Back to Journals » Journal of Pain Research » Volume 16
Prediction of the Cervical Epidural Space Depth from the Skin Using Cervical X-Ray, During Cervical Epidural Block with Paramedian Approach
Authors Choi DY, Lee SE ![]() , Lee MW, Lee KH, Kang E, Kwon JY, Lee HS, Kim DC
, Lee MW, Lee KH, Kang E, Kwon JY, Lee HS, Kim DC
Received 5 April 2023
Accepted for publication 9 June 2023
Published 17 June 2023 Volume 2023:16 Pages 2079—2090
DOI https://doi.org/10.2147/JPR.S409347
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Ellen Soffin
Dae Yun Choi, Sang Eun Lee, Min Woo Lee, Ki Hwa Lee, Eunsu Kang, Ji Yeon Kwon, Hyun-Seong Lee, Dong-chun Kim
Department of Anesthesiology and Pain Medicine, Inje University Haeundae Paik Hospital, Busan, South Korea
Correspondence: Sang Eun Lee, Email [email protected]
Objective: The purpose of this study is to compare the actual needle depth measured during cervical epidural block (CEB) with the predicted needle depth measured through a cervical flexion x-ray image at the paramedian approach.
Methods: The study was conducted based on the medical records of patients who underwent CEB at the pain clinic of Haeundae Paik Hospital. The actual needle distance (AD) was recorded after each successful CEB. The distance from the spinolaminar line to the skin, predicted median depth (PMD), was measured using lateral x-ray images. The medial to lateral distance (MLD), which is the distance from the midline of the spine to the needle insertion point, was measured using anteroposterior (AP) x-rays. The predicted paramedian depth (PPD) was calculated using the Pythagorean formula. The PMD represents the expected depth of the median approach, while the PPD represents the expected depth of the paramedian approach. The PMD, PPD, and AD were compared with each other.
Results: Concordance correlation coefficient (CCC) and Bland-Altman analysis were obtained for PMD and PPD. The CCC value of PMD was measured as 0.829, and the CCC value of PPD was measured as 0.830. In the Bland-Altman analysis, PPD was measured at − 0.13 ± 8.37 mm, and PMD was measured at 1.29 ± 8.38 mm.
Conclusion: When performing CEB through the paramedian approach, the depth can be predicted using a cervical flexion x-ray. At this time, the PMD can also be used to predict the depth during the paramedian approach.
Keywords: cervical epidural block, paramedian approach, median approach, prediction, cervical flexion x-ray
Introduction
The cervical epidural block (CEB) is performed for pain control in cervical disc disease, cervical stenosis, headache, facial pain, postherpetic neuralgia, and complex regional pain syndrome.1 CEB requires an experienced operator to gently access the epidural space to accurately identify the epidural space.2 CEB is more challenging than other epidural block for several reasons. The epidural space is widest at lumbar level, and narrowest at cervical level. The anatomy of the cervical vertebra has shortest inter-laminar distance. The angle of spinous process is more acute than at the lumbar level. The cervical spinal cord is the largest and closest to the brain.3–5 For these reasons, complications such as intrathecal drug injection, spinal cord puncture, epidural abscess, epidural hematoma, and arachnoiditis can occur more frequently with CEBs.6–9
Most anesthesiologists adopt the loss of resistance (LOR) technique.10 Using this technique, the sensation of penetrating the ligamentum flavum (LF) is an important marker of the needle tip location. However, anatomical variations, such as LF midline gaps and false LOR, make it more difficult to use this technique.11–14
In the past, blind CEB only relying on the LOR technique was commonly performed in clinical practice.2 However, in order to prevent complications and increase patient safety, fluoroscopic-guided CEB is now recommended.15–19 Since fluoroscopic-guided CEB can confirm the direction of the needle, both midline and paramedian approach are possible. Nevertheless, fluoroscopic-guided CEB is not perfect, as the shoulder bone can block the image at the C7/T1 level.20
Therefore, to overcome the limitations of the LOR technique and fluoroscopic-guided CEB, predicting the correct depth of the epidural space from the skin before the procedure can increase the success rate of the procedure and reduce the incidence of complications.
Most studies analyzing the depth from the skin to the cervical epidural space have been based on the midline approach, and studies based on the paramedian approach are hard to find. In this retrospective study, the actual needle distance (AD) was measured using a paramedian approach, and the predicted distance using cervical flexion x-ray images was comparatively analyzed.
