Back to Journals » International Journal of General Medicine » Volume 19
Predictive Value of Residual Cholesterol Inflammatory Index for Left Atrial Thrombus or Spontaneous Echo Contrast in Patients with Nonvalvular Atrial Fibrillation with Low CHA2DS2-VASc Scores
Authors Wang J ![]() , Jin Y, Wang L, Wang Y, Lu J
, Jin Y, Wang L, Wang Y, Lu J
Received 20 February 2026
Accepted for publication 23 April 2026
Published 30 April 2026 Volume 2026:19 604377
DOI https://doi.org/10.2147/IJGM.S604377
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Redoy Ranjan
Jiaqi Wang,1,2 Yaqiong Jin,2 Li Wang,2 Yunmeng Wang,1,2 Jingchao Lu2
1Department of Graduate, Hebei Medical University, Shijiazhuang, People’s Republic of China; 2Department of Cardiology, The Second Hospital of Hebei Medical University, Shijiazhuang, People’s Republic of China
Correspondence: Jingchao Lu, Department of Cardiology, The Second Hospital of Hebei Medical University, 215 Hepingxi Road, Shijiazhuang, Hebei, 050000, People’s Republic of China, Email [email protected]
Background: Left atrial thrombus (LAT) is the main cause of ischemic stroke in patients with atrial fibrillation. Left atrial thrombus or spontaneous echo contrast (SEC) can be best displayed by transesophageal echocardiography (TEE). This study aimed to evaluate non-valvular atrial fibrillation (NVAF) patients with LAT/SEC confirmed by transesophageal echocardiography compared with those without LAT/SEC, using residual cholesterol inflammatory index (RCII) as a sensitive biomarker.
Methods: This study was a retrospective study of 967 NVAF patients who underwent transesophageal echocardiography at a single center. Patients were divided into two groups based on the presence or absence of LAT/SEC on TEE. The levels of RCII and left atrium diameter (LAD) were compared.
Results: RCII was identified as an independent variable in patients with LAT/SEC detected by transesophageal echocardiography. (OR: 1.232, CI:1.159– 1.309, p < 0.001) The combination of RCII, LAD, and CHA2DS2-VASc scores had the highest area under the curve (AUC) value (AUC:0.787 CI:0.748– 0.826 p < 0.001).
Conclusion: Our study demonstrates that RCII and LAD are risk factors for LAT/SEC. CHA2DS2-VASc score combined with RCII and LAD can significantly improve the predictive ability of LAT/SEC.
Keywords: nonvalvular atrial fibrillation, left atrial thrombus, spontaneous echo contrast, residual cholesterol inflammatory index, transesophageal echocardiography
Introduction
Atrial fibrillation (AF) is the most common persistent arrhythmia in clinical practice, and its incidence is increasing with the improvement of chronic disease survival rate and population aging.1 Left atrial thrombosis (LAT) is significantly associated with stroke in patients with nonvalvular atrial fibrillation (NVAF). Early assessment of stroke risk and timely anticoagulant therapy are critical to reduce thromboembolic events and mortality.2 In addition, spontaneous echo contrast (SEC) in patients with AF indicates the pre-thrombotic state, which can lead to further thrombosis and is therefore an indication of anticoagulation therapy.3
At present, the CHA2DS2-VASc scores are mainly used in clinical practice to assess stroke risk in patients with AF, and anticoagulation therapy is guided according to the score.4 Current clinical guidelines recommend anticoagulation therapy for AF patients with high CHA2DS2-VASc scores, while there is still debate about whether to give anticoagulant therapy to patients with low CHA2DS2-VASc scores (women:1–2 points; men:0–1 point), who are therefore at risk for LAT/SEC and thromboembolism.5,6
Residual cholesterol (RC) is a triglyceride-rich lipoprotein cholesterol composed of very low-density lipoprotein (VLDL), medium-density lipoprotein (IDL), and chylomicron residues.7 It is not only closely related to the occurrence and development of atherosclerosis but also a risk factor for hypertension, aortic stenosis, stroke, and death from cardiovascular disease.8–11 RC can be deposited in the lining of blood vessels, leading to endothelial dysfunction and vascular inflammation. In addition, the triglycerides in RC can be broken down into free fatty acids and monoacylglycerol, thus aggravating the body’s inflammatory response.12,13 Studies have shown that elevated levels of RC and highly sensitive C-reactive protein (hs-CRP) can reflect low-grade inflammation in the body.14,15 Elevated RC levels, combined with persistent low-grade inflammation, may promote the development of LAT/SEC in patients with NVAF and further influence stroke development.
Residual cholesterol inflammatory index (RCII), calculated by RC and hs-CRP, provides a comprehensive assessment of residual cholesterol and low-grade inflammation.16 Therefore, the purpose of this study was to evaluate the predictive ability of RCII for LAT/SEC in patients with NVAF with low CHA2DS2-VASc scores, to identify patients whose CHA2DS2-VASc scores failed to detect thrombosis, give timely anticoagulant therapy, and improve their prognosis.
Materials and Methods
Study Design and Participants
This study was a single-center retrospective cohort study. This study collected data from 2681 patients with NVAF through the inpatient electronic medical record system, all of whom were admitted to the cardiology Department of the Second Hospital of Hebei Medical University between January 2022 and December 2023 and underwent transesophageal echocardiography (TEE) and transthoracic echocardiography (TTE). TEE was performed in all study participants, primarily as a clinical requirement to exclude LAT or SEC before catheter ablation or cardioversion.
