Back to Journals » Journal of Hepatocellular Carcinoma » Volume 10
Pre-S1 Mutations as Indicated by Serum Pre-S1 Antigen Negative is Associated with an Increased Risk of Hepatocellular Carcinoma in Chronic Hepatitis B Patients
Authors Zhang X, Gu C, Wei Q, Cao Y, She W, Shi H, Xie Y, Guo J ![]()
Received 2 February 2023
Accepted for publication 6 April 2023
Published 11 April 2023 Volume 2023:10 Pages 599—609
DOI https://doi.org/10.2147/JHC.S373333
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 5
Editor who approved publication: Professor Manal Hassan
Xingxin Zhang,1 Chenjian Gu,2 Qian Wei,1 Yirong Cao,1 Weimin She,1 Hong Shi,1 Youhua Xie,2 Jinsheng Guo1
1Department of Gastroenterology and Hepatology; Department of Internal Medicine, Shanghai Medical College, Zhongshan Hospital, Fudan University, Shanghai, 200032, People’s Republic of China; 2Key Laboratory of Medical Molecular Virology, Department of Microbiology and Parasitology, School of Basic Medical Sciences, Fudan University, Shanghai, People’s Republic of China
Correspondence: Jinsheng Guo, Department of Gastroenterology and Hepatology, Zhongshan Hospital, Fudan University, 180 Feng Lin Road, Shanghai, 200032, People’s Republic of China, Tel +86 21-64041990 ext. 2424, Fax +86 21 64038472, Email [email protected] Youhua Xie, Department of Microbiology and Parasitology, School of Basic Medical Sciences, Fudan University, 136 Yi Xue Yuan Road, Shanghai, 200032, People’s Republic of China, Tel +86 13651772272, Email [email protected]
Objective: Pre-S1 antigen (pre-S1) is a component of hepatitis B virus large surface antigen (L-HBsAg). This study aimed to investigate the association between clinical pre-S1 antigen (pre-S1) status and adverse prognostic events in chronic hepatitis B (CHB) patients.
Methods: This study retrospectively enrolled 840 CHB patients with comprehensive clinical data, including 144 patients with multiple follow-up of pre-S1 status. All patients were tested for serum pre-S1 and divided into pre-S1 positive and negative groups. Single factor and logistic multiple regression analyses were performed to explore the association between pre-S1 and other HBV biomarkers with the risk of hepatocellular carcinoma (HCC) in CHB patients. The pre-S1 region sequences of HBV DNA were obtained from one pre-S1 positive and two pre-S1 negative treatment-naïve patients using polymerase chain reaction (PCR) amplification followed by Sanger sequencing.
Results: The quantitative HBsAg level was significantly higher in the pre-S1 positive group than that in the pre-S1 negative group (Z=− 15.983, P< 0.001). The positive rate of pre-S1 increased significantly with the increase in HBsAg level (χ2=317.963, P< 0.001) and HBV DNA load (χ2=15.745, P< 0.001). The pre-S1 negative group had a higher HCC risk than the pre-S1 positive group (Z=− 2.00, P=0.045, OR=1.61). Moreover, patients in the sustained pre-S1 negative group had a higher HCC risk (Z=− 2.56, P=0.011, OR=7.12) than those in the sustained pre-S1 positive group. The sequencing results revealed mutations in the pre-S1 region from samples of pre-S1 negative patients, including frameshift and deletion mutations.
Conclusion: Pre-S1 is a biomarker that indicates the presence and replication of HBV. Pre-S1 sustained negativity attributed to pre-S1 mutations in CHB patients may be associated with a higher risk of HCC, which has clinical significance and warrant further investigations.
Keywords: chronic hepatitis B, pre-S1 antigen, hepatocellular carcinoma
Introduction
Chronic Hepatitis B virus (HBV) infection is a global health problem, with a prevalence of about 5% worldwide that varies significantly by region.1 In China, the prevalence of HBV infection is higher, with the domestic rate dropping from 9.75% in 1992 to 7.2% in 2006, mainly due to widespread vaccination.2,3 HBV is a hepatotropic DNA virus that can cause acute and chronic infections. The chronic infection can result in an asymptomatic carrier state, chronic hepatitis B (CHB), liver cirrhosis (LC), and hepatocellular carcinoma (HCC).4–6 Although most adults with acute HBV infection recover completely with only about 5% become chronic infection, newborns and infants (< 4 years old) have a high chance of developing chronic infection, which can be as high as 90%. LC and HCC are the main causes of death for HBV-related liver diseases, resulting in over 500,000 deaths annually.1,6 Thus, identifying risk factors for cirrhosis and HCC in CHB patients is crucial for effective health management.
Ten HBV genotypes (A-J) have been identified based on the inter-genotype genome difference of more than 8%. While all genotypes can cause liver disease, they also exhibit distinct pathogenic and therapeutic characteristics.7,8 In particular, according to the sequence, Genotypes B and C are more prevalent in the Asian region such as China and East Asia, and the infected patients show lower response rates to interferon therapy, as well as more rapid progression of liver fibrosis and liver cancer.9,10 Notably, HBV carriers of type C have a higher pre-S loss rate than those of type B.11,12
HBV, also known as Dane particle, consists of an envelope and nuclear capsid.13 The envelope contains hepatitis B surface antigen (HBsAg), glycoprotein, and lipid, while the nuclear capsid contains a viral genome composed of relaxed circular double-stranded DNA (rcDNA), viral DNA polymerase (Pol), and viral core antigen (HBcAg). HBsAg can be classified into large (L-), medium (M-), and small (S-) HBsAg based on their molecular weight. L-HBsAg is composed of pre-S1 (108 or 119 hydrophilic amino acid residues depending on genotype), pre-S2 (55 hydrophilic amino acid residues), and S protein (226 amino acid residues). M-HBsAg is made up of pre-S2 and S protein, while S-HBsAg only consists of S protein.12,13 The interaction between pre-S1 and pre-S1-specific receptors, such as asialoglycoprotein receptor (ASGPR), on the surface of human hepatocytes and hepatocellular carcinoma cells plays a key role for the entry of HBV particles into hepatocytes.14,15 The receptor binding sites of pre-S1 (amino acids 1–48) are highly conserved across multiple HBV genotypes.
Pre-S1 (pre-S1 antigen) has been used as a marker of hepatitis B since the 1980s. Currently, it has been widely used in clinical practice as an indicator of HBV replication, similar to HBeAg. It has clinical significance for the detection of early acute HBV infection, as well as for evaluating chronic HBV replication level, drug efficacy, and patient prognosis. Pre-S1 appears at the earliest stage of acute HBV infection and its seroconversion is also the earliest indicator of virus clearance.
Pre-S1 mutations, however, may alter HBV replication activity and secretion ability, potentially leading to decreased circulating HBsAg levels.16–18 The inhibition of the secretion of HBV particles due to pre-S deletion mutations (including pre-S1 and pre-S2 mutations) may result in the retention of viral particles in the endoplasmic reticulum, which consequently induces endoplasmic reticulum stress. Compared with wild-type HBV, pre-S variants may develop adaptive antigen properties to evade host immune surveillance and clearance, and enhance replication capabilities.19,20
Several studies have reported a higher pre-S1 mutation rate in CHB patients with liver cancer compared to those without liver cancer.11,21,22 Therefore, caution should be taken when interpreting the clinical significance of pre-S1, along with other HBV markers, for the prognosis of CHB patients. The aim of this study was to investigate the association between clinical pre-S1 status and adverse prognostic events in CHB patients.
