Back to Journals » Diabetes, Metabolic Syndrome and Obesity » Volume 19
Association Between First-Trimester Gestational Weight Gain and the Risks of Gestational Diabetes Mellitus and Macrosomia
Authors Yang D, Yu Z, Chen J, Zhuang L, Wang X
Received 30 January 2026
Accepted for publication 31 May 2026
Published 24 June 2026 Volume 2026:19 564746
DOI https://doi.org/10.2147/DMSO.S564746
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Hillary Keenan
Dan Yang, Zhi Yu, Jin Chen, Lin Zhuang, Xiaoyin Wang
Department of Obstetrics, Hospital of Chengdu University of Traditional Chinese Medicine, Chengdu, Sichuan, 610072, People’s Republic of China
Correspondence: Xiaoyin Wang, Department of Obstetrics, Hospital of Chengdu University of Traditional Chinese Medicine, No. 39 Shi-er-qiao Road, Chengdu, Sichuan, 610072, People’s Republic of China, Email [email protected]
Purpose: To investigate the association between first-trimester gestational weight gain and the risks of gestational diabetes mellitus (GDM) and macrosomia.
Patients and Methods: This single-center retrospective cohort study was based on our hospital’s obstetric record-establishment database. Between January 2022 and January 2025, 516 women with singleton pregnancies were screened, and 500 eligible women were included in the final analysis. Data on pre-pregnancy weight, first-trimester weight, demographic characteristics, fasting plasma glucose, dietary energy intake, and physical activity were collected. Participants were categorized into low, appropriate, and excessive gestational weight gain groups according to weekly gestational weight gain during the first trimester. Multivariable logistic regression, ROC curve analysis, and sensitivity analyses across pre-pregnancy BMI strata were performed.
Results: The incidence of GDM (63.1%) and macrosomia (69.0%) was higher in excessive weight gain group. Excessive gestational weight gain in the first trimester was associated with higher odds of GDM (OR = 2.209, 95% CI: 1.313– 3.717) and macrosomia (OR = 2.103, 95% CI: 1.235– 3.579). Sensitivity analysis across BMI strata suggested a consistently elevated risk trend in the excessive weight gain group.
Conclusion: Excessive gestational weight gain during the first trimester was associated with higher risks of GDM and macrosomia. These findings suggest that first-trimester gestational weight gain may be useful as a potential early risk marker, although the conclusions should be interpreted cautiously and require confirmation in future prospective studies.
Keywords: first trimester, gestational weight gain, gestational diabetes mellitus, macrosomia, pregnancy management
Introduction
During gestation, one of the most common metabolic complications encountered is gestational diabetes mellitus (GDM), with a global prevalence of approximately 7%–25%. Multicenter studies in China have reported an incidence of around 14%–18%, showing an increasing trend year by year.1 GDM not only elevates the risk of gestational hypertension, polyhydramnios, cesarean delivery, and postpartum hemorrhage, but also significantly increases the risk of maternal type 2 diabetes mellitus and cardiovascular diseases after delivery.2 In addition, GDM has profound effects on fetal intrauterine development, often leading to excessive fetal growth and subsequently macrosomia.3 It has been reported that the incidence of macrosomia is about 8%–12% in the general population but rises to 15%–20% among women with GDM.4 Macrosomia markedly raises the risks of neonatal hypoglycemia, obesity, metabolic syndrome, and type 2 diabetes mellitus in adulthood.5 Therefore, early identification and intervention in high-risk populations during pregnancy are of great importance for reducing adverse maternal and neonatal outcomes.
Gestational weight gain is an important and modifiable indicator during pregnancy, closely related to maternal glucose homeostasis and fetal growth. Excessive gestational weight gain is strongly correlated with increased risks of GDM and macrosomia.6,7 However, most previous studies have focused on weight changes in mid-to-late pregnancy, whereas evidence on gestational weight gain during the first trimester (≤13 gestational weeks) remains limited. The first trimester is a critical stage of rapid embryonic and placental development, during which changes in maternal energy metabolism and insulin sensitivity may influence subsequent glucose regulation and fetal growth. Therefore, gestational weight gain during the first trimester may serve as an early marker of later risks of GDM and macrosomia, although its clinical significance requires further clarification.
Moreover, the association between first trimester gestational weight gain and pregnancy outcomes may be influenced by a woman’s pre-pregnancy body mass index (BMI). Previous research has suggested that patterns of weight gain and associated metabolic risks differ between women who are underweight or obese before pregnancy, indicating that the association between gestational weight gain in the first trimester and the risks of GDM and macrosomia may vary across BMI categories.8 Therefore, incorporating pre-pregnancy BMI into the risk assessment of first trimester weight gain may help develop individualized intervention strategies.
Based on the above background, this study aimed to evaluate the association between first-trimester gestational weight gain and the risks of GDM and macrosomia, and to perform stratified analyses according to pre-pregnancy BMI in order to further clarify its potential clinical value as an early risk marker. We hypothesized that greater gestational weight gain in the first trimester would be associated with higher risks of GDM and macrosomia, and that this association might differ across pre-pregnancy BMI categories.
Materials and Methods
Study Population
We conducted a single-center retrospective cohort study. During the study period, 516 women with singleton pregnancies were initially screened from the obstetric record-establishment database of our hospital between January 2022 and January 2025, of whom 500 were ultimately included in the final analysis. The detailed selection process is shown in Figure 1.
