Back to Journals » Nature and Science of Sleep » Volume 17

Predictive Value of Neutrophil-to-Lymphocyte Ratio for Cerebral Infarction in Obstructive Sleep Apnea: A Nomogram-Based Analysis
Authors Hou Z, Chen C, Liu H, Wang Y, Li Z
Received 4 May 2025
Accepted for publication 26 July 2025
Published 6 August 2025 Volume 2025:17 Pages 1777—1787
DOI https://doi.org/10.2147/NSS.S536799
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Ahmed BaHammam
Ziwei Hou,1 Chen Chen,2 Hong Liu,2 Yunpeng Wang,3 Zongxuan Li1
1Academy of Medical Sciences, Shanxi Medical University, Taiyuan, People’s Republic of China; 2Neurology Department, The Affiliated Cardiovascular Hospital of Shanxi Medical University, Taiyuan, People’s Republic of China; 3Clinical Discipline Construction Center, Shanxi Medical University, Taiyuan, People’s Republic of China
Correspondence: Chen Chen, Shanxi Cardiovascular Hospital Affiliated to Shanxi Medical University, 18 Yifen Street, Taiyuan, 030024, People’s Republic of China, Email [email protected]
Purpose: Obstructive sleep apnea (OSA) is associated with cerebral infarction (CIF) through inflammatory pathways. The neutrophil-to-lymphocyte ratio (NLR) serves as an inflammation biomarker, but its relationship with CIF in OSA patients remains unclear.
Methods: A total of 188 OSA patients from The Affiliated Cardiovascular Hospital of Shanxi Medical University (January 2022 to December 2023) were included, consisting of 68 patients with CIF (case group) and 120 without CIF (control group). Data on admission, biochemical tests, and clinical characteristics were collected and compared. Multivariate logistic regression and a nomogram model were employed to identify risk factors, evaluated using receiver operating characteristic (ROC) curves, calibration curves and decision curve analysis (DCA).
Results: Elevated log-transformed NLR (LnNLR), CRP, age, and reduced albumin levels were independently associated with increased CIF risk. The developed nomogram demonstrated excellent discriminative performance (AUC = 0.9372), superior to LnNLR alone (AUC = 0.665). At the optimal cutoff, the model achieved a sensitivity of 82.35% and specificity of 92.50%. Calibration plots showed good agreement between predicted and observed outcomes, and DCA confirmed the model’s potential clinical utility.
Conclusion: High NLR can be used as an emerging criterion for evaluating CIF risk in OSA. The nomogram model is capable of estimating CIF risk accurately, providing useful aid to clinical decision-making. The developed nomogram can be implemented in practice as an aid to help healthcare personnel identify high-risk OSA participants who would be offered early intervention in terms of increased monitoring and prophylaxis. External validation in larger, multi-center cohorts is warranted.
Keywords: cerebral infarction, obstructive sleep apnea, inflammation neutrophil-to-lymphocyte ratio, nomogram
A Letter to the Editor has been published for this article.
A Response to Letter by Dr Ma has been published for this article.
Introduction
Cerebral infarction (CIF), or ischemic stroke, results from impaired cerebral blood flow due to arterial occlusion, stenosis, or embolism, often secondary to atherosclerosis or cardiac sources.1,2 It remains a leading cause of disability and mortality worldwide. Obstructive sleep apnea (OSA), characterized by recurrent episodes of upper airway obstruction during sleep, has emerged as an independent risk factor for CIF.3 OSA contributes to vascular dysfunction through intermittent hypoxia, oxidative stress, and chronic inflammation, and is frequently comorbid with hypertension, diabetes, atrial fibrillation, and dyslipidemia—all of which further elevate cerebrovascular risk.4
OSA and CIF share overlapping pathophysiological mechanisms, including intermittent hypoxia, oxidative stress, systemic inflammation, and endothelial dysfunction. These factors promote atherogenesis, arterial plaque instability, and thrombus formation, increasing the risk of cerebrovascular events. Inflammatory markers such as C-reactive protein (CRP), interleukin-6 (IL-6), and IL-8 are frequently elevated in OSA patients and are known to activate pro-inflammatory and pro-thrombotic pathways.5
Among systemic inflammatory indicators, the neutrophil-to-lymphocyte ratio (NLR) has emerged as a simple, cost-effective, and reproducible biomarker that captures both neutrophil-mediated inflammation and lymphocyte-mediated immune suppression. Previous studies have demonstrated its predictive value in cardiovascular disease, atrial fibrillation, and all-cause mortality.6–8 However, its role in predicting cerebrovascular risk, particularly in OSA patients, remains insufficiently explored.
Recent evidence suggests that chronic inflammation may serve as a mechanistic link between OSA and CIF, yet there is a lack of clinically applicable tools to quantify this risk. To address this gap, we investigated the independent association between NLR and CIF in patients with OSA and developed a novel nomogram model that integrates inflammatory (CRP, NLR) and clinical (age, albumin) variables. We hypothesize that elevated NLR significantly contributes to CIF risk in OSA and that our model may enhance predictive performance and aid individualized clinical decision-making.
Materials and Methods
General Information
This retrospective analysis included 188 patients who were diagnosed with OSA at the Department of Neurology, The Affiliated Cardiovascular Hospital of Shanxi Medical University, from January 2022 to December 2023. The case group consisted of 68 individuals who had undergone a CIF, while the control group consisted of 120 patients who had not (Figure 1). According to the 1964 Declaration of Helsinki and its later revisions, the research was carried out as planned. This study was approved by Shanxi Cardiovascular Hospital’s Ethical Committee.