Materials and Methods
Study Population
This clinical retrospective study was approved by the ethical committee of Zhongshan Hospital affiliated with Fudan University. The study protocol conformed to the provisions of the Declaration of Helsinki. Informed consent was obtained from all subjects. A total of 840 patients with chronic HBV infection who visited the hospital from January 2016 to January 2021 were enrolled. Chronic infection was defined as HBsAg positive, with or without HBV-DNA positivity. All patients were tested for pre-S1 and divided into pre-S1 positive and negative groups. Among them, 144 HBsAg positive patients were followed up with multiple detections of pre-S1 at intervals of at least 6 months, including 122, 13, and 9 patients tested for pre-S1 twice, thrice, and four times, respectively.
The exclusion criteria were: (1) acute hepatitis B virus infection; (2) co-infection with other hepatitis viruses, eg, hepatitis C, A, or E; (3) autoimmune liver diseases, including primary biliary cirrhosis and autoimmune hepatitis; (4) drug-induced liver injury; (5) schistosomiasis cirrhosis; (6) other diseases that may lead to liver cirrhosis or other serious liver diseases.
Data Collection
The clinical data were collected, including: (1) general information, such as age and gender; (2) biomarkers of HBV infection, including HBV pre-S1 antigen (pre-S1), HBV markers (HBsAg, HBsAb, HBeAg, HBeAb, HBcAb, HBcAb IgM), and HBV-DNA; (3) liver function tests, including alanine aminotransferase (ALT), aspartate aminotransferase (AST), alkaline phosphatase (ALP), gamma-glutamyltransferase (GGT), total bilirubin (TB), conjugated bilirubin (CB), and albumin (ALB); (4) blood lipids, including total cholesterol and serum triglyceride levels; (5) blood routine, including total hemoglobin (Hb) and platelet count (PLT); (6) coagulation function, including prothrombin time (PT) and activated partial thrombin time (APTT); (7) tumor markers, including alpha-fetoprotein (AFP), carcinoembryonic antigen (CEA), and carbohydrate antigen 19-9 (CA19-9); (8) imaging results, including ultrasound of the liver and biliary system, Fibroscan, abdominal computed tomography (CT), upper abdominal magnetic resonance imaging (MRI), and positron emission tomography-computed tomography (PET-CT), and liver biopsy results if available; and (9) Child-Pugh stage of cirrhosis.
Diagnosis of Liver Cirrhosis and Liver Cancer
The diagnosis of hepatitis B-related cirrhosis should conform to the (1) and (2) pathological diagnosis, or (1) and (3) clinical diagnosis, as follows: (1) current HBsAg positive, or HBsAg negative, anti-HBc positive, with a definite history of chronic HBV infection (past HBsAg positive for >6 months), except for other causes; (2) pathological results of liver biopsy consistent with liver cirrhosis; (3) at least 2 of the followings: imaging examination showing signs of cirrhosis and/or portal hypertension; endoscopic examination showing esophageal and gastric varices; liver hardness tested by Fibroscan was consistent with cirrhosis; decreased albumin level (<35g/L) and/or prolonged PT (compared with the control group) on blood biochemical examination; and platelet count <100×10^9/L in blood routine examination.
The diagnostic criteria for HBV-related hepatocellular carcinoma (HCC) are as follows: (1) with HBV-related liver cirrhosis, intrahepatic nodules with diameter ≤2cm, and presence of typical HCC characteristics shown in at least 2 of the following imaging examinations: dynamic enhanced MRI, dynamic enhanced CT, ultrasound imaging, and hepatocyte-specific Gd-EOB-DTPA enhancement MRI; (2) intrahepatic nodules with diameter >2cm, and at least one typical liver cancer characteristic found in the above 4 imaging examinations; (3) Focal liver biopsy and/or surgery showing a pathological diagnosis of HCC, including HBV-related liver cirrhosis, intrahepatic nodules with a diameter ≤2cm, without or with only one of the typical liver cancer characteristics found in the above four imaging examinations; or nodules with a diameter of >2 cm without typical features of liver cancer.
Detection of Pre-S1
Serum pre-S1 was detected using standardized procedures of enzyme-linked immunosorbent assay (ELISA) (Shanghai Alpha Biotechnology Co., LTD) with an ST-360 automatic quantitative ELISA detection system (Shanghai Kehua Experimental System Co., LTD).
Sequence Analysis and Detection of Pre-S1 Variations
Serum samples (5 mL each) were collected from two pre-S1 positive and two pre-S1 negative treatment-naive patients who were positive for HBV DNA was extracted using the DNeasy Blood & Tissue Kit (Qiagen, Hilden, Germany). The pre-S1 region was amplified by PCR using the following primers: pre-S1 forward: 5’-GTCACCATATTCTTGGGAACA-3’; and pre-S1 reverse: 5’-GTCCACCACGAGTCTAGACTC-3’. The PCR products were cloned using the pLB Lethal Based Fast Cloning Kit, and 10 positive clones were selected and sequenced by Sanger sequencing. The sequences were analyzed and compared with the control sequences of HBV type B (GenBank Accession No. KR152339), type C (GenBank Accession No. KY881972.1) and type D (GenBank Accession No. V01460.1).
Statistical Analysis
Statistical analysis was performed using t-test and Wilcoxon rank sum test to compare the average level of measurement data, and Chi-square test and Fisher exact test to compare the average level of count data. Single-factor and logistic multiple regression analyses were applied to explore the correlation between pre-S1 status and the risks of cirrhosis and HCC. P < 0.05 was considered statistically significant.
Results
Characteristics of the Study Population
The general characteristics of the 840 CHB patients are shown in Table 1. The pre-S1 negative and positive groups comprised 305 and 535 patients, respectively. Although there was a statistical difference in age (P<0.050), there was no difference in gender distribution between the two groups. The level of HBsAg in the pre-S1 negative group was significantly lower than that of the positive group (P<0.001). However, there was no statistical difference in HBV DNA positive rate between the two groups.
