Back to Journals » Open Access Rheumatology: Research and Reviews » Volume 18
Lupus Enteritis Presenting as Acute Abdomen with Clear Gelatinous Stools in a Woman with Systemic Lupus Erythematosus: A Case Report and Literature Review
Received 14 May 2026
Accepted for publication 10 June 2026
Published 13 June 2026 Volume 2026:18 622552
DOI https://doi.org/10.2147/OARRR.S622552
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Chuan-Ju Liu
Minghao Wang, Zhiqiang Liang
Department of Rheumatology, The Affiliated Hospital of Chengde Medical College, Chengde, Hebei, People’s Republic of China
Correspondence: Zhiqiang Liang, Email [email protected]
Abstract: Lupus enteritis is a recognized but uncommon and potentially life-threatening gastrointestinal manifestation of systemic lupus erythematosus. Its symptoms are often nonspecific and may mimic infectious enteritis, pseudomembranous colitis, intestinal obstruction, or a surgical acute abdomen. We report a 19-year-old woman with a prior diagnosis of SLE and irregular use of maintenance therapy who developed abdominal pain, watery diarrhea, nausea, vomiting, and progressive abdominal distension after ingestion of suspected contaminated food. During hospitalization, she passed large amounts of clear, gelatinous, pseudomembrane-like stool material. Laboratory evaluation showed anemia, thrombocytopenia, hypocomplementemia, positive antinuclear antibodies, positive anti-Ro52 antibodies, and negative microbiological studies, including stool culture and Clostridioides difficile toxin assays. Contrast-enhanced abdominal computed tomography demonstrated segmental small-bowel wall thickening with the target sign, mesenteric vascular engorgement with the comb sign, and ascites, supporting the diagnosis of lupus enteritis. After infection was considered unlikely, empirical antibiotics were discontinued. High-dose intravenous methylprednisolone, adjunctive intravenous immunoglobulin, and cyclophosphamide led to rapid clinical improvement within 48– 72 hours, with subsequent radiological resolution. The novelty of this case lies not in lupus enteritis itself, but in its presentation with substantial clear gelatinous pseudomembrane-like stool material, a rarely emphasized manifestation that may mislead clinicians toward infectious or pseudomembranous colitis. Early recognition based on SLE activity, characteristic CT findings, exclusion of infection, and multidisciplinary assessment is essential to avoid diagnostic delay and prevent severe complications.
Keywords: systemic lupus erythematosus, lupus enteritis, gastrointestinal involvement, mesenteric vasculitis, case report
Introduction
Systemic lupus erythematosus (SLE) is a chronic autoimmune disease characterized by autoantibody production, immune-complex deposition, and multisystem inflammation. It predominantly affects women of reproductive age and may involve multiple organs and systems.1,2 Gastrointestinal involvement is relatively common in patients with SLE, affecting approximately 40–60% of patients.3 However, clinically severe gastrointestinal manifestations are less frequent and may be difficult to distinguish from infection, drug-related adverse effects, or surgical abdominal conditions.4
Lupus enteritis (LE), also referred to as lupus mesenteric vasculitis, is an uncommon but potentially life-threatening gastrointestinal manifestation of SLE. It usually presents with nonspecific symptoms such as abdominal pain, nausea, vomiting, diarrhea, abdominal distension, or features of intestinal pseudo-obstruction.5 In published descriptions of LE, diarrhea is recognized as one of the common gastrointestinal symptoms, but the passage of large amounts of clear, gelatinous, pseudomembrane-like stool material has rarely been described as a presenting manifestation. Contrast-enhanced abdominal computed tomography is central to early recognition, with typical findings including bowel-wall thickening, the target sign, the comb sign, mesenteric edema, and ascites.5,6
The present case is clinically notable because the patient developed an acute abdomen accompanied by the passage of large amounts of clear, gelatinous, pseudomembrane-like stool material, an unusual finding that could easily be misinterpreted as infectious enteritis, pseudomembranous colitis, ischemic colitis, or inflammatory bowel disease. The diagnostic significance of this observation lies not in its specificity, but in its value as a clinical warning sign when interpreted in the context of active SLE. In this patient, negative microbiological studies, active SLE features, characteristic CT findings, and rapid improvement after glucocorticoid-based immunosuppressive therapy supported the diagnosis of LE. This case highlights the need to consider autoimmune intestinal involvement in patients with active SLE, even when the stool appearance appears suggestive of infection.
