Back to Journals » Cancer Management and Research » Volume 13
Predicting Survival for Patients with Malignant Pleural Effusion: Development of the CONCH Prognostic Model
Authors Zhang X, Yi FS ![]() , Shi HZ
, Shi HZ
Received 3 February 2021
Accepted for publication 12 April 2021
Published 14 June 2021 Volume 2021:13 Pages 4699—4707
DOI https://doi.org/10.2147/CMAR.S305223
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Chien-Feng Li
Xin Zhang *, Feng-Shuang Yi *, Huan-Zhong Shi
Department of Respiratory and Critical Care Medicine, Beijing Institute of Respiratory Medicine and Beijing Chao-Yang Hospital, Capital Medical University, Beijing, 100020, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Huan-Zhong Shi; Feng-Shuang Yi
Department of Respiratory and Critical Care Medicine, Beijing Institute of Respiratory Medicine and Beijing Chao-Yang Hospital, Capital Medical University, 8 Gongti Nanlu, Chao-Yang District, Beijing, 100020, People’s Republic of China
Tel/Fax +86 10 85231890
Email [email protected]; [email protected]
Background: Malignant pleural effusion (MPE) is a frequent complication of advanced malignancies that leads to a poor quality of life and limits treatment options.
Objective: The objective of this study was to identify biomarkers of survival in patients with MPE, which will greatly facilitate the clinical management of this complication.
Methods: This retrospective study recruited patients who had been pathologically diagnosed with MPE, regardless of the type of primary cancer, at Beijing Chao-Yang Hospital over 158 months. Demographic, clinical, hematological, and pleural fluid data were collected and analyzed as potential predictors of survival, and a new predictive model was developed based on Cox and logistic regression analyses.
Results: In our alternative prognostic model (n = 281), four routinely detected variables, namely, carcinoembryonic antigen (CEA) level, monocyte count, N-terminal pro B-type natriuretic peptide (NT-pro-BNP) level, and pleural effusion chloride level on admission, were identified as predictors (the CONCH prognostic score). Patients were divided into three prognosis subgroups based on risk stratification, with median survival periods of 17, 11, and 5 months, respectively. In comparison with the low-risk group, patients in the medium- and high-risk groups showed significantly poorer survival (medium-risk group: hazard ratio [HR], 1.586; 95% confidence interval [CI], 1.047– 2.402; P = 0.029; high-risk group: HR, 4.389; 95% CI, 2.432– 7.921; P < 0.001).
Conclusion: Four routinely detected variables were used to develop the CONCH scoring system, which was confirmed to be an accurate prognostic score for patients with MPE. This system can guide the selection of interventions and management for MPE.
Keywords: malignant pleural effusion, prognosis, CEA, monocyte, NT-pro-BNP
Introduction
Malignant pleural effusion (MPE) is a frequently occurring complication associated with poor patient outcomes, high mortality rates, and increased healthcare costs. The most common complaint in patients with MPE is dyspnea, which is prior to chest distress and cough.1 Metastatic disease is the leading cause of MPE, among which most commonly observed is lung cancer, followed by breast cancer. Mesothelioma, which accounts for the majority of primary pleural tumors leading to the formation of MPE,2 has attracted wide attention and is a challenging diagnosis. Cytological examination of pleural fluid and pleural biopsy are the two main diagnostic methods for mesotheliomas.3,4 More recently, immunohistochemistry (IHC) using soluble mesothelin-related peptide (SMRP) and the combination of MTAP and BAP1 have been confirmed to be useful for diagnosis.5,6 In addition, based on the multiple chromosomal imbalances in a series of malignant peritoneal mesothelioma cases, Serio et al hypothesized that the loss of function of ubiquitination, as well as of the defensins, could play an important role in the initial development and subsequent progression of mesothelioma.7
The treatment strategy for patients with MPE remains palliative, and mainly aims to relieve symptoms and improve patients’ quality of life. At present, pleurectomy is usually replaced by less invasive management procedures such as pleurodesis and indwelling pleural catheters, and trials for some novel technologies are underway.8–10 Determination of the most appropriate treatment is challenging when the precise survival of certain patients is unpredictable, since patients with longer life expectancy may adopt more positive treatment options.
Predictive indicators for many malignant diseases have been thoroughly studied over the past few decades. However, evaluation of the prognosis of patients with MPE remains challenging. Psallidas et al reported the pleurodesis response markers in MPE (PROMISE) for assessments of survival; however, these markers were largely associated with prior chemotherapy or radiotherapy and focused less on patients without any anticancer treatment.11 For newly diagnosed or recurrent MPE, the LENT prognostication score proposed by Clive et al was applied to predict patient survival based on tumor type, lactate dehydrogenase (LDH) level, Eastern Cooperative Oncology Group performance status (ECOG PS), and blood neutrophil-to-lymphocyte ratio (NLR).12 However, in comparison with patients showing MPE secondary to lung adenocarcinoma from a study in Singapore,13 the LENT score appears to predict a much shorter survival. To identify predictors suitable for patients with MPE in our center, we conducted the present study.
The present study was designed with the objective of taking as many clinical and biological variables as possible into consideration and to develop an alternative risk stratification tool to help guide clinical management decisions.