Materials and Methods
All work was conducted according to a protocol approved by the Institutional Review Board of Inje University Haeundae Paik Hospital (IUHPH). This study was conducted retrospectively by searching our electronic medical records (EMR) for CEB procedures performed in our pain clinic between January 1, 2019 and July 30, 2022. Patient informed consent was not required as this study was conducted retrospectively using EMR data only, and patient identifiers such as individual names and patient numbers are not included in this study. We included all patients who underwent CEB at the C7-T1 level, had a final needle tip located at midline section, had an actual needle depth recorded, had cervical flexion anterior-posterior (AP) and lateral x-ray images, and had complete demographic data, including age, sex, weight, and height. Patients were excluded if they did not have a cervical x-ray image, had a poor-quality x-ray image, did not have an actual depth recorded, underwent CEB using a median approach, had a final needle tip outside of midline section, experienced CEB failure, or had the procedure performed below C7-T1 or above C7-T1. The success of each patient’s CEB was confirmed by both C-arm fluoroscopic imaging and symptom relief. This study aimed to place the final needle tip at the midline of the epidural space. To address the challenge of precise midline placement, we divided the vertebral body into five equal sections. Cases were included if the final needle tip fell within the midpoint section and excluded if it was outside of this range.
We reviewed 151 patients who had undergone 206 CEBs. Among the 206 CEBs, 20 had failed, 6 had no demographic data, 3 had CEBs not performed by the paramedian approach, 16 had a needle tip located outside of midline section, 59 had no cervical flexion x-ray image or had bad quality images, and 7 had CEBs performed above or below C7-T1 (Figure 1). A total of 95 CEB cases met the inclusion criteria.
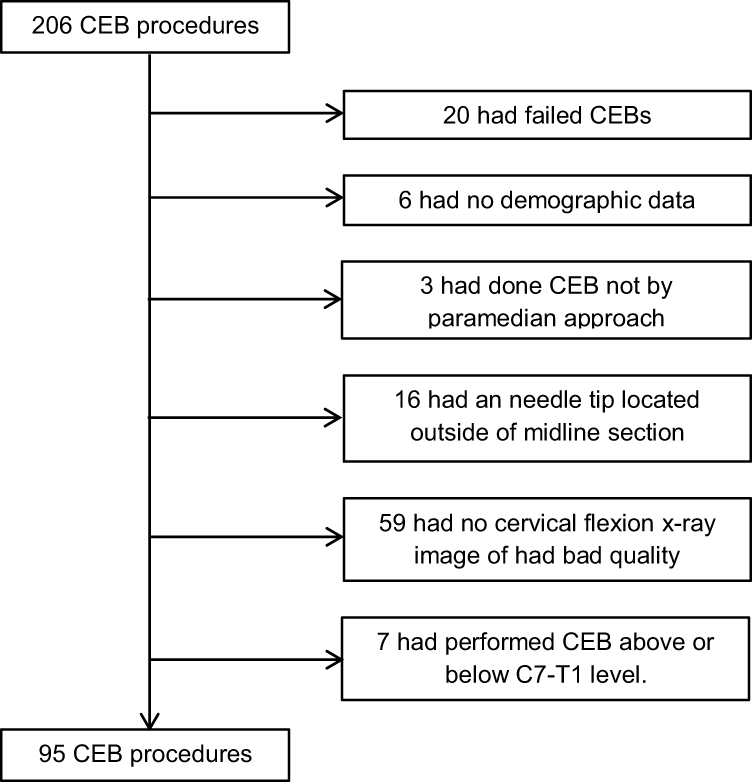 |
Figure 1 Patient selection flow diagram. Abbreviation: CEB, cervical epidural block. |
The C-arm guided cervical epidural block with a paramedian approach at C7/T1 was performed by a skilled pain expert as follows: First, a prone positioning system (Oakworks medical) was installed on the operating table, and then the patient was placed in a prone position (Figure 2). The neck and upper back were disinfected and prepared. The puncture site was confirmed as the T1 left lower angle point with the C-arm, and local anaesthesia was infiltrated with 3 mL of 0.2% ropivacaine. A 20G Tuohy needle was then inserted, and under C-arm guidance, the epidural space at the C7/T1 level was approached with a paramedian approach. After confirming the loss of resistance, 3–5 mL of Omnipaque was injected, and the spread of the contrast medium into the epidural space was confirmed by C-arm AP and lateral views (Figure 3).21,22 No vascular uptake was also checked. Then, 4mL of 0.1% ropivacaine + 5mg of dexamethasone were injected into the cervical epidural space. After the successful procedure, the needle was marked with an oil pen, pulled out of the skin, and the length of the needle was measured using a ruler and recorded in the EMR. The length of the needle measured by ruler is named actual distance (AD) (Figure 4).
