Back to Journals » Journal of Pain Research » Volume 18
Pragmatic Randomized Controlled Trial of Pharmacopuncture Therapy for Cervical Disc Herniation: A Pilot Study
Authors Lee SW ![]() , Ahn YJ, Kim S
, Ahn YJ, Kim S ![]() , Lee Y, Cho HW, Hong Y, Nam D, Park YC, Kim EJ
, Lee Y, Cho HW, Hong Y, Nam D, Park YC, Kim EJ ![]() , Lee YJ
, Lee YJ ![]() , Ha IH
, Ha IH ![]()
Received 12 March 2025
Accepted for publication 8 July 2025
Published 23 July 2025 Volume 2025:18 Pages 3689—3707
DOI https://doi.org/10.2147/JPR.S527880
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Houman Danesh
Su Won Lee,1 Yong-Jun Ahn,2 Suna Kim,3 Yeonsun Lee,4 Hyun-Woo Cho,5 Yejin Hong,6 Dongwoo Nam,7 Yeon-Cheol Park,7 Eun-Jung Kim,8 Yoon Jae Lee,1 In-Hyuk Ha1
1Jaseng Spine & Joint Research Institute, Jaseng Medical Foundation, Seoul, Republic of Korea; 2Jaseng Clinical Research Center, Jaseng Hospital of Korean Medicine, Seoul, Republic of Korea; 3Jaseng Clinical Research Center, Daejeon Jaseng Hospital of Korean Medicine, Daejeon, Republic of Korea; 4Jaseng Clinical Research Center, Bucheon Jaseng Hospital of Korean Medicine, Bucheon, Republic of Korea; 5Jaseng Clinical Research Center, Haeundae Jaseng Hospital of Korean Medicine, Busan, Republic of Korea; 6Department of Acupuncture and Moxibustion, Kyung Hee University Korean Medicine Hospital, Seoul, Republic of Korea; 7Department of Acupuncture & Moxibustion, College of Korean Medicine, Kyung Hee University, Seoul, Republic of Korea; 8Department of Acupuncture & Moxibustion, College of Korean Medicine, Dongguk University Bundang Oriental Hospital, Seongnam, Republic of Korea
Correspondence: In-Hyuk Ha, Jaseng Spine & Joint Research Institute, Jaseng Medical Foundation, 540, Gangnamdae-ro, Gangnam-gu, Seoul, 06110, Republic of Korea, Tel +82-2-2222-2740, Email [email protected]
Purpose: Cervical disc herniation (CDH) is increasingly prevalent, highlighting the need for more effective treatments. Although pharmacopuncture therapy is one of the most widely used treatment methods for CDH in Korean medicine clinical practice, there are few high-quality studies conducted in Korea. Therefore, we aimed to evaluate the efficacy and safety of pharmacopuncture therapy for CDH through a pragmatic clinical trial that reflects clinical practice while utilizing well-designed study settings of a randomized controlled trial.
Patients and Methods: This three-armed, pragmatic, pilot, randomized controlled trial included pharmacopuncture (Phm-Acu), acupuncture (Acu), and usual care (UC) groups in a 1:1:1 ratio. Participants were treated twice a week for 6 weeks, with follow-up extending to week 25. The primary outcome was the neck pain Numeric Rating Scale (NRS). The secondary outcomes were arm pain NRS, neck and arm pain Visual Analog Scale, Neck Disability Index (NDI), Northwick Park Questionnaire (NPQ), Patient Global Impression of Change (PGIC), Short Form-12 Health Survey (SF-12), and EuroQol-5-dimension-5-level (EQ-5D-5L).
Results: Eighty participants (Phm-Acu: 29, Acu: 29, and UC: 26) were selected. At week 7, neck pain NRS significantly decreased in the Phm-Acu group than that in the UC (2.73, 95% confidence interval (CI) 1.87– 3.59) and Acu groups (1.68, 95% CI 0.84– 2.53). Survival analysis revealed that the Phm-Acu group showed the fastest recovery rate. The Phm-Acu group showed significant improvement compared with the Acu and UC groups for all other pain outcomes and PGIC and compared with the UC group for NDI, NPQ, EQ-5D-5L, and SF-12 [physical]. The area under the curve analysis showed that the Phm-Acu group showed significant differences in all outcomes except SF-12 [mental] compared with the UC group. No serious adverse events occurred; four patients experienced mild adverse events.
Conclusion: In CDH, pharmacopuncture was more effective in reducing pain and achieving functional recovery than acupuncture and usual care.
Keywords: neck pain, non-invasive therapy, pain management, functional recovery
Introduction
Cervical disc herniation (CDH) results from the displacement of the nucleus pulposus within an intervertebral disc, with nerve root or spinal cord inflammation and compression, causing pain or neurological symptoms over a wide region, including the neck and upper extremities.1 CDH may be acute or chronic; acute CDH commonly occurs as a result of trauma, whereas chronic CDH occurs when the intervertebral disc degenerates and becomes desiccated during natural aging.2 A CDH epidemiology study reported a 107 and 63.5 annual incidence in men and women, respectively, per 100000 people.3 A study in Korea reported a trend of annual increases in CDH prevalence, with a higher occurrence in women than in men; however, the prevalence increased with age for both sexes.4 The study results are based on the responses of individuals who had CDH symptoms and received treatment; the actual figures are even higher when including patients with asymptomatic CDH.5 The increasing CDH prevalence translates into a substantial socioeconomic burden. According to the National Health Insurance Statistical Yearbook, medical care costs for CDH in 2022 were approximately KRW 337.1 billion, with CDH ranking 31st in conventional (Western) medicine and 16th in Korean medicine (KM) regarding frequent diagnosis requiring inpatient care.6 Furthermore, the frequency of surgical treatments, such as cervical discectomy and fusion, has increased owing to diagnostic and surgical tool development and rising CDH prevalence in an aging society.7,8
CDH treatment is generally categorized into conservative and surgical therapies. Conservative CDH management includes pharmacotherapy, traction, physiotherapy, and spinal orthoses use. For conditions refractory to conservative therapies, surgical treatments, such as anterior or posterior cervical discectomy, for removing bone spurs and affected discs, combined with adjacent vertebrae fusion, are considered.9 However, these surgeries are invasive interventions that may lead to side effects and complications, such as nerve damage, vascular injury, and enhanced degenerative changes, in the adjacent segments.10 In addition, a study confirmed that surgical decompression is effective in the short term; however, no significant difference is observed in the long-term outcomes compared with those of conservative treatment.11 Recently, with increasing personal and socioeconomic losses due to CDH, more aggressive treatments, such as cervical epidural steroid injections and nerve blocks, such as stellate ganglion blocks, have been used as alternatives before surgery; however, their effectiveness remains controversial.12
In KM clinical practice, various combinations of nonsurgical modalities, such as acupuncture, pharmacopuncture, herbal medicine, Chuna manual therapy, and acupotomy, have been used, with several studies reporting their effectiveness for CDH.13–20 Among them, pharmacopuncture therapy integrates acupuncture and pharmacotherapy, involving the injection of filtered and sterilized herbal medicine extracts into acupoints to enhance efficacy.21 The therapeutic effects of pharmacopuncture arise from the combined influence of physical stimulation at acupoints and the chemical stimulation of the pharmacopuncture solution.22 Acupoint stimulation leads to changes in neurotransmitter secretion, activation of pain modulation pathways, muscle relaxation, and improved blood flow.23,24 The pharmacopuncture solution, depending on the type of medicinal herb used, has been reported to have effects such as anti-inflammatory, analgesic, and neuroprotective properties. For example, bee venom exhibits anti-inflammatory effects by modulating macrophage polarization via melittin25 and Jungsongouhyul pharmacopuncture was related to pain reduction and motor nerve recovery.26 In addition, hominis placenta has been reported to have antioxidant and immune-enhancing properties.27,28 Beyond the benefits of traditional acupuncture, pharmacopuncture offers advantages such as rapid onset of action (bypassing the gastrointestinal tract), applicability for patients who struggle with oral medication, and easy dosage adjustment.
Meanwhile, According to a survey of KM doctors (KMDs) treating CDH, pharmacopuncture was the most used modality, followed by acupuncture, herbal medicine, and Chuna manual therapy in similar percentages.29 A systematic review and meta-analysis investigating the effectiveness of pharmacopuncture for cervical spondylosis showed that pharmacopuncture, either as monotherapy or combined therapy, significantly decreased pain and improved quality of life.30 However, the studies included in the meta-analysis were highly heterogeneous, had low-quality evidence, and provided limited information on the safety of pharmacopuncture, which indicates that existing studies do not reflect active pharmacopuncture use in clinical practice, resulting in a lack of quality evidence. Moreover, all the studies were conducted solely in China, with only one randomized controlled trial (RCT) on pharmacopuncture for chronic neck pain reported in the Republic of Korea, and no specific studies on CDH were identified. Therefore, given the scarcity of research despite the widespread clinical use of pharmacopuncture in Korea, we designed a pragmatic RCT to better reflect clinical practice in KM. This study aimed to evaluate the efficacy and safety of pharmacopuncture therapy for CDH compared with acupuncture and usual care group. The result of this study may provide foundational evidence for future large-scale studies and contribute to the selection of conservative treatment strategies.
