Back to Journals » International Journal of Women's Health » Volume 18
Predictive Value of Placental Growth Factor and Soluble FMS-Like Tyrosine Kinase-1 Detection in Early Pregnancy for Gestational Diabetes Mellitus: A Case-Control Study
Received 22 May 2025
Accepted for publication 14 January 2026
Published 10 February 2026 Volume 2026:18 542217
DOI https://doi.org/10.2147/IJWH.S542217
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Matteo Frigerio
Wen Wu, Xinli Liu
Department of Obstetrics and Gynecology, The Third Xiangya Hospital of Central South University, Changsha, Hunan, 410013, People’s Republic of China
Correspondence: Xinli Liu, Department of Obstetrics and Gynecology, The Third Xiangya Hospital of Central South University, No. 139, Tongzipo Road, Changsha, Hunan, 410013, People’s Republic of China, Email [email protected]
Background: Gestational diabetes mellitus (GDM) increases the risk of complications such as gestational hypertension, genital tract infections, preterm birth, and adverse perinatal outcomes including fetal distress and macrosomia. Identifying serum biomarkers in early pregnancy may aid in prevention and improve maternal and fetal outcomes.
Aim: To evaluate the predictive value of placental growth factor (PIGF) and soluble FMS-like tyrosine kinase-1 (sFlt-1) for GDM in early pregnancy.
Methods: A retrospective case-control study was conducted including 140 pregnant women screened for GDM in early pregnancy. Seventy women diagnosed with GDM formed the observation group, and 70 women with normal glucose levels served as controls. Inclusion criteria were singleton pregnancies with complete laboratory data and delivery follow-up at the same hospital. Primary outcomes were serum PIGF and sFlt-1 levels, and their predictive value for GDM was assessed.
Results: Pre-pregnancy BMI, fasting plasma glucose, HbA1c, HOMA-IR, and sFlt-1 levels were significantly higher in the observation group, while PIGF levels were lower. Pre-pregnancy BMI, PIGF, and sFlt-1 were independent predictors of GDM (P < 0.05). The incidence of gestational hypertension, preterm birth, genital tract infection, and macrosomia was higher in the observation group (P < 0.05). PIGF was negatively correlated with HOMA-IR, whereas sFlt-1 showed a positive correlation (P < 0.05). The area under the curve (AUC) for predicting GDM was 0.875 (95% CI: 0.818– 0.932) for PIGF and 0.824 (95% CI: 0.752– 0.897) for sFlt-1.
Conclusion: Lower PIGF and higher sFlt-1 levels in early pregnancy may be associated with GDM development and adverse outcomes. These biomarkers demonstrate potential predictive value, but large-scale prospective studies are required to confirm clinical utility.
Keywords: gestational diabetes mellitus, placental growth factor, PIGF, soluble FMS-like tyrosine kinase-1, sFlt-1, early pregnancy, predictive value
Introduction
Gestational diabetes mellitus (GDM) refers to varying degrees of glucose metabolism abnormalities that first occur or are diagnosed during pregnancy. It is one of the most common perinatal complications.1 Pregnant women with GDM are prone to gestational hypertension, reproductive tract infections, preterm birth, and have an increased risk of adverse pregnancy outcomes such as fetal distress and macrosomia.2 Therefore, exploring the relationship between serum markers and the condition of GDM patients in early pregnancy is of great significance for preventing GDM and improving pregnancy outcomes.
Placental growth factor (PIGF) is a placental-derived angiogenic factor that normally regulates the growth of endothelial cells and trophoblasts in the placenta. Abnormal expression of PIGF levels can exacerbate placental tissue ischemia and hypoxia, causing vascular spasms.3,4 Soluble vascular endothelial growth factor receptor-1 (sFlt-1) is a selectively spliced circulating form of the vascular endothelial growth factor (VEGF) receptor, belonging to the VEGF receptor family. It can bind to VEGF and related ligands, playing a crucial role in angiogenesis and endothelial function impairment.5 Previous studies have found that serum PIGF and sFlt-1 levels are associated with pregnancy complications. The abnormal changes of serum PIGF and sFlt-1 levels precede the onset of preeclampsia and may serve as early markers for predicting preeclampsia.6,7 The mechanisms of pregnancy complications are often accompanied by changes of peripheral blood cytokines level, and the serological values of diabetic patients are frequently associated with the deposition of various cytokines.8
Based on previous systematic reviews of placental pathology in patients with GDM, common pathological features include villous maturation disorders and abnormalities in angiogenesis.9 These morphological and functional changes of the placenta may reflect compensatory mechanisms aimed at counteracting maternal insulin resistance and optimizing fetal nutrient supply, achieved through modulation of angiogenic status to maintain adequate perfusion. PIGF plays a critical role in promoting healthy placental vascular development, and reduced production and secretion can be regarded as a manifestation of placental dysfunction. sFlt-1 regulates angiogenic balance by binding and neutralizing the biological activity of PIGF and VEGF. Imbalance between PIGF and sFlt-1 levels leads to abnormal formation of the placental vascular network, resulting in placental ischemia and hypoxia.10 This pathological state not only impairs placental function but may also trigger systemic inflammatory responses and oxidative stress, damage endothelial function, interfere with insulin signaling pathways, and ultimately contribute to peripheral tissue insulin resistance.11 This vascular mechanism may represent an important link between placental dysfunction and abnormal glucose metabolism.
