontaneous echo contrast; NVAF, non-valvular atrial fibrillation. |
Non-Linear Relationship Between UAR and LAT/SEC
Adjusted RCS analysis revealed a significant overall association (P < 0.001) and a significant nonlinear relationship (P for non-linearity = 0.031; Figure 2A) between UAR and LAT/SEC, which was supported by smooth curve fitting and GAM analysis (Figure 2B). Segmented regression identified a clear inflection point at a UAR of 12.11 (Supplementary Table 3). Below this threshold, each unit increase in UAR was associated with a significantly higher risk of LAT/SEC (OR: 1.61, 95% CI: 1.36–1.92; P < 0.001). Conversely, above this threshold, the association lost statistical significance (OR: 0.82, 95% CI: 0.51–1.31; P = 0.398). A log-likelihood ratio test confirmed that the two-piecewise linear regression model provided a superior fit compared with the standard linear model (P = 0.015).
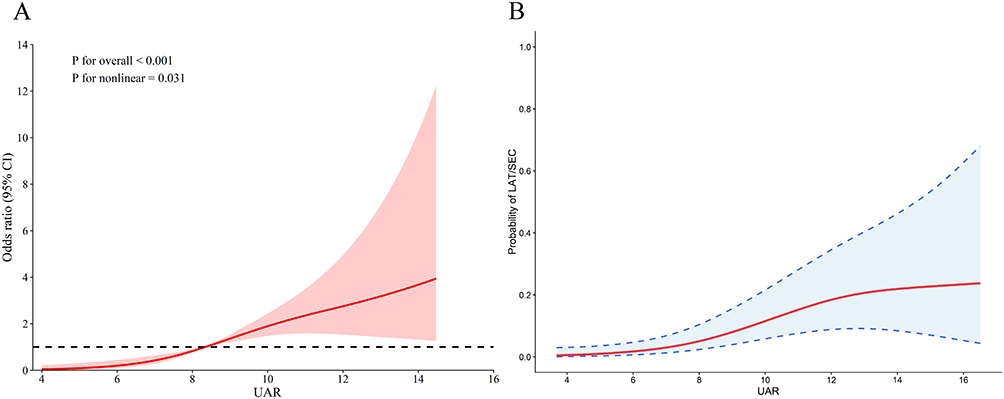 |
Figure 2 Non-linear relationship between UAR and LAT/SEC in NVAF patients. (A) The restricted cubic spline plot of UAR. (B) The smooth curve fitting diagram of UAR. Abbreviations: UAR, uric acid-to-albumin ratio; LAT/SEC, left atrial thrombus or spontaneous echo contrast; NVAF, non-valvular atrial fibrillation. |
Predictive Value Analysis
ROC analysis showed a significantly higher AUC for UAR than for UA (0.712 vs. 0.684, P < 0.001) and albumin (0.712 vs. 0.612, P = 0.002) (Figure 3A and Supplementary Table 4). At the optimal cutoff value of 8.59 (sensitivity: 74.2%; specificity: 61.2%), UAR substantially enhanced the predictive performance of the CHA2DS2-VASc score. Specifically, the addition of UAR increased its AUC from 0.708 to 0.766 (Figure 3B). These improvements were supported by significant risk reclassification and discrimination, with an NRI of 0.603 (95% CI: 0.371–0.846) and IDI of 0.058 (95% CI: 0.026–0.107) (both P < 0.01) (Supplementary Table 5). Calibration curves demonstrated good agreement between predicted and observed LAT/SEC risk upon adding UAR to the score (MAE = 0.006; Figure 4). Decision curve analysis (DCA) further confirmed that integrating UAR yielded superior clinical net benefit over the original score alone across a wide range of threshold probabilities (Figure 5).