 |
Figure 2 Prone positioning equipment (spine positioning system II, Oakworks Medical Co., USA). |
 |
Figure 3 Antero-posterior view (A) and oblique view (B) of C-arm fluoroscopic image of confirmation of needle tip. Note radiopaque area dispersing widely following epidural anatomy. |
 |
Figure 4 20G Tuohy needle (EH20080D, UNISIS Co., Japan) and ruler measurements (APL-SMP-001, All Pro Co., China). |
The distance from the skin to the epidural space at the paramedian approach is determined by measuring cervical flexion AP and lateral x-ray images. When performing a paramedian approach CEB, the needle insertion point is typically near the lower margin angle of the T1 vertebrae (see Figure 5). The distance from the midline to the lateral aspect of the vertebral body is measured using a picture archiving and communication system (PACS) on a cervical flexion AP x-ray image (see Figure 6A). This distance is referred to as the midline to lateral distance (MLD). The distance from the epidural space to the skin midline is measured using a cervical flexion lateral x-ray image on PACS. This distance is called the predicted midline depth (PMD). PMD is measured from the midpoint of the spinolaminar line of C7-T1 to a skin point where the line along the lower margin of the T1 vertebra meets (see Figure 6B). Measurements are taken to the nearest millimeter. PMD and MLD are nearly vertical to each other, so the Pythagorean formula can be used to calculate the predicted paramedian depth (PPD) (see Figure 7).
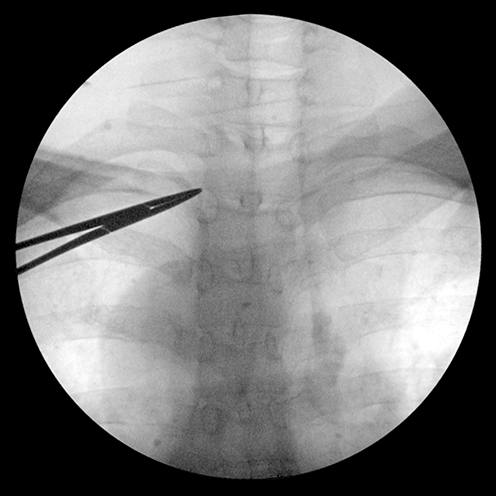 |
Figure 5 Needle insertion point is directed with tip of curved forcep at the lower left angle of T1 vertebrae. |
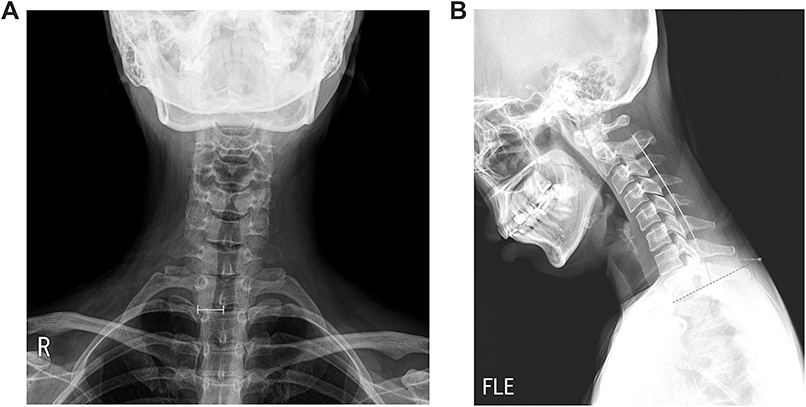 |
Figure 6 (A) AP image of cervical x-ray; MLD is measured from midline of cervical vertebra to lateral border of vertebral body. (B) Lateral image of cervical x-ray; dashed line represents line along the lower margin of T1 vertebra. Solid line is spinolaminar line. Dash-dotted line represents PMD. PMD is measured from skin where dashed line meets to spinolaminar line at middle of between C7 and T1 spinous process. Abbreviations: MLD, medial to lateral distance; PMD, predicted median depth. |
 |
Figure 7 A schematic drawing of the cervical epidural block. Abbreviations: PMD, predicted median depth; PPD, predicted paramedian depth; MLD, medial to lateral distance. |

Statistical Analysis
Lin’s concordance correlation coefficient analysis (CCC) and Bland-Altman analysis were used to analyze PMD and PPD. The analyses were performed using the epiR package in R version 4.2.1.
