Back to Journals » International Medical Case Reports Journal » Volume 19
Pleural Effusion and Neuropsychiatric Involvement in a Patient with SLE: A Report from a Resource-Limited, Tuberculosis-Endemic Country
Authors Hersi AA, Ahmed SI ![]() , Adam AM, Ibrahim KJ
, Adam AM, Ibrahim KJ ![]()
Received 21 May 2026
Accepted for publication 18 June 2026
Published 22 June 2026 Volume 2026:19 584784
DOI https://doi.org/10.2147/IMCRJ.S584784
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Thomas E Hutson
Ahmed Abdi Hersi,1,2 Sadam Ismail Ahmed,3 Abdifatah Musa Adam,4 Khadar Jama Ibrahim5
1College of Medicine and Health Science, Department of Medicine and Surgery, University of Hargeisa, Hargeisa, Somaliland; 2Department of Internal Medicine, Hargeisa Group Hospital, Hargeisa, Somaliland; 3Faculty of Medicine and Health science, University of Burao, Burao, Somaliland; 4Department of Medical Ward, Hargeisa Group Hospital, Hargeisa, Somaliland; 5College of Health Sciences, School of Medicine and Surgery, Amoud University, Borama, Somaliland
Correspondence: Sadam Ismail Ahmed, Email [email protected]
Background: Systemic lupus erythematosus (SLE) is a multisystem autoimmune disease with diverse clinical manifestations that may mimic infectious conditions, particularly in tuberculosis-endemic regions. Pleural effusion and respiratory symptoms are often attributed to tuberculosis, leading to delayed recognition of autoimmune disease. Neuropsychiatric involvement represents a severe manifestation that may be under recognized in low-resource settings where access to specialized investigations is limited.
Case Presentation: We report a 19-year-old Somali female who presented with a three-month history of progressive symmetrical polyarthritis, malar rash, and discoid lesions. She subsequently developed respiratory symptoms and bilateral pleural effusion. Despite negative GeneXpert testing, she was initially treated for tuberculosis due to high regional prevalence. After failing to improve and developing neuropsychiatric symptoms (hallucinations, agitation, and a seizure), she was referred to a tertiary center. Immunological testing confirmed Systemic Lupus Erythematosus (SLE) with positive ANA, anti-ds DNA, and SS-A/Ro antibodies. Treatment with high-dose corticosteroids, mycophenolate mofetil, and hydroxychloroquine led to significant clinical recovery.
Conclusion: In resource-limited, TB-endemic settings, SLE can be easily misdiagnosed. Clinicians must maintain a high index of suspicion for autoimmune diseases when patients with unexplained serositis or neuropsychiatric symptoms fail to respond to empirical TB therapy.
Keywords: systemic lupus erythematosus, neuropsychiatric lupus, pleural effusion, tuberculosis misdiagnosis, low-resource settings, case report
Introduction
Systemic lupus erythematosus (SLE) is a chronic autoimmune disease characterized by multisystem involvement resulting from immune dysregulation and autoantibody formation.
Serositis, including pleural effusion, is a recognized manifestation of SLE and is associated with increased disease activity.1 In tuberculosis-endemic regions, pleural effusion is frequently attributed to pulmonary tuberculosis (TB), often leading to empirical anti-TB therapy and delayed recognition of underlying autoimmune disease.2,3 This diagnostic overlap represents a significant challenge where access to advanced immunological testing is limited. Neuropsychiatric systemic lupus erythematosus (NPSLE) represents a severe manifestation including seizures, psychosis, and behavioral disturbances.4,5 These manifestations frequently mimic infectious or primary psychiatric conditions, increasing the risk of delayed diagnosis in resource-limited settings.6 We report a case of SLE presenting with neuropsychiatric manifestations and pleural effusion initially misdiagnosed as TB.