Materials and Methods
The study protocol was approved by the Institutional Review Boards of the participating study centers in November 2021: Jaseng Hospital of Korean Medicine, Daejeon Jaseng Hospital of Korean Medicine, Bucheon Jaseng Hospital of Korean Medicine, Haeundae Jaseng Hospital of Korean Medicine, Kyung Hee University Korean Medicine Hospital, Kyung Hee University Korean Medicine Hospital at Gangdong, and Dongguk University Bundang Korean Medicine Hospital (approval numbers: JASENG 2021–10-016, JASENG 2021–10-018, JASENG 2021–10-014, JASENG 2021–10-017, KOMCIRB 2021–10-002, KHNMCOH 2021–10-009, and DUBOH 2021–0013). This study was registered at Clinicaltrials.gov (NCT05240586) on 13 February 2022 and cris.nih.go.kr (KCT0006616) on 21 February 2022, before participant recruitment.
Study Design and Procedures
This three-armed, parallel, pragmatic RCT aimed to analyze and confirm the comparative effectiveness of pharmacopuncture therapy for patients with CDH. Conducted as a multicenter study, it targeted 84 patients recruited based on competitive enrollment from seven KM hospitals in Korea. The volunteers underwent screening, and if they met the inclusion/exclusion criteria, they were randomized into three arms: The pharmacopuncture (Phm-Acu), acupuncture (Acu), and Western medicine-based usual care (physiotherapy and medication) (UC) strategy groups in a 1:1:1 ratio. The selected participants attended intervention sessions for their allocated groups twice a week for 6 weeks. Assessments were tailored to the outcome measures; weekly assessments were conducted during the treatment period, with follow-up assessments at weeks 7, 13, and 25. We observed changes in treatment efficacy and potential relapse at week 7, which follows the completion of treatment sessions, week 13, which falls within the typical 6–12 week period for re-evaluating non-surgical treatments,31 and week 25, which is a critical juncture for monitoring the progression of chronic CDH. The detailed schedule is presented in Table 1.
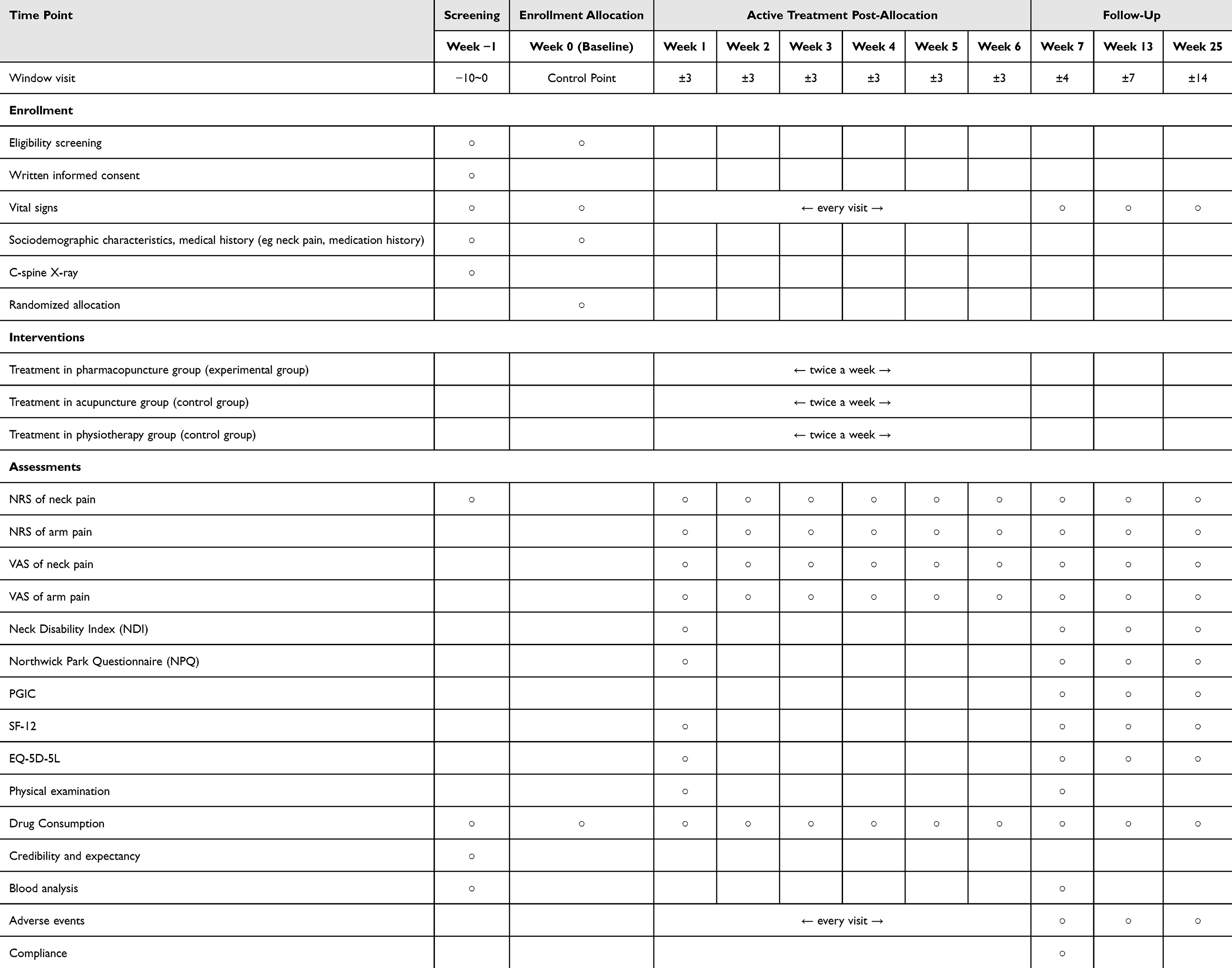 |
Table 1 Trial Timetable |
Participants
The study recruited patients who had CDH symptoms for ≤ 12 months and needed medical care. The inclusion/exclusion criteria are described below. The study was fully explained to participants before enrollment, and they voluntarily completed and signed the informed consent form.
Inclusion Criteria
- CDH Symptoms for < 12 months
- Neck pain Numeric Rating Scale (NRS) score > 5
- Neuromuscular symptoms in one or both upper limbs (including pain, pull, numbness, sensory abnormalities, and motor abnormalities)
- Discrimination findings above a protrusion that could explain clinical symptoms on cervical spine magnetic resonance imaging (MRI) or computed tomography (CT)
- Aged 19–69 years
- Provided written informed consent
Exclusion Criteria
- A diagnosis of a specific serious disease that could cause neck pain (such as cancer spread to the spine, acute spine fracture, and spine dislocation)
- Progressive or severe neurological deficits
- Pain due to soft tissue disease rather than spinal pathology (such as cancer, fibromyalgia, rheumatoid arthritis, and gout)
- Other chronic diseases (including stroke, myocardial infarction, kidney disease, diabetic neuropathy, dementia, and epilepsy) that could interfere with therapeutic effects or outcome interpretation
- Current use of steroids, immunosuppressants, or psychotropic or other medications that could affect outcomes
- Conditions that made pharmacopuncture therapy inappropriate or unsafe, such as hemorrhagic disease, taking anticoagulant drugs, severe diabetes, or patients at high risk of infection
- Taking non-steroidal anti-inflammatories or undergoing pharmacopuncture, acupuncture, or physiotherapy within 1 week
- Pregnancy, planning pregnancy, or lactating
- Cervical surgery within the past 3 months
- Participation in another clinical trial within 1 month, participation in another study within 6 months of the date of selection, or plans to participate in another trial during the follow-up period
- Inability to provide written informed consent
- Participants who would have difficulty participating in the trial based on the decision of the investigator.
Sample Size
This study was a pragmatic RCT designed to compare the effects of pharmacopuncture, acupuncture, and physiotherapy and medication in patients with CDH. No previous studies with the same design were available to determine the sample size. The minimum sample size recommended for a pilot clinical trial was 25; therefore, 25 patients were allocated to each of the three groups.32 In addition, considering a 10% dropout rate and the participation of seven hospitals, the sample size was set at 84, and participants were recruited accordingly.
Randomization and Blinding
Eligible participants were randomly assigned to one of the three groups (Phm-Acu, Acu, and UC) in a 1:1:1 ratio. A random number table was created using R studio 1.1.463 (© 2009–2018 R Studio, Inc.) by a statistician in advance, and 28 participants were randomly assigned to each group. Random sequence generation was based on block randomization, with block sizes of three or six randomly selected. The randomization results were sealed in an opaque envelope and stored in a double-locked cabinet. Investigators/coordinators at each study institution opened the envelopes to assign participants who met the inclusion/exclusion criteria and had provided informed consent. The randomization number was documented in the electronic chart. Owing to the nature of the intervention and study design, blinding the participants and KMDs performing the interventions was impossible, and only assessor blinding was maintained. The assessors did not participate in the intervention and performed assessments in a separate place before the intervention.
Interventions
While this study was designed as a pragmatic clinical trial and did not impose strict limitations on intervention procedures, we provided all participating institutions with the following basic guidelines to ensure a reasonable degree of standardization in treatment methods.
Pharmacopuncture
Pharmacopuncture was performed twice a week for 6 weeks. Treatment details, such as the type of pharmacopuncture solution, the dose administered, selected acupoints, and injection depth, were based on the clinical judgment of the KMDs, considering patient symptoms, radiological findings, and degree of improvement. The pharmacopuncture solutions were produced in extramural herbal dispensaries that continued to manufacture pharmacopuncture solutions for each medical institution. The acupoints used for pharmacopuncture were the GB20, GV16, GB21, SI15, SI14, and Hyeopcheok points at 0.5 cun (unit of length: 1 cun is approximately 1.31 inches) of C3–C5. Procedural details, including the acupoints where pharmacopuncture was administered, type of pharmacopuncture solution used, and dose administered (range: 0.1‒6 cc), were recorded in the electronic chart. An example of a procedural image for pharmacopuncture therapy is shown in Supplementary Figure 1.