PIGF and sFlt-1 exhibit characteristic dynamic changes during normal pregnancy, and this physiological pattern highlights the special value of the early gestational detection window.12 The early stage of pregnancy represents a critical period in which pathophysiological changes occur before clinical manifestations become evident. Therefore, measurement of these biomarkers in early pregnancy may provide a unique time window for the early warning of GDM. This study explores the potential role of early pregnancy serum levels of PIGF and sFlt-1 as predictive factors for GDM, and their relationship with pregnancy outcomes. This could aid in evaluating the role of indicators such as PIGF and sFlt-1 in screening and developing prevention and treatment strategies for GDM.
Materials and Methods
General Data
This study retrospectively collected clinical data of pregnant women who underwent early pregnancy GDM screening at our hospital’s Department of Obstetrics and Gynecology from April 2023 to October 2024. All enrolled pregnant women completed early pregnancy serum biomarker testing and gestational follow-up within this time period. Inclusion criteria: (1) Underwent oral glucose tolerance test (OGTT); (2) Completed pregnancy follow-up and delivery at our hospital; (3) Underwent pregnancy-related laboratory tests, including blood glucose and lipid levels, at our hospital, with complete clinical data; (4) No history of hypertension, diabetes, or thyroid dysfunction before pregnancy. Exclusion criteria: (1) Multiple pregnancies; (2) Presence of heart, kidney, or other primary organ diseases; (3) Pre-pregnancy immune system diseases; (4) Mental disorders. Participants were consecutively enrolled, and a total of 140 subjects were included. The observation group consisted of pregnant women diagnosed with GDM during this period based on OGTT results and meeting the diagnostic criteria. The control group comprised pregnant women with normal blood glucose levels who underwent routine prenatal examinations and completed OGTT screening during the same period. All subjects met the inclusion and exclusion criteria. This study has been approved by The Third Xiangya Hospital of Central South University ethics committee (Approval No.: 25350).
Sample Size
According to previously reported incidence rates of GDM in pregnant women,3 the preliminary estimation indicated that at least 58 subjects per group were required. Considering the retrospective design of the study and the potential for incomplete case records or missing data, an additional 20% was added to account for possible attrition. The final sample size was therefore determined as 70 subjects per group.
Observation Indicators
A standard structured questionnaire using an electronic information collection system was employed to collect baseline data of pregnant women in detail, including the number of pregnancies, number of deliveries, family history of diabetes, body mass index (BMI), educational level, and adverse obstetric history. Early pregnancy serum indicators for the two groups were obtained through the hospital’s case system, including fasting blood glucose (FPG), glycated hemoglobin (HbA1c), high-density lipoprotein (HDL), low-density lipoprotein (LDL), total cholesterol (TC), and triglycerides (TG). The insulin resistance index (HOMA-IR) was calculated.
Serum PIGF and sFlt-1 Level Testing: All pregnant women underwent testing in early pregnancy (11+0-13+6 weeks) after fasting for more than 10h the previous night. The following morning, 5mL of fasting venous blood was drawn from the elbow. The blood was centrifuged at 2500g for 20min at a temperature of 20–25°C to separate the serum, which was then stored at −80°C. The levels of PIGF and sFlt-1 were measured using the enzyme-linked immunosorbent assay (ELISA) method. All procedures were strictly performed according to the kit instructions provided by Shanghai Kanglang Biotechnology Co., Ltd.
Adverse Pregnancy Outcomes: This study recorded all adverse pregnancy outcomes, including gestational hypertension, preterm birth, genital tract infections, fetal distress, and macrosomia. Gestational hypertension was defined as a systolic blood pressure ≥140 mmHg and/or diastolic blood pressure ≥ 90 mmHg occurring after 20 weeks of gestation, which returned to normal within 12 weeks postpartum.13 Preterm birth was defined as delivery between 28 weeks and less than 37 weeks of gestation.14 Genital tract infections were defined as infectious diseases of the reproductive tract (including both internal and external genitalia) caused by various pathogens such as bacteria, viruses, chlamydia, mycoplasma, fungi, etc.15 Fetal distress was defined as a syndrome indicating acute or chronic hypoxia of the fetus in utero that endangers its health and life.16 Macrosomia was defined as the birth weight of the fetus reaching or exceeding 4000g.17
Statistical Methods
Statistical analysis of the data was conducted using SPSS 20.0 software. Measurement data conforming to a normal distribution is expressed as ( ) and independent sample t test was used for comparison between the two groups. Non-normally distributed measurement data were expressed as median (Q25,Q75) and compared between groups using the rank-sum test. Count data were expressed as numbers (%) and compared between groups using the χ2 test. Pearson correlation analysis was employed to assess the relationships. To control for potential confounding factors, variables showing differences between the two groups at baseline were included in the model as covariates. Multifactor logistic regression analysis was used to identify factors influencing the occurrence of GDM. ROC curves (receiver operating characteristic curves, ROC) were plotted to evaluate the predictive value of serum PIGF and sFlt-1 levels for GDM in pregnant women. P<0.05 was considered statistically significant.