Inclusion criteria: 1) age>18 years old; 2) transthoracic and transesophageal echocardiography were completed, and the relevant clinical data were complete; 3) non-valvular atrial fibrillation. Exclusion criteria: 1) patients with high CHA2DS2-VASc scores (women≥3; men≥2); 2) patients with heart valve disease or who have previously undergone valve replacement or remodeling surgery; 3) patients with congenital heart disease; 4) Patients with cardiomyopathy; 5) patients with autoimmune diseases, hyperthyroidism, and other systemic diseases; 6) patients with severe hepatic and renal insufficiency or malignant tumor; 7) complicated with acute myocardial infarction or acute heart failure; 8) patients with incomplete clinical data. Eventually, 967 patients were enrolled in the study. All relevant information, including general clinical data, echocardiogram results, and laboratory test results, was collected from the electronic medical record system. Figure 1 shows the flow chart of the study. Ethical approval was obtained from the Ethics Committee of The Second Hospital of Hebei Medical University (Ethical Review number:2025-R528). The research was conducted according to the Helsinki Declaration guidelines.
 |
Figure 1 Flowchart for the study. Abbreviations: NVAF, non-valvular atrial fibrillation; TEE, transesophageal echocardiography; LAT/SEC, left atrial thrombus/spontaneous echo contrast. |
The diagnosis of AF is based on the ECG characteristics of AF on the routine 12-lead electrocardiograms, the persistent event of atrial fibrillation > 30s on the 24-hour Holter electrocardiogram, or the presence of a previous episode of AF. Hypertension is defined as systolic blood pressure ≥140 mmHg and/or diastolic blood pressure ≥90 mmHg, or the use of antihypertensive drugs. To diagnose diabetes, fasting serum glucose levels of at least 7.0 mmol/L and/or random glucose levels of at least 11.1 mmol/L were required. Congestive heart failure is diagnosed based on characteristic symptoms and subsequently confirmed by a physician’s diagnosis. Peripheral artery disease (PAD) was diagnosed using vascular Doppler ultrasound or past medical history. The diagnosis of ischemic stroke is based on imaging evidence or ischemic stroke history. The diagnosis of coronary heart disease is based on relevant clinical guidelines or coronary heart disease history. Transthoracic echocardiography and transesophageal echocardiography were examined and measured by experienced senior sonographers, in which the left ventricular ejection fraction (LVEF) was measured by the modified Simpson method, and the left atrial diameter (LAD) was measured by the anterior and posterior diameters of the left atrium.17 RC (mg/dL) was calculated as: RC=TC-(HDL-C+LDL-C). RCII was calculated by multiplying RC by hs-CRP, RCII=RC(mg/dL)×hs-CRP(mg/L)/10.16
CHA2DS2-VASc Scores
Based on the collected clinical information, the CHA2DS2-VASc scores were recalculated. 1 point is assigned for each risk variable, including congestive heart failure or left ventricular dysfunction, hypertension, diabetes, and vascular disease. Patients aged 65–74 years scored 1 point, and patients aged ≥75 years scored 2 points. Females get an extra point, 2 for stroke or transient ischemic attack. Low CHA2DS2-VASc scores included scores of 1–2 in female patients and 0–1 in male patients.18
Echocardiographic Examination
All patients underwent transesophageal echocardiography to determine the presence of LAT or SEC. The diagnostic criteria for LAT are mobile, independent, round, or irregular in shape, uniform in density but different from that of the surrounding myocardial tissue, and can be detected in multiple parts of the left atrial lumen.19 The diagnostic criteria for SEC are smoke, swirl, or pre-thrombotic states in the left atrium, but are distinct from the illusion caused by high-gain and near-field artifact changes.20 Data related to cardiac cavity size and ventricular wall motion were collected by completing TTE. The echocardiogram is performed by two professional ultrasound physicians, one of whom is responsible for completing the procedure and making the diagnosis, while the other is responsible for reviewing the results. Neither doctor was aware of the patient’s clinical condition before the examination.
Statistical Analyses
Statistical analysis was performed using SPSS (Version 26.0, SPSS Inc., Chicago, IL, USA). Categorical variables were compared between groups using the χ2 test and expressed as numbers (%). Continuous variables were first tested for normality by Kolmogorov–Smirnov, continuous variables with normal distribution were analyzed by t-test, and expressed as mean ± standard deviation, and continuous variables with non-normal distribution were analyzed by Mann–Whitney U-test. Logistic regression analysis was used to explore the influencing factors of LAT/SEC formation in patients with NVAF. The predictive power of RCII and other risk variables was analyzed by mapping receiver operating characteristics (ROC). With two-sided P<0.05, the difference was considered to be statistically significant.
Results
Characteristics of the Study Population
A total of 967 patients with NVAF were enrolled, with a mean age of 55.82±9.81 years. According to the results of transesophageal echocardiography, they were divided into the non-LAT/SEC group (n=849) and the LAT/SEC group (n=118). In the LAT/SEC group, 75 patients developed LAT, of which 25 patients combined with SEC, and only 43 patients developed SEC. The incidence of LAT and SEC accounted for 7.76% and 4.45% of the population, respectively. As shown in Table 1, heart failure (HF) (16.95% vs. 2.24%) was more prevalent in the LAT/SEC group, with higher body mass index (BMI) levels [27.12 ± 3.77 kg/m2 vs. 26.15 ± 3.67 kg/m2, P<0.01], total cholesterol (TC) levels[181.72 (156.70–208.29) mg/dL vs. 166.32 (145.15–190.19) mg/dL, P<0.01], and lipoprotein(a) (Lp(a)) levels [15.63 (7.09–26.13) mg/L vs. 11.91 (6.11–23.42) mg/L, P=0.023]compared to the non-LAT/SEC group. In addition, serum uric acid (SUA) [367.10 ± 90.81 umol/L vs. 340.83 ± 94.38 umol/L, P <0.005], aspartate aminotransferase (AST) [20.00 (16.30–26.00) U/L vs. 18.65 (15.20–23.00) U/L, P=0.006], high-sensitivity C-reactive protein (hs-CRP) [2.00 (1.48–4.48) mg/L vs. 1.70 (1.00–3.98) mg/L, P<0.01], monocyte count [0.60 (0.43–0.80)×109/L vs. 0.54 (0.41–0.70)×109/L, P=0.021], red blood cell count (RBC) [4.67 (4.38–5.03) g/L vs. 4.54 (4.23–4.89) g/L, P=0.004], red cell distribution width standard deviation (RDWSD) [43.80 (42.00–45.03) fl vs. 42.90 (41.10–44.60) fl, P=0.017], and residual cholesterol inflammatory index (RCII) [9.04 (5.18–16.90) vs. 3.81 (2.00–7.84), P<0.01] were also higher in this group. Left ventricular ejection fraction (LVEF) [60.00 (51.75–61.70) % vs. 61.40 (59.10–65.40) %, P<0.01], Lymphocyte count [1.75 ± 0.49×109/L vs. 1.93 ± 0.63×109/L, P=0.003], and paroxysmal atrial fibrillation (AF) (55.90% vs. 88%) in the LAT/SEC group were lower. No statistical differences were observed in terms of gender, age, systolic blood pressure, diastolic blood pressure, CHA2DS2-VASc scores, fasting plasma glucose (FPG), triglyceride (TG), high-density lipoprotein cholesterol (HDL-C), low-density lipoprotein cholesterol (LDL-C), serum creatinine (SCr), alanine aminotransferase (ALT), white blood cell count (WBC), neutrophil count, platelet count (PLT), platelet distribution width (PDW), mean platelet volume (MPV), smoke, alcohol consumption, previous diabetes, ischemic stroke, peripheral vascular disease (PAD), hyperlipidemia, chronic kidney disease (CKD), and pre-hospitalization medication.