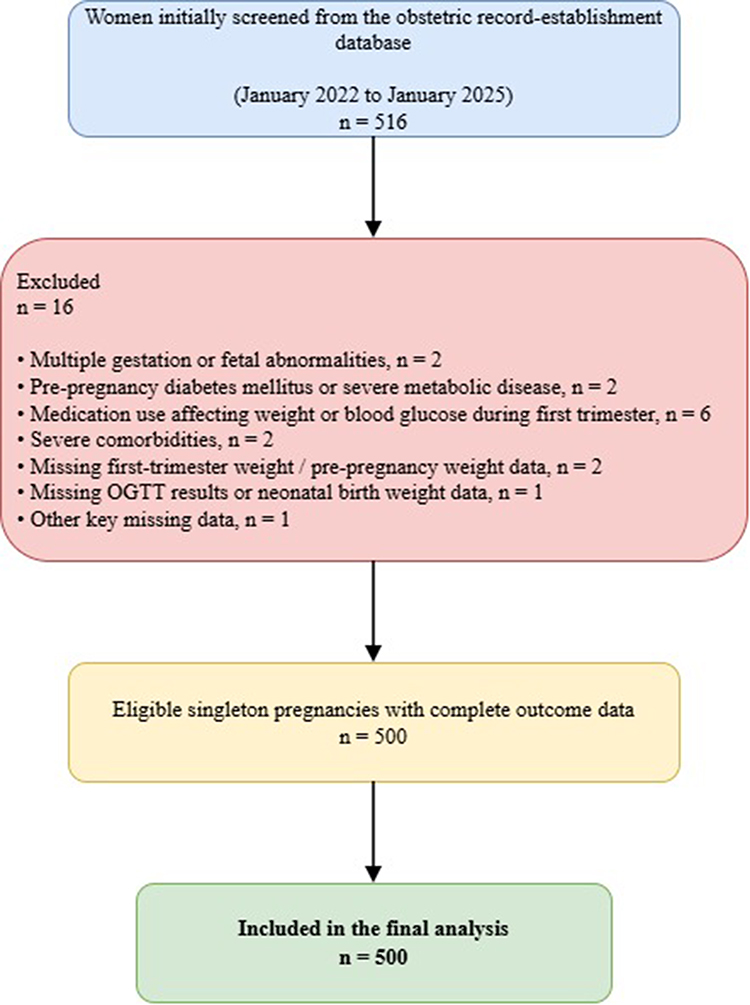 |
Figure 1 Flowchart of participant selection. |
Inclusion criteria were as follows: (1) established records during first trimester (≤13 weeks) with available pre-pregnancy weight or first-visit weight; (2) followed up until delivery with complete pregnancy outcomes, including the diagnosis of GDM and neonatal birth weight; (3) aged 18–45 years; (4) no history of diabetes mellitus or severe endocrine/metabolic diseases; (5) availability of pregnancy weight, dietary, and physical activity data.
Exclusion criteria included: (1) multiple gestation or fetal abnormalities; (2) pre-pregnancy diabetes mellitus or other severe metabolic diseases; (3) use of medications affecting weight or blood glucose during first trimester (eg., glucocorticoids, insulin); (4) severe comorbidities (eg., cardiovascular diseases, active autoimmune diseases); (5) missing key data.
Ethical approval was obtained from the Institutional Review Board of the Hospital of Chengdu University of Traditional Chinese Medicine (Approval No. 2025KL-249). As this was a retrospective study based on routinely collected clinical data, the requirement for written informed consent was waived by the ethics committee. The manuscript was prepared in accordance with the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) recommendations. The primary endpoint was GDM, with an estimated overall incidence of approximately 18%, including about 120 cases in the excessive weight gain group. Based on the approximation for two independent proportions (two-sided α = 0.05, power = 80%), the study was powered to detect an effect size of approximately two-fold risk of GDM. Considering multivariable logistic regression analysis (about 90 events, events per variable ≈ 10) and potential missing data, a final sample size of 500 participants was determined to ensure sufficient statistical power for the primary analyses.
Grouping and Definitions
Participants were grouped according to weekly gestational weight gain during the first trimester, estimated as weight change (kg) divided by gestational weeks at measurement. Participants were then categorized into low, appropriate, and excessive gain groups using BMI-specific reference ranges adapted from the 2009 Institute of Medicine gestational weight gain framework.9 Because universally accepted cutoffs for weekly gestational weight gain during the first trimester are lacking, these categories were used as study-specific operational definitions for exploratory analysis. Specifically, the three categories were defined as follows: (1) low gain group: underweight <0.08 kg/week; normal weight/overweight/obese <0.04 kg/week; (2) appropriate gain group: underweight 0.08–0.15 kg/week; normal weight/overweight 0.04–0.15 kg/week; obese 0.04–0.08 kg/week; and (3) excessive gain group: underweight/normal weight/overweight >0.15 kg/week; obese >0.08 kg/week.
Outcomes and Data Collection
The primary outcome was GDM, diagnosed according to the oral glucose tolerance test (OGTT) performed at 24–28 weeks of gestation following established criteria.10 The secondary outcome was macrosomia, defined as birth weight ≥4000 g.
Pre-pregnancy weight was obtained from the obstetric record-establishment files, primarily based on self-reported pre-pregnancy weight recorded at the first prenatal visit. When pre-pregnancy weight was unavailable, the first-visit weight was used as a proxy, as specified in the eligibility criteria. Maternal demographic and clinical data collected included: age, pre-pregnancy BMI, family history of diabetes mellitus (presence of diabetes in parents or siblings), gravidity/parity, fasting plasma glucose (FPG) in first trimester, blood pressure, smoking history and passive smoking exposure (yes/no), and socioeconomic indicators (educational level). Pregnancy-related behavioral factors included dietary intake and physical activity. Dietary intake and physical activity information were extracted from routinely recorded obstetric record-establishment forms in the medical records. Pregnancy-related behavioral factors included dietary intake and physical activity, both of which were extracted from routinely recorded obstetric record-establishment forms in the medical records. Dietary intake was assessed using a three-day 24-hour dietary recall documented at the time of record establishment, from which average daily energy intake was calculated. Physical activity was assessed using a standardized obstetric questionnaire routinely completed during record establishment, which recorded the total weekly duration (minutes/week) of moderate-to-vigorous activities during the first trimester, such as walking, brisk walking, and prenatal exercises. All data were reviewed by trained researchers before entry into the electronic database to ensure completeness and accuracy.