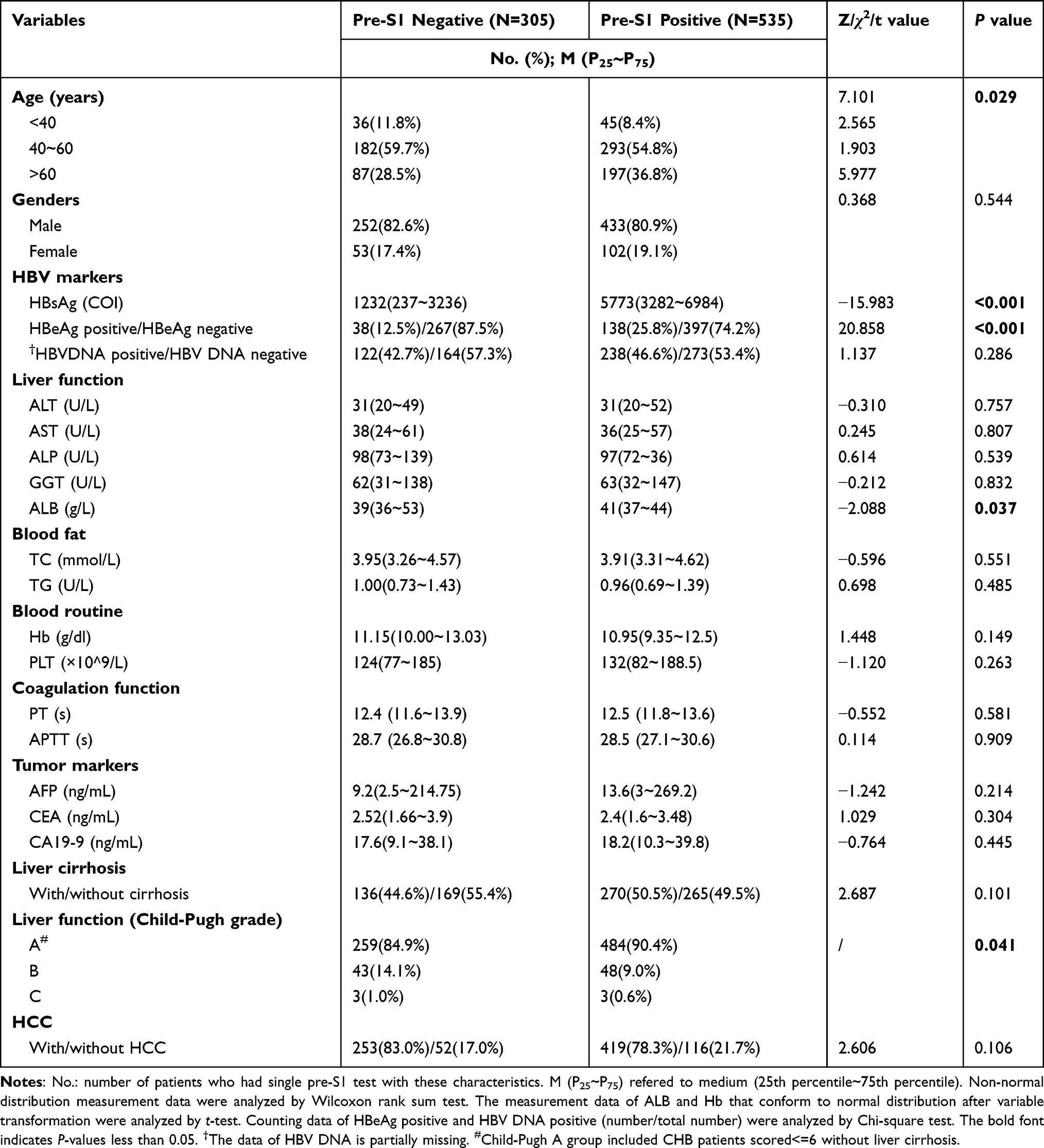 |
Table 1 Association of Pre-S1 Single Test Result with Clinical Parameters |
A statistical difference was found in the ALB level between the two groups, although the levels were within the normal range. However, no difference was observed in other parameters, such as liver function, blood lipids, blood routine, coagulation function, and tumor markers, between the two groups.
Pre-S1 Status is Associated with Other HBV Markers
As shown in Table 2, there was a significant difference in the positive rates of pre-S1 in patients with different HBsAg titers ranging from HBsAg <1000COI, 1000~2000COI, 2000~5000COI, to >5000COI. The positive rates of pre-S1 detected in patients with a single test showed an increasing trend with the increase in HBsAg titers. The positive rate of HBeAg in the pre-S1 positive group was also significantly higher than that in the pre-S1 negative group. The correlation analysis between HBV DNA content and the positive rate of pre-S1 in a single test also showed that the positive rate of pre-S1 increased significantly with the increases in HBV DNA loads (Table 2).
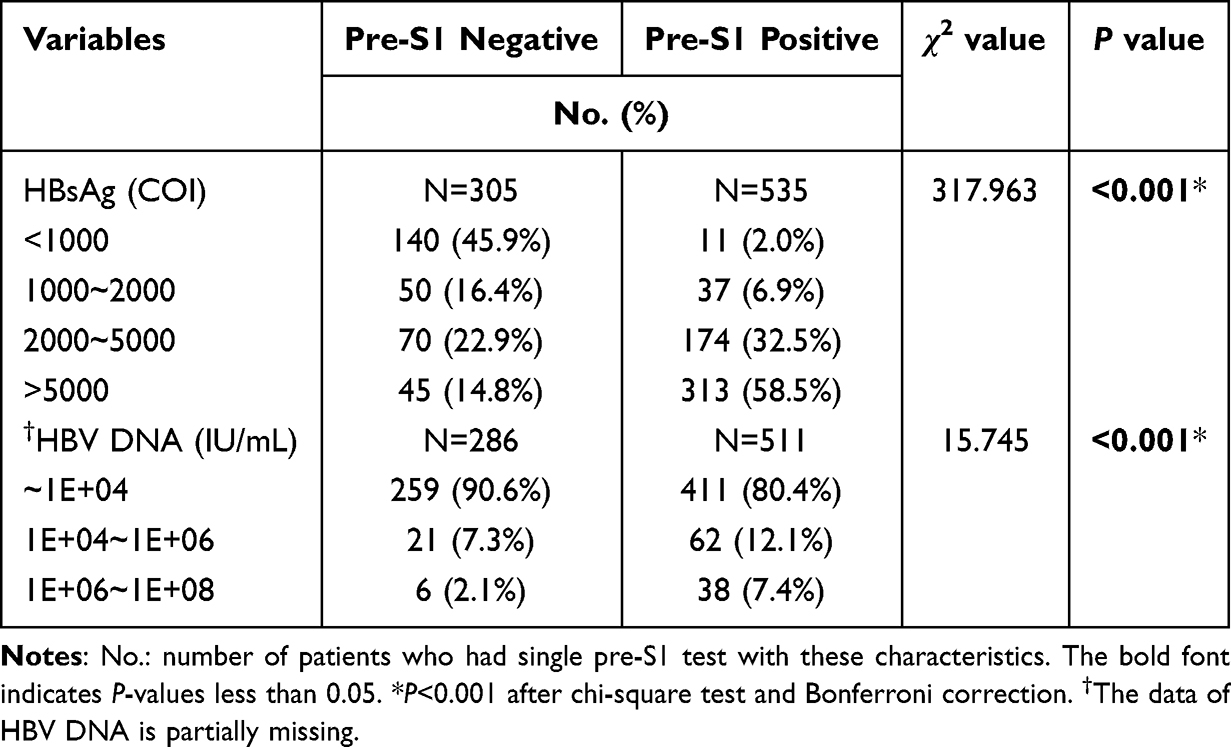 |
Table 2 Association of Pre-S1 Single Test Result with Other HBV Markers |
Correlation Analysis Between Pre-S1 Status and Hepatitis B-Related Cirrhosis and HCC
Single and multivariate analyses of the association between clinical factors and HCC risk in CHB patients are shown in Table 3. Pre-S1 negative, cirrhosis, age ≥50, and male gender were associated with a higher HCC risk.
