Back to Journals » International Journal of General Medicine » Volume 17
Predictive Factors for First-Pass Intubation Failure in Trauma Patients
Authors Kilkenny K, McGrinder S ![]() , Najac MJ, LeBaron J, Carpenito P, Lakhi N
, Najac MJ, LeBaron J, Carpenito P, Lakhi N ![]()
Received 17 November 2023
Accepted for publication 23 February 2024
Published 6 March 2024 Volume 2024:17 Pages 855—862
DOI https://doi.org/10.2147/IJGM.S446728
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Katherine Kilkenny,1 Shea McGrinder,1 Michael J Najac,2 Johnathon LeBaron,3 Pietro Carpenito,4 Nisha Lakhi1,5
1School of Medicine, New York Medical College, Valhalla, NY, USA; 2Lewis Katz School of Medicine, Temple University, Philadelphia, PA, USA; 3Department of Emergency Medicine, Richmond University Medical Center, Staten Island, NY, USA; 4Department of Anesthesiology, Richmond University Medical Center, Staten Island, NY, USA; 5Department of Trauma Surgery, Richmond University Medical Center, Staten Island, NY, USA
Correspondence: Nisha Lakhi, Associate Professor of Obstetrics and Gynecology, Richmond University Medical Center, 355 Bard Avenue, Staten Island, NY, 10310, USA, Email [email protected]
Objective: The primary objective of this study was to elucidate risk factors for multiple intubation attempts (MIA) in trauma patients requiring emergent tracheal intubation (ETI). Risk factors for mortality, intensive care unit (ICU) admission, and prolonged ventilation were assessed as secondary outcomes. The association between multiple intubation attempts and adverse outcomes has been well described in the literature. Though previous studies have identified anatomical risk factors for difficult airways, no study to date has investigated predictors for MIA in a trauma setting.
Methods: The retrospective study involved 174 adult patients who required ETI and who presented to a Level 1 Trauma Center’s emergency department between January 2019 and December 2022. Comorbidities, demographic information, triage vitals, intubation characteristics, and patient outcomes were identified to ascertain predictive risk factors for MIA. Variables were assessed for statistical significance on unadjusted analysis. Significant variables were entered into multivariate logistic regression models to test for adjusted associations, with p≤ .0.05 as statistically significant, and presented as adjusted odds ratios with 95% confidence intervals.
Results: Twenty-six (14.9%) of the 174 patients required multiple intubation attempts. There were no significant associations between MIA and patient gender, age, BMI, race, injury mechanism, or specific body region injuries. On univariate analysis, the MIA group had a statistically significant elevation in mean systolic blood pressure (151.71 ± 45.96 vs 133.55 ± 32.11, p = 0.019) and heart rate (106.30 ± 34.92 vs 93.35 ± 24.82, p < 0.032) compared to subjects with first-pass success. Elevation in systolic blood pressure (SBP) (151.71 ± 45.96 vs 133.55 ± 32.11, aOR 1.03 (1.01– 1.06), p < 0.015) was an independent predictor of multiple intubation attempts.
Conclusion: Elevation in SBP was a significant predictor of multiple intubation attempts. Critical appraisal of patients requiring ETI with elevated SBP may mitigate risk in trauma settings.
Keywords: trauma, multiple intubation attempts, first-pass intubation failure, emergency tracheal intubation, airway, adult, intubation trauma
Introduction
The most urgent priority in the initial workup of trauma patients is confirmation of a patent airway to ensure adequate oxygenation and ventilation.1,2 Early and appropriate management of the airway in trauma patients is a critical component of care that reduces morbidity and mortality. Patients with hypoxia, hypoventilation, and failure to maintain or protect the airway due to altered mental status may require emergency tracheal intubation (ETI). Although this procedure is potentially lifesaving, it is not without risks, particularly when multiple intubation attempts (MIA) are necessary.3–5 The incidence of complications associated with ETI ranges from 3% to 60%, and decreases the likelihood of survival in trauma patients.5–7
The importance of first-pass intubation success cannot be overstated, as multiple intubation attempts have been associated with significant morbidity and mortality.4,8–13 Mort et al demonstrated that more than two intubation attempts increases the risk of severe hypoxemia 14-fold and the risk of cardiac arrest 7-fold.5 Other ETI-associated complications that occur more frequently with MIA include increased likelihood of esophageal intubation, aspiration, laryngospasm, bronchospasm, hypotension, and death.5–7 In addition to these acute adverse events, MIA is associated with longer hospital stays and higher mortality rates.14 These adverse events have significant implications for patient outcomes, healthcare costs, and resource utilization.