Acupuncture
Acupuncture was performed twice a week for 6 weeks. Treatment details, such as acupoint selection, number of needles used, and needling depth, were based on the clinical judgment of the KMDs, considering patient symptoms, radiological findings, and degree of improvement. The acupoints used were the GB20, GV16, GB21, SI15, SI14, and Hyeopcheok points at 0.5 cun of C3–C5. The needles typically range from 30–60 mm in length and 0.2–0.4 mm in thickness. Procedural details, such as the acupoints where acupuncture was administered and the number of needles used (range: 5‒30 EA), were recorded in the electronic chart.
Usual Care (Medication & Physiotherapy)
Physiotherapy was performed twice a week for 6 weeks. Details, such as physiotherapy method selection, area of application, and physiotherapy duration, were based on the clinical judgment of the physician, considering patient symptoms, radiological findings, and degree of improvement. Details of the prescribed and performed physiotherapy, such as the type, frequency, and area of application, were recorded in the electronic chart. Regarding medication, analgesics and muscle relaxants were prescribed as needed, based on the clinical judgment of the physician. The types, dosage, and duration of use of the prescribed medication were recorded in the case report form. Data on all orally administered medicines used for CDH symptom management and treatment in clinical practice were collected. These included the N02 (analgesics), M01, and M02 subgroups, according to the Anatomical Therapeutic Chemical Classification System. Medications were administered within the permissible dose range applied in clinical practice.
Outcomes
Primary Outcome
The primary outcome of this study was the NRS for neck pain, an objective measure of subjective pain intensity experienced by patients. Participants rated their neck pain intensities over the past week on a 0‒10 scale, where 0 represented no pain and 10 represented the worst imaginable discomfort, selecting the number that best reflected their current discomfort. Measurements were taken weekly during the treatment period (six times) and at follow-up (weeks 7, 13, and 25 from baseline).
Secondary Outcomes
NRS of Radiating Arm Pain
Participants rated the intensity of their radiating arm pain over the past week on a 0–10 scale by selecting a number that best represented the severity of their discomfort. NRS measurements were conducted weekly during the treatment period (six measurements in total) and at follow-up (weeks 7, 13, and 25 from baseline).
Visual Analog Scale (VAS) of Neck and Radiating Arm Pain
The VAS is an outcome measure used to assess and record pain intensity on a 100-mm horizontal line, with one end indicating “no pain” and the other indicating “worst pain imaginable.” Patients marked a specific point on the scale to indicate the intensity of their neck and radiating arm pain over the past week. This measurement was performed weekly during the treatment period (six measurements in total) and at follow-up (weeks 7, 13, and 25 from baseline).
Neck Disability Index (NDI)
The NDI is designed to assess disability associated with daily activities due to neck pain. It is a 10-item questionnaire scored on a 0–5 scale. The total score is divided by the number of scored items to obtain an average score.33 NDI assessments were conducted at baseline and during follow-up (weeks 7, 13, and 25 from baseline).
Northwick Park Questionnaire (NPQ)
The NPQ is a self-report questionnaire comprising nine items related to daily activities affected by neck pain. Each item is scored on a 0–4 scale, with higher scores indicating worse dysfunction.34 The total score is calculated by summing the individual item scores. The NPQ percentage can be obtained by dividing the total score by the maximum score of the responded items and multiplying it by 100. We used the Korean version of the NPQ, with proven reliability and validity in a previous study.35 NPQ assessment was performed at baseline and during follow-up (weeks 7, 13, and 25 from baseline).
Patient Global Impression of Change (PGIC)
The PGIC is used for subjective assessment of the perceived improvement of a patient and comprises seven levels, where lower scores indicate more improvement. PGIC assessment was performed at baseline and during follow-up (weeks 7, 13, and 25 from baseline).
Short Form-12 Health Survey (SF-12)
The SF-12 is a questionnaire used for assessing health-related quality of life. It comprises 12 items across eight categories, with higher scores indicating better health-related quality of life. It provides two types of summary scores: the physical (PCS) and mental (MCS) component summaries. A validated Korean version of the questionnaire was used in this study.36 Assessment with SF-12 was performed at baseline and during follow-up (weeks 7, 13, and 25 from baseline).
EuroQol-5-Dimension-5-Level (EQ-5D-5L)
EQ-5D-5L comprises five dimensions (mobility, self-care, usual activities, pain/discomfort, and anxiety/depression), with each item assessing the level of each dimension. Weights were assigned based on the level of each dimension, and preference scores were calculated accordingly.37 The EQ-5D-5L was measured at baseline and during follow-up (weeks 7, 13, and 25 from baseline).
Safety Assessment
For safety assessment, clinical pathology tests (complete blood count, clinical chemistry tests, and C-reactive protein) were performed before and after treatment, and adverse events (AEs) were surveyed at each visit. AEs are undesirable and unintended signs, symptoms, or diseases occurring after an intervention during a clinical trial, including events without a confirmed causal relationship with the applied intervention. During this study, AE data were collected and analyzed through patient-reported symptoms and investigator observations. For all AEs, causality between the treatment and the event was assessed using a 6-level scale based on the World Health Organization Uppsala Monitoring Center Causality Assessment System. AE severity was assessed in three levels based on the Spilker classification.38 Safety assessment was performed by comparatively analyzing the frequency of AEs that occurred, AEs suspected to be treatment-related, and serious AEs across the three groups.
Statistical Analysis
In this study, intention-to-treat (ITT) was the primary analysis, and a per-protocol (PP) analysis was performed separately for participants who underwent at least nine treatment sessions during the 6-week treatment period. Between-group comparisons were made as follows: Phm-Acu vs UC and Phm-Acu vs Acu. The comparative analysis aimed to test and verify Phm-Acu treatment superiority. A mixed model for repeated measures was implemented for missing values. For sensitivity analysis, multiple imputation was used to process missing data, and the last observation carried forward method was applied to replace missing values.
For analysis of participant demographic characteristics in each group, between-group comparisons were performed using the Student’s t-test or Wilcoxon-rank sum test for continuous variables, and the chi-square test or Fisher’s exact test for categorical variables. The efficacy endpoint was the between-group difference in changes from baseline for continuous outcomes (NRS, VAS, NDI, NPQ, EQ-5D-5L, and SF-12) at different time points. Primary analysis was performed using a linear mixed model (LMM), wherein, for fixed effects, baseline values and factors showing significant between-group differences at baseline were included as covariates. Time*group interaction was included to examine differences in time-dependent changes. To compare between-group differences in each outcome throughout the period (treatment and total study periods), we calculated the area under the curve (AUC) for each time point after randomization.
Furthermore, Kaplan–Meier survival analysis was used to compare the proportion of patients that achieved a decrease in neck pain NRS by minimal clinically important difference (MCID) of 2,39 and the curves were compared using the Log rank test. A Cox proportional hazard model was used to compare the hazard ratios.
Due to multiple comparisons, a significance threshold of 0.025 was applied for unadjusted comparison, such as baseline characteristics, and a significance threshold of 0.05 was applied for Bonferroni-adjusted comparison, such as outcome analysis. All statistical analyses were performed using SAS 9.4 (© SAS Institute, Inc., Cary, NC, USA) and R version 4.1.1. (© The R Foundation for Statistical Computing).
Results
Participants
Ninety-three patients underwent screening between April 2022 and May 2023; nine dropped out at the screening stage, and 84 were finally selected and randomized into three groups (Phm-Acu: 29, Acu: 29, and UC: 26). Of these, four participants withdrew their consent during the study period, and 84 participants were included in the ITT analysis (Figure 1).
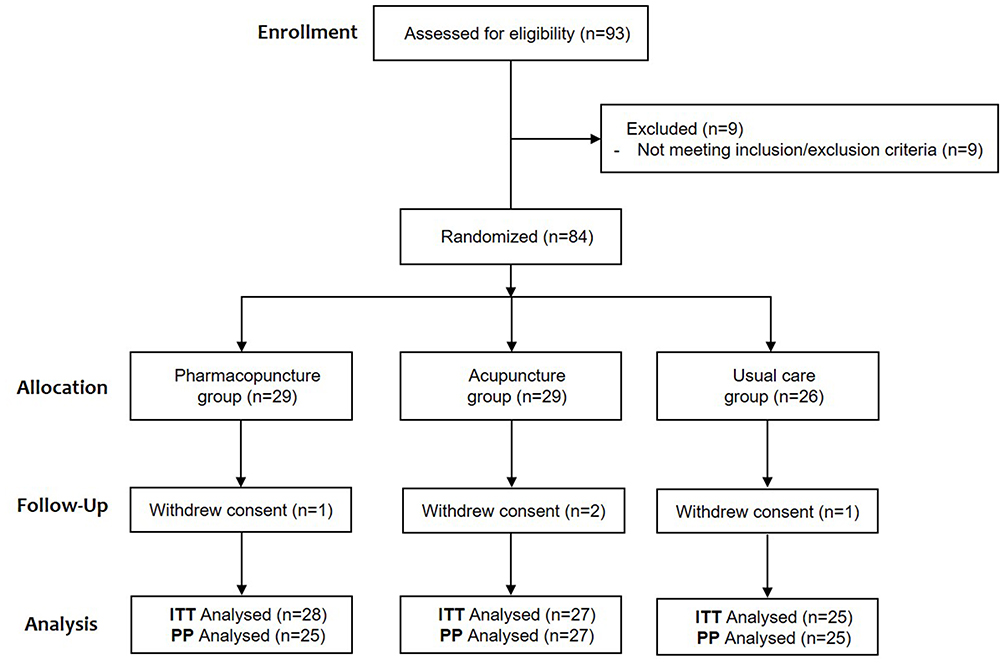 |
Figure 1 Participant flowchart. Abbreviations: ITT, intention-to-treat; PP, per-protocol. |
Participant baseline characteristics are presented in Table 2. No significant differences were observed in baseline characteristics between the groups, considering multiple comparisons with a significance level of 0.025. In the outcome analysis, p-values were adjusted using the Bonferroni correction.
