Back to Journals » Risk Management and Healthcare Policy » Volume 16
Potentially Inappropriate Medication Dispensing in Outpatients: Comparison of Different Measurement Approaches
Authors Eggli Y ![]() , Halfon P, Zeukeng MJ
, Halfon P, Zeukeng MJ ![]() , Kherad O, Schaller P, Raetzo MA, Klay MF, Favre BM, Schaller D, Marti J
, Kherad O, Schaller P, Raetzo MA, Klay MF, Favre BM, Schaller D, Marti J
Received 20 July 2023
Accepted for publication 13 October 2023
Published 23 November 2023 Volume 2023:16 Pages 2565—2578
DOI https://doi.org/10.2147/RMHP.S427516
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Gulsum Kaya
Yves Eggli,1 Patricia Halfon,1 Minette-Joëlle Zeukeng,2 Omar Kherad,3 Philippe Schaller,2 Marc-André Raetzo,2 Michael Frédéric Klay,2 Benoît Marc Favre,2 Dorian Schaller,2 Joachim Marti1
1Centre for Primary Care and Public Health (Unisanté), University of Lausanne, Lausanne, Switzerland; 2Réseau Delta, Lancy, Switzerland; 3Internal Medicine Department, La Tour Hospital and University of Geneva, Geneva, Switzerland
Correspondence: Yves Eggli, Centre for Primary Care and Public Health (Unisanté), ECOSAN, Route de la Corniche 10, Lausanne, 1010, Switzerland, Tel +41 21 314 33 83, Email [email protected]
Purpose of the Research: This paper aims at comparing different approaches to measure potentially inappropriate medication (PIM) with routinely collected data on prescriptions, patient age institutionalization status (ie in nursing home or in the community). A secondary objective is to measure the rate and prevalence of PIM dispensing and to identify problematic practices in Switzerland.
Material and Methods: The studied population includes about 90,000 insured over 17 years old from a Swiss health maintenance organization in 2019 and 2020. We computed and compared the number of PIM per patient for Beers criteria, Priscus list, Laroche, NORGEP and Prescrire approaches. We also created a composite indicator that accounts for the specificities of the Swiss context (adaptation to the Swiss drugs’ market, recommendations in force related to sleeping pills, anxiolytics and NSAIDs). We also stratified the analysis per physician, including initiation and cessation of PIM prescription.
Results: Our comparison revealed similarities between the approaches, but also that each of them had specific gaps that provides further motivation for the development of a composite approach. PIM rate was particularly high for sleeping pills, anxiolytics, NSAIDs, even when analyses were limited to chronic use. Drugs with anticholinergic effect were also frequently prescribed. Based on our composite indicator, 27% of insured over 64 years old received at least one PIM in 2020, and 8% received more than one. Our analyses also reveal that for sleeping pills and anxiolytics, half of the volume (or prevalence?) occurs in the < 65 population. We observed strong variations between physicians and a significant proportion of new users among patients with PIM.
Conclusion: Our results show that PIMs prescribing is very frequent in Switzerland and is driven mostly by a few drug categories. There is important physician variation in PIM prescribing that warrants the development of intervention targeted at high PIM-prescribers.
Keywords: low-value care, inappropriateness, medication, outpatients, Switzerland
Introduction
Countries generally authorize market access for new medicines if the treatment demonstrates its efficacy, without generating disproportionate undesirable effects.1–3 Recommendations can then restrict prescription if the benefit-risk balance for specific indications and/or patient groups is not favorable, ie if the medication is unnecessary or dangerous. The elderly population (>64 years old) is particularly at risk of using inappropriate treatments, as they are more vulnerable to adverse drug events. In addition, polypharmacy, the concurrent use of multiple medications, which increases the risk of interactions, is common in this population, costly and harmful.4 Some types of medication, such as anxiolytics or sleeping pills, might also be inappropriate in younger patients especially in chronic use. Many implicit (ie, judgment-based) and explicit (ie, criterion-based) approaches are available to identify potentially inappropriate medications (PIM) and provide reference guides for comprehensive medication reviews.5,6
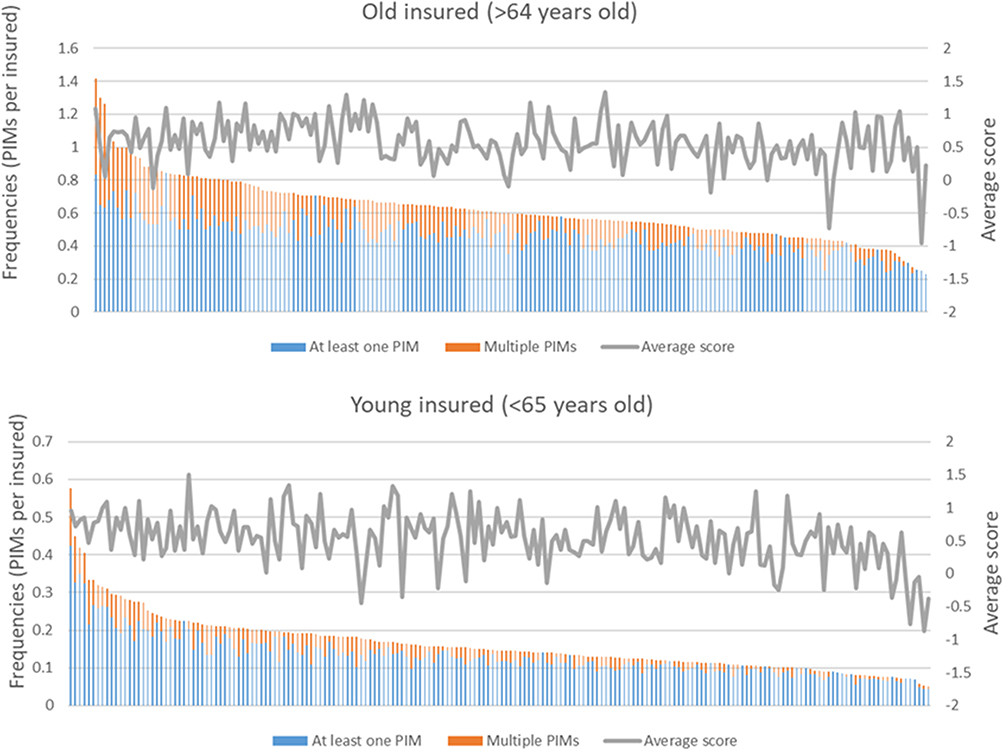 |
Figure 1 Variations in PIM frequencies and scores among 190 physicians with at least 10 eligible insured. |
Implicit approaches rely on expert professional judgement, are patient-oriented, and address entire medication regimen. These instruments are time consuming to implement and might have a low reliability.7 For instance, the Medication Appropriateness Index8,9 provides a comprehensive list of criteria with corresponding scores to assess the appropriateness of drugs prescriptions. Such tools can be useful to support medical decision-making,10 but they require in-depth information on the clinical context. Since data on diagnoses or labs results are not routinely collected, those tools are not suitable to build monitoring indicators.
Explicit approaches have been developed from literature reviews, expert opinions, and consensus techniques. Based on lists of drugs, drug-classes, and dosages known to cause harmful effects, such approaches are easy to implement, not costly, and need regular updates.