Materials and Methods
Patients and Data Collection
We carried out a retrospective study on patients pathologically diagnosed as malignant pleural effusion (MPE) at Beijing Chao-Yang Hospital during October 2005 to December 2018. Patients who had received anticancer therapy (surgery, chemotherapy, radiotherapy, targeted therapy) at the time of admission were excluded from this study.
We collected the clinical and laboratory data (Table 1) of all patients during the first hospital visit before they received any kind of anticancer therapy. Data for general indicators, including age, sex, smoking history, and Eastern Cooperative Oncology Group performance status were collected. Laboratory indexes, including leukocyte, neutrophil, lymphocyte, monocyte, eosinophil, and platelet (PLT) counts; mean platelet volume (MPV), NLR, lymphocyte-to-monocyte ratio (LMR), platelet-to-lymphocyte ratio (PLR), erythrocyte sedimentation rate (ESR); hemoglobin (HGB), C-reactive protein (CRP), albumin, LDH, alkaline phosphatase (ALP), serum Ca2+, fibrinogen, D-dimer, N-terminal pro B-type natriuretic peptide (NT-Pro-BNP), carcinoembryonic antigen (CEA), neuron-specific enolase (NSE), squamous cell carcinoma antigen (SCC), and cytokeratin 19 fragment (CYRFA) levels; and pleural effusion variables, including total cell, leukocyte, mononuclear cell, and multinuclear cell counts and chloride, glucose, LDH, adenosine deaminase (ADA), CEA, and albumin levels were recorded and presented as median (range).
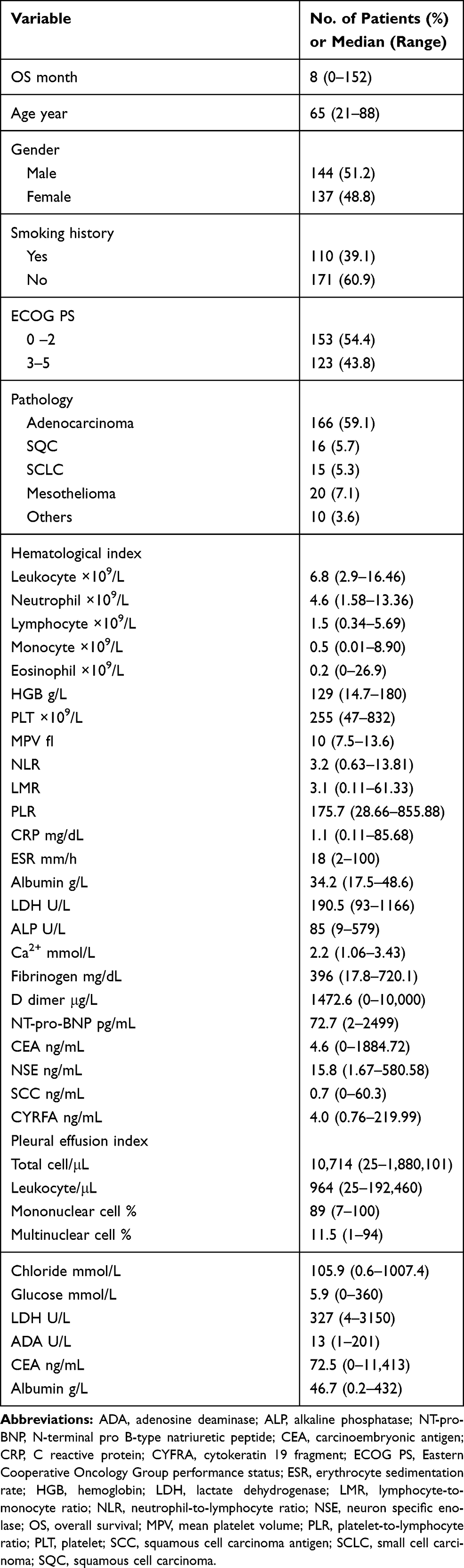 |
Table 1 Demographics and Baseline Patient Characteristics |
Overall survival (OS) was defined as the duration from diagnosis to death for any reason or the last date on which the patient was known to be alive. Clinical and laboratory data used in the survival analysis were recorded at the time of admission.
Statistical Analysis
SPSS software (version 20.0; Chicago, USA) was used for performing the analyses. We used proportions for categorical variables and medians with ranges for continuous variables. Descriptive statistical methods were used to describe the baseline characteristics.
Survival curves were estimated using the Kaplan–Meier survival function. To describe the association between a certain factor and an increased or decreased OS, we reported hazard ratios (HRs) from univariate and multivariate Cox logistic regressions with their respective 95% confidence intervals (95% CIs). Patients were stratified by various factors including age, sex, smoking history, ECOG PS, pathological findings, and laboratory data, and the median values of continuous variables served as cutoff values. Univariate survival analyses were applied to detect potential independent factors associated with prognosis, and variables with P values no more than 0.05 were further fitted into a multivariate Cox’s proportional hazard model. Differences with P values less than 0.05 were defined as statistically significant.