Results
A total of 95 cases of CEBs met the inclusion criteria. Demographic data are summarized in Table 1. A total of 54 cases were male, and 41 cases were female. The average age was 55.15±10.84 years, average height was 164.72±8.08 cm, average weight was 65.35±12.18 kg, and average BMI was 23.99±3.68 kg/m2. The actual depth (AD) average was 61.17±7.01 mm, range from 45.00 to 80.00 mm.
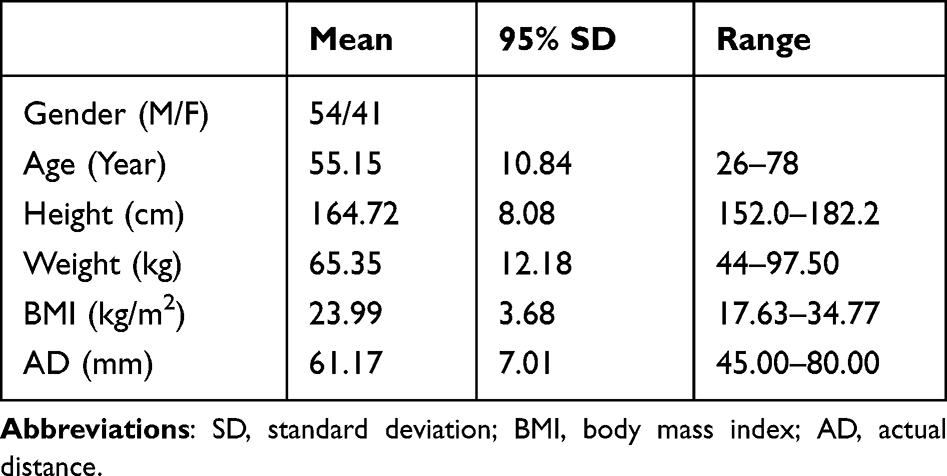 |
Table 1 Demographic Data of Patient |
CCC, precision, and accuracy values of PMD and PPD are described in Table 2. PMD’s CCC, precision, and accuracy values are 0.829, 0.834, and 0.993, respectively. PPD’s CCC, precision, and accuracy values are 0.830, 0.834, and 0.996, respectively.
 |
Table 2 Correlation Between Predicted Depth and Actual Depth |
Maximum difference of AD and PMD was 8.74 mm. Maximum difference of AD and PPD was 7.95 mm. At Bland-Altman precision analysis, PMD mean difference was measured 0.50 ± 8.38 mm and PPD mean difference was measured −0.13 ± 8.37 mm, respectively (Figure 8A and B).
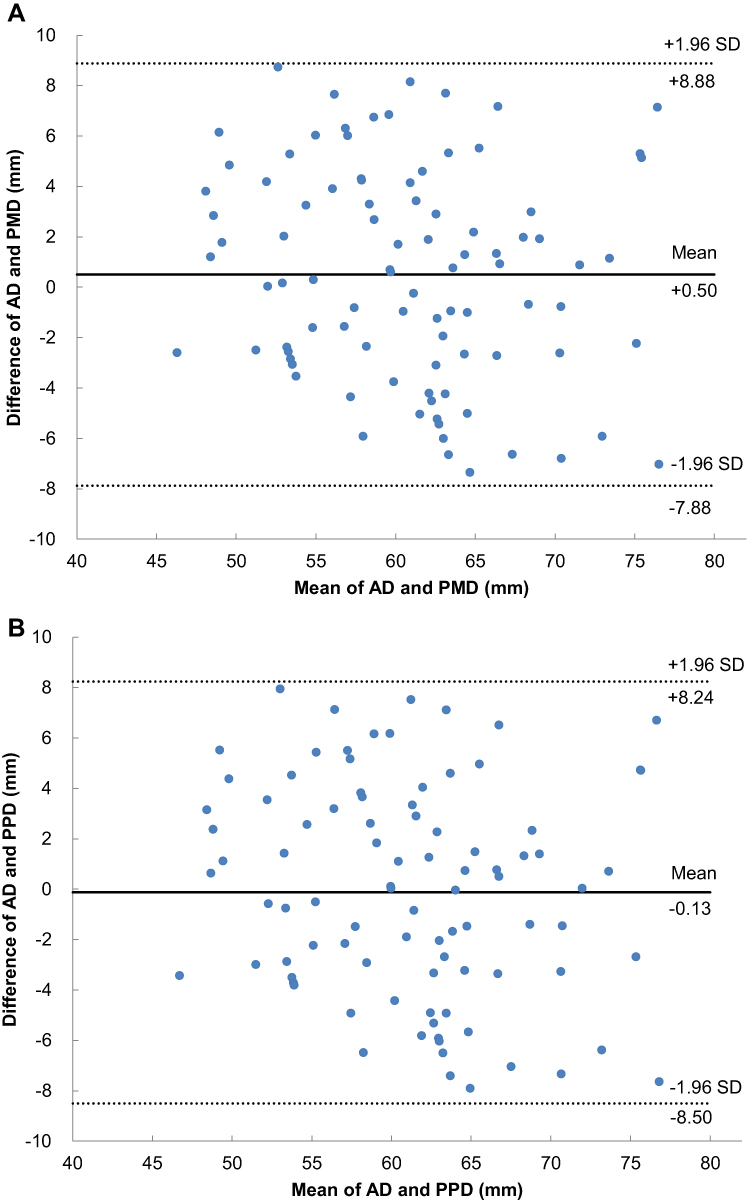 |
Figure 8 (A) Bland-Altman precision analysis of the measured differences between AD and PMD. (B) Bland-Altman precision analysis of the measured differences between AD and PPD. Abbreviations: PMD, predicted median depth; PPD, predicted paramedian depth; AD, actual distance. |
Discussion
Analysis of Result
Our study’s results showed that the CCC value of both PMD and PPD was similar and above 0.8. This indicates that we can use both PMD and PPD to predict AD.23,24 We had expected PPD to have better predictive power for AD, but there seems to be no significant difference between PMD and PPD. Even though PMD is based on a median approach and PPD is based on a paramedian approach, MLD did not have a significant enough effect to make a difference. The power of MLD affecting PMD can be calculated as follows.