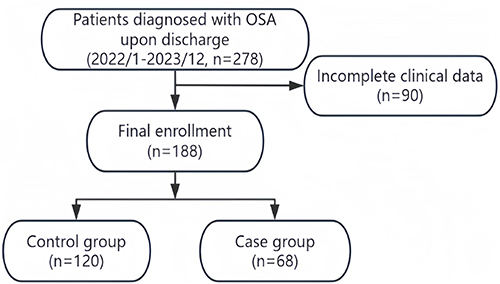 |
Figure 1 Flowchart of participants analyzed in this study. |
Inclusion criteria: Patients diagnosed with OSA, confirmed by full-night polysomnography (PSG), with an apnea-hypopnea index (AHI) ≥ 5 events/hour, in accordance with international guidelines. CIF was diagnosed based on standard clinical criteria,9 supported by neurological signs, symptoms, and imaging findings. To ensure temporal proximity, only patients whose CIF event occurred within six months before or after the diagnosis of OSA were included in the case group. This criterion was applied to minimize misclassification bias and to better reflect the potential pathophysiological link between the two conditions.
Exclusion criteria: Patients with severe liver, kidney, or other organ insufficiency, malignant tumors, hematological diseases, or those with consciousness or hearing impairments were excluded. Additionally, patients who had difficulty communicating with clinical staff, had transmissible infections, or incomplete medical histories were excluded. Patients with symptoms of infection, who had recently undergone surgery, or had autoimmune diseases were also excluded.
Clinical and Biochemical Assessment
All patients diagnosed with CIF had their general clinical information gathered from their electronic medical records. This included their gender, age, body mass index (BMI), smoking history, HT, alcohol use history, and diabetes mellitus (DM). All blood samples were collected in the early morning following 12 hours of fasting under standardized laboratory conditions. White blood cell count (WBC) and red blood cell distribution width coefficient of variation (RDW-CV) were measured as part of a routine blood test performed on a complete blood count analyzer (Sysmex XT1800i, Sysmex Corporation). Albumin (ALB), fasting blood glucose (FPG), total cholesterol (TC), triglycerides (TG), low-density lipoprotein cholesterol (LDL-C), and high-density lipoprotein cholesterol (HDL-C) were all quantified in a thorough biochemical panel. Also measured were C-reactive protein levels. Moreover, PSG’s Apnea-Hypopnea Index (AHI) was documented. To get the NLR, we divided the neutrophil count by the lymphocyte count (LYM) and then used the constant (e) to do a logarithmic transformation. Variables with P < 0.10 in univariate logistic regression or with known clinical relevance were included in the multivariate model.
Data Analysis
Statistical analysis was performed using SPSS (version 22.0). The Shapiro–Wilk test was applied to assess the normality of the distribution of continuous variables. Data were presented as mean ± standard deviation ( ), and group differences were evaluated using or non-parametric Mann–Whitney U-test. Due to the skewed distribution of NLR, a natural logarithmic transformation (LnNLR) was applied to improve normality and stabilize variance. Univariate logistic regressions were used to analyze for putative predictors of CIF, with subsequent analysis using multivariate logistic regression model to identify independent correlates of CIF. A nomogram prediction model based on results of analyses of multivariate logistic regressions was created using the rms package (version 4.4.3). Each of the multivariate logistic regression coefficients was normalized to a range of 0 to 100 points to serve as a foundation for developing the nomogram model. Total scores for all variables were calculated before subsequent conversion to prediction probability.
), and group differences were evaluated using or non-parametric Mann–Whitney U-test. Due to the skewed distribution of NLR, a natural logarithmic transformation (LnNLR) was applied to improve normality and stabilize variance. Univariate logistic regressions were used to analyze for putative predictors of CIF, with subsequent analysis using multivariate logistic regression model to identify independent correlates of CIF. A nomogram prediction model based on results of analyses of multivariate logistic regressions was created using the rms package (version 4.4.3). Each of the multivariate logistic regression coefficients was normalized to a range of 0 to 100 points to serve as a foundation for developing the nomogram model. Total scores for all variables were calculated before subsequent conversion to prediction probability.
An ROC curve is a graphical analysis used to assess diagnostic test performance, most notably in medicine. The ROC curve illustrates how performance of a continuous diagnostic test varies at all available diagnostic cut-off values by comparing sensitivity to specificity at different thresholds. The area under the ROC curve, denoted by AUC, is an important overall performance measure of a diagnostic test, with it mirroring how effectively the test identifies disease versus non-disease across various thresholds.
The calibration curve of the nomogram was employed to assess the accuracy of the predictive model. The curve was constructed by plotting the actual incidence against the predicted probability, with the predicted probability shown on the x-axis and the actual incidence on the y-axis. A reference line (y = x) was included as the line of perfect agreement. The model’s predictive ability was evaluated by visually inspecting how closely the calibration curve aligns with the reference line. A model with a calibration curve closer to this line demonstrates better predictive accuracy. Internal validation of the nomogram was conducted using bootstrap resampling (1000 iterations) to assess its predictive accuracy and calibration performance.
Results
Clinical Baseline Data
188 patients diagnosed with obstructive sleep apnea were included, comprising 135 males and 53 females. Within the studied population, 68 individuals presented with CIF, constituting the case group, whereas 120 individuals were identified without CIF, forming the control group. The average age of the CIF group was 61.6 years with a standard deviation of 9.6 years, while the non-CIF group exhibited an average age of 57.9 years with a standard deviation of 11.6 years. No notable variations were detected between the two cohorts regarding gender, BMI, smoking history, hypertension, diabetes mellitus, alcohol intake, WBC, RDW, NED, cholesterol levels, triglycerides, LDL, HDL, and fasting plasma glucose (P > 0.05). Nevertheless, notable variations were observed in the mean age, LYM, ALB, AHI, CRP, NLR, and logarithmic NLR (LnNLR) (P < 0.05) (Table 1).