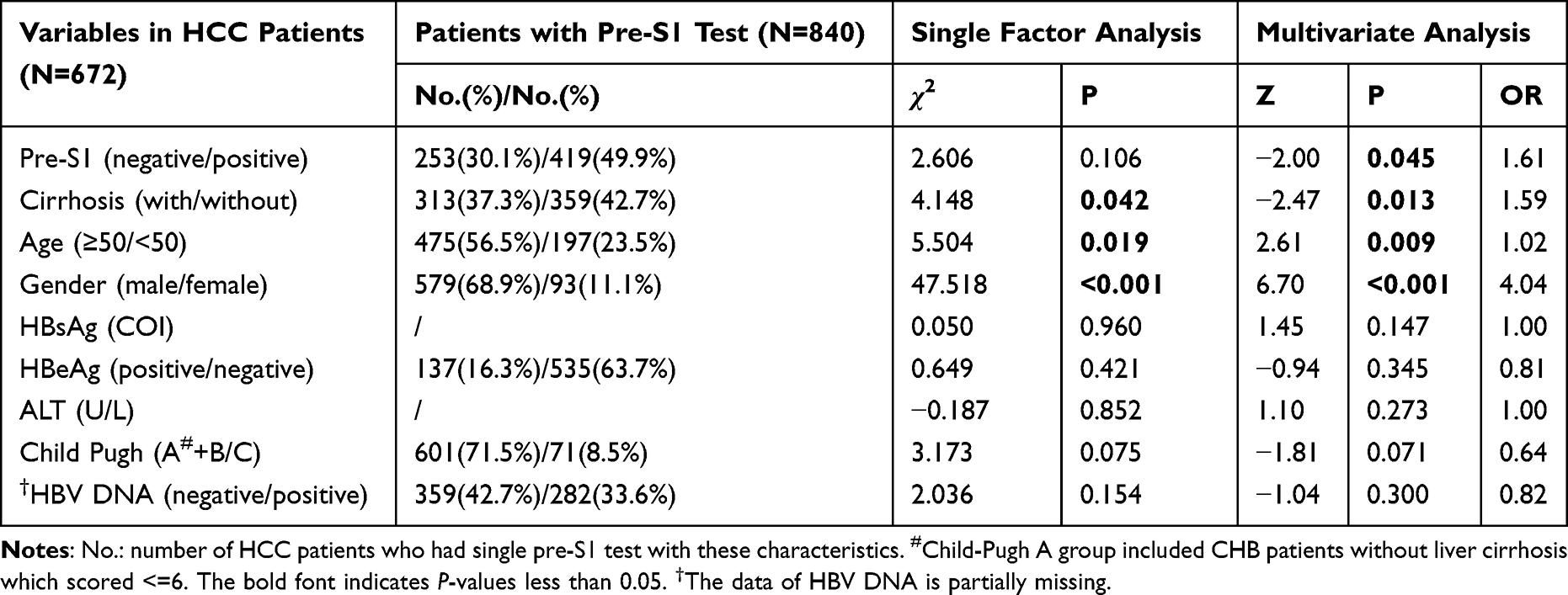 |
Table 3 Single and Multivariate Analysis for the Association of Clinical Factors with HCC Risk in Chronic HBV Infected Patients |
A total of 144 HBsAg positive patients were followed up with pre-S1 testing multiple times. The pre-S1 status was classified into four modes based on the changing trend (ie, negative-negative, positive-positive, positive-negative, and negative-positive). No significant association was found in cirrhosis risk between the pre-S1 follow-up modes. However, a significant difference was observed in HCC risk between the pre-S1 sustained negative and sustained positive groups (Table 4).
 |
Table 4 The Association Between Four Pre-S1 Follow-Up Modes with Cirrhosis and HCC, and Antiviral Treatment |
Logistic multiple regression analysis showed that patients with sustained pre-S1 negativity in multiple follow-up tests were associated with a higher HCC risk than that of the sustained positive group (Table 5). The odds ratio (OR) of multiple tests with negative pre-S1 maintenance versus multiple tests with positive pre-S1 maintenance was 7.12.
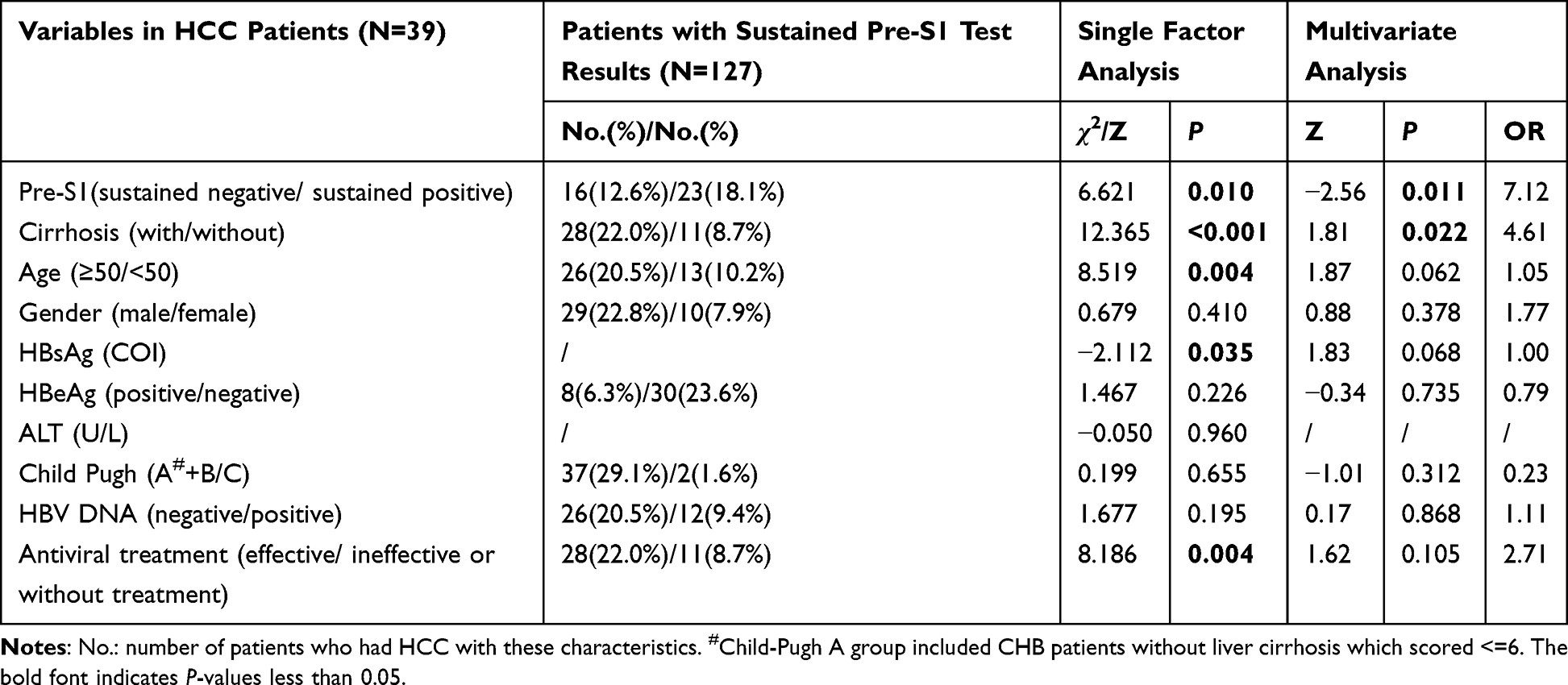 |
Table 5 Single and Multivariate Analysis for the Association of Clinical Factors with HCC Risk in Chronic HBV Infected Patients with Sustained Pre-S1 Test Results |
During the pre-S1 follow-up period, the antiviral drugs used by the patients included entecavir, tenofovir, telbivudine, adefovir, and lamivudine. As shown in Table 5, there was no significant difference in the multiple follow-up tests of pre-S1 status with antiviral treatments (χ2=4.895, P=0.180).