Case Presentation
Medical History
History of Present Illness
A 19-year-old Han Chinese woman with a known history of SLE was admitted in October 2024 because of abdominal pain, watery diarrhea, nausea, vomiting, and progressive abdominal distension. The total duration of hospitalization was 23 days.
Three days before admission, after ingesting latiao, a spicy wheat-gluten snack commonly consumed in China and suspected to be contaminated in this case, she developed paroxysmal periumbilical pain. This was accompanied by non-bloody, non-purulent watery diarrhea up to five times daily, with transient relief of abdominal pain after defecation. She also reported nausea and vomiting of gastric contents, without coffee-ground material. She developed a low-grade fever, with a maximum temperature of 37.8°C, but had no chills or rigors. Review of systems was negative for cough, sputum production, dysuria, urinary frequency or urgency, gross hematuria, suprapubic pain, flank pain, and headache. She was initially diagnosed with acute gastroenteritis at a local clinic and received symptomatic antiemetic and rehydration therapy, without significant improvement. One day before admission, she presented to our emergency department and received intravenous levofloxacin for empirical antimicrobial coverage, together with fluid resuscitation and antiemetic treatment. Because of persistent symptoms, she was admitted for further evaluation and management.
She had been diagnosed with SLE approximately two years before the current hospitalization. Five years before admission, she had noticed unexplained alopecia but did not seek medical care. Approximately two years before the current admission, she developed fatigue, poor appetite, and nausea, and was admitted to a local hospital in February 2022. At that time, laboratory evaluation showed pancytopenia, hypocomplementemia, elevated IgG, positive