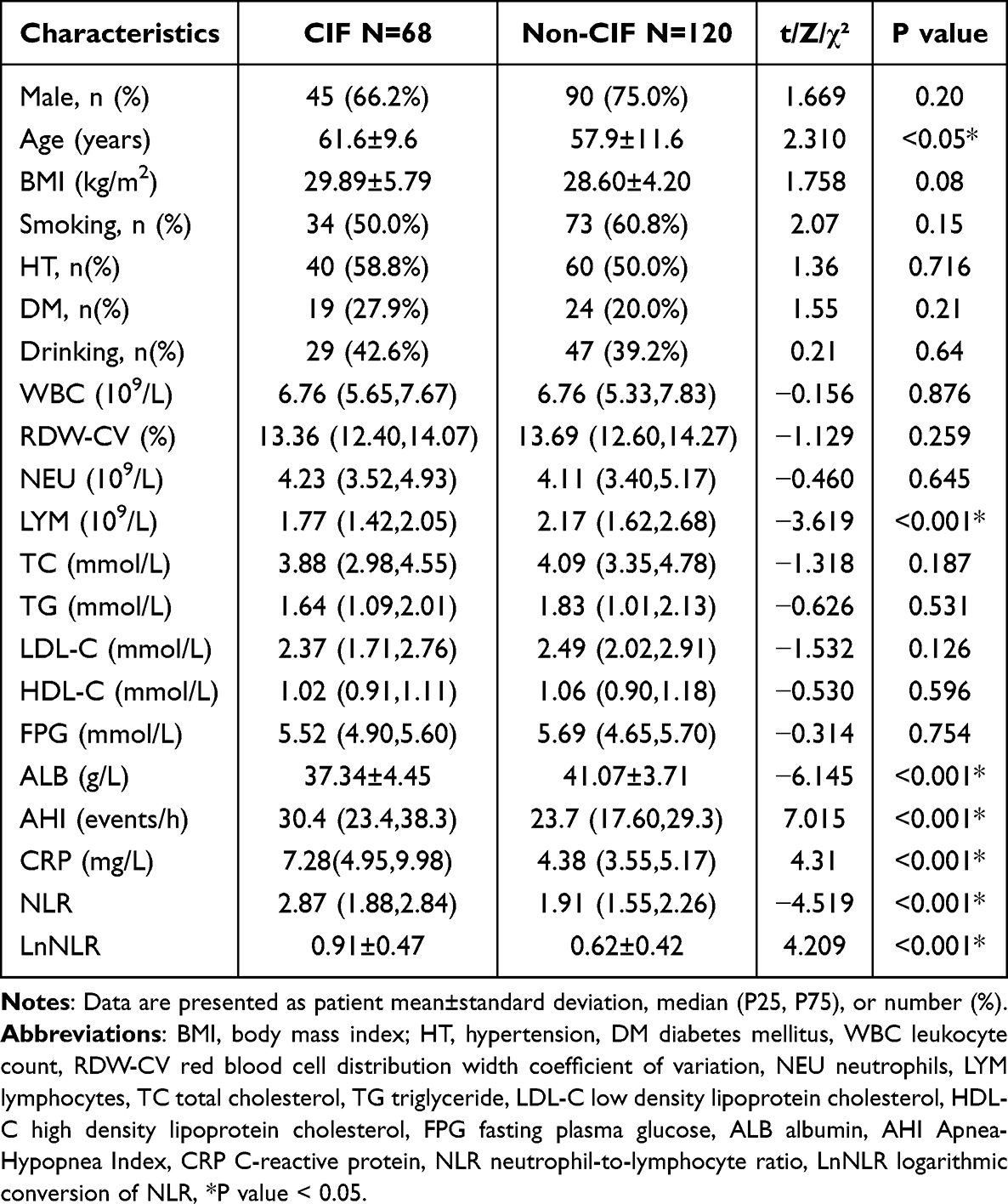 |
Table 1 Baseline Characteristics of Participants |
Independent Protective and Risk Factors for CIF in OSA
Comprehensive multiple regression analyses were conducted on the variables identified as significant through univariate regression analysis. In the context of univariate logistic regression, the variables age, LYM, ALB, AHI, CRP, and LnNLR exhibited independent associations with CIF in patients diagnosed with OSA. Nevertheless, following the execution of multivariate regression analysis, LYM and AHI ceased to exhibit independent associations with CIF risk. In contrast, age (OR, 1.057; 95% CI, 1.006–1.110; P = 0.029), ALB (OR, 0.727; 95% CI, 0.631–0.837; P < 0.001), CRP (OR, 3.289; 95% CI, 2.173–4.980; P < 0.001), and LnNLR (OR, 4.682; 95% CI, 1.149–19.070; P < 0.001) were identified as significant factors influencing the incidence of CIF in patients with OSA. Among these factors, age, CRP and LnNLR were recognized as contributors to the elevated risk of CIF in patients with OSA. Conversely, ALB was identified as protective factors, mitigating the risk of CIF. The findings are presented in Table 2 and Table 3, as well as in Figure 2.
