Back to Journals » Open Access Emergency Medicine » Volume 18
Predictive Value of Systemic Immune-Inflammation Index Combined with D-Dimer Levels and Injury Severity Score for the Prognosis of Patients with Multiple Injuries: A Retrospective Analysis
Received 24 June 2025
Accepted for publication 18 February 2026
Published 10 March 2026 Volume 2026:18 549167
DOI https://doi.org/10.2147/OAEM.S549167
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Charles V Pollack
Xinlong Du,1 Yongming He,1 Xing Liu2
1Department of Emergency Medicine, Shenzhen Longhua District Central Hospital, Shenzhen, Guangdong, 518110, People’s Republic of China; 2Department of Emergency Medicine, The Second People’s Hospital of Futian District Shenzhen, Shenzhen, Guangdong, 518049, People’s Republic of China
Correspondence: Xing Liu, Department of Emergency Medicine, The Second People’s Hospital of Futian District Shenzhen, 27 Zhongkang Road, Shangmeilin, Futian, Shenzhen, Guangdong, 518049, People’s Republic of China, Email [email protected]
Background: The prognosis of patients with multiple injuries (MI) remains challenging to predict accurately due to the complexity and heterogeneity of trauma. Traditional scoring systems or single biomarkers often have limitations in terms of sensitivity or specificity.
Purpose: The objective of the present study was to investigate the predictive value of combining the systemic immune-inflammation index (SII), D-dimer (D-D) and injury severity score (ISS) for evaluating the prognosis of patients with MI.
Patients and Methods: A total of 142 patients with MI admitted to the Emergency Department of Shenzhen Longhua District Central Hospital (Shenzhen, China) from January 2019 to December 2023 were retrospectively analyzed. Patients were then divided into survival (n=102) and non-survival (n=40) groups according to their survival status on postoperative day 28. Logistic regression analysis was performed on indicators with significant differences between the two groups to identify prognostic factors in severe MI. Data were retrospectively analyzed using SPSS 26.0 software. In addition, receiver operating characteristic (ROC) curves were plotted to assess the predictive value of the combined SII, D-D and ISS.
Results: The median SII was found to be 340.11 (182.72– 578.31) in the survival group and 849.93 (300.83– 1034.14) in the non-survival group, yielding a significant difference (P< 0.001). Logistic regression indicated that SII, D-D and ISS at admission were independent prognostic factors for mortality. Furthermore, SII, D-D, ISS and their combination showed predictive value [area under the curve (AUC) > 0.5] for 28-day mortality, with the combination exhibiting the highest predictive accuracy. Based on the optimal ROC cut-off values (308.8), patients were divided into groups with SII ≤ 308.8 (n=58) and SII > 308.8 (n=84), with significantly lower mortality in the former group (P< 0.05). Similarly, patients were categorized into D-D ≤ 2.35 (n=117) and D-D > 2.35 (n=25) groups, with significantly lower mortality in the former group (P< 0.05). In conclusion, each indicator demonstrated prognostic significance (AUC > 0.5), with the combined model achieving the highest predictive accuracy (AUC =0.969).
Conclusion: The integrated indicators offered improved predictive performance compared with individual measures for MI, providing a clinically valuable reference for patient management.
Keywords: multiple injuries, systemic immune-inflammation index, D-dimer, injury severity score, prognosis
Introduction
Trauma is recognized as a major public health issue worldwide,1 with traffic accidents being the leading cause of mortality among individuals aged 15–29 years globally, accounting for ~1.3 million cases of mortality and 50 million injuries annually.2 Multiple injuries (MI), defined as serious injuries involving two or more anatomical locations or organs caused by a single event,3 is characterized by rapid clinical deterioration, high fatality rates and increased susceptibility to infection compared with single-system injuries. MI can trigger systemic inflammatory response (SIR) syndrome (SIRS) due to the marked release of inflammatory factors following the activation of the SIR.4 Prognostic assessment using simple and effective clinical indicators during early hospitalization, combined with timely interventions, can notably improve survival rates in patients with severe MI.5
Although traditional tools, such as the injury severity score (ISS), a scoring system that quantifies overall trauma severity by summing the squares of the three highest Abbreviated Injury Scale (AIS) grades from three different body regions,6 can be used to assess anatomical injury severity, they lack the capability to dynamically monitor immune-inflammatory reactions, which represent a key pathological link influencing prognosis.7 Given the strong association between complex immune-inflammatory responses and patient outcomes,8 identifying reliable indices that can quantify this pathophysiological process has become a notable research objective. Recently, the systemic immune-inflammation index (SII), integrating neutrophil, lymphocyte and platelet counts, has demonstrated unique value in injury-related immune monitoring.9 Proposed by Hu et al,10 the SII is calculated based on peripheral neutrophil (N), platelet (P) and lymphocyte (L) counts, using the formula (P x N)/L The SII serves as a comprehensive indicator of systemic immune-inflammatory status and can be utilized to reflect the clinical progression or deterioration through the collective action of multiple immune-inflammatory cells.11 It demonstrates superior predictive capability for trauma-related mortality and complications compared with the neutrophil-to-lymphocyte ratio and platelet-to-lymphocyte ratio, since it encompasses three key immune response pathways.12 Higher levels of SII in patients with trauma are an indication of the complex interaction between pro- and anti-inflammatory responses, which forms the key issue in the pathophysiology of secondary organ injury. In particular, higher SII values may indicate greater severity of inflammation and poorer prognosis.13,14 Due to its accessibility and cost-effectiveness, the SII offers valuable guidance for therapeutic strategies and long-term outcomes.
ISS has been recognized as the gold standard for trauma assessment, whereas SII and D-dimer levels (D-D) have been extensively studied as markers of systemic inflammation and coagulation activation,15,16 respectively. However, to the best of our knowledge, studies dynamically integrating these three parameters into a comprehensive predictive model for the early and accurate prediction of 28-day mortality remain limited. The 28-day mortality is widely adopted in critical care and trauma research as it captures the peak period of post-traumatic complications (such as sepsis and multiple organ dysfunction) while ensuring a stable outcome assessment with minimal loss to follow-up, thereby allowing for meaningful comparisons with existing literature.17 Therefore, the present study aims to systematically assess the predictive efficacy of a combined SII, D-D and ISS model for 28-day mortality in patients with MI. Through receiver operating characteristic (ROC) curve analysis, optimal cut-off values for SII and D-D in predicting mortality were calculated, thereby providing clinicians with a quantitative tool for rapidly identifying patients at high-risk of 28-day mortality. Specifically, the clinical data of 142 patients were analyzed, aiming to obtain a prognostic indicator that is more convenient compared with traditional assessment indicators.