To date, few studies investigated PIM dispensing in Switzerland. For instance, an insurance company used Beers and Priscus lists independently to raise awareness of doctors about inappropriate prescriptions of drugs.11 They found a prevalence of 22.5% of PIM in a managed care sample (N = 49,668)12 and of 79% among nursing homes residents (N = 72,106).13 Another Swiss study, combining Beers and NORGEP approaches found that 30% of consumed drugs were potentially inappropriate among nursing home residents.14
In this paper, we retained five approaches: Beers criteria, Priscus list, Laroche, NORGEP, and Prescrire approaches (references in the Method section) because they rely on explicitly listed substances, which is a necessary condition to automatize computation. Our source of information in the Swiss system is insurance claims data. Thus, another rationale for the use these tools is that they do not require information on comorbidities (except, to a limited extent, for the Beers criteria). PIM-approaches relying on clinical and physiological criteria,15–19 were not retained, as such information (hypokalaemia, hypertension, history of myocardial infarction, renal failure for instance) are is rarely available in claims data.
The aim of our paper consists in assessing and comparing different potentially inappropriate medication (PIM) measurement approaches based on routinely available data on drugs dispensed to more than 90,000 individuals enrolled in an Health Maintenance Organization (HMO) plan in Switzerland. Our analysis was conducted in light of the Swiss context (ie product availability, local guidelines, etc.), potentially justifying the design of an adapted tool. A secondary objective was to measure the rate and prevalence of PIM and to identify problematic practices (differences between physicians, initiating or stopping PIM).
Methods
Study Population and Setting
In Switzerland, the population has a mandatory basic health care insurance package. Insured can lower their premium by choosing an HMO contract with a primary care physician as gatekeeper. The Delta Network is such an HMO, established in 1992 in the French-speaking part of Switzerland (canton of Geneva, Vaud, Fribourg, Valais, and Jura), proposing a network of 700 gate keepers (primary care physicians).20 The Delta Network is available in for enrollees of any health insurance company. We focused on enrollees from Geneva and Vaud that represents 95% of Delta enrollees. In 2019 and 2020, more than 250,000 individuals were enrolled in the Delta Network. Delta network gatekeeping physicians (GP), all paid fee-for-service, agreed to be accountable for the quality, cost, and overall care of HMO beneficiaries. GP committed to a smart medicine philosophy, ie “doing only necessary care, but all necessary care, based on both scientific medicine and patients’ preferences”.
Our setting included 91,739 insured over 17 years old contracting with Swiss insurance companies, enrolled in the Delta network in 2020, and having received at least one drug with oral route of administration in 2020 (insured <18 or without those drugs prescriptions were excluded). To analyze the frequency of PIM stopping or initiating, we also analyzed the data of 85,894 insured from the year 2019.
The data used for this research were anonymous, without any possibility to identify patients (no birth date or precise residence information for instance). Patient-level information collected included anonymous identifiers, age (years), gender, canton of residence, year of insurance contract (2019, 2020), an anonymous identifier of the primary care physician, and data on medication, products code, and the quantity of delivered packages. From the medication data, the Delta network derived defined daily dose (DDDs) by Anatomic Therapeutic Chemical codes (ATC), the classification system of the World Health Organization. We created a flag for PIM for each approach as described below (ie Beers, Priscus, Laroche, etc.).
The analysis was limited to all patients receiving oral drugs prescriptions. Anesthetic and healing products, contraceptive, disinfectant, antiseptic, diagnostic tests, nutriments, and vaccines were not considered as drugs and therefore excluded. We also excluded homeopathy and herbal medicine, because they were not included in most PIM lists studied here.
PIM Criteria
All approaches relied on a list of substances to be avoided, sometimes for specific conditions (age, institutionalization status, Table 1). According to the Swiss drug market specificities, we excluded some substances (not included in the PIM list, see Appendix A).
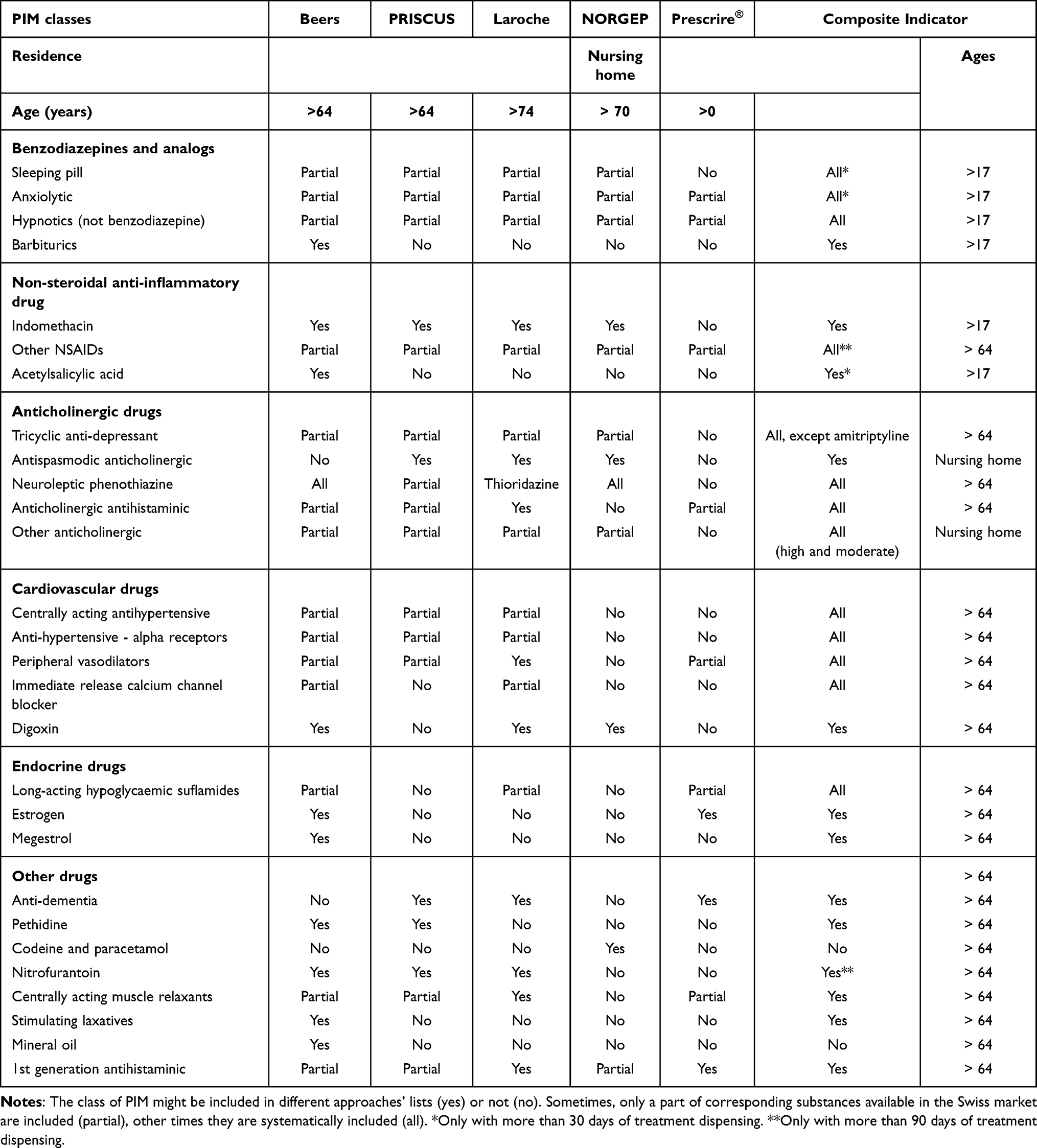 |
Table 1 Comparison of the Different Approaches, by Class of PIM |
Beers Criteria
We used the American Society of Geriatrics 2019 updated list21 for patients older than 64 years. Those recommendations included substances that should be avoided, sometimes with specific criteria (eg, treatment duration, minimal dose). It provided for each criterion the quality of the evidence and the strength of recommendations and was also used in several European countries. If the recommendation was to avoid chronic use only, we applied the condition of at least 90 days of treatment (deduced from DDD) during the year.
