")
Back to Journals » Infection and Drug Resistance » Volume 15
Polymyxin B-Based Regimens for Patients Infected with Carbapenem-Resistant Gram-Negative Bacteria: Clinical and Microbiological Efficacy, Mortality, and Safety
Authors Qu J , Qi TT, Qu Q, Long WM , Chen Y, Luo Y, Wang Y
Received 20 January 2022
Accepted for publication 11 March 2022
Published 22 March 2022 Volume 2022:15 Pages 1205—1218
DOI https://doi.org/10.2147/IDR.S357746
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Suresh Antony
Jian Qu,1,2 Ting-Ting Qi,1,2 Qiang Qu,3,4 Wen-Ming Long,5 Ying Chen,6 Yue Luo,7 Ying Wang1,2
1Department of Pharmacy, The Second Xiangya Hospital, Central South University, Changsha, 410011, People’s Republic of China; 2Institute of Clinical Pharmacy, Central South University, Changsha, 410011, People’s Republic of China; 3Department of Pharmacy, Xiangya Hospital, Central South University, Changsha, 410078, People’s Republic of China; 4National Clinical Research Center for Geriatric Disorders, Xiangya Hospital, Central South University, Changsha, 410078, People’s Republic of China; 5Department of Pharmacy, Jingzhou District, Second People’s Hospital of Huaihua City, Huaihua, 418400, People’s Republic of China; 6Department of Pharmacy, Wuhan University, Renmin Hospital, Wuhan, 430060, People’s Republic of China; 7Department of Pharmacy, The People’s Hospital of Liuyang, Liuyang, 410300, People’s Republic of China
Correspondence: Ying Wang, Department of Pharmacy, The Second Xiangya Hospital, Central South University, Institute of Clinical Pharmacy, Central South University, No. 139 Middle Renmin Road, Changsha, 410011, People’s Republic of China, Tel +86-15173198700, Fax +86-731-85292072, Email [email protected]
Background: The increasing prevalence of carbapenem-resistant Gram-negative bacteria (CR-GNB) represents a global healthcare crisis. This study explored the efficacy and safety of Polymyxin B (PMB)-based regimens and factors influencing their effectiveness.
Methods: Patients with CR-GNB infections treated with PMB for more than three days were enrolled in this retrospective study from 1st June 2018 to 30th April 2020. Data were collected on patient characteristics, bacterial culture, and drug-sensitivity test results; anti-infection treatment regimens, particularly details of PMB use; and adverse drug reactions. Clinical and microbiological efficacy, mortality, and safety of PMB-based regimens in CR-GNB infected patients were evaluated. Univariate analysis and multivariate logistic regression analyses were used to assess factors influencing efficacy and mortality.
Results: A total of 373 CR-GNB strains were cultured from 268 patients. About 41.04% of patients used PMB loading dose of 1.01 (0.84– 1.69) mg/kg. Maintenance dose was 0.85 (0.82– 1.00) mg/kg q12h. The clinical efficacy rate was 36.57% (98/268), the total bacterial clearance rate of PMB was 39.42%, and the all-cause mortality rate was 33.96%. The adverse drug reaction rate was 19.58%, among which the incidence of renal toxicity was highest (8.21%). Multivariate logistic regression analysis showed that clinical efficacy, bacterial clearance rate, and all-cause mortality were associated with patient-related facts, including mechanical ventilation use, underlying diseases (such as respiratory disease), the type and site of CR-GNB infection, and PMB administration timing and loading dose.
Conclusion: PMB is a relatively safe and effective antibiotic drug for treatment of critically ill patients with CR-GNB infection; however, PMB use should be subject to guidelines recommendations for early administration, loading administration, and adequate administration, which could help to improve the clinical efficacy, microbiological efficacy, and mortality.
Keywords: polymyxin B, carbapenem-resistant Gram-negative bacteria, clinical efficacy, bacterial elimination, mortality, adverse effect
Introduction
The increasing prevalence of carbapenem-resistant Gram-negative bacteria (CR-GNB) represents a global healthcare crisis.1 In particular, carbapenem-resistant Enterobacteriaceae (CRE) has been listed as an urgent threat by the World Health Organization.2 Furthermore, according to a report from the China Antimicrobial Resistance Surveillance System in 2019, the detection rates of carbapenem-resistant Klebsiella pneumonia (CRKP), carbapenem-resistant Pseudomonas aeruginosa (CRPA), and carbapenem-resistant Acinetobacter baumannii (CRAB) were 10.90%, 19.10%, and 56%, respectively.3,4
Therapeutic options against CR-GNB infections include novel beta-lactam/beta-lactamase inhibitors such as ceftazidime/avibactam, cefiderocol, plazomicin, eravacycline, and polymyxins, such as colistin and polymyxin B (PMB).5,6 PMB (but not colistin) and ceftazidime/avibactam are currently available on the market in mainland China, which are used to treat infections with clinically resistant bacteria.7 Others were not available in mainland China. To date, research into the pharmacokinetic/pharmacodynamic (PK/PD) features of PMB is limited, and there remains a lack of consensus on the most appropriate dosing regimen for PMB.8 The international consensus guidelines for the optimal use of the polymyxins suggested that an average steady-state plasma concentration of PMB of 2–4 mg/L may be acceptable in terms of toxicity;9 however, there are no reports of large-scale detection of PMB concentrations in clinical practice. The current recommended loading dose of PMB is 2.0–2.5mg/kg (equivalent to 20,000–25,000 IU/kg), with a maintenance dose of 1.25–1.5 mg/kg every 12 h, for patients with severe infections;9 however, many patients did not get the guideline recommended dose of PMB in clinical treatment.
There is limited research on the clinical and microbiological efficacy, mortality, and safety of PMB. A retrospective study of 40 patients found that early use of PMB reduces mortality resulting from CRKP bloodstream infection.10 Another investigation reported that a sizable proportion of patients with CR-GNB infection treated with high-dose PMB developed acute kidney injury (AKI), suggesting that the potential benefits of treatment must be weighed against an increased risk of AKI.11 A retrospective analysis of 39 patients with sepsis also showed that PMB could be an effective treatment option for patients with severe infection with extensively drug-resistant Gram-negative bacteria;12 however, the roles of patient characteristics, different CR-GNB infections, and infection sites, as well as details of PMB use, such as presence or absence of loading dose, and the efficacy of PMB in combination regimens, are poorly-investigated. In this study, we reviewed clinical data from 268 patients with CR-GNB infections treated with PMB-based regimens to explore the efficacy and safety of PMB-based regimens and the factors influencing these.
Patients and Methods
Ethics
The Ethics Committees of the Second Xiangya Hospital of Central South University approved the study protocol (LYF-2020021). The study was conducted according to the ethical standards of the Helsinki Declaration (1964). Patients gave their written informed consent to have their data included in this study.
Patients
This retrospective study involved patients admitted to the Second Xiangya Hospital of Central South University (a 3500-bed general hospital) from 1st June 2018 to 30th April 2020. The inclusion criteria were as follows: (1) CR-GNB infection confirmed by bacterial culture and drug sensitivity test; (2) a history of medication with PMB (Shanghai Number 1 Biochemical & Pharmaceuticals, Shanghai, China) for treatment ≥ 3 days; and (3) underwent infection index (such as white blood cell count, c-reactive protein, Procalcitonin, erythrocyte sedimentation rate) assessment at the end of the treatment course. The exclusion criteria were as follows: (1) < 18 years old or pregnant; (2) no CR-GNB was detected during the treatment; (3) the treatment efficacy could not be evaluated.