Materials and Methods
Patients
Clinical data from 142 patients with MI [mean age, 43.29±16.39 years; 116 male patients (81.7%) and 26 female patients (18.3%)] admitted to the Emergency Department of Shenzhen Longhua District Central Hospital (Shenzhen, China) between January 2019 and December 2023 were retrospectively analyzed.
The inclusion criteria were the following: i) Primary injury; ii) injury-to-admission time <24 h; iii) >14 years of age; iv) clinical confirmation of MI; and v) complete clinical records. The exclusion criteria were the following: i) Patients ≤14 years of age; ii) death upon admission; and iii) history of chronic diseases (including cardiac, cerebral and renal diseases, in addition to malignant tumors). The study protocol was approved by the Ethics Committee of Shenzhen Longhua District Central Hospital (Shenzhen, China; approval no. 2025–062-01).
Methods Upon Admission to the Emergency Resuscitation Room
Appropriate resuscitative measures were immediately performed, which included tracheal intubation, cardiopulmonary resuscitation, defibrillation, volume expansion, hemostasis, bandaging and immobilization to maintain vital signs. Patient information was collected from electronic medical records.
Routine blood tests, biochemical tests and coagulation tests were conducted. Blood samples were drawn at the time of initial presentation to the emergency department, prior to any major surgical intervention or blood transfusion. Routine blood tests were performed using a Mindray BC-7500 (Shenzhen Mindray Bio-Medical Electronics Co., Ltd.) fully automatic hematology analyzer. Biochemical analyses were conducted using a Johnson & Johnson VITROS-5600 automated biochemical analyzer and coagulation tests were performed using a Sysmex CICO (Sysmex America, Inc.) automated coagulation analyzer.
The 142 patients were categorized into survival (n=102) and death (n=40) groups based on their survival status on postoperative day 28. Differences in clinical data between groups were retrospectively analyzed, with indicators yielding statistically significant differences undergoing further evaluation.
Statistical Analysis
Statistical analyses were performed using SPSS 26.0 software (IBM, Corp)., Categorical variables (such as sex) are expressed in counts. Continuous variables that conform to the normal distribution are expressed as the mean ± standard deviation [such as hemoglobin (HGB)]. For most continuous variables that do not conform to the normal distribution, the interquartile range is used to describe their central tendency and degree of dispersion. Data with a non-normal distribution are presented as median (first quartile, third quartile) and were compared using the Mann–Whitney U-test. The comparison of HGB between the two groups was conducted using an unpaired t-test. Categorical data are presented as n (%). Group comparisons were performed using the χ2-test or Fisher’s exact test when expected frequencies were <5 (for example, for the comparison of 28-day survival rates). To construct the cumulative predictive model, multivariate binary logistic regression was conducted using SII, D-D and ISS as continuous independent variables. A linear predictor score derived from the model as regression coefficients were used to predict a 28-day mortality log-odds value of each patient. The combination predictor (combined score) formula was as follows: Combined score = β0 + β1 x SII + β2 x D-D + β3 x ISS. In this formula, β0 is the intercept, whereas β1, β2 and β3 are the regression coefficients of the individual variables. ROC analysis was used to evaluate the predictive performance of the combined model, where the area under the curve (AUC) was compared with that of the individual indicators. The results of this ROC analysis are presented in Figure 1. Plots of ROC curves were made to assess the prognostic capabilities of SII, D-D, ISS and the combined model (integrating SII, D-D and ISS), where AUC with the 95% CI was calculated for each indicator. P<0.05 was considered to indicate a statistically significant difference. The DeLong test of paired ROC curves was used to compare the joint model and individual indicators to evaluate the correctness of the prediction of the joint model.
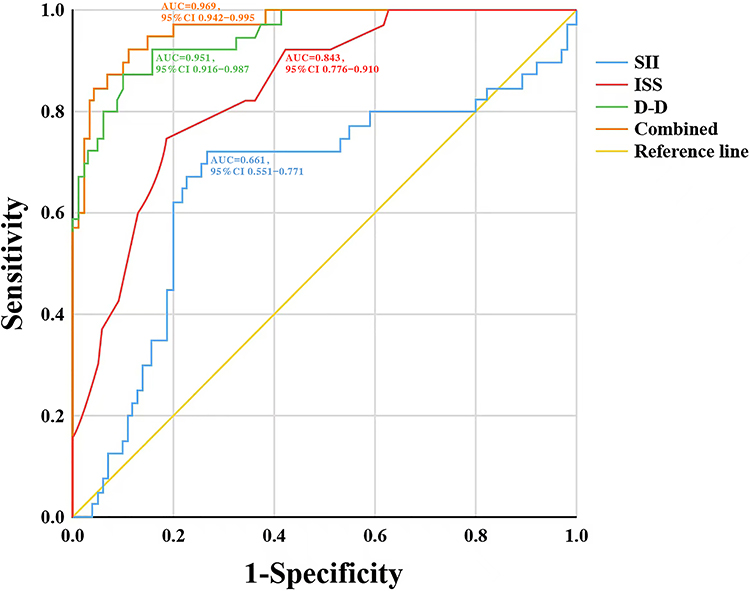 |
Figure 1 Predictive ability of SII, D-D, ISS and their combination for survival in patients with multiple injuries. Abbreviations: SII, systemic immune-inflammation index; D-D, D-dimer; ISS, injury severity score. |
Results
Comparison of General Patient Characteristics Between the Two Groups
A total of 142 patients were included in the present study, which were divided into survivor (n=102) and non-survivor (n=40) groups according to 28-day outcomes. The primary injury causes were traffic accidents (65 cases; 45.77%), high falls (37 cases; 26.05%) and low falls (20 cases; 14.08%). The distribution of injury mechanisms was compared between the survivor and non-survivor groups. There was no significant difference in survival rate among patients with different injury mechanisms (P>0.05; χ2 test; Table 1). Other injury causes included stab wounds (13 cases; 9.15%) and blunt injuries (7 cases; 4.93%).
