Back to Journals » Journal of Hepatocellular Carcinoma » Volume 13
Predictive Efficacy of a Combined Triphasic CT Radiomics and Clinical Feature Model for Ki-67 Expression in Hepatocellular Carcinoma
Authors Huang H ![]() , Yang J
, Yang J ![]() , Zhang Y
, Zhang Y ![]() , Pan X, Chen L
, Pan X, Chen L ![]() , Huang Y, Wang X
, Huang Y, Wang X ![]() , Lu W
, Lu W ![]() , Huang Z, Ding K
, Huang Z, Ding K
Received 5 March 2026
Accepted for publication 7 May 2026
Published 15 May 2026 Volume 2026:13 605592
DOI https://doi.org/10.2147/JHC.S605592
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Ahmed Kaseb
Haibo Huang,1,* Jie Yang,1,* Yingdan Zhang,1,* Xianpan Pan,2 Lei Chen,2 Yingying Huang,3 Xiaocheng Wang,4 Wei Lu,5 Zehe Huang,3 Ke Ding1
1Department of Radiology, Nanning Second People’s Hospital, Nanning, Guangxi, 530031, People’s Republic of China; 2Shanghai United Imaging Intelligence Co., Ltd, Shanghai, 200232, People’s Republic of China; 3Department of Radiology, The First People’s Hospital of Qinzhou, Qinzhou, Guangxi, 530550, People’s Republic of China; 4Department of Oncology, Nanning Second People’s Hospital, Nanning, Guangxi, 530031, People’s Republic of China; 5Department of Pathology, Nanning Second People’s Hospital, Nanning, Guangxi, 530031, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Ke Ding, Department of Radiology, Nanning Second People’s Hospital, No. 13 Dancun Road, Nanning, 530031, People’s Republic of China, Tel +86-15907718322, Email [email protected] Zehe Huang, Department of Radiology, the First People’s Hospital of Qinzhou, Qinzhou, 530550, Guangxi, People’s Republic of China, Tel +86-18977765011, Email [email protected]
Objective: Ki-67 is a well-established biomarker for tumor aggressiveness and poor prognosis in hepatocellular carcinoma (HCC). A reliable non-invasive method for preoperative Ki-67 assessment is clinically needed for risk stratification and individualized treatment. This study aimed to develop and validate a prediction model integrating triphasic contrast-enhanced CT radiomics with clinical features for preoperative Ki-67 expression status in HCC.
Materials and Methods: This retrospective dual-center study enrolled 200 patients with 213 pathologically confirmed HCC lesions, Ki-67 expression was dichotomized as high (Ki-67 > 20%) and low (≤ 20%) based on established clinical criteria. Radiomic features were extracted from arterial, portal venous, and delayed phases. After rigorous feature selection, logistic regression was used to construct single-phase models, a multi-phase radiomics fusion model, a clinical model, and a combined clinical-radiomics fusion model. Performance was assessed by area under the curve, net reclassification index, integrated discrimination improvement, and decision curve analysis.
Results: The combined fusion model showed robust discrimination, with AUCs of 0.866 and 0.824 in the training and internal test sets, respectively. In independent external validation (n=64), it achieved an AUC of 0.829 (95% CI: 0.709– 0.948), significantly outperforming the arterial phase model (AUC=0.713, P=0.031) and the radiomics-only fusion model (AUC=0.722, P=0.031). NRI and IDI confirmed significant incremental value (NRI=0.374, P=0.005; IDI=0.191, P< 0.001), and DCA demonstrated superior clinical net benefit.
Conclusion: The fusion model integrating multi-phase CECT radiomic features with clinical indicators provides an effective, non-invasive tool for preoperative prediction of Ki-67 expression in HCC. It may facilitate risk stratification and inform individualized treatment planning in clinical practice.
Plain Language Summary: Question: A reliable non-invasive method for preoperative Ki-67 assessment in HCC is needed for risk stratification and personalized treatment.
Findings: A model combining triphasic CT radiomics and clinical features effectively predicted Ki-67 expression, showing robust performance (AUC=0.829) in external validation.
Clinical Relevance Statement: This CT-based model provides an accessible, non-invasive tool to preoperatively assess tumor proliferation, potentially aiding individualized treatment planning and improving prognosis in HCC patients. Diagram of a five-step process: tumor segmentation, feature extraction, selection, model building, evaluation.The diagram outlines a five-step process for creating a model to predict Ki-67 non-invasively before surgery. Step 1 involves segmenting the tumor using liver images and CT scans. Step 2 extracts features like statistics, texture, shape and high-order elements, combined with clinical data. Step 3 selects features using methods like correlation coefficient, mMRMR, KBEST and LASSO. Step 4 constructs models integrating radiomics, clinical and clinical-radiomics data via logistic regression. Step 5 evaluates the model with graphs showing true positive rate vs. false positive rate and net benefit vs. threshold probability. Data from 200 patients with 213 HCC lesions, using triphasic CECT and radiomics plus clinical features, supports clinical-radiomics fusion. External validation shows AUC 0.829, surpassing AP with p=0.031, NRI=0.374 and IDI=0.191. The model aids in risk stratification and personalized treatment.
Keywords: hepatocellular carcinoma, tomography, x-ray computed, radiomics, ki-67 antigen, predictive model, clinical features
Introduction
Hepatocellular carcinoma (HCC) is a leading cause of cancer-related mortality worldwide.1 Although surgical resection offers a curative option for early-stage disease, postoperative recurrence rate remains high, posing a significant clinical challenge.2,3 Ki-67, a nuclear protein associated with cell proliferation, is a well-established biomarker correlating with aggressive pathological features and unfavourable prognosis in HCC, serving as an important tool for risk stratification.4–6 Therefore, an accurate, non-invasive preoperative assessment of Ki-67 expression level holds significance value for formulating individualized treatment strategies.
Radiomics, by extracting high-throughput quantitative features from medical images, offers a promising approach for non-invasive assessment of tumor heterogeneity.7 While magnetic resonance imaging (MRI)-based radiomics has shown efficacy in predicting HCC biology.8,9 Contrast-enhanced CT (CECT) remains the more widely accessible and standardised imaging modality for preoperative HCC evaluation. Previous CT radiomics studies have primarily focused on single-phase analysis,10–12 potentially underutilising the comprehensive haemodynamic and microenvironmental information inherent in multi-phase imaging.13 Furthermore, tumour aggressiveness arises from complex interactions between genomic, phenotypic, and host microenvironmental factors, which may not be fully captured by unimodal imaging or clinical data alone. The former may miss key macroscopic pathological features like satellite nodules,14 while the latter lacks detailed quantification of tumor micro-heterogeneity.15
Several CT-based radiomics models have been developed for Ki-67 prediction in HCC. Wu et al constructed a combined model integrating radiomics features and clinical indicators, achieving a C-index of 0.88 for Ki-67 prediction.16 Similarly, Cai et al developed an enhanced CT-based predictive model for preoperative Ki-67 assessment in HCC.17 However, most existing studies rely on single-phase CT data and lack independent external validation, limiting their generalizability. To our knowledge, no study has developed a triphasic CT fusion model with dual-center validation for preoperative Ki-67 stratification in HCC.
This study hypothesises that integrating radiomic features from arterial, venous, and delayed phase CT images with key clinicopathological indicators can provide a more comprehensive characterisation of HCC, leading to improved preoperative prediction of Ki-67 expression status. We aimed to develop and rigorously validate such a clinical-radiomics fusion model through internal testing and independent external centre validation.
Materials and Methods
The overall study design and analytical workflow are illustrated in Figure 1.
