")
Back to Journals » Journal of Pain Research » Volume 16
Postural Control of Patients with Low Back Pain Under Dual-Task Conditions
Authors Xiao W , Yang H , Wang Z, Mao H, Wang H, Hao Z, Zu Y , Wang C
Received 10 October 2022
Accepted for publication 20 December 2022
Published 10 January 2023 Volume 2023:16 Pages 71—82
DOI https://doi.org/10.2147/JPR.S392868
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Alaa Abd-Elsayed
Wenwu Xiao,1 Huaichun Yang,1 Zhuangfu Wang,2 Haian Mao,1 Hongjiang Wang,1 Zengming Hao,1 Yao Zu,1 Chuhuai Wang1
1Department of Rehabilitation Medicine, the First Affiliated Hospital, Sun Yat-Sen University, Guangzhou, People’s Republic of China; 2Faculty of Population Health Sciences, Institute of Child Health I, University College London, London, UK
Correspondence: Chuhuai Wang, Department of Rehabilitation Medicine, the First Affiliated Hospital, Sun Yat-Sen University, No. 58 Zhongshan Er Road, Guangzhou, 510080, People’s Republic of China, Tel +86 13316191023, Email [email protected]
Abstract: Low back pain is a major global public health problem, but the current intervention effect is not ideal. A large body of previous literature suggests that patients with chronic low back pain may have abnormal postural control, which is more evident in the dual task situation. In recent years, research on postural control in patients with low back pain under dual-task conditions has gradually become a hot topic. However, the results obtained from these studies were not entirely consistent. In this review, we summarized relevant studies on the performance of postural control in patients with low back pain under dual-task conditions, analyze it from the perspective of the theoretical model of dual-task interaction, the specific research paradigm of dual task, the performance of postural control, and the related factors affecting postural control performance, etc. It was reasonable to assume that patients with low back pain might have a certain degree of abnormal postural control, and this abnormality was affected by comprehensive factors such as age, cognitive resource capacity, attention needs, complex sensorimotor integration, external environment, etc. Furthermore, postural control performance in low back pain patients under dual-task conditions was further influenced by the nature and complexity of the different tasks. In general, the more attention resources were needed, the external environmental conditions were worse, and the age-related functions were degenerate, etc., the weaker posture control ability was. In short, a deeper understanding of postural control in patients with low back pain under dual-task conditions may shed light on more references for the rehabilitation and management of low back pain, as well as some new ideas for scientific research on cognition and postural control.
Keywords: postural control, low back pain, dual-task, cognitive, motor
Introduction
Low back pain (LBP) is the second leading cause of years living with disability (YLDs) in China,1 and is also an important cause of the global disease burden.2 Studies have reported that disability and economic costs caused by LBP will increase in the coming decades.2,3 It is important to note that a high proportion of low back pain becomes chronic, about 90% of which is non-specific, and the etiology of this population is usually unclear and effective treatment is lacking.4 Therefore, it deserves to pay more attention to low back pain, especially for chronic low back pain.
Postural control is the ability to control the stability and directionality of the body’s spatial position and is fundamental to everyday activities, including motor strategies, sensory strategies, biomechanical components, cognitive strategies, dynamic activity control, and spatial positioning.5,6 In addition, postural control requires varying with task and environment.
LBP patients may suffer from certain degrees of postural control abnormalities, mainly manifested as decreased trunk coupling ability,7 impaired gait,8 increased center of gravity and center of mass deviation,9 prolonged or disappeared preactivation time of postural muscles,10 proprioceptive disturbances,11 decreased attention and executive ability,12 and reorganized structural or functional of the central nervous system.13
Dual task (DT) is a combination of multiple different types of tasks, which generally include cognitive and motor tasks.14,15 It is widespread for people to perform dual task in their daily life (such as talking while walking, talking to people while carrying a water cup upstairs, etc.). Dual-task training (DTT) is based on the dual-task examination and evaluation of the subjects to determine the specific dysfunction and then adopt targeted training treatment methods. Early dual-task studies of neurological diseases such as stroke, Parkinson’s diseases and Alzheimer’s diseases have shown that postural control requires cognitive attention needs.16–19 In recent years, the research on dual task in the field of postural control in patients with low back pain has also attracted the attention of scholars.20–22
By reviewing the research reports on postural control of patients with low back pain under dual-task conditions, we refined and summarized the important views and research results from the dual-task theoretical basis, research paradigms, postural control performance, and the factors that affect performance, etc. To summarize, we aimed to provide some new ideas for postural control research on low back pain.
Theoretical Model of Dual-Task Interaction
It is a common phenomenon that there is often a decline trend in performance for one or two tasks when performing a dual task. To explain this appearance of task performance decline after being disturbed, scholars have carried out a series of explorations to form the following three relatively accepted theoretical models, namely, the cross-domain competition model, the U-shaped nonlinear interaction model and the task prioritization model.23
The cross-domain competition model believes that the total cognitive resources of the human body have a certain limit. When more than one task is completed at a certain time, postural control and cognitive activities will compete for attentional resources, and the capacity assigned to each task will become smaller, then the performance of completing the task will decrease. After increasing the cognitive load in the case of external disturbance, Jarrett P et al found that the additional cognitive load led to delay muscle activation responses and subsequently greater intersegmental lumbar spine flexion in response to a sudden loading perturbation.24 Ge L et al observed the different levels of cognitive load of older women with low back pain under different postural conditions and found that cognition was involved in the postural regulation, and cognitive load showed more disturbing effects on postural control in older women with low back pain, which was associated with falling.25 These studies suggested that cognitive tasks engage in competition for attention resources, and that loading cognitive load results in decreased performance on postural control.