 |
Figure 3 Receiver operating characteristic (ROC) analysis of each prediction model. (A): Comparison of UAR, UA, and Albumin in predicting LAT/SEC. (B): CHA2DS2- VASc and CHA2DS2-VASc + UAR to predict LAT/SEC in NVAF patients. Abbreviations: UA, uric acid; UAR, uric acid-to-albumin ratio; LAT/SEC, left atrial thrombus or spontaneous echo contrast; NVAF, non-valvular atrial fibrillation. |
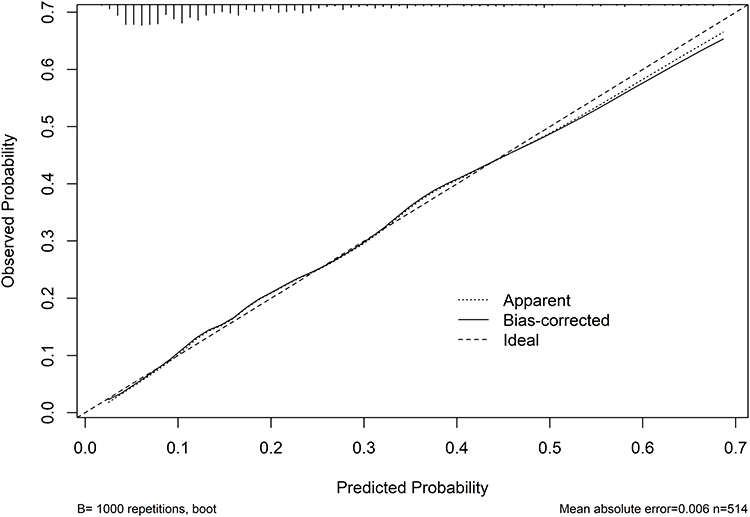 |
Figure 4 Calibration curve for the CHA2DS2-VASc + UAR to predict the LAT/SEC in patients with NVAF. Abbreviations: UAR, uric acid-to-albumin ratio; LAT/SEC, left atrial thrombus or spontaneous echo contrast; NVAF, non-valvular atrial fibrillation. |
 |
Figure 5 Decision curve analyses of the CHA2DS2-VASc and CHA2DS2-VASc + UAR for the incidence of LAT/SEC in NVAF patients. Abbreviations: UAR, uric acid-to-albumin ratio; LAT/SEC, left atrial thrombus or spontaneous echo contrast; NVAF, non-valvular atrial fibrillation. |
Subgroup and Sensitivity Analyses
Subgroup analyses by gender, age, BMI, smoking, comorbidities, and medication use showed no significant interactions with UAR (Supplementary Figure 3; all P for interaction > 0.05), indicating a consistent association between UAR and LAT/SEC across clinical subpopulations. Sensitivity analyses further corroborated the robustness of these findings (Table 3). The independent association between UAR and LAT/SEC remained significant after excluding patients with stroke/TIA, hypertension, DM, CHD, or HF in separate analyses (all P < 0.01). Furthermore, UAR maintained its predictive value in high-risk groups, including patients aged ≥ 50 years and those on anticoagulants. Notably, UAR was significantly associated with LAT/SEC regardless of CHA2DS2-VASc score (score ≥ 2: OR 1.42, 95% CI 1.21–1.68; score < 2: OR 1.60, 95% CI 1.08–2.56; both P < 0.05). Finally, the AUC did not differ significantly between the total population and these subgroups.