Results
Baseline Patient Characteristics
Between October 2005 and December 2018, 281 patients were diagnosed with malignant pleural effusion (MPE) by pleural biopsy or cytopathology before receiving any anticancer treatment. A total of hundred and ninety-five (69.4%) patients died during the follow-up period; 58 (20.6%) patients were alive until the end of our follow-up period; and 28 (10.0%) patients were lost to follow-up.
Baseline descriptive statistics are shown in Table 1. The mean follow-up period was 8 months (range, 0–152 months), and the mean age of the patients was 65 years (range, 21–88 years). The numbers of male and female patients with MPE in our study were similar (144 vs 137). One hundred and ten (39.1%) patients had been smoking, quitting or not. All patients were graded according to the ECOG PS; a slightly larger proportion of patients (153, 54.4%) scored 0–2 points. Metastasis of lung adenocarcinoma was the leading cause of MPE in our study (166, 59.1%), followed by squamous cell carcinoma (16, 5.7%), small cell carcinoma (15, 5.3%), mesothelioma (20, 7.1%), and other pathological types (10, 3.6%), including metastatic spindle cell carcinoma, lymphoma, colon cancer, breast cancer, Wilms tumor, neuroendocrine carcinoma, thyroid cancer, renal carcinoma, fibrosarcoma, and liver cancer. Available hematological indices, including leukocyte, neutrophil, lymphocyte, monocyte, eosinophil, and PLT counts; MPV, NLR, LMR, ESR, and PLR; HGB, CRP, albumin, LDH, ALP, serum Ca2+, fibrinogen, D dimer, NT-Pro-BNP, CEA, NSE, SCC, and CYRFA levels; as well as pleural effusion variables, including total cell, leukocyte, mononuclear cell, and multinuclear cell counts and chloride, glucose, LDH, ADA, CEA, and albumin levels are presented as median (range).
Survival Analysis
The median overall survival (OS) was 9 (95% CI 10.2–14.3) months, with 1-, 2-, and 3-year OS rates of 42.4%, 18.4%, and 7.4%, respectively. As shown in Table 2, univariate survival analyses (UVA) indicated that other pathological patterns rather than mesothelioma, ECOG PS > 2, CEA level > 4.6 ng/mL, NT-pro-BNP level > 72.7 pg/mL, chloride level in pleural effusion ≤ 105.9 mmol/L, leukocyte count > 6.8 × 109/L, neutrophil count > 4.6 × 109/L, monocyte count > 0.5 × 109/L, CRP level > 1.12 mg/dL, ESR > 18 mm/h, and LMR ≤ 3.1 may be significantly associated with a shorter OS (shown in Supplementary Figure 1, 2). No significant differences were found in age, sex, smoking history; lymphocyte, eosinophil, and PLT counts; MPV, NLR, LMR, PLR; HGB, albumin, LDH, ALP, Ca2+, fibrinogen, D dimer, NSE, SCC, and CYRFA levels; and pleural effusion-derived total cell, leukocyte, mononuclear cell, and multinuclear cell counts and glucose, LDH, ADA, CEA, and albumin levels. As shown in Table 3, variables with P values < 0.05, along with NSE level, the P value of which was 0.05, were further fitted into a multivariate Cox’s proportional hazard model, and CEA level (HR, 1.966; 95% CI 1.365–2.851; P < 0.001), monocyte count (HR, 1.534; 95% CI, 1.058–2.225; P = 0.024), NT-pro-BNP level (HR, 1.470; 95% CI, 1.021–2.116; P = 0.038), and pleural effusion chloride level (HR, 0.623; 95% CI, 0.433–0.895; P = 0.011) were identified as independent indicators of OS in patients with MPE.
 |
Table 2 Univariate Analysis of Variables in MPE Patients with Statistic Difference |
 |
Table 3 Prognostic Scoring Method and Multivariate Analysis of Prognostic Factors |
Development and Assessment of CONCH Prognostic Score Model
To precisely distinguish patients with different risk stratifications, CEA level, monocyte count, NT-pro-BNP level, and pleural effusion chloride level were employed to develop the CONCH prognostic score model. Patients would receive 1 point when they met any of the following conditions: CEA level > 4.6 ng/mL, monocyte count > 0.5 × 109/L, NT-pro-BNP level > 72.7 pg/mL, or pleural effusion chloride level ≤ 105.9 mmol/L. On the basis of this prognostic score, the patients were divided into low-risk (score 0–1), medium-risk (score 2–3), and high-risk (score 4) subgroups, with median survival periods of 17, 11, and 5 months, respectively (Table 4). The survival curves of the subgroups are shown in Figure 1. In comparison with the low-risk group, the medium-and high-risk groups showed significantly poorer survival (medium-risk group: HR, 1.586; 95% CI, 1.047–2.402, P = 0.029; high-risk group: HR, 4.389; 95% CI, 2.432–7.921, P < 0.001).