Notably, some scholars have found that performing secondary cognitive tasks does not always have a detrimental effect on postural control. For example, using a modified Stroop color test to observe the effect of attentional demand on trunk muscle postural activation, Moseley et al26 found that postural activation of deep trunk muscles was not affected in tasks with lower attentional demands. However, Van et al27 found that a dual task with cognitive load reduced postural sway in patients with non-specific chronic low back pain (NCLBP). Vuillerme N et al28 also reported that visual-auditory stimulation and language task seems to improve postural stability in healthy young participants. In addition, by giving subjects different levels of cognitive load during standing, Huxhold et al29 found that the range of postural sway was smaller and the postural was more stable at low levels of the cognitive tasks. These studies revealed that postural stability would be improved when subtask cognitive demand is low, the reason may be that low cognitive demand could divert attention from postural control and increase the automation of postural processing to improve stability. Interestingly, Huxhold’s study also demonstrated that postural swing increased as the difficulty of cognitive task increased.29 Similar conclusions have been obtained by Legrand A30 and Rowley KM’s31 research. To explain this phenomenon, Lacour M proposed the concept of the U-shaped nonlinear model,23 deemed that the improvement or decrease of postural control performance depends on the level of cognitive task demand, and when cognitive tasks require higher attention resources, the performance of postural control decreased, and vice versa.
As early as 1997, “the Lancet” reported that “stopping walking while talking can be used as a predictor of falls in the elderly”.32 In addition, BrownL A et al33 also detected that in the presence of increased postural threat, the elderly were more likely to prioritize the postural control task over the cognitive task, which also reflects the posture-first strategy. Note-worthily, inconsistent with this view, a previous review revealed that the postural strategy typically adopted by people with Parkinson’s disease in their daily lives was that “task-first, postural second”, which increases the risk of falls in dual-task situations.34 These studies have shown that performing two tasks that requires attentional resources at the same time not only causes competition for attentional resources but also challenges the brain’s prioritization of the two tasks, a phenomenon that scholars define as the task-prioritization model.23
It is worth noting that the U-shaped nonlinear interaction model and the cross-domain competition model are not contradictory. In all, when the attention resources required by the task do not exceed the total resource capacity, the cognitive task will be conducive to postural control, while when the attention resources required by the task increase and exceed the resource capacity, the cognitive task would be decreased with the performance of postural control due to the competition of attention resources. Moreover, the task prioritization model assumed that postural control and cognitive tasks interact with each other, and the changes were due to individual changes in attention allocation strategies, rather than resource competition or decreased attention capacity.
The Specific Implementation of the Dual Task in the Study of Low Back Pain
Patients with low back pain may have some degree of abnormal postural control, but most studies have been conducted under single-task conditions without cognitive load. In daily work, the postural environment is always complex and cognitive tasks diverse, so it is very essential to conduct postural control research under dual-task conditions with cognitive load.
By reviewing dual task studies related to low back pain, the detailed standards were as follows. A search was conducted in “Pubmed, Web of science, and Embase” databases, using the keywords of “dual task” and “low back pain” with “AND” character concatenation, and excluding the review or case report types of studies, experimental studies were selected for analysis and summarization. The characteristics of these studies are as follows. First, all studies were conducted with the cognitive-motor dual-task paradigm (only one piece of literature included both motor-motor and cognitive-motor dual-task paradigms in the intervention paradigm).21 Among them, the motor task is mostly about standing/sitting posture and walking under different conditions, while cognitive tasks involve reaction time, numerical calculation, working memory, and language fluency tasks. Second, most of the research were done in the past 5 years, especially in the past 3 years, indicating that dual-task research is relatively new in the field of low back pain research. Third, the research subjects were mainly young and middle-aged patients with chronic low back pain.21,22,25,27,31,35–39 In addition, most of the research were observational study, only one piece of literature was a randomized controlled study.40 Moreover, there is only one piece of literature on the performance of patients with low back pain under dual-task conditions after dual-task training.40 Last, the observation and measurement indicators are mostly focused on peripheral behavioral performance, only one piece of literature involves the research of the central nervous system,40 and there is also a lack of combined research on the relationship between pain and psychology.41 For a summary of the above-related studies, see Table 1 for details.
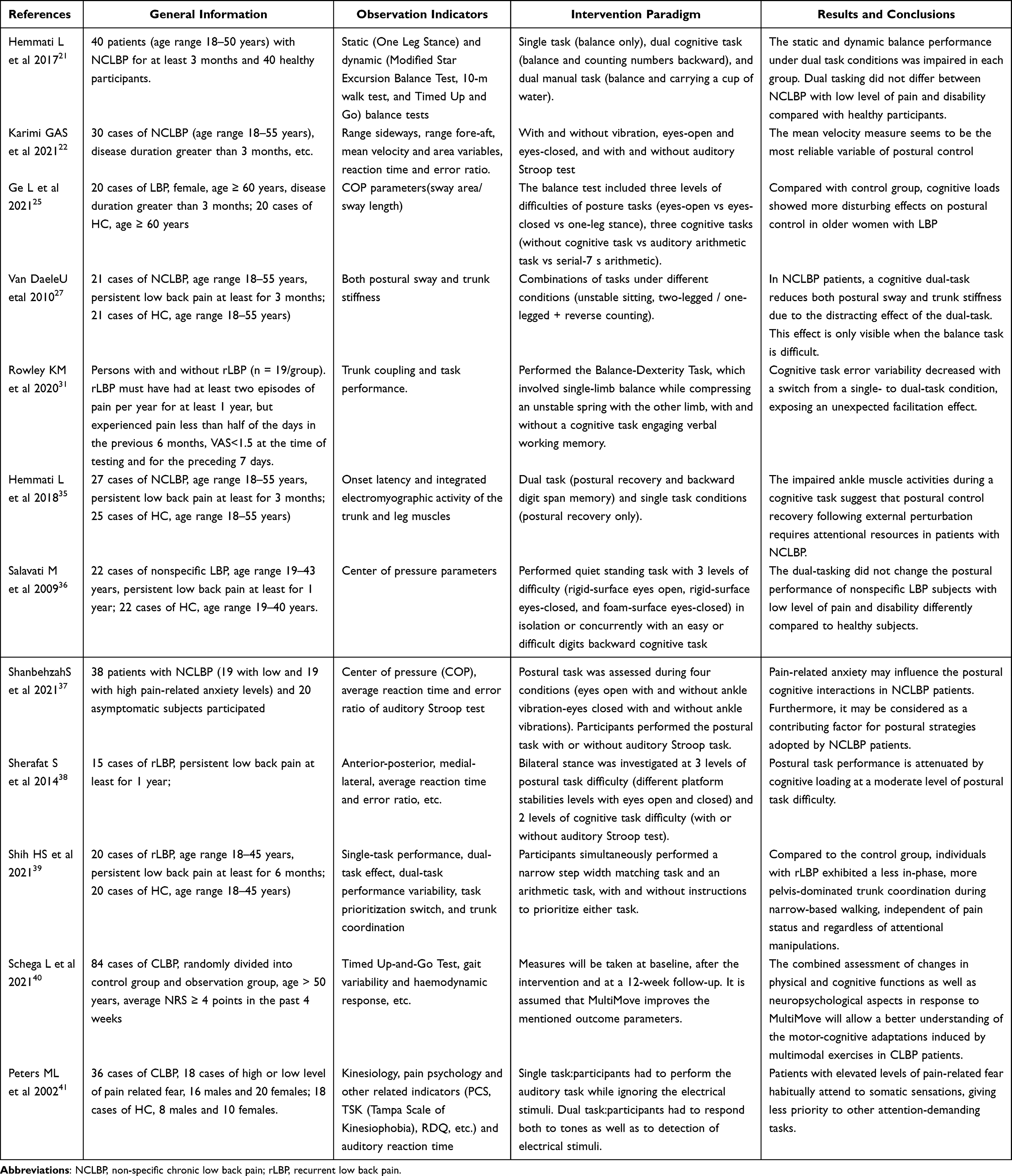 |
Table 1 The Summary of Research on the Application of Dual Task in Low Back Pain |
Postural Control Performance of Patients with Low Back Pain Under Dual-Task Conditions