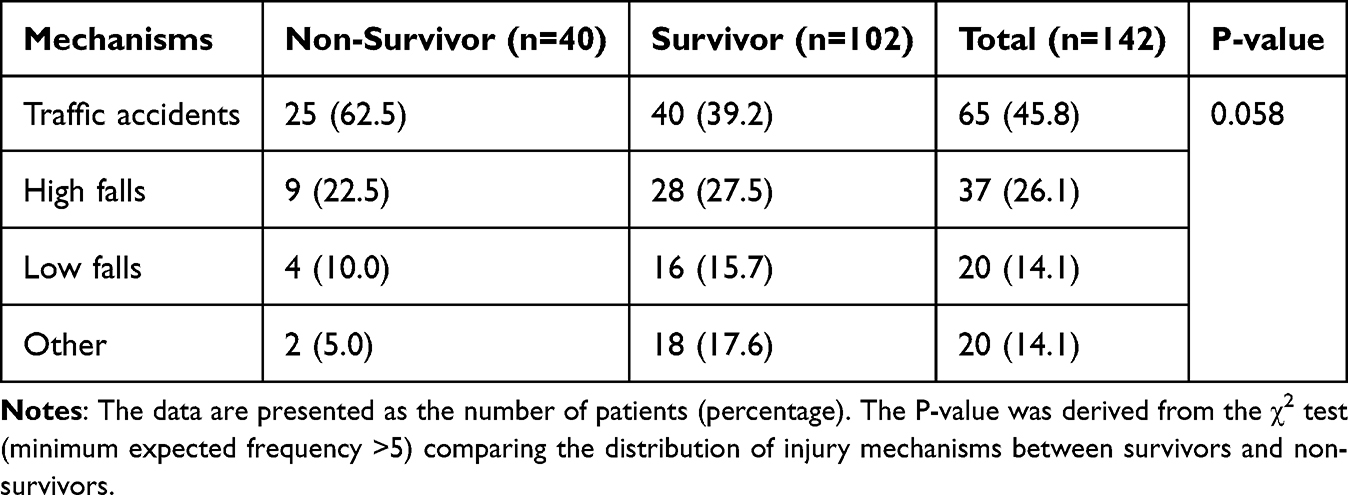 |
Table 1 Comparison of Patients with Different Injury Mechanisms |
No significant differences were found between groups regarding sex, age, white blood cell count, platelet count, total protein, neutrophils, lymphocytes, creatinine, systolic blood pressure, diastolic blood pressure and mean arterial pressure. By contrast, significant differences were observed for HGB, D-D, ISS, heart rate, respiratory rate and SII (all P<0.05; Table 2). The median SII was significantly higher in the non-survivor group [849.93 (300.83, 1034.14)] than in the survivor group [340.11 (182.72, 578.31); P<0.001] The median HGB level was 116.29±29.49 g/l in the non-survivor group and 129.73±23.22 g/l in the survivor group, where the HGB levels were significantly lower in the non-survivor group (P<0.05). The median D-D level was 28.07 µg/mL (18.03, 34.44 µg/mL) in the non-survivor group and 6.9 µg/mL (3.88, 10.98 µg/mL) in the survivor group, where the D-D levels were significantly lower in survivors (P<0.001). The median ISS score was 41.00 (34.25, 50.00) in the non-survivor group and 26.00 (20.00, 34.00) in the survivor group, where the ISS score was significantly lower in survivors (P<0.001). The median heart rate was 132.00 bpm (124.25, 137.00 bpm) in the non-survivor group and 114.00 bpm (104.50, 124.25 bpm) in the survivor group, where the heart rate was significantly lower in survivors (P<0.001). The median respiration was 29.00 bpm (25.00, 31.00 bpm) in the non-survivor group and 22.00 bpm (20.00–24.25 bpm) in the survivor group, where the respiration was significantly lower in survivors (P<0.001).
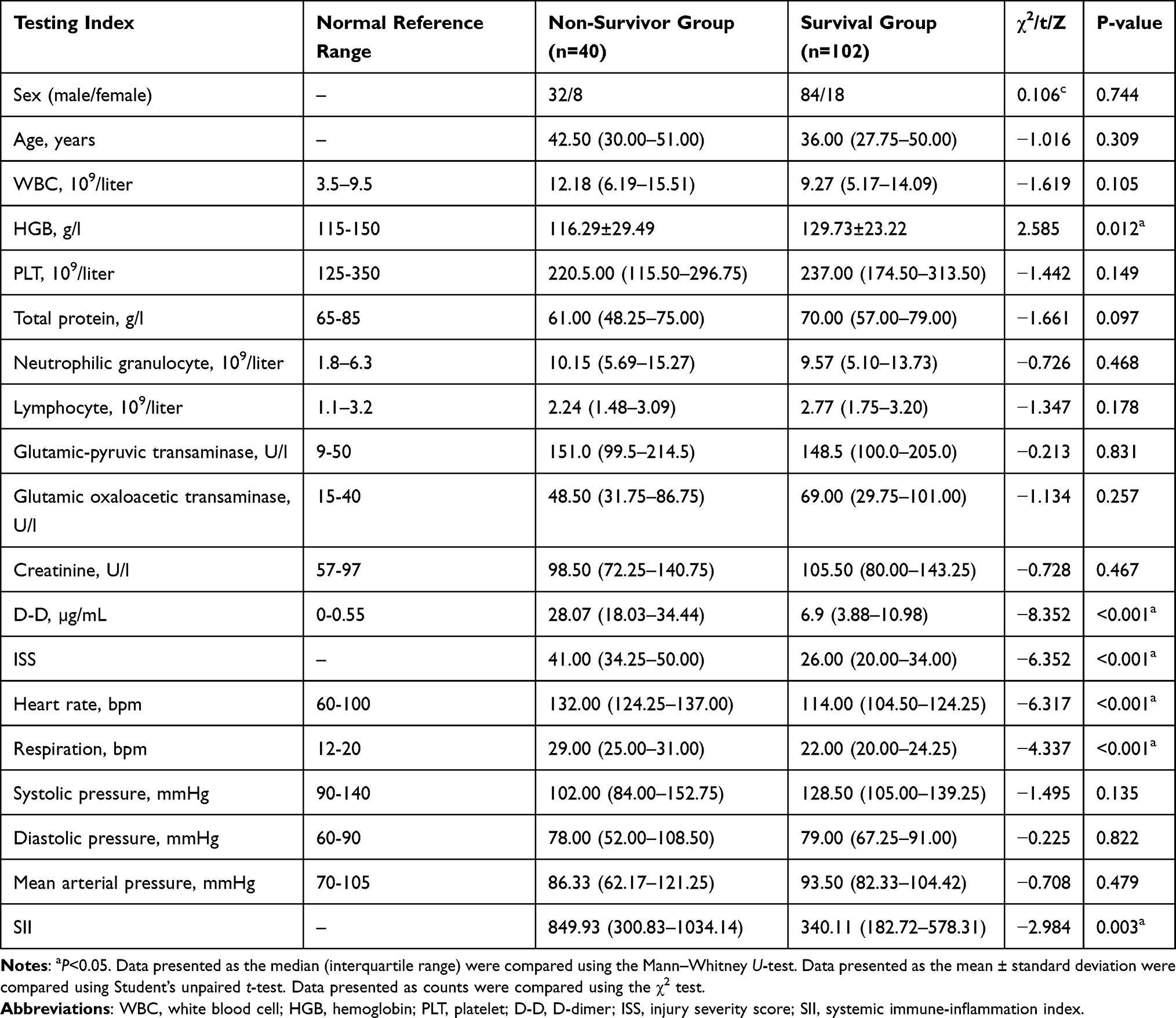 |
Table 2 Comparison of General Characteristics Between Survival and Non-Survivor Groups in Patients with Multiple Injuries |
Factors Influencing Prognosis in Patients with Severe MI (ISS ≥16)
Logistic regression analysis was performed on variables with significant differences between groups that are pathophysiological relevant. The results indicated that admission levels of SII (P=0.036), D-D (P<0.001) and ISS (P=0.008) were independent predictors of 28-day mortality in these patients (Table 3).