Quality Control
To minimize selection bias, all potentially eligible women in the obstetric record-establishment database during the predefined study period were screened using the same prespecified inclusion and exclusion criteria. All data were collected and entered into the electronic database by trained researchers to ensure accuracy and completeness. Maternal weight at the first prenatal visit was measured by trained medical staff using a calibrated electronic scale with an accuracy of 0.1 kg according to routine obstetric practice in our hospital. Because this was a retrospective study based on routinely collected clinical data, detailed information such as clothing status and bladder status at the time of weighing was not consistently available in the medical records. Data were double-entered and checked for logical consistency. Before analysis, completeness of the core exposure, outcome, and covariate variables was assessed. In the final analytic cohort of 500 women, no missing values were found in the variables included in the main analyses; therefore, no additional imputation procedure was required. Outliers and influential points were also examined.
Statistical Analysis
Statistical processing employed R software (v4.3.0, R Foundation for Statistical Computing, Vienna, Austria) together with SPSS software (v26.0, IBM Corp., Armonk, NY, USA). A two-sided P<0.05 was considered statistically significant. Continuous variables were first tested for normality. Data following a normal distribution are expressed as mean ± SD and compared among groups via one-way ANOVA. Skewed continuous data are reported as median (IQR) and evaluated using the Kruskal–Wallis test. Categorical data are presented as frequency (percentage) and analyzed using χ2 or Fisher’s exact tests as appropriate. To evaluate the association between gestational weight gain during the first trimester and pregnancy outcomes, separate multivariable logistic regression models were constructed for GDM and macrosomia. Sensitivity analyses included: (1) repeating analyses stratified by pre-pregnancy BMI; (2) excluding women with severe early-pregnancy comorbidities; and (3) substituting absolute weight gain for weekly gestational weight gain during the first trimester. For trend analyses across BMI-stratified groups, the Cochran–Armitage test for trend was employed. All tests were two-sided, and statistical significance was confirmed when p < 0.05.
Results
Comparison of Baseline Characteristics
Baseline maternal age, gravidity, parity, FPG, systolic blood pressure, dietary energy intake, exercise time, family history of diabetes mellitus, smoking, passive smoking, and educational level did not differ significantly among the three groups (all P > 0.05). Pre-pregnancy BMI was significantly different among groups (F = 6.417, P = 0.002). The groups also differed substantially in absolute weight change during the first trimester and in weekly gestational weight gain (both P < 0.001), whereas gestational weeks at weight assessment were comparable across groups (P = 0.751), indicating that the between-group difference in weekly gestational weight gain was mainly driven by actual weight change rather than timing of assessment (Table 1).
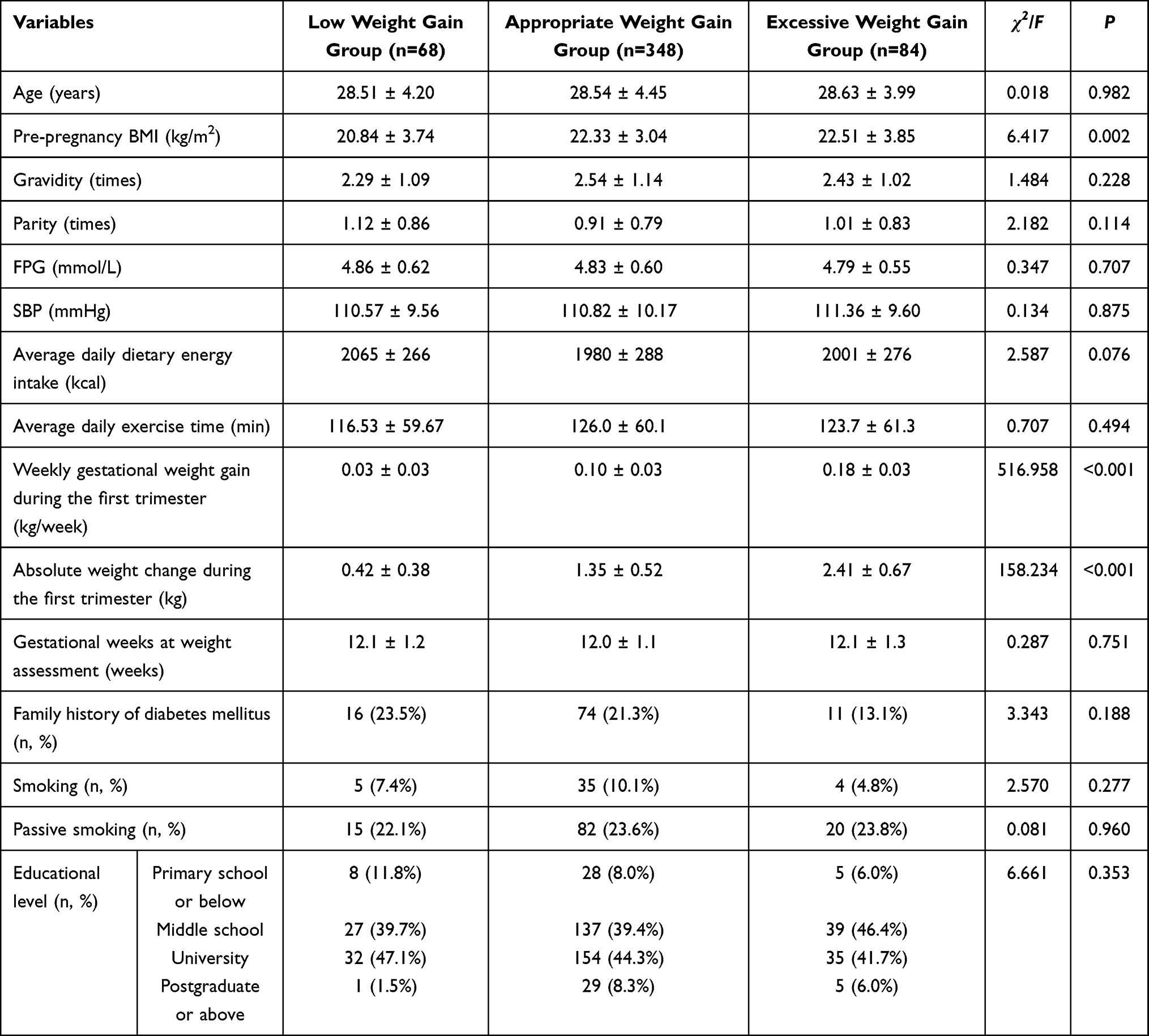 |
Table 1 Comparison of Baseline Characteristics |
Distribution of Pregnancy Outcomes
Regarding outcomes, the incidence of GDM and macrosomia differed significantly among the three groups (P < 0.05). Specifically, the excessive weight gain group had significantly higher incidences of both GDM and macrosomia compared with the appropriate and low gain groups (P < 0.05) (Table 2).