Regarding the research on postural control of patients with low back pain under dual-task conditions, in terms of task performance, the results were not uniform. Ladan Hemmati et al35 deemed that patients with nonspecific low back pain require attention resources for postural control recovery after external disturbances, which may increase the risk of injury when performing high-attention cognitive tasks. Compared with single-task, Hamacher D et al20 found that patients with chronic low back pain had greater variability in stride length and stride time under dual-task conditions. Shih HS et al39 performed a numerical calculation task while walking in patients with recurrent low back pain, and observed arithmetic performance, walking performance, and trunk coordination; they found that the variability increased under dual-task conditions. In addition, using the dual-task to explore the cognitive load on postural control in older women with low back pain, Ge L et al25 found that despite the difficulty level of the cognitive tasks being very low, the patients’ center of pressure and other parameters also changed more. Moreover, the research of Peters ML41 and Mazaheri M42 also obtained similar results that was under the dual-task condition with cognitive demands, the postural control ability of patients with low back pain deteriorated, and the difference was more pronounced under the condition of high cognitive load.
Contrary to the above findings, some scholars regarded that cognitive load could enhance the postural control performance of patients with low back pain. For instance, one study conducted by Rowley KM et al31 demonstrated that low attention loads interfered with memory-of-pain related conscious processing of postural and resulted in improved trunk coupling when the dual-task was added, compared to the single-task condition; another study performed by Van Daele U at al27 found that reverse counting cognitive load reduced postural sway and trunk stiffness in patients with non-specific low back pain, and increased postural control ability. In addition, Salavati M et al36 also suggested that the degree of postural sway in patients with non-specific low back pain decreased with the increasing of cognitive load. The reasons for these contrary results may be as follows: Firstly, cognitive load distracts attention, reduces pain recall, and increases the ability of automatically adjust posture, which makes the area, amplitude of posture swing, and trunk coordination become well. Secondly, these studies have relatively strict admission standards, and the cognitive function of the study population was relatively high. The attentional resources required for the intervention in the study may not exceed the total attentional resource capacity of the subjects. Alternatively, subjects may also adopt the “postural-first” strategy. Thirdly, postural stability increases or decreases also depending on the complexity of the secondary cognitive tasks, the postural stability could increase in the case of the less complex cognitive tasks and fewer resources required, precisely, the cognitive tasks in these studies were not of high complexity. Fourth, the differences in outcomes might also be due to differences in study populations, types of dual-task interventions, and assessment methods. In addition, low back pain was a typical chronic disease with low-level dysfunction, patients could still compensate through redundant postural control regardless of whether cognitive load affected daily living functions to a great extent or not. Moreover, the researcher of Sherafat S deemed that the influence of cognitive load and postural control were bidirectional, which was, the performance of postural control was not only affected by cognitive load but also affected the performance of the cognitive tasks to a certain extent.38
In addition, there was only one piece of literature on dual-task training in low back pain: this prospective, dual-arm, single-blind, randomized controlled study that integrated cognitive and motor components in a multimodal treatment of chronic low back pain patients. By observing the indicators of physical function, cognitive function, and neuropsychology, the author regarded that multimodal training might contribute to some extent to improve the physical and physiological functions of patients with low back pain. It was worth noting that this study not only reflects the dual-task training mode, but also uses the functional near-infrared to observe the hemodynamic changes of the prefrontal cortex, explores brain plasticity from a central perspective, and observes from a social psychological perspective.40 Based on the rehabilitation discipline, multimodal intervention for diseases under the “peripheral-central-peripheral” closed-loop rehabilitation network was advocated, and patients’ social and psychological functions are actively concerned. The research methods and treatment schemes included in this study could reflect these advantages and were worthy of reference. On all account details, it is reasonable to expect the results reported of this prospective study.
The former related studies have shown that, compared with single task, under the condition of dual-task with cognitive load, the performance of postural control might change to a certain extent, and the improvement or decline of postural control performance depends on the level of attentional resources required by the cognitive tasks. At the same time, postural control also has a certain impact on cognitive performance.
Factors Affecting Postural Control in Patients with Low Back Pain Under Dual-Task Condition
Studies using a dual-task interference paradigm on postural control in patients with low back pain have yielded mixed results, and the reasons for these differences in performance may be as follows.