antinuclear antibodies, and a positive direct antiglobulin test. Tests for systemic vasculitis-related antibodies were negative. The detailed laboratory results from the previous hospitalization are summarized in Table 1. She was diagnosed with SLE complicated by immune-mediated cytopenia and was treated with oral prednisone and cyclosporine, after which her symptoms partially improved. According to the available medical records, hydroxychloroquine had not been included in her previous treatment regimen, and the reason was not clearly documented. Her subsequent follow-up was irregular. She discontinued cyclosporine on her own and gradually tapered prednisone to 10 mg daily, which she continued until the present admission.
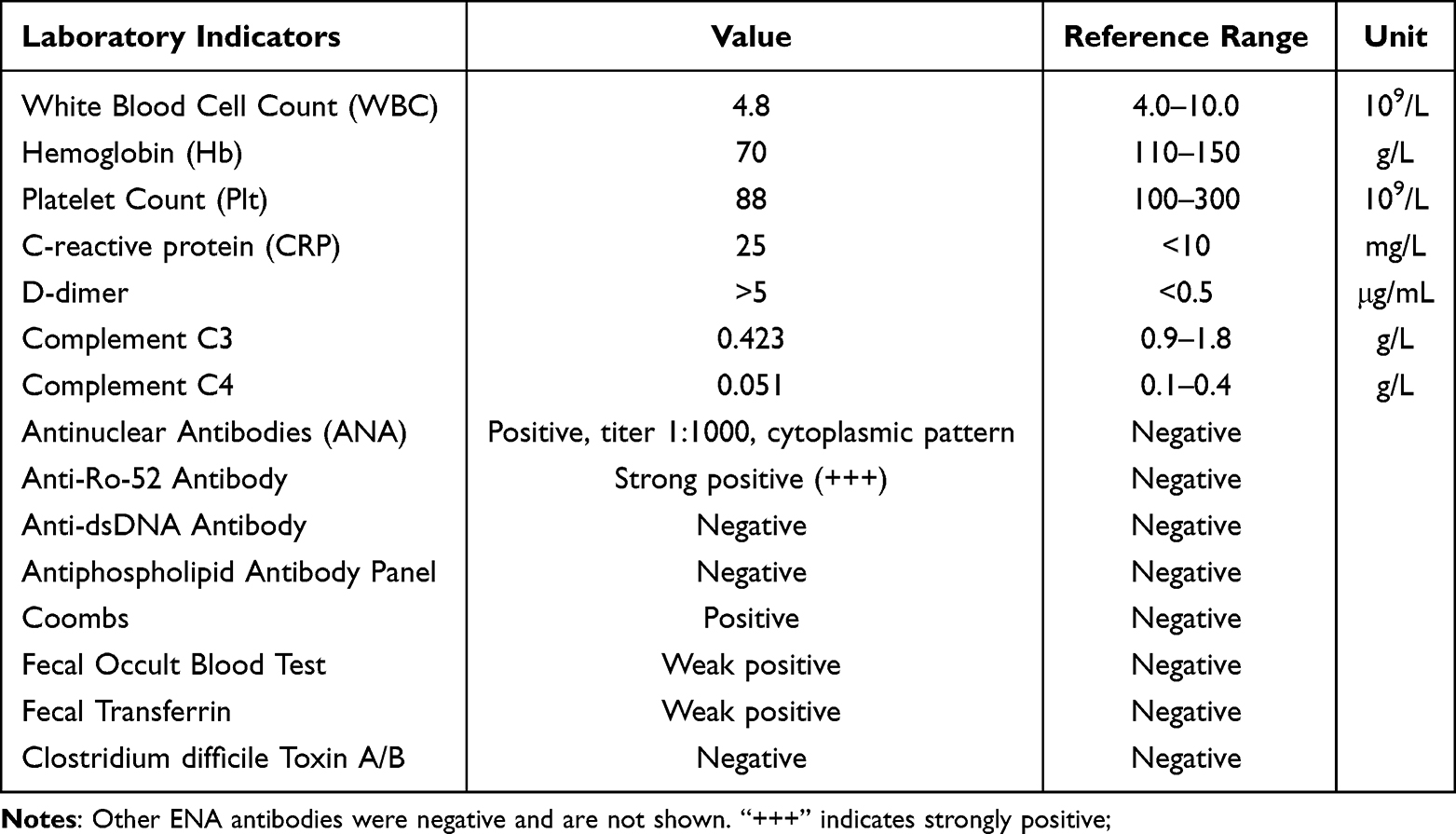 |
Table 1 Laboratory Parameters and Values |
She reported no other chronic illnesses and had no history of surgery, major trauma, or blood transfusion. She had no known drug or food allergies, and her vaccination history was unclear. She denied a family history of autoimmune disease, gastrointestinal disease, or relevant inherited disorders. She did not smoke, misuse alcohol, or use illicit drugs.
Physical Examination
On admission, her temperature was 36.7°C, pulse rate 92 beats/min, respiratory rate 20 breaths/min, blood pressure 102/74 mmHg, and oxygen saturation was 98% on room air. She was alert but lethargic, with a pale appearance. No clinical signs of dehydration were observed. Fading erythematous rashes were noted on the face and left upper limb. No oral ulcers, active alopecia, synovitis, or lower-extremity edema were observed. No typical malar rash was observed.
Abdominal examination revealed mild tenderness in the epigastric and periumbilical regions, without rebound tenderness or guarding. Bowel sounds were normal. Shifting dullness was present. Cardiopulmonary examination was unremarkable.