 |
Table 2 Distribution of Pregnancy Outcomes According to Early Gestational Weight Gain Rate |
Association Between First-Trimester Gestational Weight Gain and GDM
Multivariable logistic regression analysis (Model 1) was conducted, which aims to assess the association between gestational weight gain during the first trimester and GDM. The dependent variable was GDM (0 = no, 1 = yes). The main independent variable was first-trimester weight gain group (1 = low gain, 2 = appropriate gain [reference], 3 = excessive gain). Covariates included age, pre-pregnancy BMI, family history of diabetes mellitus, FPG, dietary energy intake, and physical activity. In the preliminary model, dietary energy intake and physical activity had coefficients close to zero and non-significant P values (β ≈ 0, P > 0.8); therefore, these variables were excluded from the final model to improve stability and interpretability. After adjustment, excessive gestational weight gain during the first trimester was significantly associated with higher odds of GDM (odds ratio [OR]=2.209, 95% confidence interval [CI]: 1.313–3.717, P = 0.003), while the low gain group showed no significant difference compared with the reference group (OR =1.371, 95% CI: 0.784–2.397, P = 0.268). Pre-pregnancy BMI was also independently associated with GDM (OR =1.166, 95% CI: 1.098–1.238, P < 0.001). Collinearity analysis indicated that all variance inflation factors (VIFs) were less than 2, suggesting no evident multicollinearity (Table 3).
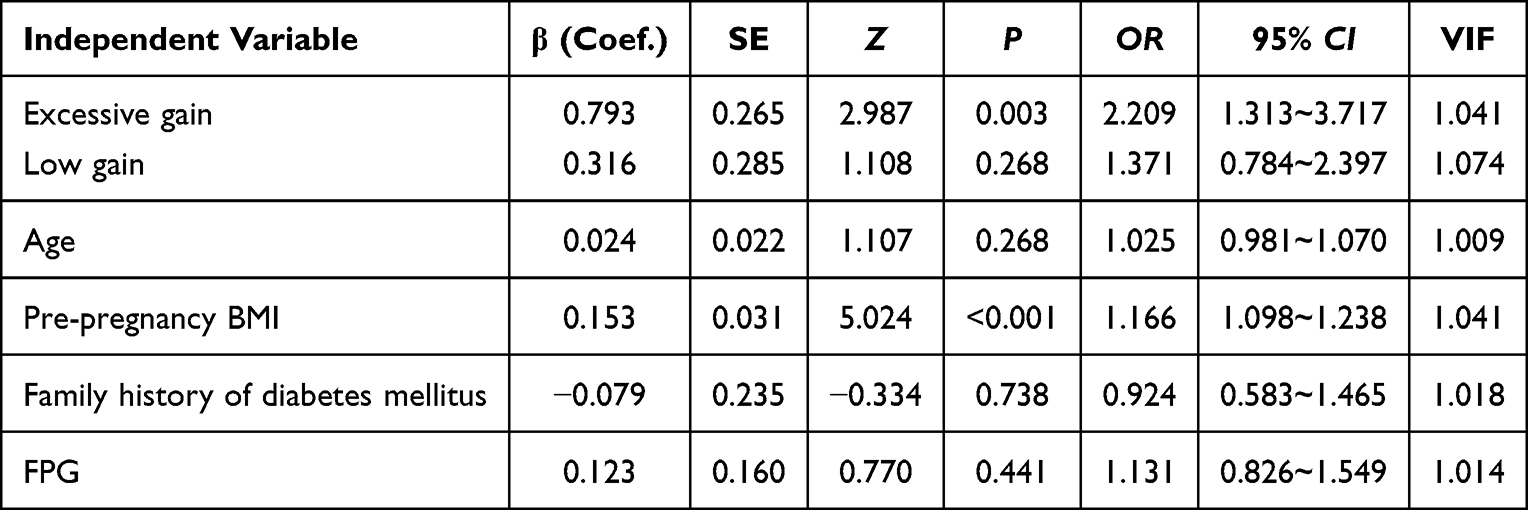 |
Table 3 Multivariate Logistic Regression Analysis of the Effect of Early Gestational Weight Gain Rate on the Risk of GDM (Model 1) |
Association Between First-Trimester Gestational Weight Gain and Macrosomia
We applied multivariable logistic regression (Model 2) to evaluate whether gestational weight gain during the first trimester was independently associated with macrosomia. The dependent variable was macrosomia (0 = no, 1 = yes). Independent variables and covariates were set consistent with the GDM analysis. As in Model 1, dietary energy intake and physical activity were excluded in the final model.
Excessive gestational weight gain during the first trimester was significantly associated with higher odds of macrosomia (β = 0.743, standard error [SE] = 0.271, z = 2.738, P = 0.006; OR = 2.103, 95% CI: 1.235–3.579). The low gain group did not differ significantly from the reference group (β = 0.389, SE = 0.285, z =1.366, P = 0.172; OR =1.475, 95% CI: 0.844–2.577). Additionally, both maternal age and pre-pregnancy BMI had significant positive associations with macrosomia (age: β = 0.069, P = 0.002; pre-pregnancy BMI: β = 0.154, P<0.001), suggesting that increases in these factors were linked to a higher risk of macrosomia. Family history of diabetes mellitus and FPG were not significantly associated with macrosomia (P > 0.4). Collinearity analysis confirmed that all VIFs were less than 2, with no evidence of multicollinearity (Table 4).