From the perspective of sensory strategies, when the proprioceptive information from the ankle is reliable (such as on the solid plane), people tend to use the ankle strategy to maintain postural stability, and when the information from the ankle is unreliable (such as on the foam surface), people use more back muscle information strategies to control posture balance and stability. Because patients with low back pain may have a certain degree of decrease or loss of back proprioceptive sensation,43,44 the reliability of low back sensory information decreases, which leads to poor performance of postural control. The sense of visual, vestibular, and auditory are also important components of sensory information. When this input information is insufficient, it will inevitably cause adverse effects on postural control.45 In addition, Mohammadi M et al46 also suggested that postural compensation in patients with chronic low back pain relies on the proprioceptive system. Through dual-task studies under different sensory information input conditions, Salavati M’s study,36 Ulrike Van Daele’s study,27 Hemmati L’s study,35 et al found that the less the sensory information, the worse the postural control ability of patients with low back pain. The above studies implied that sensory information was an important factor affecting postural control in patients with low back pain, and postural control was more significantly affected by the condition of multi-sensory conflict and cognitive load.
From the perspective of cognitive strategy, a study in which subjects received water from a bucket in a standing condition (water dropped with and without cueing)47 found that when the load was cued, the subjects’ deep multifidus muscle was preactivated at 140–30ms before loading, followed by a quiet period, and another activation period appeared at 50–90ms after loading. When the load was not cued, there was no preactivation, indicating that postural control requires cognitive involvement. A systematic review and meta-analysis classified cognitive tasks into five categories, which contains reaction time tasks, discrimination and decision-making tasks, mental tracking tasks, working memory tasks, and verbal fluency tasks.48 Different types of cognitive tasks also have different effects on postural control. Cognitive demands affect the performance of postural control, and when sub-task cognitive demands are high, postural control would be adversely affected by the competition of attentional resources between cognitive and sensorimotor processing. Some scholars reached a consensus that postural control depends on the difficulty of cognitive and motor tasks, and cognitive load presents a bidirectional regulation of postural control. This low cognitive load may promote postural control, but with the increase of cognitive load and resource competition, postural control becomes worse.25,49,50 The reason for this phenomenon is not difficult to explain by the U-shaped theoretical model mentioned above. Additionally, a study using motion capture to quantify individuals’ step length and width, trunk-pelvis and hip excursion, inter-segmental coordination, and stride-to-stride variability found that switching attention resources during gait affected patients’ changes in stride variability, hip axial and sagittal motion.51 From a therapeutic perspective, Paolucci T et al52 found that intensive cognitive rehabilitation training could improve trunk coordinate and postural stability and reduce pain symptoms in patients with low back pain. In this sense it is pertinent to note that, cognitive strategy is a factor that affects postural control of patients with low back pain. Notably, by performing a backward numerical task of varying difficulty under rigid surface eyes-open/closed and foam-surface eyes-closed conditions, compared with healthy subject, Salavati M36 found that patients with non-specific low back pain had less postural sway, while postural sway decreased with increase in the level of cognitive load. The reason for this discrepant result, which was contrary to most studies, might be as follows: firstly, “Postural priority” and attention resources release during postural control; secondly, related to the difficulty level of the cognitive tasks; thirdly, it might be related to the age and health status of the research subjects. Notability, based on the interaction between pain and cognition, long-term pain would be accompanied by cognitive impairments such as attention, reaction speed, and executive function.53,54 For patients with low back pain, pain may interfere with cognition, leading to insufficient attention resources, resulting in decreased postural control and poor motor performance.
Noteworthy, some people develop low back pain while standing for prolonged periods, while others do not, possibly due to the use of different motor control strategies during standing.55 By reducing the stability of the standing platform, EhsaniF et al56 found that the core posture muscles (transverse abdominal muscle, internal oblique muscle, etc. measured by ultrasound) increased in both low back pain and healthy people, and the deeper the activation was, the greater the activation was. Furthermore, the external disturbance reduced the balance, changed motion control, and impaired posture control. A study by Rowley et al31 also found that the trunk kinematics of patients with low back pain changed under cognitive dual-task conditions, believed that trunk motor control (trunk coupling, dexterity, trunk fatigue, etc.) was an important factor affecting postural control, and was affected by cognitive, pain psychology, sensation and other factors. However, little is known about the interaction between pain, cognitive, and postural control, and some scholars have explored this issue to some extent. For instance, based on postural control in patients with low back pain of varying degrees of pain, T Sipko et al found that patients with high pain relied more on visual input on hard surface than those with low pain, and that balance control required more investment of cognitive resource when increasing the difficulty of the plantar support surface.57 In terms of postural control (sit-to-stand strategy), T Sipko et al also found that patients with high chronic low back pain used compensatory motor strategies and presented avoidance behaviors when performing sit-to-stand maneuvers, compared to low pain patients.58 Indeed, considering that pain requires attention resources, T Sipko et al deemed that chronic low back pain patients had simply no available attention resources, which could back up more conscious and less automatic control of posture, and found that possible benefits of proprioceptive neuromuscular facilitation exercise for pain and postural control in chronic low back pain patients.59 Another study also showed that pain catastrophizing may affect postural control and should be considered when interpreting postural control and managing low back pain.60 Considering these interesting findings, it is reasonable to believe that chronic pain impairs postural control to some extent and is influenced by cognitive function. In addition, patients with low back pain often suffer from motor control impairment due to more obvious activation of superficial trunk muscles,56 decreased proximal joint torque and increased trunk stiffness,61 delayed response of postural muscles,62 and back muscle fatigue.63 In addition, the motor control and related postural adjustments were synchronous processes and depend on several mechanical conditions (movement speed, perturbation symmetry, structural stability and integrity), sensory conditions (eyes open or closed, foam and rigid support), behavior conditions (self-rhythm, command, feedback) and cognitive conditions (speed of reaction, executive function, etc.).64,65 In short, different motor strategies under dual-task conditions were important factors affecting human postural control and were affected by sensory, cognitive, pain intensity, environmental and other comprehensive factors.