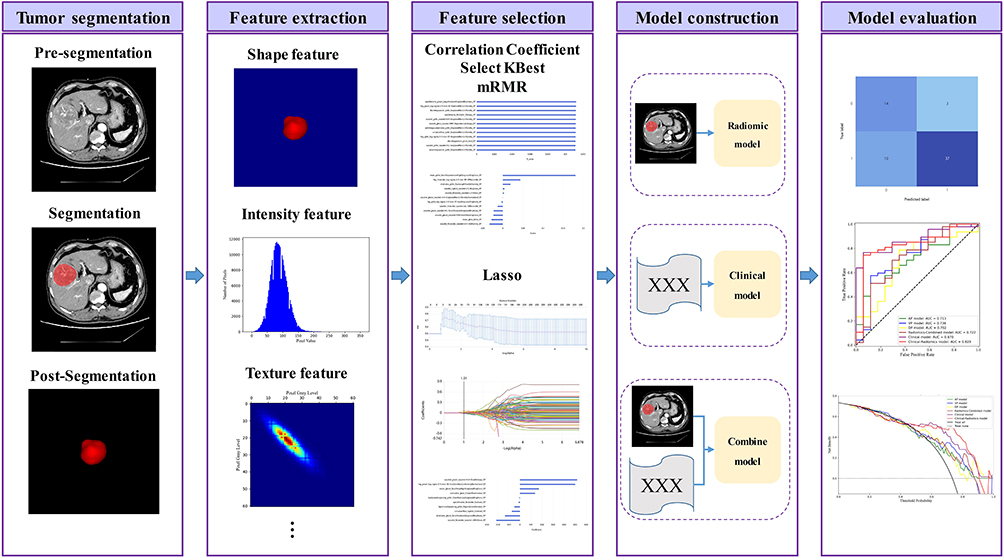 |
Figure 1 Study flowchart. |
Study Population
This retrospective dual-center study was conducted in accordance with the Declaration of Helsinki. Consecutive patients who underwent radical liver resection for solitary HCC between January 2018 and October 2025 at Nanning Second People’s Hospital (Centre A) and Qinzhou First People’s Hospital (Centre B) were screened.
The study was approved by the Ethics Committee of Nanning Second People’s Hospital on December 12, 2025 (Approval No.: Y2025341), as a pre-specified sub-study of the approved project “Pathological characteristics of Hepatocellular Carcinoma: Correlation Analysis and Clinical prognostic Value”. The research content of this manuscript, including the triphasic CT radiomics analysis and Ki-67 expression prediction, falls entirely within the scope of the initial ethical review, so no separate ethical approval was required for this sub-study. Informed consent was waived due to the retrospective nature of the study.
Inclusion Criteria Were
① Standard triphasic liver CECT performed within 4 weeks preoperatively with diagnostic image quality; ② Available postoperative Ki-67 immunohistochemistry results; ③ Complete clinicopathological data.
Exclusion Criteria Were
① Any prior antitumor therapy; ② Severe image artifacts or indistinct lesion borders; ③ Pathological diagnosis other than HCC (eg, mixed hepatocellular-cholangiocarcinoma); ④ Infiltrative HCC.
A total of 200 patients with 213 lesions were finally enrolled (comprising 149 lesions from Center A and 64 lesions from Center B). Lesions from Center A were randomly split into a training set (n=104 lesions) and a internal test set (n=45 lesions) in a 7:3 ratio. All lesions from Center B constituted an independent external validation set (n=64). The patient screening and enrollment process is summarized in Figure 2. The sample size was deemed adequate based on the events-per-variable criterion >10 in the training set to mitigate overfitting.18
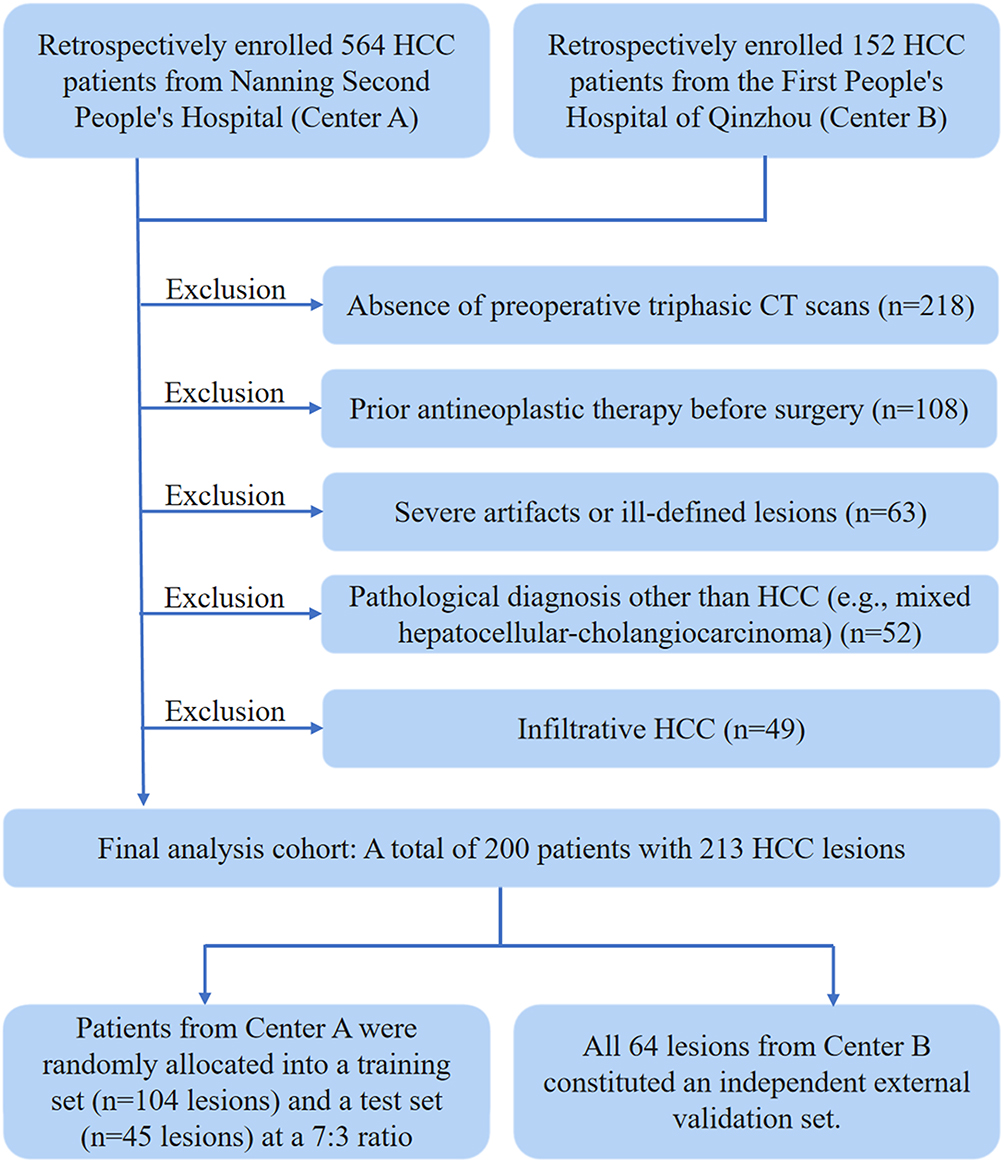 |
Figure 2 Cohort of patients. |
Clinical Data and Pathological Reference Standard
Preoperative clinical data (age, gender, hepatitis B/C virus history, cirrhosis, serum alpha-fetoprotein [AFP]) were retrieved from electronic medical records. Surgical specimens were evaluated by two senior pathologists blinded to imaging data, recording Edmondson-Steiner grade, microvascular invasion (MVI) grade (M0: none; M1: ≤5 MVIs within ≤1 cm of tumor; M2: >5 MVIs or >1 cm from tumor),17,19 and satellite nodules presence (defined as microscopic/macroscopic nodules ≤2 cm from main tumor). Ki-67 expression index was determined by immunohistochemistry. Based-on relevant guidelines and consensus,5,20 a Ki-67 index >20% defined the high-expression group, and ≤20% the low-expression group. The 20% threshold for Ki-67 stratification was selected based on its widespread use in previous imaging-based prediction studies of HCC, where it has demonstrated robust prognostic discrimination.