Clinical Data Collection
Patients enrolled according to the inclusion and exclusion criteria were followed up until discharge or death. Data extracted from patient inpatient charts and electronic records included demographics, such as age, sex, baseline comorbidities, type of infections, type of CR-GNB, Acute Physiology and Chronic Health Evaluation II (APACHE II) score, details of PMB use (loading dose, daily dose based on total body weight, duration of treatment, and cumulative PMB dose), concomitant infections and antibiotic use, and probable adverse effects of PMB.
Outcomes and Definitions
Indicators used to evaluate the efficacy of PMB in this study included clinical treatment efficacy, microbiological efficacy (bacterial clearance after 7-days and at the end of PMB treatment), and in-hospital all-cause mortality.
Clinical efficacy was defined as meeting all of the following conditions: being hemodynamically stable without the need for vasopressors; body temperature <37.5°C within 72 hours; improvements of microbiologic and parameters including APACHE II score, biochemistry indicators of infection (White blood cell count in adults ≤ 109, C-reactive protein ≤ 10mg/L, Procalcitonin < 0.05ng/mL, erythrocyte sedimentation rate < 15mm/h), twice negative culture results at least, control of infection symptoms and clinician documented improvements at the end of treatment.13,14 Clinical treatment failure was defined as patients who failed to meet any clinical efficacy criteria, stopped treatment with low blood pressure, or died in hospital.14
Microbiological efficacy was defined as the clearance of CR-GNB within 7 days, or within the total course of PMB, demonstrated by negative microbial culture results of samples from the same site after PMB treatment.
In-hospital all-cause mortality was defined as all-cause death or stopped treatments with blood pressure less than 90/60 mmHg under pressure medication maintenance, who were transitioned to hospice.
Adverse reactions (ADRs) to PMB were defined as harmful reactions unrelated to the purpose of treatment that emerged after PMB use, including nerve-muscle blockade, nephrotoxicity, and skin pigmentation. Nephrotoxicity was evaluated based on the risk, injury, failure, or loss of kidney function and end-stage kidney disease criteria (RIFLE).15
Microbiology
Laboratory physicians tested drug sensitivity by the broth microdilution method using analytical instruments. Bacteria isolates were identified using VITEK®2 system (bioMérieux, Marcy-l’Étoile, France). Based on the Clinical and Laboratory Standards Institute recommendations, the minimum inhibitory concentration (MIC) values were also determined using a VITEK®2 system (bioMérieux, Marcy-l’Étoile, France). Carbapenem resistance was defined as MIC value for imipenem and meropenem ≥ 4 mg/L. Meanwhile, according to the European Committee on Antimicrobial Susceptibility Testing (EUCAST, v10.0, 2020), “MIC >2 mg/L” represented bacterial resistance to PMB.16 “MIC ≤2 mg/L” represented the sensitivity of Enterobacteriaceae and Acinetobacter to tigecycline, and “MIC ≥8 mg/L” represented tigecycline resistance according to US Food and Drug Administration (FDA) standards (https://www.accessdata.fda.gov/drugsatfda_docs/label/2013/021821s026s031lbl.pdf). Since no TGC MIC breakpoint was available for Acinetobacter spp. We used the same breakpoints defined by the FDA for Enterobacteriaceae for the interpretation of susceptibility testing results obtained for A. baumannii.
Statistical Processing
Statistical analyses were undertaken using SPSS v21.0 (IBM, Armonk, NY, USA). Quantitative data are represented by median and interquartile range or mean ± standard deviation. For comparisons between two groups, t-tests were used for normally distributed data, and Mann-Whitney non-parametric tests were used for non-normally distributed data. Categorical data are expressed as numbers of cases and percentages and were analyzed by chi-square test. Multivariate logistic regression was used to assess potential independent predictors of PMB efficacy. Factors with p-values < 0.1 by univariate analysis were entered into the multivariate logistic analysis. P < 0.05 was considered significant. Patients with lean or normal body weight are calculated according to their actual body weight, and overweight patients are calculated according to their adjusted body weight. Adjusted body weight was calculated as ideal body weight + 0.4 (actual body weight - ideal body weight).17
Results
Clinical Characteristics
A total of 268 patients with CR-GNB infection were enrolled; general patient information is listed in Table 1. The median age of patients was 57.5 years (range, 46–71 years). One hundred eighty-two patients (67.91%) were admitted to the ICU, and 144 cases (53.73%) were maintained with vasoactive drugs. Patient comorbidities were as follows: respiratory diseases, 226 cases (84.33%); cardiovascular and cerebrovascular diseases, 169 cases (63.06%); kidney-related diseases, 120 cases (44.78%); hepatobiliary system diseases, 67 cases (25.00%); gastrointestinal and pancreatic disease, 52 cases (19.40%); malnutrition, 34 cases (12.69%); and diabetes, 44 cases (16.42%). In addition, there were 254 cases (94.78%) had respiratory tract infection, 84 cases (31.34%) bloodstream infection, 29 (10.82%) cases of urinary system infection, 17 (6.34%) cases of central nervous system infection, 30 cases (11.19%) of abdominal infection, and 21 cases (7.84%) of skin and soft tissue infection.