It is widely recognized that the impairment of postural control in the elderly may be related to the decline of sensorimotor function, neuromuscular control, and central decision-making ability. Some scholars have analyzed the factor of age to explore the performance of postural control in patients with low back pain of different ages, ie, Silva RA et al66 compared postural control during one leg stance in subjects with and without chronic low back pain, the results showed that chronic low back pain affected balance in both young and old, and the balance was worse in elderly patients, while another study by Silva RA et al67 showed that elderly patients with low back pain exhibited lower trunk activation during a one-leg stance balance task. By studying the back proprioception in young and middle-aged patients with low back pain, Pinto SM et al68 found that the central and peripheral processing of proprioceptive signals in the lumbar spine had age-related deterioration. Through these studies, it is not difficult to deduce that age is an important factor affecting postural control in patients with low back pain. However, these studies were mostly conducted under single-task condition, considering the total capacity of attentional resources decreased in the elderly, it was more difficult to transfer attention between dual-task, increased attentional resource demands related to postural control, either resource allocated barriers, or decreased dynamic activity control and spatial orientation, or a combination of these factors. It is reasonable to speculate that age has a certain impact on postural control under dual-task conditions. Unfortunately, there was no research report on age-related postural control of low back pain under dual-task conditions.
A large amount of low back pain patients needs to be involved in work or community life. The variety and complexity of living and working environment may also affect the patient’s postural control. A study examined how postural sway measured using central of pressure and trunk acceleration parameters is influenced by the aquatic environment along with the effects of visual information, found that the aquatic environment increases postural instability, and the mean velocity or area were more significantly affected when individuals stood with eyes closed in the aquatic environment.69 Another study of genetic and environmental effects on lumbar posture, flexibility, and motion control in healthy adults suggested that lumbar motion control might be more influenced by environmental factors.70 In addition, Helmich I et al71 also showed that altered environments could increase the attention-demanding processes during postural control in individuals with persistent post-concussion symptoms. The above studies have shown the effect of environmental conditions on postural control, but to the best of our knowledge, single/dual-task studies on low back pain were mostly conducted under changing support conditions (rigid/foam, wide/narrow) or visual environment (eyes open/closed), and there was no research under changing conditions of the actual environment.
In addition, factors such as the placement of attention points, individual professional skills, and biomechanical components could also affect postural control performance under dual-task conditions. For example, performing word memory tasks in different standing conditions, compared to non-dancers, Stins JF et al found that the level of automaticity was already reached maximal in professional dancers standing with eyes open, and that adding an attention-shifting task did not lead to a further increase in postural automaticity. And arguing that the degree of attentional involvement in postural control is a process that varies along an automatic continuum, influenced by factors such as relatively stable subject characteristics (expertise) and attentional demands of the task at hand.72 But unfortunately, there are still no reports on these aspects of patients with low back pain.
Summary and Outlook
Postural stability is an important part of the process of body motion control and coordination, which is affected by age, the capacity of cognitive resources, attention needs, complex sensorimotor integration, external environment, and other comprehensive factors. Moreover, the performance of postural control under dual-task condition is further affected by the nature and complexity of different tasks. It can be roughly summarized as follows: more attention resources are required, the external environmental conditions are worse, the age-related functional deterioration, etc., the postural control ability is weaker.
Currently, there are limited reports on postural control in low back pain under dual-task conditions, and little is known about the impact of cognitive on postural control. In the sense of this sight, we regard that more in-depth research is needed in the following areas. Firstly, at present, most postural control studies on low back pain are conducted under single-task conditions, and further research on dual-task assessment and treatment that is closer to real life and environment needs to be carried out. Such as how the postural control strategies of people with low back pain differ from those of healthy people during “sitting to standing” or “squatting to standing” activities, which are common daily postural transitions, or even how their postural control strategies change when performing cognitive dual-task in these conditions, are interactive and complex postural control strategies that deserve further exploration. Secondly, the results of postural control research in patients with low back pain under dual-task conditions are not completely consistent, and the relevant theoretical models still need further experiment verification, which can integrate the “central effect model”, neurophysiology and social psychological mechanism of postural control, and deeply explore the neural mechanism of postural control and the theory of “physiology-psycho-sociology”. Thirdly, considering the complex relationship between pain, cognition and postural control, different levels of chronic pain have different effects on both cognition and postural control, and how to unravel the complex relationship between them is an element that requires special attention, and this work is particularly valuable for researchers working on postural control of chronic low back pain. Fourthly, the current studies mostly contain small samples, and there is a lack of comparative research on different age groups, different external environments, different task nature and attention needs, which can be studied deeply in the future. The fifth, the therapeutic research on dual-task training for low back pain is extremely lacking. Studies on postural control after targeted dual-task training intervention would be conducted to further explore the long-term or short-term benefits and duration of benefits, which is especially suitable for the management and treatment of non-specific low back pain. In addition, the abnormal posture control of elderly patients with low back pain is more obvious, and age-related cognitive function decline. However, there is a relative lack of research on cognitive postural control in elderly patients with low back pain. In the context of an increasingly aging population, it is necessary to pay more attention to elderly patients with low back pain. Finally, postural control is the result of active control of the whole-body muscles by the central nervous system based on muscle proprioceptive, visual and vestibular information under various complex tasks and environmental conditions, which requires central and peripheral integration, involves brain activation and compensation, integrates the cognitive-sensory-motor system, and activates peripheral muscle activation. However, most of the current studies are related to the evaluation of peripheral kinematics and behavioral parameters, and few studies explore the complex neural network mechanisms related to postural control under dual-task conditions from a central perspective. In other words, combining the central image for in-depth discussion will enhance the persuasiveness of the research.
Funding
This study was supported by “the National Natural Science Foundation of China (82172532)” and “Development Center for Medical Science & Technology National Health Commission of China (DCMST-NHC-2019-AHT-01)”.
Disclosure
The authors declare no conflicts of interest regarding this study.