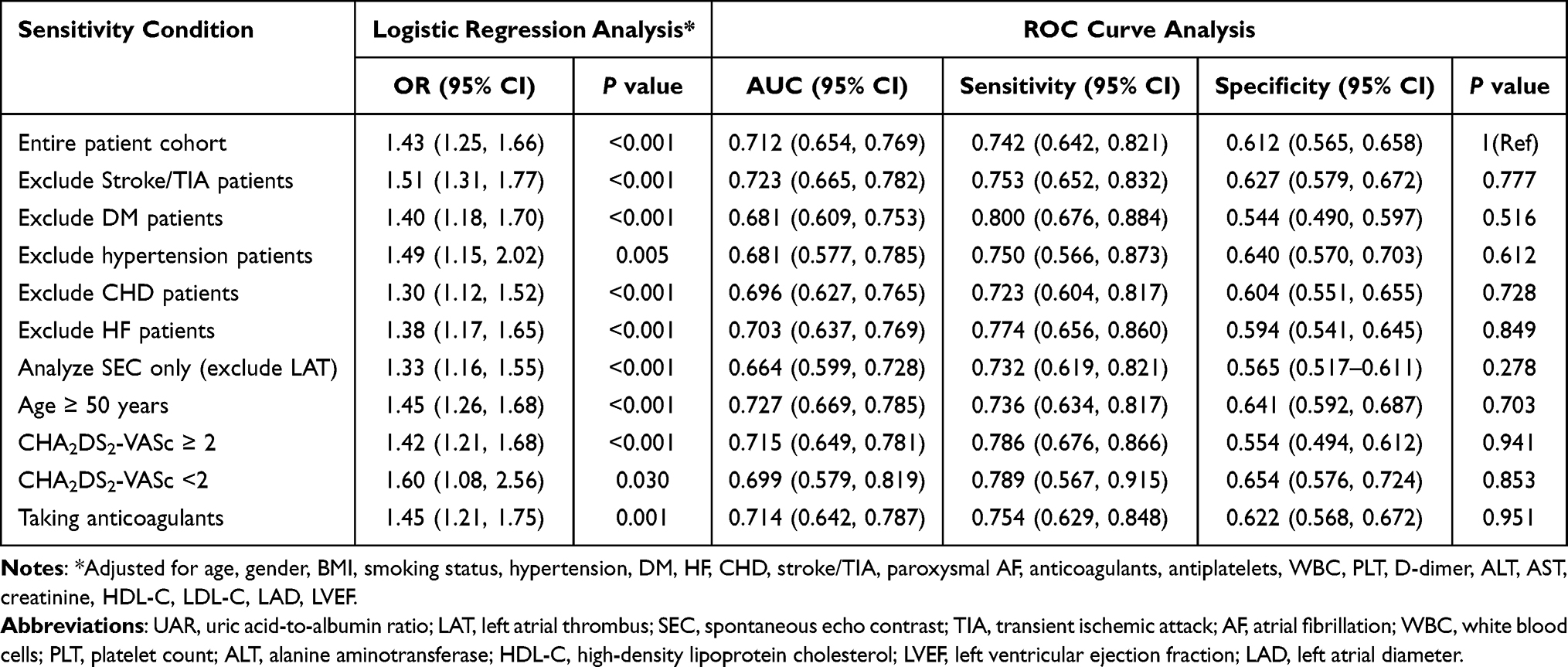 |
Table 3 Sensitivity Analysis of the UAR in Predicting LAT/SEC |
Mediation Analysis of UAR and LAT/SEC
Of the 10 clinically relevant candidates evaluated, only LAD and LVEF were identified as significant mediators of the association between UAR and LAT/SEC (Supplementary Table 6). Mediation analysis revealed that LAD (8.26%, P < 0.01) and LVEF (9.75%, P < 0.01) partially mediated the total effect of UAR on LAT/SEC risk (Figure 6). Importantly, the average direct effect (ADE) of UAR remained significant in both mediation pathways (P < 0.001), indicating that these factors only partially account for the association and suggesting that UAR may also exert its effect through alternative biological pathways.
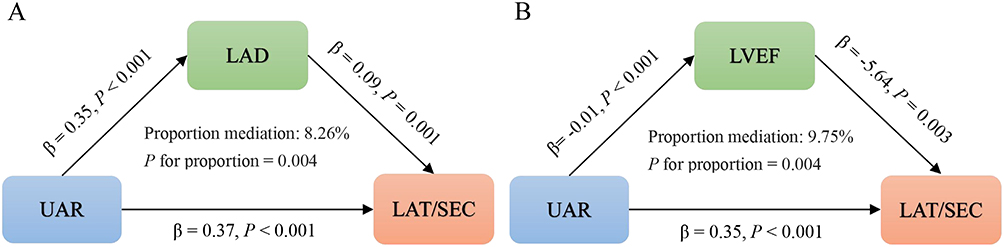 |
Figure 6 Mediating role of LAD (A) and LVEF (B) in the association between UAR and LAT/SEC. Abbreviations: UAR, uric acid-to-albumin ratio; LAT/SEC, left atrial thrombus or spontaneous echo contrast; LAD, left atrial diameter; LVEF, left ventricular ejection fraction. |
Discussion
To the best of our knowledge, this study is the first to evaluate the relationship between UAR and LAT/SEC in patients with NVAF and to elucidate the underlying mediating pathways. Our primary findings are fourfold: (1) UAR is independently associated with LAT/SEC risk, exhibiting a distinct non-linear relationship with a critical inflection point at 12.11; (2) UAR significantly outperforms UA or albumin alone and provides incremental predictive value beyond the CHA2DS2-VASc score; (3) this association remains consistent across clinical subgroups and sensitivity analyses; and (4) structural remodeling (LAD) and functional impairment (LVEF) partially mediate the impact of UAR on LAT/SEC. These results highlight UAR as a simple, cost-effective, and promising biomarker for optimizing thromboembolic risk stratification in NVAF.