Priscus List
A similar approach, named Priscus, was developed in Germany, with a simple list of substances to avoid in patients 65 years and over.22 Drugs combining several substances with at least one included in Priscus list were also considered as PIM.14
Laroche Criteria
In France, Laroche et al developed a list of drugs to be avoided, targeting people aged 75 and over, based on a consensus panel.23 The goal of the list was to propose safer or more effective therapeutic alternatives, with a particular attention to drug interactions.
This approach was more challenging to implement, due to a lack of clarity in its description. To obtain explicit ATC codes, we used all substances with a high or moderate anticholinergic burden from a recent review of the literature on this topic24 (34th Laroche criteria). We had also to specify drugs considered as anticholinesterase, namely: tacrine, donepezil, rivastigmine, galantamine, ipidacrine, neostigmine, pyridostigmine, distigmine, ambenonium and associations with one the listed substances.
We used the dates of delivery as first day of treatment, DDD and prescribed doses to estimate the duration of treatment (last day of treatment) to identify prescriptions with overlapping periods. Doing this, we assumed that patients took the prescribed drugs regularly and completely.
NORGEP-NH Criteria
In Norway, another list of drugs to avoid in people over 70 in nursing home was developed, paying some attention to drug interactions.25 It also identifies PIMs based on simultaneous use of other drugs.17 Deprescribing criteria including biphosphonates, statins, antidepressants, were not implemented, since the recommendation was only to reassess regularly their use.
The same rules than Laroche were applied to detect concomitant use of drugs. We computed all interactions, most of them being of first order (criteria 12–25) and one of second order with a triple interaction (criteria 26).
Prescrire List
In France, a collective of independent pharmacists and physicians established a list of drugs, whose prescriptions should be avoided regardless of the age of the patients.26 They developed a list based on a continuous review of the literature during the last 15 years (Prescrire review), claiming independence from pharmaceutical companies. They did not formally consider them as PIMs, but we examined this approach to understand similarities and differences with the other approaches.
We considered all medications that the Journal Prescrire recommends avoiding. Of note, more than half of the substances advised against were not present on the Swiss market in 2020.
Quantitative Analysis and Outcomes
To build indicators on the quality of drug prescribing, it is necessary to define numerators (occurrence of PIM) and denominators (eligible population).
A PIM corresponds to at least one inappropriate prescription for a given ATC code during the year. Some patients may therefore have several PIM at the same time. The rationale of this definition is that PIM of different ATC codes correspond to independent decisions. The rate of PIM is the sum of the prevalence of PIM (at least one PIM par patient) and of the frequency of multiple PIM per patient.
We used two types of numerators, one static, counting the number of PIM per patient (PIM rate), and another one as a score that takes into account the dynamic of prescriptions.
A primary outcome was the rate of PIM over one year (2020) according to each approach in the delta network, categorized by age, computed by counting PIMs of different ATC codes and dividing this sum by the 2020 eligible population. We also computed the proportion of the eligible population receiving at least one drug prescription (prevalence). We computed PIM rates globally and per physician to analyze its variation among prescribers.
As secondary outcome we built a score to reflect changes in prescription patterns between 2019 and 2020. This score is based on points assigned to various situations, with higher points reflecting poorer prescribing and less physician effort to limit PIM. Initiating a new PIM between 2019 and 2020 is assigned 2 points. The most favorable situation (−2) consists in PIM discontinuation between years. One point is attributed if a PIM was maintained during both years. If no PIM was prescribed over both years, the score does not change. The proposed score considers that it is more difficult to stop a PIM (−2) than not to start such a prescription (0). We computed scores among insured eligible for the two years (2019 and 2020) and identified PIM with our composite approach.
Despite higher rates among elderly, we did not standardize these per GPs’ indicators for age because we consider that adverse events are potentially at least as harmful among old people than younger individuals and that potential interactions are more frequent in the elderly (more polypharmacy). In other words, we consider that doctors must be even more careful with elderly patients, even if it is perhaps more challenging to avoid PIMs among them.
Results
Comparison of PIM Lists and Creation of a Composite PIM Indicator
The comparison of the various approaches showed that most relied on common PIM classes (Table 1), but often with partial lists of ATC codes, despite similar undesirable effects. We observed that the various lists included similar classes of drugs (sleeping pills, anxiolytics, non-steroidal anti-inflammatory drugs (NSAIDs), anticholinergic drugs, etc.,) but also that the list of ATC codes were different without medical reasons. Thus, we built a composite indicator to include them systematically (see Appendix B for details and rationale). According to usual recommendations in place in Switzerland, we considered sleeping pills, anxiolytics, and NSAIDs as PIM only if they were used for >90 days (chronic use). A third difficulty was related to the justification of the limitations (age, nursing home residence, etc.). We considered for instance that chronic use of sleeping pills and anxiolytics should be avoided in the same way among young and old people, because the problem of addiction does not depend on age. Consequently, the composite indicator was extended to people under 65 for benzodiazepines and analogs, indomethacin and acetylsalicylic acid (chronic use only). We included most medications of the Prescrire list as it overlapped quite well with the other lists. However, we excluded from our composite list more controversial substances included in Prescrire, such as nasal decongestants, combinations of hypoglycaemics, renin inhibitors, other anti-depressants (see Appendix C). We analyzed them separately but did not include them in the composite approach.
Frequency of PIM
Table 2 gives the frequency of PIM according to the different approaches, with the corresponding eligible populations. We observe the same frequency of PIM in 2020 according to the criteria of Beers and Priscus (0.360 and 0.334 PIM/patient respectively), even if targeted substances are not identical. The population at risk was the same, 16,927 eligible insured for both methods, corresponding to the population aged 65 and over having received at least one prescription for oral medication. Laroche’s approach targets about the half of this population (8705 insured aged 75 and over), while the NORGEP method addressed an even smaller eligible population (1583 nursing homes residents, aged 70 and over). For these last two approaches, the frequency is 0.907 and 0.848 PIM/patient respectively. The Prescrire approach had the highest proportion of PIM, especially among the youngest.