References
1. Wu A, Dong W, Liu S, et al. The prevalence and years lived with disability caused by low back pain in China, 1990 to 2016: findings from the global burden of disease study 2016. Pain. 2019;160:237–245. doi:10.1097/j.pain.0000000000001396
2. Knezevic NN, Candido KD, Vlaeyen JWS, Van Zundert J, Cohen SP. Low back pain. Lancet. 2021;398:78–92. doi:10.1016/S0140-6736(21)00733-9
3. Hartvigsen J, Hancock MJ, Kongsted A, et al. What low back pain is and why we need to pay attention. Lancet. 2018;391:2356–2367. doi:10.1016/S0140-6736(18)30480-X
4. Maher C, Underwood M, Buchbinder R. Non-specific low back pain. Lancet. 2017;389:736–747. doi:10.1016/S0140-6736(16)30970-9
5. Ivanenko Y, Gurfinkel VS. Human postural control. Front Neurosci. 2018;12:171. doi:10.3389/fnins.2018.00171
6. Low DC, Walsh GS, Arkesteijn M. Effectiveness of exercise interventions to improve postural control in older adults: a systematic review and meta-analyses of centre of pressure measurements. Sports Med. 2017;47:101–112. doi:10.1007/s40279-016-0559-0
7. Rowley KM, Smith JA, Kulig K. Reduced trunk coupling in persons with recurrent low back pain is associated with greater deep-to-superficial trunk muscle activation ratios during the balance-dexterity task. J Orthop Sports Phys Ther. 2019;49:887–898. doi:10.2519/jospt.2019.8756
8. Krekoukias G, Sakellari V, Anastasiadi E, et al. Gait kinetic and kinematic changes in chronic low back pain patients and the effect of manual therapy: a randomized controlled trial. J Clin Med. 2021;10(16):3593. doi:10.3390/jcm10163593
9. Li R, Wang N, Yan X, Wei K. Comparison of postural control between healthy subjects and individuals with nonspecific low back pain during exposure to visual stimulus. Chin Med J. 2014;127:1229–1234. doi:10.1142/S0192415X14500773
10. Yu Q, Huo Y, Chen M, et al. A study on the relationship between postural control and pain-related clinical outcomes in patients with chronic nonspecific low back pain. Pain Res Manag. 2021;2021:9054152. doi:10.1155/2021/9054152
11. Shokouhyan SM, Davoudi M, Hoviattalab M, et al. Linear and non-linear dynamic methods toward investigating proprioception impairment in non-specific low back pain patients. Front Bioeng Biotechnol. 2020;8:584952. doi:10.3389/fbioe.2020.584952
12. Corti EJ, Gasson N, Loftus AM. Cognitive profile and mild cognitive impairment in people with chronic lower back pain. Brain Cogn. 2021;151:105737. doi:10.1016/j.bandc.2021.105737
13. Li X, Liu H, Ge L, et al. Cortical representations of transversus abdominis and multifidus muscles were discrete in patients with chronic low back pain: evidence elicited by tms. Neural Plast. 2021;2021:6666024. doi:10.1155/2021/6666024
14. Abou L, Peters J, Fritz NE, Sosnoff JJ, Kratz AL. Motor cognitive dual-task testing to predict future falls in multiple sclerosis: a systematic review. Neurorehabil Neural Repair. 2022;36:757–769. doi:10.1177/15459683221131791
15. Gallou-Guyot M, Mandigout S, Bherer L, Perrochon A. Effects of exergames and cognitive-motor dual-task training on cognitive, physical and dual-task functions in cognitively healthy older adults: an overview. Ageing Res Rev. 2020;63:101135. doi:10.1016/j.arr.2020.101135
16. De Freitas TB, Leite PHW, Doná F, Pompeu JE, Swarowsky A, Torriani-Pasin C. The effects of dual task gait and balance training in Parkinson’s disease: a systematic review. Physiother Theory Pract. 2020;36(10):1088–1096. doi:10.1080/09593985.2018.1551455
17. Fritz NE, Cheek FM, Nichols-Larsen DS. Motor-cognitive dual-task training in persons with neurologic disorders: a systematic review. J Neurol Phys Ther. 2015;39:142–153. doi:10.1097/NPT.0000000000000090
18. Mancioppi G, Fiorini L, Rovini E, Cavallo F. The use of motor and cognitive dual-task quantitative assessment on subjects with mild cognitive impairment: a systematic review. Mech Ageing Dev. 2021;193:111393. doi:10.1016/j.mad.2020.111393
19. Raffegeau TE, Krehbiel LM, Kang N, et al. A meta-analysis: parkinson’s disease and dual-task walking. Parkinsonism Relat Disord. 2019;62:28–35. doi:10.1016/j.parkreldis.2018.12.012
20. Hamacher D, Hamacher D, Herold F, Schega L. Are there differences in the dual-task walking variability of minimum toe clearance in chronic low back pain patients and healthy controls? Gait Posture. 2016;49:97–101. doi:10.1016/j.gaitpost.2016.06.026
21. Hemmati L, Rojhani-Shirazi Z, Malek-Hoseini H, Mobaraki I. Evaluation of static and dynamic balance tests in single and dual task conditions in participants with nonspecific chronic low back pain. J Chiropr Med. 2017;16:189–194. doi:10.1016/j.jcm.2017.06.001
22. Karimi GAS, Akhbari B, Salavati M. Reliability of postural control during double-leg standing in subjects with nonspecific chronic low back pain: dual-task paradigm and manipulated visual and somatosensory inputs. J Bodyw Mov Ther. 2021;26:49–56. doi:10.1016/j.jbmt.2020.09.005
23. Lacour M, Bernard-Demanze L, Dumitrescu M. Posture control, aging, and attention resources: models and posture-analysis methods. Neurophysiol Clin. 2008;38:411–421. doi:10.1016/j.neucli.2008.09.005
24. Norrie JP, Larson DJ, Brown S. Think about it: cognitive-motor dual-tasking affects sub-regional spine responses to unexpected trunk perturbations. Hum Mov Sci. 2021;76:102766. doi:10.1016/j.humov.2021.102766
25. Ge L, Yu Q, Wang C, et al. How cognitive loads modulate the postural control of older women with low back pain? BMC Geriatr. 2021;21:82. doi:10.1186/s12877-021-02025-z