CT Image Acquisition, Preprocessing, and Feature Extraction
Both centers used CT scanners (GE Discovery CT 750HD; Siemens SOMATOM Definition Flash) for standard liver triphasic enhanced scanning. Thin-slice images (≤1.5 mm) in DICOM format were imported into the United Imaging uAI Research Portal for standardised preprocessing: window width/level normalization (width 300 HU, level 40 HU) and isotropic voxel resampling (1×1×1 mm3). Two radiologists blinded to pathology, independently manually delineated three-dimensional volume of interest (VOI) encompassing the entire tumor on each phase, avoiding large vessels, necrosis, and hemorrhage areas. Inter-observer consistency was excellent (Dice=0.945). Using the PyRadiomics engine, 2264 radiomic features (first-order, shape, texture [GLCM, GLDM, GLRLM, GLSZM, NGTDM]), and wavelet-filtered features) were extracted from each phase VOI per reader. Feature stability was assessed via intraclass correlation coefficient (ICC); features with ICC > 0.75 (92.0% of features) were retained for subsequent analysis.
Feature Selection and Model Construction
All modeling steps were performed within the training set (n=104 lesions).
Radiomics Feature Selection for Single-Phase Models
For features from each phase (arterial [AP], portal venous [PVP], delayed [DP]), Z-score normalization was applied. Dimensionality reduction was performed in a strict, stepwise manner: (a) initial screening using Pearson correlation analysis (retaining features with P < 0.05); (b) selection of the top 100 most relevant features using the SelectKBest algorithm; (c) further refinement to 50 features with maximum relevance and minimum redundancy using the minimum Redundancy Maximum Relevance (mRMR) algorithm; (d) final selection of the most parsimonious and predictive feature subset via LASSO regression with 10-fold cross-validation.
Multi-Phase Feature Fusion Model
Radiomic features from all three phases were merged into an initial multi-phase feature pool. Feature selection was then performed following the same sequential procedure described above (Pearson correlation → SelectKBest → mRMR → LASSO with 10-fold cross-validation). The selected features were used to construct the multi-phase radiomics fusion model.
Clinical Feature Selection
Clinicopathological variables were first evaluated by univariate analysis (P < 0.1). Variables with statistical significance were subsequently entered into multivariate logistic regression using a forward stepwise method (P < 0.05 for entry) to identify independent predictors, which were then used to build the clinical model.
Clinical-Radiomics Fusion Model
The features selected for the multi-phase radiomics fusion model (ie., the LASSO-selected subset) were combined with the independent clinical predictors identified in step (3). The mRMR algorithm was reapplied to this combined feature set to select the most discriminative features. These features were used to build the final clinical-radiomics fusion model via logistic regression.
Statistical Analysis
Statistical analysis was performed using R (version 4.2.0) and the uAI Research Portal. Continuous variables are presented as mean ± SD or median (interquartile range); categorical variables as frequency (percentage). Inter-group comparisons used ANOVA, Kruskal–Wallis H-test, chi-square test, or Fisher’s exact test. Model performance was evaluated by AUC, sensitivity, specificity, accuracy, and F1-score. DeLong’s test compared AUCs in the external validation set. Net reclassification improvement (NRI) and integrated discrimination improvement (IDI) assessed incremental value. Decision curve analysis (DCA) evaluated clinical net benefit. A two-sided P < 0.05 considered statistical significance.
Results
Patient Baseline Characteristics
Baseline characteristics were balanced across the training, internal test, and external validation sets (P > 0.05 for all comparisons), including age, gender, aetiology, Edmondson-Steiner grade, MVI grade, satellite nodule status, serum AFP, and liver function markers (Table 1). The proportion of patients with high Ki-67 expression was relatively high in the overall cohort.
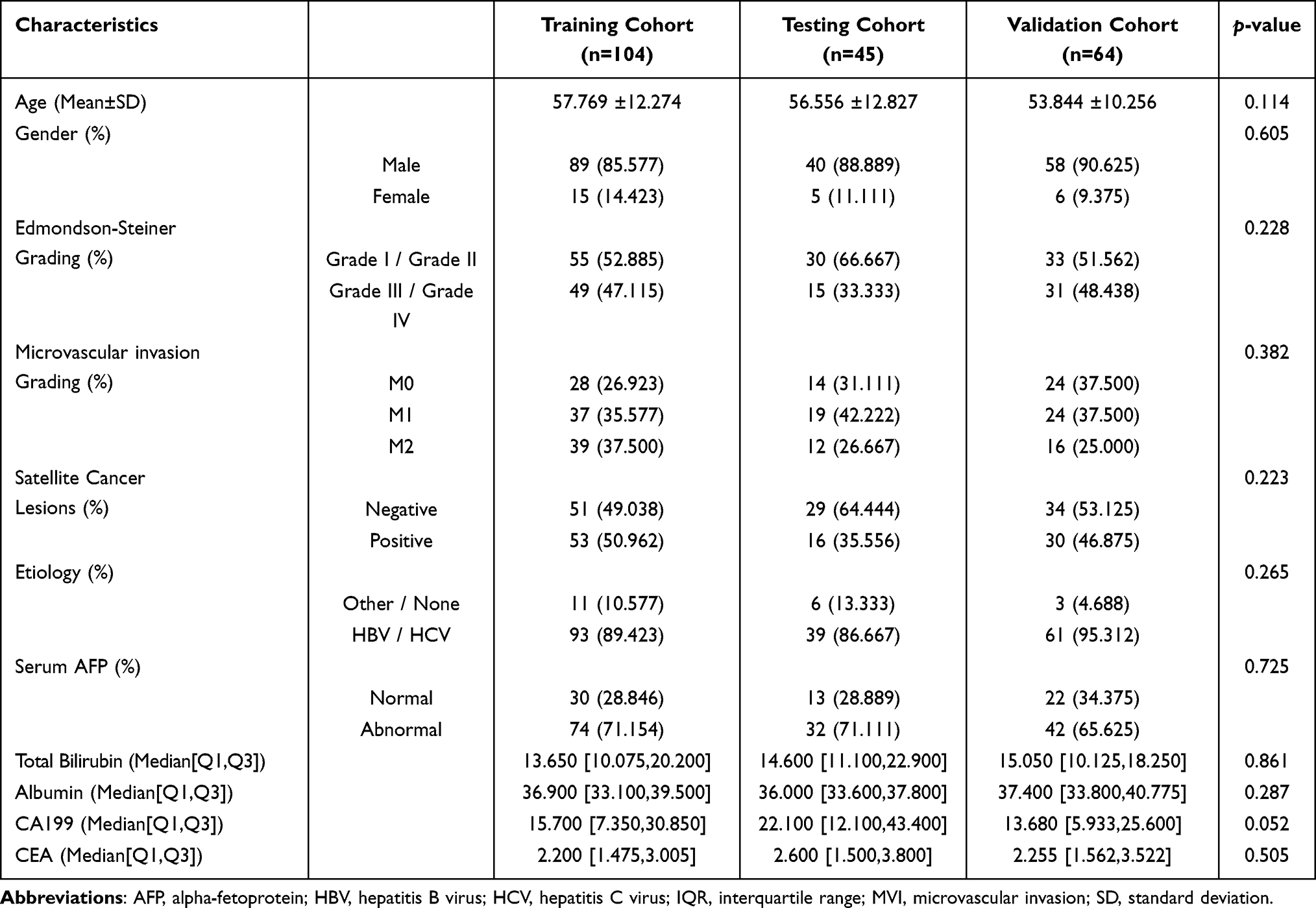 |
Table 1 Baseline Demographic and Clinicopathological Characteristics of Patients |
Comparison of Model Predictive Performance
Performance metrics are summarised in Table 2, and the corresponding ROC curves are shown in Figure 3. In the external validation set, the clinical model achieved the highest AUC (0.867), followed by the clinical-radiomics fusion model (AUC=0.829, 95% CI: 0.709–0.948). The AUCs for AP, PVP, and DP multi-phase radiomics fusion model were 0.713, 0.736, 0.702 and 0.722, respectively. DeLong’s test (Table 3) showed the fusion’s AUC was significantly higher than that of the AP model (P=0.031) and the multi-phase radiomics fusion model (P=0.031). The differences in AUC between the fusion model and the PVP, DP and clinical models were not statistically significant (P>0.05). The fusion models also showed robust performance in the training (AUC=0.866) and internal test (AUC=0.824) sets.