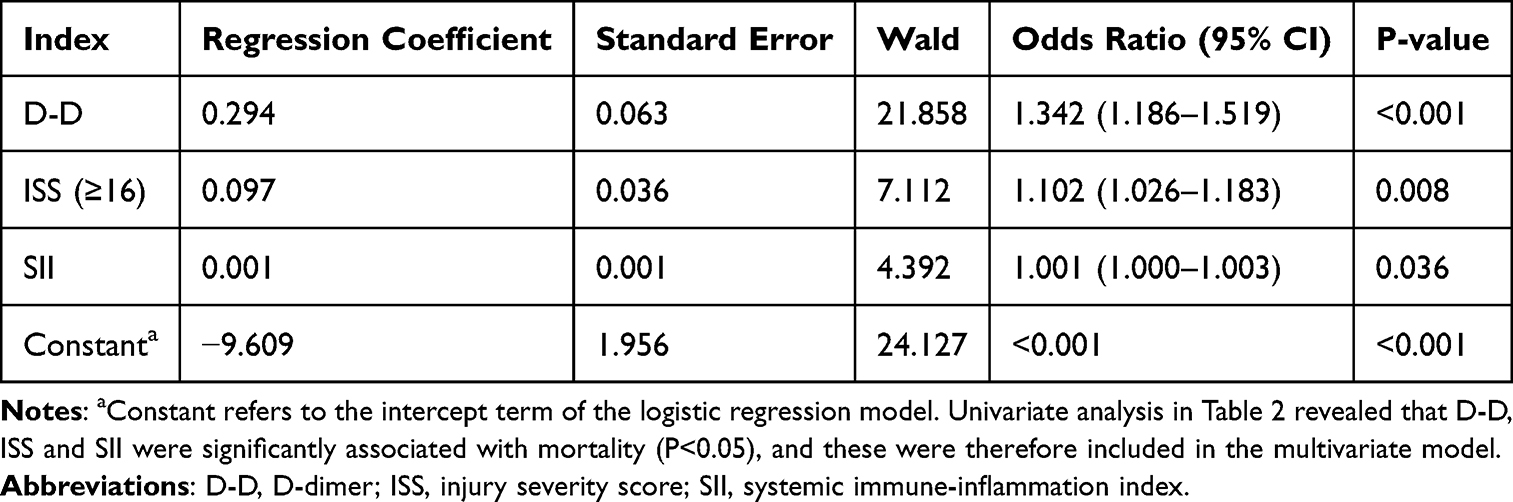 |
Table 3 Multivariate Logistic Regression Analysis of Factors Influencing Mortality Outcomes |
Predictive Value of SII, D-D, ISS and Their Combination in MI Prognosis
ROC curves and AUC values were calculated to compare the predictive abilities of SII, D-D, ISS and their combination for 28-day mortality. Based on optimal ROC cut-off values, patients were classified into groups: SII ≤308.8 or SII >308.8; and D-D ≤2.35 or D-D >2.35. The 28-day mortality rates were compared between these groups.
The results showed that the AUC of D-D levels was 0.951, the AUC of ISS was 0.843, the AUC of SII was 0.661 and the AUC of the combination was 0.969, and all indicators had prognostic predictive value (AUC>0.5), with their combination demonstrating the highest predictive accuracy (Figure 1; Table 4).
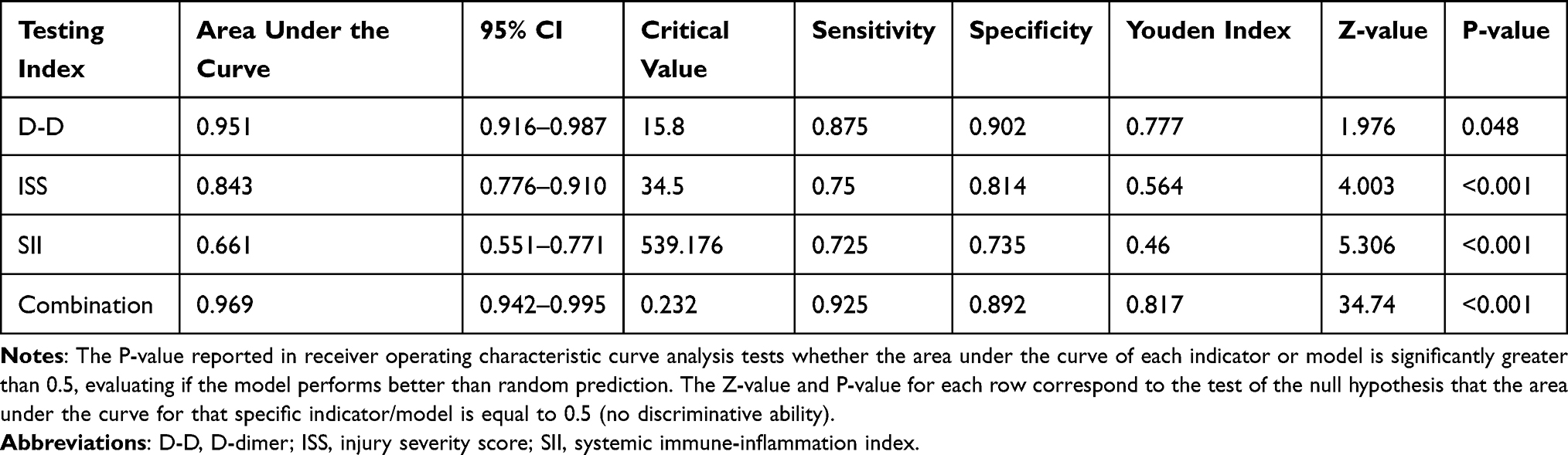 |
Table 4 Predictive Value of SII, D-D and ISS for Mortality in Patients with Multiple Injuries |
Comparison of Mortality Among Patients with MI Grouped by SII Levels
ROC analysis revealed an optimal SII cut-off value of 308.8. Therefore, patients were divided into two groups (SII ≤308.8 and SII >308.8). The group with SII ≤308.8 had significantly lower D-D levels (P=0.0244) and a lower 28-day mortality rate (P=0.0267) compared with the group with an SII >308.8 (Table 5).