AF is no longer regarded merely as an isolated electrophysiological abnormality, but as a complex systemic disorder driven by profound metabolic and inflammatory remodeling.5,19 In this context, UAR has gained increasing attention as a reliable surrogate marker for this systemic burden. Derived from routine laboratory tests, it encapsulates the pathophysiological crosstalk among oxidative stress, inflammation, and nutritional status, thereby facilitating a more holistic assessment of the inflammatory-metabolic burden in AF. Owing to its resilience against confounding from comorbidities, UAR demonstrates robust predictive value across various AF phenotypes. For instance, Selçuk et al identified elevated UAR as an independent predictor of new-onset AF in ST-elevation myocardial infarction patients,20 while a retrospective study found a similar association with postoperative AF following coronary artery bypass grafting.21 In addition, both studies reported that UAR outperforms its individual components—a trend supported by our findings, where UAR achieved a significantly higher AUC (0.712) than UA (0.684) or albumin (0.612) alone. Beyond onset prediction, UAR has also emerged as a significant risk factor for AF recurrence post-catheter ablation.22 These findings, coupled with the established link between elevated UAR and adverse outcomes in hypertension,23 heart failure,24 coronary heart disease,25,26 and stroke,27 underscore its broad clinical utility as a composite marker. However, previous studies have primarily focused on general cardiovascular outcomes, leaving the specific impact of UAR on atrial thrombogenicity—the primary driver of thromboembolism in NVAF—insufficiently explored. Our findings address this critical gap by demonstrating that the systemic imbalance reflected by an elevated UAR promotes atrial thrombus formation.
Although UA and albumin exert opposing physiological effects, their concurrent dysregulation synergistically promotes a prothrombotic microenvironment in AF. Elevated UA induces excessive reactive oxygen species (ROS) production, exacerbates oxidative stress, reduces nitric oxide (NO) bioavailability, and leads to endothelial dysfunction.28 Additionally, UA activates the NLRP3 inflammasome, triggering the release of pro-inflammatory cytokines (eg, IL-1β, IL-18),29 which drive platelet and coagulation activation.30 In contrast to UA, serum albumin scavenges ROS, mitigating oxidative stress and metabolic imbalance.31 This antioxidant capacity confers anticoagulant and antiplatelet effects, preserving endothelial homeostasis.32 Moreover, hyperuricemia-induced inflammatory cascades not only suppress hepatic albumin synthesis but also increase vascular endothelial permeability, promoting albumin leakage and aggravating hypoalbuminemia.29,33 Hypoalbuminemia elevates blood viscosity and disrupts microvascular hemorheological properties.34 Consequently, an elevated UAR drives a vicious cycle of endothelial injury, platelet activation, and abnormal hemorheology. Consistent with Virchow’s triad, this distinct hematological mechanism establishes the core pathological basis for LAT/SEC, acting in concert with macroscopic structural remodeling to drive thrombus formation.
While current guidelines prioritize the CHA2DS2-VASc score for thromboembolic risk stratification in NVAF, this clinically based system may not fully capture the complex biological heterogeneity of individual patients.1 Our findings demonstrate that incorporating UAR as an objective biomarker significantly refines this assessment: adding UAR to the CHA2DS2-VASc score markedly improved the C-index, while significant positive NRI and IDI values confirmed superior risk reclassification and enhanced identification of high-risk individuals. Calibration curves showed strong agreement between predicted and observed risks, providing a reliable basis for clinical decision-making. Moreover, DCA verified that the integrated model yields a higher net benefit across a broad range of threshold probabilities. This enables clinicians to more precisely tailor anticoagulation therapy, reducing both overtreatment and undertreatment. The utility of this integrated strategy is supported by Gong et al, who recently validated the incremental prognostic value of incorporating UAR into the CHA2DS2-VASc score for predicting mortality in AF.35 However, our study provides a critical mechanistic complement to their findings. Whereas their work underscores the prognostic utility of UAR for adverse clinical endpoints, our approach offers pathophysiological insights by leveraging the direct visualization of embolic precursors. By linking UAR profiles to these early-stage pathological markers, we position UAR as a biologically anchored biomarker that refines individualized risk management in NVAF.