Comparison of the Sequence of the Pre-S1 Region Between Pre-S1 Positive and Negative Patients
The DNA and amino acid sequences of the pre-S1 region in the pre-S1 positive sample were consistent with those of type D HBV. The samples from two pre-S1 negative patients were of type C HBV origin and contained multiple pre-S1 sequences, including frameshift and deletion mutations. The general information and specific sequences are shown in Table 6 and Figure 1, respectively.
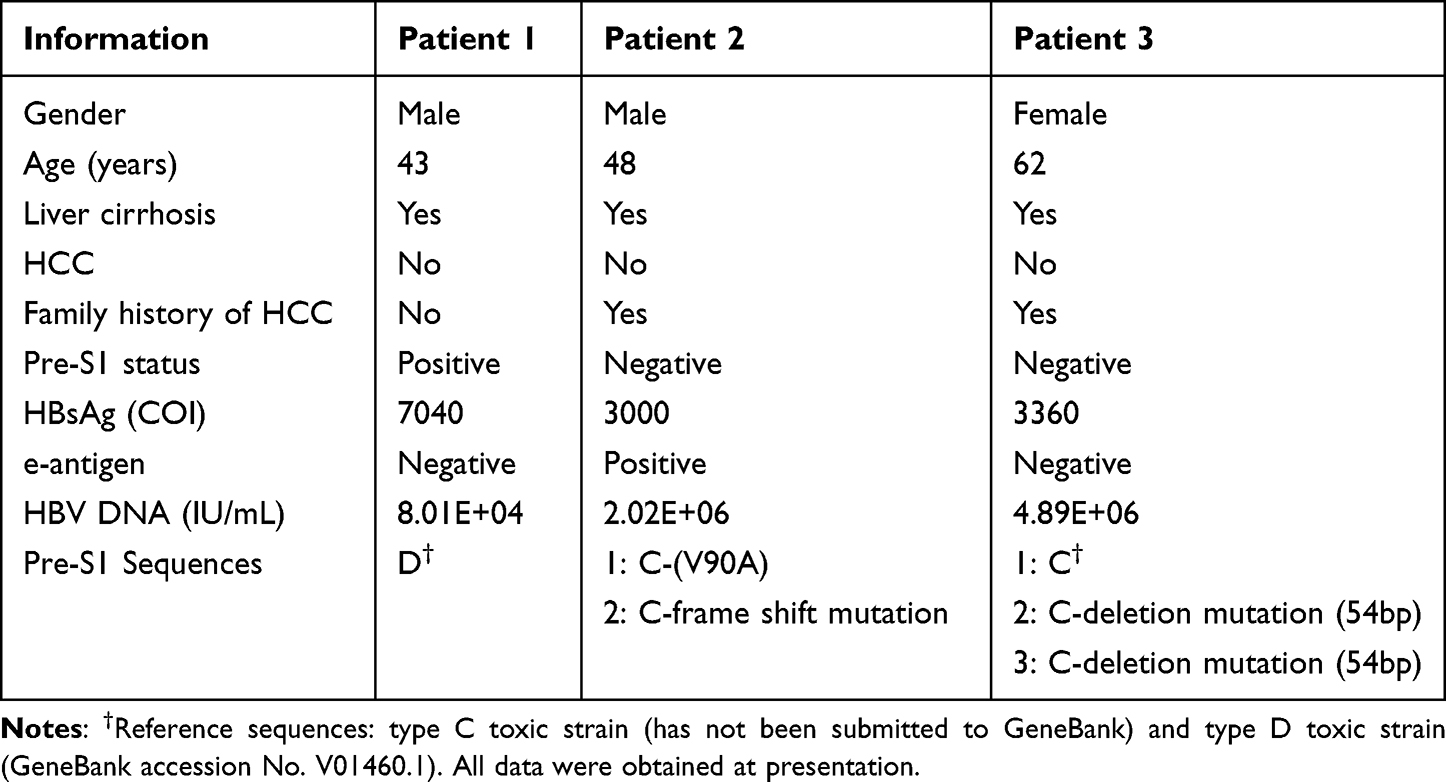 |
Table 6 Information of Pre-S1 Sequence Results of Pre-S1 Negative and Positive, Treatment Naïve Patients |
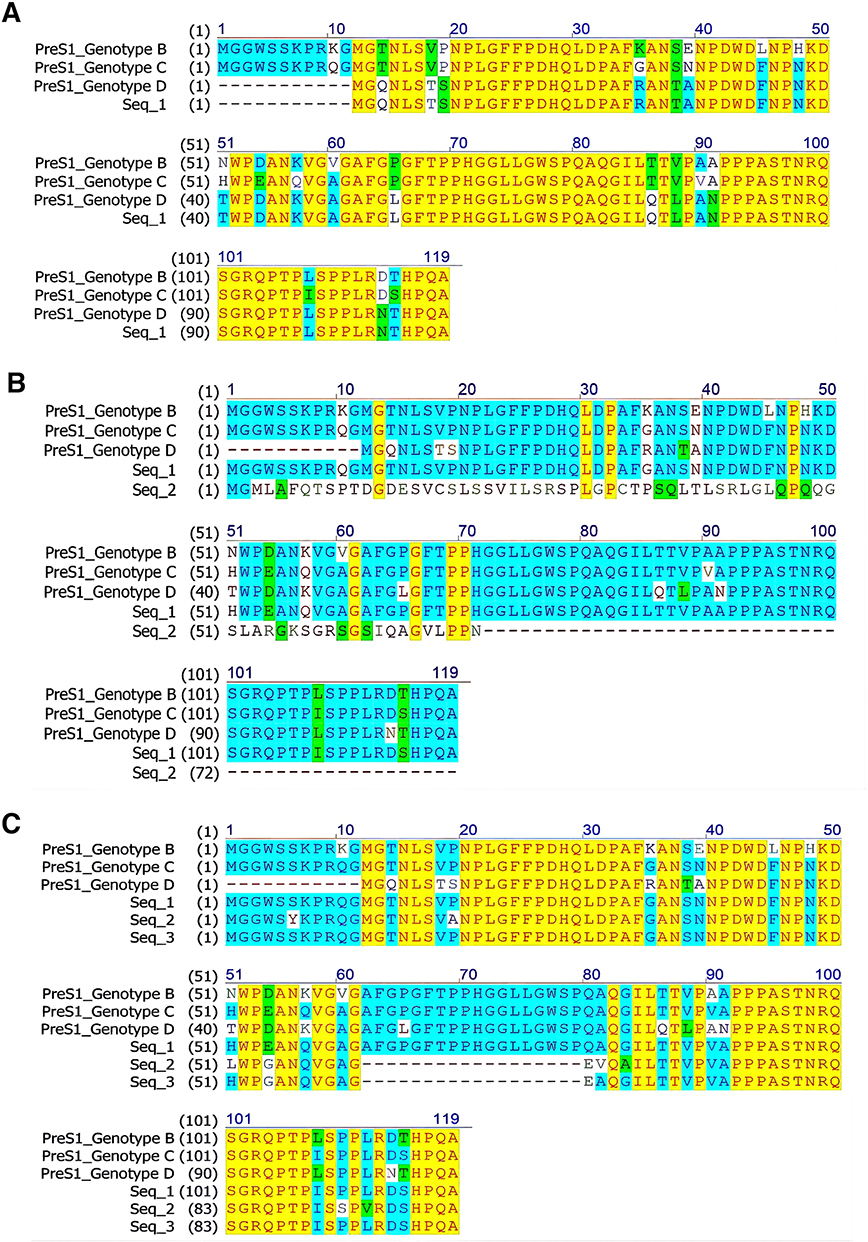 |
Figure 1 Pre-S1 amino acid sequences of pre-S1 positive and Pre-S1 negative treatment naïve patients. (A) The pre-S1 amino acid sequence of pre-S1 positive patient 1 (Seq_1) was consistent with D-type HBV. (B) The sample of pre-S1 negative patient 2 contained two pre-S1 sequences. Compared with C-type HBV, Seq_1 of the pre-S1 amino acid sequence had only one site mutation (V90A); another pre-S1 sequence had frame shift mutation resulting the mutation and premature termination. (C) Sequence analysis showed that the sample of pre-S1 negative patient 3 contained three pre-S1 sequences. Among them, the amino acid sequence of pre-S1 Seq_1 was identical with that of C type HBV; pre-S1 Seq_2 and Seq_3 contained deletion mutations. |
Discussion
The present study investigated the association between clinical pre-S1 status with other HBV markers and the adverse prognostic events of CHB in 840 patients with chronic HBV infection with a single test of pre-S1, and 144 CHB patients with multiple follow-up tests of pre-S1.