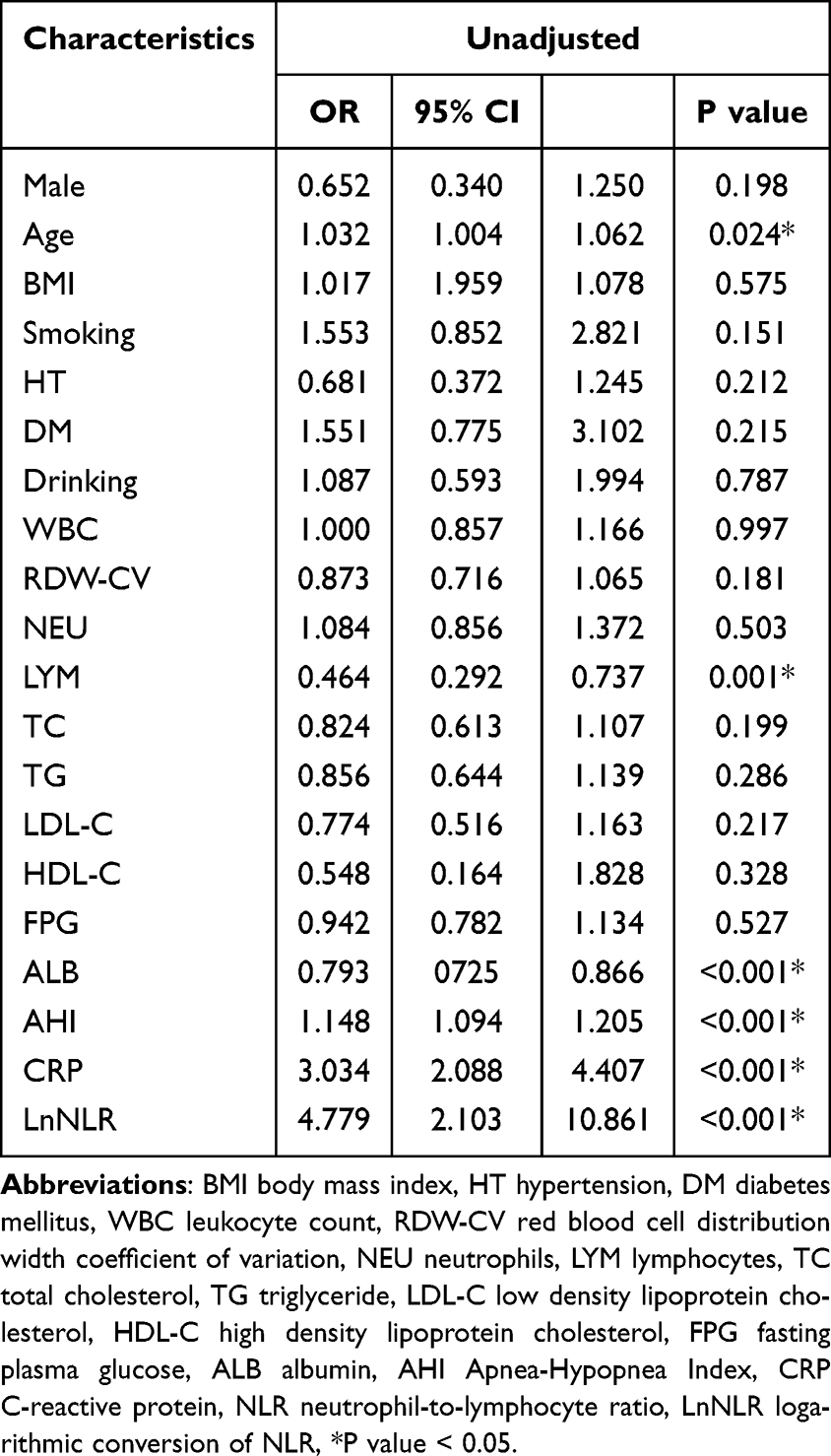 |
Table 2 Univariate Logistic Regression Analysis |
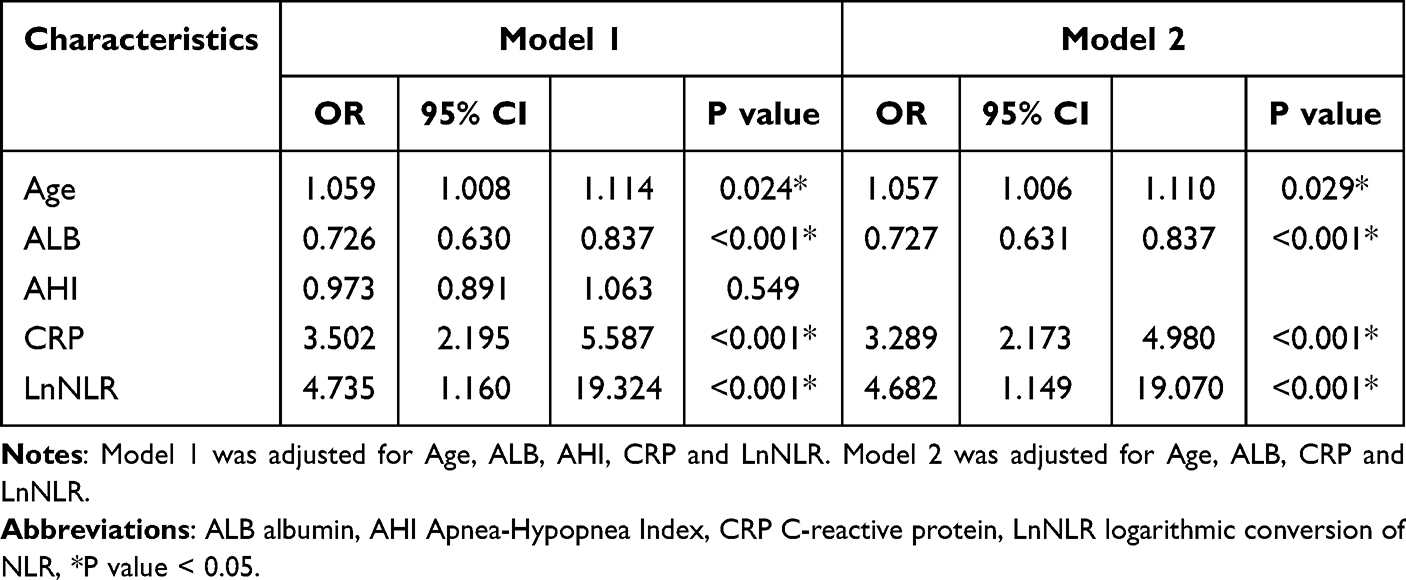 |
Table 3 Multivariate Logistic Regression Analysis |
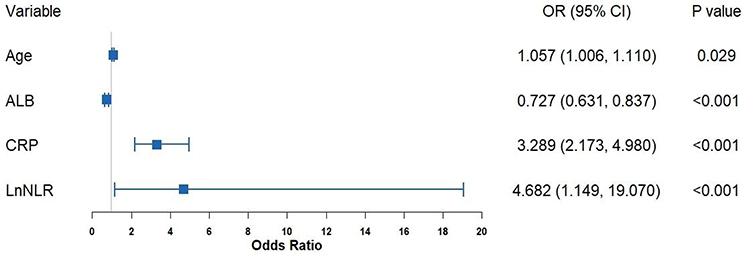 |
Figure 2 Forest plot of independently associated factors for CIF in OSA. |
Development and Validation of the CIF Predicting Nomogram
In multivariate logistic regression analysis, the variables of age (OR, 1.057; 95% CI, 1.006–1.110; P = 0.029), ALB (OR, 0.727; 95% CI, 0.631–0.837; P < 0.001), CRP (OR, 3.289; 95% CI, 2.173–4.980; P < 0.001), and LnNLR (OR, 4.682; 95% CI, 1.149–19.070; P < 0.001) demonstrated independent associations with the CIF. The variables were utilized to develop a nomogram aimed at evaluating the risk of CIF (Figure 3). The nomogram was subjected to internal validation through the bootstrap method (B = 1000 replications), revealing a high level of accuracy in predicting cumulative incidence function risk, evidenced by a concordance index of 0.9372 (95% CI, 0.8990–0.9754). The calibration plots demonstrated a strong alignment between the risk estimates provided by the nomogram and the actual cumulative incidence function clinical outcomes (Figure 4). The nomogram demonstrated enhanced net benefits in identifying CIF in OSA patients when compared to the utilization of LnNLR alone, as well as in both the intervention-for-all and intervention-for-none strategies. Moreover, the decision curve analysis (DCA) demonstrated that the nomogram provided superior predictive performance for the occurrence of CIF in OSA patients (Figure 5). Compared to using LnNLR alone, the nomogram yielded a greater net clinical benefit in identifying CIF among OSA patients, as well as outperformed both the treat-all and treat-none strategies. Among the four independent predictors in the final model, age (OR 1.057; 95% CI, 1.006–1.110) was positively associated with CIF risk, indicating that older OSA patients are at higher risk. Subgroup analyses were not feasible due to limited sample size, but future studies should explore potential interactions between risk factors across age, sex, and comorbidity strata.