Laboratory Findings
Laboratory tests on admission showed anemia, thrombocytopenia, hypocomplementemia, positive antinuclear antibodies, strongly positive anti-Ro52 antibodies, and a positive direct antiglobulin test. Anti–double-stranded DNA, anti-Sm, anti–ribosomal P, anticardiolipin antibodies, lupus anticoagulant, and anti–β2-glycoprotein I antibodies were negative. Coagulation testing showed an elevated D-dimer level. Inflammatory markers, including procalcitonin and C-reactive protein, were mildly elevated. Urinalysis showed no findings suggestive of urinary tract infection or clinically evident urinary tract involvement. In combination with the absence of dysuria, urinary frequency or urgency, gross hematuria, suprapubic pain, or flank pain, there was no clinical evidence supporting concomitant lupus cystitis during the current episode.
Stool testing showed weakly positive fecal occult blood and transferrin. Stool routine examination and microscopy showed no visible red blood cells, pus cells, ova, or parasites. Repeated blood cultures, stool cultures, and Clostridioides difficile toxin assays were negative. There was no hematemesis, coffee-ground emesis, melena, or overt bloody stool. The patient’s anemia was evaluated in the context of her previous SLE-associated immune-mediated cytopenia and current positive direct antiglobulin test. Detailed laboratory findings before admission, on admission, during hospitalization, and at follow-up are summarized in Table 1.
Imaging Studies
Initial contrast-enhanced abdominopelvic CT performed after admission showed segmental small-bowel wall edema and thickening with circumferential enhancement, consistent with the target sign. Prominent mesenteric vascular engorgement and dilatation were also observed, consistent with the comb sign. Minimal abdominopelvic free fluid and a small pericardial effusion were present. No bladder-wall thickening, hydroureter, or hydronephrosis was observed on abdominopelvic CT, providing no imaging evidence of concomitant lupus cystitis. An incidental accessory spleen was noted. These initial CT findings are shown in Figure 1A and B.
 |
Figure 1 Enhanced abdominal and pelvic CT on October 18, 2024, revealed small bowel wall edema with thickening and annular enhancement, presenting with a target sign appearance. Mesenteric vessels showed congestion and dilation with a comb-like pattern (A and B). Following treatment, bowel wall edema resolved, and the target sign and comb-like pattern disappeared (C and D). |
Diagnostic Considerations
The patient’s established history of SLE, progressive abdominal symptoms, negative microbiological studies, hypocomplementemia, and characteristic contrast-enhanced CT findings raised strong suspicion for LE. Infectious enteritis and pseudomembranous colitis were initially considered because of the history of suspected contaminated food intake, watery diarrhea, and passage of clear gelatinous pseudomembrane-like stool. However, repeated microbiological studies were negative. The patient’s disease activity was assessed using the SLEDAI. At admission, her SLEDAI score was 7, based on active rash, hypocomplementemia, thrombocytopenia, and serosal involvement manifested as a small pericardial effusion. Although this score indicated active SLE, it may still have underestimated the clinical severity of this episode because gastrointestinal involvement related to LE is not directly captured as a separate descriptor in the SLEDAI.
Colonoscopy was not performed during the acute phase. At that time, the patient continued to pass clear gelatinous stools, and CT showed marked bowel-wall edema. Considering the potential risk of intestinal injury or perforation, colonoscopy was not regarded as the first-line diagnostic modality in the acute phase. The potential risks and benefits were discussed with the patient’s family, who declined endoscopic evaluation.