) and independent sample t test was used for comparison between the two groups. Non-normally distributed measurement data were expressed as median (Q25,Q75) and compared between groups using the rank-sum test. Count data were expressed as numbers (%) and compared between groups using the χ2 test. Pearson correlation analysis was employed to assess the relationships. To control for potential confounding factors, variables showing differences between the two groups at baseline were included in the model as covariates. Multifactor logistic regression analysis was used to identify factors influencing the occurrence of GDM. ROC curves (receiver operating characteristic curves, ROC) were plotted to evaluate the predictive value of serum PIGF and sFlt-1 levels for GDM in pregnant women. P<0.05 was considered statistically significant.
Results
Comparison of Clinical Characteristics Between the Two Groups of Pregnant Women
The pre-pregnancy BMI of the observation group was significantly higher than that of the control group (P<0.05, Table 1). There were no significant differences in other general data, such as age, between the two groups (P>0.05, Table 1).
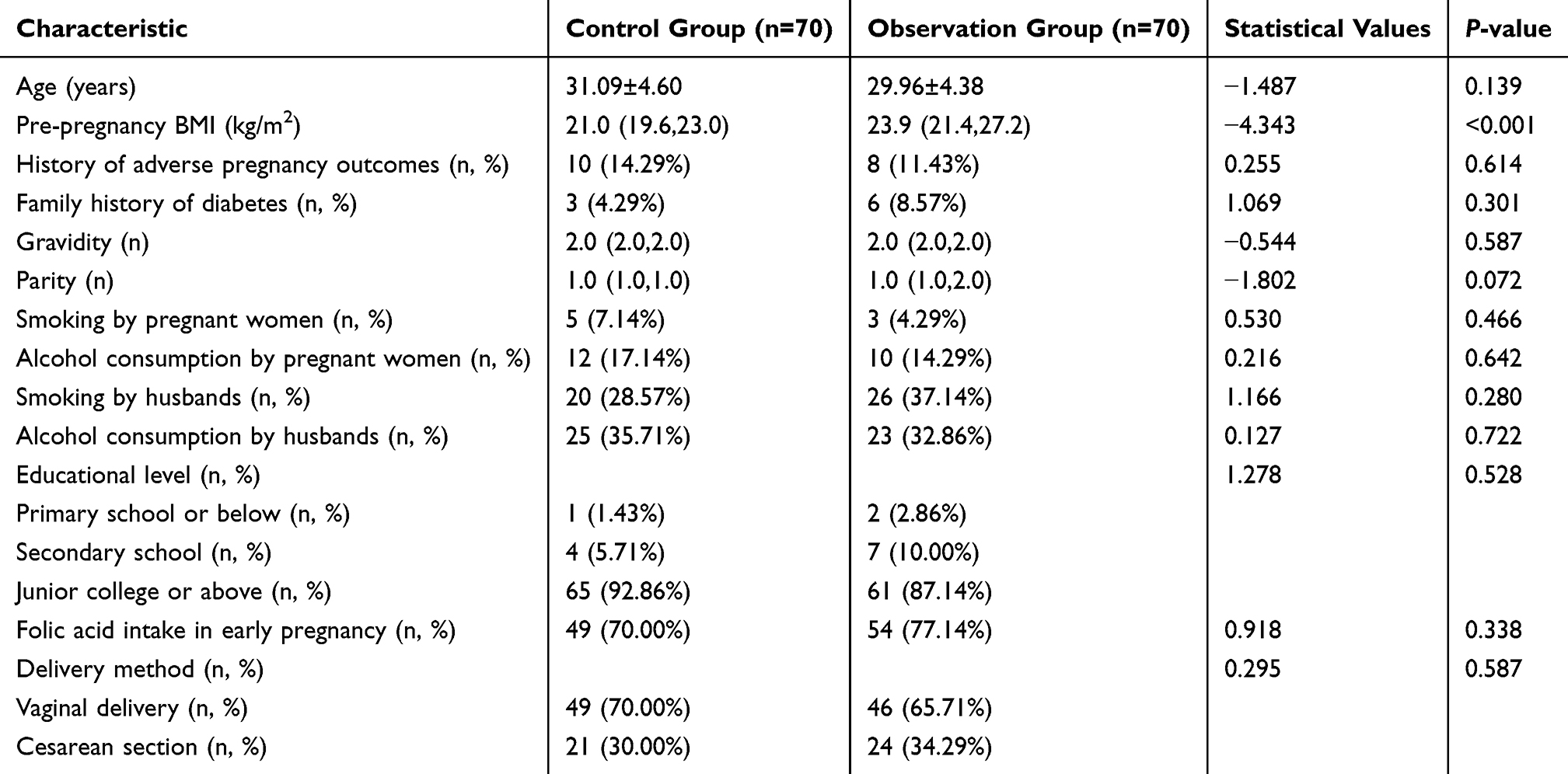 |
Table 1 Comparison of Clinical Characteristics of Pregnant Women |
Comparison of Laboratory Indicators Between the Two Groups of Pregnant Women
The PIGF levels in the observation group were lower than those in the control group, while the levels of FPG, HbA1c, HOMA-IR, and sFlt-1 were higher in the observation group. These differences were statistically significant (P<0.05, Table 2). There were no significant differences in the levels of TC, LDL, HDL, and TG between the two groups (P>0.05, Table 2).