It was found that the HBsAg level was significantly higher in the pre-S1 positive group than in the pre-S1 negative group (Z=−15.983, P<0.001). The positive rate of pre-S1 was also found to increase significantly with the increase in HBsAg level (χ2=317.963, P<0.001) and HBV DNA load (χ2=15.745, P<0.001), indicating that pre-S1 positivity is an indicator of HBV presence and replication, similar to HBsAg and HBV DNA. In addition, single and logistic multiple regression analyses revealed an association between pre-S1 negativity and HCC risk, highlighting the importance of monitoring pre-S1 clinically.
HBsAg originates from sources including Dane particles and non-infectious filaments or globular “viral shells”, which are 102 to 103 times more abundant than Dane particles. Serum HBsAg level is associated with the content of covalently closed circular DNA (cccDNA), the original HBV cDNA template, in the liver nuclei. However, it may not always be parallel to HBV DNA levels, as the mRNA of HBsAg synthesis can also come from the integrated viral DNA in the host genome.18 Serum HBsAg is an important serum marker for screening and diagnosis of HBV infection, as well as for assessing the effects of HBV treatment. HBsAg level can independently predict long-term treatment efficacy and the effectiveness of the treatment regimen, with a lower baseline HBsAg indicating a higher likelihood of HBsAg seroconversion.
Pre-S1 is an important component of L-HBsAg, and in normal circumstances, the large surface protein encoded by the pre-S1 gene is closely associated with the virus cycle, including the interaction between viruses and hepatocyte receptors. Pre-S1 positivity can therefore be considered as a marker of HBV presence and replication, and thus can serve as an auxiliary indicator of HBV clearance status.23 In contrast, pre-S1 negativity in clinical tests may be due to an overall reduction in HBsAg or L-HBsAg synthesis to an undetectable level, or mutations that occur in the pre-S1 region.10,20
HBV polymerase lacks a proofreading function for DNA replication, leading to HBV mutants being selected during the reverse transcription step under immune and/or drug pressure.24 Mutations, such as base substitutions, deletions, or insertions, in the pre-S region may alter the phenotype of HBsAg, therefore affecting HBV infectivity, nucleic acid replication, serological markers, viral protein expression, and secretion. These mutations may also impact the immunogenicity and antigen-antibody binding capacity of HBV. Compared to the wild-type, pre-S1 variants may have adaptive antigenic properties or different replication capabilities that allow them to evade host immune surveillance or clearance.24
Studies have reported that HBsAg with pre-S deletion mutations (including pre-S1 and pre-S2 mutations) can accumulate in the endoplasmic reticulum (ER) of ground-glass hepatocytes (GGH).16,17,25 In fact, two pre-S mutants have been detected in the serum and HCC tissues of 60% of HCC patients,25,26 highlighting the clinical relevance of these mutations. Another study found that pre-S1 interacts with β-catenin to inhibit its phosphorylation, thereby activating the Wnt signaling pathway and promoting the transformation of normal hepatocytes to cancerous hepatocytes. Different types of GGH are related to different expression patterns and viral replication stages of HBsAg/HBcAg,16,17 with GGH type I containing pre-S1 deletion mutant.27 Deletion mutations in pre-S1 have been associated with an increased risk of HCC,21,22,28–30 these mutations are often observed in patients with HBV genotype C. Large deletion mutations involving the pre-S1 or pre-S2 regions have also been linked to an increased risk of HCC,31 as well as HCC recurrence after surgical resection.32
There are multi-mechanisms of chronic HBV infection in promoting the development of HCC. Within them, pre-S1 deletion mutations have been considered as a potential attributing factor. It was shown that these mutations can lead to the accumulation of virus particles in cells, causing endoplasmic reticulum stress, DNA oxidative damage, and genomic instability, all of which may contribute to an increased risk of HCC.26,33 In transgenic mice, pre-S mutants were found to induce hepatocyte dysplasia and hepatocellular carcinoma. Moreover, in a nested control study, the presence of pre-S mutants in HBV carriers was associated with a high risk of developing liver cancer.33 In the present study, no statistically significant differences in the ratios of cirrhosis between the pre-S1 negative and positive groups were found. However, logistic multiple regression analysis of the correlation between pre-S1 status, age, gender, HBsAg level and incidence of HCC in CHB patients with multiple follow-up pre-S1 tests showed that pre-S1 negativity (Z=−2.00, P=0.045, OR=1.61) and cirrhosis (Z=−2.47, P=0.013, OR=1.59) were risk factors for HCC. The OR of patients with sustained negative pre-S1 versus those with sustained positive pre-S1 was the highest (Z=−2.56, P=0.011, OR=7.12) (Table 5). These results suggest that pre-S1 negativity, especially sustained pre-S1 negativity, is associated with a higher risk of HCC. Furthermore, two pre-S1 negative patients with HBV DNA load were found to have type C HBV origin by sequencing and contain multiple pre-S1 sequences with frameshift mutations and deletion mutations. In sustained pre-S1 negative CHB patients, even when the HBsAg titers were lower than other types, they could still be detected in plasma, indicating the potential existence of pre-S1 mutations. Therefore, emphasizing pre-S1 detection in follow-up and early detection of mutations in the pre-S1 region may facilitate active treatment and intervention, close monitoring of the occurrence of HCC, and improved adverse prognostic events.