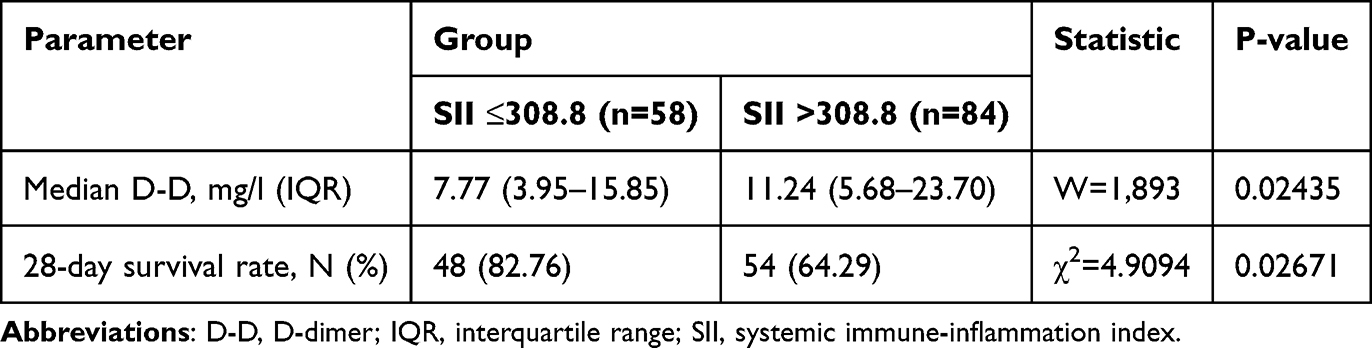 |
Table 5 Mortality Comparison Between Groups with Different SII Levels |
Comparison of Mortality Among Patients with MI Grouped by D-D Levels
ROC curve analysis indicated an optimal D-D cut-off value of 2.35, resulting in the division of patients into the D-D ≤2.35 (n=117) and D-D >2.35 (n=25) groups. The group with D-D ≤2.35 had a significantly lower 28-day mortality rate (P<0.001). Similarly, SII values in the D-D ≤2.35 group were lower (P<0.001; Table 6).
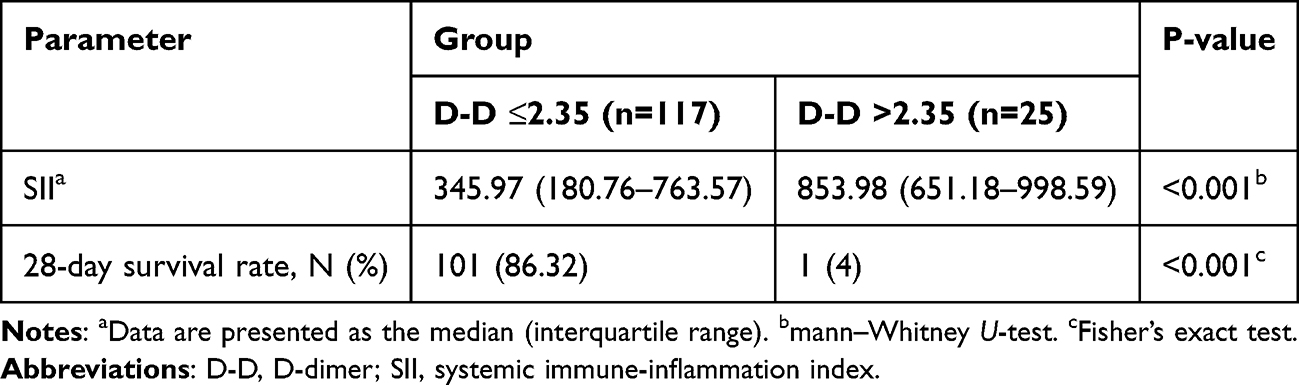 |
Table 6 Mortality Comparison Between Groups with Different D-D Levels |
Discussion
In the present retrospective study, it was demonstrated that the independent variables of 28-day mortality in patients with MI were the admission level of SII >308.8, D-D >2.35 µg/mL and the ISS score (analyzed as a continuous variable). The model that combined these three parameters showed improved predictive accuracy compared with each of the individual variables, supporting the concept of synergetic importance for assessing inflammatory, coagulative and anatomical injury in the initial prognostic model.18,19
Early assessment of injury severity, prompt transport and appropriate interventions effectively can reduce mortality and disability rates in patients with MI, improving prognosis.20 Although medical advances and trauma center systems have enhanced MI management, mortality and disability rates remain high due to injury complexity and rapid progression.21 Treatment outcomes for MI reflect the comprehensive capabilities of trauma centers. Given the rapidly changing condition of patients with MI, real-time risk assessment using accessible tools is essential.