26. Moseley GL, Nicholas MK, Hodges PW. Pain differs from non-painful attention-demanding or stressful tasks in its effect on postural control patterns of trunk muscles. Exp Brain Res. 2004;156:64–71. doi:10.1007/s00221-003-1766-0
27. Van Daele U, Hagman F, Truijen S, Vorlat P, Van Gheluwe B, Vaes P. Decrease in postural sway and trunk stiffness during cognitive dual-task in nonspecific chronic low back pain patients, performance compared to healthy control subjects. Spine. 2010;35:583–589. doi:10.1097/BRS.0b013e3181b4fe4d
28. Vuillerme N, Nougier V, Teasdale N. Effects of a reaction time task on postural control in humans. Neurosci Lett. 2000;291:77–80. doi:10.1016/S0304-3940(00)01374-4
29. Huxhold O, Li SC, Schmiedek F, Lindenberger U. Dual-tasking postural control: aging and the effects of cognitive demand in conjunction with focus of attention. Brain Res Bull. 2006;69:294–305. doi:10.1016/j.brainresbull.2006.01.002
30. Legrand A, Bui-Quoc E, Doré-Mazars K, Lemoine C, Gérard CL, Bucci MP. Effect of a dual task on postural control in dyslexic children. PLoS One. 2012;7:e35301. doi:10.1371/journal.pone.0035301
31. Rowley KM, Winstein CJ, Kulig K. Persons in remission from recurrent low back pain alter trunk coupling under dual-task interference during a dynamic balance task. Exp Brain Res. 2020;238:957–968. doi:10.1007/s00221-020-05772-4
32. Lundin-Olsson L, Nyberg L, Gustafson Y. ”stops walking when talking” as a predictor of falls in elderly people. Lancet. 1997;349:617. doi:10.1016/S0140-6736(97)24009-2
33. Brown LA, Sleik RJ, Polych MA, Gage WH. Is the prioritization of postural control altered in conditions of postural threat in younger and older adults? J Gerontol a Biol Sci Med Sci. 2002;57:M785–92. doi:10.1093/gerona/57.12.M785
34. Bloem BR, Grimbergen YA, van Dijk JG, Munneke M. The “posture second” strategy: a review of wrong priorities in Parkinson’s disease. J Neurol Sci. 2006;248:196–204. doi:10.1016/j.jns.2006.05.010
35. Hemmati L, Piroozi S, Rojhani-Shirazi Z. Effect of dual tasking on anticipatory and compensatory postural adjustments in response to external perturbations in individuals with nonspecific chronic low back pain: electromyographic analysis. J Back Musculoskelet Rehabil. 2018;31:489–497. doi:10.3233/BMR-170992
36. Salavati M, Mazaheri M, Negahban H, et al. Effect of dual-tasking on postural control in subjects with nonspecific low back pain. Spine. 2009;34:1415–1421. doi:10.1097/BRS.0b013e3181a3a917
37. Shanbehzadeh S, Salavati M, Talebian S, Khademi-Kalantari K, Tavahomi M. Attention demands of postural control in non-specific chronic low back pain subjects with low and high pain-related anxiety. Exp Brain Res. 2018;236:1927–1938. doi:10.1007/s00221-018-5267-6
38. Sherafat S, Salavati M, Takamjani IE, et al. Effect of dual-tasking on dynamic postural control in individuals with and without nonspecific low back pain. J Manipulative Physiol Ther. 2014;37:170–179. doi:10.1016/j.jmpt.2014.02.003
39. Shih HS, Winstein CJ, Kulig K. Young adults with recurrent low back pain demonstrate altered trunk coordination during gait independent of pain status and attentional demands. Exp Brain Res. 2021;239:1937–1949. doi:10.1007/s00221-021-06106-8
40. Schega L, Kaps B, Broscheid KC, et al. Effects of a multimodal exercise intervention on physical and cognitive functions in patients with chronic low back pain (multimove): study protocol for a randomized controlled trial. BMC Geriatr. 2021;21:151. doi:10.1186/s12877-021-02093-1
41. Peters ML, Vlaeyen JW, Kunnen AM. Is pain-related fear a predictor of somatosensory hypervigilance in chronic low back pain patients? Behav Res Ther. 2002;40:85–103. doi:10.1016/S0005-7967(01)00005-5
42. Mazaheri M, Salavati M, Negahban H, Sanjari MA, Parnianpour M. Postural sway in low back pain: effects of dual tasks. Gait Posture. 2010;31:116–121. doi:10.1016/j.gaitpost.2009.09.009
43. Claeys K, Brumagne S, Dankaerts W, Kiers H, Janssens L. Decreased variability in postural control strategies in young people with non-specific low back pain is associated with altered proprioceptive reweighting. Eur J Appl Physiol. 2011;111:115–123. doi:10.1007/s00421-010-1637-x
44. Ito T, Sakai Y, Morita Y, et al. Proprioceptive weighting ratio for balance control in static standing is reduced in elderly patients with non-specific low back pain. Spine. 2018;43:1704–1709. doi:10.1097/BRS.0000000000002817
45. Drozdova-Statkeviciene M, Cesnaitiene VJ, Pukenas K, Levin O, Masiulis N. Sway regularity and sway activity in older adults’ upright stance are differentially affected by dual task. Neurosci Lett. 2018;666:153–157. doi:10.1016/j.neulet.2017.12.054
46. Mohammadi M, Ghamkhar L, Alizadeh A, Shaabani M, Salavati M, Kahlaee AH. Comparison of the reliance of the postural control system on the visual, vestibular and proprioceptive inputs in chronic low back pain patients and asymptomatic participants. Gait Posture. 2021;85:266–272. doi:10.1016/j.gaitpost.2021.02.010
47. Macdonald D, Moseley GL, Hodges PW. People with recurrent low back pain respond differently to trunk loading despite remission from symptoms. Spine. 2010;35:818–824. doi:10.1097/BRS.0b013e3181bc98f1
48. Al-Yahya E, Dawes H, Smith L, Dennis A, Howells K, Cockburn J. Cognitive motor interference while walking: a systematic review and meta-analysis. Neurosci Biobehav Rev. 2011;35:715–728. doi:10.1016/j.neubiorev.2010.08.008