A thorough review of published literature indicates that the prevalence of multiple intubation attempts ranges from 8% to 25% across various clinical settings and patient populations.4,7,14,15 Given the prevalence of MIA and the well-defined association with adverse patient outcomes, further investigation is needed to guide trauma teams in anticipation and prevention of first-pass intubation failure. Previous studies have identified anatomical risk factors for difficult airways, and risk factors for cardiovascular decompensation following intubation in the ICU, but additional research is needed to determine predictive factors for MIA in a trauma setting.12,16 Identifying such risk factors may help trauma units anticipate a difficult intubation and recruit the most experienced and qualified team member to initiate the ETI, thereby reducing the potential for patient morbidity and mortality.
Materials and Methods
Study Design, Setting, and Participants
This IRB approved (Study #18258) retrospective cohort study was conducted at Richmond University Medical Center, a Level I Trauma Center in Staten Island, New York, between January 1, 2019, and December 31, 2022. The protocol was reviewed and approved by the IRB of New York Medical College, Valhalla, New York. Given the retrospective nature of this study involving chart review with anonymized data points, the IRB approved a waiver for individual patient consent. The study complies with the Declaration of Helsinki. The medical records of all adult patients who presented to the trauma center and who required emergency tracheal intubation during their hospital admission were identified using a trauma registry. We defined “adult” as individuals aged 18 years old and greater. International Classification of Diseases, 10th Revision, Clinical Modification (ICD-10-CM) codes for tracheal intubation were utilized to identify 265 subjects meeting this description. Patients who underwent primary intubation in the operating room and intensive care unit (ICU) were excluded, leaving 176 patients for analysis. All intubations by Emergency Department (ED) physicians and anesthesiologists occurred in the ED and were conducted by attending-level physicians. Qualified emergency medical service (EMS) personnel performed intubations in prehospital settings. ETI at this institution are routinely performed with etomidate as an anesthetic and succinylcholine as a neuromuscular blocking agent. Both direct and video laryngoscope (VLS) were used in this study, and the breakdown of usage by specialty of intubator is reported in our results section. All cases of VLS in this study involved a Macintosh blade. Generally, VLS was used in anticipation of a difficult airway or as part of a second intubation attempt.
Data Collection and Management
Electronic medical record (EMR) review, which allowed access to all patient encounters, in conjunction with current procedural terminology (CPT) and ICD-10-CM codes were used to identify demographic and comorbid factors included in the analysis. Collected data points from the EMR included age, gender, body mass index (BMI), mechanism of injury (MOI), injury severity score (ISS), abbreviated injury scale (AIS) by body region, antithrombotic use, and any known comorbidities. Triage data obtained from initial patient presentation to the emergency department (ED) were obtained including systolic blood pressure (SBP), heart rate (HR), respiratory rate, oxygen saturation (SpO2%), Glasgow coma score (GCS), and international normalized ratio (INR). For each patient in this study, these data (vital signs) were obtained prior to an attempted ETI, and prior to administration of anesthetics, neuromuscular blockers, fluids, and vasoactive agents. Shock index (SI), defined as HR divided by SBP, was calculated for each patient using the “DIVIDE” function in Microsoft Excel to automate the calculation and ensure accuracy.
Presence of comorbidities was identified using ICD-10-CM codes and included coronary artery disease, obstructive airway disease (asthma, chronic obstructive pulmonary disease (COPD)), history of dementia, and diabetes mellitus. Anti-thrombotic use was identified via EMR review and included current anticoagulant use (novel oral anticoagulants, warfarin, and any formulary of heparin (unfractionated heparin, low molecular weight heparin)) and antiplatelet use (aspirin, clopidogrel, dipyridamole).