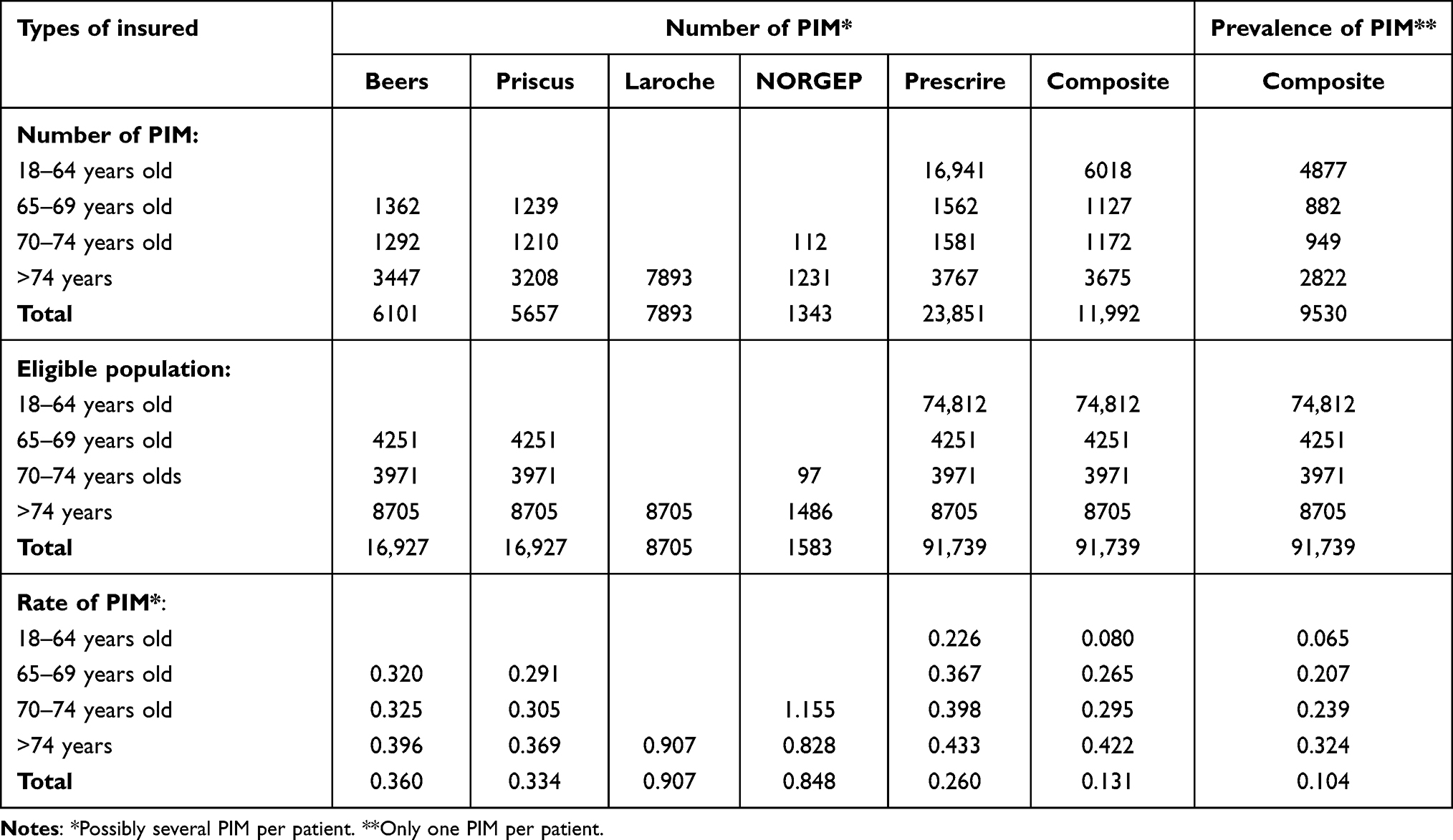 |
Table 2 Occurrence of PIM (One per ATC Code) per Eligible Insured (2020) |
The global prevalence measured with the composite approach was about one in 10 enrollees (10.4% with at least a PIM) with 2.7% having multiple PIM, leading to the global PIM rate of 0.131 (Table 2 people above 18 years old). Considering only enrollees over 64 years, the prevalence was 27.5% (at least a PIM) with 8% received more than one (computed from Table 2 outcomes) leading to a global PIM rate of 0.353.
With the composite indicator, PIM rates increased with the age of patients, with a prevalence of 32.4% among older patients (>74 years old). However, the composite approach, extended to younger people, show that the half of PIM occurred among people under 65 years old, which include much more eligible people.
The detailed analysis by PIM class makes it possible to compare the different approaches for a better understanding of their specificities (Table 3).
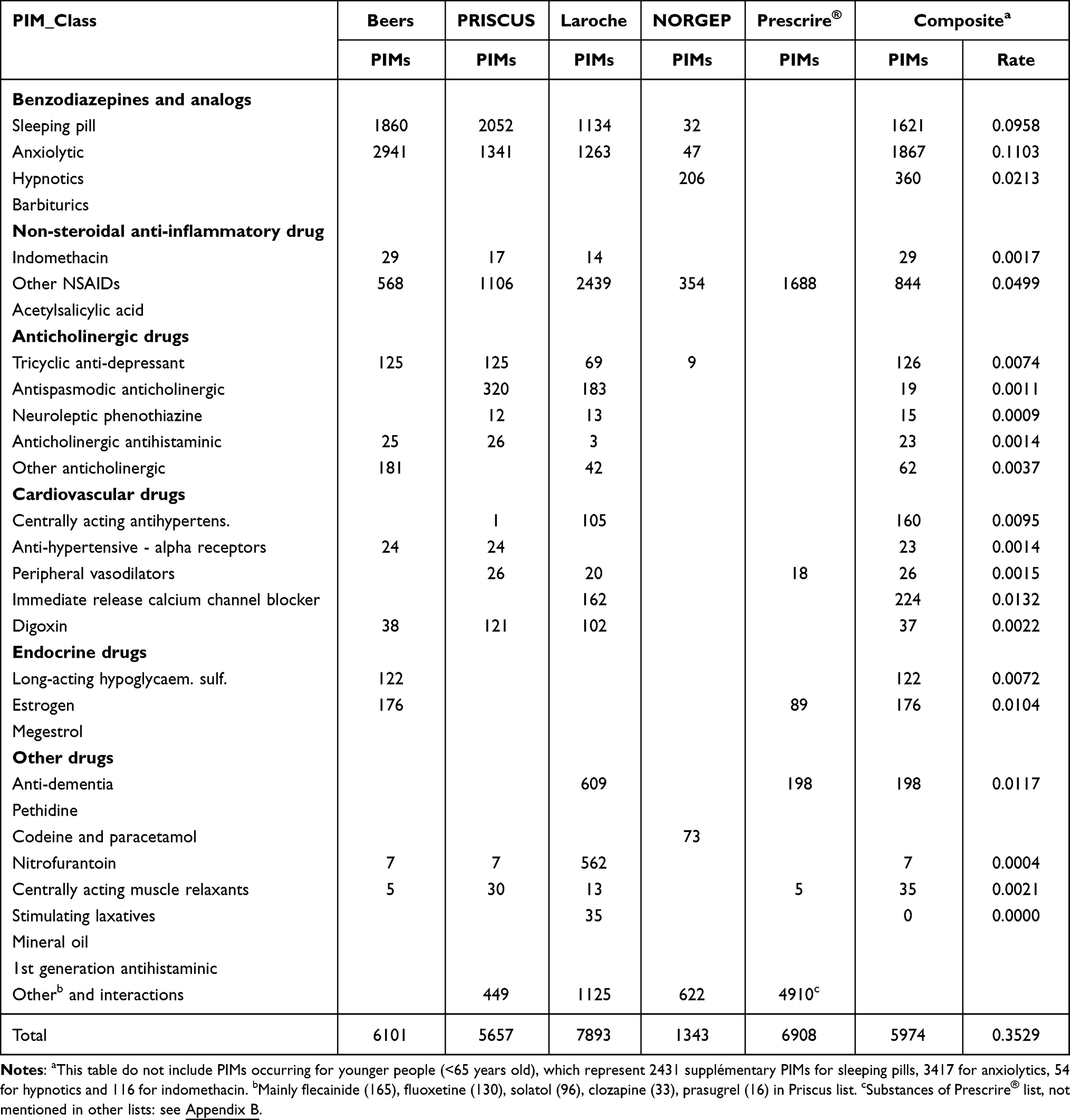 |
Table 3 Detailed Occurrence of PIMs (One per ATC Code) per Eligible Insured (2020, >64 Years Old) |
Globally, the composite indicator indicates a frequency of 0.35 PIM par patient among patients older than 64 years old. Sleeping pills, anxiolytics, and hypnotics represented almost the half of those cases. No consumption of barbiturate was identified as this drug is not on the market. The only hypnotics delivered was clometiazole.