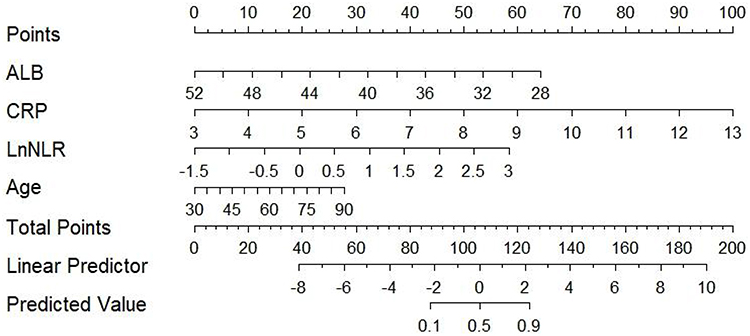 |
Figure 3 Nomogram predicting CIF risk in OSA patients. |
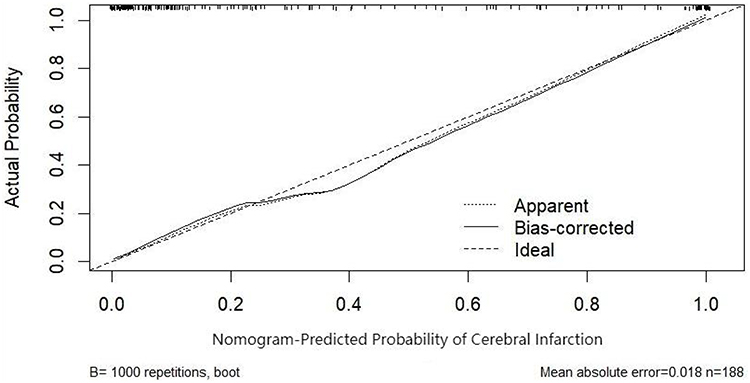 |
Figure 4 Calibration curves for the nomograms. |
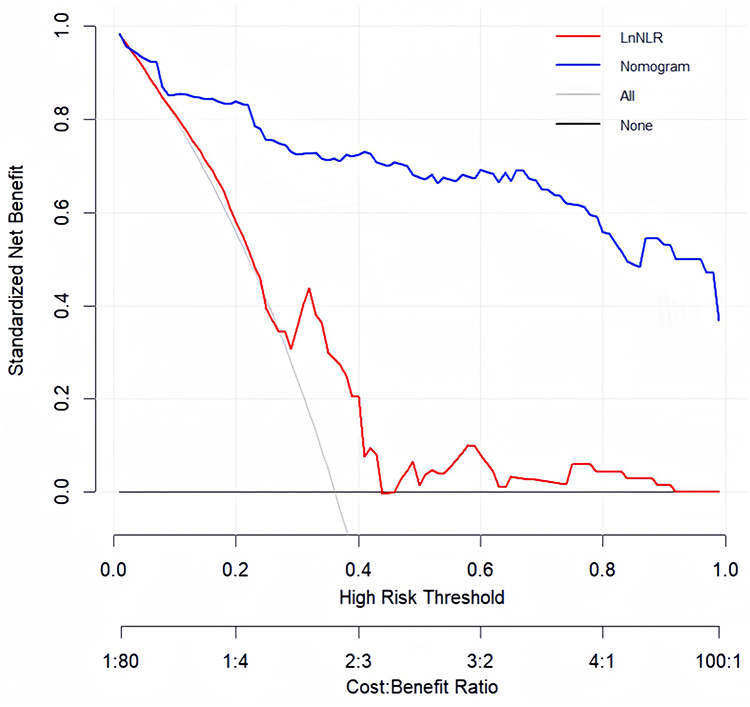 |
Figure 5 The decision curve analysis (DCA) of the nomogram’s calculation model. |
ROC Curve Analysis of LnNLR and Nomogram Computational Model
The nomogram model achieved an AUC of 0.9372 (95% CI: 0.8990–0.9754), which was significantly higher than that of LnNLR alone (AUC = 0.665, 95% CI: 0.584–0.747) (Figure 6). At the optimal cut-off value of 0.436, the nomogram demonstrated a sensitivity of 82.35% and specificity of 92.50%, indicating strong discriminative ability. Compared with LnNLR alone, which showed moderate sensitivity and limited specificity, the integrated model offers a more balanced performance in correctly identifying both CIF and non-CIF cases among OSA patients. This balance between sensitivity and specificity enhances the clinical utility of the model in early risk stratification.