Case Presentation
A 19-year-old Somali female student with no prior medical history presented with a three-month progression of symptoms. The illness began in July with symmetrical joint pain in the small joints of the hands (MCP and PIP joints), accompanied by morning stiffness and fatigue. Three weeks later, she developed a malar rash and dark scaly lesions on her ears (Figure 1).
 |
Figure 1 An erythematous flat, non-scarring malar rash, was present symmetrically across the cheeks and the bridge of the nose sparing nasolabial folds. |
She subsequently developed a dry cough, pleuritic chest pain, and shortness of breath. A chest radiograph (Figure 2) showed bilateral pleural effusion and left lower zone consolidation. Despite a negative sputum GeneXpert test, empirical anti-TB therapy (HRZE) was started based on regional epidemiology. One month later, she developed vomiting and abdominal pain, leading to treatment interruption. She was later re-started on anti-TB therapy in Ethiopia, but her condition deteriorated.
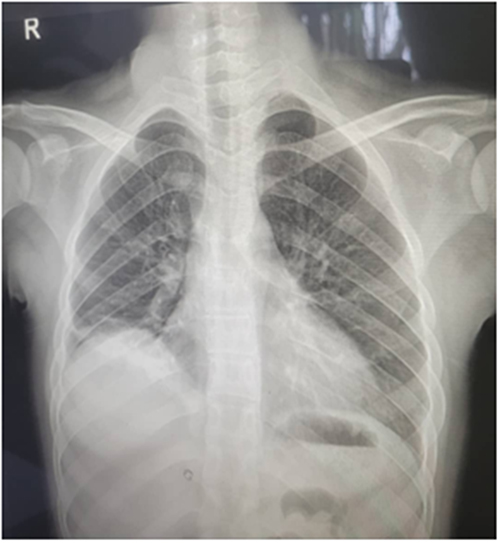 |
Figure 2 Posteroanterior chest radiograph revealed bilateral pleural effusion, predominantly on the right side, with associated consolidation in the left lower lung zone. |
The patient developed new neuropsychiatric symptoms: persistent headache, visual and auditory hallucinations, delusions, agitation, and a one-minute generalized tonic-clonic seizure. Upon transfer to Hargeisa Group Hospital, physical examination revealed an anxious, restless patient with a well-defined malar rash and discoid plaques (Figures 3 and 1). Respiratory exam showed bilateral fine crackles and decreased air entry.
 |
Figure 3 Scaly discoid plaques were observed involving the outer ear and ear lobes with well-defined margins and adherent scaling. |
Laboratory investigations (Summarized in the Table 1) were notable for anemia of chronic disease, elevated ESR, and positive autoimmune serology (ANA 400 U/mL, positive anti-dsDNA, and SS-A/Ro 60 kD). Complement levels were unavailable due to resource limitations.