PPD and PMD difference would be:

MLD had a mean value of 8.69 ± 1.04 mm, with a range from 5.56 to 11.14 mm (Table 2). Figure 9 shows how MLD can affect PMD values based on changes in MLD value. As shown in Figure 9, the power of MLD affecting PMD is not significant. Even with the largest MLD value of 11.14 mm and the lowest PMD value of 45.85 mm, MLD only affects PMD value by 1.33 mm. Moreover, since MLD tends to get bigger when PMD increases, the effect of MLD would be much smaller. In our study, the difference value between PPD and PMD was 0.63 ± 0.14 mm, ranging from 0.24 to 1.14 mm. As described in the Bland-Altman analysis, the difference value between PMD and AD was 0.50 ± 4.28 mm. Thus, MLD could not affect PMD significantly enough.
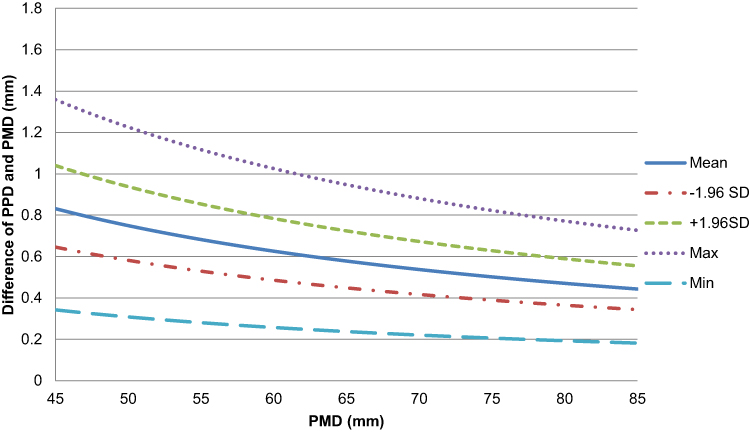 |
Figure 9 PPD and PMD difference change by PMD. Each line is drawn based on a different MLD. Dotted line is drawn based on maximum MLD value. Dashed line is drawn based on positive 95% standard deviation (SD) MLD value. Dash-dotted line is drawn based on negative 95% SD MLD value. Long-dashed line is drawn based on minimum MLD value. Abbreviations: PPD, predicted paramedian depth; PMD, predicted median depth; MLD, medial to lateral distance. |
Although the Bland-Altman analysis showed a slightly lower mean difference for PPD, this does not necessarily mean that one method is superior to the other. The Bland-Altman precision analysis of PPD and PMD showed mean differences of −0.13 ± 4.27 mm and 0.50 ± 4.28 mm, respectively. These results can provide insight into the prediction of AD.