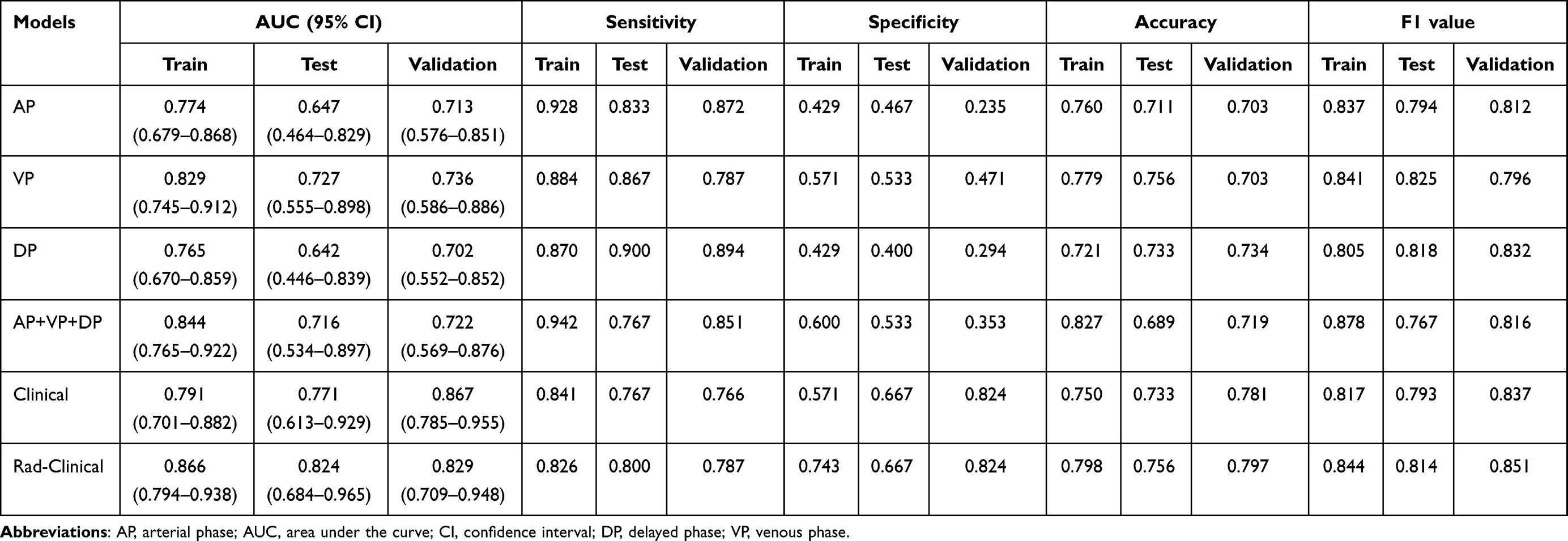 |
Table 2 Performance of Logistic Regression-Based Prediction Models Across Different Datasets |
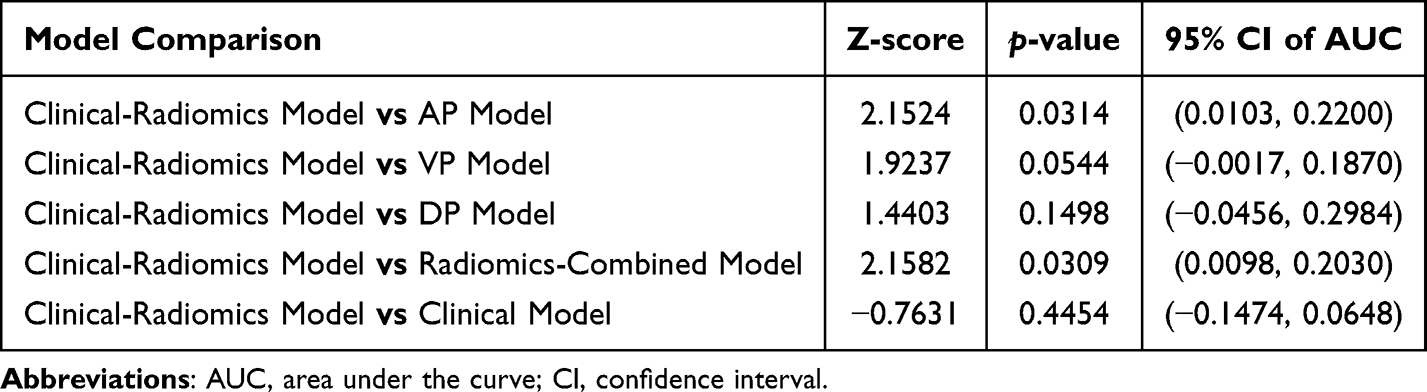 |
Table 3 Comparison of Model AUCs in the External Validation Set Using DeLong’s Test |
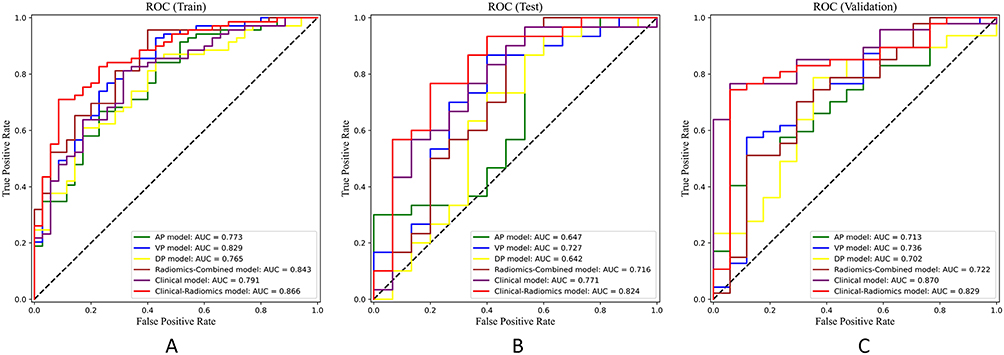 |
Figure 3 ROC curves in different predictive models in the (A) training set, (B) internal test set, and (C) external validation set. |
Incremental Predictive Value of the Models
NRI and IDI analysis (Table 4) confirmed the significant incremental value of the fusion model. For example, compared to the AP model at a risk threshold of 0.6, the categorical NRI was 0.374 (P=0.005), continuous NRI was 0.774 (P=0.003), and IDI was 0.191 (P<0.001). Decision curve analysis (Figure 4) demonstrated that within a threshold probability range of 0.1 to 0.7, the clinical-radiomics fusion model provided a higher net benefit than both thetreat all and “treat none” strategies, as well as the single-phase and the radiomics-only fusion model.