Definition of Multiple Intubation Attempts, Prolonged Ventilation, and Elevated INR
Although the term “multiple intubation attempts (MIA)” has been inconsistently defined in the literature, the gold standard for emergency airway management is first-pass intubation success and studies have shown increased risk of adverse outcomes with two intubation attempts compared to one.1,2 Therefore, in this study, we described MIA as intubations requiring greater than one intubation attempt. In this study, we defined “elevated INR” as an INR greater than 1.5 as this threshold has been associated with an increased risk of bleeding and mortality in various clinical settings.17,18 Additionally, we defined “Prolonged Ventilation” as greater than or equal to 3 days of ventilatory support. This criterion is justified by the well-defined ventilator-associated complications (eg, infection, diaphragmatic dysfunction, acidosis) that may occur after just two days on mechanical ventilation and are increasingly likely with each additional day of ventilation.19
Outcomes
The primary objective of this study was to identify predictive risk factors for multiple intubation attempts in the adult population presenting to an urban Level I Trauma Center. Secondary outcomes examined were ICU admission, prolonged ventilation, and mortality. None of our outcomes were treated as mutually exclusive and all were categorized as independent events.
Statistical Analysis
Statistical analysis was carried out using IBM SPSS 29.0. Unadjusted analyses for continuous variables were compared using means. Categorical data were compared via chi-square analysis and unadjusted logistic regression. Associations between two continuous variables were assessed for collinearity using Pearson’s correlation. Goodness of Fit was performed for all categorical variables using chi-square test, with a p-value of ≤0.05 considered statistically significant. Variables that were statistically significant on unadjusted analysis were tested for interaction of terms. Non-redundant variables were entered into a multivariable logistic regression model to test for adjusted associations (see Supplementary Tables 1-5). This process was completed for each outcome assessed. Variables that retained statistical significance on multivariable regression were reported as adjusted odds ratios (aOR) with 95% confidence intervals. For quantitative response variables, medians and interquartile ranges (IQR) were compared across groups using median k-sample testing.
An a priori power analysis (“G*Power Erdfelder, Faul, * Buchner, Behavior Research Methods and Instruments & Computers, 1996) was performed using t-test for statistical tests. Based on data from Gaither et al that assessed risk factors for intubation complications in obese patients, we estimate a medium effect (d = 0.45) size attributed to MIA.16 Assuming two tails test with at least 80% power and alpha = 0.05, the total number of 158 patients will be enough to provide a sample of sufficient power.
Results
Patient Demographics and Comorbidities
During the study period, 174 patients meeting the inclusion criteria presented to the trauma center and required ETI during their hospital course. Demographics are presented in Table 1. The mean age of our patient sample was 55.5 years old (19–99 years) with a median BMI of 26 kg/m2 (IQR 9 kg/m2). Patients required ventilatory support for a median of 2.0 days (IQR 8 days), were admitted to the ICU for a median of 2 days (IQR 11 days) and had a median ISS of 14 (IQR 22). Mean systolic blood pressure was 136.36 ± 35.1. ED doctors performed the majority (57.5%) of intubations, followed by anesthesiologists (28.2%) and emergency medical services (EMS) personnel (14.4%).