Non-steroidal anti-inflammatory represented another frequent type of PIM, especially in the Laroche approach; limiting PIMs to chronic use in the composite approach reduced significantly their prevalence. Inappropriate prescriptions of acetylsalicylic acid (chronic intake > 325 mg) were not observed.
PIM related to cardiovascular, hormonal or anticholinergic drugs are relatively rare. Several classes of PIM are never prescribed in Switzerland as corresponding substances (pethidine, first generation antihistamines for example) were not available in the Swiss market. PIM related to anti-dementia drugs were relatively rare (rate of 0.01).
A large part of the PIM according to the Laroche’s approach concerned the delivery of nitrofurantoin. Such PIM were much less frequent in the composite approach because only chronic consumption (more than 90 days per year) is considered problematic.
Initiating and Stopping PIM Dispensation
PIM scores are given in Table 4. Most PIM (6782) occurred during both 2019 and 2020 years. About a third of PIM were stopped in 2020 [=3449/3449+6782]. A little bit more was initiated in 2020 (3751), mostly driven by sleeping pills and anxiolytics (see column “excess”).
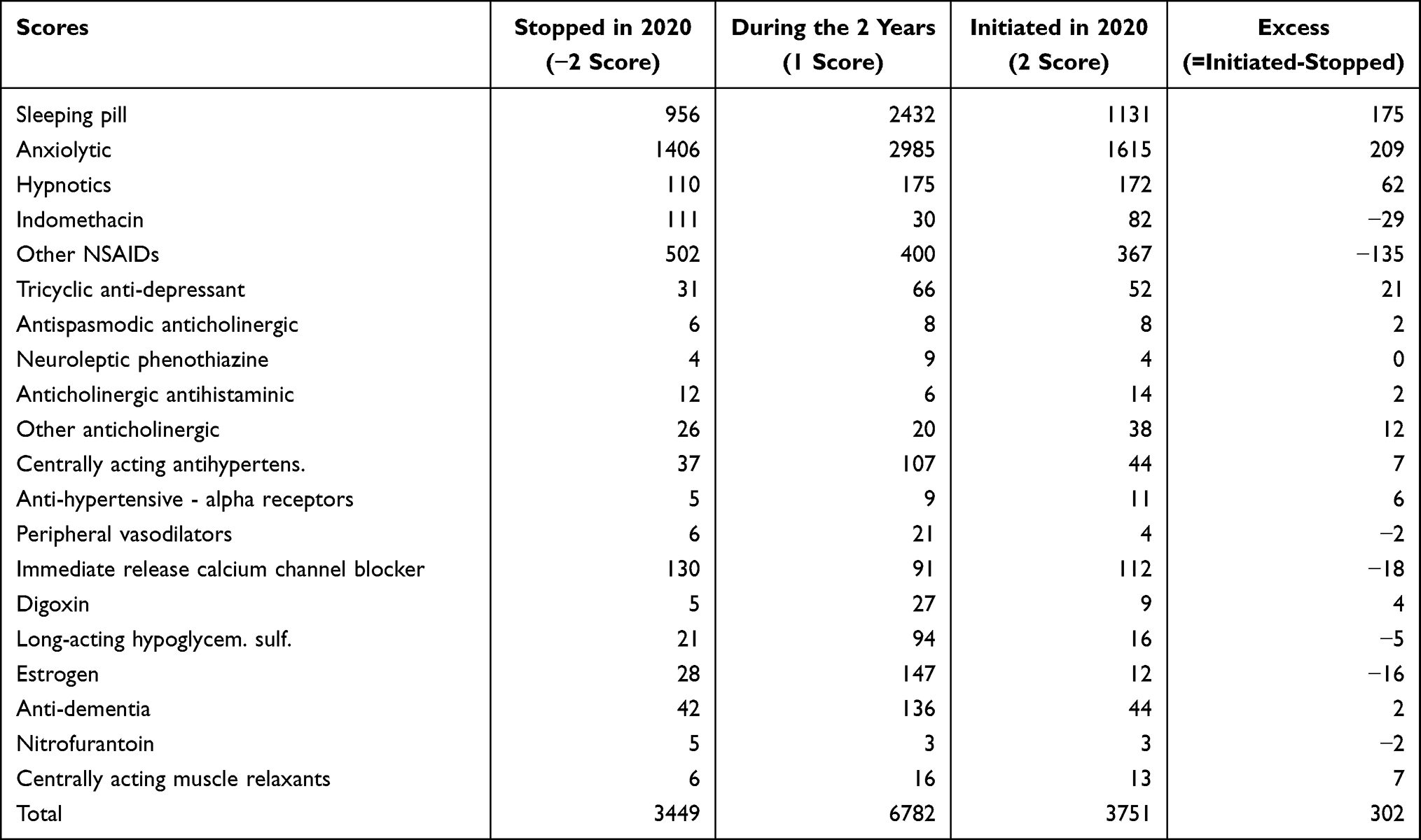 |
Table 4 PIM Scores |
There is a great variability in the frequency of PIM dispensing among physicians (Figure 1). Physicians dispensing a lot of PIM are set on the left with about 1.0 PIM per patient in elderly, and the lowest PIM prescriber on the right (0.25 PIM par patient). Only physicians with at least 10 eligible enrollees are included in the figure, to avoid too much random variation. The same variation is observed among younger insured, from 0.5 to less than 0.1 PIM/insured. The PIM scores are given by the grey line, also showing great variability between physicians, between about +1 and −1. However, there was no clear correlation between low PIM prescribing (frequencies) and the effort to stop PIM (scores), except perhaps for some physicians shown on the far right (Figure 1). However, the difference of average scores among young and old people was not statistically significant (0.36 probability that they were due to hazard according to bilateral t-test).
Discussion
Main Findings
To the best of our knowledge, this is the first study comparing five approaches for PIM identification in the same setting. The comparison of PIM frequencies is difficult because it can be biased by various factors27 (country, age of patients, and possible overlap between PIM lists) and patient selection. For instance, it is difficult to compare our results with a study focusing on hospitalized patients (higher rates5) or another taking into consideration only certain duplicated prescriptions (lower rates28). Our study has the advantage to compare PIM approaches from the same data set, with explicit explanations of the differences.
Our results are in line with a previous study and confirm the high rate of PIM in Switzerland, using data from an HMO.29 The rates are slightly higher than the prevalence of PIM per patient (considering only one PIM per patient) with the composite approach.30
We found similarities between the different approaches in the choice of listed drugs categories, mainly sleeping pills, anxiolytics, NSAIDs and drugs with anticholinergic effects. However, the lists of substances included in these categories differed across approaches for unclear reasons. Such discrepancies probably reflect different drug markets. We also identified categories of drugs such as nitrofurantoin or anti-dementia drugs, that are not consistently listed in all the approaches. Possible explanation includes the lack of evidence for some these recommendations; this might alter the interpretation of the results. Indeed, some interventions fall into a grey zone for which the balance of benefits and harms varies substantially among patients and are backed by little evidence to help decide which patients may benefit. We have therefore proposed a composite approach that systematically includes substances with analogous effects. Several substances considered as PIM were not prescribed because they were not or no longer authorized on the Swiss market. Furthermore, we introduced some restrictions to comply with the best practices in Switzerland, by tolerating certain short-term treatments (sleeping pills, anxiolytics, NSAIDs) for example. Conversely, we considered that long-term sleeping pills and anxiolytic treatments were not appropriate in younger patients either. Globally, the composite indicator indicates a frequency of 0.35 PIM par patient among patients older than 64 years old.