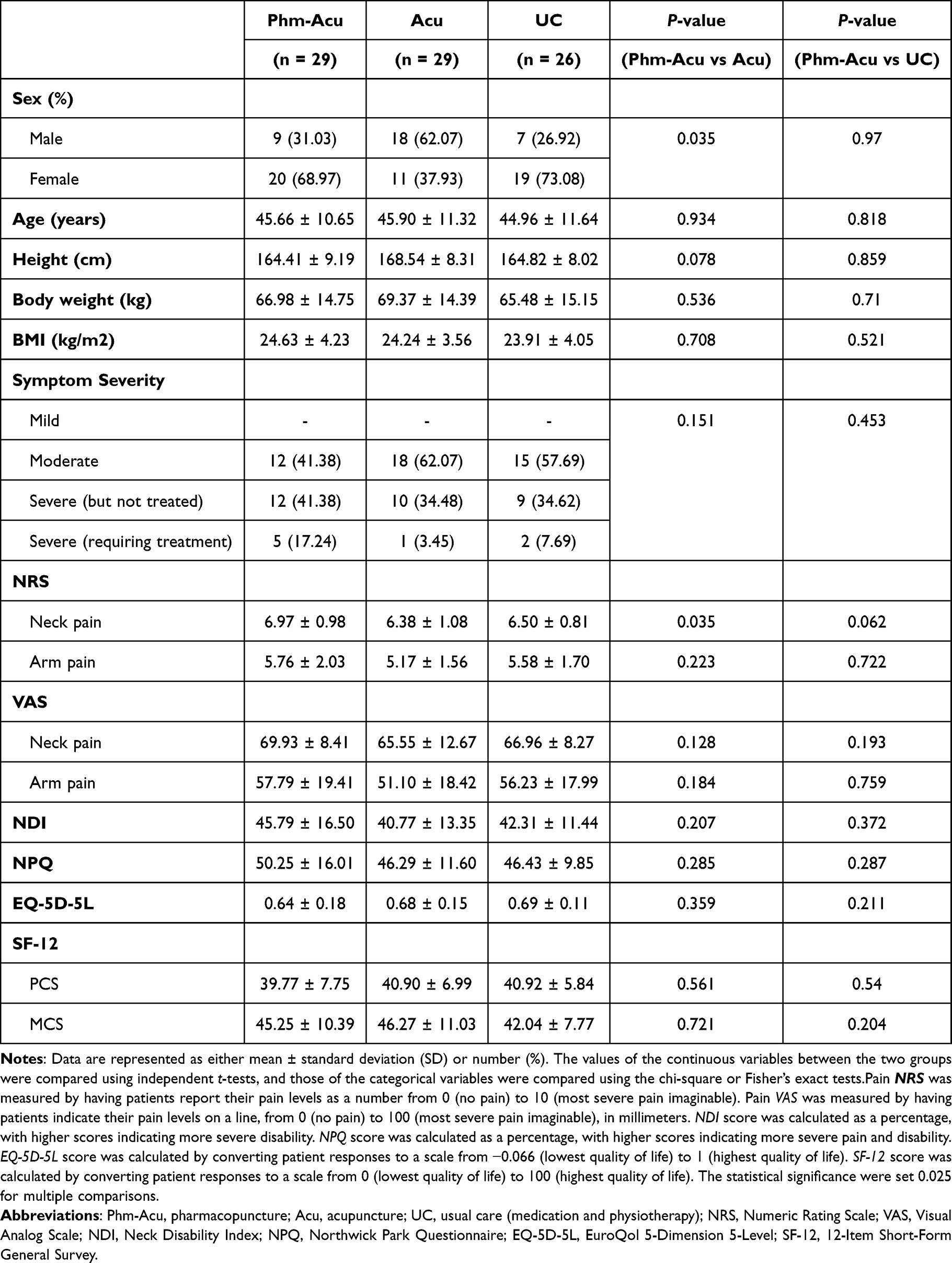 |
Table 2 Participant Baseline Characteristics |
Treatment
Treatment details for the three groups are shown in Supplementary Table 1. As this study was a pragmatic RCT, the treatment methods were not completely unified among the study institutions, and various methods were used. In summary, in the Phm-Acu group, Shinbaro2, Shinbaro3, and Hangryunhaedok-tang were the most frequently used pharmacopuncture, and the GB20, GB21, and cervical hyeopcheok (EX B2) points were the most frequently used acupoints. The average number of treatment sessions and volumes of pharmacopuncture solutions differed slightly based on pharmacopuncture type. Similarly, for the Acu group, GB20, GB21, and GV16 were the most frequently used acupoints; however, a slight difference was observed, as a broader range of acupoints on areas, such as the shoulders and arms, were used. For the UC group, all participants underwent physiotherapy, and the frequently used methods were, in order of use, interferential current therapy, ultrasound, and transcutaneous electrical nerve stimulation. Medications included analgesics and digestive agents and were used for a small number of patients.
Outcomes
Primary Outcome
At week 7 in Table 3, the primary outcome (NRS neck pain score) showed a greater reduction in pain in the Phm-Acu group than that in the UC group (2.73, 95% confidence interval [CI] 1.87–3.59, P < 0.001***) compared with that in the Acu group (1.68, 95% CI 0.84–2.53, P < 0.001***). As depicted in Figure 2, all three groups demonstrated a continuous reduction in neck pain NRS throughout the 7-week treatment period, with the effects largely sustained up to week 25. Notably, the Phm-Acu group exhibited the most significant difference in pain reduction.
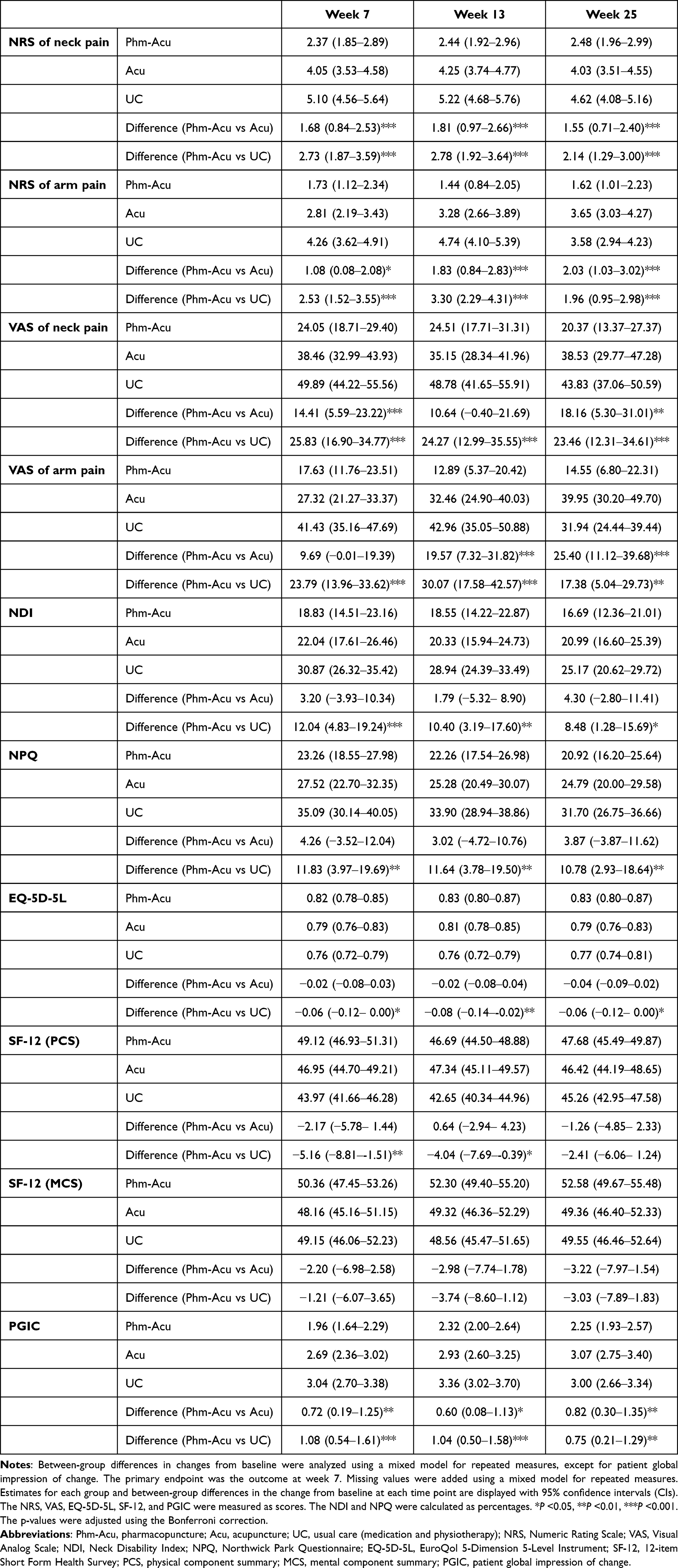 |
Table 3 Primary and Secondary Outcomes After Treatment |
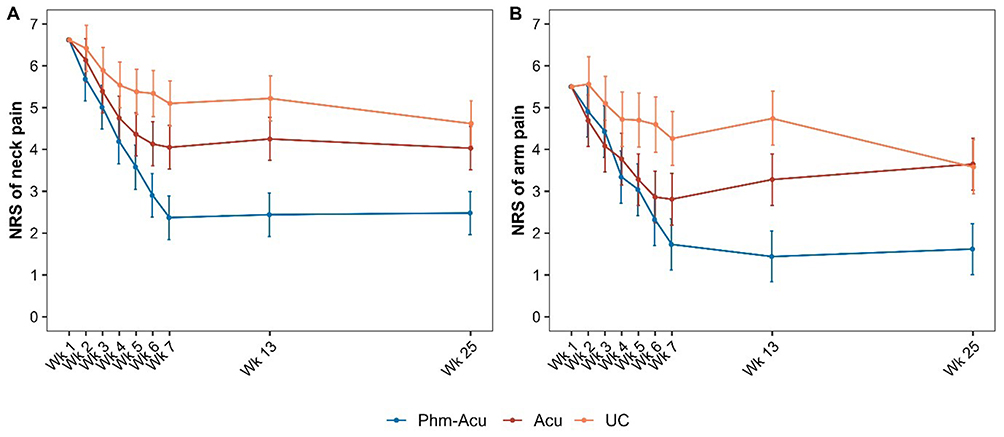 |
Figure 2 Changes in NRS of neck and arm pain over time in LMM analysis (A) Neck pain NRS; (B) arm pain NRS Dots and error bars indicate mean scores and 95% confidence intervals, respectively. Abbreviations: Phm-Acu, pharmacopuncture; Acu, acupuncture; UC, usual care (medication & physiotherapy); NRS, Numeric Rating Scale; LMM, linear mixed model. |
Secondary Outcomes
In the analysis by time point, the Phm-Acu group showed statistically significant improvement in all the outcome measures, including the NRS for arm pain, VAS of neck and arm pain, NDI, NPQ, EQ-5D-5L, SF-12 (PCS), and PGIC, compared to the UC group. These superior effects were maintained through weeks 13 and 25 of the follow-up period, except SF-12. Compared with the Acu group, the Phm-Acu group showed statistically significant improvement in the NRS for arm pain, VAS for neck pain, and PGIC at week 7, with the superior effect persisting through weeks 13 and 25 (Table 3). This overall trend was consistent with the results of the PP and sensitivity analyses (Supplementary Tables 2–4).