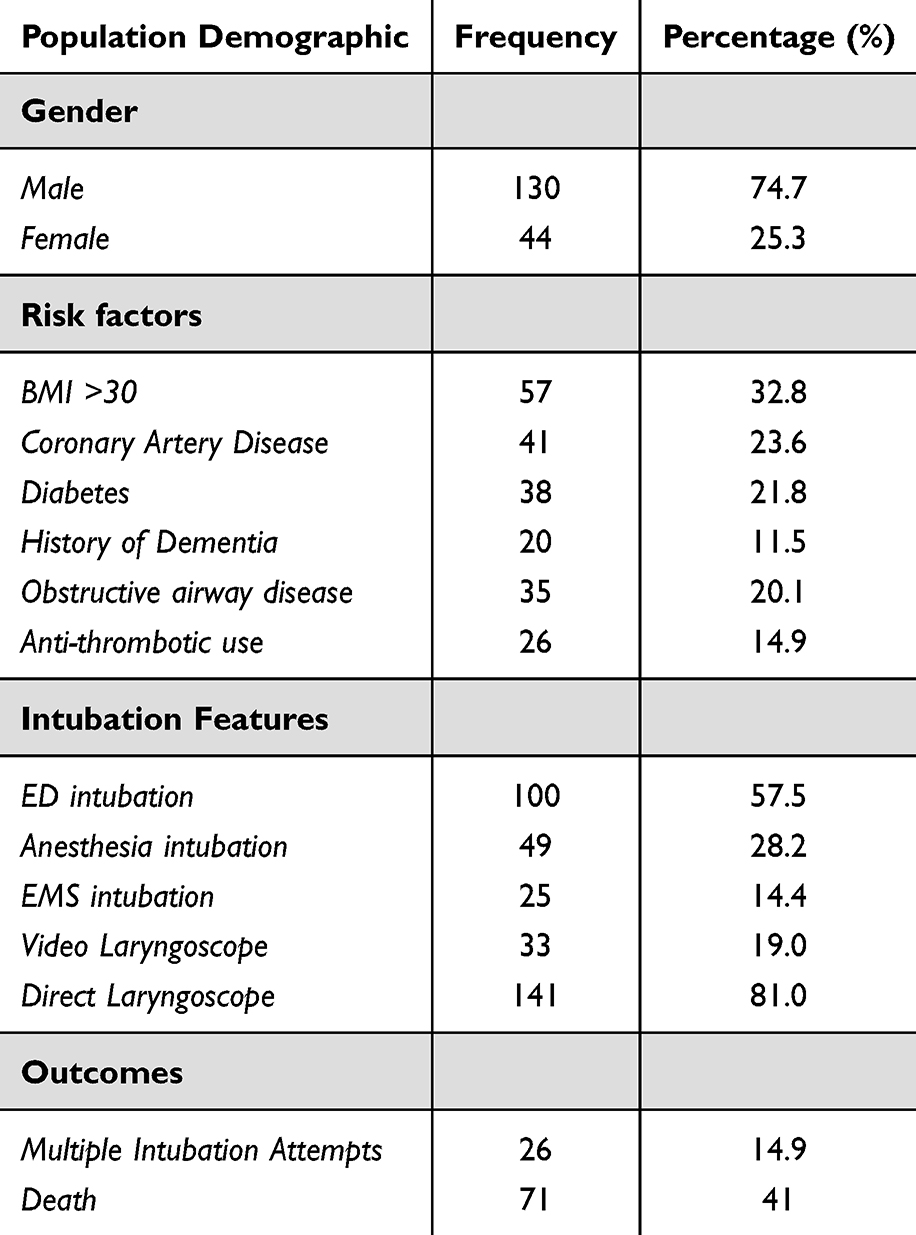 |
Table 1 Population Demographics |
Patient demographics, their specific comorbidities, details about their intubation, and outcomes of their intubation are presented in Table 1. Of the 33 intubations utilizing video laryngoscope, 54.5% (18) were performed by anesthesiologists, 39.4% (13) were performed by ED physicians, and 6.1% (2) were performed by EMS personnel.
Multiple Intubation Attempts
In our study, a total of 174 patients underwent emergency endotracheal intubation, out of which 26 patients (14.9%) required multiple intubation attempts. We found no significant association between multiple intubation attempts (MIA) and patient characteristics (gender, age, BMI), injury mechanism, or specific body region injuries (Supplementary Table 1). However, our univariate analysis revealed that the MIA group had a statistically significant elevation in mean systolic blood pressure (151.71 ± 45.96 vs 133.55 ± 32.11, p = 0.019) and heart rate (106.30 ± 34.92 vs 93.35 ± 24.82, p < 0.032) compared to subjects with first-pass success. Subjects who underwent VLS were less likely to experience MIA compared to those who underwent direct laryngoscope (30.8% vs 12.7% OR 0.55, 95% CI 0.28–1.08).