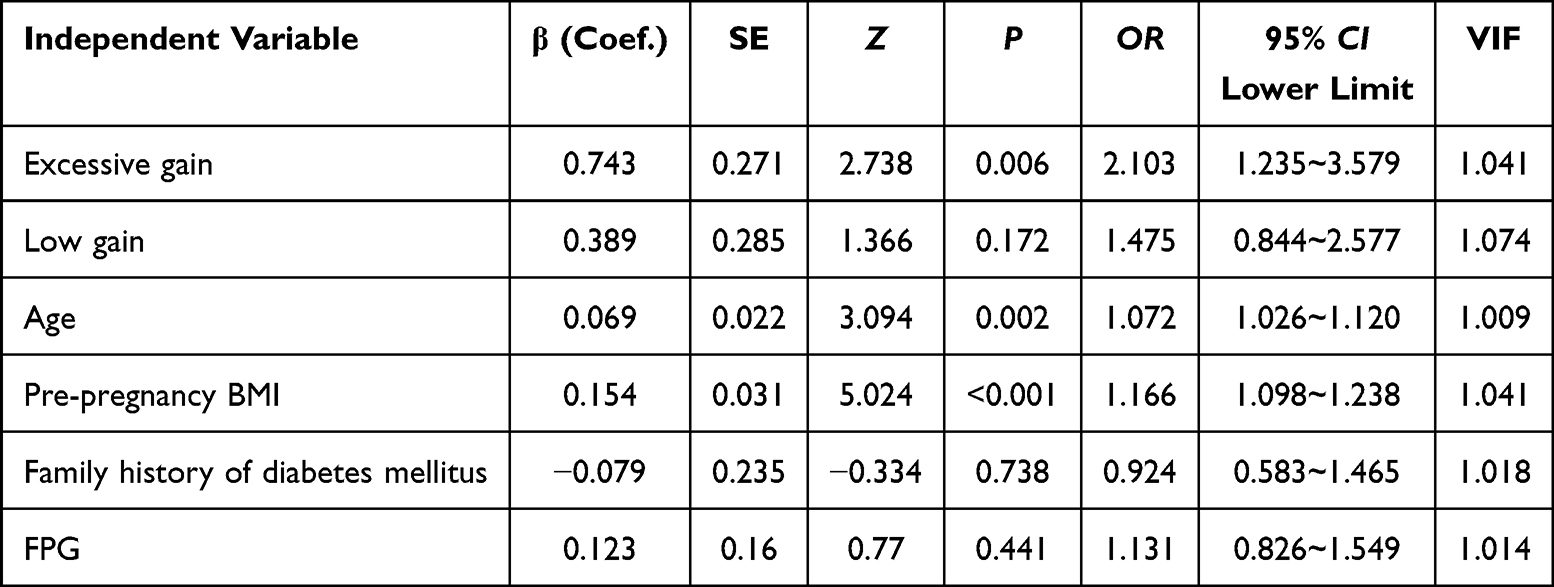 |
Table 4 Multivariate Logistic Regression Analysis of the Effect of Early Gestational Weight Gain Rate on the Risk of Macrosomia (Model 2) |
ROC Curve Analysis on Impacts of Pre-Pregnancy Weight Gain on GDM and Macrosomia
ROC curve analysis based on Model 1 indicated moderate predictive ability for GDM (AUC = 0.682, 95% CI: 0.634–0.723). Similarly, Model 2 showed moderate predictive ability for macrosomia (AUC = 0.667, 95% CI: 0.620–0.712) (Figure 2).
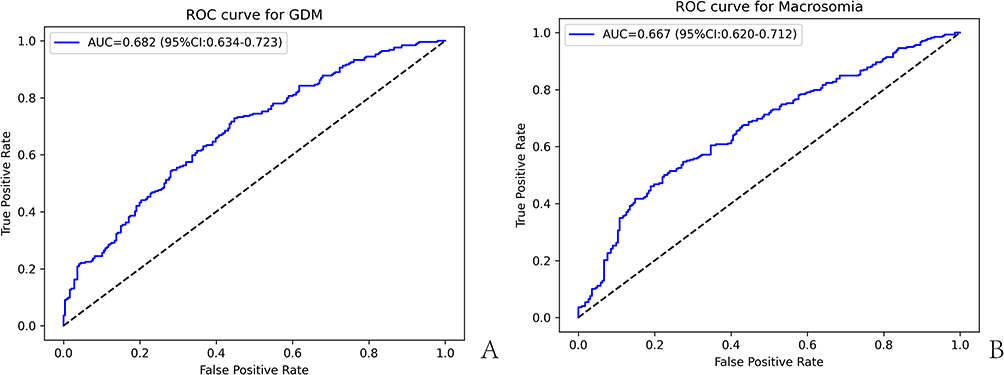 |
Figure 2 ROC curve analysis of the predictive value of first-trimester gestational weight gain for GDM and macrosomia. Note: (A) ROC curve of Model 1 for predicting GDM; (B) ROC curve of Model 2 for predicting macrosomia. |
Sensitivity Analysis Stratified by Pre-Pregnancy BMI
The stratified sample sizes were as follows: underweight, n = 73; normal weight, n = 285; overweight, n = 116; obese, n = 26. Across all BMI categories, the excessive weight gain group consistently showed higher incidences of GDM and macrosomia compared with the appropriate gain group, with more pronounced differences in the normal and overweight categories (normal weight group: GDM 59.5% vs. 48.4%, macrosomia 69.0% vs. 48.4%; overweight group: GDM 66.7% vs. 56.0%, macrosomia 81.0% vs. 66.7%). In the underweight group, the excessive gain subgroup showed higher GDM incidence (64.3% vs. 20.0%), while the low gain subgroup also exhibited a relatively high macrosomia rate (45.8%), suggesting that overly restricted weight gain in underweight women may also entail adverse risks. In the obese group, overall incidence rates were high, with the excessive gain subgroup showing the greatest risks (GDM 71.4%, macrosomia 71.4%), consistent with the primary analysis.
Statistical analysis demonstrated a significant difference in GDM incidence within the overweight group (P = 0.006), and a significant difference in macrosomia incidence within the normal weight group (P = 0.043). Trend analyses using the Cochran–Armitage test indicated that, except for a few non-significant strata, increasing gestational weight gain during the first trimester was associated with higher risks of GDM and macrosomia (Table 5). Overall, the sensitivity analyses suggested that excessive first trimester weight gain was consistently linked to increased risks of GDM and macrosomia, while insufficient gain in underweight women might also confer potential risks.