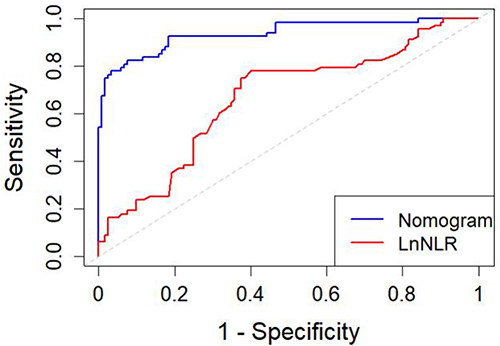 |
Figure 6 ROC curve analysis of LnNLR and nomogram computational models. |
Discussion
This study highlights the crucial role of systemic inflammation, particularly an elevated NLR, in the pathogenesis of CIF in patients with OSA. Our analysis identified LnNLR as an independent risk factor for CIF (OR, 4.682; 95% CI, 1.149–19.070; P < 0.001), underscoring the contribution of chronic immune dysregulation and persistent low-grade inflammation to cerebrovascular injury. NLR, a composite biomarker reflecting neutrophil-driven inflammation and lymphocyte-mediated immune suppression, has gained recognition for its predictive value in cardiovascular and cerebrovascular diseases.7,10,11 Earlier research has identified NLR as a potential prognostic marker for ischemic stroke, indicating that elevated NLR levels correlate with heightened risks of early delirium, mortality, and unfavorable functional outcomes in individuals affected by ischemic stroke.12–14 Our findings extend this association to the OSA population and support NLR’s use as a valuable biomarker for early risk stratification.
Systemic inflammation in OSA is driven by repetitive hypoxia-reoxygenation cycles and sleep fragmentation, which activate transcription factors, resulting in the upregulation of pro-inflammatory cytokines.15–17 The inflammatory mediators are essential in the processes of endothelial dysfunction, the compromise of the blood-brain barrier, and the remodeling of vascular structures.18 Moreover, increased levels of CRP, recognized as an independent risk factor (P < 0.001), indicate the persistent influence of chronic inflammation and its harmful impact on vascular stability. CRP has been associated with the promotion of plaque instability and thrombogenesis, consequently heightening the risk of ischemic events in susceptible individuals.19
Our findings align with previous studies reporting an association between systemic inflammation and an increased incidence of atrial fibrillation in OSA patients,8 a condition known to elevate CIF risk by 3- to 5-fold. Inflammation-induced atrial remodeling and autonomic imbalance may serve as a mechanistic link between OSA and atrial fibrillation, suggesting that the inflammatory state in OSA not only directly contributes to cerebrovascular damage but may also predispose patients to cardioembolic events.20
In our study, age was independently associated with an increased risk of CIF among OSA patients (OR = 1.057; 95% CI: 1.006–1.110). This finding is consistent with established clinical knowledge that advancing age is a major non-modifiable risk factor for cerebrovascular disease. Age-related vascular changes—such as increased arterial stiffness, endothelial dysfunction, and impaired cerebral autoregulation—contribute to heightened vulnerability to ischemic events. Moreover, older individuals with OSA may have accumulated vascular risk burden over time, including comorbidities like hypertension, atrial fibrillation, and diabetes, which synergistically amplify cerebrovascular risk. Our results support the inclusion of age as a critical variable in cerebrovascular risk prediction models among OSA populations.20
In addition, serum albumin (ALB), a negative acute-phase reactant, was found to be inversely associated with CIF risk in our study. While low ALB levels are often indicative of malnutrition or systemic illness, emerging evidence suggests that hypoalbuminemia may reflect a state of heightened oxidative stress and impaired vascular protection. Albumin possesses several physiological properties relevant to cerebrovascular health, including antioxidant capacity, free radical scavenging, and endothelial stabilization.21 It also exerts antiplatelet effects and maintains oncotic pressure, thereby reducing the risk of vasogenic edema formation.22 Mechanistically, albumin has been shown to modulate inflammation by binding and neutralizing pro-inflammatory molecules and preserving capillary integrity during ischemic insults. Clinical studies have reported that lower serum albumin levels are associated with increased stroke severity, infarct volume, cerebral edema, and mortality.23,24 In our cohort, ALB was independently protective, suggesting that preserved albumin levels may counteract inflammatory and thrombotic processes in OSA-related CIF. This finding underscores the potential role of ALB not only as a biomarker of systemic condition but also as a modifiable factor that could be targeted through nutritional or anti-inflammatory interventions. Further research is warranted to explore whether improving serum albumin levels—via nutritional support or anti-inflammatory therapies—may reduce cerebrovascular risk, particularly in vulnerable OSA populations.
NLR is a practical and accessible biomarker, its non-specificity limits its discriminatory value in patients with other inflammatory or chronic comorbidities. Considering OSA’s complex pathophysiology and multifaceted effect on cerebrovascular health, an individual biomarker would be unlikely to truly account for CIF risk. To address this, we developed a nomogram incorporating age, ALB, CRP, and LnNLR. The model demonstrated excellent discriminative ability (AUC = 0.9372), significantly outperforming LnNLR alone (AUC = 0.665). At the optimal cut-off (0.436), the nomogram achieved a sensitivity of 82.35% and specificity of 92.50%, indicating a favorable balance in identifying true positives and minimizing false positives. This sensitivity-specificity trade-off supports its utility in clinical screening and individualized decision-making. Moreover, calibration plots showed good agreement between predicted and observed outcomes, and DCA confirmed the net clinical benefit of the model over both treat-all and treat-none strategies.