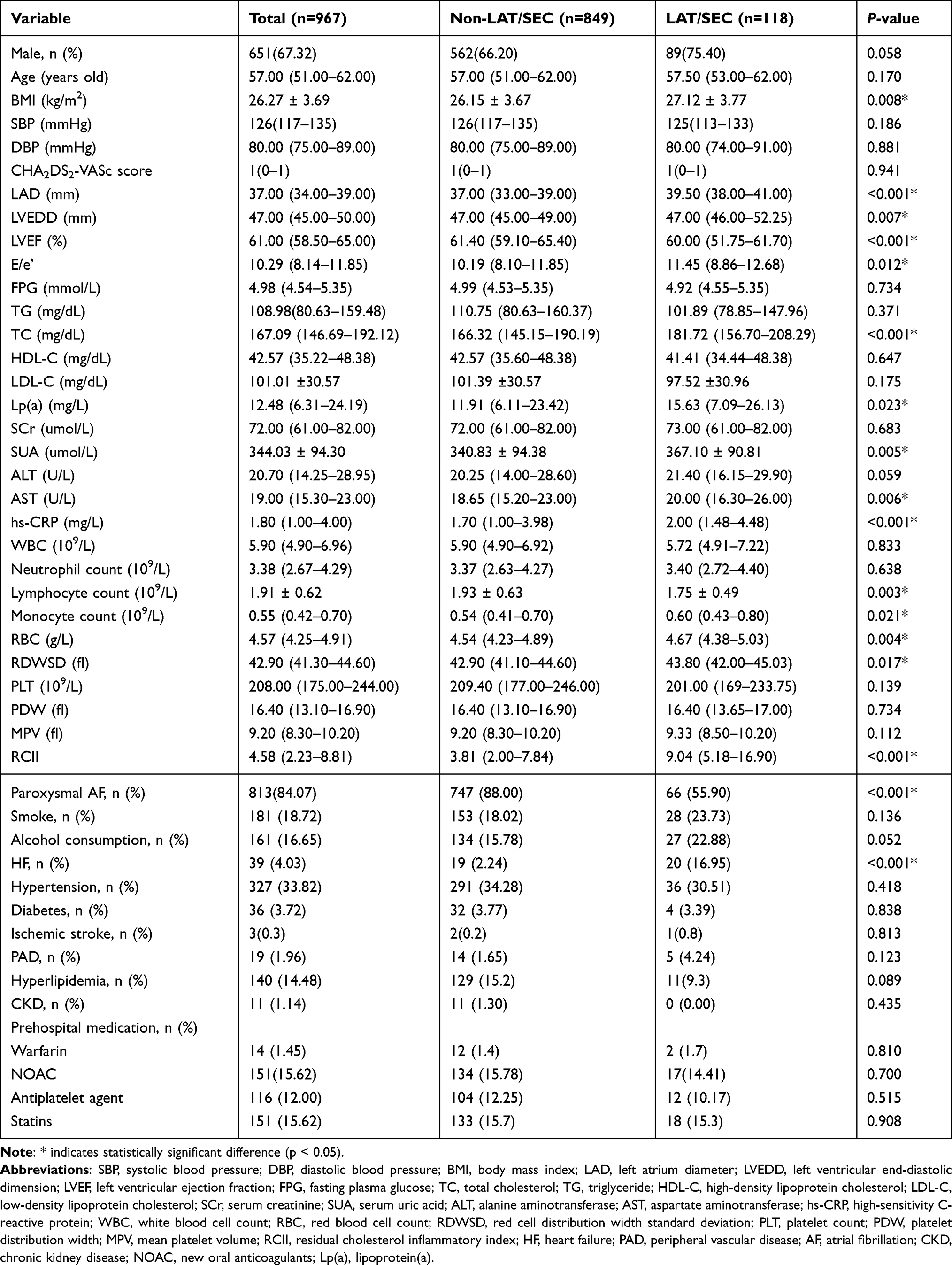 |
Table 1 Baseline Characteristics of NVAF Patients with/Without LAT/SEC |
Variables with P<0.05 in the baseline table were selected to be included in univariable logistic regression to determine the risk factors for the formation of LAT/SEC, and multivariate logistic regression analysis was performed. The results showed that LAD, lipoprotein(a), hs-CRP, lymphocyte count, monocyte count, history of heart failure, non-paroxysmal atrial fibrillation, and RCII were all predictors of LAT/SEC (Table 2).