Immune-inflammatory dysregulation is a central mechanism of secondary injury and markedly influences prognosis in patients with MI, necessitating accurate evaluation.22 Among the inflammatory markers, SII has garnered attention due to its simple calculation method, low cost and ability to reflect inflammatory activation and immunosuppressive states simultaneously.23 A previous study has indicated that SII is associated with surgical trauma severity in elderly patients with hip-fracture, as evidenced by its significant positive association with increased risks of 30-day and 1-year all-cause mortality (adjusted hazard ratio, 1.065; 95% CI, 1.044–1.087; P<0.001).24 Logistic regression analysis in the present study suggested that SII is an independent risk factor for predicting 28-day mortality in patients with MI, with higher values indicating increased mortality risk. The prognostic ability of SII may involve the following mechanisms: i) SII integrates multiple immune processes involving neutrophils, lymphocytes and platelets. Neutrophils, the first inflammatory cell types to activate after injury, release reactive oxygen species and proteases, causing direct tissue damage, where prolonged elevation of neutrophils indicates an excessive inflammatory response.25 Lymphocytes reflect compensatory anti-inflammatory responses associated with immunosuppression and secondary infection risk,26 where increased lymphocyte apoptosis after injury reduces lymphocyte counts. Platelets serve as coagulation carriers and inflammation modulators27 by releasing mediators, such as platelet factor 4 and TGF-β,28 influencing the organ injury-repair balance.29 ii) SII dynamically reflects the transition from excessive inflammation to immunosuppression following MI.30 During the early post-injury stages (24–72 h), increased neutrophils and decreased lymphocytes markedly elevate SII, indicating SIRS risk. In the latter stages (3–7 days), persistently elevated SII reflects an immunosuppressive state associated with sepsis and multiple organ dysfunction syndrome. iii) SII is associated with molecular mediators of organ damage, such that higher SII values are positively associated with endothelial cell injury31 and mitochondrial DNA release,32 reflecting microcirculatory disturbances.
Accumulating evidence increasingly supports the association between elevated plasma D-D levels and injury severity.33 A recent study involving patients with MI demonstrated notably higher D-D levels upon admission in patients who were severely injured compared with patients who were mildly injured. Furthermore, non-survivors had markedly higher D-D levels compared with those in survivors, likely reflecting coagulopathy induced by inflammatory stress.34 Lee et al35 previously reported that, compared with patients with D-D levels ≤34.53 mg/l, those with D-D levels >34.53 mg/l within 24 h after injury (trauma mechanisms such as drowning or hanging) had a 1.033-fold increased risk of 28-day mortality. Results from the present study similarly indicated increased mortality risk when admission D-D levels were >2.35 µg/mL, consistent with previous findings. Notably, the optimal D-dimer cut-off value identified in the present study (2.35 µg/mL) was markedly lower than the threshold of 34.53 mg/l associated with mortality in the study by Lee et al.35
ISS is a commonly used injury scoring system, with higher scores indicating greater injury severity and increased mortality risk.36 Liu et al37 reported that ISS effectively predicted mortality in elderly patients with trauma (AUC=0.74; 95% CI, 0.71–0.79). Another previous study demonstrated that Trauma and Injury Severity Score and ISS reliably predicted outcomes in pediatric patients with traumatic brain injury, assisting clinicians in risk-adjusted decision-making.38 In the present study, ISS was found to be an independent predictor of 28-day mortality in patients with MI. Higher ISS scores are associated with increased mortality, likely due to the objective quantification of anatomical injury severity and systemic pathophysiological disturbances. However, ISS has limitations when predicting prognosis. It neglects physiological factors, such as shock or low Glasgow Coma Scale scores, which markedly impacts patient outcomes.39 Additionally, ISS underestimates isolated severe injuries (such as high AIS-score injuries confined to a single body region, such as the head, chest or abdomen), despite higher actual mortality compared with patients with multiple-region injuries and identical ISS scores.40 Future studies should address these limitations by combining ISS with physiological scoring systems to improve prediction of coagulopathy and shock or by using alternative metrics, such as the New Injury Severity Score, which, despite greater sensitivity for single-region injuries,41 is less frequently used clinically, primarily due to the entrenched historical use and global standardization of the ISS for trauma triage, registry reporting and outcomes research, which creates a high barrier for the adoption of modified scales.
The association of SII and D-D with mortality in the present study supports the close interaction of inflammatory and coagulation pathways in multiple trauma.42 It is worth noting that the ISS was not included in the comparative analysis as the established cutoff of ISS ≥16 serves as a well‐validated threshold for identifying patients with elevated mortality risk in trauma populations.43 Thus, further comparative analysis of ISS was not performed in this context. Tissue injuries generated due to trauma trigger both innate immunity and the coagulation cascade, causing a pro-thrombotic state, which is marked by increased levels of D-D.44 In addition, the stimulation of immune cells and endothelial dysfunction is mediated by systemic inflammation that is indicated by elevated SII. This nexus of inflammation-coagulation helps to advance trauma-induced coagulopathy and dysfunction of multiple organs, which eventually affects the survival of the patient.45 The results of the present study have been consistent with this new evidence that combined measurement of inflammatory and coagulation biomarkers reveals improved prognostic data compared with individual measurements of each of the two pathways.46–48
Due to the limited sample size in each injury cause subgroup, a comparative analysis of mortality rates among these specific mechanisms was not performed. Future studies with larger cohorts are warranted to explore potential prognostic differences associated with different injury etiologies.
In summary, data from the present study suggest that SII and D-D are valuable early prognostic predictors for patients with MI. Mortality significantly increases when D-D is >2.35 µg/mL or SII is >308.8 upon admission. Combined assessment using SII, D-D and ISS provides the most accurate prognostic evaluation, indicating that early intervention based on these predictive indicators may reduce mortality in patients with MI. However, the present study has several limitations. Its retrospective, single-center design and relatively small sample size (142 cases) limit result generalizability and introduce potential selection bias. Additionally, the present study lacks an external validation cohort to verify the combined generalizability of the model. Only baseline SII and D-D values were assessed at admission without dynamic monitoring over time, potentially overlooking important prognostic information. Future studies should conduct large-scale, multicenter, prospective cohort studies for external model validation and explore whether changes in SII and D-D over time have greater predictive value. Additionally, investigating the molecular mechanisms underlying immune-coagulation interactions associated with these indicators may offer theoretical foundations for developing novel therapeutic targets.
Data Sharing Statement
The data generated in the present study may be requested from the corresponding author.
Ethics Approval and Consent to Participate
The present study was approved by the Medical Ethics Committee of Shenzhen Longhua District Central Hospital (approval no. 2025-062-01). All patients provided written informed consent for participation, which included the use of their clinical data and samples for research purposes.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
No funding was received.
Disclosure
The authors declare that they have no competing interests in this work.