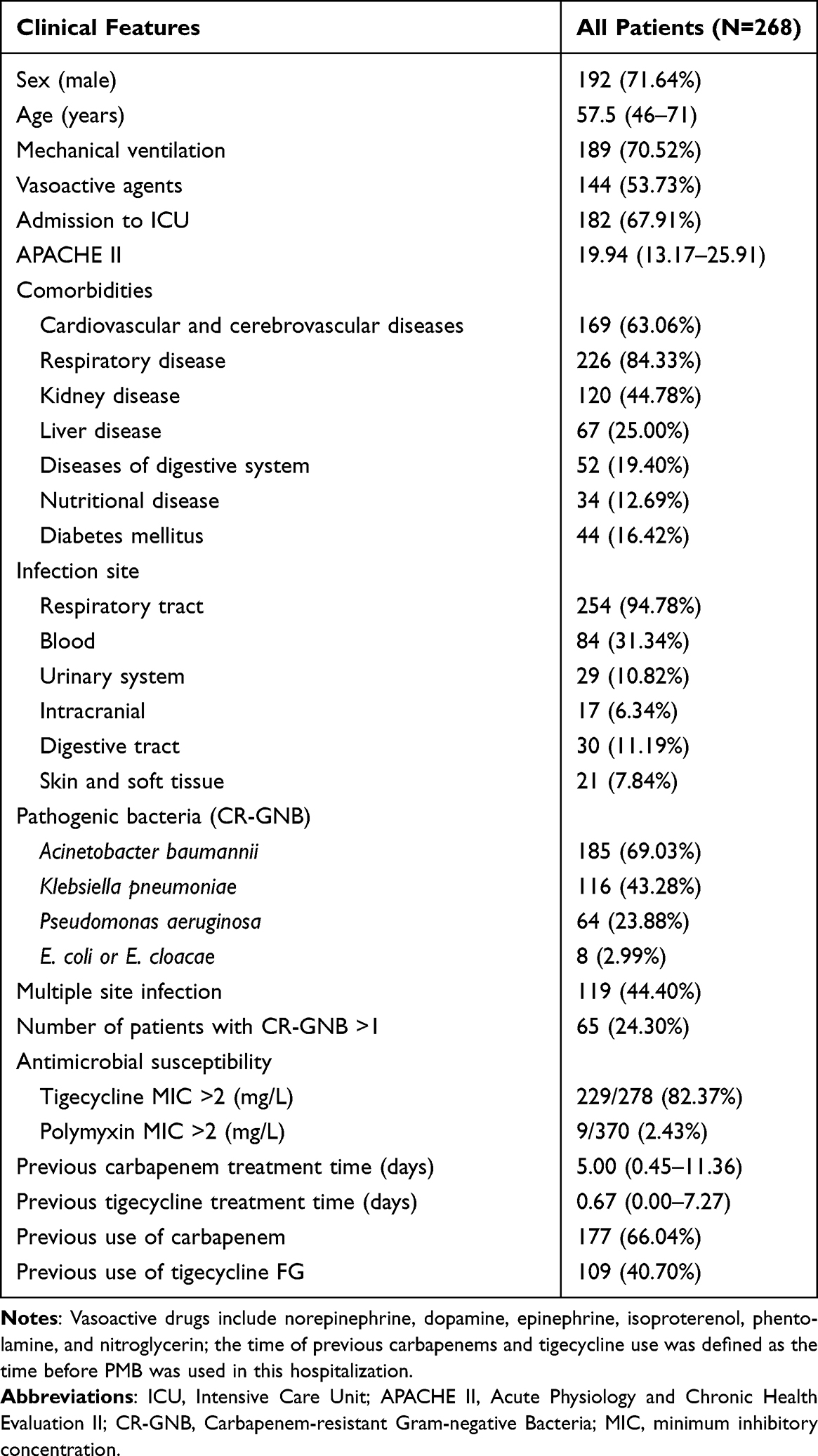 |
Table 1 Demographic and Clinical Characteristics of the Study Cohort |
Pathogenic Examination
Bacterial culture and drug sensitivity tests confirmed that 268 patients were infected by CR-GNB, and a total of 373 CR-GNB samples were isolated. Among isolated strains were 185 of CRAB (49.60%), 116 of CRKP (31.10%), 64 of CRPA (17.16%), and 8 of carbapenem-resistant E. coli and E. cloacae (2.14%). Drug sensitivity analysis results showed that the tigecycline MICs of 229 strains (82.37%) were > 2 mg/L, while the PMB MICs of 9 strains (2.43%) were > 2 mg/L. The numbers of patients with multi-site infection and multi-CR-GNB infection were 119 (44.40%) and 65 (24.30%), respectively (Table 1).
Medications and Outcomes
Among the 268 patients, 177 cases (66.04%) had previously used carbapenems, for a median duration of 5 days and 109 cases (40.70%) had previously used tigecycline, for a median duration of 0.67 days. Further, of the 268 patients treated with PMB, PMB treatment was combined with tigecycline, carbapenems, β-lactams, glycopeptides, or other drugs (such as aminoglycosides and quinolones) in 84 (31.34%), 75 (27.99%), 90 (33.58%), 44 (16.24%), and 41 (15.30%) cases, respectively. A PMB loading dose was used in 110/268 patients (41.04%); median loading dose was 1.01 mg/kg, while 59 patients (22.01%) received a loading dose ≥ 2.0 mg/kg. Maintenance dose was calculated based on body weight; median maintenance dose was 0.85 mg/kg, and 39 cases (14.55%) had a maintenance dose > 1.25 mg/kg. The median cumulative dose was 925.57 mg, and the median duration of treatment was 9.67 days. After the course of PMB treatment, 136 strains (39.42%) were cleared. Ninety-six strains (29.36%) were cleared within seven days. In 98 cases (36.57%), clearance was clinically effective, and the median time for bacterial clearance was 6.67 days. All-cause mortality (including in-hospital deaths and critically ill patients who stopped treatment and were discharged) was 36.19% (97 cases). The median duration of hospitalization was 36 days (Table 2).
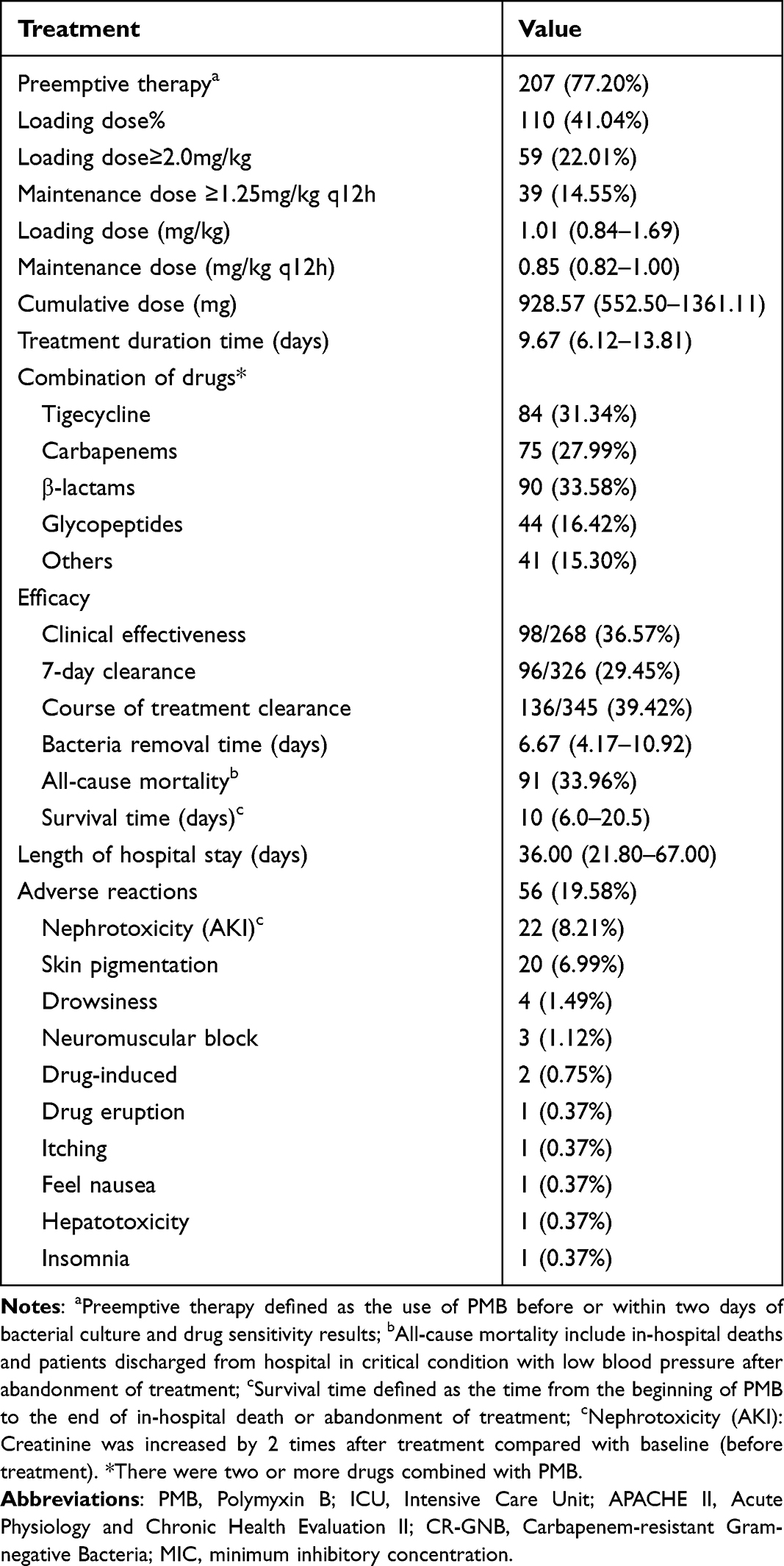 |
Table 2 Regimens, Adverse Reactions and Outcomes |
Evaluation Results of Factors Associated with PMB Efficacy
Clinical Efficacy
According to our definition of PMB clinical efficacy, there were 98 patients in which treatment was clinically effective and 170 in which it was clinically ineffective; hence, the effective clinical rate was 36.57%. Risk factors for poor clinical efficacy after PMB treatment, determined by analysis of 268 patients, are listed in Table 3. The results of the univariate analysis showed that older age, treatment with vasoactive agents, mechanical ventilation use, admission to ICU, comorbid respiratory disease, comorbid liver disease, bloodstream infection, different CR-GNB infection, multiple site infections, more than one CR-GNB infection, treatment duration, cumulative dose of PMB, and regimen combining carbapenems and PMB were risk factors for clinical efficacy of PMB treatment (P < 0.05). The portion of CRAB in the clinical success group is higher in the failure group, while the portion of CRKP in the clinical success group is lower in the failure group (p=0.013, p=0.04). Moreover, binary logistic regression showed that vasoactive agent and mechanical ventilation use, admission to ICU, and respiratory disease were independent risk factors for poor clinical efficacy of PMB treatment (all P < 0.05); Loading dose ≥ 2.0 mg/kg of PMB was an independent protective factor for poor clinical efficacy (P < 0.05).