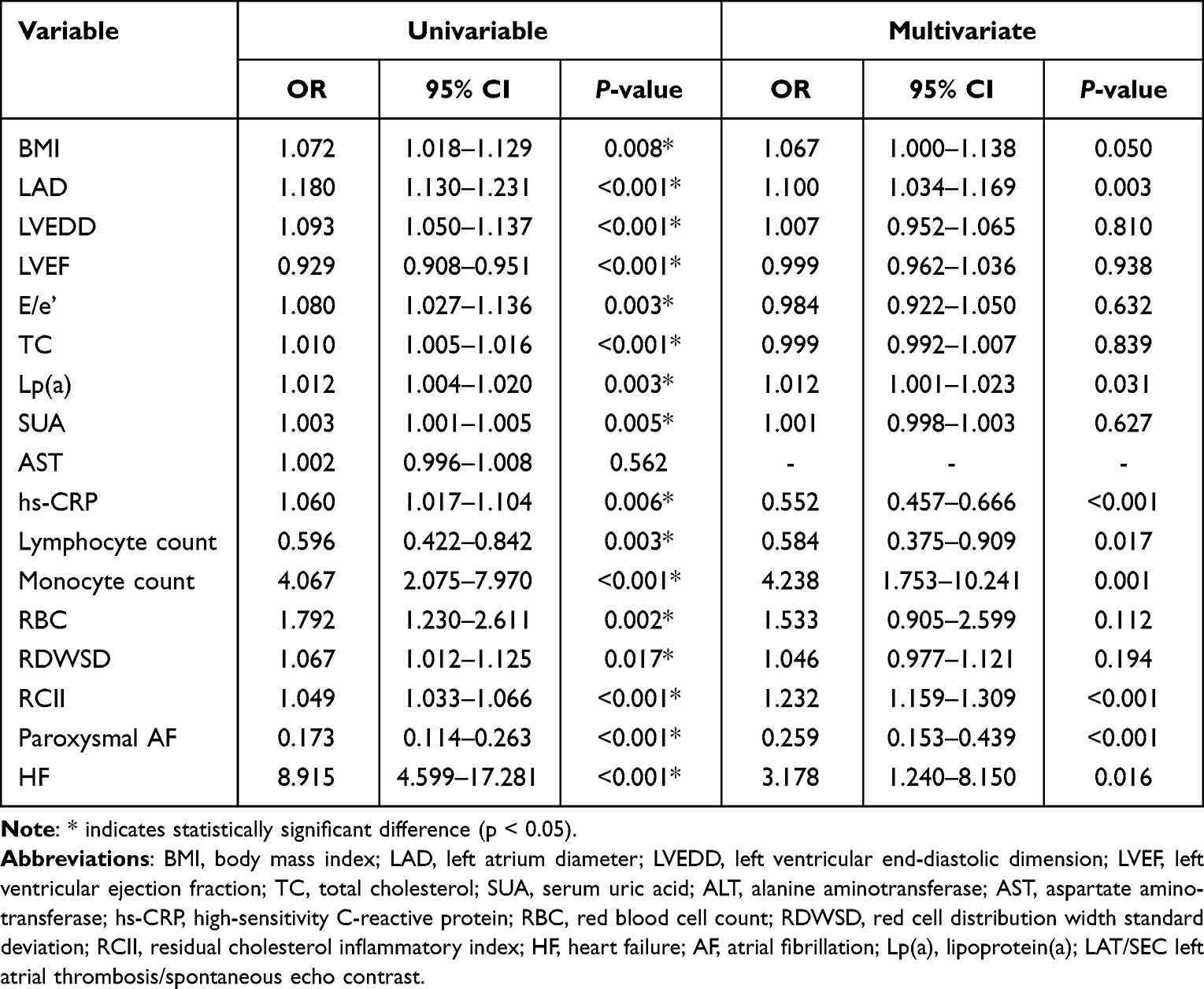 |
Table 2 Univariable and Multivariate Logistic Regression for Risk Factors of LAT/SEC |
Subjects were divided into four groups according to the quartile of RCII and LAD levels. Multivariate logistic regression analysis showed that RCII level was correlated with LAT/SEC (Table 3). Specifically, patients with the highest quartile array showed a higher incidence of LAT/SEC compared to the lowest quartile array. After adjusting for age and gender in Model I and other confounding factors including gender, age, body mass index, left ventricular ejection fraction, left ventricular end-diastolic dimension, E/e’, total cholesterol, lipoprotein(a), serum uric acid, alanine aminotransferase, aspartate aminotransferase, high-sensitivity C-reactive protein, heart failure, and paroxysmal atrial fibrillation in Model II, the association between RCII and LAT/SEC formation remained consistent.
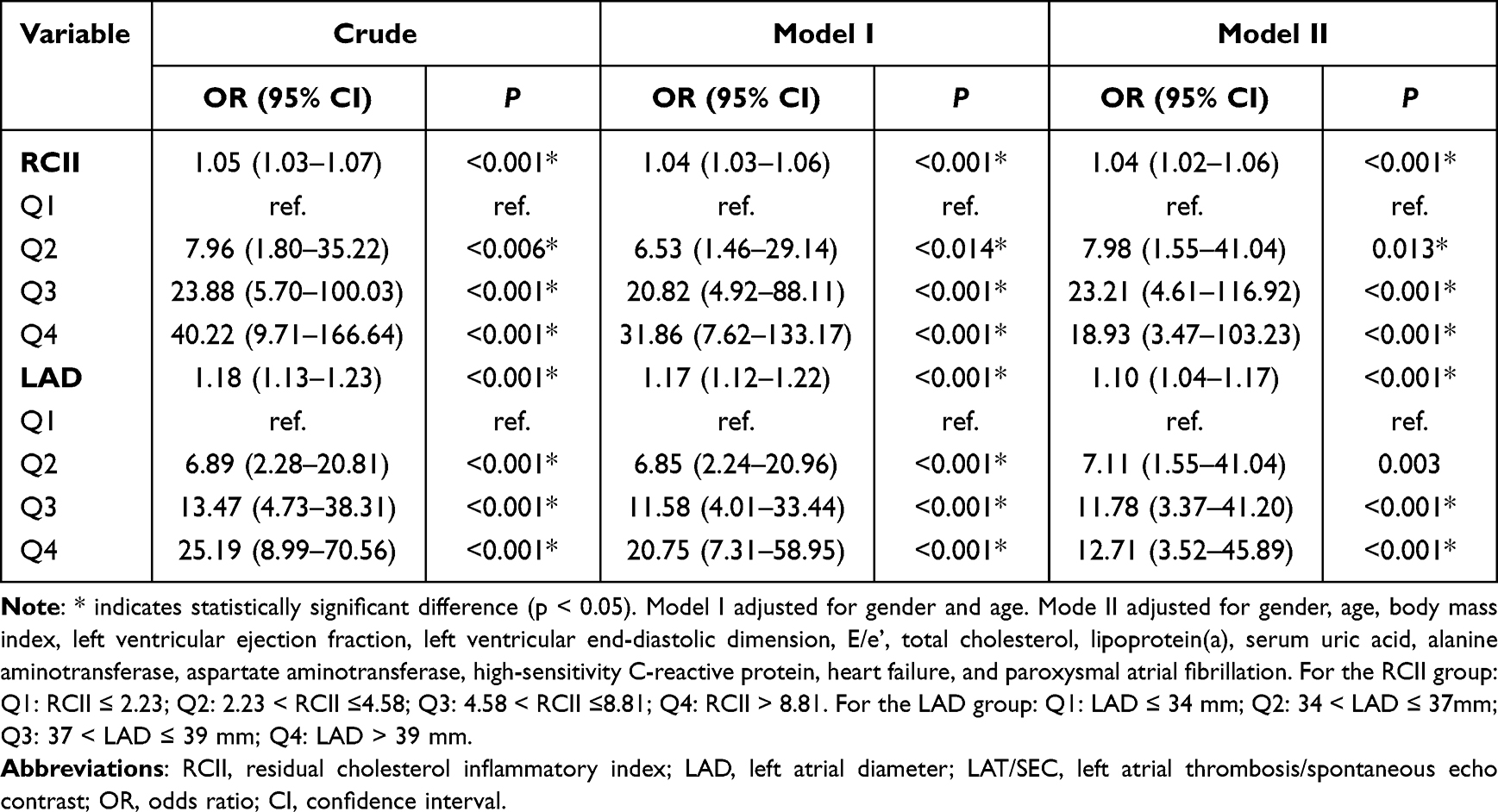 |
Table 3 The relationship of RCII and LAD to LAT/SEC |
Regardless of adjusting for confounding factors, the incidence of LAT/SEC increased significantly with the enlargement of the left atrium. As shown in Figure 2, the ROC curve was drawn to analyze the prediction efficiency of RCII and LAD for LAT/SEC. The results showed that the area under the curve (AUC) of RCII was 0.746 (95% CI 0.705–0.787, P<0.01), while that of LAD was 0.736 (95% CI 0.707–0.764, P<0.01).