 |
Table 2 Comparison of Laboratory Indicators Between the Two Groups of Pregnant Women |
Comparison of Pregnancy Outcomes Between the Two Groups of Pregnant Women
The proportions of gestational hypertension, preterm birth, genital tract infections, and macrosomia in the observation group were significantly higher than those in the control group (P<0.05, Table 3).
 |
Table 3 Comparison of Pregnancy Outcomes Between the Two Groups of Pregnant Women |
Correlation Between Early Pregnancy Serum PIGF, sFlt-1 and Insulin Resistance
The level of PIGF was significantly negatively correlated with HOMA-IR (r=−0.569, P<0.001, Figure 1), while the level of sFlt-1 was significantly positively correlated with HOMA-IR (r=0.425, P<0.001, Figure 2).
 |
Figure 1 Correlation Analysis Between PIGF Levels and HOMA-IR. |
 |
Figure 2 Correlation Analysis Between sFlt-1 Levels and HOMA-IR. |
Independent Predictors of the Risk of Developing GDM
Pre-pregnancy BMI, FPG, HbA1c, HOMA-IR, PIGF, and sFlt-1 were used as independent variables, and whether the subjects had GDM was used as the dependent variable in a logistic regression analysis. The results showed that pre-pregnancy BMI, PIGF, and sFlt-1 levels were independent predictors of the occurrence of GDM (P<0.05, Tables 4 and 5).
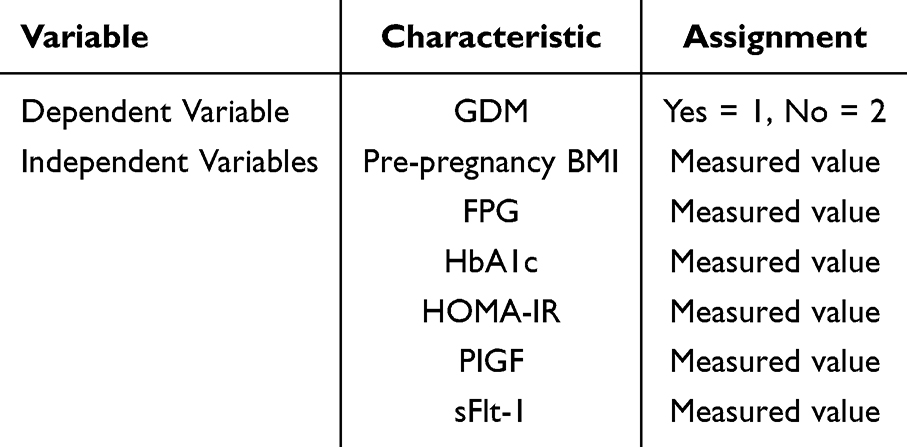 |
Table 4 Logistic Regression Analysis Assignment Table |
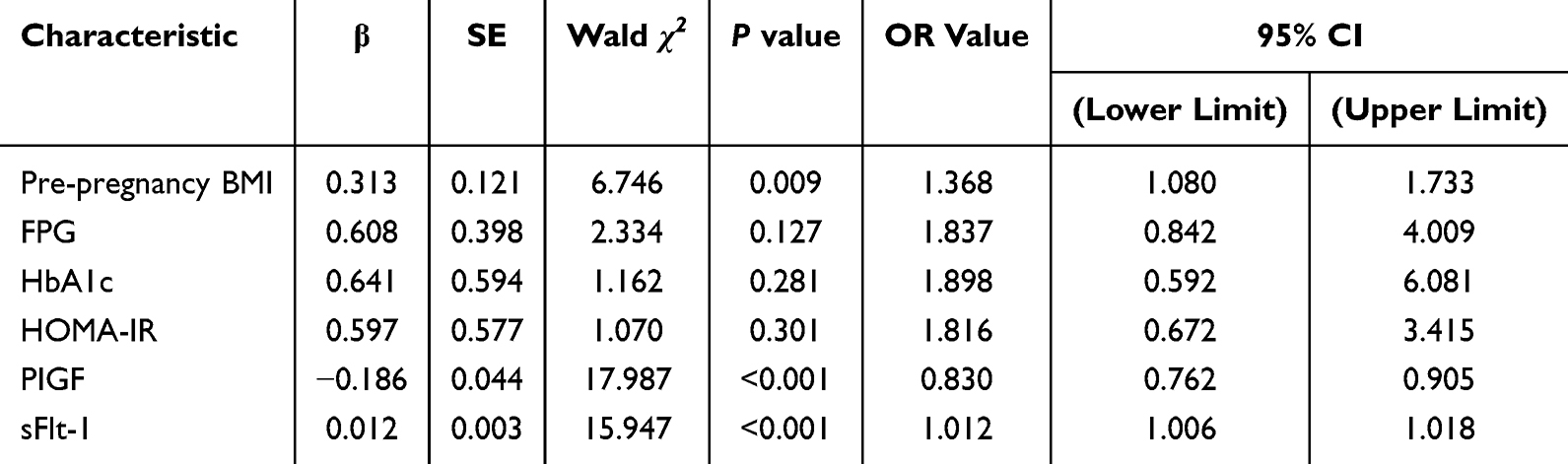 |
Table 5 Logistic Regression Analysis of Risk Factors for Developing GDM |
Predictive Efficacy of PIGF and sFlt-1 Levels for GDM
The AUC (area under the curve) for predicting GDM using early pregnancy PIGF levels was 0.875 (95% CI: 0.818–0.932), and for sFlt-1 levels, it was 0.824 (95% CI: 0.752–0.897). The optimal cutoff value of PlGF for predicting GDM was 48.22 pg/mL, with a sensitivity of 82.9% and a specificity of 75.7%. The optimal cutoff value of sFlt-1 for predicting GDM was 898.39 pg/mL, with a sensitivity of 71.4% and a specificity of 87.1% (Figure 3).