Treatment and Prognosis
Upon admission, initial management included gastric acid suppression with omeprazole, fluid resuscitation, symptomatic supportive treatment, and empirical antimicrobial coverage with ceftriaxone and ornidazole because infectious enterocolitis or intra-abdominal infection could not be excluded at presentation. By hospital day 2, her abdominal distension had worsened, and she continued to pass clear gelatinous pseudomembrane-like stool (Figure 2). After repeated microbiological studies were negative and LE was considered the most likely diagnosis, treatment was escalated to intravenous methylprednisolone sodium succinate at 500 mg/day for 3 days, together with adjunctive intravenous immunoglobulin at 25 g/day for 5 days. Empirical antibiotics were discontinued after repeated microbiological studies were negative and infection was considered unlikely.
 |
Figure 2 Appearance of the clear, gelatinous, pseudomembranous material passed by the patient on the second day of hospitalization, suggesting severe gastrointestinal involvement during the acute phase. |
Two days after initiation of glucocorticoid-based immunosuppressive therapy, her abdominal pain and distension markedly improved, vomiting ceased, and bowel function gradually recovered. Her stool changed from clear and gelatinous to yellow loose stool and then progressively became formed. After completion of high-dose methylprednisolone therapy, she was transitioned to intravenous methylprednisolone at 40 mg/day and received sequential intravenous cyclophosphamide at 400 mg.
Under this regimen, her abdominal distension and diarrhea resolved, and her vital signs remained stable without new symptoms. Follow-up laboratory tests showed improvement in anemia and normalization of complement levels. Routine stool examination became unremarkable. A repeat abdominal CT performed after treatment showed near-complete resolution of the previous bowel-wall abnormalities and abdominopelvic fluid, with reduction of pericardial effusion. These follow-up CT findings are shown in Figure 1C and D. The patient was discharged in November 2024 after a total hospitalization of 23 days. Discharge medications included oral prednisone, starting at 60 mg/day with a tapering schedule, and she was advised to attend regular rheumatology outpatient follow-up.
Patient Perspective
During the acute phase, the patient described the abdominal pain, repeated vomiting, and frequent passage of clear gelatinous stool as particularly distressing and anxiety-provoking. She felt that these symptoms developed rapidly and were unlike her previous SLE manifestations. After treatment, her gastrointestinal symptoms improved markedly, and she felt reassured by the diagnosis and favorable treatment response. The overall clinical course, diagnostic workup, treatment, and response are summarized in Figure 3.
 |
Figure 3 Timeline of Disease Progression, Diagnosis, and Treatment. Abbreviations: SLE, systemic lupus erythematosus; LE, lupus enteritis; IVIG, intravenous immunoglobulin; ED, emergency department; Hb, hemoglobin; PLT, platelet count. |
Discussion and Literature Review
SLE is a multisystem autoimmune disease. Although gastrointestinal involvement is common, severe manifestations such as LE are relatively rare and may be life-threatening. We report a 19-year-old woman with SLE who discontinued maintenance therapy after diagnosis and subsequently presented with severe abdominal pain and watery diarrhea that progressed to the passage of large amounts of transparent, gelatinous pseudomembrane-like material, accompanied by dark green emesis and signs of bowel obstruction. Contrast-enhanced abdominal CT demonstrated the characteristic target sign and comb sign. Laboratory findings suggested highly active disease, including hypocomplementemia and pancytopenia. Her symptoms and imaging abnormalities improved rapidly after high-dose glucocorticoid pulse therapy combined with intravenous immunoglobulin and cyclophosphamide. From the perspective of existing knowledge, LE is a recognized but uncommon gastrointestinal manifestation of SLE, and its typical clinical and radiological features, including abdominal pain, diarrhea, vomiting, bowel-wall edema, ascites, the target sign, and the comb sign, have been described previously. Therefore, the novelty of the present case does not lie in the diagnosis of LE itself. Rather, this case is notable for the passage of large amounts of transparent gelatinous pseudomembrane-like stool material, which has rarely been emphasized in previous reports of LE. This unusual manifestation is clinically important because it may strongly suggest infectious enteritis or Clostridioides difficile-associated pseudomembranous colitis, particularly in the setting of suspected contaminated food exposure and early empirical antibiotic use. Thus, the value of this case lies in highlighting a potential diagnostic pitfall and emphasizing that apparent pseudomembrane-like stool should be interpreted together with SLE activity, microbiological results, characteristic CT findings, and treatment response.