In the AUC analysis comparing cumulative outcomes, the Phm-Acu group also showed statistically significant improvements in the NRS and VAS for neck and arm pain, NDI, NPQ, EQ-5D-5L, and SF-12 (PCS) compared with the UC group. Compared with the Acu group, the Phm-Acu group showed statistically significant improvements in the NRS for neck and arm pain and VAS for neck pain (Figure 3, Supplementary Table 5).
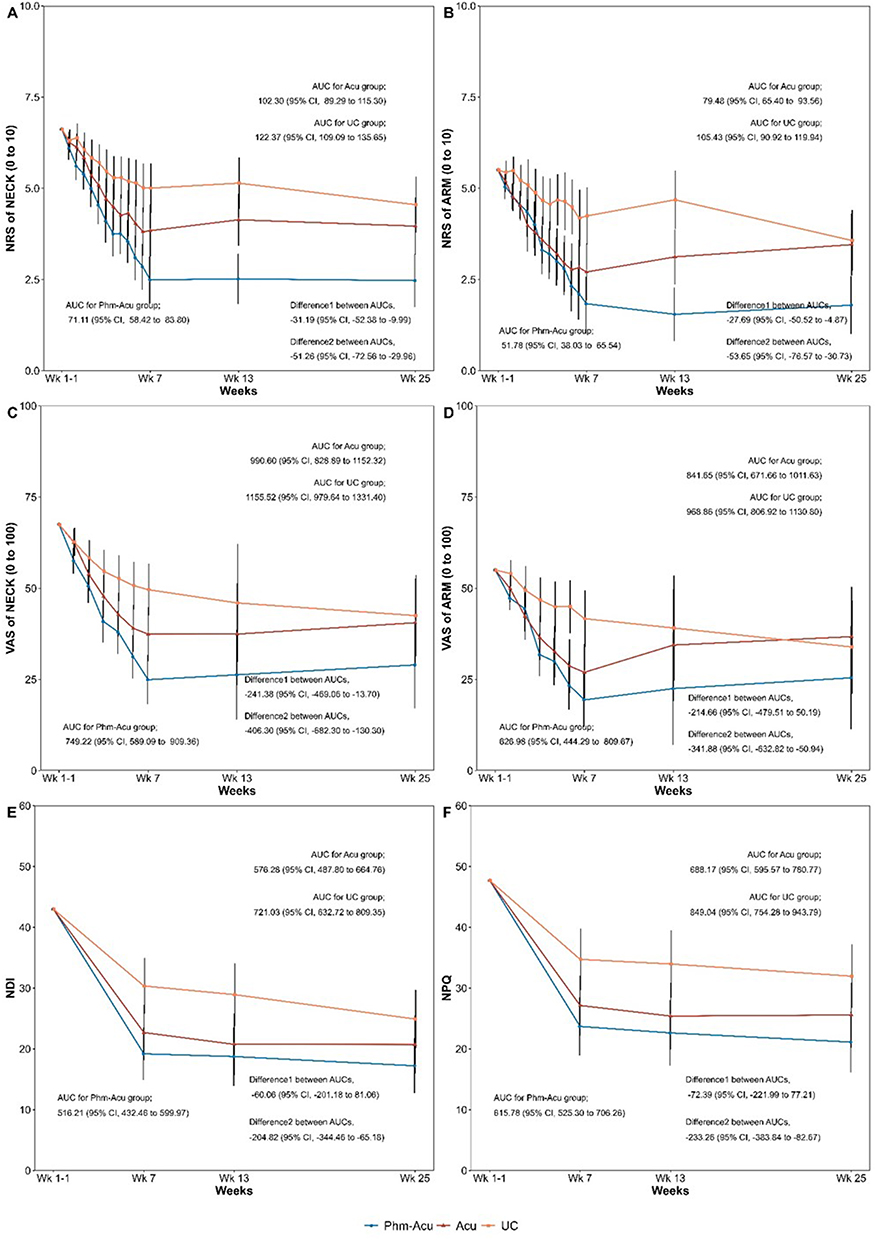 |
Figure 3 Changes in outcomes over time and areas under the curves (A) Neck pain NRS; (B) arm pain NRS; (C) neck pain VAS; (D) arm pain VAS; (E) NDI; (F) NPQ. Dots and error bars indicate mean scores and 95% confidence intervals, respectively. Missing values were added using multiple imputations. Abbreviations: Phm-Acu, pharmacopuncture; Acu, acupuncture; UC, usual care (medication & physiotherapy); NRS, Numeric Rating Scale; VAS, Visual Analog Scale; NDI, Neck Disability Index; NPQ, Northwick Park Questionnaire. |
Survival Analysis
A survival analysis was conducted, where recovery was defined as a decrease in the NRS for neck pain by 2 (MCID) from baseline.39 The analysis revealed that the Phm-Acu group had significantly faster recovery than the UC group (P<0.001 by Log rank test). The median survival times (time to recovery) were 10 (95% CI: 9–18), 22 (95% CI: 15–28), and 31 (95% CI: 21–NA) d in the Phm-Acu, Acu, and UC groups, respectively. When comparing usual care with Korean medicine treatment, the hazard ratio was 3.645 (95% CI: 1.877‒7.079) for the Phm-Acu group versus the UC group and 1.654 (95% CI: 0.88–3.109) for the Acu group versus the UC group (Figure 4). The hazard ratio when the Phm-Acu group was used as the reference are presented in Supplementary Table 6.
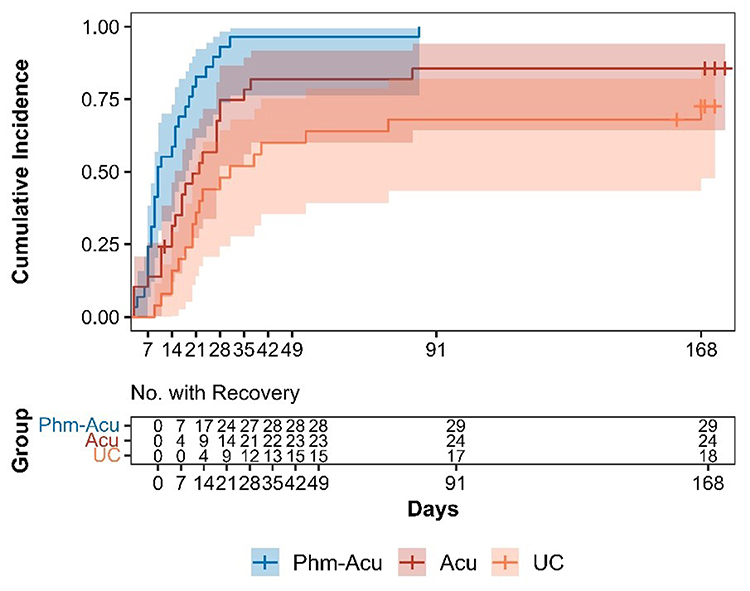 |
Figure 4 Recovery cumulative incidence curves by group A survival analysis based on patient recovery (a decrease of NRS 2 of neck pain [MCID] from baseline) revealed that the Phm-Acu group experienced faster recovery than the UC group (P < 0.001 by Log rank test). The cumulative incidence curves for recovery events were obtained for each group. The median /w to recovery were 10 (95% CI, 9–18), 22 (95% CI, 15–28), and 31 (95% CI, 21–NA) d in the Phm-Acu, Acu, and UC groups, respectively. Shaded areas indicate 95% CIs. Abbreviations: Phm-Acu, pharmacopuncture; Acu, acupuncture; UC, usual care (medication & physiotherapy); NRS, Numeric Rating Scale. |
Safety
Intervention safety was evaluated by recording AEs, including blood test results. In total, 27 cases of AEs occurred in 18 participants (Phm-Acu: 7, Acu: 6, and UC: 5), including cases, such as COVID-19 and dyspepsia. From these, seven cases in four participants were suspected of causality with the intervention. All AEs displayed mild symptoms, such as localized pruritus or fatigue. Apart from one participant who complained of fatigue and was lost to follow-up, the AEs of all other participants resolved (Supplementary Table 7). No serious AEs occurred during the study or follow-up period.