 |
Figure 3 ROC Curves for Predicting GDM Using PIGF and sFlt-1 Levels. |
Discussion
The resistance to insulin caused by progesterone, human placental lactogen, and estrogen secreted by the placenta in late pregnancy is the main cause of GDM. Additionally, studies have suggested that high-risk factors for GDM include a family history of diabetes, obesity, and hypertension.18 The results of this study showed that pre-pregnancy BMI in GDM patients was significantly higher than in normal pregnant women, and the levels of FPG, HbA1c, and HOMA-IR were also significantly elevated. Pregnant women with higher pre-pregnancy BMI are more likely to develop insulin resistance and struggle to maintain stable blood glucose levels due to weight gain and hormonal changes during pregnancy, thus leading to the development of GDM.19
For GDM patients without high-risk lifestyle habits, typical symptoms like obvious thirst, frequent urination, dizziness, or hunger are usually not present, leading to most GDM cases being detected in the mid to late stages of pregnancy. Previous studies have found that endothelial dysfunction associated with GDM is related to abnormal fetal growth.20,21 The results of this study showed that the proportions of gestational hypertension, preterm birth, genital tract infections, and macrosomia in the observation group were significantly higher than those in the control group. Maternal hyperglycemia can induce gestational hypertension, exacerbating the condition. It can also accelerate lipid metabolism, leading to elevated serum ketone levels in the body, and causing complications such as fetal distress. The hyperglycemic state increases the risk of macrosomia and the likelihood of preterm birth.22 This suggests that exploring serum-related biological indicators in early pregnancy is significant for GDM screening, monitoring GDM conditions, and improving pregnancy outcomes.
Abnormally elevated concentrations of sFlt-1 in the placenta and circulation can inhibit free VEGF and PIGF, leading to the typical abnormal placental angiogenesis and systemic endothelial dysfunction characteristic of gestational syndromes.8 sFlt-1 and PIGF have been extensively studied as biomarkers for preeclampsia, as their level changes occur before the clinical symptoms of preeclampsia.23,24 However, the complex interaction between the expression levels of sFlt-1 and PIGF and gestational syndromes in the context of pre-GDM remains unresolved.
The results of this study showed that the PIGF levels in the observation group were lower than those in the control group, while the sFlt-1 levels were higher than those in the control group. Additionally, the PIGF levels were negatively correlated with HOMA-IR, while the sFlt-1 levels were positively correlated with HOMA-IR. This suggests that serum sFlt-1 and PIGF levels are closely related to insulin resistance in patients. High blood sugar and diabetes-induced metabolic disorders, oxidative stress, and inflammatory responses trigger relevant cells, such as vascular endothelial cells and placental trophoblast cells, to increase the secretion of sFlt-1.25 The study by Madiwale et al26 also supports this perspective, demonstrating that the expression of placental angiogenic biomarkers PIGF and sFlt-1 in patients with GDM is significantly altered compared with non-GDM women, potentially affecting placental development and function. Moreover, the negative correlation between these abnormal expressions and placental size suggests that such changes may adversely influence pregnancy outcomes in GDM. It should be emphasized, however, that as a case-control study, the present research can only indicate an association between early pregnancy PIGF and sFlt-1 level changes and GDM, without establishing causality. Whether these biomarker alterations represent causal factors for GDM or early effects of the disease remains to be clarified through prospective cohort studies and further mechanistic investigations.