References
1. Bai Z, Han J, An J, et al. The global, regional, and national patterns of change in the burden of congenital birth defects, 1990-2021: an analysis of the global burden of disease study 2021 and forecast to 2040. EClinicalMedicine. 2024;77:102873. doi:10.1016/j.eclinm.2024.102873
2. Ketenci HC, Özsoy S, Aydoğdu HI, et al. Drowning in submerged cars caused by traffic accidents. Ulus Travma Acil Cerrahi Derg. 2022;28:1115–10. doi:10.14744/tjtes.2021.35915
3. Fabig S, Weigert N, Migliorini F, et al. Predictive parameters for early detection of clinically relevant abdominal trauma in multiple-injury or polytraumatised patients: a retrospective analysis. Eur J Med Res. 2024;29:394. doi:10.1186/s40001-024-01969-3
4. Zhang Y, Wu W, Zhang Z. The predictive value of the systemic inflammatory response index for the occurrence of multiple organ dysfunction syndrome in patients with wasp sting injury. Toxicon. 2023;234:107269. doi:10.1016/j.toxicon.2023.107269
5. Chen X, Li L, Yang Z, et al. Predictive value of D-dimer coupled with injury severity score in prognosis of trauma patients. Chin J Emerg Med. 2018;27:486–491. doi:10.3760/CMA.J.ISSN.1671-0282.2018.05.006
6. Wyatt JP, Beard D, Busuttil A. Quantifying injury and predicting outcome after trauma. Forensic Sci Int. 1998;95(1):57–66. PMID: 9718671. doi:10.1016/s0379-0738(98)00085-1
7. Mortaz E, Zadian SS, Shahir M, et al. Does neutrophil phenotype predict the survival of trauma patients? Front Immunol. 2019;10:2122. doi:10.3389/fimmu.2019.02122
8. Zhou L, Huang C, Zhu X, et al. Combined systemic immune-inflammatory index (SII) and geriatric nutritional risk index (GNRI) predict survival in elderly patients with hip fractures: a retrospective study. J Orthop Surg Res. 2024;19:125. doi:10.1186/s13018-024-04585-3
9. Lord JM, Midwinter MJ, Chen YF, et al. The systemic immune response to trauma: an overview of pathophysiology and treatment. Lancet. 2014;384(9952):1455–1465. PMID: 25390327; PMCID: PMC4729362. doi:10.1016/S0140-6736(14)60687-5
10. Hu B, Yang XR, Xu Y, et al. Systemic immune-inflammation index predicts prognosis of patients after curative resection for hepatocellular carcinoma. Clin Cancer Res. 2014;20:6212–6222. doi:10.1158/1078-0432.CCR-14-0442
11. Liu K, Tang S, Liu C, et al. Systemic immune-inflammatory biomarkers (SII, NLR, PLR and LMR) linked to non-alcoholic fatty liver disease risk. Front Immunol. 2024;15:1337241.
12. Kosidło JW, Wolszczak-Biedrzycka B, Matowicka-Karna J, et al. Clinical significance and diagnostic utility of NLR, LMR, PLR and SII in the course of COVID-19: a literature review. J Inflamm Res. 2023;16:539–562. doi:10.2147/JIR.S395331
13. Ding P, Guo H, Sun C, et al. Combined systemic immune-inflammatory index (SII) and prognostic nutritional index (PNI) predicts chemotherapy response and prognosis in locally advanced gastric cancer patients receiving neoadjuvant chemotherapy with PD-1 antibody sintilimab and XELOX: a prospective study. BMC Gastroenterol. 2022;22:121.
14. Zhou Y, Dai M, Zhang Z. Prognostic significance of the systemic immune-inflammation index (SII) in patients with small cell lung cancer: a meta-analysis. Front Oncol. 2022;12:814727.
15. Gosselin AR, Bargoud CG, Sawalkar A, et al. Injury severity is a key contributor to coagulation dysregulation and fibrinogen consumption. bioRxiv [Preprint]. 2024:
16. Rousselet B, Rocheteau P, Hureau TJ, et al. D-dimer levels and risk of poor outcome in trauma patients: a systematic review and meta-analysis. Eur J Trauma Emerg Surg. 2023;49(2):767–779.
17. Rougerie L, Charbit J, Mezzarobba M, et al. Epidemiology of civilian’s gunshot wound injuries admitted to intensive care unit: a retrospective, multi-center study. Injury. 2024;55(10):111735. PMID: 39153311. doi:10.1016/j.injury.2024.111735
18. Cao C, Li C, Li X, et al. Association of systemic immune-inflammation index (SII) and aggregate index of systemic inflammation (AISI) with thyroid nodules in patients with type 2 diabetes mellitus: a retrospective study. BMC Endocr Disord. 2023;23:251. doi:10.1186/s12902-023-01509-w
19. Zhai GH, Zhang W, Xiang Z, et al. Diagnostic value of sIL-2R, TNF-α and PCT for sepsis infection in patients with closed abdominal injury complicated with severe multiple abdominal injuries. Front Immunol. 2021;12:741268. doi:10.3389/fimmu.2021.741268
20. Ting RS, Lewis DP, Yang KX, et al. Incidence of multiple organ failure in adult polytrauma patients: a systematic review and meta-analysis. J Trauma Acute Care Surg. 2023;94:725–734. doi:10.1097/TA.0000000000003923
21. Chen P, Billiar T. Gut Microbiota and Multiple Organ Dysfunction Syndrome (MODS). Adv Exp Med Biol. 2020;1238:195–202.
22. Güiza F, Depreitere B, Meyfroidt G. Novel approaches to multi-organ dysfunction in the critically ill: from injury to repair. Intensive Care Med. 2018;44(9):1403–1405.