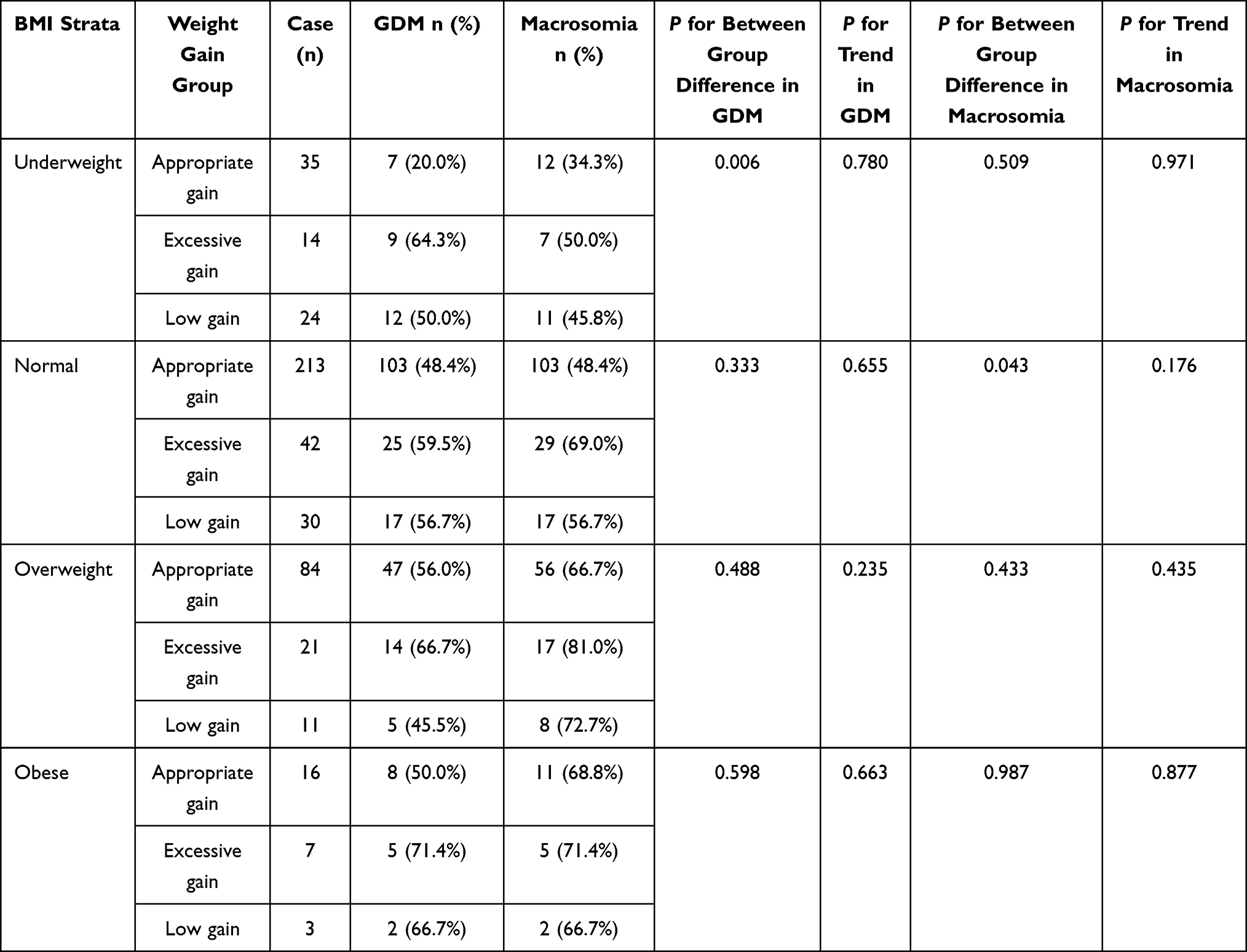 |
Table 5 Sensitivity Analysis of Early Gestational Weight Gain Rate and the Risks of GDM and Macrosomia Stratified by Pre-Pregnancy BMI |
Discussion
During pregnancy, weight management impacts on pregnancy outcomes. The first trimester is a critical stage for placental development, embryonic organogenesis, and maternal metabolic adaptation. Abnormal rates of weight gain during this period may affect insulin sensitivity, glycemic regulation, and placental nutrient transport, thereby increasing the risk of gestational GDM and macrosomia.11 Previous studies have mainly focused on the association between total gestational weight gain and pregnancy outcomes, while the potential role of gestational weight gain during the first trimester and its modifying effect in women with different pre-pregnancy BMI categories have been relatively underexplored. In this study, we employed multivariable logistic regression and stratified sensitivity analyses to investigate the association between gestational weight gain during the first trimester and the risks of GDM and macrosomia, thereby adding to the limited evidence on its potential value as an early risk marker for adverse pregnancy outcomes.
This retrospective analysis of 500 singleton pregnancies examined the association between first-trimester gestational weight gain and the risks of GDM and macrosomia. Our findings showed that excessive gestational weight gain in the first trimester was associated with higher risks of GDM and macrosomia. Moreover, in women with low pre-pregnancy BMI, inadequate weight gain may also pose potential risks. Multivariate logistic regression analysis showed that the association of excessive first-trimester gestational weight gain with GDM and macrosomia remained significant after adjusting for age, pre-pregnancy BMI, family history of diabetes, and FPG. ROC curve analysis further indicated that weekly gestational weight gain during the first trimester had moderate predictive ability for GDM and macrosomia. Stratified sensitivity analyses revealed that underweight women with low weight gain had a slightly higher incidence of macrosomia, while overweight and obese women in the excessive gain group demonstrated the highest risks. These results suggest that pre-pregnancy nutritional status may influence the observed association between first-trimester gestational weight gain and pregnancy outcomes. However, given the retrospective observational design of the present study, these mechanistic considerations should be interpreted as possible biological explanations for the observed associations rather than definitive causal inferences.