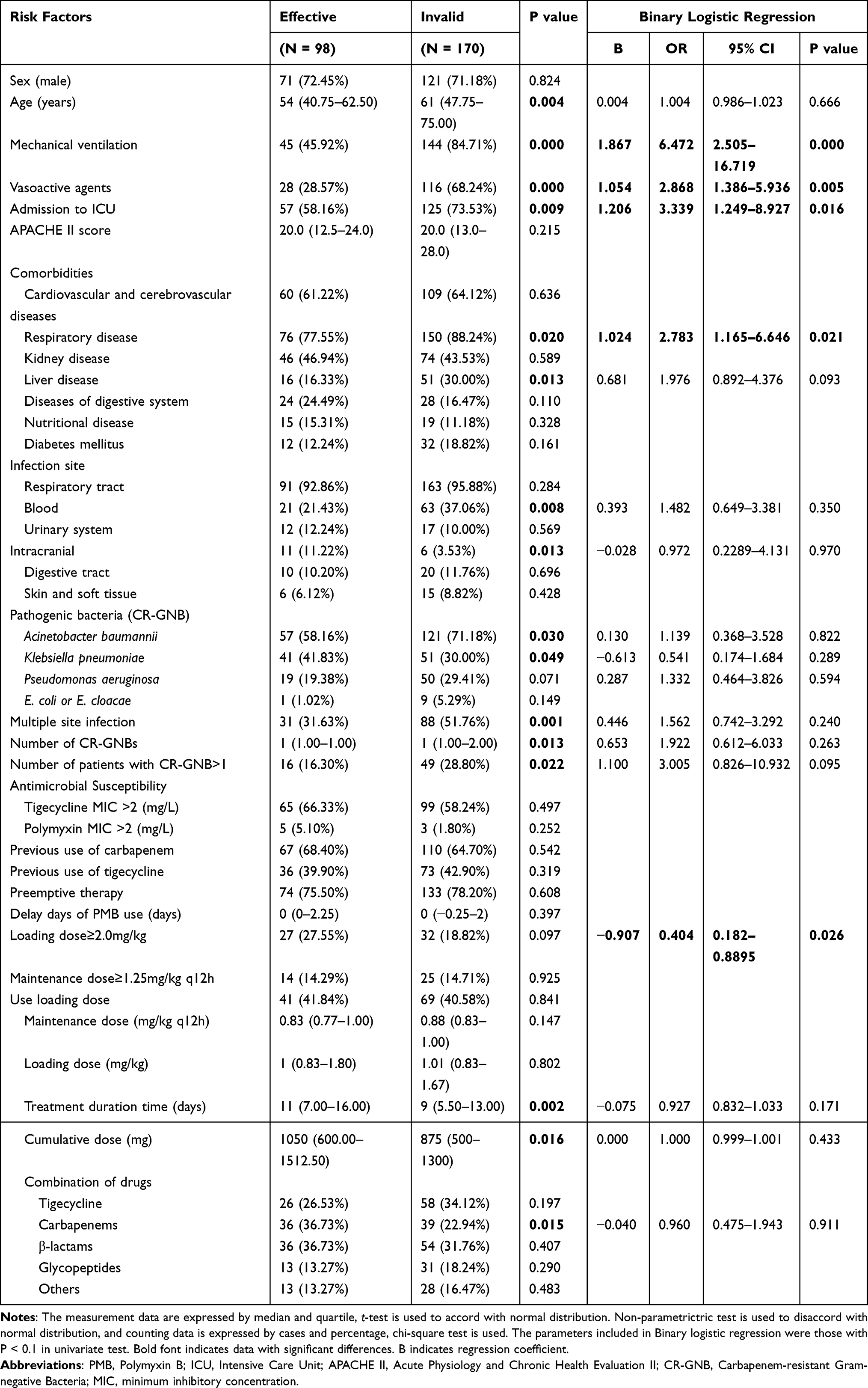 |
Table 3 Analysis of the Risk Factors of Poor Clinical Efficacy After PMB Treatment |
Microbiological Efficacy
To identify factors influencing the total bacterial clearance rate of PMB, we compared the characteristics and regimens of patients with CR-GNB that was cleared with those of patients whose infection was not cleared after PMB treatment (Table 4). After the treatment with PMB, 136 CR-GNB strains were cleared and residual CR-GNB was detected in 209 patients.