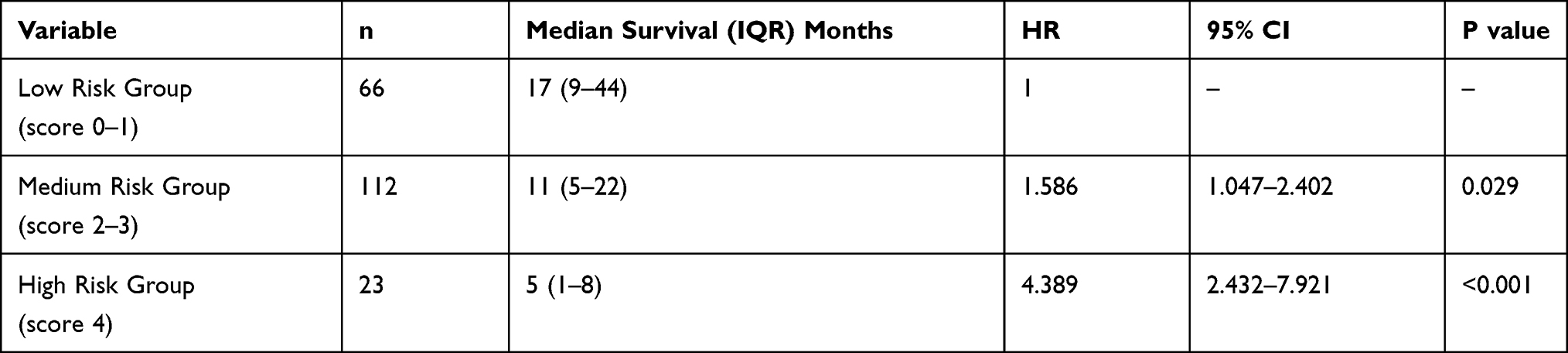 |
Table 4 Median Survival of Patients According to the CONCH Prognostic Score |
 |
Figure 1 Survival curves estimated by the Kaplan–Meier survival function for the 3 groups stratified by the CONCH score system. |
The Prognostic Model for Only Metastatic Cases
When focusing on metastatic MPE, we excluded 20 cases diagnosed with mesothelioma and performed UVA in 261 cases. Ten indicators (ECOG PS; NSE, CRP, CEA, and NT-pro-BNP levels; ESR and LMR; and monocyte and neutrophil counts and chloride level in pleural effusion) were then fitted into multivariate Cox’s proportional hazard model, showing that CEA level > 4.5 ng/mL, monocyte count > 0.5 × 109/L, and pleural effusion Cl− level ≤ 105.9 mmol/L were significantly associated with a shorter OS (Supplementary Table 1). On the basis of these three indicators, patients were divided into two prognosis subgroups: low-risk group (score 0–1) and high-risk group (score 2–3), with median survival periods of 19 and 9 months, respectively (Supplementary Table 2). The survival curves are shown in Supplementary Figure 3. In comparison with the low-risk group, the high-risk group showed significantly poorer survival (HR, 1.791; 95% CI, 5.563–12.437; P = 0.001).
Discussion
In our study, lung cancer accounted for the majority (70.1%) of the primary diseases causing MPE, and mesothelioma (20%) was the only primary tumor of the pleura, the distribution of which is consistent with previous studies. The median survival of patients with mesothelioma is 13 months, and the corresponding value for patients with lung cancer is 10 months. The LENT score study showed a median survival of 3 months in patients with lung cancer.12 Similar to our results, John Abisheganaden et al in Singapore13 reported a median survival period of 8 months in MPE patients secondary to lung adenocarcinoma, which prompted us to wonder whether race has an underlying influence on the differences. Pleural fluid LDH level, ECOG PS, NLR, and tumor type were the four factors employed in the LENT prognostic score system,12 none of which showed statistical significance in our multivariate survival analysis. These differences imply that outcomes vary with the diversity of the study population, and differences in races may play a role.
The CONCH score model we developed involves four key factors, among which CEA, a routinely tested indicator for detecting lung cancer, seems to be the least surprising. The term CEA is used to refer to a group of glycoprotein antigens associated with cell adhesion, which have been generally considered to be prognostic indicators of colorectal cancer and a sensitive index for its recurrence.14–17 Several studies have identified the role of CEA in the prevention, screening, treatment, and surveillance of breast cancer.18,19 Additionally, serum CEA level has also been shown to be associated with the prognosis in patients with intrahepatic cholangiocarcinoma after partial hepatectomy,20 and in postoperative patients with medullary thyroid cancer.21
As for respiratory tumors, several studies have shown that in addition to carbohydrate antigen 125 (CA125) and cytokeratin-19 fragment (CYFRA21-1), CEA can facilitate the diagnosis and surveillance of lung cancer.22–24 In the present study, we identified CEA as an independent indicator of prognosis for patients with MPE, and an elevated level of serum CEA on admission indicated a shorter survival.