Several biologically plausible mechanisms may help explain the observed association between greater gestational weight gain in the first trimester and higher risks of GDM and macrosomia. Excessive weight gain may exacerbate first trimester insulin resistance, leading to hyperglycemia and subsequently elevating the likelihood of developing GDM. Concurrently, excessive adipose tissue accumulation may trigger inflammatory responses, elevating levels of mediators such as tumor necrosis factor-α (TNF-α) and interleukin-6 (IL-6), which interfere with insulin signaling and further aggravate glucose metabolism abnormalities.12 In addition, maternal hyperglycemia may enhance placental glucose and lipid transport, thereby promoting fetal overgrowth and macrosomia.13 Interestingly, our sensitivity analysis also indicated that insufficient weight gain in underweight women may paradoxically increase the risk of macrosomia, possibly due to adaptive placental alterations or hemodynamic adjustments in the setting of maternal undernutrition. This finding is consistent with previous reports suggesting that overly restrictive weight control in underweight women may increase the risk of adverse fetal outcomes.14
Most prior research has emphasized weight gain during the second trimester or total gestational weight gain,15 whereas evidence specifically addressing the clinical relevance of first-trimester gestational weight gain remains relatively limited. This study adds to the limited observational evidence suggesting that gestational weight gain during the first trimester may be associated with subsequent risks of GDM and macrosomia, and further suggests that these associations may differ across pre-pregnancy BMI categories. These results underscore the importance of individualized management. The persistence of significant associations after multivariate adjustment strengthens the reliability of our findings and provides a rationale for first trimester interventions.
Previous studies have reported that in some countries, the incidence of macrosomia among women with GDM declined between 2012 and 2021, but remained higher compared with non-GDM women, suggesting that gestational weight management still requires reinforcement.16 Our findings indicate that weight management during first trimester should be a priority for obstetric interventions. Pregnant women should establish a baseline weight early in gestation and undergo regular monitoring of weight gain velocity to promptly identify both excessive and insufficient gain. Individualized weight management goals should be developed according to pre-pregnancy BMI. For example, underweight women should avoid overly restrictive weight control, while overweight and obese women should prevent rapid weight gain. Comprehensive interventions involving balanced diet, moderate physical activity, and health education throughout pregnancy may help reduce the risks of GDM and macrosomia.
It should also be noted that gestational weight gain during the second and third trimesters is a well-established factor associated with both GDM and macrosomia. In the present study, we specifically focused on gestational weight gain during the first trimester as an early risk marker; however, second- and third-trimester weight gain data were not further incorporated into the analysis. Therefore, the relative contribution of first-trimester versus later gestational weight gain could not be fully distinguished, and the observed findings should be interpreted as associative rather than causal. In addition, among women who developed GDM, subsequent glycemic control may also have influenced fetal growth and the occurrence of macrosomia, although this could not be further evaluated because detailed follow-up glycemic data were not consistently available in the present retrospective dataset.
Strengths and Limitation
This study systematically evaluated the association between first-trimester gestational weight gain and the risks of GDM and macrosomia, and further incorporated sensitivity analyses stratified by pre-pregnancy BMI, thereby providing additional evidence for individualized weight management in the first trimester. Our findings suggest that excessive first-trimester gestational weight gain was associated with higher risks of GDM and macrosomia, while overly restricted weight gain in underweight women may also be associated with potential adverse outcomes. These results may provide a useful reference for early maternal health education and weight monitoring strategies. Strengths of this study include the use of a relatively complete single-center cohort, rigorous data collection, multivariable adjustment, ROC-based evaluation of predictive performance, and sensitivity analyses that supported the robustness of the main findings. Nevertheless, several limitations should be acknowledged. First, the retrospective single-center design may be subject to selection bias and residual confounding, which may limit the generalizability of the findings. Second, pre-pregnancy weight was partly based on self-reported information recorded in the obstetric files, and weekly gestational weight gain during the first trimester was estimated from routinely recorded clinical measurements. Therefore, some degree of reporting or measurement error, as well as the inability to fully capture the potentially non-linear pattern of weight change within the first trimester, cannot be excluded. In addition, dietary and physical activity data were partly based on self-reported information, which may introduce information bias. Third, this study did not further account for gestational weight gain during the second and third trimesters, which are also well-established factors related to GDM and macrosomia. Therefore, the relative contribution of first-trimester versus later gestational weight gain could not be fully separated in the present analysis. Fourth, among women who developed GDM, post-diagnosis glycemic control may have substantially influenced fetal growth and the occurrence of macrosomia. However, detailed follow-up data on glycemic control, as well as management measures such as medical nutrition therapy, insulin, or hypoglycemic treatment, were not consistently available in this retrospective dataset. Therefore, residual confounding in the association between first-trimester gestational weight gain and macrosomia cannot be excluded. Future multicenter prospective studies with more comprehensive longitudinal metabolic and pregnancy management data are warranted to further validate these findings.
Conclusion
In this retrospective single-center study, excessive gestational weight gain in the first trimester was associated with higher risks of GDM and macrosomia, while pre-pregnancy BMI may modify these associations. These findings suggest that gestational weight gain in the first trimester may serve as a potential early risk marker; however, the conclusions should be interpreted cautiously, and further large-scale prospective studies are needed to confirm these findings.
Data Sharing Statement
The datas used and/or analyzed during the current study are available from the corresponding author.
Ethics Approval and Consent to Participate
The study was approved by the Ethics Committee of the Hospital of Chengdu University of Traditional Chinese Medicine (Approval No. 2025KL-249). As this was a retrospective study based on routinely collected clinical data, the requirement for written informed consent was waived by the ethics committee. All procedures were conducted in accordance with the Declaration of Helsinki and institutional guidelines.
Author Contributions
Dan Yang and Zhi Yu are regarded as co-first authors.
Dan Yang: Conceptualization, Data curation, Formal analysis, Writing–original draft.
Zhi Yu: Formal analysis, Methodology, Data curation, Writing–original draft.
Jin Chen: Supervision, Validation, Writing–review & editing.