Discussion
The results of this pilot RCT revealed that pharmacopuncture exhibited greater effectiveness than acupuncture and usual care in reducing pain and improving functional disability and the quality of life of patients with CDH. Regarding the primary outcome, the NRS for neck pain at week 7 (the primary endpoint upon completion of all treatment sessions) showed a significantly greater reduction in pain in the Phm-Acu group than that in the UC group, and the superior effects lasted up to weeks 13 and 25 in the follow-up period (P < 0.001). Furthermore, in the time-point analysis, AUC analysis comparing the cumulative outcomes, and survival analysis comparing the recovery rates, the Phm-Acu group showed a faster recovery rate and maintained the reduced pain effect during the follow-up compared with the UC group, suggesting that pharmacopuncture successfully maintained recovery state, which is crucial in the clinical management of patients with CDH. The pain reduction also contributed to improvements in functional disability and quality of life.
Looking into the results obtained from this RCT in detail, the recruited participants comprised more women than men (50 women [59.52%] and 34 men [40.48%]), and the average age was in the mid-40s. Regarding CDH symptom severity, 45 participants had moderate symptoms, and 39 had severe symptoms, indicating that all the participants had moderate or severe CDH symptoms. Regarding efficacy outcomes, from baseline to week 7, the difference in the NRS for neck pain was 4.45±1.99, 2.38±1.76, and 1.42±1.30 in the Phm-Acu, Acu, and UC groups, respectively. Considering that the MCID derived from a previous study investigating changes in neck pain after cervical spine fusion was 2.5,40 the improvement after pharmacopuncture in this study was considerably greater, and acupuncture showed a similar level of improvement to that of surgery. Thus, both interventions (pharmacopuncture and acupuncture) have clinically significant effects.
Regarding usual care, although pain improved after the intervention, compared to the baseline, the improvement fell short of MCID. Similar improvement patterns were observed in the NRS scores of arm pain. Regarding VAS, which is an additional pain outcome measure, the Phm-Acu group showed the most improvement in neck and arm pain between the three group. Although the statistically significant differences in the Phm-Acu group compared to the other groups further support the NRS findings, they should be interpreted with consideration for the rather wide confidence interval of the VAS results.
Considering the changes in these pain outcomes over time, the Phm-Acu group began to show significant differences from the Acu and UC groups at weeks 3–4; thus, a treatment period of 3–4 weeks or longer is appropriate for patients with CDH. In addition, regarding the NDI and NPQ outcome measures assessing how neck pain affects functional disability in daily life, no significant difference was observed between the Phm-Acu and Acu groups; however, the outcomes differed significantly between the Phm-Acu and UC groups. The results indicate that pharmacopuncture and acupuncture achieved meaningful improvements in patients’ daily lives to a similar extent. Regarding health-related quality of life outcomes, no significant difference was observed between the Phm-Acu and Acu groups for EQ-5D-5L and SF-12 (PCS); however, the difference was significant between the Phm-Acu and UC groups. No significant difference was observed between these two groups for SF-12 (MCS). However, considering that the reported MCIDs of SF-12 (PCS) and SF-12 (MCS) were 8.1 and 4.7, respectively, the Phm-Acu group achieved clinically important changes.39 PGIC, an instrument for self-reported evaluation of global perception of improvement after treatment, also indicated more improvement in the Phm-Acu group than that in the Acu and UC groups, and the difference was significant up to week 25. In the AUC analysis comparing the cumulative values of these outcomes from baseline to week 25, the Phm-Acu group showed statistically significant improvement in pain outcome measures (NRS and VAS for neck and arm pain), functional outcome measures (NDI, NPQ), and quality of life outcome measures (EQ-5D-5L and SF-12[PCS]) compared with the UC group. In addition, compared with the Acu group, the Phm-Acu group demonstrated significant improvements in NRS for neck and arm pain and VAS of neck pain, indicating that the superior effects lasted for the entire study period and not just a single time point.
Furthermore, in the survival analysis, the Phm-Acu group showed faster recovery than the other groups, and its hazard ratio versus the UC group was 3.645 (95% CI, 1.877–7.079), indicating a higher probability of the Phm-Acu group achieving recovery than the UC group. However, it needs to be noted that the time-to-recovery variable used in the survival analysis was discontinuous due to weekly outcome assessments, which means it may not fully capture the continuous nature of differences between groups. Nevertheless, the Phm-Acu group achieved faster pain reduction in the early stage, and this superior effect was maintained up to week 25 without relapse, confirming the clinical significance of pharmacopuncture for CDH treatment.
Safety assessment was performed through blood tests taken before and after treatment, with AEs recorded at each visit. Seven AEs were reported in four patients having a possible or stronger causal relationship with the intervention. All AEs involved localized pruritus or redness at the procedure site, and most cases recovered quickly. These results are consistent with the findings of a retrospective analysis and survey on the safety of pharmacopuncture, which reported that the AEs caused by pharmacopuncture were very low and that most were mild.41,42
As reported in many domestic studies, pharmacopuncture therapy is used for treating musculoskeletal disorders in most KM hospitals and clinics; moreover, it is actively applied in clinical practice as the most used treatment modality for CDH.29,43 However, few RCT studies on pharmacopuncture exist in Korea, and the quality of evidence is low in studies that verified the effectiveness of the treatment in other countries.30,44 Referring to the Korean Medicine Clinical Practice Guidelines,44,45 bee venom pharmacopuncture is recommended for lumbar disc herniation, and pharmacopuncture treatment is also recommended for neck pain. However, it is not specifically indicated for CDH. Most studies on pharmacopuncture for CDH treatment are case reviews; moreover, there is a lack of previous studies that can be used as references for this study. Nevertheless, compared with the few existing studies, the pharmacopuncture in one study evaluating pharmacopuncture and physiotherapy for chronic neck pain46 demonstrated improvement with significant differences in the outcome measures of NRS, VAS, NPQ, EQ-5D, and SF-12 PCS, compared with the control group, consistent with the results of our study. In all the outcomes, the degree of the differences between the Phm-Acu and UC groups was larger in this study than that in previous studies [19, 29].
In a meta-analysis of pharmacopuncture for cervical spondylosis treatment,30 the mean difference in the VAS scores in studies comparing pharmacopuncture therapy with acupuncture therapy was 1.79, and a similar difference was confirmed at week 25 in this study. However, as the quality of the studies used in the meta-analysis was low, with a high level of heterogeneity, more follow-up studies should be conducted for meta-analysis with improved quality of evidence.
Meanwhile, as mentioned in the introduction, the effect of pharmacopuncture is synergistic, combining the physical stimulation of acupoints with the chemical stimulation of the pharmacopuncture solution. This multimodal mechanism integration has led to research findings indicating that pharmacopuncture, whether as a monotherapy or part of a combined treatment, is more effective and sustainable compared to normal saline, single acupuncture, or Chuna therapy.47 Furthermore, there are reports suggesting that pharmacopuncture is a more cost-effective treatment from a societal perspective, showing faster improvement in chronic neck pain and long-term effects when compared to existing therapeutic approaches like physical therapy.48 Pharmacopuncture offers immediate effects due to direct injection, and it’s also a convenient treatment option for patients with digestive absorption issues or the elderly, who might find oral medication challenging. These advantages suggest that pharmacopuncture could be a viable conservative treatment alternative to consider before surgery in clinical practice.
To investigate the specific mechanisms of pharmacopuncture, the types of pharmacopuncture solutions used in this study were examined. The most common type was Shinbaro2, which is frequently used for diseases, such as CDH and lumbar spinal stenosis in clinical practice.29,49 The anti-inflammatory and pain-relieving effects of Shinbaro2 pharmacopuncture were confirmed in rat models,50,51 and its main ingredient, GCSB-5, was also reported to have anti-inflammatory, neuroregenerative, and cartilage protection effects.52–54 Following Shinbaro2, the next most frequently used pharmacopuncture types were Shinbaro3 and Hwangryunhaedok-tang. Shinbaro3 uses a single medicinal herb, Harpagophytum procumbens, which has analgesic and anti-inflammatory effects.55 Hwangryunhaedok-tang is a herbal medicine with anti-inflammatory effects that has been commonly used for a long time and is applied not only to musculoskeletal disorders but also to respiratory and dermatological symptoms.56 This pragmatic RCT provided valuable insights into the clinical application of pharmacopuncture. The effectiveness observed in the pharmacopuncture group in this study is consistent with findings from previous studies, suggesting that the reported benefits of pharmacopuncture contributed to the observed outcomes.