Multivariate logistic regression analysis was performed to assess the predictors of MIA in the sample population. Our model (χ2 (3, N = 174)= 14.969, p < 0.001) outperformed the null model and demonstrated that systolic blood pressure (aOR 1.03 (1.01–1.06), p < 0.015) retained statistical significance, indicating independent prediction of MIA (Table 2).
 |
Table 2 Multivariable Regression Analysis of Risk Factors |
Mortality
Of the 174 patients included in our study, 71 (41%) died during their hospital admission. Older age (59.39 ± 24.51 vs 52.6 ± 19.6), lower oxygen saturation (95.90 ± 5.46 vs 97.41 ± 3.0), depressed GCS (7.46 ± 5.21 vs 10.82 ± 4.7), elevated injury severity score (ISS) (20.77 ± 20.69 vs 15.11 ± 12.5), and elevated INR (0.83 ± 0.1 vs 0.74 ± 0.29) were predictors of mortality on univariate analysis. Intubations performed by ED physicians carried a decreased mortality risk (31% vs 54.8%, OR 0.37, 95% CI 0.20–0.69), and those performed by EMS personnel carried an increased mortality risk (80% vs 34.5%, OR 7.61, 2.70–21.46). No patient characteristics (BMI, gender, race, ethnicity), comorbidities, or body region (AIS) were statistically associated with mortality (Supplementary Table 2).
Multivariate logistic regression analysis was performed to assess independent predictors of death in the sample population. Our model outperformed the null model (χ2 (5, N = 174)= 40.620, p < 0.001). Age (aOR 1.05 (1.02–1.07), p < 0.001), GCS (aOR 0.88 (0.80–0.96), p = 0.004), oxygen saturation (aOR 0.85 (0.75–0.96), p = 0.007), ISS (aOR 1.03 (1.00–1.07), p = 0.048), and INR (aOR 2.61 (1.18–5.76), p = 0.017) retained statistical significance, and were independent predictors of mortality (Table 2).
Intensive Care Unit Admission
Admission to the ICU was necessary for 114 (65.5%) patients. Patient characteristics, ISS score, and specific body region injury were not found to be associated with ICU admission (Supplementary Table 3). Multiple intubation attempts (92.3% vs 60.8%, OR 7.73, 95% CI 1.76–33.96), elevated SBP (139.91 ± 35.74 vs 126.8 ± 31.6, p < 0.038), higher GCS (10.56 ±4.73 vs 7.40 ± 5.36, p < 0.001), fall injury (79.1 vs 50.6, OR 3.7, 95% CI 1.91–7.19), coronary artery disease (85.4% vs 59.8%, OR 3.914, 95% CI 1.54–9.95), history of dementia (95.0% vs 62.1%, OR 11.6, 95% CI 1.51–88.96), and diabetes mellitus (86.8% vs 60.0%, OR 4.40, 95% CI 1.62–11.98) had statistically significant increased associations with ICU admission on univariate analysis. Intubations performed by anesthesiologists were associated with an increased risk of ICU admission (87.8% vs 56.8%, OR 5.45, 95% CI 2.16–13.74), while intubations performed by EMS had an inverse association with ICU admission (32% vs 71.1%, OR 0.19, 95% CI 0.077–0.48). Penetrating injury (40.0% vs 69.8%, OR 0.288, 95% CI 0.12–0.69) and elevated INR (37.8% vs 75.2%, OR 0.20, 95% CI 0.10–0.41) had significantly decreased associations with ICU admission.
Multivariate logistic regression analysis was performed to assess the predictors of ICU admission in the sample population. Our model outperformed the null model (χ2 (6, N = 174)= 51.353, p < 0.001). MIA (aOR 7.63 (1.54–37.79), p = 0.013) was found to be an independent risk factor for ICU admission. Elevated INR (37.8% vs 75.2%, aOR 0.19 (0.083–0.44), p < 0.001) had a statistically significant decreased association with ICU admission (Table 2).