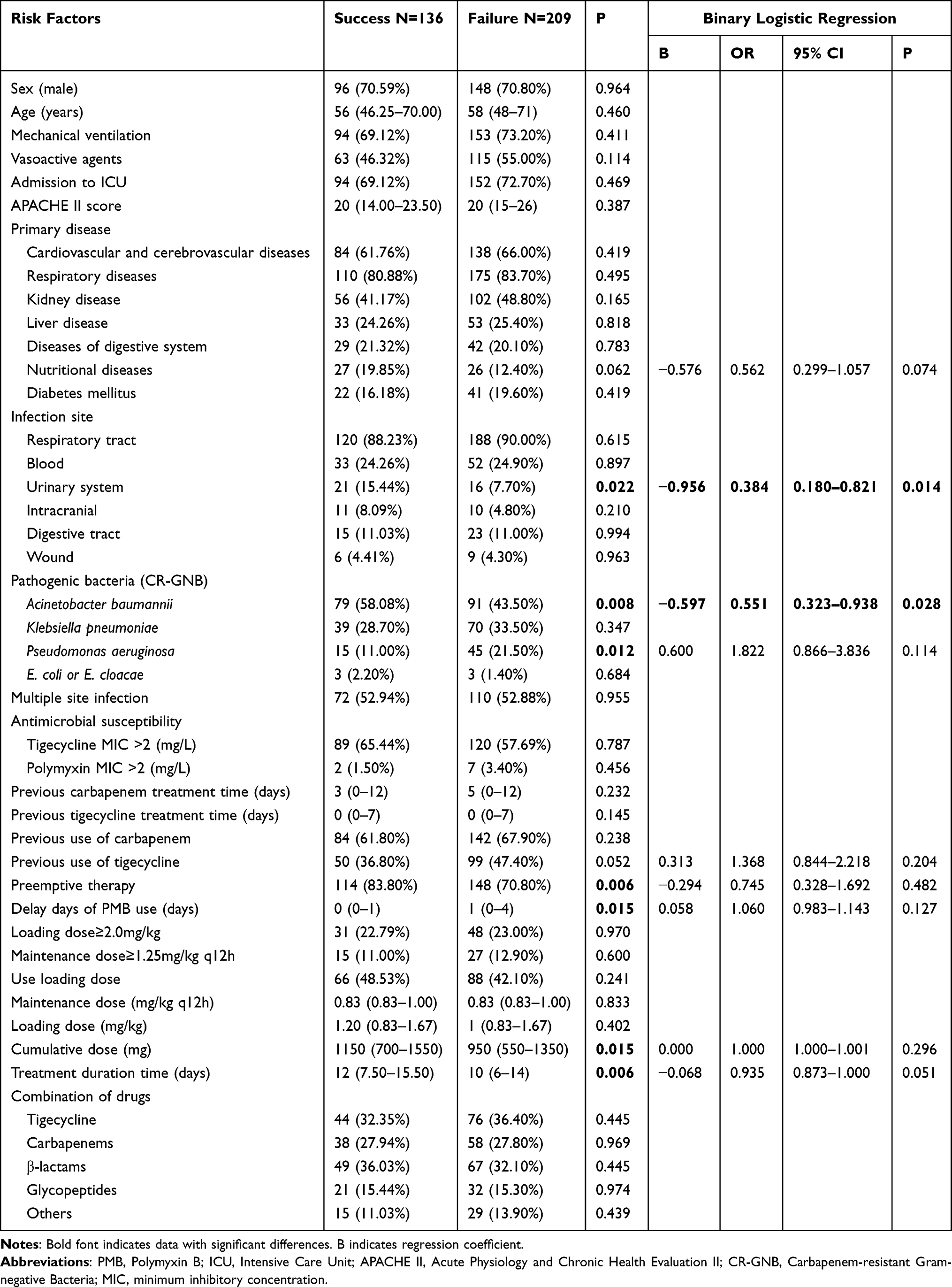 |
Table 4 Analysis of Risk Factors of CR-GNB Clearance Failure After PMB Treatment |
Univariate analysis results showed that urinary tract infection, different CR-GNB infection, preemptive therapy, PMB use delay days, treatment duration, and cumulative dose of PMB were related to CR-GNB clearance after PMB treatment (P < 0.05). The portion of CRAB in the microbiological cleaned group is lower in the microbiological failure groups, while the portion of CRPA in the microbiological cleaned group is lower in the microbiological failure clean group (p=0.008, p=0.012, respectively). In addition, binary logistic regression results also confirmed that urinary tract infection and CRAB infection were independent risk factors that could influence bacterial clearance by PMB treatment.
We also performed the univariate analysis and binary logistic regression analyses to identify factors influencing the PMB 7-day bacterial clearance rate (Table S1). Binary logistic regression results showed that nutritional diseases, urinary tract infection, CRAB infection, and preemptive therapy were related to the 7-day bacterial clearance rate of PMB (P<0.05).
Mortality
After evaluating the outcomes of patients treated with PMB, we analyzed the risk factors related to all-cause mortality. According to our definition, there were 177 surviving and 91 dead patients, with an all-cause mortality rate of 33.96%. Patients who died were older and more likely to have undergone mechanical ventilation, been treated with vasoactive agents, and been admitted to the ICU (P < 0.05) (Table 5). Further, patients who died had more underlying diseases, such as liver disease (P = 0.006). The dead group had 41.8% CR-GNB BSI compared with 26.0% in survivors (P=0.008), and Escherichia coli or Enterobacter cloacae infections were more common in patients who died (7.7% vs.1.7%, P = 0.003). Furthermore, multiple site infections were more frequent among patients that died (56.0% vs 38.4%).
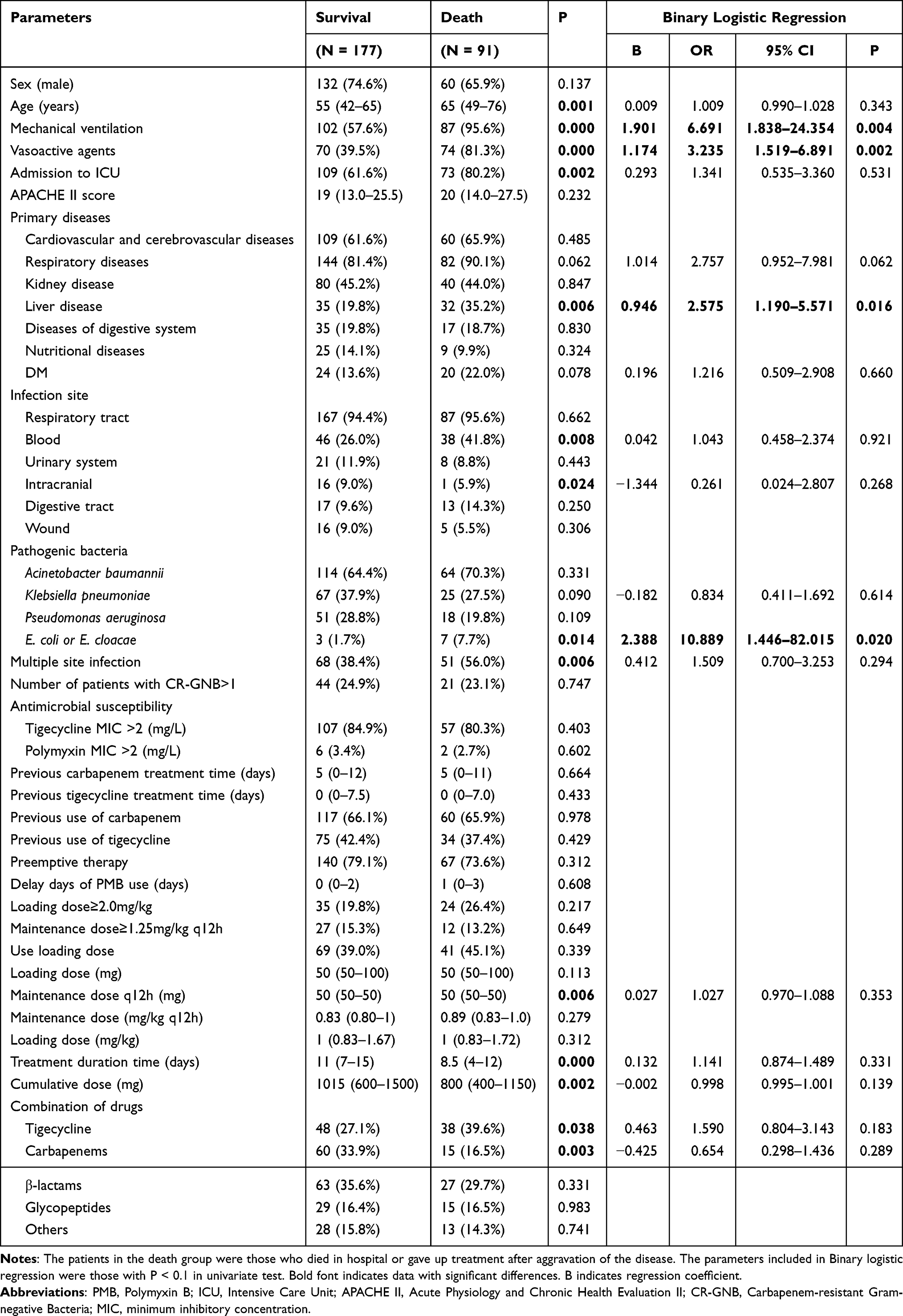 |
Table 5 Analysis of Risk Factors of All-Cause Mortality After PMB Treatment |
Regarding PMB treatment, maintenance dose (mg), treatment duration, cumulative dose (mg), and combination of drugs, such as tigecycline and carbapenems, differed significantly between the patients who survived and those who did not (P < 0.05). Binary logistic regression analysis demonstrated that mechanical ventilation, vasoactive agents, and having liver disease, as well as E. coli or E. cloacae infection, were independent factors associated with all-cause mortality (P < 0.05).