This feature is clinically important because it may mimic infectious enteritis or Clostridioides difficile-associated pseudomembranous colitis, especially in patients presenting with acute diarrhea and suspected food exposure. Therefore, this case highlights the need to consider LE in patients with active SLE who present with acute abdominal symptoms and unusual mucus-rich or pseudomembrane-like stool. This case report, together with a literature review, discusses potential pathogenesis, clinical implications, diagnostic pitfalls, and management considerations. For the literature review, we searched PubMed and Web of Science using combinations of the following terms: “systemic lupus erythematosus,” “SLE,” “lupus enteritis,” “lupus mesenteric vasculitis,” “intestinal vasculitis,” “pseudomembrane,” “pseudomembranous,” “gelatinous stool,” “mucus-rich stool,” and “case report.” Additional relevant articles were identified by manually screening the reference lists of eligible publications. We included English-language case reports or case series describing patients with SLE-related enteritis or mesenteric vasculitis, particularly those with severe or atypical gastrointestinal manifestations. Cases in which infectious enteritis, inflammatory bowel disease, mesenteric ischemia, or other non-SLE causes were considered the primary explanation were excluded.
The diagnosis of SLE in this patient was supported by her previous clinical history and the 2019 EULAR/ACR classification criteria.7 She fulfilled the obligatory entry criterion of positive antinuclear antibody, with an ANA titer of 1:1000. Based on the available clinical and laboratory data, she had thrombocytopenia, low C3 and low C4 levels, and a history of alopecia. These findings reached at least 8 points, and if the previous alopecia was clinically consistent with non-scarring alopecia, the total score reached 10 points, meeting the classification threshold for SLE. In addition, her positive direct antiglobulin test and anemia supported immune-mediated cytopenia, although complete hemolysis parameters were not available.
Pathogenesis of LE
LE is considered one of the most severe gastrointestinal manifestations of SLE.8 Its pathogenesis is primarily driven by immune complex–mediated vasculitis of small- and medium-sized vessels, accompanied by complement activation and amplification of local inflammatory cascades. These processes lead to bowel-wall edema, increased mucosal permeability, and ischemic injury.9 This mechanism represents a classic type III hypersensitivity reaction and shares a pathological basis with vasculitic involvement in other target organs of SLE, such as lupus nephritis.10 In addition, the mesenteric microvasculature—characterized by abundant arterioles and dense capillary networks—may predispose the bowel to acute exudation and layered edema,3 which correspond clinically to the target sign and comb sign on contrast-enhanced CT.
In patients with SLE, polyclonal B-cell activation leads to the production of abundant autoantibodies (eg., ANA and anti-Ro antibodies), which form circulating immune complexes (ICs) with nuclear antigens and cellular debris.11 Because of relatively slow flow, low shear stress, and high endothelial expression of Fcγ receptors, ICs preferentially deposit in mesenteric microvessels and small vessels, particularly arterial branches and postcapillary venules. After deposition, ICs engage Fcγ receptors on endothelial cells and resident macrophages, inducing upregulation of adhesion molecules (ICAM-1 and VCAM-1) and chemokines. This promotes recruitment of neutrophils and monocytes, establishing a local inflammatory milieu that culminates in fibrinoid necrosis of the vessel wall and endothelial dysfunction—key early events in the acute onset of LE.12 In parallel, deposited ICs activate complement predominantly through the classical pathway: C1q binds the Fc portion of ICs, triggering sequential activation of C1r/C1s, C4, and C3, and generating the anaphylatoxins C3a and C5a as well as the C5b-9 membrane attack complex (MAC).