49. Lovden M, Schaefer S, Pohlmeyer AE, Lindenberger U. Walking variability and working-memory load in aging: a dual-process account relating cognitive control to motor control performance. J Gerontol B Psychol Sci Soc Sci. 2008;63:P121–8. doi:10.1093/geronb/63.3.P121
50. Mak L, Yeh TT, Boulet J, Cluff T, Balasubramaniam R. Interaction between delayed visual feedback and secondary cognitive tasks on postural control in older adults. Movement Sport Sci. 2011;74:81–88. doi:10.3917/sm.074.0081
51. Smith JA, Gordon J, Kulig K. The influence of divided attention on walking turns: effects on gait control in young adults with and without a history of low back pain. Gait Posture. 2017;58:498–503. doi:10.1016/j.gaitpost.2017.09.019
52. Paolucci T, Fusco A, Iosa M, et al. The efficacy of a perceptive rehabilitation on postural control in patients with chronic nonspecific low back pain. Int J Rehabil Res. 2012;35:360–366. doi:10.1097/MRR.0b013e328356427c
53. Ng SK, Urquhart DM, Fitzgerald PB, et al. Neural activity during cognitive reappraisal in chronic low back pain: a preliminary study. Scand J Pain. 2021;21:586–596. doi:10.1515/sjpain-2020-0146
54. van der Leeuw G, Eggermont LH, Shi L, et al. Pain and cognitive function among older adults living in the community. J Gerontol a Biol Sci Med Sci. 2016;71:398–405. doi:10.1093/gerona/glv166
55. Stewart DM, Gregory DE. The use of intermittent trunk flexion to alleviate low back pain during prolonged standing. J Electromyogr Kinesiol. 2016;27:46–51. doi:10.1016/j.jelekin.2016.01.007
56. Ehsani F, Arab AM, Jaberzadeh S, Salavati M. Ultrasound measurement of deep and superficial abdominal muscles thickness during standing postural tasks in participants with and without chronic low back pain. Man Ther. 2016;23:98–105. doi:10.1016/j.math.2016.01.003
57. Sipko T, Kuczynski M. Intensity of chronic pain modifies postural control in low back patients. Eur J Pain. 2013;17:612–620. doi:10.1002/j.1532-2149.2012.00226.x
58. Sipko T, Glibowski E, Barczyk-Pawelec K, Kuczynski M. The effect of chronic pain intensity on sit-to-stand strategy in patients with herniated lumbar disks. J Manipulative Physiol Ther. 2016;39:169–175. doi:10.1016/j.jmpt.2016.02.014
59. Sipko T, Glibowski E, Kuczynski M. Acute effects of proprioceptive neuromuscular facilitation exercises on the postural strategy in patients with chronic low back pain. Complement Ther Clin Pract. 2021;44:101439. doi:10.1016/j.ctcp.2021.101439
60. Zhang C, Zhang Z, Li Y, et al. Pain catastrophizing is related to static postural control impairment in patients with nonspecific chronic low back pain: a cross-sectional study. Pain Res Manag. 2020;2020:9629526. doi:10.1155/2020/9629526
61. Rum L, Brasiliano P, Vannozzi G, Laudani L, Macaluso A. Non-specific chronic low back pain elicits kinematic and neuromuscular changes in walking and gait termination. Gait Posture. 2021;84:238–244. doi:10.1016/j.gaitpost.2020.12.005
62. Marshall P, Murphy B. Delayed abdominal muscle onsets and self-report measures of pain and disability in chronic low back pain. J Electromyogr Kinesiol. 2010;20:833–839. doi:10.1016/j.jelekin.2009.09.005
63. Lin D, Nussbaum MA, Seol H, Singh NB, Madigan ML, Wojcik LA. Acute effects of localized muscle fatigue on postural control and patterns of recovery during upright stance: influence of fatigue location and age. Eur J Appl Physiol. 2009;106:425–434. doi:10.1007/s00421-009-1026-5
64. Hlaing SS, Puntumetakul R, Wanpen S, Boucaut R. Balance control in patients with subacute non-specific low back pain, with and without lumbar instability: a cross-sectional study. J Pain Res. 2020;13:795–803. doi:10.2147/JPR.S232080
65. Mok NW, Brauer SG, Hodges PW. Failure to use movement in postural strategies leads to increased spinal displacement in low back pain. Spine. 2007;32:E537–43. doi:10.1097/BRS.0b013e31814541a2
66. Da SR, Vieira ER, Carvalho CE, Oliveira MR, Amorim CF, Neto EN. Age-related differences on low back pain and postural control during one-leg stance: a case-control study. Eur Spine J. 2016;25:1251–1257. doi:10.1007/s00586-015-4255-9
67. Da SR, Vieira ER, Leonard G, et al. Age- and low back pain-related differences in trunk muscle activation during one-legged stance balance task. Gait Posture. 2019;69:25–30. doi:10.1016/j.gaitpost.2019.01.016
68. Pinto SM, Cheung J, Samartzis D, et al. Differences in proprioception between young and middle-aged adults with and without chronic low back pain. Front Neurol. 2020;11:605787. doi:10.3389/fneur.2020.605787
69. Marinho-Buzelli AR, Rouhani H, Masani K, Verrier MC, Popovic MR. The influence of the aquatic environment on the control of postural sway. Gait Posture. 2017;51:70–76. doi:10.1016/j.gaitpost.2016.09.009
70. Bayartai ME, Ferreira PH, Pappas E, et al. Genetic and environmental effects on lumbar posture, flexibility and motion control in healthy adults. Musculoskelet Sci Pract. 2020;50:102253. doi:10.1016/j.msksp.2020.102253
71. Helmich I, Berger A, Lausberg H. Neural control of posture in individuals with persisting postconcussion symptoms. Med Sci Sports Exerc. 2016;48:2362–2369. doi:10.1249/MSS.0000000000001028
72. Stins JF, Michielsen ME, Roerdink M, Beek PJ. Sway regularity reflects attentional involvement in postural control: effects of expertise, vision and cognition. Gait Posture. 2009;30:106–109. doi:10.1016/j.gaitpost.2009.04.001
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.