 |
Figure 2 Receiver operating characteristic (ROC) curves for the prediction of left atrial thrombus/spontaneous echo contrast (LAT/SEC) of residual cholesterol inflammatory index (RCII) (A) and left atrial diameter (LAD) (B). Abbreviations: AUC, area under the curve. |
Increased RCII and left atrial enlargement are risk factors for LAT/SEC formation. RCII and LAD were incorporated into the new forecast model. As shown in Table 4 and Figure 3, the CHA2DS2-VASc scores had poor predictive power for LAT/SEC (AUC = 0.502, P>0.05). After the inclusion of RCII (Model A), the prediction efficiency was significantly improved (AUC difference=0.248, Z=7.350, P<0.01). After combining RCII and LAD (Model B), the model prediction efficiency was improved (AUC difference=0.285, Z=8.589, P<0.01). The prediction efficiency of Model B was higher than that of Model A, and the difference was statistically significant (AUC difference=0.037, Z=2.061, P=0.039).
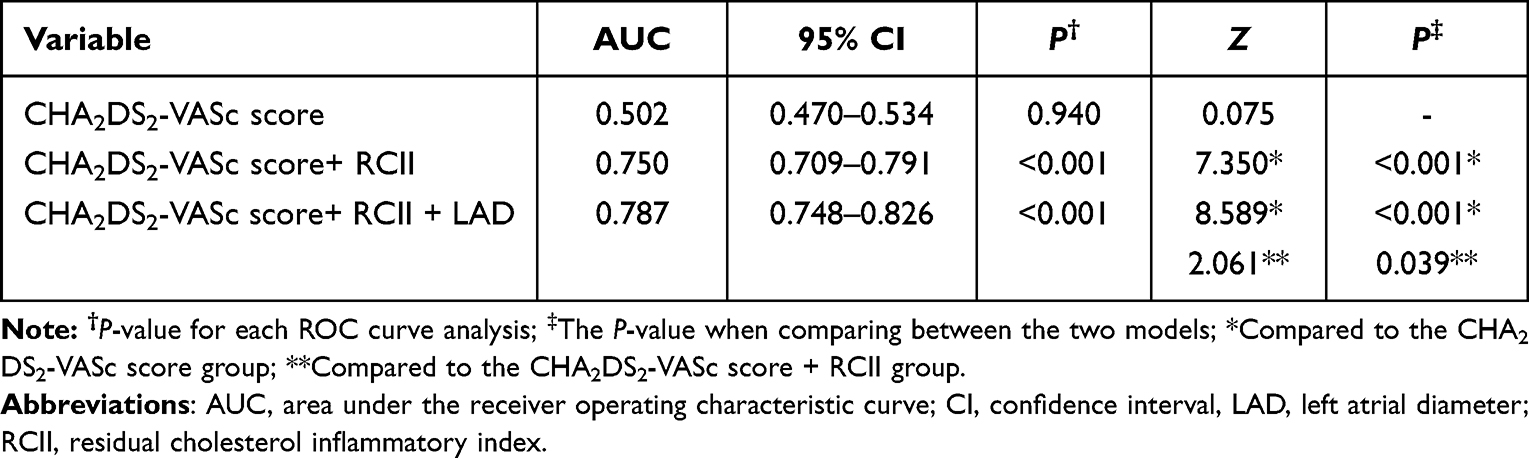 |
Table 4 Comparison Between the Prediction Models |
 |
Figure 3 Receiver operating characteristic (ROC) analysis of each prediction model. Abbreviations: RCII, residual cholesterol inflammatory index; LAD, left atrial diameter. |
Discussion
Atrial fibrillation (AF) is the most common arrhythmia, and because there are usually no obvious symptoms, it significantly increases the risk of stroke and all-cause death.21 Studies have shown that SEC and LAT are significantly correlated with AF-related embolism.22 Early identification of high-risk patients and timely anticoagulation therapy are of great significance for improving patient prognosis. Current clinical guidelines recommend anticoagulation therapy for patients with high CHA2DS2-VASc scores, while there is still controversy over whether patients with low CHA2DS2-VASc scores (0–1 in men and 1–2 in women) should be treated with anticoagulation.18 Many studies have shown that the CHA2DS2-VASc scores have limited predictive power in clinical practice, especially for patients with low thrombosis scores and poor sensitivity to LAT.23,24 Previous studies have shown that patients with NVAF with low CHA2DS2-VASc scores will still have thromboembolic events, among which the annual stroke rate of women with a score of 2 and men with a score of 1 is about 3%, while the incidence of thrombotic events is as high as 11.4% in patients with a score of 0–1.25,26 However, the CHA2DS2-VASc scores may be delayed to some extent for low-risk patients without previous embolic events, only after the occurrence of embolic events, and this scoring system mainly takes stroke as the main outcome event rather than left atrial thrombosis.27
In patients with NVAF, LAT may occur when atrial fibrillation lasts longer than 48 hours, and SEC is an important marker of thrombosis.28 LAT and SEC were independently associated with thromboembolic events in patients with atrial fibrillation.29 Previous studies have shown that the average incidence of LAT in patients with NVAF is about 9.8%.30 Another study showed that the incidence of LAT and SEC in 481 NVAF patients was 12.47% and 11.43%, respectively.27 However, the incidence rates of SEC and LAT in this study were 4.45% and 7.76%, respectively, lower than those reported in previous studies. This difference between the results of the studies may be related to demographic differences in the included populations and potential selection bias in the studies. Therefore, this study was designed to evaluate patients at high risk of thromboembolism with low CHA2DS2-VASc scores, to provide references for clinical treatment to improve patient outcomes.