In the present study, no statistical difference was found in pre-S1 results between CHB patients treated with different antiviral drugs, indicating that existing drug therapy was not correlated with pre-S1 serological status. Current clinical practice guidelines recommend antiviral therapy for CHB patients to prevent disease progression to liver cirrhosis and HCC.34–38 However, even with effective antiviral therapy, most HBeAg positive CHB patients cannot achieve complete clearance of HBeAg (with or without anti-HBe seroconversion); the ideal endpoint of HBsAg negative conversion is also rarely achieved in CHBpatients with or without detectable HBV DNA replication. In addition, antiviral therapy can not eliminate the risk of liver cancer, especially in patients with liver cirrhosis. The eradication of HBV requires the clearance of cccDNA in liver cells.39,40 The expression of HBsAg is attributable to viral transcriptional template cccDNA and integrated HBV DNA in patients with low viral load.41 Currently, the commonly used therapeutic drugs for HBV infection are nucleoside analogs (NAs), which mainly inhibit HBV replication by inhibiting HBV polymerase but have no effect on cccDNA and the expression of integrated HBV DNA. Therefore, studying multi-target new drugs for HBV treatment is of great significance. Studies have shown that a significant decrease in type I and type II GGH can only be observed in patients after a long duration of treatment (median duration of 4.3 years), and the persistence of GGHs could explain the residual risk of HCC development under anti-HBV treatment. Intrahepatic GGHs and pre-S mutants are potential additional targets for HCC prevention in patients already receiving anti-HBV treatment.42,43
In conclusion, pre-S1 positivity reflects the presence of HBV and viral replication, similar to other HBV markers. Current oral anti-HBV drugs have no significant effect on pre-S1 serological reversion. Sustained positivity of pre-S1 and HBsAg or HBV DNA can reflect the unclearance of HBV. Pre-S1 mutations as indicated by sustained pre-S1 negativity and HBsAg positivity are associated with a higher risk of HCC. Thus, it is clinically significant for patients with chronic HBV infection to be monitored for pre-S1 status in follow-up visits. However, more studies are needed to establish the clinical significance of pre S1 status with the adverse prognostic events of CHB patients, and to understand HBV mutation sites and their roles in carcinogenesis of hepatitic B related HCC.
Acknowledgments
The authors want to thank Dr. GW Cao of the Department of Epidemiology, Second Military Medical University of China for the helpful discussion on the study. The authors would also like to thank TopEdit (www.topeditsci.com) for its linguistic assistance during the preparation of this manuscript.
Author Contributions
All authors made substantial contributions to conception and design, acquisition of data, or analysis and interpretation of data; took part in drafting the article or revising it critically for important intellectual content; agreed to submit to the current journal; gave final approval of the version to be published; and agree to be accountable for all aspects of the work.
Funding
This work was supported by the National Fund of Nature Science of P.R. China (Nos. 91129705, 81070340, 81971921) and Shanghai Pujiang Talent Program (09PJ1402600).
Disclosure
The authors have no conflict of interest in this work.
References
1. Stanaway JD, Flaxman AD, Naghavi M, et al. The global burden of viral hepatitis from 1990 to 2013: findings from the Global Burden of Disease Study 2013. Lancet. 2016;388:1081–1088. doi:10.1016/S0140-6736(16)30579-7
2. Zhang S, Wang F, Zhang Z. Current advances in the elimination of hepatitis B in China by 2030. Front Med. 2017;11:490–501. doi:10.1007/s11684-017-0598-4
3. Cai Y, Jia J. Update on epidemiology of hepatitis B and C in China. J Gastroenterol Hepatol. 2013;28:7–10. doi:10.1111/jgh.12220
4. Fattovich G. Natural history of hepatitis B. J Hepatol. 2003;39:S50–S58. doi:10.1016/S0168-8278(03)00139-9
5. Trépo C, Chan HL, Lok A. Hepatitis B virus infection. Lancet. 2014;384:2053–2063. doi:10.1016/S0140-6736(14)60220-8
6. Sarin SK, Kumar M, Eslam M, et al. Liver diseases in the Asia-Pacific region: a Lancet Gastroenterology & Hepatology Commission. Lancet Gastroenterol Hepatol. 2020;5:167–228. doi:10.1016/S2468-1253(19)30342-5
7. Liu CJ, Kao JH. Global perspective on the natural history of chronic hepatitis B: role of hepatitis B virus genotypes A to J. Semin Liver Dis. 2013;33:97–102. doi:10.1055/s-0033-1345716
8. Zhang Q, Cao GW, Zhang H. Genotypes, mutations, and viral load of hepatitis B virus and the risk of hepatocellular carcinoma: HBV properties and hepatocarcinogenesis. Hepat Mon. 2011;11:86–91. doi:10.1002/cncr.25522
9. Tian QJ, Jia JD. Hepatitis B virus genotypes: epidemiological and clinical relevance in Asia. Hepatol Int. 2016;10:854–860. doi:10.1007/s12072-016-9745-2
10. Chen BF. Hepatitis B virus pre-S/S variants in liver diseases. World J Gastroenterol. 2018;24:1507–1520. doi:10.3748/wjg.v24.i14.1507
11. Sugauchi F, Ohno T, Orito E, et al. Influence of hepatitis B virus genotypes on the development of preS deletions and advanced liver disease. J Med Virol. 2003;70:537–544. doi:10.1002/jmv.10428
12. Choi MS, Kim DY, Lee DH, et al. Clinical significance of pre-S mutations in patients with genotype C hepatitis B virus infection. J Viral Hepat. 2007;14:161–168. doi:10.1111/j.1365-2893.2006.00784.x
13. Hu JM, Liu KC. Complete and incomplete hepatitis B virus particles: formation, function, and application. Viruses. 2017;9:56. doi:10.3390/v9030056
14. Meier A, Mehrle S, Weiss TS, et al. Myristoylated PreS1-domain of the hepatitis B virus L-protein mediates specific binding to differentiated hepatocytes. Hepatology. 2013;58(1):31–42. PMID: 23213046. doi:10.1002/hep.26181
15. Yan H, Zhong G, Xu G, et al. Sodium taurocholate cotransporting polypeptide is a functional receptor for human hepatitis B and D virus. eLife. 2012;1:e00049. doi:10.7554/eLife.00049
16. Hadziyannis S, Gerber MA, Vissoulis C, et al. Cytoplasmic hepatitis B antigen in “ground-glass” hepatocytes of carriers. Arch Pathol. 1973;96:327–330.