Prolonged Ventilation
In this cohort of 174 patients who required ETI, 80 (46%) required ventilatory support for greater than 3 days. On univariate analysis, older age (62.05 ± 20.75 vs 50.00 ± 21.54), CAD (63.4% vs 40.9%, OR 4.06, 95% CI 1.41–11.74), history of dementia (75.0% vs 42.5%, OR 1.24, 95% CI 0.81–1.89), penetrating injury (24.0% vs 49.7%, OR 0.32, 95% CI 0.12–0.85), intubation by anesthesia (67.3% vs 37.6%, OR 3.42, 95% CI 1.70–6.88), and anti-thrombotic use (61.5% vs 43.2%, OR 2.10, 95% 0.89–4.94) were associated with an increased risk of prolonged ventilation. Intubations performed by EMS had a negative association with prolonged ventilation (20% vs 50.3%, OR 0.25, 95% CI 0.09–0.69). Demographic factors and ISS score were not associated with prolonged ventilation (Supplementary Table 4). The median and interquartile range for chest AIS was significantly higher in subjects who underwent prolonged intubation versus those who did not (0 (IQR 2) vs 0 (IQR 0), p < 0.013).
Multivariate logistic regression analysis was performed to assess the predictors of prolonged ventilation time in the sample population. Our model outperformed the null model (χ2 (4, N = 174)= 17.491, p = 0.002). Older age was the only independent predictor of prolonged ventilation that retained significance (aOR1.02 (1.00–1.04), p < 0.029) (Table 2).
Discussion
Principal Findings
This study analyzed data from an ethnically diverse urban cohort at a New York City-based Level I trauma center to identify independent predictors of multiple intubation attempts in the setting of ETI. This study was unique in that it examined demographic variables, primary triage vitals, blood indices, and injury mechanism. To the best of our knowledge, this is the first demonstration of non-anatomical predictive risk factors for multiple intubation attempts in a trauma setting. Though standard difficult airway predictors (eg, Mallampati scores, thyromental distance, and neck mobility) are routinely and successfully used by anesthesiologists in preoperative settings, studies have shown limited feasibility in ED settings.20,21 The goal of this study was to provide alternative predictors of MIA that may be leveraged in settings where a critically ill patient requires an urgent airway without time to conduct physiognomic assessment of difficult airway predictors.
Our analysis of 174 emergent tracheal intubations demonstrated that patients with elevations in systolic blood pressure were more likely to incur MIA. To the best of our knowledge, no study has demonstrated an association between SBP and first-pass intubation failure. However, previous studies have identified adverse effects associated with increased blood pressure in trauma patients.22 We postulate that elevated systolic blood pressure may contribute to a stiffening of atlanto-occipital and atlanto-axial joints, resulting in strenuous laryngoscopy. Previous studies have linked elevations in blood pressure to constitutional joint stiffness.23 Moreover, increased sympathetic tone to the larynx may contribute to laryngospasm and tightening of cervical muscles.24 Our study contributes to the evidence highlighting the multifaceted implications of SBP and sympathetic activation on clinical outcomes in high-acuity medical contexts. This information may contribute to trauma algorithms, allowing ED providers to anticipate a difficult intubation and recruit the most experienced member of the team to initiate ETI with techniques that have been shown to improve first-pass intubation success rate (video laryngoscope, pre-oxygenation, and appropriate patient positioning).25,26 Further, larger cohort studies may be beneficial in confirming our findings and identifying additional predictors of MIA in trauma settings.
In this study, there was no association between specialty of intubator or setting of intubation and MIA. Interestingly, although VLS was protective against MIA on univariate analysis, the association did not hold on multivariate regression. The increased mortality rate observed in subjects intubated by EMS personnel is likely indicative of more severe underlying injuries necessitating earlier, pre-hospital intervention. This is supported by decreased rates of ICU admission and prolonged ventilation in the EMS group of intubations, suggesting early demise of those subjects. The increased risk of ICU admission and prolonged mechanical ventilation in the anesthesia group of intubations may reflect a tendency to call for anesthesia in anticipation of a difficult intubation or for a more critical initial presentation.
Strengths and Limitations
Our study had many strengths, beginning with a sizable population of adult patients who presented to a Level 1 Trauma Center in New York City. Additionally, our patient population was drawn from an ethnically diverse community with a wide array of comorbidities. Furthermore, we collected data over a 3-year period, allowing us to capture trends and to account for any temporal changes in the data. This allowed for a robust examination of our research question and enhanced the generalizability of our findings.