Benzodiazepines (BZD) used as sleeping pills and/or anxiolytics are the main reported PIM irrespectively of the approach used, accounting for about a quarter of PIM in the group of elderly people. Of note, it must be emphasized that this BZD rate was not higher using the new composite indicator even if we extend the list to all substances because short-term prescriptions were tolerated in our approach. The problems associated with the abuse of sleeping pills and anxiolytics are well known.31,32 BZD overuse is endemic in western countries, especially in hospital settings for insomnia disorders. Studies showed that up to 30% of inpatients33 and about 20% of outpatients34 had at least one BZD prescription in Switzerland. It is interesting to note that sleeping pills are precisely the ones that gave rise to a greater number of new treatments as opposed to discontinuations (Table 4). A recommendation would therefore be to educate doctors to stop treatment before addiction sets in.30 If this proves too difficult, perhaps they should be encouraged to initiate these types of treatments less often. Among different strategies, a recent meta-analysis revealed that patient education interventions were promising for BZD deprescription.35 Even a small reduction of sleeping pills and anxiolytics prescription rate may have a significant impact in reducing potential serious complications of BZD such as cognitive impairment, delirium, falls and hip fractures and possibly readmissions.36–38
Our results based on the composite score highlighted that such problems also concern younger patients, for whom we observed half of the total PIM volume. It is interesting to note that 60% of inappropriate sleeping pills and anxiolytics were observed in patients under 65, even if the prevalence of PIM was much lower. Knowing that a lot of consumption began before retirement, this result shows that it is important to monitor this issue among younger individuals as well.
This study confirms PIM are frequent in the HMO but there is also a large variation among GP working within Delta network, from 0.25 per patient to 1.0 per patient in elderly. The same variation is observed among younger insured, from 0.5 to less than 0.1 PIM/insured. Clinical variation is an accepted way to identify whether there is overuse in medicine among practitioners. Variation analyses can show significant differences that are warning signs of overuse and a strong quality indicator. Clinical variation can play as catalysts for change by stimulating debate, engaging all participants in the health system so that patient-focused care can be achieved. Process standardization can dramatically decrease variation and eventually improve performance. Furthermore, the case mix of studied populations has little importance when interpreting variation results, which avoids some bias and makes benchmarking between providers easier. For this purpose, data measurement and reporting are again essential and represent a powerful tool.
The average of PIM score also varied, between about +1 and −1, with lower values (more PIM stopped) for physicians with rare PIM among young people (Figure 1). We note though that stopping NSAIDs treatments is observed more frequently.
PIM related to anti-dementia drugs were fairly common. The effects of anti-dementia drugs are modest, symptomatic, and limited to short-term.39,40 Thus, they should it be avoided for a prolonged period, this being not observed currently (Table 4). The frequent use of clometiazole might similarly be questionable because it also generates dependence and undesirables effects.41
It is interesting to note that substances belonging only to the Prescrire list were not typically PIMs, but rather substances which might be substituted by others with less side effects (olmesartan for instance) or low added value.
Perspective and Limitations of the Study
Irrespectively of the approached used, PIM seem high enough to consider that it is a public health issue, requiring corrective measures. It is interesting to note that if one targeted the analysis on BZD (and analogues), on NSAIDs and anti-dementia drugs, one would address 83% of PIM detected by the composite approach.
An approach targeting these three drug classes could therefore be effective in reducing the number of PIM in Switzerland. There are many actions to take:
- Informing and raising awareness of doctors working in the Delta network, by preparing documentation on the disadvantages of these treatments and recommendations for alternative treatments;
- Targeted mail to doctors with a particularly high rate of PIM (Figure 1), with the list of patients and PIM identified;
- Continuous training and physicians pharmacists peer review groups (meeting regularly42) to discuss these four themes to promote alternative treatments.
The effectiveness of each of these measures might be evaluated by the evolution of the PIM rates.
The dissemination of guidelines alone does not appear to change physician behavior. Only multifaceted interventions may have an impact to reduce PIM.43 Behavioral interventions with provider assessment and feedback have proven to affect practice in medicine.44
A recent study published in the same setting, suggests that among primary care practices working in the delta network, thematic quality circle intervention with data feedback and peer comparison resulted in lower mean of PPI prescription and statin prescriptions over age 75 years of age.27 Another study using the same approach with audit and data feedback revealed a modest but statistically significant effect of a multifaceted educative intervention in reducing the BZD prescription rate at discharge in hospitalized patients.45
General information aimed at patients would probably also be necessary to raise their awareness of the dangers of PIMs, as well as to participate in campaigns targeted at the general population.
Several methodological choices are also worth discussing. We did not adjust the results for patients’ characteristics, as we were not able to capture the clinical context from our data; the consequence might be ignoring some PIM. For instance, opioids might be considered inappropriate in certain circumstances (history of falls, cognitive impairment for example21) but justified in a palliative context. Determining whether the use of opioids – even chronically – could be avoided by other effective treatments without knowing all clinical information is difficult. We hypothesized that patients were taking the full amount of delivered drugs, while this is not necessarily the case; the prevalence of PIM might thus be overrated, especially for sleeping pills or inappropriate painkillers. We know that elderly patients have more PIM than young people. One might advocate that old people are more often ill and more frequently suffer from multiple pathologies. However, we considered that the problem of PIM is then also more serious because of the greater risk of side effects (in the event of renal failure or interactions between drugs, for example). Another point is the question of the quantification of PIM. We could have calculated the proportion of patients with at least one PIM; however, we preferred to count all PIM because their accumulation can be harmful for patients. We adopted a 90-day criterion to define chronic medication intake. This complicated the calculation of the indicators because it is necessary to calculate the DDDs, which is not always easy, in particular for drugs combining several substances. We preferred this measure to others such as the number of packages per quarter, which do not take into account the number of tablets and the dosages and which pose problems of delimitation (treatment started at the end of the quarter and continued at the beginning of the following quarter, for example).
Furthermore, we have circumscribed the analysis to drugs administered orally. It could perhaps be interesting to extend the approach to other administration routes, especially for patches (estrogen, anti-inflammatory for example), provided however that the side effects are significant, which is not always the case.46
The drugs have been allocated to primary care physicians, who have a gatekeeping role. It is possible that some PIM were prescribed by subcontracted physicians (psychiatrists for example). Although some approaches (Laroche for example) emphasize drug interactions, we did not retain such drugs’ combinations in the composite model, considering that it was beyond the aim of our study. Similarly, we ignored the issue of polypharmacy and deprescribing.47 We have limited ourselves to drugs that should in principle not be prescribed because their effectiveness is too low in relation to their disadvantages. This reflection can contribute to reducing polypharmacy, but it is not the only the question of the justification of medications according to the indications, which depend on detailed clinical information.48 Since our approach is limited to an indicator that can be calculated from routinely available data, this aspect was not addressed. Doctors will be able to justify this or that exception. For example, the prescription of nitrofurantoin may be justified as first choice treatment if there are no severe side effects and no renal failure (frequent among elderly).49 Another example concerns the prescription of certain anticholinergic treatments, which can be justified in some circumstances.50 Such PIM are relatively infrequent in Switzerland, so it seems appropriate to focus on areas where overuse of drugs seems clearly established.
Finally, we examined all the prescriptions advised against by the Prescrire journal, apart from the PIM mentioned above. This type of approach could be useful for reducing polypharmacy, but none of the substances concerned appeared sufficiently harmful to be added to the list of PIM (see list in Appendix C).