Residual cholesterol (RC) refers to the cholesterol content in all triglyceride-rich lipoproteins (TRL), including the sum of the cholesterol in fasting very low-density lipoprotein (VLDL) and intermediate density lipoprotein (IDL), and the cholesterol in non-fasting chylomicron.31 It is calculated by subtracting high-density lipoprotein cholesterol (HDL-C) and low-density lipoprotein cholesterol (LDL-C) from total cholesterol (TC).32 Recent studies have found that residual cholesterol (RC) is associated with an increased risk of cardiovascular diseases such as myocardial infarction, atrial fibrillation, and ischemic stroke.33–35 Results from a genetic study show that RC has a greater effect on cardiovascular risk than LDL-C.36 Compared with LDL-C, RC can carry more cholesterol and is more easily captured by macrophages, so RC has a stronger ability to cause arteriosclerosis.37 In addition, RC can promote the expression of cytokines interleukin and other inflammatory mediators, leading to chronic low-grade inflammation, and then promote the formation and progression of atherosclerosis.38 Another study showed that in the LDL-C quartile group, the highest group had a significantly lower cumulative incidence of atrial fibrillation than the lowest group.39 However, there is currently a cholesterol paradox, and there is still little evidence for a relationship between RC and thromboembolic risk in AF, so this study aimed to evaluate the relationship between RC and LAT/SEC in NVAF.
Atrial remodeling caused by inflammatory states is the basis for the occurrence and maintenance of atrial fibrillation.40 C-reactive protein (CRP), as a commonly used clinical indicator of inflammation, is associated with the occurrence of AF.41 Previous studies have shown that CRP is slightly elevated in patients with AF, which may reflect the chronic inflammatory state of the body to a certain extent, which can lead to the remodeling of the heart and blood vessels, and thus promote the occurrence of AF.42 In addition, previous studies have shown that elevated CRP increases the risk of atrial myocyte calcium influx.43 A retrospective study showed that IL-6, highly sensitive C-reactive protein (hs-CRP), and white blood cell count were positively correlated with the occurrence of AF in elderly patients.44 CRP, as an inflammatory marker, can predict the recurrence of AF after electrocardioversion.45
The Residual Cholesterol Inflammation Index (RCII), calculated by RC and hs-CRP, provides a comprehensive assessment of residual cholesterol and low-grade inflammation. Therefore, this study aimed to evaluate the predictive power of RCII for LAT/SEC in NVAF patients with low CHA2DS2-VASc scores. The study structure shows that RCII has a good predictive ability for LAT/SEC, the area under the curve is 0.746, and the optimal critical value is 4.46 (sensitivity 86.44%, specificity 54.48%). In this study, in addition to RCII, left atrial diameter (LAD) was also found to be a predictor of LAT/SEC. Changes in atrial structure, such as atrial cardiomyocyte hypertrophy and fibrosis, and atrial dilation, can lead to shortened action potential, reduced electrical connections between cells, and altered Ca2+ processing.46
This study showed a significant increase in LAD in the LAT/SEC group compared to the non-LAT/SEC group (39.50 (38.00–41.00) vs. 37.00 (33.00–39.00), P<0.001). After combining RCII and LAD, the ability of the CHA2DS2-VASc scores to predict LAT/SEC was significantly improved (AUC difference =285, Z=8.589, P<0.001). Therefore, in assessing the risk of thrombosis in NVAF patients with low CHA2DS2-VASc scores, when RCII≥4.46 and LAD ≥36.5 mm indicate an increased likelihood of LAT formation, TEE should be actively performed to detect intra-atrial thrombosis.
At present, there are few studies on the incidence of LAT/SEC in NVAF patients with low CHA2DS2-VASc scores. This study was the first to establish the predictive efficacy of RCII for the occurrence of LAT/SEC in patients with NVAF, with an optimal cut-off value of 4.46. In addition, left atrial enlargement was found to be an independent risk factor for LAT/SEC, which was consistent with previous studies. This study found that the combination of RCII, LAD, and CHA2DS2-VASc scores could significantly enhance the prediction efficiency of LAT/SEC. Therefore, RCII and LAD should be combined to assess thromboembolic risk in NVAF patients with low CHA2DS2-VASc scores. This helps to assess and identify patients with potential thrombosis as early as possible, and perform TEE examination promptly to improve patient outcomes.
Limitations
However, there are some limitations in this study. First of all, TEE is not routinely performed in all patients with NVAF, and TEE is mainly performed in patients undergoing ablation or cardioversion to rule out LAT/SEC, so there may be selection bias in patients enrolled in the study. In addition, the relevant clinical data collected in this study were limited; only LAD was used to evaluate left atrial structure, and no other indicators of left atrial function were collected. Therefore, elevated RCII may indicate higher biological risk, but its role in guiding anticoagulation strategies must be verified by future large-scale, multicenter prospective trials.
Conclusions
In conclusion, increased RCII and LAD were independent risk factors for LAT/SEC in NVAF patients with low CHA2DS2-VASc scores. CHA2DS2-VASc scores combined with RCII and LAD can significantly improve their prediction efficiency. Therefore, RCII, LAD, and CHA2DS2-VASc scores should be combined for comprehensive analysis in assessing thromboembolism risk in patients with NVAF.
Data Sharing Statement
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Ethical Approval and Consent to Participate
All methods were carried out in accordance with the Declaration of Helsinki. The Ethics Review Committee of the Second Hospital of Hebei Medical University approved the study, and written informed consents were obtained from all participants.
Funding
There is no funding to report.
Disclosure
The authors declare no competing interests in this work. This paper has been uploaded to ResearchSquare as a preprint: https://www.researchsquare.com/article/rs-7452942/v1.