Adverse Drug Reactions
Overall, 56 patients (19.58%) experienced ADRs to PMB treatment during hospitalization. The most prevalent ADR was nephrotoxicity (AKI) (28 cases; 8.21%), followed by skin hyperpigmentation (20 cases; 6.99%), drowsiness (4 cases; 1.49%), and neuromuscular block (3 cases; 1.12%). Moreover, some rare ADRs occurred, including drug-induced fever, drug-induced eruption, pruritus, nausea, general weakness, lethargy, and hepatotoxicity (Table 2).
Discussion
CR-GNB, especially CRE infection, has been flagged as an urgent threat by the World Health Organization.2 In China, CR-GNB infections have been treated with PMB since 2018. In this study, we aimed to explore the efficacy and safety of PMB-based regimens and factors influencing their efficacy. We enrolled 268 patients infected with 373 CR-GNB strains and treated them using PMB-based regimens. After treatment, the overall clinical effective rate was 36.57%, the bacterial clearance rate of PMB was 39.42%, the 7-day bacterial clearance rate was 29.36%, and the all-cause mortality rate was 33.96%. Binary logistic regression analysis showed that use of vasoactive agents and mechanical ventilation, admission to ICU, and having respiratory disease were independent risk factors for poor clinical efficacy after PMB treatment; PMB loading dose ≥ 2.0 mg/kg was an independent protective factor for poor clinical efficacy after PMB treatment. Further, urinary tract infection and CRAB infection were independent risk factors associated with bacterial clearance of PMB treatment. Moreover, mechanical ventilation, vasoactive agents, having liver disease, and E. coli or E. cloacae infection were independent factors associated with all-cause mortality.
The increasing prevalence of infections caused by CR-GNB has led to fewer effective antibiotics, and PMB has been used as a first-line agent to treat infections caused by these pathogens;18 however, information about its pharmacokinetics, efficacy, and safety profile are scarce.18 A previous study investigated the efficacy of PMB and found a treatment success rate of 25.1%,19 which is lower than that reported here; however, the mortality rate described in the previous study (32.8%) is similar to our findings.19 We also investigated potential risk factors for treatment failure and found that vasoactive agents and mechanical ventilation, admission to ICU, and respiratory disease were independent risk factors for clinical efficacy following PMB treatment. Further, patients benefited from a PMB loading dose > 2.0 mg/kg. Recent guidelines recommend a loading dose of 2–2.5 mg/kg of PMB for severely ill patients.9 In this study, the PMB loading dosage was ≥ 2 mg/kg in 22.01% of the cases, while the maintenance dose was ≥ 1.25 mg/kg in 14.55% of cases, which represented a significant deviation from the dose recommended in the literature.9,20 A population pharmacokinetic study of patients with severe infections showed that administration of 1.25 mg/kg (equivalent to 12,500 IU/kg) every 12 h resulted in plasma PMB concentration after the first administration of approximately 56–70% of the observed steady-state concentration.21 Further, the results of a Monte Carlo simulation analysis showed that, at a loading dose of 2.0 mg/kg (equivalent to 20,000 IU/kg), the probability of exposure to steady-state drug levels on the first day is 76%–94%.21
For the combination use of PMB, the international guideline recommended that PMB should be combined with other drugs to treat CR-GNB, including CRAB, CRE, and CRPA.9 A study investigated the colistin versus colistin plus meropenem for the treatment of CRAB in critically ill patients, and found that the meropenem plus colistin regimen caused a reduction in 30-day mortality, higher clinical and microbiological responses, and did not increase nephrotoxicity compared to colistin monotherapy.22 Colistin combination with vancomycin was not necessary for the management of critically ill patients infected with CRAB.23 In patients with septic shock, the mean arterial pressure and ventilator use are related to mortality,24 which is consistent with the conclusions of the clinical efficacy analysis in our study; that is, mechanical ventilation, use of vasoactive drugs, respiratory diseases, hepatobiliary diseases, and the number of CR-GNB infections were related to clinical failure of patients.
Few studies have investigated the microbiological efficacy of PMB for treatment of CR-GNB.25 Here, we investigated the microbiological clearance rate of the total course of treatment and 7-day microbiological clearance, which were 39.42% and 29.45%, respectively. Our results showed that urinary tract infection and CRAB infection were independent risk factors associated with bacterial clearance following PMB treatment. Further, clearance rates varied among different bacteria, with the rates higher for patients with CRAB infection and lower for those with CRKP and CRPA infection. Although there was no difference between patients who survived and those who died in terms of response to preemptive PMB therapy, we found that PMB delay was shorter in patients with successful bacterial clearance than in the failure group (Table 4). Moreover, preemptive therapy was also more common in patients with successful bacteria clearance than that in those with clearance failure (Tables 4 and S1), implying that preemptive PMB therapy can improve microbiological efficacy in patients infected with CR-GNB.
The mortality rate from CR-GNB infection in critically ill patients was high. A previous study found that delayed administration of both the initial and first appropriate antimicrobial therapy were independent risk factors for mortality and prolonged organ dysfunction.26 A small case-control study found that early use of PMB reduces mortality from CRKP bloodstream infection.10 In our research, we also analyzed the effects of preemptive PMB therapy and found no difference between patients who survived and those who died. Further, we found that patient-related factors, such as mechanical ventilation, vasoactive agent use, admission to ICU, more underlying diseases (eg, liver disease), and E. coli or E. cloacae infection, were associated with death. In patients with septic shock, the mean arterial pressure and ventilator use are related to mortality.24 A study also found that the number of patients on mechanical ventilation or having septic shock was lower in the survivor group than in the nonsurvivor group in patients infected with CR-GNB treated with PMB.27
Moreover, patients who died had a lower maintenance dose, cumulative dose of PMB, and treatment duration. A previous study also found that a PMB dose ≥ 200 mg/day was associated with lower in-hospital mortality.28 Further, a combination of carbapenems with PMB was more frequently administered to patients who survived than those who died, while the combination of tigecycline with PMB was less frequently administered to surviving patients.