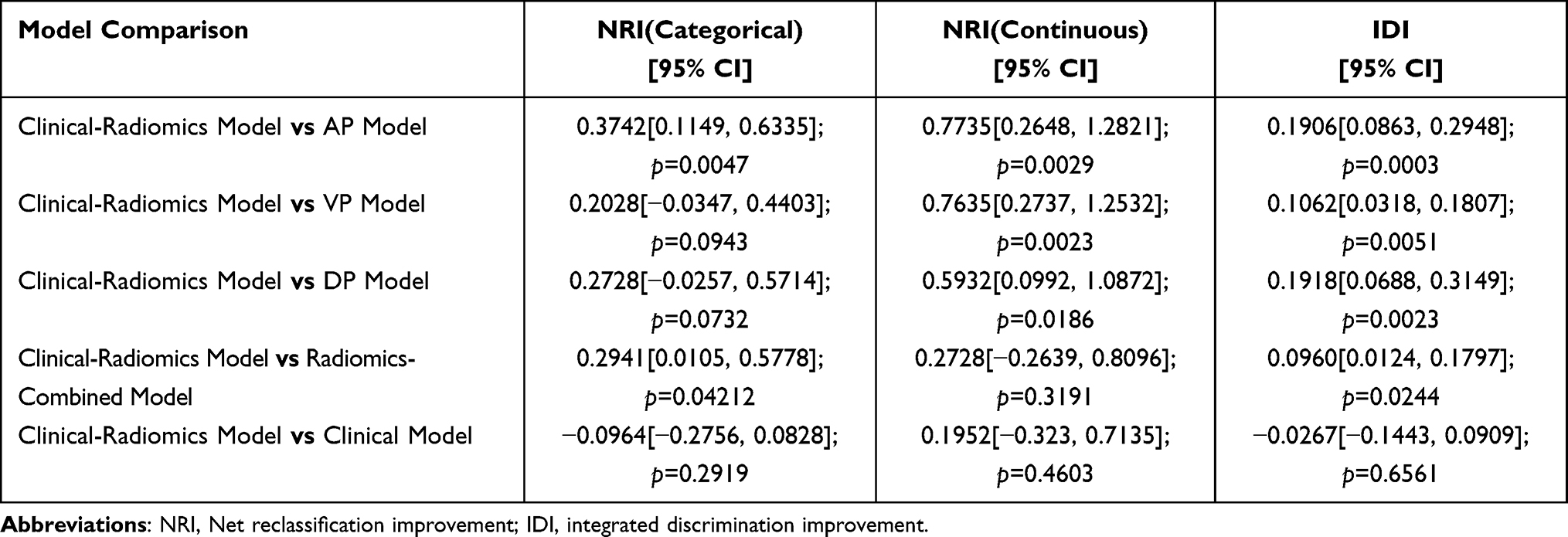 |
Table 4 NRI and IDI Test (External Validation Set, Categorical Threshold Set to 0.6) |
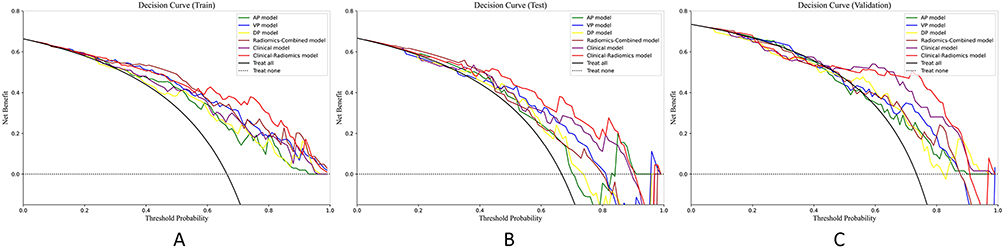 |
Figure 4 DCA for the clinical-radiomics fusion model and other models in the (A) training set, (B) internal test set, and (C) external validation set. |
Analysis of Key Features
Key features selected by LASSO regression for each model are shown in Figure 5. In the final clinical-radiomics fusion model, features with higher weights included venous-phase texture features (eg., mean_glszm_SmallAreaHighGrayLevelEmphasis) and the clinical feature “Satellite Nodule (Positive).” Some arterial-phase texture features (eg., wavelet-HHL_glcm_Correlation) had negative weights.
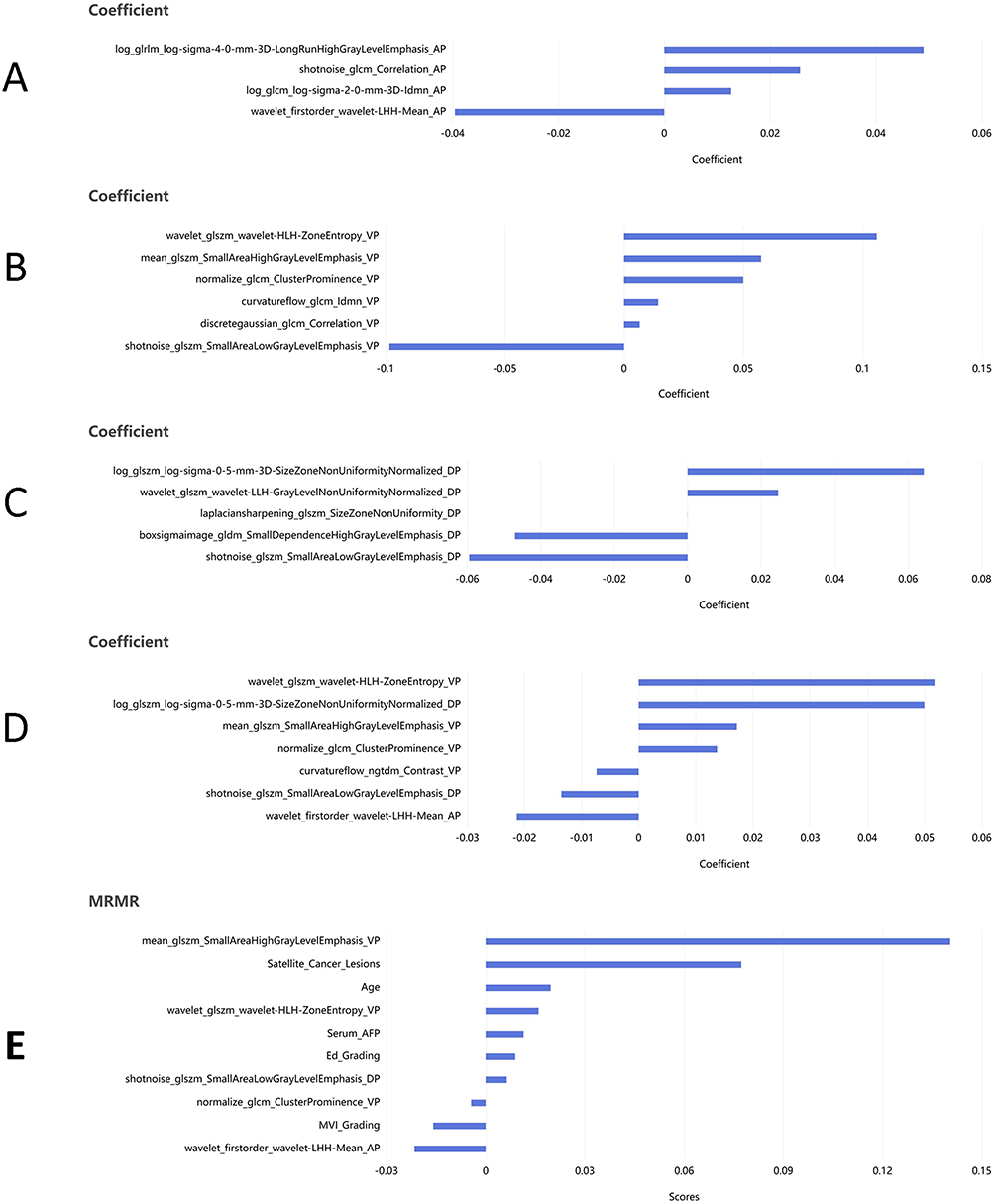 |
Figure 5 LASSO feature importance analysis.(A) Key features selected by LASSO regression for the arterial phase model. (B) Key features selected by LASSO regression for the venous phase model. (C) Key features selected by LASSO regression for the delayed phase model. (D) Key features selected by LASSO regression for the multi-phase radiomics fusion model. (E) Key features for the clinical-radiomics fusion model selected via mRMR optimization and LASSO regression. |
Discussion
This study developed and validated a clinical-radiomics fusion model integrating triphasic CT radiomics and clinical features for preoperative prediction of Ki-67 expression in HCC. The model demonstrated robust performance in independent external validation (AUC 0.829), confirming the hypothesis that multi-dimensional information enables a more comprehensive assessment of tumor proliferative activity than single-dimension approaches.