The findings of our study highlight the importance of systemic inflammation—particularly elevated NLR and CRP levels—in predicting CIF risk among patients with OSA. However, several limitations should be acknowledged. First, this was a retrospective, single-center analysis based on clinically collected data, which may introduce selection bias and limit the generalizability of our findings. Second, the overall sample size was relatively small (n = 188), and larger, prospective studies are warranted to confirm the robustness of our results. Third, while internal validation using bootstrap resampling and decision curve analysis demonstrated strong model performance, external validation with independent, multi-center cohorts is necessary to confirm the reliability and applicability of the nomogram in broader clinical settings. Fourth, NLR and CRP were assessed only at baseline, which may not reflect dynamic fluctuations during disease progression or therapeutic intervention. Inflammatory activity in OSA is known to vary over time, especially in response to CPAP therapy, comorbidity progression, or acute events. Future prospective studies should incorporate serial biomarker measurements at defined time points (eg, day 0, 7, 14, 30, and 90) to better characterize the temporal evolution of systemic inflammation and its relationship with CIF risk. Such dynamic profiling could help identify critical windows for risk prediction and intervention, and improve the understanding of inflammation-mediated stroke pathophysiology in OSA. Finally, several clinically relevant confounding variables—such as medication use (eg, statins or antiplatelet drugs), OSA duration and severity, and comorbid inflammatory diseases (eg, IL-6 and fibrinogen)—were not fully adjusted for in our model due to data limitations. Future research should incorporate these factors to further enhance model accuracy. Moreover, studies with larger and more diverse populations would allow for formal subgroup and sensitivity analyses. Stratifying patients by sex, OSA severity, or comorbid conditions could help uncover potential heterogeneity in inflammatory responses and cerebrovascular risk, offering deeper insights into patient-specific mechanisms and enhancing the precision of risk prediction. Overall, large-scale, prospective, multicenter studies are needed to validate and refine inflammation-based prediction models for individualized cerebrovascular risk assessment in OSA patients.
Conclusion
Our results suggest that increased NLR levels can be used as an indirect biomarker for CIF in patients with OSA. The nomogram is an algebraic model that combines various independent correlates and is capable of forecasting CIF risk in OSA patients. This instrument can help health care professionals to identify high-risk OSA patients. It is postulated that an important role in CIF in OSA is played by inflammation. NLR is presented as an economical, non-invasive biomarker to predict CIF risk in OSA. Large-scale prospective studies need to be conducted to evaluate OSA’s interaction with CIF through inflammation and support clinical decision-making.
Abbreviations
OSA, obstructive sleep apnoea; NLR, neutrophil-to-lymphocyte ratio; ROC, receiver operating characteristic; DCA, decision curve analysis; AUC, area under the ROC curve; CRP, C-reactive protein; TNF-α, tumour necrosis factor-alpha; IL-6, interleukin-6; IL-8, interleukin-8; ICAM, intercellular adhesion molecule; VCAM, vascular cell adhesion molecule; HT, hypertension; BMI, body mass index; DM, diabetes mellitus; WBC, white blood cell count; RDWCV, red blood cell distribution width coefficient of variation; TC, total cholesterol; TG, triglycerides; LDL-C, low-density lipoprotein cholesterol; HDL-C, high-density lipoprotein cholesterol; FPG, fasting blood glucose; ALB, albumin; LYM, lymphocytes; AHI, Apnea-Hypopnea Index.
Data Sharing Statement
The datasets generated/analysed during the current study are available. Further enquiries can be directed to the corresponding author.
Ethics Approval and Consent to Participate
We certify that the study was performed in accordance with the 1964 declaration of Helsinki and later amendments. This study protocol was reviewed and approved by the Ethics Committee of Shanxi Cardiovascular Hospital, approval number [XXGYY2022101]. Written informed consent was obtained from all the participants prior to the enrollment of this study.
Consent for Publication
Consent for publication was obtained from the participants.
Acknowledgments
We would like to thank all authors for their valuable contributions to this work. Additionally, we gratefully acknowledge the financial support from Four Batches “ innovation Project of invigorating Medical through Science a Technology of Shanxi Province (2022XM07); Scientific Research Incentive Fund of Shanxi Cardiovascular Hospital (XYS20220107); Shanxi Province Chinese Medicine Science and Technology special research project (2024ZYY2A023).
Author Contributions
All authors gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Ziwei Hou: Writing – Original Draft, Writing – Review & Editing, Methodology, Investigation, Conceptualization. Chen Chen: Writing – Review & Editing, Formal Analysis, Visualization. Hong Liu: Writing – Review & Editing, Methodology, Resources, Validation. Yunpeng Wang: Writing – Review & Editing, Data Curation, Software, Conceptualization. Zongxuan Li: Writing – Review & Editing, Data Curation, Software, Conceptualization.
Funding
Four Batches innovation Project of invigorating Medical through Science a Technology of Shanxi Province (2022XM07); Scientific Research Incentive Fund of Shanxi Cardiovascular Hospital (XYS20220107); Shanxi Province Chinese Medicine Science and Technology special research project (2024ZYY2A023).
Disclosure
The author(s) report(s) no conflicts of interest in this work.
References
1. Zhao Y, Zhang X, Chen X, Wei Y. Neuronal injuries in cerebral infarction and ischemic stroke: from mechanisms to treatment. Int J Mol Med. 2022;49(2):15. doi:10.3892/ijmm.2021.5070
2. Bailey EL, Smith C, Sudlow CL, Wardlaw JM. Pathology of lacunar ischemic stroke in humans-a systematic review. Brain Pathol. 2012;22(5):583–591. doi:10.1111/j.1750-3639.2012.00575.x
3. Iannella G, Magliulo G, Greco A, et al. Obstructive sleep apnea syndrome: from symptoms to treatment. Int J Environ Res Public Health. 2022;19(4):2459.PMID: 35206645; PMCID: PMC8872290. doi:10.3390/ijerph19042459
4. Hoang-Anh T, Duong-Minh Q, Nguyen-Thi-Y N, Duong-Quy S. Study of the obstructive sleep apnea syndrome in cerebral infarction patients. Front Neurol. 2023;14:1132014. PMID: 37416312; PMCID: PMC10321128. doi:10.3389/fneur.2023.1132014
5. Nadeem R, Molnar J, Madbouly EM, et al. Serum inflammatory markers in obstructive sleep apnea: a meta-analysis. J Clin Sleep Med. 2013;9(10):
6. Kim S, Eliot M, Koestler DC, Wu W-C, Kelsey KT. Association of neutrophil-to-lymphocyte ratio with mortality and cardiovascular disease in the Jackson Heart Study and modification by the Duffy antigen variant. JAMA Cardiol. 2018;3(6):
7. Adamstein NH, MacFadyen JG, Rose LM, et al. The neutrophil-lymphocyte ratio and incident atherosclerotic events: analyses from five contemporary randomized trials. Eur Heart J. 2021;42(9):
8. Yu B, Wei J, Zhao J, et al. The neutrophil-to-lymphocyte ratio is a potential biomarker for the occurrence of atrial fibrillation in patients with obstructive sleep apnea: a BIOMARKER OF AF IN OSA PATIENTS. Sleep Med. 2023;110:259–267. doi:10.1016/j.sleep.2023.08.004
9. Chinese Society of Neurology, Chinese Stroke Society. Chinese guidelines for diagnosis and treatment of acute ischemic stroke 2018. Zhonghua Shen Jing Ke Za Zhi. 2018;51(666):682.