However, there are a few considerations regarding pharmacopuncture therapy. The effects of pharmacopuncture can vary somewhat depending on the type of pharmacopuncture, its extraction method (eg, distillation, pressing, ethanol, etc)., and even the same pharmacopuncture solution can be used for various conditions.57 Therefore, future research needs to focus on the mechanisms of action specific to each disease and pharmacopuncture type. Additionally, large-scale multi-center studies on diverse conditions are essential to broaden its application scope. Previous studies have already confirmed efficacy of pharmacopuncture in reducing pain in musculoskeletal disorders, promoting weight loss in obesity, and alleviating cancer-related symptoms.47,58 Furthermore, while Republic of Korea manages the quality control of pharmacopuncture solutions through an external herbal dispensary certification system,59 each country’s food and drug administration (FDA) has different standards. This might make it challenging to precisely replicate the solution production used in other regions.
This study had some limitations. First, the study design did not allow blinding of the participants and the KMD performing the intervention owing to the nature of the intervention and the pragmatic trial design. However, this design reflects real-world clinical settings without reducing generalizability. To minimize bias, careful interpretation of the results is necessary, and efforts were made to reduce other potential biases by ensuring that outcome assessors were blinded to the group allocation position of the participants. Second, as this study was conducted exclusively in KM hospitals, other clinical settings, such as KM clinics, could not be reflected; however, this limitation arose from the need to confirm CDH severity, such as protrusion or above, through CT or MRI scans, differentiating this study from previous studies and improving the quality of evidence with objective and scientific data. Third, this study was an exploratory trial with a small sample size; however, it was conducted as a multi-center trial, reflecting regional and institutional diversity. Consequently, the results could be susceptible to confounding factors and exhibit heterogeneity across institutions, necessitating careful interpretation. Further confirmation is required to determine whether consistent results can be observed in other healthcare settings with larger sample sizes. Based on this study and previous research, future investigations should focus on specifying commonly used pharmacopuncture types (eg, bee venom, Shinbaro, Hwangryunhaedok-tang) or elucidating their mechanisms of action in different diseases, using significantly larger sample sizes. Fourth, there was a slight difference in the recruitment ratio between the groups, likely due to competitive recruitment. This issue should be addressed and improved in future studies.
The significance of this study lies in being the first pragmatic RCT to evaluate the effectiveness of pharmacopuncture for CDH in Korea and confirm its efficacy and safety in KM clinical practice in a well-designed setting. Although this was a relatively small-scale pilot study, we utilized diverse analytical approaches to not only compare change scores at each time point but also to analyze long-term cumulative effects, conducting follow-up observations accordingly. The results of this study contribute to the provision of a conservative treatment option with superior and lasting efficacy for patients with CDH based on quality evidence. Furthermore, as the study verified the relative superiority of pharmacopuncture against other treatment strategies, it may provide useful data and insights for follow-up studies. Future large-scale, prospective trials that include cost-effectiveness evaluations and longitudinal treatment assessments would be beneficial for developing KM clinical practice guidelines, and healthcare policy decisions.
Conclusion
This pilot study demonstrated that pharmacopuncture therapy exhibited greater effectiveness in reducing pain and achieving functional recovery with improved functional outcomes in CDH than acupuncture therapy and usual care (medication and physiotherapy). Therefore, pharmacopuncture therapy can serve as an effective and safe conservative treatment option for CDH. Future studies should include larger sample sizes and a wide range of patient populations to further validate our results and economic evaluation to establish health and societal utility.
Abbreviations
Acu, acupuncture; AEs, adverse events; AUC, area under the curve; CDH, cervical disc herniation; CI, confidence interval; EQ-5D-5L, EuroQol-5-dimension-5-level; KM, Korean medicine; KMDs, Korean medicine doctors; MCID, minimal clinically important difference; MCS, mental component summary; NDI, Neck Disability Index; NPQ, Northwick Park Questionnaire; NRS, Numeric Rating Scale; PCS, physical component summary; PGIC, Patient Global Impression of Change; Phm-Acu, pharmacopuncture; PP, per-protocol; RCT, randomized controlled trial; SF-12, Short Form-12 Health Survey; UC, usual care; VAS, Visual Analog Scale.
Data Sharing Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Ethics Approval and Consent to Participate
This study was conducted in accordance with the Declaration of Helsinki and approved by the Institutional Review Board of the Jaseng Hospital of Korean Medicine (approval number: JASENG 2021-10-016). Informed consent was obtained from all participants before participation in the study.
Author Contributions
All authors made a substantial contribution to the work reported, including the conception, study design, execution, acquisition of data, analysis, and/or interpretation; participated in drafting, revising, or critically reviewing the article; gave final approval of the version to be published; agreed on the journal to which the article was submitted; and accept responsibility for all aspects of the work.
Funding
This study was supported by the Korea Health Industry Development Institute (grant number: RS-2021-KH111842).
Disclosure
The authors declare that they have no competing interests in this work.
References
1. Winkelstein BA, Allen KD, Setton LA. Intervertebral disc herniation: pathophysiology and emerging therapies. The Int Dis. 2014;305–326.
2. Caridi JM, Pumberger M, Hughes AP. Cervical radiculopathy: a review. HSS Journal®. 2011;7(3):265–272. doi:10.1007/s11420-011-9218-z
3. Woods BI, Hilibrand AS. Cervical radiculopathy: epidemiology, etiology, diagnosis, and treatment. Clin Spine Surg. 2015;28(5):E251–E259.
4. Kim Y-K, Kang D, Lee I, Kim S-Y. Differences in the incidence of symptomatic cervical and lumbar disc herniation according to age, sex and national health insurance eligibility: a pilot study on the disease’s association with work. Int J Environ Res Public Health. 2018;15(10):2094. doi:10.3390/ijerph15102094
5. Lee TH, Kim SJ, Lim SM. Prevalence of disc degeneration in asymptomatic Korean subjects. Part 2: cervical spine. J Korean Neurosurg Soc. 2013;53(2):89–95. doi:10.3340/jkns.2013.53.2.89
6. Ksj JGK. 2022 national health insurance statistical yearbook. Health Insurance Review & Assessment Service National Health Insurance Service. 2023.
7. Baird EO, Egorova NN, McAnany SJ, Qureshi SA, Hecht AC, Cho SK. National trends in outpatient surgical treatment of degenerative cervical spine disease. Global Spine J. 2014;4(3):143–149. doi:10.1055/s-0034-1376917
8. Wang MC, Kreuter W, Wolfla CE, Maiman DJ, Deyo RA. Trends and variations in cervical spine surgery in the United States: medicare beneficiaries, 1992 to 2005. Spine. 2009;34(9):955–961. doi:10.1097/BRS.0b013e31819e2fd5
9. Mazas S, Benzakour A, Castelain J-E, Damade C, Ghailane S, Gille O. Cervical disc herniation: which surgery? Int Orthop. 2019;43:761–766. doi:10.1007/s00264-018-4221-3
10. Daniels AH, Riew DK, Yoo J, et al. Adverse events associated with anterior cervical spine surgery. J Am Acad Orthop Surg. 2008;16(12):729–738. doi:10.5435/00124635-200812000-00005
11. Nikolaidis I, Fouyas IP, Sandercock PA, Statham PF. Surgery for cervical radiculopathy or myelopathy. Cochrane Database Syst Rev. 2010. doi:10.1002/14651858.CD001466.pub3
12. Lee YG, Kim SC, Kim SA, Kim MS, Choi E. clinical analysis on the efficacy of stellate ganglion block in the patients with cervical herniated intervertebral disc. J Korean Academy Rehabilitation Med. 2002;26(5):567–570.
13. Lee H-E, Cho J-H, Moon J-Y, et al. The clinical study on 88 patients of cervical disc herniation. J Acupuncture Res. 2008;25(6):145–152.
14. Park J-M, Lee M-J. The effectiveness of oriental medical treatments to symptoms and quality of life in the patients with herniated cervical disc being suggested operation. J Korea CHUNA Manual Med Spine Nerves. 2011;6(1):35–42.
15. Moon J-Y, Song J-H, Lim M-J, et al. magnetic resonance imaging follow-up study on five cases of HIVD-cervical spine patients treated with oriental medical treatment. J Acupuncture Res. 2007;24(5):229–240.
16. Cho N-H, Kim M-R, Jeong H, Yang S-H. A case report of prescribing yanghyeolgeopung-tang (yangxuequfeng-tang) to two patients with cervical disc herniation and headache. J Korea CHUNA Manual Med Spine Nerves. 2011;6(2):33–44.
17. Kim K, Kim HW, Lee GH, Lee GM. The clinical study on effects of acupotomy therapy in patients with cervical herniated intervertebral disc. J Acupuncture Res. 2009;26(1):67–79.
18. K-s L, G-m L. Yeom S-c. A clinical study on the patient of cervical radiculopathy by bee-venom threapy. J Acupuncture Res. 2005;22(3):201–213.
19. Yeom S-C, Kim D-H, Ryu S-W, et al. A clinical study of carthmi-flos herbal acupuncture treatment on cervical disc herniation patients. J Acupuncture Res. 2006;23(3):21–35.
20. Kim S, Kim M, Lim Y, Shin B, Kwon Y, Song Y. A clinical study on the effect of chuna and traction to herniated cervical disc patients. J Korean Med Rehabil. 2001;12:39–48.