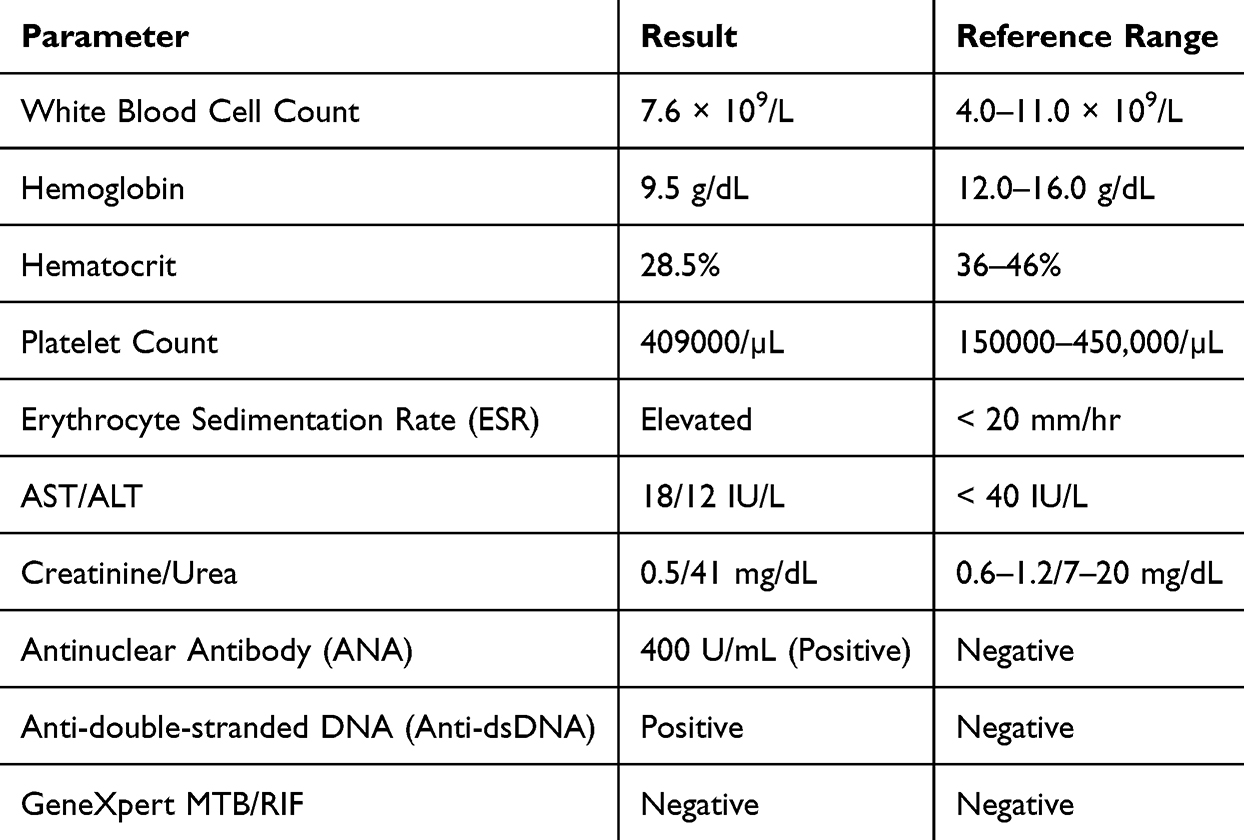 |
Table 1 Summary of Laboratory Investigations |
Imaging Studies
Chest radiography: demonstrated consolidation in the left lower lung zone with bilateral pleural effusion, more prominent on the left side. These findings were initially interpreted as suggestive of pulmonary tuberculosis but were later considered compatible with lupus-related pleuritis.
Echocardiography: revealed normal cardiac chamber size and ventricular function, with no evidence of pericardial effusion.
Abdominopelvic ultrasonography revealed no hepatosplenomegaly, ascites, or structural renal abnormalities.
Therapeutic Intervention
The diagnosis was confirmed as SLE with NPSLE and lupus pleuritis. Management included intravenous methylprednisolone (1g daily for 5 days), followed by oral prednisolone (40mg tapering), mycophenolate mofetil (titrated to 2g daily), and hydroxychloroquine (200mg twice daily). Risperidone (2mg daily) was used briefly for psychosis and completed by the outer ear discoid manifestation after the treatment (Figure 4).
 |
Figure 4 The outer ear discoid manifestations completely resolution after treatment. |
Follow-Up and Outcomes
The patient showed marked improvement for the malar rash by the completely resolved the treatment as (Figure 5). At six months, all neuropsychiatric and joint symptoms had resolved. At 16 months, she returned to school and remained stable Follow-up ANA levels decreased to 135.6 U/mL, and anti-ds DNA normalized. (Figures 1 and 2) (panels B) show the complete resolution of cutaneous lesions.
 |
Figure 5 The malar rash completely resolved following treatment. |
Discussion
Systemic lupus erythematosus often mimics infectious conditions, particularly in TB endemic regions.2 In such settings, pleural effusion is frequently attributed to TB, leading to empirical therapy even when microbiological confirmation is lacking,7 (Table 2) compares the overlapping and distinguishing features of SLE and TB to aid clinical differentiation.