17. Popper H. The ground glass hepatocyte as a diagnostic hint. Hum Pathol. 1975;6:517–520. doi:10.1016/S0046-8177(75)80069-4
18. Jiang B, Wu Q, Kuhnhenn L, et al. Formation of semi-enveloped particles as a unique feature of a hepatitis B virus PreS1 deletion mutant. Aliment Pharmacol Ther. 2019;50:940–954. doi:10.1111/apt.15381
19. Ogura S, Tameda M, Sugimoto K, et al. A substitution in the pre-S1 promoter region is associated with the viral regulation of hepatitis B virus. Virol J. 2019;16:59. doi:10.1186/s12985-019-1169-x
20. Fan YF, Lu CC, Chen WC, et al. Prevalence and significance of hepatitis B virus (HBV) pre-S mutants in serum and liver at different replicative stages of chronic HBV infection. Hepatology. 2001;33:277–286. doi:10.1053/jhep.2001.21163
21. Gao ZY, Li T, Wang J, et al. Mutations in preS genes of genotype C hepatitis B virus in patients with chronic hepatitis B and hepatocellular carcinoma. J Gastroenterol. 2007;42:761–768. doi:10.1007/s00535-007-2085-1
22. Jang JS, Kim HS, Kim HJ, et al. Association of concurrent hepatitis B surface antigen and antibody to hepatitis B surface antigen with hepatocellular carcinoma in chronic hepatitis B virus infection. J Med Virol. 2009;81:1531–1538. doi:10.1002/jmv.21577
23. van Ditzhuijsen TJ, Kuijpers LP, Koens MJ, et al. Hepatitis B pre-S1 and pre-S2 proteins: clinical significance and relation to hepatitis B virus DNA. J Med Virol. 1990;32(2):87–91. doi:10.1002/jmv.1890320204
24. Locarnini S, Zoulim F. Molecular genetics of HBV infection. Antivir Ther. 2010;15(Suppl 3):3–14. doi:10.3851/IMP1619
25. Lin WL, Hung JH, Huang W. Association of the hepatitis B virus large surface protein with viral infectivity and endoplasmic reticulum stress-mediated liver carcinogenesis. Cells. 2020;9:2052. doi:10.3390/cells9092052
26. Liu W, Cai S, Pu R, et al. HBV preS mutations promote hepatocarcinogenesis by inducing endoplasmic reticulum stress and upregulating inflammatory signaling. Cancers. 2022;14(13):3274. doi:10.3390/cancers14133274
27. Su IJ, Wang HC, Wu HC, et al. Ground glass hepatocytes contain pre-S mutants and represent preneoplastic lesions in chronic hepatitis B virus infection. J Gastroenterol Hepatol. 2008;23:1169–1174. doi:10.1111/j.1440-1746.2008.05348.x
28. Chen BF, Liu CJ, Jow GM, et al. High prevalence and mapping of pre-S deletion in hepatitis B virus carriers with progressive liver diseases. Gastroenterology. 2006;130(4):1153–1168. doi:10.1053/j.gastro.2006.01.011
29. Huy TT, Ushijima H, Win KM, et al. High prevalence of hepatitis B virus pre-S mutant in countries where it is endemic and its relationship with genotype and chronicity. J Clin Microbiol. 2003;41:5449–5455. doi:10.1128/JCM.41.12.5449-5455.2003
30. Yin J, Xie J, Zhang H, et al. Significant association of different preS mutations with hepatitis B-related cirrhosis or hepatocellular carcinoma. J Gastroenterol. 2010;45(10):1063–1071. doi:10.1007/s00535-010-0253-1
31. Teng CF, Wu HC, Su IJ, et al. Hepatitis B virus pre-S mutants as biomarkers and targets for the development and recurrence of hepatocellular carcinoma. Viruses. 2020;12:945. doi:10.3390/v12090945
32. Teng CF, Li TC, Huang HY, et al. Next-generation sequencing-based quantitative detection of hepatitis B virus pre-S mutants in plasma predicts hepatocellular carcinoma recurrence. Viruses. 2020;12:796. doi:10.3390/v12080796
33. Choi YM, Lee SY, Kim BJ. Naturally occurring hepatitis B virus mutations leading to endoplasmic reticulum stress and their contribution to the progression of hepatocellular carcinoma. Int J Mol Sci. 2019;20:597. doi:10.3390/ijms20030597
34. Sarin SK, Kumar M, Lau GK, et al. Asian-Pacific clinical practice guidelines on the management of hepatitis B: a 2015 update. Hepatol Int. 2016;10:1–98. doi:10.1007/s12072-015-9675-4
35. World Health Organization. Guidelines for the Prevention, Care and Treatment of Persons with Chronic Hepatitis B Infection. Geneva, Switzerland: World Health Organization; 2015. PMID: 26225396 Bookshelf ID: NBK305553.
36. European Association for the Study of the Liver. EASL 2017 Clinical Practice Guidelines on the management of hepatitis B virus infection. J Hepatol. 2017;67:370–398. doi:10.1016/j.jhep.2017.03.021
37. Terrault NA, Lok ASF, McMahon BJ, et al. Update on prevention, diagnosis, and treatment of chronic hepatitis B: AASLD 2018 hepatitis B guidance. Hepatology. 2018;67:1560–1599. doi:10.1002/hep.29800
38. Yim HJ, Kim JH, Park JY, et al. Comparison of clinical practice guidelines for the management of chronic hepatitis B: when to start, when to change, and when to stop. Clin Mol Hepatol. 2020;26:411–429. doi:10.3350/cmh.2020.0049
39. Dias JD, Sarica N, Neuveut C. Early steps of hepatitis B life cycle: from capsid nuclear import to cccDNA formation. Viruses. 2021;13:757. doi:10.3390/v13050757
40. Martinez MG, Boyd A, Combe E, et al. Covalently closed circular DNA: the ultimate therapeutic target for curing hepatitis B virus infections. J Hepatol. 2021;75:706–717. doi:10.1016/j.jhep.2021.05.013
41. Meier M, Calabrese D, Suslov A, et al. Ubiquitous expression of HBsAg from integrated HBV DNA in patients with low viral load. J Hepatol. 2021;75(4):840–847. doi:10.1016/j.jhep.2021.04.051
42. Tsai HW, Lin YJ, Wu HC, et al. Resistance of ground glass hepatocytes to oral antivirals in chronic hepatitis B patients and implication for the development of hepatocellular carcinoma. Oncotarget. 2016;7:27724–27734. doi:10.18632/oncotarget.8388
43. Coppola N, Onorato L, Minichini C, et al. Clinical significance of hepatitis B surface antigen mutants. World J Hepatol. 2015;7:2729–2739. doi:10.4254/wjh.v7.i27.2729
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Validation of Hepatocellular Carcinoma Risk Prediction Models in Patients with Hepatitis B-Related Cirrhosis
Cheng R, Xu X
Journal of Hepatocellular Carcinoma 2022, 9:987-997
Published Date: 12 September 2022
Comparison of Clinical Manifestations and Related Factors of Hepatocellular Carcinoma with Chronic Hepatitis B
Hou H, Liang L, Deng L, Ye W, Wen Y, Liu J
International Journal of General Medicine 2024, 17:2877-2886
Published Date: 25 June 2024
The Mechanism of APOBEC3B in Hepatitis B Virus Infection and HBV Related Hepatocellular Carcinoma Progression, Therapeutic and Prognostic Potential
Yang X, Wang H, Yu C
Infection and Drug Resistance 2024, 17:4477-4486
Published Date: 17 October 2024
Machine Learning-Based Model Used for Predicting the Risk of Hepatocellular Carcinoma in Patients with Chronic Hepatitis B
Wu T, Yan J, Xiong F, Liu X, Zhou Y, Ji X, Meng P, Jiang Y, Hou Y
Journal of Hepatocellular Carcinoma 2025, 12:659-670
Published Date: 3 April 2025
Combined Analysis of Protein Induced by Prothrombin Induced by Vitamin K Absence (PIVKA) and Alpha-L-Fucosidase (AFU) with Alpha-Fetoprotein (AFP) May Improve the Diagnostic Efficacy for Liver Cirrhosis and Hepatocellular Carcinoma in Chronic Hepatitis B
Hou H, Weng R, Liang L, Han W
International Journal of General Medicine 2025, 18:6031-6042
Published Date: 2 October 2025