The main route of polymyxin-induced nephrotoxicity is both concentration-dependent and time-dependent;29 however, there is evidence that reducing the daily dose of PMB to avoid nephrotoxicity is not feasible because it use of < 15,000–25,000 IU/kg of PMB per day can lead to sub-therapeutic antibiotic exposure.21,30 Such sub-therapeutic exposure may have multiple harmful effects, including the impairment of clinical results, due to insufficient drug exposure, and the expansion of PMB-resistant subgroups.31,32 However, our data indicate that the proportion of clinical success (27.55%) was only greater than that of clinical failure (18.82%) when the loading dose was ≥ 2 mg/kg; thus, clinical treatment efficacy was better in patients treated with a loading dose ≥ 2 mg/kg, relative to that in patients without a loading dose ≥ 2 mg/kg. Maintenance dose was not significantly related to clinical efficacy. In addition, total treatment course and 7-day bacterial clearance rates were not related to the recommended dosage requirements, which was not wholly consistent with previous population pharmacokinetic research, which suggests that PMB injection dosage should be calculated based on body weight.29
ADRs (particularly severe ADRs) to PMB are infrequent. Our study found that 56 patients (19.58%) suffered from ADRs to PMB during hospitalization. The most prevalent ADR was AKI (28 cases; 8.21%) in our study, which is lower than in previous publications.11,19,33–35 The difference may be due to the variation in PMB doses administered to patients. For example, Mattos et al reported nephrotoxicity of PMB in 40.5% of cases administered doses of 15,000–25,000 UI/kg/d in patients with normal kidney function.19 In comparison, our enrolled patients were administered with relatively low doses. Moreover, a study found that the nephrotoxicity rates were similar for colistin alone group and colistin plus vancomycin group.23 While another study also found the use of two or more nephrotoxic drugs combination with PMB was the independent risk factor for the occurrence of nephrotoxicity.36 Although the guidelines recommend that the dose of PMB in patients with renal insufficiency does not need to be adjusted,9 many studies have found that the AKI caused by PMB is related to high dose and concentration, combined use of other nephrotoxic drugs.11,37 Therefore, physicians and pharmacists could cooperate with each other to formulate the optimal scheme according to the monitoring results of therapeutic drug concentration and other individualized conditions of patients, so as to improve the curative effect and reduce the occurrence of AKI.
Our study has some limitations. First, it was a single-center retrospective study with a limited sample size. Second, because of the limited sample size, we did not conduct sub-group analysis according to types of CR-GNB and infection sites. Thus, the data may not be representative of PMB characterization in other carbapenem-resistant pathogens and sites of infection. Third, we did not consider other pathophysiological conditions, such as albumin levels, which may also influence PMB efficacy. Fourth, the combination of PMB with other antimicrobial drugs made it difficult to isolate ADR and the sole efficacy of PMB, which may have also caused certain limitations in the results. Moreover, as a retrospective study, the medication histories or the combinations of other medications used by patients were not strictly controlled, as this would have severely limited the sample size; however, this is a double-edged sword, since medications are inherently present in clinical situations; hence the results of our research are relevant to real-world situations. The results should be interpreted with caution due to possible confounders. Due to limited data and lack of dynamic monitoring of renal function, this study only defined renal toxicity without further investigating its severity. Further studies will assess this aspect, focusing on the severity of nephrotoxicity.
Conclusions
PMB is a relatively safe and effective antibiotic drug for patients critically ill with CR-GNB infection; however, PMB use should be subject to guideline recommendations for early administration, loading administration, and adequate administration, which could help to improve clinical efficacy, microbiological efficacy, and mortality.
Acknowledgments
We thank the support from the National Scientific Foundation of China (No. 81903052, No. 82073944), Scientific research project of Hunan Health Commission (No. 202113010170, 202213014496) and the Fundamental Research Funds for the Central Universities of Central South University (2021zzts1077).
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by the National Scientific Foundation of China (No. 81903052, No. 82073944), Scientific research project of Hunan Health Commission (No. 202113010170, 202213014496) and the Fundamental Research Funds for the Central Universities of Central South University (2021zzts1077).
Disclosure
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
References
1. Brennan-Krohn T, Manetsch R, O’Doherty GA, Kirby JE. New strategies and structural considerations in development of therapeutics for carbapenem-resistant Enterobacteriaceae. Transl Res. 2020;220:14–32. doi:10.1016/j.trsl.2020.02.008
2. World Health Organization. Critically Important Antimicrobials for Human Medicine – 5th Rev. Geneva: World Health OrganizationLicence: CC BY‐NCSA3.0 IGO; 2017.
3. Hu F, Guo Y, Yang Y, et al. Resistance reported from China antimicrobial surveillance network (CHINET) in 2018. Eur J Clin Microbiol Infect Dis. 2019;38(12):2275–2281. doi:10.1007/s10096-019-03673-1
4. Hu F, Guo Y, Zhu D. CHINET surveillance of bacterial resistance across tertiary hospitals in 2019. Chin J Infect Chemother. 2020;20(3):233–243.
5. Bassetti M, Vena A, Sepulcri C, Giacobbe DR, Peghin M. Treatment of bloodstream infections due to Gram-negative bacteria with difficult-to-treat resistance. Antibiotics. 2020;9(9):632.