We focused on two cantons insured of a Swiss HMO and cannot be inferred to other regions, even if there is some evidence of overuse of benzodiazepine in most French speaking cantons.33 A comparison with other countries, other languages speaking regions in Switzerland and non-HMO insurance might be interesting.
Overall, our results show that PIM prescribing is very common with more than 0.5 PIM prescribed per patient in half of the doctors, and that prescription rates tend to increase over time. Also, there is no evidence that doctors seek to stop these treatments even among those who prescribe few. It should be noted that this high prevalence of PIM delivery was obtained after excluding short-term prescriptions for benzodiazepines and NSAIDs. On the brighter side, we observe that:
- There are doctors who rarely prescribe PIM; it is therefore feasible reducing their occurrence;
- There is a about one-third patients who are newly receiving PIM per year, which means that if fewer new prescriptions are made, there should be a gradual reduction in the prevalence of PIM;
- PIM concentrate on four types of medicine only, which allows for targeted information.
Conclusion
Our comparison highlighted broad convergences between the different PIM approaches. However, as most of these lists were incomplete, combining them in a composite tool was of interest. The main result shows that the PIM rate is too high in Switzerland for sleeping pills, anxiolytics, NSAIDs and drugs with an anticholinergic effect. There are strong variations between doctors and we recommend to provide feedback to doctors who have particularly high rates. The dynamics of prescriptions show that a score measuring the efforts of physicians to limit PIMs could constitute an interesting indicator, particularly for sleeping pills and anxiolytics in the context of an increasing rate.
Ethics Approval and Informed Consent
We confirm that the data accessed complied with relevant data protection and privacy regulations. The rules applicable in Switzerland in terms of ethics specify that an authorization by an Ethics Commission is not required for a study with anonymous data where it is not possible to identify patients by crosschecking of data. Reference: Federal Act on Research involving Human Beings (HRA) of 30 September 2011 (Status as of 26 May 2021, article 2 paragraph 2c). The data used in the study was anonymized before its use.
Acknowledgments
The authors thank Henrique da Costa (Delta network) for collecting and validating the data.
Disclosure
The authors report no competing interests in this work.
References
1. European medicines agency. Evaluate applications for marketing authorization; 2023. Available from: https://www.ema.europa.eu/en/about-us/what-we-do#evaluate-applications-for-marketing-authorisation-section.
2. U.S. Food and drugs administration. What we do – mission; 2023. Available from: https://www.fda.gov/about-fda/what-we-do#mission.
3. Swiss medic. The tasks. Medicinal products and medical devices: from development to market surveillance; 2023. Available from: https://www.swissmedic.ch/swissmedic/en/home/about-us/swissmedic--swiss-agency-for-therapeutic-products/patients-and-users.html.
4. Gallagher P, Lang PO, Cherubini A, et al. Prevalence of potentially inappropriate prescribing in an acutely ill population of older patients admitted to six European hospitals. Eur J Clin Pharmacol. 2011;67(11):1175–1188. doi:10.1007/s00228-011-1061-0
5. Motter FR, Fritzen JS, Hilmer SN, et al. Potentially inappropriate medication in the elderly: a systematic review of validated explicit criteria. Eur J Clin Pharmacol. 2018;74(6):679–700. doi:10.1007/s00228-018-2446-0
6. Storms H, Marquet K, Aertgeerts B, Claes N. Prevalence of inappropriate medication use in residential long-term care facilities for the elderly: a systematic review. Eur J Gen Pract. 2017;23(1):69–77. doi:10.1080/13814788.2017.1288211
7. Kaufmann CP, Tremp R, Hersberger KE, Lampert ML. Inappropriate prescribing: a systematic overview of published assessment tools. Eur J Clin Pharmacol. 2014;70(1):1–11. doi:10.1007/s00228-013-1575-8
8. Hanlon JT, Schmader KE, Samsa GP, et al. A method for assessing drug therapy appropriateness. J Clin Epidemiol. 1992;45(10):1045–1051. doi:10.1016/0895-4356(92)90144-C
9. Somers A, Mallet L, van der Cammen T, et al. Applicability of an adapted medication appropriateness index for detection of drug-related problems in geriatric inpatients. Am J Geriatr Pharmacother. 2012;10(2):101–109. doi:10.1016/j.amjopharm.2012.01.003
10. Awad A, Hanna O. Potentially inappropriate medication use among geriatric patients in primary care setting: a cross-sectional study using the beers, STOPP, FORTA and MAI criteria. PLoS One. 2019;14(6):e0218174. doi:10.1371/journal.pone.0218174
11. Schur N, Twerenbold S, Reinau D, Schwekglenks M, Meier CR. Helsana-Arzneimittelreport für die Schweiz 2020. Auswertungsergebnisse der Helsana Arzneimitteldaten aus den Jahren 2016 bis 2019 [Helsana drug report for Switzerland 2020. Evaluation results of the Helsana drug data from 2016 to 2019]. Zürich: Helsana Gruppe; 2021.
12. Reich O, Rosemann T, Rapold R, Senn O, Senn O. Potentially inappropriate medication use in older patients in Swiss managed care plans: prevalence, determinants and association with hospitalization. PLoS One. 2014;9(8):e105425. doi:10.1371/journal.pone.0105425
13. Schneider R, Schur N, Reinau D, Schwenkglenks M, Meier CR. Helsana Arzneimittel [Helsana medicines. Report edition 2017]. Report Ausgabe 2017. Zürich: Helsana Gruppe; 2021.
14. Cateau D, Bugnon O, Niquille A. Evolution of potentially inappropriate medication use in nursing homes: retrospective analysis of drug consumption data. Res Social Adm Pharm. 2021;17(4):701–706. doi:10.1016/j.sapharm.2020.05.032
15. Renom-Guiteras A, Meyer G, Thurmann PA. The EU(7)-PIM list: a list of potentially inappropriate medications for older people consented by experts from seven European countries. Eur J Clin Pharmacol. 2015;71(7):861–875. doi:10.1007/s00228-015-1860-9
16. Gallagher P, Ryan C, Byrne S, et al. STOPP (Screening Tool of Older Person’s Prescriptions) and START (Screening Tool to Alert doctors to Right Treatment). Consensus validation. Int J Clin Pharmacol Ther. 2008;46(2):72–83. doi:10.5414/cpp46072
17. O’Mahony D, Sullivan DO, Byrne S, et al. STOPP/START criteria for potentially inappropriate prescribing in older people: version 2. Age Ageing. 2015;44(2):213–218. doi:10.1093/ageing/afu145
18. Krüger C, Schäfer I, van den Bussche H, et al. Comparison of FORTA, PRISCUS and EU(7)-PIM lists on identifying potentially inappropriate medication and its impact on cognitive function in multimorbid elderly German people in primary care: a multicentre observational study. BMJ Open. 2021;11(9):e050344. doi:10.1136/bmjopen-2021-050344
19. Desnoyer A, Blanc AL, Pourcher V, et al. PIM-Check: development of an international prescription-screening checklist designed by a Delphi method for internal medicine patients. BMJ Open. 2017;7(7):e016070. doi:10.1136/bmjopen-2017-016070
20. Kherad O, Selby K, Martel M, et al. Physician assessment and feedback during quality circle to reduce low-value services in outpatients: a pre-post quality improvement study. J Gen Intern Med. 2021;36(9):2672–2677. doi:10.1007/s11606-021-06624-9
21. Fick DM, Semla TP, Steinman M, et al. American Geriatrics Society 2019 updated AGS Beers criteria for potentially inappropriate medication use in older adults. JAGS. 2019;67:674–694.