Our study also provides quantitative evidence supporting the “inflammation–cardiac remodeling–thrombosis” cascade. Spearman correlation analyses revealed that elevated UAR was positively correlated with LAD and negatively correlated with LVEF, reflecting adverse structural and functional remodeling. Moreover, mediation analysis identified LAD and LVEF as key partial mediators, accounting for 8.26% and 9.75% of the total effect of UAR on LAT/SEC risk, respectively (both P < 0.01). While the direct effect of UAR (P < 0.001) reflects endothelial dysfunction and hypercoagulability, its indirect effects capture the structural and functional facets of stasis. Mechanistically, we hypothesize that the inflammatory and oxidative milieu reflected by elevated UAR likely promotes atrial interstitial fibrosis and disrupts intracellular calcium handling,35,36 which clinically manifests as progressive atrial dilatation and impaired myocardial contractility in our cohort. Although enlarged LAD and reduced LVEF are established predictors of LAT/SEC,37–40 our study reframes them as mechanistic mediators within the inflammatory-metabolic axis associated with UAR. This represents a key distinction from previous studies that primarily viewed them as isolated predictors rather than intermediate links in this thrombogenic cascade. These findings suggest that upstream interventions targeting this axis may optimize cardiac architecture and function, thereby indirectly mitigating thromboembolic risk in NVAF.
Limitations and Future Directions
Despite these novel findings, several limitations warrant consideration. First, the retrospective, single-center design and relatively small sample size preclude establishing causality. The lack of an independent external validation cohort may limit the generalizability of our results. Second, the absence of head-to-head comparisons with traditional inflammatory markers (eg, CRP, IL-6) restricts our ability to define the clinical specificity of UAR. Third, biomarkers were assessed only at admission, without tracking dynamic fluctuations during hospitalization; thus, the temporal association between UAR and LAT/SEC risk remains to be fully elucidated. Fourth, our study was restricted to patients undergoing TEE prior to cardioversion or ablation. This highly selected cohort may not represent the general AF population, inherently introducing selection bias and potentially overestimating the clinical risk of LAT/SEC. Fifth, the relatively low event count may increase the risk of overfitting in multivariable models; therefore, results should be interpreted with caution. Finally, despite adjusting for known confounders, residual confounding from unmeasured variables—such as dietary patterns, medication adherence, and comorbidity severity—cannot be entirely excluded. In light of these considerations, UAR should be viewed as a complementary marker rather than a replacement for clinical evaluation or TEE in these settings.
Future research should focus on the following directions: (1) large-scale prospective and multi-center studies with external validation; (2) directly comparing the predictive value of UAR against established inflammatory markers and assessing its dynamic temporal changes; and (3) elucidating the underlying mechanisms to explore the potential of inflammation-targeted therapies for improving patient outcomes.
Conclusion
This study demonstrates that UAR independently predicts LAT/SEC in patients with NVAF, with superior predictive accuracy over its individual components and significant incremental value beyond the CHA2DS2-VASc score. Furthermore, our findings underscore the significance of the inflammatory-metabolic axis, suggesting that the synergistic imbalance between UA and albumin contributes to atrial thrombogenesis, a process partially mediated by left atrial structural (LAD) and functional (LVEF) remodeling. As an easily accessible and cost-effective biomarker, UAR provides a practical strategy to refine thromboembolic risk stratification and may help guide personalized anticoagulation. Future large-scale prospective studies are warranted to validate these findings and explore the therapeutic potential of targeting this axis to mitigate thromboembolic risk in NVAF.
Data Sharing Statement
The data used to support the findings of this study are available from the corresponding author upon reasonable request.
Ethics Approval and Consent to Participate
This study was approved by the Ethics Committee of the First Affiliated Hospital of Dalian Medical University (No. PJ-KS-KY-2026-122) and conducted in accordance with the Declaration of Helsinki. Written informed consent was obtained from all participants, and all data were anonymized to ensure confidentiality. This study was reported in accordance with the REporting of studies Conducted using Observational Routinely-collected health Data (RECORD) guidelines.
Acknowledgments
We acknowledge Yidu Cloud (Beijing) Technology Ltd. for their cooperation in data searching, extraction, and processing.