6. Paterson DL, Isler B, Stewart A. New treatment options for multiresistant gram negatives. Curr Opin Infect Dis. 2020;33(2):214–223. doi:10.1097/QCO.0000000000000627
7. Yu Z, Yu L, Zhu J. Patterns of polymyxin B use in eight major cities of China in its first year of use. J Glob Antimicrob Resist. 2020;20:342–343. doi:10.1016/j.jgar.2020.02.009
8. Xie J, Roberts JA, Lipman J, et al. Pharmacokinetic/pharmacodynamic adequacy of polymyxin B against extensively drug-resistant Gram-negative bacteria in critically ill, general ward and cystic fibrosis patient populations. Int J Antimicrob Agents. 2020;55(6):105943. doi:10.1016/j.ijantimicag.2020.105943
9. Tsuji BT, Pogue JM, Zavascki AP, et al. International consensus guidelines for the optimal use of the polymyxins: endorsed by the American College of Clinical Pharmacy (ACCP), European Society of Clinical Microbiology and Infectious Diseases (ESCMID), Infectious Diseases Society of America (IDSA), International Society for Anti-infective Pharmacology (ISAP), Society of Critical Care Medicine (SCCM), and Society of Infectious Diseases Pharmacists (SIDP). Pharmacotherapy. 2019;39(1):10–39. doi:10.1002/phar.2209
10. Liang Q, Huang M, Xu Z. Early use of polymyxin B reduces the mortality of carbapenem-resistant Klebsiella pneumoniae bloodstream infection. Braz J Infect Dis. 2019;23(1):60–65. doi:10.1016/j.bjid.2018.12.004
11. Cai Y, Leck H, Tan RW, et al. Clinical experience with high-dose polymyxin B against carbapenem-resistant Gram-negative bacterial infections-A cohort study. Antibiotics. 2020;9(8). doi:10.3390/antibiotics9080451
12. Zhao S, Yan L, Wang C, Peng M. [Clinical analysis of sepsis with extensively drug resistant Gram-negative bacteria in intensive care unit treated with polymyxin B-based combination therapy]. Zhonghua Wei Zhong Bing Ji Jiu Yi Xue. 2020;32(2):150–154. Chinese. doi:10.3760/cma.j.cn121430-20200108-00028
13. Lu Q, Li GH, Qu Q, et al. Clinical efficacy of polymyxin B in patients infected with carbapenem-resistant organisms. Infect Drug Resist. 2021;14:1979–1988. doi:10.2147/IDR.S312708
14. Gibson GA, Bauer SR, Neuner EA, Bass SN, Lam SW. Influence of colistin dose on global cure in patients with bacteremia due to carbapenem-resistant Gram-negative bacilli. Antimicrob Agents Chemother. 2016;60(1):431–436. doi:10.1128/AAC.01414-15
15. Anania MC, Miranda C, Vizioli MG, et al. S100A11 overexpression contributes to the malignant phenotype of papillary thyroid carcinoma. J Clin Endocrinol Metab. 2013;98(10):E1591–1600. doi:10.1210/jc.2013-1652
16. Satlin MJ, Lewis JS, Weinstein MP, et al. Clinical and laboratory standards institute and European committee on antimicrobial susceptibility testing position statements on polymyxin B and colistin clinical breakpoints. Clin Infect Dis. 2020;71(9):e523–e529. doi:10.1093/cid/ciaa121
17. Miglis C, Rhodes NJ, Avedissian SN, et al. Population pharmacokinetics of polymyxin B in acutely ill adult patients. Antimicrob Agents Chemother. 2018;62(3). doi:10.1128/AAC.01475-17
18. Doi Y. Treatment options for carbapenem-resistant Gram-negative bacterial infections. Clin Infect Dis. 2019;69(Suppl 7):S565–S575. doi:10.1093/cid/ciz830
19. Mattos KPH, Gouvea IR, Quintanilha JCF, Cursino MA, Vasconcelos P, Moriel P. Polymyxin B clinical outcomes: a prospective study of patients undergoing intravenous treatment. J Clin Pharm Ther. 2019;44(3):415–419. doi:10.1111/jcpt.12801
20. Chambers HF, Eliopoulos GM, Gilbert DNP, Saag MSE. Sanford Guide to Antimicrobial Therapy 2018.
21. Sandri AM, Landersdorfer CB, Jacob J, et al. Population pharmacokinetics of intravenous polymyxin B in critically ill patients: implications for selection of dosage regimens. Clin Infect Dis. 2013;57(4):524–531. doi:10.1093/cid/cit334
22. Katip W, Uitrakul S, Oberdorfer P. A comparison of colistin versus colistin plus meropenem for the treatment of carbapenem-resistant acinetobacter baumannii in critically ill patients: a propensity score-matched analysis. Antibiotics. 2020;9(10). doi:10.3390/antibiotics9100647
23. Katip W, Oberdorfer P. Clinical efficacy and nephrotoxicity of colistin alone versus colistin plus vancomycin in critically ill patients infected with carbapenem-resistant acinetobacter baumannii: a propensity score-matched analysis. Pharmaceutics. 2021;13(2):162. doi:10.3390/pharmaceutics13020162
24. Klein DJ, Foster D, Walker PM, Bagshaw SM, Mekonnen H, Antonelli M. Polymyxin B hemoperfusion in endotoxemic septic shock patients without extreme endotoxemia: a post hoc analysis of the Euphrates trial. Intensive Care Med. 2018;44(12):2205–2212. doi:10.1007/s00134-018-5463-7
25. Lu Q, Zhu HH, Li GH, et al. A comparative study of the microbiological efficacy of polymyxin B on different carbapenem-resistant Gram-negative bacteria infections. Front Med. 2021;8:620885. doi:10.3389/fmed.2021.620885
26. Weiss SL, Fitzgerald JC, Balamuth F, et al. Delayed antimicrobial therapy increases mortality and organ dysfunction duration in pediatric sepsis. Crit Care Med. 2014;42(11):2409–2417. doi:10.1097/CCM.0000000000000509
27. Zhang X, Qi S, Duan X, et al. Clinical outcomes and safety of polymyxin B in the treatment of carbapenem-resistant Gram-negative bacterial infections: a real-world multicenter study. J Transl Med. 2021;19(1):431. doi:10.1186/s12967-021-03111-x
28. Elias LS, Konzen D, Krebs JM, Zavascki AP. The impact of polymyxin B dosage on in-hospital mortality of patients treated with this antibiotic. J Antimicrob Chemother. 2010;65(10):2231–2237. doi:10.1093/jac/dkq285
29. Azad MA, Akter J, Rogers KL, Nation RL, Velkov T, Li J. Major pathways of polymyxin-induced apoptosis in rat kidney proximal tubular cells. Antimicrob Agents Chemother. 2015;59(4):2136–2143. doi:10.1128/AAC.04869-14
30. Onufrak NJ, Rao GG, Forrest A, et al. Critical need for clarity in polymyxin B dosing. Antimicrob Agents Chemother. 2017;61(5). doi:10.1128/AAC.00208-17
31. Pogue JM, Ortwine JK, Kaye KS. Clinical considerations for optimal use of the polymyxins: a focus on agent selection and dosing. Clin Microbiol Infect. 2017;23(4):229–233. doi:10.1016/j.cmi.2017.02.023
32. Pogue JM, Ortwine JK, Kaye KS. Are there any ways around the exposure-limiting nephrotoxicity of the polymyxins? Int J Antimicrob Agents. 2016;48(6):622–626. doi:10.1016/j.ijantimicag.2016.11.001
33. Aggarwal R, Dewan A. Comparison of nephrotoxicity of colistin with polymyxin B administered in currently recommended doses: a prospective study. Ann Clin Microbiol Antimicrob. 2018;17(1):15. doi:10.1186/s12941-018-0262-0
34. Katip W, Yoodee J, Uitrakul S, Oberdorfer P. Efficacy of loading dose colistin versus carbapenems for treatment of extended spectrum beta lactamase producing Enterobacteriaceae. Sci Rep. 2021;11(1):18. doi:10.1038/s41598-020-78098-4
35. Katip W, Uitrakul S, Oberdorfer P. Clinical efficacy and nephrotoxicity of the loading dose colistin for the treatment of carbapenem-resistant Acinetobacter baumannii in critically ill patients. Pharmaceutics. 2021;14(1):31. doi:10.3390/pharmaceutics14010031
36. Chang K, Wang H, Zhao J, et al. Risk factors for polymyxin B-associated acute kidney injury. Int J Infect Dis. 2022;117:37–44. doi:10.1016/j.ijid.2022.01.055
37. Nation RL, Rigatto MHP, Falci DR, Zavascki AP. Polymyxin acute kidney injury: dosing and other strategies to reduce toxicity. Antibiotics. 2019;8(1). doi:10.3390/antibiotics8010024
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.