21. M-r K, Lee SM, Lee YJ, Ha I. clinical research on pharmacopuncture in Korea: a scoping review. Perspectives on Integrative Medicine. 2023.
22. Lee K-H, Cho -Y-Y, Kim S, Sun S-H. History of research on pharmacopuncture in Korea. J Pharmacopunct. 2016;19(2):101. doi:10.3831/KPI.2016.19.010
23. Ma X, Chen W, Yang -N-N, et al. Potential mechanisms of acupuncture for neuropathic pain based on somatosensory system. Front Neurosci. 2022;16:940343. doi:10.3389/fnins.2022.940343
24. Chen T, Zhang WW, Chu Y-X, Wang Y-Q. Acupuncture for pain management: molecular mechanisms of action. Am J Chin Med. 2020;48(04):793–811. doi:10.1142/S0192415X20500408
25. Kim H, Hong JY, Jeon W-J, Lee J, Lee YJ, Ha I-H. Melittin regulates iron homeostasis and mediates macrophage polarization in rats with lumbar spinal stenosis. Biomed Pharmacother. 2022;156:113776. doi:10.1016/j.biopha.2022.113776
26. Jung M-J, Lee J-H, Yeom S-R, et al. Effects of Ohyaksungi-san (Wuyaoshungi-san) and Jungsongouhyul pharmacopuncture on pain reduction and nerve regeneration after crush injury in rat sciatic nerve. J Korean Med Rehabil. 2009;19(2):51–72.
27. Ryoo D-W, Kim HG, Kim SJ, et al. Systematic review of hominis placenta pharmacopuncture in English and Korean literature. J Acupuncture Res. 2017;34(4):153–158. doi:10.13045/jar.2017.02236
28. S-i T, Takahashi N, Iwama M, Watanabe S, Tamagawa K, Fukui T. Antioxidative collagen-derived peptides in human-placenta extract. Placenta. 2002;23(6):497–502. doi:10.1053/plac.2002.0833
29. Choi HS, Lee YJ, M-r K, et al. Survey of integrative treatment practices of Korean medicine doctors for cervical disc herniation: preliminary data for clinical practice guidelines. Evid Based Complement Alternat Med. 2019;2019(1):2345640. doi:10.1155/2019/2345640
30. Lee S, Shin JS, Lee J, et al. Effectiveness of pharmacopuncture for cervical spondylosis: a systematic review and meta-analysis. Eur J Int Med. 2018;20:154–164. doi:10.1016/j.eujim.2018.05.010
31. Wong JJ, Côté P, Quesnele JJ, Stern PJ, Mior SA. The course and prognostic factors of symptomatic cervical disc herniation with radiculopathy: a systematic review of the literature. Spine J. 2014;14(8):1781–1789. doi:10.1016/j.spinee.2014.02.032
32. Whitehead AL, Julious SA, Cooper CL, Campbell MJ. Estimating the sample size for a pilot randomised trial to minimise the overall trial sample size for the external pilot and main trial for a continuous outcome variable. Stat Methods Med Res. 2016;25(3):1057–1073. doi:10.1177/0962280215588241
33. Vernon H, Mior S. The neck disability index: a study of reliability and validity. J Manipulative Physiol Ther. 1991;14(7):409–415.
34. Leak A, Cooper J, Dyer S, Williams K, Turner-Stokes L, Frank A. The Northwick Park Neck Pain Questionnaire, devised to measure neck pain and disability. Rheumatology. 1994;33(5):469–474. doi:10.1093/rheumatology/33.5.469
35. Lee K-W, Seo H-D, Jung K-S, Kim S-H, Chung Y-J. Reliability and validity of Korean version Northwick Park Neck Pain Questionnaire in neck pain patients. Phys Ther Korea. 2010;17(3):68–76.
36. Kim S-H, Jo M-W, Ahn J, Ock M, Shin S, Park J. Assessment of psychometric properties of the Korean SF-12 v2 in the general population. BMC Public Health. 2014;14:1–7. doi:10.1186/1471-2458-14-1086
37. Kim S-H, Ahn J, Ock M, et al. The EQ-5D-5L valuation study in Korea. Qual Life Res. 2016;25:1845–1852. doi:10.1007/s11136-015-1205-2
38. Spilker B. Guide to Clinical Trials. Raven Press; 1991.
39. Parker SL, Godil SS, Shau DN, Mendenhall SK, McGirt MJ. Assessment of the minimum clinically important difference in pain, disability, and quality of life after anterior cervical discectomy and fusion. J Neurosurg Spine. 2013;18(2):154–160. doi:10.3171/2012.10.SPINE12312
40. Carreon LY, Glassman SD, Campbell MJ, Anderson PA. Neck Disability Index, short form-36 physical component summary, and pain scales for neck and arm pain: the minimum clinically important difference and substantial clinical benefit after cervical spine fusion. Spine J. 2010;10(6):469–474. doi:10.1016/j.spinee.2010.02.007
41. Kim M-R, Shin J-S, Lee J, et al. Safety of acupuncture and pharmacopuncture in 80,523 musculoskeletal disorder patients: a retrospective review of internal safety inspection and electronic medical records. Medicine. 2016;95(18):e3635. doi:10.1097/MD.0000000000003635
42. Hong, Eui HK K-E. Analysis study of survey for safety and efficacy of pharmacopuncture. J Pharmacopunct. 2010;13(3):91–102. doi:10.3831/KPI.2010.13.3.091
43. Lee YJ, Shin J-S, Lee J, et al. Usage report of pharmacopuncture in musculoskeletal patients visiting Korean medicine hospitals and clinics in Korea. BMC Complement Altern Med. 2016;16:1–8. doi:10.1186/s12906-016-1288-5
44. Korean Medicine Clinical Practice Guideline for Neck Pain. Guideline center for Korean Medicine; 2021.
45. Mm SK. Herniation of Lumbar Disk: Clinical Practice Guideline of Korean Medicine. Koonja Publishing; 2021.
46. Park K-S, Kim S, Kim C, et al. A comparative study of the effectiveness of pharmacopuncture therapy for chronic neck pain: a pragmatic, randomized, controlled trial. J Clin Med. 2021;11(1):12. doi:10.3390/jcm11010012
47. Park J, Lee H, Shin B-C, Lee MS, Kim B, Kim JI. Pharmacopuncture in Korea: a Systematic Review and Meta‐Analysis of Randomized Controlled Trials. Evid Based Complement Alternat Med. 2016;2016(1):4683121. doi:10.1155/2016/4683121
48. Kim D, Kim ES, Song HJ, et al. An economic evaluation of pharmacopuncture versus usual care for chronic neck pain: a pragmatic randomized controlled trial. BMC Health Serv Res. 2023;23(1):1286. doi:10.1186/s12913-023-10325-w
49. Lee YJ, Shin J-S, Lee J, et al. Survey of integrative lumbar spinal stenosis treatment in Korean medicine doctors: preliminary data for clinical practice guidelines. BMC Complement Altern Med. 2017;17:1–12. doi:10.1186/s12906-017-1942-6
50. Park SH, Hong J-Y, Kim WK, et al. Effects of SHINBARO2 on rat models of lumbar spinal stenosis. Mediators Inflamm. 2019;2019(1):7651470. doi:10.1155/2019/7651470
51. Kim WK, Shin J-S, Lee J, et al. Effects of the administration of Shinbaro 2 in a rat lumbar disk herniation model. Front Neurol. 2023;14:1044724. doi:10.3389/fneur.2023.1044724
52. Chung H-J, Lee H-S, Shin J-S, et al. Modulation of acute and chronic inflammatory processes by a traditional medicine preparation GCSB-5 both in vitro and in vivo animal models. J Ethnopharmacol. 2010;130(3):450–459. doi:10.1016/j.jep.2010.05.020
53. Kim J-K, Park S-W, Kang J-W, et al. Effect of GCSB‐5, a herbal formulation, on monosodium iodoacetate‐induced osteoarthritis in rats. Evid Based Complement Alternat Med. 2012;2012(1):730907. doi:10.1155/2012/730907
54. Kim T-H, Yoon S-J, Lee W-C, et al. Protective effect of GCSB-5, an herbal preparation, against peripheral nerve injury in rats. J Ethnopharmacol. 2011;136(2):297–304. doi:10.1016/j.jep.2011.04.037
55. McGregor G, Fiebich B, Wartenberg A, Brien S, Lewith G, Wegener T. Devil’s claw (Harpagophytum procumbens): an anti-inflammatory herb with therapeutic potential. Phytochem Rev. 2005;4:47–53. doi:10.1007/s11101-004-2374-8
56. Lee S-H, Kim S-J. An intensive review on clinical thesis about Hwangryunhaedok-tang pharmacopuncture treatment: focused on case reports and controlled studies in Korean Academic Journals. J Korean Med Rehabil. 2019;29(2):171–188. doi:10.18325/jkmr.2019.29.2.171
57. Lee I-S, Kang KS, Kim S-Y. Panax ginseng pharmacopuncture: current status of the research and future challenges. Biomolecules. 2019;10(1):33. doi:10.3390/biom10010033
58. Cheon S, Zhang X, Lee I-S, Cho S-H, Chae Y, Lee H. Pharmacopuncture for cancer care: a systematic review. Evid Based Complement Alternat Med. 2014;2014(1):804746. doi:10.1155/2014/804746
59. Han J-E, Park M, Park JH, Oh D, Kim KH, Sung S-H. Quality control of pharmacopuncture: a comparative study of good manufacturing practice and external herbal dispensary standards. J Pharmacopunct. 2021;24(2):59. doi:10.3831/KPI.2021.24.2.59
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.