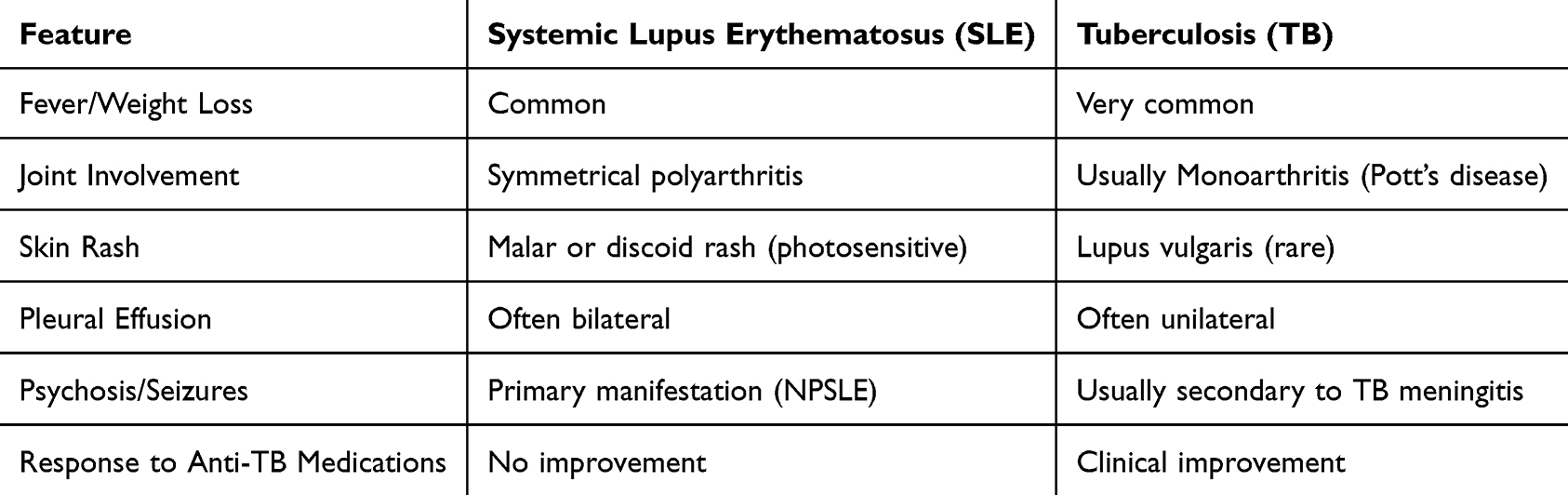 |
Table 2 Clinical Comparison: Systemic Lupus Erythematosus (SLE) vs. Tuberculosis |
Neuropsychiatric SLE includes a wide range of symptoms, including seizures and psychosis.4 In this case, these symptoms contributed to diagnostic confusion, especially without advanced neuroimaging.8 Early recognition is essential, as delayed treatment may result in irreversible neurological damage.9
Serositis is a well-recognized manifestation of SLE.1 Lupus pleuritis can mimic infectious pleural disease, and in TB-endemic areas, it is commonly misinterpreted as tuberculosis pleurisies due to overlapping clinical and radiologic features.2 Persistent or unexplained pleural effusion should prompt reconsideration of alternative diagnoses when TB therapy fails.3
Similar cases in the literature emphasize the risk of misdiagnosis in resource-limited settings.2,3
Management of severe SLE requires prompt initiation of high-dose corticosteroids and immune suppressants.10 Despite limited diagnostic resources, targeted serologic testing enabled a favorable outcome in this patient. This case underscores several lessons: First, failure to improve on empirical TB therapy should prompt immediate reconsideration of autoimmune disease.2 Second, neuropsychiatric symptoms in patients with systemic inflammation are a red flag for NPSLE.4 Third, clinicians in endemic areas must maintain high suspicion for SLE in patients with unexplained multisystem involvement.
Conclusion
The main take-home messages are:
1) SLE is a great mimicker of TB in resource-limited settings;
2) Empirical TB therapy should be re-evaluated if no response is seen within weeks; and
3) Early use of targeted autoimmune serology is cost-effective in preventing irreversible organ damage and unnecessary TB treatment.