The study by Tsiakkas et al27 observed a significant decreasing trend in early pregnancy serum PIGF levels in women with pre-existing type 1 and type 2 diabetes, highlighting the role of PIGF level changes in screening for pregnancy complications. Additionally, the study by Mordwinkin et al28 demonstrated that in women with GDM, maternal circulating endothelial progenitor cells decrease, soluble adhesion molecules increase, superoxide dismutase expression decreases, and endothelial nitric oxide synthase expression increases. These mechanisms may involve changes in the balance of angiogenesis, leading to fluctuations in serum factors such as PIGF and sFlt-1. Obesity and overweight (pre-pregnancy BMI ≥25 kg/m2) are also critical risk factors. Increased adipose tissue, particularly visceral fat accumulation, promotes chronic low-grade inflammation and abnormal adipokine secretion, thereby exacerbating insulin resistance. In addition, obesity is often accompanied by lipotoxicity and disturbances in insulin signaling pathways, which further impair the insulin secretory reserve capacity of β-cells.29 This study confirmed through logistic regression analysis that pre-pregnancy BMI, PIGF, and sFlt-1 are independent predictors of GDM occurrence and further utilized ROC curve analysis to assess the predictive efficacy of PIGF and sFlt-1 for GDM. The results showed that early pregnancy serum levels of PIGF and sFlt-1 have good predictive value for the occurrence of GDM, providing a basis for early prediction of GDM. Advanced maternal age is a well-established independent risk factor for GDM, with the risk further increasing in women aged ≥35 years.30 The underlying mechanisms may be related to age-associated decline in insulin sensitivity, accumulation of oxidative stress, and progressive deterioration of pancreatic β-cell function with advancing age. A history of GDM, family history of diabetes, and ethnic or racial differences have also been widely documented as risk factors for GDM.31 Such disparities may be attributed to genetic susceptibility, differences in body fat distribution (eg, central obesity), and ethnicity-specific variations in insulin sensitivity and β-cell function. The development of GDM results from the combined effects of multiple risk factors, with the core pathophysiological pathways involving exacerbated insulin resistance and β-cell functional decompensation. Integrating serum biomarkers such as PIGF and sFlt-1, which reflect early placental function and vascular homeostasis, with traditional clinical risk factors including advanced maternal age, BMI, and ethnicity, may enable the construction of a more precise and forward-looking predictive model for GDM risk.
This study has several limitations. First, as a single-center retrospective case-control study, all participants were recruited from the same institution, which may restrict the generalizability of the findings to rural populations, different ethnic groups, or other healthcare systems. Second, due to the retrospective design, the sample size was relatively small and primarily dependent on existing medical records, making it difficult to systematically collect and adjust for all potential confounding factors (such as detailed dietary patterns, physical activity levels, genetic background, and gestational weight gain). Consequently, the study was insufficient to construct a highly robust multivariable predictive model. Although key variables such as pre-pregnancy BMI, maternal age, and family history were controlled in the analysis, residual confounding cannot be completely excluded. Finally, only a single time point of serum PIGF and sFlt-1 levels in early pregnancy was measured, without dynamic monitoring throughout gestation. This limitation makes it difficult to clarify the longitudinal trajectories of these biomarkers and their temporal relationship with the onset and progression of GDM. Future large-scale prospective cohort studies are needed to establish more comprehensive predictive models and to further validate the independent predictive value of these angiogenic biomarkers, thereby enabling the development of more reliable early risk prediction tools.
Conclusions
In summary, reduced serum PIGF and elevated sFlt-1 levels in early pregnancy may be associated with the development of GDM and the progression of adverse pregnancy outcomes, and preliminary ROC analysis demonstrated certain discriminatory ability. Measurement of PIGF and sFlt-1 in early pregnancy shows potential predictive value for GDM. However, given the retrospective design and single-center sample source of this study, these conclusions require further validation through large-scale prospective cohort studies to assess their true clinical translational significance.
Data Sharing Statement
The data supporting this study’s findings are available from the corresponding author upon reasonable request.
Ethics Approval and Informed Consent
This study has been approved by The Third Xiangya Hospital of Central South University ethics committee (Approval No.: 25350). This study complies with the Declaration of Helsinki. This study obtained the informed consent of the participants.
Author Contributions
Wen Wu contributed to data analysis and interpretation. Xinli Liu was responsible for figure preparation. Wen Wu and Xinli Liu drafted the main manuscript text. All authors participated in revising and critically reviewing the article, approved the final version for publication, agreed on the journal of submission, and accept accountability for all aspects of the manuscript.
Funding
There is no funding to report.
Disclosure
The authors declare that they have no conflicts of interest in this work.