22. Holt S, Schmiedi S, Thürmann PA. Liste potentziell inadäquater Medikation für ältere Menschen [List of potentially inappropriate medications for older people]. Herdecke: Universität Witten; 2011.
23. Laroche ML, Charmes JP, Merle L. Potentially inappropriate medications in the elderly: a French consensus panel list. Eur J Clin Pharmacol. 2007;63(8):725–731. doi:10.1007/s00228-007-0324-2
24. Salahudeen MS, Duffull SB, Nishtala PS. Anticholinergic burden quantified by anticholinergic risk scales and adverse outcomes in older people: a systematic review. BMC Geriatr. 2015;15(1):31. doi:10.1186/s12877-015-0029-9
25. Nyborg G, Straand J, Klovning A, Brekke M. The Norwegian general practice - nursing home criteria (NORGEP-NH) for potentially inappropriate medication use: a web-based delphi study. Scand J Prim Health Care. 2015;33(2):134–141. doi:10.3109/02813432.2015.1041833
26. Revue Prescrire. Pour mieux soigner, des médicaments à écarter. Bilan 2021. La revue Prescrire. 2020;40(446):929–941.
27. Blozik E, Rapold R, Reich O. Prescription of potentially inappropriate medication in older persons in Switzerland: does the dispensing channel make a difference? Risk Manag Healthc Policy. 2015;8:73–80. doi:10.2147/RMHP.S78179
28. Migliazza K, Bähler C, Liedtke D, Signorell A, Boes S, Blozik E. Potentially inappropriate medications and medication combinations before, during and after hospitalizations: an analysis of pathways and determinants in the Swiss healthcare setting. BMC Health Serv Res. 2021;21(1):522. doi:10.1186/s12913-021-06550-w
29. Chauvin P, Fustinoni S, Seematter-Bagnoud L, Herr M, Santos Eggimann B. Potentially inappropriate prescriptions: associations with the health insurance contract and the quality of the patient-physician relationship? Health Policy (New York). 2021;125(9):1146–1157. doi:10.1016/j.healthpol.2021.06.011
30. NICE guideline CG113. Generalised Anxiety Disorder and Panic Disorder in Adults: Management. London: National Institute for Health and Clinical Excellence (NICE); 2011.
31. Glass J, Lanctôt KL, Herrmann N, et al. Sedative hypnotics in older people with insomnia: meta-analysis of risks and benefits. BMJ. 2005;331(7526):1169. doi:10.1136/bmj.38623.768588.47
32. Lader M, Petursson H. Rational use of anxiolytic/sedative drugs. Drugs. 1983;25(5):514–528. doi:10.2165/00003495-198325050-00004
33. Luta X, Bagnoud C, Lambiris M, et al. Patterns of benzodiazepine prescription among older adults in Switzerland: a cross-sectional analysis of claims data. BMJ Open. 2020;10(1):e031156. doi:10.1136/bmjopen-2019-031156
34. Schumacher L, Dobrinas M, Tagan D, Sautebin A, Blanc AL, Widmer N. Prescription of sedative drugs during hospital stay: a swiss prospective study. Drugs Real World Outcomes. 2017;4(4):225–234. doi:10.1007/s40801-017-0117-6
35. de Souza Ribeiro PR, Schlindwein AD. Benzodiazepine deprescription strategies in chronic users: a systematic review. Fam Pract. 2021;38(5):684–693. doi:10.1093/fampra/cmab017
36. Winkelman JW. Clinical practice. Insomnia Disorder. N Engl J Med. 2015;373(15):1437–1444. doi:10.1056/NEJMcp1412740
37. Xing D, Ma XL, Ma JX, Wang J, Yang Y, Chen Y. Association between use of benzodiazepines and risk of fractures: a meta-analysis. Osteoporos Int. 2014;25(1):105–120. doi:10.1007/s00198-013-2446-y
38. Allain H, Bentue-Ferrer D, Polard E, Akwa Y, Patat A. Postural instability and consequent falls and Hip fractures associated with use of hypnotics in the elderly: a comparative review. Drugs Aging. 2005;22(9):749–765. doi:10.2165/00002512-200522090-00004
39. Courtney C, Farrell D, Gray R, et al. Long-term donepezil treatment in 565 patients with Alzheimer’s disease: randomised double-blind trial. Lancet. 2004;363(9427):2105–2115.
40. Hogan DB. Long-term efficacy and toxicity of cholinesterase inhibitors in the treatment of Alzheimer disease. Can J Psychiatry. 2014;59(12):618–623. doi:10.1177/070674371405901202
41. Dumur J, Csajka C, Pavec O, et al. Quelle alternative aux benzodiazépines, Z-pills et autres hypnotiques pour les personnes âgées ?: mélatonine, valériane ou clométhiazole ? [Which alternative to benzodiazepines, Z-pills and other hypnotics for aged people ? Melatonin, valerian, or clomethiazole] Rev Med Suisse. 2018;14(626):2018–2023.
42. Macé F, De Vriese C, Nelissen-Vrancken M, Ruggli M, Brülhart M, Peyron C. General practitioners-community pharmacists pharmacotherapy discussion groups: analysis of their implementation through a series of case studies. Explor Res Clin Soc Pharm. 2023;12:100331. doi:10.1016/j.rcsop.2023.100331
43. Kjelle E, Andersen ER, Soril LJJ, van Bodegom-Vos L, Hofmann BM. Interventions to reduce low-value imaging - A systematic review of interventions and outcomes. BMC Health Serv Res. 2021;21(1):983. doi:10.1186/s12913-021-07004-z
44. Yoong SL, Hall A, Stacey F, et al. Nudge strategies to improve healthcare providers’ implementation of evidence-based guidelines, policies and practices: a systematic review of trials included within Cochrane systematic reviews. Implement Sci. 2020;15(1):50. doi:10.1186/s13012-020-01011-0
45. Kherad O, Bottequin E, Steiner D, Alibert A, Eurin R, Bothorel H. Implementing a multifaceted intervention among internal medicine residents with audit and educative data feedback significantly reduces low-value care in hospitalized patients. J Clin Med. 2022;11(9):2435. doi:10.3390/jcm11092435
46. Lin J, Zhang W, Jones A, Doherty M. Efficacy of topical non-steroidal anti-inflammatory drugs in the treatment of osteoarthritis: meta-analysis of randomised controlled trials. BMJ. 2004;329(7461):324. doi:10.1136/bmj.38159.639028.7C
47. Rodríguez-Pérez A, Alfaro-Lara ER, Albiñana-Perez S, et al. Novel tool for deprescribing in chronic patients with multimorbidity: list of evidence-based deprescribing for chronic patients criteria. Geriatr Gerontol Int. 2017;17(11):2200–2207. doi:10.1111/ggi.13062
48. Curtin D, Gallagher PF, O’Mahony D. Explicit criteria as clinical tools to minimize inappropriate medication use and its consequences. Ther Adv Drug Saf. 2019;10:2042098619829431. doi:10.1177/2042098619829431
49. Betschart C, Albrich WC, Brandner S. Guideline of the Swiss Society of Gynaecology and Obstetrics (SSGO) on acute and recurrent urinary tract infections in women, including pregnancy. Swiss Med Wkly. 2020;150(1920):w20236. doi:10.4414/smw.2020.20236
50. Kiesel EK, Hopf YM, Drey M. An anticholinergic burden score for German prescribers: score development. BMC Geriatr. 2018;18(1):239. doi:10.1186/s12877-018-0929-6
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.