References
1. Kornej J, Börschel CS, Benjamin EJ, et al. Epidemiology of atrial fibrillation in the 21st century: novel methods and new insights. Circ Res. 2020;127(1):4–11. doi:10.1161/CIRCRESAHA.120.316340
2. Jame S, Barnes G. Stroke and thromboembolism prevention in atrial fibrillation. Heart. 2020;106(1):10–17. doi:10.1136/heartjnl-2019-314898
3. Shi B, Suo R, Song W, et al. Plasma metabolomic characteristics of atrial fibrillation patients with spontaneous echo contrast. BMC Cardiovasc Disord. 2024;24(1):654. doi:10.1186/s12872-024-04306-y
4. Joglar JA, Chung MK, Armbruster AL, et al. ACC/AHA/ACCP/HRS guideline for the diagnosis and management of atrial fibrillation: a report of the American college of cardiology/american heart association joint committee on clinical practice guidelines. Circulation. 2024;149(1):e167. doi:10.1161/CIR.0000000000001193
5. Hao L, Chen X, Sun W, et al. Risk factors for silent brain infarction in nonvalvular atrial fibrillation patients with low cha 2 ds 2 -vasc score. Curr Neurovasc Res. 2025;21(4):503–510. doi:10.2174/0115672026354260241218115435
6. Kim YK, Lee SR, Choi EK, et al. Risk of death from various causes according to prevalent atrial fibrillation: a nationwide population-based study. J Korean Med Sci. 2024;39(47):e306. doi:10.3346/jkms.2024.39.e306
7. Ouyang X, Tang X, Peng L, et al. Remnant cholesterol and new-onset atrial fibrillation: the atherosclerosis risk in communities study. Heart Rhythm. 2024;S1547-5271(24):03456–3458. doi:10.1016/j.hrthm.2024.10.030
8. Zhang K, Qi X, Zhu F, et al. Remnant cholesterol is associated with cardiovascular mortality. Front Cardiovasc Med. 2022;9:984711. doi:10.3389/fcvm.2022.984711
9. Navarese EP, Vine D, Proctor S, et al. Independent causal effect of remnant cholesterol on atherosclerotic cardiovascular outcomes: a mendelian randomization study. Arterioscler Thromb Vasc Biol. 2023;43(9):e373–e380. doi:10.1161/ATVBAHA.123.319297
10. Li ZH, Hao QY, Zeng YH, et al. Remnant cholesterol and the risk of aortic valve calcium progression: insights from the Mesa study. Cardiovasc Diabetol. 2024;23(1):20. doi:10.1186/s12933-023-02081-2
11. Guo DC, Gao JW, Wang X, et al. Remnant cholesterol and risk of incident hypertension: a population-based prospective cohort study. Hypertens Res. 2024;47(5):1157–1166. doi:10.1038/s41440-023-01558-7
12. Van Diepen JA, Berbée JF, Havekes LM, et al. Interactions between inflammation and lipid metabolism: relevance for efficacy of anti-inflammatory drugs in the treatment of atherosclerosis. Atherosclerosis. 2013;228(2):306–315. doi:10.1016/j.atherosclerosis
13. Chait A, Ginsberg HN, Vaisar T, et al. Remnants of the triglyceride-rich lipoproteins, diabetes, and cardiovascular disease. Diabetes. 2020;69(4):508–516. doi:10.2337/dbi19-0007
14. Wadström BN, Pedersen KM, Wulff AB, et al. Elevated remnant cholesterol, plasma triglycerides, and cardiovascular and non-cardiovascular mortality. Eur Heart J. 2023;44(16):1432–1445. doi:10.1093/eurheartj/ehac822
15. Small AM, Pournamdari A, Melloni GEM, et al. Lipoprotein(a), C-reactive protein, and cardiovascular risk in primary and secondary prevention populations. JAMA Cardiol. 2024;9(4):385–391. doi:10.1001/jamacardio.2023.5605
16. Chen J, Wu Q, Liu H, et al. Predictive value of remnant cholesterol inflammatory index for stroke risk: evidence from the China health and Retirement Longitudinal study. J Adv Res. 2024;2024. doi:10.1016/j.jare.2024.12.015
17. Lang RM, Badano LP, Mor-Avi V, et al. Recommendations for cardiac chamber quantification by echocardiography in adults: an update from the American Society of Echocardiography and the European Association of Cardiovascular Imaging. Eur Heart J Cardiovasc Imaging. 2015;16(3):233–270. doi:10.1093/ehjci/jev014
18. Hindricks G, Potpara T, Dagres N, et al. Corrigendum to: 2020 ESC Guidelines for the diagnosis and management of atrial fibrillation developed in collaboration with the European Association for Cardio-Thoracic Surgery (EACTS): the Task Force for the diagnosis and management of atrial fibrillation of the European Society of Cardiology (ESC) Developed with the special contribution of the European Heart Rhythm Association (EHRA) of the ESC. Eur Heart J. 2021;42(40):4194. doi:10.1093/eurheartj/ehab648
19. Koca V, Bozat T, Akkaya V, et al. Left atrial thrombus detection with multiplane transesophageal echocardiography: an echocardiographic study with surgical verification. J Heart Valve Dis. 1999;8(1):63–66.