The monocyte count in peripheral blood was determined to be a predictor for patients with MPE, according to our data. As an immature member of the reticuloendothelial system, monocytes are capable of developing into macrophages or histiocytes and then participating in the multiple functions of this system, especially in phagocytosis.25 Although none of our patients met the diagnostic criteria for infectious mononucleosis, an enhanced monocyte count may occur in a variety of conditions, most notably infectious diseases and several hematologic disorders. In addition, monocyte proliferation related to obesity,26 chronic stress,27 acute alcoholic liver disease,28 pre-eclampsia,29 idiopathic pulmonary fibrosis30 and hyperlipidemia31 has drawn attention. The monocyte count also tends to increase in patients with various cardiovascular diseases, most frequently left ventricular (LV) dysfunction and LV aneurysm.32,33
In addition to the benign conditions mentioned above, solid tumor malignancies were associated with a significant elevation in the monocyte count in comparison with the count in normal individuals.34 Several lines of studies have revealed that a low monocyte count may be associated with favorable outcomes in patients with some types of malignancy.35,36 In accordance with previous studies, we found that MPE patients with high monocyte levels had poor survival rates. Instead of initially suppressing the immune system, monocytes or macrophages assist in cancer progression by being educated by the tumor microenvironment,37,38 which may be part of the underlying mechanisms. In addition, a recent study showed that glycolysis levels in the peritumoral area of hepatocellular carcinoma can be significantly enhanced by monocytes, which induces PD-L1 expression and weakens cytotoxic T lymphocyte responses.39 These studies identified the pro-tumour effects of monocytes in the tumor microenvironment.
NT-pro-BNP, along with BNP secreted in equal molar, is known to be secreted in relation to cardiac stretch40 and left ventricular hypertrophy, which have been generally considered to be vital biomarkers guiding the management of patients with cardiovascular disease.41,42 Increased NT-pro-BNP levels are associated with cardiovascular disease (including heart failure, chronic coronary disease, and acute coronary syndromes)43–45 or renal disease due to decreased clearance.46,47 Furthermore, some studies have confirmed that plasma NT-pro-BNP is an independent indicator of the prognosis of patients with chronic renal disease,48 cardiovascular diseases,41 and multiple myeloma.49
In general, cardiac dysfunction in patients with cancer may result from anticancer-treatment-induced myocardial destruction, and NT-pro-BNP can serve as an indicator of prognosis, which has been well studied.48,50 However, the laboratory examination results used in our research were recorded at the time of admission before any anticancer treatment, thereby excluding therapy-related cardiac dysfunction. As for complications associated with plasma NT-pro-BNP levels, 2 (0.7%) patients in our study met the diagnostic criteria of heart failure, 40 (14.2%) patients had hypertension, 7 (2.5%) patients had coronary atherosclerotic heart disease, and 1 (0.4%) patient had renal failure.
Nevertheless, the underlying reasons for the elevated NT-proBNP levels in patients without cardiovascular or renal diseases are unclear. Pavo et al indicated that NT-pro-BNP levels could be elevated in cancer patients ahead of any cardiotoxic therapy and increased with advancing tumor stage, and this elevation is closely related to all-cause mortality.51 This was especially the case in our study since MPE occurs in the late stages of almost all types of malignancies. A recent study showed that early cardiac remodeling nurtures tumor growth and metastasis, and therefore promotes cancer progression.52 These theories imply the interaction between malignant diseases and cardiovascular injury, that is, cancermay contribute to the increased values of NT-pro-BNP, neverthless, early myocardial injury may nurture the genesis and progression of cancer.
We show that NT-pro-BNP is a strong prognostic indicator of MPE, and patients with a serum NT-pro-BNP level > 72.7 pg/mL tend to have a shorter survival, suggesting that subclinical myocardial injury may be associated with the prognosis of patients with MPE. Interestingly, when cases with mesothelioma were excluded, the prognostic significance of NT-proBNP appeared to reduce. Although very limited research has focused on the relationship between NT-pro-BNP and mesothelioma, Tsolaki et al’s work indicates that BNP can be secreted by mesothelial cells.53 However, there is no evidence suggesting that NT-pro-BNP is associated with cancer metastasis, and further study is needed on this subject.
Chloride tends to receive less attention, and depressed chloride levels in the cerebrospinal fluid (CSF) have long been considered to occur in patients with central nervous system infections, especially tubercular meningitis, but it is not a sensitive prognostic index.54,55 On the other hand, Dr. Lincoln’s work shows that the chloride level is simply a reflection of nutrient consumption or secondary to prolonged vomiting, and is of limited assistance in evaluating the course of tuberculous meningitis.55,56
Although very few studies have assessed the levels of chloride in body fluids, we identified chloride levels in pleural effusion as an independent indicator of prognosis for patients with MPE. A decreased chloride level in pleural effusion indicates a shorter survival, which may be related to total-body chloride depletion resulting from poor nutrition. Other relevant mechanisms should be investigated further.
We include 281 patients in our study, which is very large population in this subject. The CONCH score model based on four indicators shows great practical value in the prognosis of patients with MPE. This model highlights the stratified survival prospects in different patients and identifies routinely tested markers as key predictors. Although more studies are needed to further confirm its effectiveness, this convenient and clinically relevant score may help guide the selection of appropriate treatment options for patients with MPE.