Ethical Approval
In our institute, the ethical approval is not required for publication of case reports, so our hospital is waived for case reports.
Informed Consent
Informed consent was obtained from both patient and the patient’s Parent (Primary care giver) for publication of this case report.
Consent for Publication
Written informed consent was obtained from the patient and her primary caregiver for publication of this case report and accompanying images.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
No funding for this case.
Disclosure
The authors declare no conflicts of interest in this work.
References
1. Zhao J, Bai W, Zhu P, et al. CSTAR registry VII: prevalence and clinical significance of serositis in Chinese patients with systemic lupus erythematosus. Lupus. 2016;25(6):652–6. doi:10.1177/0961203315625460
2. Gyawali R, Bhandari L, Shah S, et al. Familial systemic lupus erythematosus with pleural and articular involvement mimicking tuberculosis: a case report. Ann Med Surg. 2026;88:1892–1896. doi:10.1097/ms9.0000000000004686
3. Huynh TM, Huynh N, Vo TLT, et al. Atypical presentation of systemic lupus erythematosus flare with ileocecal ulceration and lymphadenopathy in a tuberculosis-endemic region. Medicine. 2025;104:e44964. doi:10.1097/MD.0000000000044964
4. Justiz-Vaillant AA, Gopaul D, Soodeen S, et al. Neuropsychiatric systemic lupus erythematosus: molecules involved in its immunopathogenesis, clinical features, and treatment. Molecules. 2024;29(4):778. doi:10.3390/molecules29040747
5. Carrión-Barberà I, Salman-Monte T, Vílchez-Oya F, Monfort J. Neuropsychiatric involvement in systemic lupus erythematosus: a review. Autoimmun Rev. 2021;20(2):102780. doi:10.1016/j.autrev.2021.102780
6. Sarwar S, Mohamed AS, Rogers S, et al. Neuropsychiatric systemic lupus erythematosus: a 2021 update on diagnosis, management, and current challenges. Cureus. 2021;13(9):e17815. doi:10.7759/cureus.17969
7. Gong W, Wu X. Differential diagnosis of latent tuberculosis infection and active tuberculosis: a key to a successful tuberculosis control strategy. Front Microbiol. 2021;12:747214. doi:10.3389/fmicb.2021.747214
8. Nikolopoulos D, Fanouriakis A, Bertsias G. Treatment of neuropsychiatric systemic lupus erythematosus: clinical challenges and future perspectives. Expert Rev Clin Immunol. 2021;17(4):407–421. doi:10.1080/1744666X.2021.1899810
9. Fanouriakis A, Tziolos NR, Bertsias G, Boumpas DT. Update on the diagnosis and management of systemic lupus erythematosus. Ann Rheum Dis. 2021;80(1):14–25. doi:10.1136/annrheumdis-2020-218272
10. Pons-Estel GJ, Ramírez-Flores MF, Quintana R, et al. Addressing the challenge of global delays in diagnosis and treatment of systemic lupus erythematosus. Nat Rev Rheumatol. 2025;21:566–574. doi:10.1038/s41584-025-01277-y
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Fusobacterium nucleatum-Induced Pyopneumothorax: A Rare but Serious Clinical Entity
Chen Y, Yu C, Chai J, Chai M, Xiao Y, Loong H, Xu D, Wang L
Infection and Drug Resistance 2025, 18:4293-4300
Published Date: 25 August 2025
From Nerve to Autoimmunity: Acute Guillain-Barré Syndrome in a 4-Year-Old with Early-Onset Pediatric Systemic Lupus Erythematosus
Kanan M, Hasan HA, Hassan AM, Sbitan L
Open Access Rheumatology: Research and Reviews 2026, 18:578137
Published Date: 8 February 2026
Lupus Enteritis Presenting as Acute Abdomen with Clear Gelatinous Stools in a Woman with Systemic Lupus Erythematosus: A Case Report and Literature Review
Wang M, Liang Z
Open Access Rheumatology: Research and Reviews 2026, 18:622552
Published Date: 13 June 2026