As mentioned earlier, MLD only has a slight effect on PMD. Therefore, we could use PMD as a paramedian approach to predict AD.
Limitation of Blind Technique; False LOR and Midline Gap
The blind technique has limitations due to false LOR, which refers feeling LOR above LF, and Midline Gap, a discontinuity of the ligamentum flavum in the midline. False LOR occurs when the needle is felt in the supraspinous and interspinous ligaments instead of passing through the ligamentum flavum. This happens because the ligamentum flavum is mainly composed of elastic fibers, while the supraspinous and interspinous ligaments are collagen-based and can create spaces between the fibers.14,25 The occurrence rate of false LOR ranges from 30% to 70% according to studies.13,26,27 Midline gaps in the ligamentum flavum, particularly in the cervical and thoracic levels, make it challenging to rely solely on the LOR technique for identifying the epidural space.11,12 Predicting the depth of the epidural space before the procedure using imaging could reduce complications and improve success rates. However, many centers still do not use image information before and during procedures.10
Paramedian Approach vs Median Approach
According to current knowledge, there is no significant difference in clinical outcomes between the median approach and the paramedian approach.28 There are pros and cons to both the median and the paramedian approach. The epidural space has the characteristic of being widest in the center and narrowing laterally.3 With this characteristic, the space of the epidural space becomes narrower at the paramedian approach than when entering the center, making dura puncture more likely. During the midline approach, false LOR may occur more frequently due to the LF midline gap.11,12 According to the study done by Joo et al,29 abrupt pressure change was more common in the median approach compared to the paramedian approach (51.5% vs 17.6%). The choice of approach should be based on the specific clinical situation.
Comparing with Other Studies; Significance of Our Study
Various methods have been used to predict the depth from the skin to the epidural space, including demographic data and imaging modalities such as MRI, CT, Ultrasound, and x-rays.13,30–35 However, most studies focus on the median approach rather than the paramedian approach. Ultrasound has limitations due to LF discontinuity and difficulties in obese patients.36,37 MRI and CT imaging have limitations in terms of cost and differences in positioning compared to the actual procedure.38 Our study demonstrates that x-rays can easily predict paramedian depth, which is clinically available and economical. Previous studies have shown higher CCC values using ultrasonography and x-ray lateral images due to their prospective study designs.32,33 The study by Pak et al13 showed similar results to our study.
Study Limitations
Our retrospective study has some limitations, including a small sample size, variations in the needle entry point and angle, and differences in posture during the x-ray flexion image and block performance. In addition, measurement errors could have occurred due to the thickness of the marking pen, repeated LOR, and swelling of the skin caused by local anaesthesia. However, we minimized these errors by having the same person perform every CEB procedure using the same method. We also blinded the personnel who performed the depth prediction to the AD measurements to prevent measurement bias.
Additional Research
As an additional future research project, it would be possible to conduct a study comparing the significance of depth prediction in clinical outcome. The contralateral oblique (CLO) view during C-arm fluoroscopic-guided block has gained popularity recently, making it worth considering using this method for the study.39 Furthermore, conducting the study using a prospective design is also feasible.
Conclusion
In conclusion, when performing CEBs, it would be helpful for the practitioner to predict the depth of cervical epidural space to skin using cervical flexion x-ray image before the procedures. Both PMD and PPD can be used, and the depth predicted by the PMD can also be used for the paramedian approach.
Ethics and Consent
This study was conducted as a retrospective study and was exempt from obtaining individual patient consent as it was conducted without any patient identification and based on EMR data. This study has been approved by the Institutional Review Board of Inje University Haeundae Paik Hospital. This study is in compliance with the Declaration of Helsinki.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Baylot D, Mahul P, Navez ML, Hajjar J, Prades JM, Auboyer C. Anesthésie péridurale cervicale [Cervical epidural anesthesia]. Ann Fr Anesth Reanim. 1993;12(5):483–492. French. doi:10.1016/s0750-7658(05)80996-7
2. Benyamin RM, Singh V, Parr AT, Conn A, Diwan S, Abdi S. Systematic review of the effectiveness of cervical epidurals in the management of chronic neck pain. Pain Physician. 2009;12(1):137–157. doi:10.36076/ppj.2009/12/137
3. Hogan QH. Epidural anatomy examined by cryomicrotome section. Influence of age, vertebral level, and disease. Reg Anesth. 1996;21(5):395–406.