Abbreviations
ADA, adenosine deaminase; ALP, alkaline phosphatase; CEA, carcinoembryonic antigen; CI, confidence interval; CRP, C reactive protein; CYFRA, Cytokeratin 19 fragment; ECOG PS, Eastern Cooperative Oncology Group performance status; ESR, erythrocyte sedimentation rate; HGB, hemoglobin; HR, hazard ratio; LDH, lactate dehydrogenase; LMR, lymphocyte-to-monocyte ratio; MPE, malignant pleural effusion; MPV, mean platelet volume; MVA, multivariate analysis; NLR, neutrophil-to-lymphocyte ratio; NSE, neuron specific enolase; NT-pro-BNP, N-terminal pro B-type natriuretic peptide; OS, overall survival; PLR, platelet-to-lymphocyte ratio; PLT, platelet; SCC, squamous cell carcinoma antigen; SCLC, small cell carcinoma; SQC, squamous cell carcinoma; UVA, Univariate analysis.
Statement of Ethics
The study was approved by the Institutional Review Board of Beijing Chao-Yang Hospital. Patients’ consent was not required because this is a retrospective study. We declare keep patients’ data confidential and comply with the Declaration of Helsinki.
Author Contributions
Huan-Zhong Shi and Feng-Shuang Yi conceived the idea, supervised the study; Xin Zhang and Feng-Shuang Yi collected data. All authors contributed to data analysis, drafting or revising the article, have agreed on the journal to which the article will be submitted, gave final approval of the version to be published, and agree to be accountable for all aspects of the work.
Funding
This work was supported by grants from Beijing Municipal Administration of Hospitals’ Mission Plan (SML20150301), and 1351 Talents Program of Beijing Chao-Yang Hospital (WXZXZ-2017-01).
Disclosure
The authors have no financial or other conflicts of interest.
References
1. Martínez-Moragón E, Sanchis J, Menéndez R, Cruz Rogado M, Sanchis F. Malignant pleural effusion: prognostic factors for survival and response to chemical pleurodesis in a series of 120 cases. Respiration. 1998;65(2):108–113. doi:10.1159/000029240
2. Roberts ME, Neville E, Berrisford RG, Antunes G, Ali NJ; Group BTSPDG. Management of a malignant pleural effusion: British thoracic society pleural disease guideline 2010. Thorax. 2010;65(Suppl 2):ii32–40. doi:10.1136/thx.2010.136994
3. Peto J, Decarli A, La Vecchia C, Levi F, Negri E. The European mesothelioma epidemic. Br J Cancer. 1999;79(3–4):666–672. doi:10.1038/sj.bjc.6690105
4. Renshaw AA, Dean BR, Antman KH, Sugarbaker DJ, Cibas ES. The role of cytologic evaluation of pleural fluid in the diagnosis of malignant mesothelioma. Chest. 1997;111(1):106–109. doi:10.1378/chest.111.1.106
5. Dipalma N, Luisi V, Di Serio F, et al. Biomarkers in malignant mesothelioma: diagnostic and prognostic role of soluble mesothelin-related peptide. Int J Biol Markers. 2011;26(3):160–165. doi:10.5301/JBM.2011.8614
6. Kinoshita Y, Hida T, Hamasaki M, et al. A combination of MTAP and BAP1 immunohistochemistry in pleural effusion cytology for the diagnosis of mesothelioma. Cancer Cytopathol. 2018;126(1):54–63. doi:10.1002/cncy.21928
7. Serio G, Vimercati L, Pennella A, et al. Genomic changes of chromosomes 8p23.1 and 1q21: novel mutations in malignant mesothelioma. Lung Cancer. 2018;126:106–111. doi:10.1016/j.lungcan.2018.10.012
8. Psallidas I, Kalomenidis I, Porcel JM, Robinson BW, Stathopoulos GT. Malignant pleural effusion: from bench to bedside. Eur Respir Rev. 2016;25(140):189–198. doi:10.1183/16000617.0019-2016
9. Antony VBLR, Astoul P, Boutin C, et al. Management of malignant pleural effusions. Eur Respir J. 2001;18(2):402–419. doi:10.1183/09031936.01.00225601
10. Davies HE, Mishra EK, Kahan BC, et al. Effect of an indwelling pleural catheter vs chest tube and talc pleurodesis for relieving dyspnea in patients with malignant pleural effusion: the TIME2 randomized controlled trial. JAMA. 2012;307(22):2383–2389. doi:10.1001/jama.2012.5535
11. Psallidas I, Kanellakis NI, Gerry S, et al. Development and validation of response markers to predict survival and pleurodesis success in patients with malignant pleural effusion (PROMISE): a multicohort analysis. Lancet Oncol. 2018;19(7):930–939. doi:10.1016/S1470-2045(18)30294-8
12. Clive AO, Kahan BC, Hooper CE, et al. Predicting survival in malignant pleural effusion: development and validation of the LENT prognostic score. Thorax. 2014;69(12):1098–1104. doi:10.1136/thoraxjnl-2014-205285
13. Abisheganaden J, Verma A, Dagaonkar RS, Light RW. An observational study evaluating the performance of LENT score in the selected population of malignant pleural effusion from lung adenocarcinoma in Singapore. Respiration. 2018;96(4):308–313. doi:10.1159/000489315
14. Benson AB, Venook AP, Al-Hawary MM, et al. NCCN guidelines insights: colon cancer, version 2.2018. J Natl Compr Canc Netw. 2018;16(4):359–369. doi:10.6004/jnccn.2018.0021
15. Konishi T, Shimada Y, Hsu M, et al. Association of preoperative and postoperative serum carcinoembryonic antigen and colon cancer outcome. JAMA Oncol. 2018;4(3):309–315. doi:10.1001/jamaoncol.2017.4420
16. Rose JAK, Kong CY, Meropol NJ, et al. A simulation model of colorectal cancer surveillance and recurrence. BMC Med Inform Decis Mak. 2014;14.