10. Larmann J, Handke J, Scholz AS, et al. Preoperative neutrophil to lymphocyte ratio and platelet to lymphocyte ratio are associated with major adverse cardiovascular and cerebrovascular events in coronary heart disease patients undergoing non-cardiac surgery. BMC Cardiovasc Disord. 2020;20(1):230. doi:10.1186/s12872-020-01500-6
11. Dong CH, Wang ZM, Chen SY. Neutrophil to lymphocyte ratio predict mortality and major adverse cardiac events in acute coronary syndrome: a systematic review and meta-analysis. Clin Biochem. 2018;52:131–136. doi:10.1016/j.clinbiochem.2017.11.008
12. Tokgoz S, Keskin S, Kayrak M, Seyithanoglu A, Ogmegul A. Is neutrophil/lymphocyte ratio predict to short-term mortality in acute cerebral infarct independently from infarct volume? J Stroke Cerebrovasc Dis. 2014;23(8):2163–2168.Epub 2014 Aug 6. PMID: 25106834. doi:10.1016/j.jstrokecerebrovasdis.2014.04.007
13. Kocaturk O, Besli F, Gungoren F, Kocaturk M, Tanriverdi Z. The relationship among neutrophil to lymphocyte ratio, stroke territory, and 3-month mortality in patients with acute ischemic stroke. Neurol Sci. 2019;40(1):139–146. doi:10.1007/s10072-018-3604-y
14. Celikbilek A, Ismailogullari S, Zararsiz G. Neutrophil to lymphocyte ratio predicts poor prognosis in ischemic cerebrovascular disease. J Clin Lab Anal. 2014;28(1):27–31.Epub 2013 Dec 27. PMID: 24375839; PMCID: PMC6807633. doi:10.1002/jcla.21639
15. Li X, Liu X, Meng Q, et al. Circadian clock disruptions link oxidative stress and systemic inflammation to metabolic syndrome in obstructive sleep apnea patients. Front Physiol. 2022;13:932596. doi:10.3389/fphys.2022.932596
16. Kheirandish-Gozal L, Gozal D. Obstructive sleep apnea and inflammation: proof of concept based on two illustrative cytokines. Int J Mol Sci. 2019;20(3):459. doi:10.3390/ijms20030459
17. Fiedorczuk P, Polecka A, Walasek M, Olszewska E. Potential diagnostic and monitoring biomarkers of obstructive sleep apnea-umbrella review of meta-analyses. J Clin Med. 2022;12(1):60. doi:10.3390/jcm12010060
18. Orrù G, Storari M, Scano A, Piras V, Taibi R, Viscuso D. Obstructive sleep apnea, oxidative stress, inflammation and endothelial dysfunction-an overview of predictive laboratory biomarkers. Eur Rev Med Pharmacol Sci. 2020;24(12):6939–6948.PMID: 32633387. doi:10.26355/eurrev_202006_21685
19. Dix C, Zeller J, Stevens H, et al. C-reactive protein, immunothrombosis and venous thromboembolism. Front Immunol. 2022;13:1002652. doi:10.3389/fimmu.2022.1002652
20. Loke YK, Brown JW, Kwok CS, Niruban A, Myint PK. Association of obstructive sleep apnea with risk of serious cardiovascular events: a systematic review and meta-analysis. Circ Cardiovasc Qual Outcomes. 2012;5(5):720–728. doi:10.1161/CIRCOUTCOMES.111.964783
21. Arques S. Human serum albumin in cardiovascular diseases. Eur J Intern Med. 2018;52:8–12. doi:10.1016/j.ejim.2018.04.014
22. Gao Y, Zong C, Yao Y, et al. Elevated fibrinogen-to-albumin ratio correlates with incident stroke in cerebral small vessel disease. J Inflamm Res. 2024;17:4331–4343. doi:10.2147/JIR.S466879
23. Shaikh F, Shaikh FH, Chandio SA. Frequency of hypoalbuminemia and in-hospital mortality in acute ischemic stroke patients presenting at a tertiary care hospital. Hyderabad Cureus. 2021;13(4):e14256. doi:10.7759/cureus.14256
24. Arnau-Barrés I, Güerri-Fernández R, Luque S, Sorli L, Vázquez O, Miralles R. Serum albumin is a strong predictor of sepsis outcome in elderly patients. Eur J Clin Microbiol Infect Dis. 2019;38(4):743–746. doi:10.1007/s10096-019-03478-2
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Construction and Validation of a Nomogram Model for Predicting Pulmonary Hypertension in Patients with Obstructive Sleep Apnea
Zhang R, Liu Z, Li R, Ai L, Li Y
Nature and Science of Sleep 2025, 17:1049-1066
Published Date: 24 May 2025
Prediction of First-Onset Cerebral Infarction Risk in Patients with Acute Myocardial Infarction: A Retrospective Cohort Study
Zeng Z, Luo R, Xu W, Yao H, Lan X
International Journal of General Medicine 2025, 18:3501-3513
Published Date: 27 June 2025
Clinical Prediction of Secondary Bloodstream Infections in Patients with Cerebral Infarction: A Nomogram-Driven Risk Assessment Model Based on LASSO Regression
Zhang L, Li X, Cai D, Mei C, Lu L
Infection and Drug Resistance 2025, 18:3677-3687
Published Date: 25 July 2025