Lin Zhuang: Visualization, Data curation, Writing–review & editing.
Xiaoyin Wang: Project administration, Investigation, Supervision, Writing–review & editing.
All authors gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
The authors declare that no funding was received for this study.
Disclosure
The authors declare no conflict of interest.
References
1. Juan J, Yang H. Prevalence, prevention, and lifestyle intervention of gestational diabetes mellitus in China. Int J Environ Res Public Health. 2020;17(24). doi:10.3390/ijerph17249517
2. Sweeting A, Wong J, Murphy HR, Ross GP. A clinical update on gestational diabetes mellitus. Endocr Rev. 2022;43(5):763–11. doi:10.1210/endrev/bnac003
3. Ye W, Luo C, Huang J, Li C, Liu Z, Liu F. Gestational diabetes mellitus and adverse pregnancy outcomes: systematic review and meta-analysis. BMJ. 2022;377:e067946. doi:10.1136/bmj-2021-067946
4. Ugwudike B, Kwok M. Update on gestational diabetes and adverse pregnancy outcomes. Curr Opin Obstet Gynecol. 2023;35(5):453–459. doi:10.1097/gco.0000000000000901
5. Akanmode AM, Mahdy H. Macrosomia. In: StatPearls. Treasure Island (FL): StatPearls Publishing, LLC, 2025
6. Liu N, Lyu J, Wang H, et al. Weekly weight gain in women with gestational diabetes mellitus and neonatal birth weight - China, 2011-2021. China CDC Wkly. 2023;5(32):703–709. doi:10.46234/ccdcw2023.135
7. Zheng Q, Zhu Y, Jiang X, Huang L, Li J, Liu R. The exploration of optimal gestational weight gain after oral glucose tolerance test for Chinese women with gestational diabetes mellitus. Sci Rep. 2024;14(1):1466. doi:10.1038/s41598-024-51879-x
8. Long J, Chu Z, Xiao Y, et al. Impact of pre-pregnancy body mass index and gestational weight gain on pregnancy complications and outcomes. Int J Gen Med. 2025;18:4057–4067. doi:10.2147/ijgm.S526688
9. Institute of M, National Research Council Committee to Reexamine IOMPWG. The national academies collection: reports funded by national institutes of health. In: Rasmussen KM, Yaktine AL, editors. Weight Gain During Pregnancy: Reexamining the Guidelines. Washington (DC): National Academies Press (US), National Academy of Sciences; 2009.
10. Davidson KW, Barry MJ, Mangione CM, et al. Screening for gestational diabetes: US preventive services task force recommendation statement. JAMA. 2021;326(6):531–538. doi:10.1001/jama.2021.11922
11. Hernández-Baraza L, Brito-Casillas Y, Valverde-Tercedor C, et al. Mechanisms of fetal overgrowth in gestational diabetes: the potential role of SOCS2. Nutrients. 2025;17(9). doi:10.3390/nu17091519
12. Li G, Xing Y, Wang G, et al. Differential effect of pre-pregnancy low BMI on fetal macrosomia: a population-based cohort study. BMC Med. 2021;19(1):175. doi:10.1186/s12916-021-02046-w
13. Bernea EG, Uyy E, Mihai D-A, et al. New born macrosomia in gestational diabetes mellitus. Exp Ther Med. 2022;24(6):710. doi:10.3892/etm.2022.11646
14. Parveen N, Iqbal N, Batool A, Mahmoud T, Ali S. Macrosomia predictors and pregnancy outcomes in Gestational Diabetes patients: an observational study from Ha’il, Saudi Arabia. Pak J Med Sci. 2022;38(5):1126–1131. doi:10.12669/pjms.38.5.5809
15. Parra-Cabrera MS, Delgado-Ramírez JZ, Ángeles–Llerenas AR, Hurtado-Salgado E, Méndez Gómez-Humarán I. Weight gain during pregnancy and the probability of macrosomia in women with gestational diabetes. Salud Pública de México. 2024;66(6 (nov–dec)):807–815. doi:10.21149/15577
16. He LR, Yu L, Guo Y. Birth weight and large for gestational age trends in offspring of pregnant women with gestational diabetes mellitus in southern China, 2012-2021. Front Endocrinol. 2023;14(1166533). doi:10.3389/fendo.2023.1166533
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
The Association Between the Imbalance of Single-Carbon Nutrients in Early Pregnancy and Gestational Diabetes Mellitus Risk is Influenced by Serum Selenium Status: A Cohort Study
Liu PJ, Ma L, Li R, Liu Y
Diabetes, Metabolic Syndrome and Obesity 2023, 16:3275-3283
Published Date: 20 October 2023
Serum D-Dimer, Glycated Serum Protein, and HbA1c Levels in Predicting Macrosomia in Gestational Diabetes Mellitus
Quan Y, Wang Y
Diabetes, Metabolic Syndrome and Obesity 2025, 18:2913-2921
Published Date: 15 August 2025
The Role of METS-IR in Early Screening for Gestational Diabetes Mellitus in Chinese Women: A Two-Center Prospective Study
Gao J, Song S, Duo Y, Wang S, Qiao X, Zhang Y, Xu J, Zhang J, Nie X, Sun Q, Yang X, Wang A, Sun W, Fu Y, Zhang M, Dong Y, Lu Z, Yuan T, Zhao W
Diabetes, Metabolic Syndrome and Obesity 2025, 18:3967-3984
Published Date: 25 October 2025
Predictive Value of Placental Growth Factor and Soluble FMS-Like Tyrosine Kinase-1 Detection in Early Pregnancy for Gestational Diabetes Mellitus: A Case-Control Study
Wu W, Liu X
International Journal of Women's Health 2026, 18:542217
Published Date: 10 February 2026
Predictive Value of the second-Trimester Triglyceride-Glucose Index and Its Derived Indices for Macrosomia in Gestational Diabetes Mellitus

Chen Y, Li S, Xiang L, Zhu Y, Zeng Y, Chen Y, Zhong T
Diabetes, Metabolic Syndrome and Obesity 2026, 19:577687
Published Date: 23 April 2026