20. Black IW, Hopkins AP, Lee LC, et al. Left atrial spontaneous echo contrast: a clinical and echocardiographic analysis. J Am Coll Cardiol. 1991;18(2):398–404. doi:10.1016/0735-1097(91)90592-w
21. Yildirim M, Milles BR, Hund H, et al. Outcomes and disease management in patients with atrial fibrillation ≥80 years: data from a consecutive 11-year real-world registry. J Am Heart Assoc. 2025;14(4):e036832. doi:10.1161/JAHA.124.036832
22. Li Z, Pan L, Deng Y, et al. Development and validation of a nomogram for estimation of left atrial thrombus or spontaneous echo contrast risk in non-valvular atrial fibrillation patients with low to borderline cha2ds2-vasc score. Int J Gen Med. 2022;15:7329–7339. doi:10.2147/IJGM.S384519
23. Angebrandt Belošević P, Šmalcelj A, Kos N, et al. Left ventricular ejection fraction can predict atrial thrombosis even in non-high-risk individuals with atrial fibrillation. J Clin Med. 2022;11(14):3965. doi:10.3390/jcm11143965
24. Nishimura M, Yano M, Yokota A, et al. Analysis of risk factors for left atrial appendage thrombus formation in patients with atrial fibrillation. Gen Thorac Cardiovasc Surg. doi:10.1007/s11748-025-02228-w
25. Yan S, Li Q, Xia Z, et al. Risk factors of thromboembolism in nonvalvular atrial fibrillation patients with low CHA2DS2-VASc score. Medicine. 2019;98(8):e14549. doi:10.1097/MD.0000000000014549
26. Xie X, Li T. Anticoagulation for atrial fibrillation patients with the CHA2DS2-VASc score=1 (beyond sex). Acta Cardiol. 2021;76(3):258–264. doi:10.1080/00015385.2020.1720197
27. Kamili K, Zheng T, Luo C, et al. Predictive value of lipoprotein(a) for left atrial thrombus or spontaneous echo contrast in non-valvular atrial fibrillation patients with low CHA2DS2-VASc scores: a cross-sectional study. Lipids Health Dis. 2024;23(1):22. doi:10.1186/s12944-023-01990-1
28. Kim YG, Shim J, Oh SK, et al. Risk factors for ischemic stroke in atrial fibrillation patients undergoing radiofrequency catheter ablation. Sci Rep. 2019;9(1):7051. doi:10.1038/s41598-019-43566-z
29. Yoo J, Song D, Baek JH, et al. Poor outcome of stroke patients with atrial fibrillation in the presence of coexisting spontaneous echo contrast. Stroke. 2016;47(7):1920–1922. doi:10.1161/STROKEAHA.116.013351
30. Di Minno MN, Ambrosino P, Dello Russo A, et al. Prevalence of left atrial thrombus in patients with non-valvular atrial fibrillation. A systematic review and meta-analysis of the literature. Thromb Haemost. 2016;115(3):663–677. doi:10.1160/TH15-07-0532
31. Makover ME, Surma S, Banach M, et al. Eliminating atherosclerotic cardiovascular disease residual risk. Eur Heart J. 2023;44(45):4731–4733. doi:10.1093/eurheartj/ehad446
32. Mach F, Baigent C, Catapano AL, et al. ESC/EAS Guidelines for the management of dyslipidaemias: lipid modification to reduce cardiovascular risk. Eur Heart J. 2020;41(1):111–188. doi:10.1093/eurheartj/ehz455
33. Li W, Huang Z, Fang W, et al. Remnant Cholesterol Variability and Incident Ischemic Stroke in the General Population. Stroke. 2022;53(6):1934–1941. doi:10.1161/STROKEAHA.121.037756
34. Jørgensen AB, Frikke-Schmidt R, West AS, et al. Genetically elevated non-fasting triglycerides and calculated remnant cholesterol as causal risk factors for myocardial infarction. Eur Heart J. 2013;34(24):1826–1833. doi:10.1093/eurheartj/ehs431
35. Zhong L, Xie B, Wang HL, et al. Causal association between remnant cholesterol level and risk of cardiovascular diseases: a bidirectional two sample mendelian randomization study. Sci Rep. 2024;14(1):27038. doi:10.1038/s41598-024-78610-0
36. Björnson E, Adiels M, Taskinen MR, et al. Triglyceride-rich lipoprotein remnants, low-density lipoproteins, and risk of coronary heart disease: a UK Biobank study. Eur Heart J. 2023;44(39):4186–4195. doi:10.1093/eurheartj/ehad337
37. Castañer O, Pintó X, Subirana I, et al. Remnant cholesterol, not ldl cholesterol, is associated with incident cardiovascular disease. J Am Coll Cardiol. 2020;76(23):2712–2724. doi:10.1016/j.jacc.2020.10.008
38. Baratta F, Cocomello N, Coronati M, et al. Cholesterol remnants, triglyceride-rich lipoproteins and cardiovascular risk. Int J Mol Sci. 2023;24(5):4268. doi:10.3390/ijms24054268
39. Li L, Wang C, Ye Z, et al. Association between remnant cholesterol and risk of incident atrial fibrillation: population-based evidence from a large-scale prospective cohort study. J Am Heart Assoc. 2024;13(10):e033840. doi:10.1161/JAHA.123.033840
40. Galvão Braga C, Ramos V, Vieira C, et al. New-onset atrial fibrillation during acute coronary syndromes: predictors and prognosis. Rev Port Cardiol. 2014;33(5):281–287. doi:10.1016/j.repc.2013.10.017
41. Sun GZ, Guo L, Wang J, et al. Association between hyperuricemia and atrial fibrillation in rural China: a cross-sectional study. BMC Cardiovasc Disord. 2015;15:98. doi:10.1186/s12872-015-0089-y
42. Chung MK, Martin DO, Sprecher D, et al. C-reactive protein elevation in patients with atrial arrhythmias: inflammatory mechanisms and persistence of atrial fibrillation. Circulation. 2001;104(24):2886–2891. doi:10.1161/hc4901.101760
43. Ding M, Wennberg A, Gigante B, et al. Lipid levels in midlife and risk of atrial fibrillation over 3 decades-Experience from the Swedish AMORIS cohort: a cohort study. PLoS Med. 2022;19(8):e1004044. doi:10.1371/journal.pmed.1004044
44. Shitole SG, Heckbert SR, Marcus GM, et al. Assessment of inflammatory biomarkers and incident atrial fibrillation in older adults. J Am Heart Assoc. 2024;13(24):e035710. doi:10.1161/JAHA.124.035710
45. Sonsöz MR, Demirtaş İ, Canbolat O, et al. High-density lipoprotein cholesterol to c-reactive protein ratio predicts atrial fibrillation recurrence after electrical cardioversion. Lipids. 2024;60:77–84. doi:10.1002/lipd.12423
46. Zhou X, SC D Jr. Evidence for inflammation as a driver of atrial fibrillation. Front Cardiovasc Med. 2020;7:62. doi:10.3389/fcvm.2020.00062
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Development and Validation of a Nomogram for Estimation of Left Atrial Thrombus or Spontaneous Echo Contrast Risk in Non-Valvular Atrial Fibrillation Patients with Low to Borderline CHA2DS2-VASc Score
Li Z, Pan L, Deng Y, Liu Q, Hidru T, Liu F, Li C, Cong T, Yang X, Xia Y
International Journal of General Medicine 2022, 15:7329-7339
Published Date: 18 September 2022
Predictive Value of Uric Acid-to-Albumin Ratio for Left Atrial Thrombus or Spontaneous Echo Contrast in Patients with Non-Valvular Atrial Fibrillation
Meng X, Wen Y, Wang X, Hidru TH, Tang Y, Xia Y, Yang X, Gao L
Journal of Inflammation Research 2026, 19:608168
Published Date: 13 May 2026