17. Thirunavukarasu P, Talati C, Munjal S, Attwood K, Edge SB, Francescutti V. Effect of incorporation of pretreatment serum carcinoembryonic antigen levels into AJCC staging for colon cancer on 5-year survival. JAMA Surg. 2015;150:747–755. doi:10.1001/jamasurg.2015.0871
18. Bast RCRP, Hayes DF, Bates S, et al.; American Society of Clinical Oncology Tumor Markers Expert Panel. 2000 update of recommendations for the use of tumor markers in breast and colorectal cancer: clinical practice guidelines of the American society of clinical oncology. J Clin Oncol. 2001;19(6):1865–1878. doi:10.1200/JCO.2001.19.6.1865
19. Harris L, Fritsche H, Mennel R, et al.; American Society of Clinical O. American society of clinical oncology 2007 update of recommendations for the use of tumor markers in breast cancer. J Clin Oncol. 2007;25(33):5287–5312. doi:10.1200/JCO.2007.14.2364
20. Wang Y, Li J, Xia Y, et al. Prognostic nomogram for intrahepatic cholangiocarcinoma after partial hepatectomy. J Clin Oncol. 2013;31(9):1188–1195. doi:10.1200/JCO.2012.41.5984
21. Elisei R, Pinchera A. Advances in the follow-up of differentiated or medullary thyroid cancer. Nat Rev Endocrinol. 2012;8(8):466–475. doi:10.1038/nrendo.2012.38
22. Bigbee WL, Gopalakrishnan V, Weissfeld JL, et al. A multiplexed serum biomarker immunoassay panel discriminates clinical lung cancer patients from high-risk individuals found to be cancer-free by CT screening. J Thorac Oncol. 2012;7(4):698–708. doi:10.1097/JTO.0b013e31824ab6b0
23. Guida F, Sun N, Bantis LE;Integrative Analysis of Lung Cancer E, Risk Consortium for Early Detection of Lung C. et al. Assessment of lung cancer risk on the basis of a biomarker panel of circulating proteins. JAMA Oncol. 2018;4(10):e182078. doi:10.1001/jamaoncol.2018.2078.
24. Patz EF
25. Bennett WE, Cohn ZA. The isolation and selected properties of blood monocytes. J Exp Med. 1966;123(1):145–160. doi:10.1084/jem.123.1.145
26. Nagareddy PR, Kraakman M, Masters SL, et al. Adipose tissue macrophages promote myelopoiesis and monocytosis in obesity. Cell Metab. 2014;19(5):821–835. doi:10.1016/j.cmet.2014.03.029
27. Heidt T, Sager HB, Courties G, et al. Chronic variable stress activates hematopoietic stem cells. Nat Med. 2014;20(7):754–758. doi:10.1038/nm.3589
28. McKeever UMOMC, Lawlor E, Kinsella A, Weir DG, Feighery CF. Monocytosis: a feature of alcoholic liver disease. Lancet. 1983;2.
29. Tang M-X, Zhang Y-H, Hu L, Kwak-Kim J, Liao A-H. CD14++ CD16+HLA-DR+Monocytes in peripheral blood are quantitatively correlated with the severity of pre-eclampsia. Am J Reprod Immunol. 2015;74(2):116–122. doi:10.1111/aji.12389
30. Misharin AV, Morales-Nebreda L, Reyfman PA, et al. Monocyte-derived alveolar macrophages drive lung fibrosis and persist in the lung over the life span. J Exp Med. 2017;214(8):2387–2404. doi:10.1084/jem.20162152
31. Li X, Zhu M, Penfold ME, et al. Activation of CXCR7 limits atherosclerosis and improves hyperlipidemia by increasing cholesterol uptake in adipose tissue. Circulation. 2014;129(11):1244–1253. doi:10.1161/CIRCULATIONAHA.113.006840
32. Maekawa YAT, Yoshikawa T, Asakura Y, et al. Prognostic significance of peripheral monocytosis after reperfused acute myocardial infarction: apossible role for left ventricular remodeling. J Am Coll Cardiol. 2002;39(2):241–246. doi:10.1016/S0735-1097(01)01721-1
33. van der Valk FM, Kuijk C, Verweij SL, et al. Increased haematopoietic activity in patients with atherosclerosis. Eur Heart J. 2017;38(6):425–432. doi:10.1093/eurheartj/ehw246
34. Barrett O. Monocytosis in malignant disease. Ann Intern Med. 1970;73(6):991–992. doi:10.7326/0003-4819-73-6-991
35. Martens A, Wistuba-Hamprecht K, Foppen MG, et al. Baseline peripheral blood biomarkers associated with clinical outcome of advanced melanoma patients treated with ipilimumab. Clin Cancer Res. 2016;22(12):2908–2918. doi:10.1158/1078-0432.CCR-15-2412
36. Wayne R, Rackoff RG, Robinson C, Kreissman SG, Philip P. Breitfeld: predicting the risk of bacteremia in childen with fever and neutropenia. J Clin Oncol. 1996;14(3):919–924. doi:10.1200/JCO.1996.14.3.919
37. Noy R, Pollard Jeffrey W. Tumor-associated macrophages: from mechanisms to therapy. Immunity. 2014;41(1):49–61. doi:10.1016/j.immuni.2014.06.010
38. Ringelhan M, Pfister D, O’Connor T, Pikarsky E, Heikenwalder M. The immunology of hepatocellular carcinoma. Nat Immunol. 2018;19:222–232.