Although our study identified multiple significant associations, it is important to acknowledge that the retrospective methodology employed may limit our ability to establish causation between these associations. Due to the amount of data points collected and the large number of statistical analyses performed for this study, there was an increased chance for positive associations and Type 1 error. The source hospital EMR included all hospital encounters for each patient, thus we believe that we were able to identify most of the patient comorbidities and medications of interest. However, the large quantity of data gathered from EMR is subject to information bias and reporting bias secondary to inadequate charting or incomplete medication lists. Furthermore, intubation procedure note documentation is self-reported by the operator and collected at varying times after the procedure. This creates a potential for recall bias. Operators may overstate first-pass success rates and understate adverse events. Although all intubations were performed by attending physicians or EMS personnel, years of experience could not be obtained during data abstraction, which limited our analysis. Finally, it is important to acknowledge that as a single institution study, the external validity of our findings may be constrained, limiting the generalizability of our results to other settings or populations.
Conclusion
The rate of adverse events increases when more than one attempt is required to intubate trauma patients in both pre-hospital and emergency department settings. We found that elevated systolic blood pressure was an independent predictor of first-pass intubation failure in trauma patients requiring ETI. To the best of our knowledge, our study is among the first to specifically investigate the relationship between SBP and MIA in a trauma setting. Considering the relatively high prevalence of first-pass intubation failure and the associated adverse events, SBP may serve as a quick and useful calculation in the initial survey of trauma patients requiring ETI. Future, larger cohort studies are warranted to confirm our findings and uncover additional predictors of first-pass intubation failure.
Abbreviations
AIS, abbreviated injury scale; AMS, altered mental status; aOR, adjusted odds ratio; ATC, acute traumatic coagulopathy; BMI, body mass index; CAD, coronary artery disease; COPD, chronic obstructive pulmonary disease; ED, emergency department; ETI, emergent tracheal intubation; ICU, intensive care unit; MIA, multiple intubation attempts;; OAD, obstructive airway disease; OR, odds ratio; SI, shock index.
Data Sharing Statement
The complete deidentified dataset for this investigation is available upon request, from the date of article publication by contacting Nisha Lakhi, MD, at [email protected].
Disclosure
The authors report no competing or financial interests and therefore have nothing to disclose.
References
1. Newgard CD, Fischer PE, Gestring M, et al. National guideline for the field triage of injured patients: recommendations of the National Expert Panel on Field Triage, 2021. J Trauma Acute Care Surg. 2022;93(2):e49–e60. doi:10.1097/TA.0000000000003627
2. Sakles JC, Chiu S, Mosier J, et al. The importance of first pass success when performing orotracheal intubation in the emergency department. Acad Emerg Med. 2013;20(1):71–78. doi:10.1111/acem.12055
3. Schwartz DE, Matthay MA, Cohen NH. Death and other complications of emergency airway management in critically ill adults. A prospective investigation of 297 tracheal intubations. Anesthesiology. 1995;82(2):367–376. doi:10.1097/00000542-199502000-00007
4. Hasegawa K, Shigemitsu K, Hagiwara Y, et al. Association between repeated intubation attempts and adverse events in emergency departments: an analysis of a multicenter prospective observational study. Ann Emerg Med. 2012;60(6):749–754 e2. doi:10.1016/j.annemergmed.2012.04.005
5. Mort TC. Emergency tracheal intubation: complications associated with repeated laryngoscopic attempts. Anesth Analg. 2004;99(2):607–613. doi:10.1213/01.ANE.0000122825.04923.15