References
1. Yi Y, Wang T, Xu W, Zhang SH. Epigenetic modifications of placenta in women with gestational diabetes mellitus and their offspring. World J Diabetes. 2024;15(3):378–10. PMID: 38591094; PMCID: PMC10999040. doi:10.4239/wjd.v15.i3.378
2. Balachandiran M, Bobby Z, Dorairajan G, Gladwin V, Vinayagam V, Packirisamy RM. Decreased maternal serum adiponectin and increased insulin-like growth factor-1 levels along with increased placental glucose transporter-1 expression in gestational diabetes mellitus: possible role in fetal overgrowth. Placenta. 2021;104:71–80. PMID: 33285436. doi:10.1016/j.placenta.2020.11.008
3. Lara-Barea A, Sánchez-Lechuga B, Campos-Caro A, et al. Angiogenic imbalance and inflammatory biomarkers in the prediction of hypertension as well as obstetric and perinatal complications in women with gestational diabetes mellitus. J Clin Med. 2022;11(6):1514. PMID: 35329840; PMCID: PMC8953606. doi:10.3390/jcm11061514IF:30Q1
4. Anto EO, Boadu WIO, Hughes C, et al. Angiogenic growth factors, oxidative stress and haematobiochemical measures as predictors of preeclampsia with and without foetal growth restriction: a case-control study in a Ghanaian population. Placenta. 2024;145:130–138. PMID: 38134545. doi:10.1016/j.placenta.2023.12.007
5. Lara-Barea A, Sánchez-Lechuga B, Aguilar-Diosdado M, López-Tinoco C. Higher daytime systolic BP, prepregnancy BMI and an elevated sFlt-1/PlGF ratio predict the development of hypertension in normotensive pregnant women. Reprod Biol Endocrinol. 2022;20(1):175. PMID: 36564806; PMCID: PMC9783759. doi:10.1186/s12958-022-01050-w
6. Nuzzo AM, Giuffrida D, Moretti L, et al. Placental and maternal sFlt1/PlGF expression in gestational diabetes mellitus. Sci Rep. 2021;11(1):2312. PMID: 33504861; PMCID: PMC7840991. doi:10.1038/s41598-021-81785-5
7. Zhao B, Han X, Meng Q, Luo Q. Early second trimester maternal serum markers in the prediction of gestational diabetes mellitus. J Diabetes Investig. 2018;9(4):967–974. PMID: 29288571; PMCID: PMC6031488. doi:10.1111/jdi.12798
8. Bolatai A, He Y, Wu N. Vascular endothelial growth factor and its receptors regulation in gestational diabetes mellitus and eclampsia. J Transl Med. 2022;20(1):400. PMID: 36064413; PMCID: PMC9444093. doi:10.1186/s12967-022-03603-4
9. Huynh J, Dawson D, Roberts D, Bentley-Lewis R. A systematic review of placental pathology in maternal diabetes mellitus. Placenta. 2015;36(2):101–114. PMID: 25524060; PMCID: PMC4339292. doi:10.1016/j.placenta.2014.11.021
10. Gul Kara SM, Alkan Bulbul G, Kirtis E, et al. Maternal and cord serum levels of sFlt-1 and PlGF in pregnancies complicated by gestational diabetes mellitus: a prospective cohort study. J Matern Fetal Neonatal Med. 2025;38(1):2491454. PMID: 40254554. doi:10.1080/14767058.2025.2491454
11. Lu YT, Chen CP, Sun FJ, Chen YY, Wang LK, Chen CY. Associations between first-trimester screening biomarkers and maternal characteristics with gestational diabetes mellitus in Chinese women. Front Endocrinol. 2024;15:1383706. PMID: 39175575; PMCID: PMC11339418. doi:10.3389/fendo.2024.1383706
12. Kagan KO, Sonek J, Wagner P, Hoopmann M. Principles of first trimester screening in the age of non-invasive prenatal diagnosis: screening for chromosomal abnormalities. Arch Gynecol Obstet. 2017;296(4):645–651. PMID: 28702698. doi:10.1007/s00404-017-4459-9
13. Khedagi AM, Bello NA. Hypertensive disorders of pregnancy. Cardiol Clin. 2021;39(1):77–90. PMID: 33222817; PMCID: PMC7720658. doi:10.1016/j.ccl.2020.09.005
14. Hudić I, Stray-Pedersen B, Tomić V. Preterm birth: pathophysiology, prevention, diagnosis, and treatment. Biomed Res Int. 2015;2015:417965. PMID: 26413520; PMCID: PMC4568055. doi:10.1155/2015/417965
15. Taylor-Robinson D, Horner P, Pallecaros A. Diagnosis of some genital-tract infections: part 2. Molecular tests and the new challenges. Int J STD AIDS. 2020;31(3):198–207. PMID: 32009570. doi:10.1177/0956462419890526
16. American College of Obstetricians and Gynecologists. ACOG Practice Bulletin No. 106: intrapartum fetal heart rate monitoring: nomenclature, interpretation, and general management principles. Obstet Gynecol. 2009;114(1):192–202. PMID: 19546798. doi: 10.1097/AOG.0b013e3181aef106
17. Haram K, Pirhonen J, Bergsjø P. Suspected big baby: a difficult clinical problem in obstetrics. Acta Obstet Gynecol Scand. 2002;81(3):185–194. PMID: 11966473. doi:10.1034/j.1600-0412.2002.810301.x
18. Nayak PK, Mitra S, Sahoo JP, Daniel M, Mathew A, Padma A. Feto-maternal outcomes in women with and without gestational diabetes mellitus according to the International Association of Diabetes and Pregnancy Study Groups (IADPSG) diagnostic criteria. Diabetes Metab Syndr. 2013;7(4):206–209. PMID: 24290085. doi:10.1016/j.dsx.2013.10.017