4. Hogan Quinn H. Lumbar epidural anatomy a new look by cryomicrotome section. Anesthesiology. 1991;75(5):767–775. doi:10.1097/00000542-199111000-00007
5. Mathis JM, Golovac S. Image-Guided Spine Interventions. Springer; 2011.
6. Waldman SD. Cervical epidural abscess after cervical epidural nerve block with steroids. Anesth Analg. 1991;72(5):717–718. doi:10.1213/00000539-199105000-00033
7. Williams KN, Jackowski A, Evans PJD. Epidural haematoma requiring surgical decompression following repeated cervical epidural steroid injections for chronic pain. Pain. 1990;42(2):197–199. doi:10.1016/0304-3959(90)91162-c
8. Abram SE, O’Connor TC. Complications associated with epidural steroid injections. Reg Anesth. 1996;21(2):149–162.
9. Hodges SD, Castleberg RL, Miller T, Ward R, Thornburg C. Cervical epidural steroid injection with intrinsic spinal cord damage. Two case reports. Spine. 1998;23(19):2137–2142; discussion 2141–2142. doi:10.1097/00007632-199810010-00020
10. Shanthanna H, Mendis N, Goel A. Cervical epidural analgesia in current anaesthesia practice: systematic review of its clinical utility and rationale, and technical considerations. Br J Anaesth. 2016;116(2):192–207. doi:10.1093/bja/aev453
11. Lirk P, Kolbitsch C, Putz G, et al. Cervical and high thoracic ligamentum flavum frequently fails to fuse in the midline. Anesthesiology. 2003;99(6):1387–1390. doi:10.1097/00000542-200312000-00023
12. Yoon SP, Kim HJ, Choi YS. Anatomic variations of cervical and high thoracic ligamentum flavum. Korean J Pain. 2014;27(4):321–325. doi:10.3344/kjp.2014.27.4.321
13. Pak MH, Lee WH, Ko YK, So SY, Kim HJ. Ultrasonographic measurement of the ligamentum flavum depth; is it a reliable method to distinguish true and false loss of resistance? Korean J Pain. 2012;25(2):99–104. doi:10.3344/kjp.2012.25.2.99
14. Lee JY, Lee SM, Sim WS, et al. False loss of resistance in cervical epidural injection: the loss of resistance technique compared with the epidrum guidance in locating epidural space. Pain Physician. 2016;19(3):131–138.
15. Paik NC. Radiation dose reduction in CT fluoroscopy-guided cervical transforaminal epidural steroid injection by modifying scout and planning steps. Cardiovasc Intervent Radiol. 2016;39(4):591–599. doi:10.1007/s00270-015-1230-0
16. Stojanovic MP, Vu T-N, Caneris O, Slezak J, Cohen SP, Sang CN. The role of fluoroscopy in cervical epidural steroid injections: an analysis of contrast dispersal patterns. Spine. 2002;27(5):509–514. doi:10.1097/00007632-200203010-00011
17. Kim KS, Shin SS, Kim TS, Jeong CY, Yoon MH, Choi JI. Fluoroscopically guided cervical interlaminar epidural injections using the midline approach: an analysis of epidurography contrast patterns. Anesth Analg. 2009;108(5):1658–1661. doi:10.1213/ane.0b013e31819d107b
18. Cluff R, Mehio AK, Cohen SP, Chang Y, Sang CN, Stojanovic MP. The technical aspects of epidural steroid injections: a national survey. Anesth Analg. 2002;95(2):403–408. doi:10.1097/00000539-200208000-00031
19. Manchikanti L, Malla Y, Cash KA, McManus CD, Pampati V. Fluoroscopic cervical interlaminar epidural injections in managing chronic pain of cervical postsurgery syndrome: preliminary results of a randomized, double-blind, active control trial. Pain Physician. 2012;15(1):13. doi:10.36076/ppj.2012/15/13
20. Shim E, Lee JW, Lee E, Ahn JM, Kang Y, Kang HS. Fluoroscopically Guided Epidural Injections of the Cervical and Lumbar Spine. RadioGraphics. 2017;37(2):537–561. doi:10.1148/rg.2017160043
21. Goel A, Pollan JJ. Contrast flow characteristics in the cervical epidural space: an analysis of cervical epidurograms. Spine. 2006;31(14):1576–1579. doi:10.1097/01.brs.0000222020.45794.ac
22. Lee SE, Joe HB, Park JH, et al. Distribution range of cervical interlaminar epidural injections: a comparative study with 2.5 mL, 5 mL, and 10 mL of contrast. Pain Physician. 2013;16(2):155.