Author Contributions
Xiangzhu Meng: Conceptualization, Data curation, Formal analysis, Methodology, Writing – original draft, Writing – review & editing. Yuhang Wen: Methodology, Data curation, Writing – original draft, Writing – review & editing. Xiangying Wang: Methodology, Data curation, Writing – original draft, Writing – review & editing. Tesfaldet Habtemariam Hidru: Conceptualization, Writing – review & editing, Supervision. Yuqi Tang: Conceptualization, Writing – review & editing, Supervision. Yunlong Xia: Writing – review & editing, Supervision, Funding acquisition, Project administration, Resources, Visualization. Xiaolei Yang: Writing – review & editing, Supervision, Funding acquisition, Project administration, Resources, Visualization. Lianjun Gao: Writing – review & editing, Supervision, Funding acquisition, Project administration, Resources, Visualization.
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis, and interpretation, or in all these areas; took part in drafting, revising, or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Xiangzhu Meng, Yuhang Wen, and Xiangying Wang share first authorship.
Funding
The author(s) declare that financial support was received for the research and/or publication of this article. This work was supported by the National Key Research and Development Program of China (2022YFC3601301), the National Natural Science Foundation of China (U25A2009), the Dalian Science Fund for Distinguished Young Scholars (2022RJ13), and the Medical and Industry Joint Innovation Program between the First Affiliated Hospital of Dalian Medical University and Dalian Institute of Chemical Physics (DMU-1 & DICP) (UN202201).
Disclosure
The authors have no conflicts of interest to disclose.
References
1. Joglar JA, Chung MK, Armbruster AL, et al. 2023 ACC/AHA/ACCP/HRS guideline for the diagnosis and management of atrial fibrillation: a report of the American College of Cardiology/American heart association joint committee on clinical practice guidelines. Circulation. 2024;149(1):e1–14. doi:10.1161/CIR.0000000000001193
2. Lane DA, Skjøth F, Lip GYH, Larsen TB, Kotecha D. Temporal trends in incidence, prevalence, and mortality of atrial fibrillation in primary care. J Am Heart Assoc. 2017;6(5):e005155. doi:10.1161/JAHA.116.005155
3. Al-Saady NM, Obel OA, Camm AJ. Left atrial appendage: structure, function, and role in thromboembolism. Heart. 1999;82(5):547–554. doi:10.1136/hrt.82.5.547
4. Liang D, Shi R, Zheng KI, et al. Clinical characteristics and outcomes in patients with echocardiographic left ventricular spontaneous echo contrast. Int J Cardiol. 2021;330:245–250. doi:10.1016/j.ijcard.2021.02.005
5. Karam BS, Chavez-Moreno A, Koh W, Akar JG, Akar FG. Oxidative stress and inflammation as central mediators of atrial fibrillation in obesity and diabetes. Cardiovasc Diabetol. 2017;16(1):120. doi:10.1186/s12933-017-0604-9
6. Ding WY, Gupta D, Lip GYH. Atrial fibrillation and the prothrombotic state: revisiting Virchow’s triad in 2020. Heart. 2020;106(19):1463–1468. doi:10.1136/heartjnl-2020-316977
7. Guo Y, Lip GY, Apostolakis S. Inflammation in atrial fibrillation. J Am Coll Cardiol. 2012;60(22):2263–2270. doi:10.1016/j.jacc.2012.04.063
8. Kanellis J, Kang DH. Uric acid as a mediator of endothelial dysfunction, inflammation, and vascular disease. Semin Nephrol. 2005;25(1):39–42. doi:10.1016/j.semnephrol.2004.09.007
9. Tang RB, Dong JZ, Yan XL, et al. Serum uric acid and risk of left atrial thrombus in patients with nonvalvular atrial fibrillation. Can J Cardiol. 2014;30(11):1415–1421. doi:10.1016/j.cjca.2014.06.009
10. Zhang X, Hu M, Wang X, et al. New perspective on the risk markers for left atrial thrombosis in patients with atrial fibrillation. Eur J Prev Cardiol. 2021;28(6):641–647. doi:10.1177/2047487320912084