39. Chen D-P, Ning W-R, Jiang -Z-Z, et al. Glycolytic activation of peritumoral monocytes fosters immune privilege via the PFKFB3-PD-L1 axis in human hepatocellular carcinoma. J Hepatol. 2019;71(2):333–343. doi:10.1016/j.jhep.2019.04.007
40. Hall C. Essential biochemistry and physiology of (NT-pro)BNP. Eur J Heart Fail. 2004;6(3):257–260. doi:10.1016/j.ejheart.2003.12.015
41. Kragelund C, Grønning B, Køber L. N-terminal pro-B-type natriuretic peptide and long-term mortality in stable coronary heart disease. ACC Curr J Rev. 2005;14(6):22–23. doi:10.1016/j.accreview.2005.05.052
42. Linssen GC, Bakker SJ, Voors AA, et al. N-terminal pro-B-type natriuretic peptide is an independent predictor of cardiovascular morbidity and mortality in the general population. Eur Heart J. 2010;31:120–127.
43. McKie PM, Cataliotti A, Sangaralingham SJ, et al. Predictive utility of atrial, N-terminal pro-atrial, and N-terminal pro-B-type natriuretic peptides for mortality and cardiovascular events in the general community: a 9-year follow-up study. Mayo Clin Proc. 2011;86(12):1154–1160. doi:10.4065/mcp.2011.0437
44. de Lemos JAMD, Bentley JH, Omland T, et al. The prognostic value of B-type natriuretic peptide in patients with acute coronary syndromes. N Engl J Med. 2001;345(14):1014–1021. doi:10.1056/NEJMoa011053
45. Omland T, Persson A, Ng L, et al. N-terminal pro-B-type natriuretic peptide and long-term mortality in acute coronary syndromes. Circulation. 2002;106(23):2913–2918. doi:10.1161/01.CIR.0000041661.63285.AE
46. Neda Khalifeh DH, Ho¨rl: WH. Natriuretic peptides in chronic kidney disease and during renal replacement therapy: an Update. J Investig Med. 2009;57(1).
47. Vickery S, Webb MC, Price CP, John RI, Abbas NA, Lamb EJ. Prognostic value of cardiac biomarkers for death in a non-dialysis chronic kidney disease population. Nephrol Dial Transplant. 2008;23(11):3546–3553. doi:10.1093/ndt/gfn341
48. Papazisis KT, Kontovinis LF, Papandreou CN, et al. Brain natriuretic peptide precursor (NT-pro-BNP) levels predict for clinical benefit to sunitinib treatment in patients with metastatic renal cell carcinoma. BMC Cancer. 2010;10(1):489. doi:10.1186/1471-2407-10-489
49. Milani P, Vincent Rajkumar S, Merlini G, et al. N-terminal fragment of the type-B natriuretic peptide (NT-proBNP) contributes to a simple new frailty score in patients with newly diagnosed multiple myeloma. Am J Hematol. 2016;91(11):1129–1134. doi:10.1002/ajh.24532
50. Giuseppe Curigliano M, Daniela Cardinale MD, Susan Dent MD, et al. Cardiotoxicity of anticancer treatments: epidemiology, detection, and management. CA Cancer J Clin. 2016;66(4).
51. Pavo N, Raderer M, Hulsmann M, et al. Cardiovascular biomarkers in patients with cancer and their association with all-cause mortality. Heart. 2015;101(23):1874–1880. doi:10.1136/heartjnl-2015-307848
52. Shimrit Avraham -SA-S, Shofti R, Tali Haas BK, et al. Early cardiac remodeling promotes tumor growth and metastasis. Circulation. 2020.
53. Tsolaki V, Zarogiannis S, Zygoulis P, et al. Malignant mesothelioma cells secrete natriuretic peptides: data and diagnostic clinical implications. Respirology. 2020;25(10):1060–1065. doi:10.1111/resp.13788
54. Gierson HW, Marx JI. Tuberculous meningitis: the diagnostic and prognostic significance of spinal fluid sugar and chloride. Ann Intern Med. 1955;42(4):902–908. doi:10.7326/0003-4819-42-4-902
55. Schoen EJ. Spinal fluid chloride: a test 40 years past its time. JAMA. 1984;251(1).
56. Lincoln EM, Sifontes JE. Tuberculous meningitis in children. Med Clin North Am. 1953;37(2):345–362. doi:10.1016/S0025-7125(16)35018-0
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.