6. Martin LD, Mhyre JM, Shanks AM, et al. 3423 emergency tracheal intubations at a university hospital: airway outcomes and complications. Anesthesiology. 2011;114(1):42–48. doi:10.1097/ALN.0b013e318201c415
7. Ono Y, Kakamu T, Kikuchi H, et al. Expert-Performed Endotracheal Intubation-Related Complications in Trauma Patients: incidence, Possible Risk Factors, and Outcomes in the Prehospital Setting and Emergency Department. Emerg Med Int. 2018;2018:5649476. doi:10.1155/2018/5649476
8. Bushra JS, McNeil B, Wald DA, et al. A comparison of trauma intubations managed by anesthesiologists and emergency physicians. Acad Emerg Med. 2004;11(1):66–70. doi:10.1197/j.aem.2003.08.013
9. Wong E, Ng YY. The difficult airway in the emergency department. Int J Emerg Med. 2008;1(2):107–111. doi:10.1007/s12245-008-0030-6
10. Hsiao YJ, Chen C-Y, Hung H-T, et al. Comparison of the outcome of emergency endotracheal intubation in the general ward, intensive care unit and emergency department. Biomed J. 2021;44(6 Suppl 1):S110–S118. doi:10.1016/j.bj.2020.07.006
11. Goto T, Gibo K, Hagiwara Y, et al. Multiple failed intubation attempts are associated with decreased success rates on the first rescue intubation in the emergency department: a retrospective analysis of multicentre observational data. Scand J Trauma Resusc Emerg Med. 2015;23(1):5. doi:10.1186/s13049-014-0085-8
12. De Jong A, Rolle A, Molinari N, et al. Cardiac Arrest and Mortality Related to Intubation Procedure in Critically Ill Adult Patients: a Multicenter Cohort Study. Crit Care Med. 2018;46(4):532–539. doi:10.1097/CCM.0000000000002925
13. Hubble MW, Brown L, Wilfong DA, et al. A meta-analysis of prehospital airway control techniques part I: orotracheal and nasotracheal intubation success rates. Prehosp Emerg Care. 2010;14(3):377–401. doi:10.3109/10903121003790173
14. Griesdale DE, Bosma TL, Kurth T, et al. Complications of endotracheal intubation in the critically ill. Intensive Care Med. 2008;34(10):1835–1842. doi:10.1007/s00134-008-1205-6
15. Higgs A, McGrath BA, Goddard C, et al. Guidelines for the management of tracheal intubation in critically ill adults. Br J Anaesth. 2018;120(2):323–352. doi:10.1016/j.bja.2017.10.021
16. Gaither JB, Stolz U, Ennis J, et al. Association Between Difficult Airway Predictors and Failed Prehosptial Endotracheal Intubation. Air Med J. 2015;34(6):343–347. doi:10.1016/j.amj.2015.06.001
17. Cuker A, Siegal DM, Crowther MA, et al. Laboratory measurement of the anticoagulant activity of the non-vitamin K oral anticoagulants. J Am Coll Cardiol. 2014;64(11):1128–1139. doi:10.1016/j.jacc.2014.05.065
18. Palareti G, Leali N, Coccheri S, et al. Bleeding complications of oral anticoagulant treatment: an inception-cohort, prospective collaborative study (ISCOAT). Italian Study on Complications of Oral Anticoagulant Therapy. Lancet. 1996;348(9025):423–428. doi:10.1016/S0140-6736(96)01109-9
19. Haribhai S, Mahboobi SK. Ventilator Complications. Treasure Island (FL): StatPearls; 2023.
20. Bair AE, Caravelli R, Tyler K, et al. Feasibility of the preoperative Mallampati airway assessment in emergency department patients. J Emerg Med. 2010;38(5):677–680. doi:10.1016/j.jemermed.2008.12.019
21. Levitan RM, Everett WW, Ochroch EA. Limitations of difficult airway prediction in patients intubated in the emergency department. Ann Emerg Med. 2004;44(4):307–313. doi:10.1016/j.annemergmed.2004.05.006
22. Ley EJ, Singer MB, Clond MA, et al. Elevated admission systolic blood pressure after blunt trauma predicts delayed pneumonia and mortality. J Trauma. 2011;71(6):1689–1693. doi:10.1097/TA.0b013e31823cc5df
23. Uiterwaal CS, Grobbee DE, Sakkers RJB, et al. A relation between blood pressure and stiffness of joints and skin. Epidemiology. 2003;14(2):223–227. doi:10.1097/01.EDE.0000040327.31385.9B
24. Hutauruk M. Autonomic Neuroregulation in the Larynx and Its Clinical Implication. IntechOpen; 2023.
25. Bakhsh A, Alharbi A, Almehmadi R, et al. Improving first-pass success rates during emergency intubation at an academic emergency department: a quality improvement initiative. Int J Qual Health Care. 2021;33(3). doi:10.1093/intqhc/mzab132
26. Alvarado AC, Panakos P. Endotracheal Tube Intubation Techniques. Treasure Island (FL); 2023.
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.