Innovation and Advantages of Multidimensional Fusion
Previous prediction models mostly relied on a single information dimension—either radiomics21 or clinicopathological indicators alone.15 However, the biological behavior of HCC is highly complex, and a single dimension hardly captures its full aggressiveness and proliferative nature. Radiomic features can quantify intratumoral heterogeneity, potentially reflecting microstructures such as cellular density, necrosis, and fibrosis;22 clinicopathological features (eg., satellite nodules) are macroscopic manifestations of tumor invasiveness. This study is among the first to organically integrate these two complementary information on a conventional CT platform. The fusion model’s performance significantly exceeded that of some single-dimension models (eg., arterial-phase model), aligning with the core concept of multimodal integrated analysis in precision medicine.23
Biological Plausibility of Key Radiomic and Clinical Features
The key features selected for the fusion model have clear biological rationale. The high weight of PVP texture features (eg., wavelet-LHL_glszm_SmallAreaHighGrayLevelEmphasis) corresponds to the dense microvascular structures frequently observed in highly proliferative tumors, reflecting uniform perfusion in the portal venous stage.6 This imaging phenotype may mirror the pathophysiological basis of highly proliferative HCCs, which often exhibit dense sinusoidal microvasculature and more homogeneous perfusion. Conversely, the negative weights of some arterial-phase features (eg., wavelet-HHL_glcm_Correlation) may indicate disorganized patterns of abnormal neovascularization, mirroring the angiogenic dysregulation associated with tumor proliferation.6 The extraction and interpretation of these quantitative imaging phenotypes are underpinned by standardized radiomics methodologies.24 Together, these complementary features map key pathophysiological processes—from aberrant arterial supply to the proliferative microenvironment—thereby enhancing the model’s characterization of tumor biology.
Furthermore, the inclusion of the clinical feature “Satellite nodule (Positive)” adds a direct macroscopic dimension. As a direct radiological sign of intrahepatic metastasis,14 its strong predictive power biologically complements the cellular proliferation information conveyed by the Ki-67 index, providing a multi-scale assessment of tumor aggressiveness. Consequently, our model establishes a biologically interpretable framework by synthesizing information across vascular, micro-environmental, and macro-invasive scales.
Biological Interpretability of Radiomic Features
Although our study is a purely diagnostic radiomics investigation without direct molecular correlates, it is worth speculating on potential biological links between our radiomic features and underlying molecular pathways in HCC. Emerging evidence has revealed that metabolic reprogramming—particularly lactylation modifications—plays a critical role in HCC malignant progression. For instance, ABCF1-K430 lactylation was shown to promote HCC growth and metastasis via transcriptional activation of the HIF1 signaling pathway.25 Similarly, ASH2L-K312 lactylation stimulates tumor angiogenesis and accelerates HCC progression through VEGFA-mediated mechanisms.26 Furthermore, ferritinophagy-related gene FTH1 has been identified as a key regulator linking tryptophan metabolism to redox homeostasis and ferroptosis, with prognostic implications in HCC.27
Our venous-phase texture features, which may reflect microvascular heterogeneity and perfusion abnormalities, could indirectly capture the hemodynamic consequences of HIF1 pathway activation or lactylation-driven microenvironment remodeling. The inclusion of satellite nodules as a clinical predictor in our model aligns with their known association with aggressive angiogenic phenotypes, which may be driven by ASH2L-mediated VEGFA upregulation. While these connections remain speculative, they provide a foundation for future studies to directly correlate radiomic features with tissue-based molecular markers (eg, ABCF1/ASH2L expression, FTH1 activity, or lactate levels).
Comparison with Existing Literature
The external validation efficacy of our model (AUC=0.829) is comparable to recent studies based on advanced imaging techniques like spectral CT9 and MRI (AUC=0.80–0.90).8,10 However, spectral CT is not yet widely available, and MRI has cost and accessibility limitations. In contrast, by fusing triphasic features with clinical indicators on the ubiquitous conventional CECT platform, we constructed a high-performance and more universally applicable predictive tool. This success corroborates recent similar research; for example, a 2025 study based on CT radiomics and clinical features also achieved a high AUC in external validation for predicting HCC microvascular invasion.28
It is noteworthy that in external validation, although the clinical-radiomics fusion model achieved the highest AUC (0.829), its performance did not show a statistically significant difference compared to the PVP model (AUC=0.736), the DP model (AUC=0.702), or the clinical-only model (AUC=0.867) (P > 0.05). Several reasons may account for this. First, PVP and DP images inherently capture pathophysiological features such as tumor microvascular structure, fibrosis, and extracellular space, which are intrinsically linked to Ki-67 expression, thereby endowing the single-phase models with substantial discriminative power. Second, during multi-phase feature fusion, some key predictive information might already be encapsulated within features from these two phases, resulting in a statistically non-significant incremental gain. Third, the limited sample size of the validation set may have reduced statistical power. Regarding the clinical-only model, its strong performance stems from the inclusion of powerful predictors like “satellite nodule”, a well-established marker of tumor aggressiveness. That our fusion model did not significantly surpass it statistically underscores the substantial predictive value of these conventional clinical indicators. However, the key advantage of the fusion model lies in its sole reliance on preoperative, non-invasive data, achieving predictive efficacy comparable to clinical model that incorporates some postoperative pathological factors. This makes the fusion model a novel and comprehensive tool for preoperative decision-making.
Incremental Value: NRI and IDI Analyses
Beyond conventional AUC comparison, the NRI and IDI metrics were employed to quantify the incremental clinical utility of the fusion model.29,30 Compared to the AP model, the fusion model yielded a continuous NRI of 0.774 (P=0.003) and a categorical NRI (threshold 0.6) of 0.374 (P=0.005), indicates a substantial overall improvement in risk stratification and a net correct reclassification of approximately 37.4% of patients at a clinically relevant threshold.
IDI was also significant (0.191, P<0.001). These metrics quantitatively prove the fusion model’s significant incremental predictive value over single-phase and radiomics-only models. Notably, a recent CECT-based study31 found that its fusion model did not show significant incremental value, a discrepancy that may stem from methodological differences: our study employed a rigorous phase-wise selection-then-fusion strategy and included potent clinical predictors like satellite nodules. Importantly, NRI and IDI compared to the clinical model alone did not reach statistical significance. This observation, combined with their comparable AUCs, underscores a critical finding: our clinical-radiomics fusion model, using exclusively preoperative and non-invasive data, achieved predictive performance on par with a clinical model that incorporated powerful postoperative pathological features. This parity highlights the self-contained strength of the fusion model and its unique value as a preoperative decision-support tool.
We acknowledge that more sophisticated interpretability methods, such as SHapley Additive exPlanations (SHAP) analysis or permutation-based interaction tests, would provide deeper insights into feature contributions and interactions. These approaches should be prioritized in future studies to enhance model transparency and clinical trust.
Clinical Translation Pathway and Prospects
The model is based on logistic regression, and is computationally lightweight, and can be readily integrated into existing hospital infrastructures such as PACS or radiology reporting platforms. It can be embedded into the preoperative CECT workflow as an auxiliary diagnostic module, providing a quantitative risk score for Ki-67 expression to aid preoperative risk stratification, inform treatment decisions (eg., surgical planning, adjuvant therapy), and personalize follow-up strategies. The next step requires prospective, multi-center studies to validate the model’s efficacy and clinical utility in real-world settings and to promote the development of standardized operating procedures to ensure reproducibility and generalizability.32
Summary and Clinical Implications
In summary, this study developed and validated a clinical-radiomics fusion model based on ubiquitous triphasic CECT. The model enables non-invasive, preoperative prediction of Ki-67 expression in HCC with robust performance, rooted in a biologically plausible framework that integrates features reflecting aberrant angiogenesis, proliferative microenvironment, and macroscopic invasiveness. By leveraging routinely acquired CT scans, this tool provides a feasible means for preoperative assessment of tumor proliferation potential and holds significant promise for aiding individualized treatment planning in HCC patients, meriting further prospective validation.