C3a and C5a further recruit inflammatory cells and promote mast-cell degranulation, thereby increasing vascular permeability.12 The membrane attack complex (MAC) can directly injure endothelial cells, leading to extravasation of serous fluid, fibrin, and inflammatory cells into the submucosa and resulting in characteristic edematous thickening. This cascade consumes complement, producing markedly reduced serum C3 and C4 levels, which often serve as a useful indicator of LE activity. In severe cases, complement-driven signaling may activate downstream NF-κB pathways, promoting the release of proinflammatory cytokines (eg., IL-1β and IL-6) and establishing a positive feedback loop that aggravates layered bowel-wall edema and exudation.12
Clinical Manifestations, Diagnosis, and Differential Diagnosis of LE
The pathophysiology of LE is primarily driven by immune-complex deposition and complement activation, resulting in vasculitis of small- and medium-sized vessels and subsequent bowel-wall edema, mucosal hyperemia, exudation, and ischemic injury. Clinically, LE typically presents with diffuse abdominal pain and watery diarrhea.13 Although severe mucosal exudation can occasionally produce gelatinous or mucus-rich stools, true pseudomembrane formation is exceedingly rare. In some patients, LE may be complicated by protein-losing enteropathy, characterized by marked mucus or fibrinous exudation—similar to the gelatinous material observed in the present case—which may reflect profound mucosal edema and increased vascular permeability.14 In our patient, weakly positive fecal transferrin and mildly decreased serum albumin suggested possible intestinal mucosal injury and protein loss, although these findings were not sufficient to establish protein-losing enteropathy independently. Compared with previously reported cases of LE, which more commonly presented with abdominal pain, diarrhea, vomiting, ascites, bowel-wall thickening, the target sign, or the comb sign, the present case was unusual because the patient passed large amounts of transparent gelatinous pseudomembrane-like material. Similar severe or atypical cases have included LE presenting as the only active manifestation of SLE, colorectal involvement, or gastrointestinal bleeding; however, prominent pseudomembrane-like stool has rarely been emphasized in previous reports.15,16 To further highlight the clinical context and novelty of the