19. Abell SK, De Courten B, Boyle JA, Teede HJ. Inflammatory and other biomarkers: role in pathophysiology and prediction of gestational diabetes mellitus. Int J Mol Sci. 2015;16(6):13442–13473. PMID: 26110385; PMCID: PMC4490503. doi:10.3390/ijms160613442
20. Karpova NS, Dmitrenko OP, Budykina TS. Literature review: the sFlt1/PlGF ratio and pregestational maternal comorbidities: new risk factors to predict pre-eclampsia. Int J Mol Sci. 2023;24(7):6744. PMID: 37047717; PMCID: PMC10095124. doi:10.3390/ijms24076744
21. EBM CONNECT Collaboration; Kleinrouweler CE, Wiegerinck MM, Ris-Stalpers C, et al. Accuracy of circulating placental growth factor, vascular endothelial growth factor, soluble fms-like tyrosine kinase 1 and soluble endoglin in the prediction of pre-eclampsia: a systematic review and meta-analysis. BJOG. 2012;119(7):778–787. PMID: 22433027. doi:10.1111/j.1471-0528.2012.03311.x
22. Lee KW, Ching SM, Ramachandran V, et al. Prevalence and risk factors of gestational diabetes mellitus in Asia: a systematic review and meta-analysis. BMC Pregnancy Childbirth. 2018;18(1):494. PMID: 30547769; PMCID: PMC6295048. doi:10.1186/s12884-018-2131-4
23. Frampton GK, Jones J, Rose M, Payne L. Placental growth factor (alone or in combination with soluble fms-like tyrosine kinase 1) as an aid to the assessment of women with suspected pre-eclampsia: systematic review and economic analysis. Health Technol Assess. 2016;20(87):1–160. PMID: 27918253; PMCID: PMC5165281. doi:10.3310/hta20870
24. Saleh L, van den Meiracker AH, Geensen R, et al. Soluble fms-like tyrosine kinase-1 and placental growth factor kinetics during and after pregnancy in women with suspected or confirmed pre-eclampsia. Ultrasound Obstet Gynecol. 2018;51(6):751–757. PMID: 28600845. doi:10.1002/uog.17547
25. Xiang QQ, Yang Z, Huai J, Wang GJ. Different effects of pravastatin on sFlt-1, PlGF and VEGF in different preeclampsia-like mouse models. Zhonghua Fu Chan Ke Za Zhi. 2019. 54(9):601–607. doi: 10.3760/cma.j.issn.0529-567x.2019.09.005. Chinese. PMID: 31550776.
26. Madiwale S, Kasture V, Sundrani D, Krishnaveni GV, Gupte S, Joshi S. Angiogenic markers in gestational diabetes and their association with placental dimensions. Mol Cell Biochem. 2024;480(6):3637–3646. PMID: 39724316. doi:10.1007/s11010-024-05189-5
27. Tsiakkas A, Duvdevani N, Wright A, Wright D, Nicolaides KH. Serum placental growth factor in the three trimesters of pregnancy: effects of maternal characteristics and medical history. Ultrasound Obstet Gynecol. 2015;45(5):591–598. PMID: 25653039. doi:10.1002/uog.14811
28. Mordwinkin NM, Ouzounian JG, Yedigarova L, Montoro MN, Louie SG, Rodgers KE. Alteration of endothelial function markers in women with gestational diabetes and their fetuses. J Matern Fetal Neonatal Med. 2013;26(5):507–512. PMID: 23046386; PMCID: PMC3622728. doi:10.3109/14767058.2012.736564
29. Benhalima K, Van Crombrugge P, Moyson C, et al. Risk factor screening for gestational diabetes mellitus based on the 2013 WHO criteria. Eur J Endocrinol. 2019;180(6):353–363. PMID: 31120231. doi:10.1530/EJE-19-0117
30. Japan Environment and Children’s Study Group; Tagami K, Iwama N, Hamada H, et al. Advanced maternal age is a risk factor for both early and late gestational diabetes mellitus: the Japan Environment and Children’s Study. J Diabetes Investig. 2025;16(4):735–743. PMID: 39797691; PMCID: PMC11970309. doi:10.1111/jdi.14400
31. Yuen L, Wong VW, Simmons D. Ethnic disparities in gestational diabetes. Curr Diab Rep. 2018;18(9):68. PMID: 30039471. doi:10.1007/s11892-018-1040-2
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Study on the Relationship and Predictive Value of First-Trimester Pregnancy-Associated Plasma Protein-A, Maternal Factors, and Biochemical Parameters in Gestational Diabetes Mellitus: A Large Case-Control Study in Southern China Mothers
Cui J, Li P, Chen X, Li L, Ouyang L, Meng Z, Fan J
Diabetes, Metabolic Syndrome and Obesity 2023, 16:947-957
Published Date: 1 April 2023
The Association Between the Imbalance of Single-Carbon Nutrients in Early Pregnancy and Gestational Diabetes Mellitus Risk is Influenced by Serum Selenium Status: A Cohort Study
Liu PJ, Ma L, Li R, Liu Y
Diabetes, Metabolic Syndrome and Obesity 2023, 16:3275-3283
Published Date: 20 October 2023
The Role of METS-IR in Early Screening for Gestational Diabetes Mellitus in Chinese Women: A Two-Center Prospective Study
Gao J, Song S, Duo Y, Wang S, Qiao X, Zhang Y, Xu J, Zhang J, Nie X, Sun Q, Yang X, Wang A, Sun W, Fu Y, Zhang M, Dong Y, Lu Z, Yuan T, Zhao W
Diabetes, Metabolic Syndrome and Obesity 2025, 18:3967-3984
Published Date: 25 October 2025
Association Between First-Trimester Gestational Weight Gain and the Risks of Gestational Diabetes Mellitus and Macrosomia
Yang D, Yu Z, Chen J, Zhuang L, Wang X
Diabetes, Metabolic Syndrome and Obesity 2026, 19:564746
Published Date: 24 June 2026