23. Lin L, Torbeck LD. Coefficient of accuracy and concordance correlation coefficient: new statistics for methods comparison. PDA J Pharm Sci Technol. 1998;52(2):55–59.
24. Akoglu H. User’s guide to correlation coefficients. Turk J Emerg Med. 2018;18(3):91–93. doi:10.1016/j.tjem.2018.08.001
25. Johnson GM, Zhang M. Regional differences within the human supraspinous and interspinous ligaments: a sheet plastination study. Eur Spine J. 2002;11(4):382–388. doi:10.1007/s00586-001-0378-2
26. Jain A. Pseudo loss of resistance in epidural space localization: a complication of subcutaneous emphysema or simply a faulty technique. Saudi J Anaesth. 2011;5(1):108–109. doi:10.4103/1658-354x.76464
27. White AH. Injection techniques for the diagnosis and treatment of low back pain. Orthop Clin North Am. 1983;14(3):553–567. doi:10.1016/S0030-5898(20)31334-1
28. Yoon JY, Kwon JW, Yoon YC, Lee J. Cervical interlaminar epidural steroid injection for unilateral cervical radiculopathy: comparison of midline and paramedian approaches for efficacy. Korean J Radiol. 2015;16(3):604–612. doi:10.3348/kjr.2015.16.3.604
29. Joo Y, Moon JY, Kim YC, Lee SC, Kim HY, Park SY. A pressure comparison between midline and paramedian approaches to the cervical epidural space. Pain Physician. 2014;17(2):155–162.
30. Fujinaka MK, Lawson EF, Schulteis G, Wallace MS. Cervical epidural depth: correlation between needle angle, cervical anatomy, and body surface area. Pain Med. 2012;13(5):665–669. doi:10.1111/j.1526-4637.2012.01361.x
31. Algrain H, Liu A, Singh S, Vu TN, Cohen SP. Cervical epidural depth: correlation between cervical MRI measurements of the skin-to-cervical epidural space and the actual needle depth during interlaminar cervical epidural injections. Pain Med. 2018;19(5):1015–1022. doi:10.1093/pm/pnx066
32. Kim MG, Choi DH, Kim H, et al. Prediction of midline depth from skin to cervical epidural space by lateral cervical spine X-ray. Anesth Pain Med. 2017;12(1):68–71. doi:10.17085/apm.2017.12.1.68
33. Kim SH, Lee KH, Yoon KB, Park WY, Yoon DM. Sonographic estimation of needle depth for cervical epidural blocks. Anesth Analg. 2008;106(5):1542–1547. doi:10.1213/ane.0b013e318168b6a8
34. Zhao Q, Huang K, An J, et al. The distance from skin to cervical and high thoracic epidural space on Chinese adults as read from MRI. Pain Physician. 2014;17(2):163–168.
35. McCormick ZL, Mattie R, Ebrahimi A, et al. Is there a relationship between body mass index and fluoroscopy time during cervical interlaminar epidural steroid injections? Pain Med. 2017;18(7):1326–1333. doi:10.1093/pm/pnw264
36. Avramescu S, Arzola C, Tharmaratnam U, Chin KJ, Balki M. Sonoanatomy of the thoracic spine in adult volunteers. Reg Anesth Pain Med. 2012;37(3):349–353. doi:10.1097/AAP.0b013e3182464be2
37. Schroeder K, Andrei AC, Furlong MJ, Donnelly MJ, Han S, Becker AM. The perioperative effect of increased body mass index on peripheral nerve blockade: an analysis of 528 ultrasound guided interscalene blocks. Rev Bras Anestesiol. 2012;62(1):28–38. doi:10.1016/s0034-7094(12)70100-9
38. Young DW. What does an MRI scan cost? Healthc Financ Manage. 2015;69(11):46–49.
39. Gill JS, Aner M, Nagda JV, Keel JC, Simopoulos TT. Contralateral oblique view is superior to lateral view for interlaminar cervical and cervicothoracic epidural access. Pain Med. 2015;16(1):68–80. doi:10.1111/pme.12557
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.