23. Cittadini F, Aulino G, Petrucci M, et al. Bicycle-related accidents in Rome: investigating clinical patterns, demographics, injury contexts, and health outcomes for enhanced public safety. Injury. 2024;55(4):111464. doi:10.1016/j.injury.2024.111464
24. Becker N, Hammen A, Bläsius F, et al. Effect of injury patterns on the development of complications and trauma-induced mortality in patients suffering multiple trauma. J Clin Med. 2023;12(15):5111. doi:10.3390/jcm12155111
25. Zhang XF, Qin YY. Association between SII and markers of liver injury: a cross-sectional study from the NHANES (2017-2020). PLoS One. 2024;19:e0303398. doi:10.1371/journal.pone.0303398
26. Ward NS, Casserly B, Ayala A. The compensatory anti-inflammatory response syndrome (CARS) in critically ill patients. Clin Chest Med. 2008;29(4):617–25,viii. PMID: 18954697; PMCID: PMC2786900. doi:10.1016/j.ccm.2008.06.010
27. Eisinger F, Patzelt J, Langer HF. The platelet response to tissue injury. Front Med Lausanne. 2018;5:317. PMID: 30483508; PMCID: PMC6242949. doi:10.3389/fmed.2018.00317
28. Danielpour D. Advances and challenges in targeting TGF-β isoforms for therapeutic intervention of cancer: a mechanism-based perspective. Pharmaceuticals. 2024;17(4):533. PMID: 38675493; PMCID: PMC11054419. doi:10.3390/ph17040533
29. Burnouf T, Chou ML, Lundy DJ, et al. Expanding applications of allogeneic platelets, platelet lysates, and platelet extracellular vesicles in cell therapy, regenerative medicine, and targeted drug delivery. J Biomed Sci. 2023;30(1):79. PMID: 37704991; PMCID: PMC10500824. doi:10.1186/s12929-023-00972-w
30. Moldovan F, Ivanescu AD, Fodor P, et al. Correlation between inflammatory systemic biomarkers and surgical trauma in elderly patients with hip fractures. J Clin Med. 2023;12(15):5147. doi:10.3390/jcm12155147
31. Hegdekar N, Sarkar C, Bustos S, et al. Inhibition of autophagy in microglia and macrophages exacerbates innate immune responses and worsens brain injury outcomes. Autophagy. 2023;19:2026–2044. doi:10.1080/15548627.2023.2167689
32. Thurairajah K, Briggs GD, Balogh ZJ. The source of cell-free mitochondrial DNA in trauma and potential therapeutic strategies. Eur J Trauma Emerg Surg. 2018;44(3):325–334. PMID: 29633007; PMCID: PMC6002458. doi:10.1007/s00068-018-0954-3
33. Joshi I, Carney WP, Rock EP. Utility of monocyte HLA-DR and rationale for therapeutic GM-CSF in sepsis immunoparalysis. Front Immunol. 2023;14:1130214. doi:10.3389/fimmu.2023.1130214
34. Niu Z, Ding Z, Chan Y, et al. Clinical characteristics and predictors of burn complicated with smoke inhalation injury: a retrospective analysis. Exp Ther Med. 2022;24:758. doi:10.3892/etm.2022.11694
35. Lee DH, Lee BK, Noh SM, et al. High fibrin/fibrinogen degradation product to fibrinogen ratio is associated with 28-day mortality and massive transfusion in severe trauma. Eur J Trauma Emerg Surg. 2018;44:291–298. doi:10.1007/s00068-017-0844-0
36. Hardy BM, Varghese A, Adams MJ, et al. The outcomes of the most severe polytrauma patients: a systematic review of the use of high ISS cutoffs for performance measurement. Eur J Trauma Emerg Surg. 2024;50(4):1305–1312. PMID: 38108840; PMCID: PMC11481685. doi:10.1007/s00068-023-02409-3
37. Liu XY, Qin YM, Tian SF, et al. Performance of trauma scoring systems in predicting mortality in geriatric trauma patients: comparison of the ISS, TRISS, and GTOS based on a systemic review and meta-analysis. Eur J Trauma Emerg Surg. 2024;50:1453–1465. doi:10.1007/s00068-024-02467-1
38. Kazemi F, Liu J, Nasr IW, et al. A comparative analysis of the trauma and injury severity score and the injury severity score in predicting high-value care outcomes in children with traumatic brain injury. J Neurosurg Pediatr. 2024;34:557–565. doi:10.3171/2024.8.PEDS24309
39. Jafari M, Rastegar-Kashkouli A, Yousefi P, et al. Comparison of four severity-of-disease scores in predicting mortality of trauma patients in ICU; a cross-sectional study. J Ren Endocrinol. 2024;10(1):
40. Hatchimonji JS, Luks VL, Swendiman RA, et al. Settling the score: injury severity score fails to capture nuances in pediatric trauma. Pediatr Emerg Care. 2022;38(2):e828–e832. PMID: 35100783. doi:10.1097/PEC.0000000000002363
41. McCullough AL, Haycock JC, Forward DP, et al. II. Major trauma networks in England. Br J Anaesth. 2014;113(2):202–206. doi:10.1093/bja/aeu204
42. Johansson PI, Sørensen AM, Perner A, et al. Disseminated intravascular coagulation or acute coagulopathy of trauma shock early after trauma? An Observ Study Crit Care. 2012;16:R135.
43. Tohira H, Jacobs I, Mountain D, et al. Systematic review of predictive performance of injury severity scoring tools. Scand J Trauma Resusc Emerg Med. 2012;20:63. doi:10.1186/1757-7241-20-63
44. Yuan SM, Wu N, Wang Y, et al. Combination of inflammatory and coagulation biomarkers in predicting mortality in patients with traumatic brain injury. Front Neurol. 2022;13:830593.
45. Middleton EA, He XY, Denorme F, et al. Neutrophil extracellular traps contribute to immunothrombosis in patients with major trauma. J Trauma Acute Care Surg. 2023;94:92–100.
46. Fröhlich M, Lefering R, Probst C, et al. Epidemiology and risk factors of multiple-organ failure after multiple trauma: an analysis of 31,154 patients from the TraumaRegister DGU. J Trauma Acute Care Surg. 2014;76(4):921–928. doi:10.1097/TA.0000000000000199
47. Maegele M, Schöchl H. Acute traumatic coagulopathy: from endogenous anticoagulation to therapy. Curr Opin Anesthesiol. 2014;27(2):244–249.
48. Gando S, Levi M, Toh CH. Disseminated intravascular coagulation. Nat Rev Dis Primers. 2016;2:16037. doi:10.1038/nrdp.2016.37
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
The Association of Systemic Immune Inflammation Index (SII) and Platelet-to-Lymphocyte Ratio (PLR) on Coagulopathy and Prognosis in Patients with Traumatic Brain Injury
Chen J, Fu J, Liu J, Lu Y, Han D, Zeng J, Zou Z, Li Q, Zhang K, Wei X, Li L, Gu Z
Journal of Inflammation Research 2025, 18:5637-5653
Published Date: 25 April 2025
Pretreatment Prognostic Nutritional Index Predicts Progression-Free Survival in BCLC Stage C Hepatocellular Carcinoma Treated with Sorafenib

Aydın U, Dikilitaş M, Balıkçı Çiçek İ, Pamuk ÖA, Sadak Öcal Z, Danacı Y, Alizade E
Cancer Management and Research 2026, 18:621105
Published Date: 14 July 2026