However, the generalizability of our findings is currently limited to patients with solitary lesions and HBV-predominant HCC from Chinese centers. Validation in broader populations with diverse etiologies is required before clinical implementation. Notably, the fusion model relies exclusively on preoperative data, whereas traditional clinical models often incorporate postoperative pathological features such as satellite nodules, giving our approach a distinct advantage for preoperative treatment planning and patient stratification.
Limitations and Future Directions
This study has limitations. Its retrospective design is subject to selection bias. Several additional limitations regarding generalizability should be acknowledged. First, our cohort consisted exclusively of patients with solitary lesions; the model’s performance in multifocal HCC remains unknown. Second, the study population was predominantly HBV-related, reflecting the epidemiology of HCC in China. Validation in populations with different etiologies (eg., HCV, NASH, alcoholic liver disease) is warranted. Third, although dual-center validation was performed, both centers are located in China; international multi-center studies are needed to confirm the model’s robustness across diverse populations. Finally, the external validation cohort had a relatively modest sample size, and larger studies may be required to definitively confirm the incremental value of the fusion model over single-phase approaches.
Although external validation was performed, the sample size, particularly of the validation set, could be expanded. Differences in CT scanners and protocols between centers, despite standardised preprocessing, may still affect feature stability. Future studies should validate the model’s robustness through large-scale, prospective, multi-center research. Additionally, future work should aim to construct an “imaging-clinical-molecular” triad model incorporating serum biomarkers (eg., lactate, tryptophan metabolites) or tissue-based molecular markers (eg., ABCF1/ASH2L lactylation status, FTH1 expression) into the radiomics framework. Such integrated models could enhance both predictive accuracy and biological interpretability. Federated learning approaches may help address multi-center molecular data heterogeneity while preserving patient privacy, and exploring associations between model predictions and responses to targeted therapies (eg., HIF1 inhibitors, anti-angiogenic agents, or ferroptosis inducers) could further strengthen the clinical translational value of radiomics-based biomarkers in HCC.33,34
Abbreviations
AFP, alpha-fetoprotein; AUC, area under the curve; CECT, contrast-enhanced computed tomography; CI, confidence interval; DCA, decision curve analysis; GLCM, gray-level co-occurrence matrix; GLDM, gray-level dependence matrix; GLRLM, gray-level run length matrix; GLSZM, gray-level size zone matrix; HBV, hepatitis B virus; HCC, hepatocellular carcinoma; HCV, hepatitis C virus; ICC, intraclass correlation coefficient; IDI, integrated discrimination improvement; LASSO, least absolute shrinkage and selection operator; mRMR, minimum redundancy maximum relevance; MRI, magnetic resonance imaging; MVI, microvascular invasion; NGTDM, neighboring gray tone difference matrix; NRI, net reclassification index; OR, odds ratio; ROC, receiver operating characteristic; ROI, region of interest; SD, standard deviation; SN, satellite nodule; SOP, standard operating procedure; VOI, volume of interest.
Statistics and Biometry
One of the authors (Xianpan Pan, an employee of Shanghai United Imaging Intelligence Co., Ltd.) has significant statistical expertise.
AI Disclosure
DeepSeek-R1 was used to refine the language expression of this manuscript, focusing on grammatical accuracy and fluency.
Acknowledgments
This study received technical and nursing support from Fei He, Qin Shi, and Li Zhou. Special thanks to Qingping Zhao and Lifeng Huang for providing and confirming pathological material analysis.
Ethical Approval
This retrospective study was conducted in accordance with the Declaration of Helsinki and was approved by the Ethics Committee of Nanning Second People’s Hospital (Approval No.: Y2025341; Date: December 12, 2025). The requirement for informed consent was waived by the ethics committee owing to the retrospective nature of the study. Patient data confidentiality was strictly maintained throughout the study; all data were fully anonymized prior to analysis.
Informed Consent
Written informed consent was waived by the Institutional Review Board due to the retrospective nature of this study, which utilized anonymized data.
Funding
This study was supported by two Self-raised Projects of the Health Commission of Guangxi Zhuang Autonomous Region (Grant Nos. Z-A20241055 and Z20200953).
Disclosure
Haibo Huang reports grants from Health Commission of Guangxi Zhuang Autonomous Region, non-financial support from Shanghai United Imaging Intelligence Co., Ltd., during the conduct of the study; Jie Yang reports grants from Health Commission of Guangxi Zhuang Autonomous Region, non-financial support from Shanghai United Imaging Intelligence Co., Ltd., during the conduct of the study; Yingdan Zhang reports grants from Health Commission of Guangxi Zhuang Autonomous Region, non-financial support from Shanghai United Imaging Intelligence Co., Ltd., during the conduct of the study; Xianpan Pan reports grants from Health Commission of Guangxi Zhuang Autonomous Region, non-financial support from Shanghai United Imaging Intelligence Co., Ltd., during the conduct of the study; Yingying Huang reports grants from Health Commission of Guangxi Zhuang Autonomous Region, non-financial support from Shanghai United Imaging Intelligence Co, during the conduct of the study; Xiaocheng Wang reports grants from Health Commission of Guangxi Zhuang Autonomous Region, non-financial support from Shanghai United Imaging Intelligence Co., Ltd., during the conduct of the study; Wei Lu reports grants from Health Commission of Guangxi Zhuang Autonomous Region, non-financial support from Shanghai United Imaging Intelligence Co., Ltd., during the conduct of the study; Zehe Huang reports grants from Health Commission of Guangxi Zhuang Autonomous Region, non-financial support from Shanghai United Imaging Intelligence Co., Ltd, during the conduct of the study. The authors report no other conflicts of interest in this work. Xianpan Pan and Lei Chen are employees of Shanghai United Imaging Intelligence Co., Ltd., which provided the uAI Research Portal platform used for radiomics analysis in this study. They did not have any additional role in the study design, data collection and analysis, decision to publish, or preparation of the manuscript.
References
1. Bray F, Laversanne M, Sung H, et al. Global cancer statistics 2022: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2024;74:229–15. doi:10.3322/caac.21834
2. Rumgay H, Arnold M, Ferlay J, et al. Global burden of primary liver cancer in 2020 and predictions to 2040. J Hepatol. 2022;77:1598–1606. doi:10.1016/j.jhep.2022.08.021
3. European association for the study of the l. easl clinical practice guidelines on the management of hepatocellular carcinoma. J Hepatol. 2025;82:315–374. doi:10.1016/j.jhep.2024.08.028
4. Singal AG, Llovet JM, Yarchoan M, et al. AASLD Practice Guidance on prevention, diagnosis, and treatment of hepatocellular carcinoma. Hepatology. 2023;78:1922–1965. doi:10.1097/HEP.0000000000000466
5. Department of Medical Administration. National health commission of the people’s republic of china. guideline for diagnosis and treatment of primary liver cancer (2024 edition). Chin. J. Hepatol. 2024;32:581–630.
6. Jagtap SV. Evaluation and prediction of Ki-67 expression in hepatocellular carcinoma. World J Gastrointest Oncol. 2025;17:106529. doi:10.4251/wjgo.v17.i10.106529
7. Lambin P, Leijenaar RTH, Deist TM, et al. Radiomics: the bridge between medical imaging and personalized medicine. Nat Rev Clin Oncol. 2017;14:749–762. doi:10.1038/nrclinonc.2017.141
8. Zhou L, Chen Y, Li Y, Wu C, Xue C, Wang X. Diagnostic value of radiomics in predicting Ki-67 and cytokeratin 19 expression in hepatocellular carcinoma: a systematic review and meta-analysis. Front Oncol. 2023;13:1323534. doi:10.3389/fonc.2023.1323534
9. Deng J, Tang Q, Wei Q, Ruan F, Li X, Long L. Preoperative assessment of Ki-67 expression in hepatocellular carcinoma using a multi-parametric spectral CT approach. Quant Imaging Med Surg. 2025;15:4262–4273. doi:10.21037/qims-24-2313
10. Fan Y, Yu Y, Wang X, Hu M, Hu C. Radiomic analysis of Gd-EOB-DTPA-enhanced MRI predicts Ki-67 expression in hepatocellular carcinoma. BMC Med Imaging. 2021;21:100. doi:10.1186/s12880-021-00633-0
11. Chinese College of Hepatocellular Carcinoma, Chinese Medical Doctor Association. Chinese expert consensus on diagnosis and treatment of hepatocellular carcinoma with microvascular invasion (2024 edition). Chin. J. Dig. Dis. 2024;153–164.