11. Arques S. Human serum albumin in cardiovascular diseases. Eur J Intern Med. 2018;52:8–12. doi:10.1016/j.ejim.2018.04.014
12. Bucci T, Pastori D, Pignatelli P, et al. Albumin levels and risk of early cardiovascular complications after ischemic stroke: a propensity-matched analysis of a global federated health network. Stroke. 2024;55(3):604–612. doi:10.1161/STROKEAHA.123.044248
13. Wang CS, Sun Y, Ren J. Uric acid to albumin ratio, a novel biomarker of cardiovascular disease. Angiology. 2024;75(4):394. doi:10.1177/00033197231178888
14. Benchimol EI, Smeeth L, Guttmann A, et al. The REporting of studies Conducted using Observational Routinely-collected health Data (RECORD) statement. PLoS Med. 2015;12(10):e1001885. doi:10.1371/journal.pmed.1001885
15. Aschenberg W, Schlüter M, Kremer P, Schröder E, Siglow V, Bleifeld W. Transesophageal two-dimensional echocardiography for the detection of left atrial appendage thrombus. J Am Coll Cardiol. 1986;7(1):163–166. doi:10.1016/s0735-1097(86)80275-3
16. Black IW, Hopkins AP, Lee LC, Walsh WF. Left atrial spontaneous echo contrast: a clinical and echocardiographic analysis. J Am Coll Cardiol. 1991;18(2):398–404. doi:10.1016/0735-1097(91)90592-w
17. Hsieh FY, Bloch DA, Larsen MD. A simple method of sample size calculation for linear and logistic regression. Stat Med. 1998;17(14):1623–1634. doi:10.1002/(sici)1097-0258(19980730)17:14<1623::aid-sim871>3.0.co;2-s
18. Li Z, Liu Q, Liu F, et al. Nomogram to predict left atrial thrombus or spontaneous echo contrast in patients with non-valvular atrial fibrillation. Front Cardiovasc Med. 2021;8:737551. doi:10.3389/fcvm.2021.737551
19. Bode D, Pronto JRD, Schiattarella GG, Voigt N. Metabolic remodelling in atrial fibrillation: manifestations, mechanisms and clinical implications. Nat Rev Cardiol. 2024;21(10):682–700. doi:10.1038/s41569-024-01038-6
20. Selçuk M, Çınar T, Şaylık F, et al. Predictive value of uric acid/albumin ratio for the prediction of new-onset atrial fibrillation in patients with ST-Elevation myocardial infarction. Rev Invest Clin. 2022;74(3):156–164. doi:10.24875/RIC.22000072
21. Koyuncu I, Aydın S, Gurses E, Sivri F, Emren ZY, Gul I. Predictive value of uric acid/albumin ratio for postoperative atrial fibrillation following isolated coronary artery bypass surgery. Braz J Cardiovasc Surg. 2026;41(1):e20240348. doi:10.21470/1678-9741-2024-0348
22. Karataş MB, Durmuş G, Zengin A, et al. Association of uric acid albumin ratio with recurrence of atrial fibrillation after cryoballoon catheter ablation. Medicina. 2022;58(12):1872. doi:10.3390/medicina58121872
23. Şaylık F, Çınar T, Selçuk M, Tanboğa İH. The relationship between uric acid/albumin ratio and carotid intima-media thickness in patients with hypertension. Arq Bras Cardiol. 2023;120(5):e20220819. doi:10.36660/abc.20220819
24. Liu X, Chu A, Ding X. Elevated uric acid to serum albumin ratio: a predictor of short-term outcomes in Chinese heart failure patients. Front Nutr. 2024;11:1481155. doi:10.3389/fnut.2024.1481155
25. Yalcinkaya D, Karacali K, Ilhan BC, Yarlioglues M. Relation between serum uric acid to albumin ratio and severity of chronic coronary artery disease. Angiology. 2024;75(4):386–393. doi:10.1177/00033197231161902
26. Li S, Chen H, Zhou L, Cui H, Liang S, Li H. The uric acid to albumin ratio: a novel predictor of long-term cardiac mortality in patients with unstable angina pectoris after percutaneous coronary intervention. Scand J Clin Lab Invest. 2022;82(4):304–310. doi:10.1080/00365513.2022.2084698
27. Biter HI, Tosu AR. The prognostic significance of uric acid/albumin ratio in patients with aortic stenosis following transcatheter aortic valve implantation for major adverse cardiac and cerebral events. Medicina. 2023;59(4):686. doi:10.3390/medicina59040686