12. Xia TY, Zhou ZH, Meng XP, et al. Predicting microvascular invasion in hepatocellular carcinoma using ct-based radiomics model. Radiology. 2023;307:e222729. doi:10.1148/radiol.222729
13. Huang H, Pan X, Zhang Y, et al. Triphasic CT radiomics model for preoperative prediction of hepatocellular carcinoma pathological grading. J Hepatocell Carcinoma. 2025;12:1725–1742. doi:10.2147/JHC.S527056
14. Zuo XY, Liu HF. Biparametric magnetic resonance imaging-based radiomic and deep learning models for predicting Ki-67 risk stratification in hepatocellular carcinoma. World J Hepatol. 2025;17:109530. doi:10.4254/wjh.v17.i8.109530
15. Zhou Z, Cao S, Chen C, et al. A novel nomogram for the preoperative prediction of edmondson-steiner grade iii-iv in hepatocellular carcinoma patients. J Hepatocell Carcinoma. 2023;10:1399–1409. doi:10.2147/JHC.S417878
16. Wu M, Du Z, Xiao Y, et al. CT-based radiomics for non-invasive prediction of ki-67 expression in hepatocellular carcinoma. J Hepatocell Carcinoma. 2026;13:552997. doi:10.2147/JHC.S552997
17. Cai C, Wang L, Tao L, et al. Imaging-based prediction of ki-67 expression in hepatocellular carcinoma: a retrospective study. Cancer Med. 2025;14:e70562. doi:10.1002/cam4.70562
18. Collins GS, Reitsma JB, Altman DG, Moons KG. Transparent Reporting of a multivariable prediction model for Individual Prognosis or Diagnosis (TRIPOD): the TRIPOD statement. Ann Intern Med. 2015;162:55–63. doi:10.7326/M14-0697
19. Lu M, Qu Q, Xu L, et al. Prediction for aggressiveness and postoperative recurrence of hepatocellular carcinoma using gadoxetic acid-enhanced magnetic resonance imaging. Acad Radiol. 2023;30:841–852.
20. Karabulut E, Akbulut S, Samdanci ET, et al. Are Ki-67 and procalcitonin expression levels useful in predicting the biological behavior of hepatocellular carcinoma after liver transplantation? J Clin Med. 2024;14:144. doi:10.3390/jcm14010144
21. Chang Y, Guo T, Zhu B, Liu Y. A novel nomogram for predicting microvascular invasion in hepatocellular carcinoma. Ann Hepatol. 2023;28:101136. doi:10.1016/j.aohep.2023.101136
22. Zhang LZ, Li H, Lian ZW, et al. Prediction of Ki-67 expression in hepatocellular carcinoma based on clinical and MRI radiomics model. j Clin. Radiol. 2024;43:2083–2089.
23. Ye WC, Chen WY, Lan CQ, et al. A combined radiomics model based on multi-phase contrast-enhanced MRI for predicting Ki-67 expression level in patients with hepatocellular carcinoma. J Wenzhou Med. Univ. 2024;54:1026–1033.
24. Zwanenburg A, Vallieres M, Abdalah MA, et al. The image biomarker standardization initiative: standardized quantitative radiomics for high-throughput image-based phenotyping. Radiology. 2020;295:328–338. doi:10.1148/radiol.2020191145
25. Hong H, Han H, Wang L, et al. ABCF1-K430-Lactylation promotes HCC malignant progression via transcriptional activation of HIF1 signaling pathway. Cell Death Differ. 2025;32:613–631. doi:10.1038/s41418-024-01436-w
26. Han H, Wang S, Ma L, et al. ASH2L-K312-lac stimulates angiogenesis in tumors to expedite the malignant progression of hepatocellular carcinoma. Adv Sci. 2025;12:e09477. doi:10.1002/advs.202509477
27. Cheng X, Ge X, Zhang C, et al. Tryptophan suppresses fth1-driven ferritinophagy, a key correlate of prognosis in hepatocellular carcinoma. Cell Prolif. 2026;59:e70074. doi:10.1111/cpr.70074
28. Zhong H, Zhang Y, Zhu G, et al. Preoperative prediction of microvascular invasion and relapse-free survival in hepatocellular Carcinoma >/=3 cm using CT radiomics: development and external validation. BMC Med Imaging. 2025;25:141.
29. Pencina MJ, D’Agostino RB Sr, D’Agostino RB Jr, Vasan RS. Evaluating the added predictive ability of a new marker: from area under the ROC curve to reclassification and beyond. Stat Med. 2008;27:157–172. doi:10.1002/sim.2929
30. Pencina MJ, D’Agostino RB Sr, Steyerberg EW. Extensions of net reclassification improvement calculations to measure usefulness of new biomarkers. Stat Med. 2011;30:11–21. doi:10.1002/sim.4085
31. Zhao YM, Xie SS, Wang J, et al. Added value of CE-CT radiomics to predict high Ki-67 expression in hepatocellular carcinoma. BMC Med Imaging. 2023;23:138. doi:10.1186/s12880-023-01069-4
32. Zhang J, Chen Q, Zhang Y, Zhou J. Construction of a random survival forest model based on a machine learning algorithm to predict early recurrence after hepatectomy for adult hepatocellular carcinoma. BMC Cancer. 2024;24:1575. doi:10.1186/s12885-024-13366-4
33. Hu X, Zhou J, Li Y, et al. Added value of viscoelasticity for mri-based prediction of ki-67 expression of hepatocellular carcinoma using a deep learning combined radiomics (dlcr) model. Cancers. 2022;14:2575–2585. doi:10.3390/cancers14112575
34. Shiri I, Salimi Y, Maghsudi M, et al. Differential privacy preserved federated transfer learning for multi-institutional (68)Ga-PET image artefact detection and disentanglement. Eur J Nucl Med Mol Imaging. 2023;51:40–53. doi:10.1007/s00259-023-06418-7
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
CT-Based Radiomics for the Recurrence Prediction of Hepatocellular Carcinoma After Surgical Resection
Wang F, Chen Q, Zhang Y, Chen Y, Zhu Y, Zhou W, Liang X, Yang Y, Hu H
Journal of Hepatocellular Carcinoma 2022, 9:453-465
Published Date: 23 May 2022
Clinical and Computed Tomography Characteristics of Solitary Pulmonary Nodules Caused by Fungi: A Comparative Study
Jiang J, Lv ZM, Lv FJ, Fu BJ, Liang ZR, Chu ZG
Infection and Drug Resistance 2022, 15:6019-6028
Published Date: 18 October 2022
Long-Term Follow-Up Study of COVID-19: Evaluation on Thin-Slice CT
Guan CS, Liu ZJ, Du YN, Chen H, Bai Y, Lv ZB, Xu YL, Xie RM, Chen BD
Infection and Drug Resistance 2022, 15:6029-6037
Published Date: 18 October 2022
Correlations Between Inflammatory Cell Infiltration and Relative Density and the Boundary Manifestation of Pulmonary Non-Neoplastic Ground Glass Nodules
Liu XL, Lv FJ, Fu BJ, Lin RY, Li WJ, Chu ZG
Journal of Inflammation Research 2023, 16:1147-1155
Published Date: 15 March 2023
Bridging the Gap Between Imaging and Molecular Characterization: Current Understanding of Radiomics and Radiogenomics in Hepatocellular Carcinoma
Ren L, Chen DB, Yan X, She S, Yang Y, Zhang X, Liao W, Chen H
Journal of Hepatocellular Carcinoma 2024, 11:2359-2372
Published Date: 27 November 2024