28. Maruhashi T, Hisatome I, Kihara Y, Higashi Y. Hyperuricemia and endothelial function: from molecular background to clinical perspectives. Atherosclerosis. 2018;278:226–231. doi:10.1016/j.atherosclerosis.2018.10.007
29. Zhang H, Ma Y, Cao R, et al. Soluble uric acid induces myocardial damage through activating the NLRP3 inflammasome. J Cell Mol Med. 2020;24(15):8849–8861. doi:10.1111/jcmm.15523
30. Hindle MS, Berger M, Naseem KM. The NLRP3 inflammasome in platelets - form, functions, and future of the complex. Platelets. 2025;36(1):2562267. doi:10.1080/09537104.2025.2562267
31. Tabata F, Wada Y, Kawakami S, Miyaji K. Serum albumin redox states: more than oxidative stress biomarker. Antioxidants. 2021;10(4):503. doi:10.3390/antiox10040503
32. Manolis AA, Manolis TA, Melita H, Mikhailidis DP, Manolis AS. Low serum albumin: a neglected predictor in patients with cardiovascular disease. Eur J Intern Med. 2022;102:24–39. doi:10.1016/j.ejim.2022.05.004
33. Eckart A, Struja T, Kutz A, et al. Relationship of nutritional status, inflammation, and serum albumin levels during acute illness: a prospective study. Am J Med. 2020;133(6):713–722.e7. doi:10.1016/j.amjmed.2019.10.031
34. Pajic-Lijakovic I, Milivojevic M, Barshtein G, Gural A. The mechanical properties of erythrocytes are influenced by the conformational state of albumin. Cells. 2025;14(15):1139. doi:10.3390/cells14151139
35. Gong A, Cao Y, Li Z, et al. Uric acid-to-albumin ratio as a cardiometabolic marker for predicting adverse outcomes in patients with atrial fibrillation: evidence from two independent cohorts. Front Endocrinol. 2026;17:1786997. doi:10.3389/fendo.2026.1786997
36. Packer M. Characterization, pathogenesis, and clinical implications of inflammation-related atrial myopathy as an important cause of atrial fibrillation. J Am Heart Assoc. 2020;9(7):e015343. doi:10.1161/JAHA.119.015343
37. Shi S, Zhao Q, Liu T, et al. Left atrial thrombus in patients with non-valvular atrial fibrillation: a cross-sectional study in China. Front Cardiovasc Med. 2022;9:827101. doi:10.3389/fcvm.2022.827101
38. Lin WD, Xue YM, Liu FZ, et al. Left atrial enlargement and non-paroxysmal atrial fibrillation as risk factors for left atrial thrombus/spontaneous Echo contrast in patients with atrial fibrillation and low CHA2DS2-VASc score. J Geriatr Cardiol. 2020;17(3):155–159. doi:10.11909/j.issn.1671-5411.2020.03.001
39. Rader VJ, Khumri TM, Idupulapati M, Stoner CN, Magalski A, Main ML. Clinical predictors of left atrial thrombus and spontaneous echocardiographic contrast in patients with atrial fibrillation. J Am Soc Echocardiogr. 2007;20(10):1181–1185. doi:10.1016/j.echo.2007.02.010
40. Wybraniec MT, Mizia-Szubryt M, Cichoń M, et al. Heart failure and the risk of left atrial thrombus formation in patients with atrial fibrillation or atrial flutter. ESC Heart Fail. 2022;9(6):4064–4076. doi:10.1002/ehf2.14105
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Development and Validation of a Nomogram for Estimation of Left Atrial Thrombus or Spontaneous Echo Contrast Risk in Non-Valvular Atrial Fibrillation Patients with Low to Borderline CHA2DS2-VASc Score
Li Z, Pan L, Deng Y, Liu Q, Hidru T, Liu F, Li C, Cong T, Yang X, Xia Y
International Journal of General Medicine 2022, 15:7329-7339
Published Date: 18 September 2022
Predictive Value of Residual Cholesterol Inflammatory Index for Left Atrial Thrombus or Spontaneous Echo Contrast in Patients with Nonvalvular Atrial Fibrillation with Low CHA2DS2-VASc Scores
Wang J, Jin Y, Wang L, Wang Y, Lu J
International Journal of General Medicine 2026, 19:604377
Published Date: 30 April 2026