present case, we summarized selected reported cases of LE with severe or atypical gastrointestinal manifestations in Table 2. Compared with these cases, the present patient shared typical features of LE, including abdominal pain, diarrhea or vomiting, bowel-wall edema, ascites or free fluid, and characteristic CT findings. However, the passage of large amounts of transparent gelatinous pseudomembrane-like material was particularly unusual and may represent a distinctive clinical clue to severe mucosal edema and exudation in active LE.
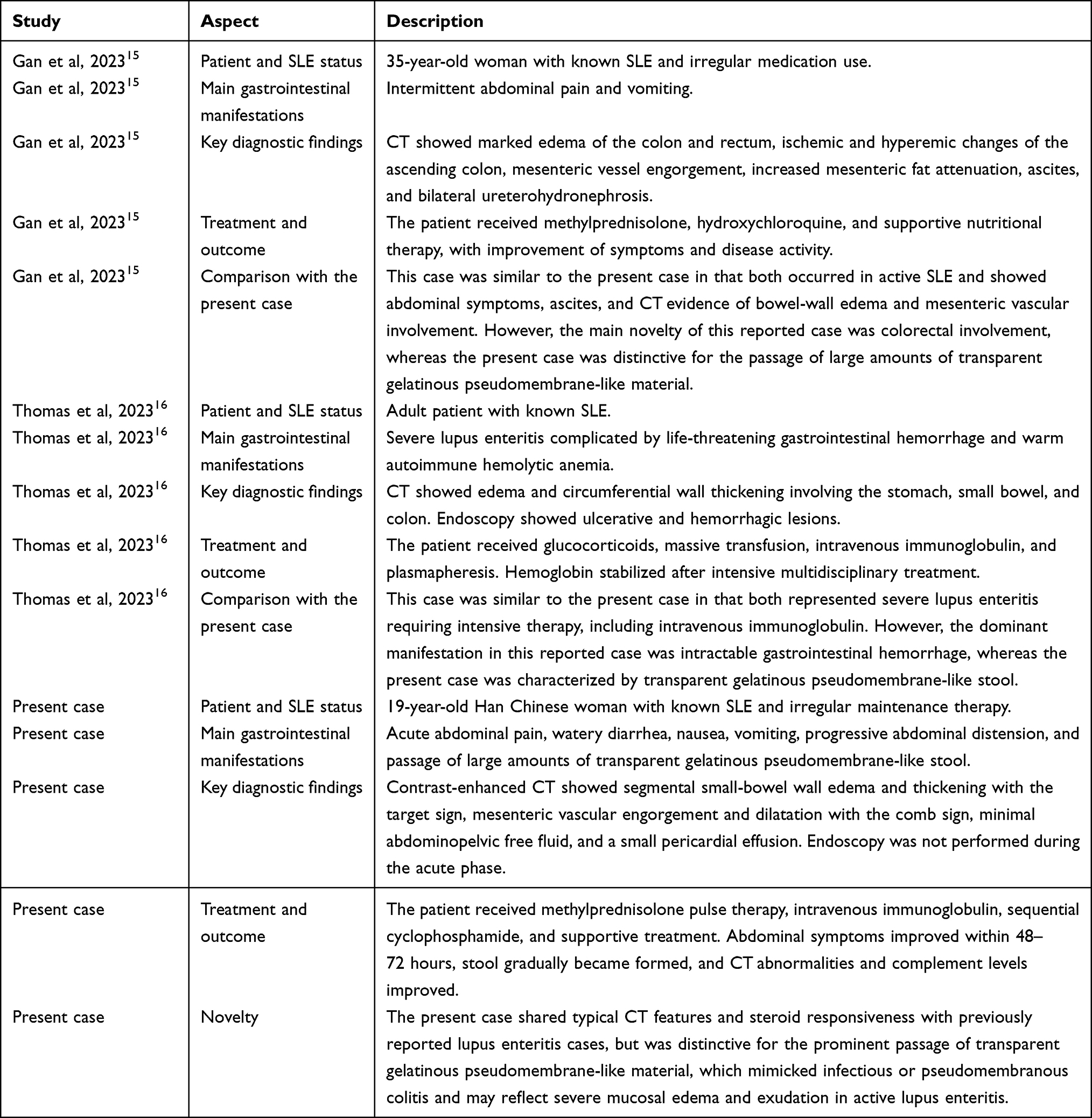 |
Table 2 Comparison of the Present Case with Previously Reported Atypical or Severe Cases of Lupus Enteritis |
The diagnosis of LE relies on an integrated assessment of a known SLE history, clinical presentation, laboratory markers of disease activity, and characteristic imaging findings. Because no single gold-standard test is available, LE is often diagnosed clinically using an exclusion-based approach. In practice, LE should be considered in patients with confirmed SLE who present with an acute abdomen, particularly when contrast-enhanced CT demonstrates typical features, while alternative etiologies—such as infection, mesenteric ischemia, and inflammatory bowel disease—are excluded. Contrast-enhanced abdominal CT remains the preferred and most diagnostically informative modality, with high diagnostic performance for the target sign and comb sign.5 With advances in imaging and increasing demand for noninvasive evaluation, adjunctive tools such as ultrasonography and endoscopy have also been reported. Ultrasonography may demonstrate bowel-wall thickening and edema, ascites, and increased mesenteric blood flow, and is particularly useful in children/adolescents and pregnant patients. However, its diagnostic utility is limited by operator dependence and interference from bowel gas, although it remains a valuable initial screening test.17 Given the risk of perforation, endoscopy is generally not recommended during the acute phase of LE. In remission or selected diagnostically challenging cases, endoscopy may reveal mucosal hyperemia, edema, ulcers; nevertheless, it is typically considered supportive rather than a primary diagnostic modality.5,15
Establishing the differential diagnosis was a major challenge in this case. The passage of hyaline, pseudomembrane-like material can strongly suggest Clostridioides difficile–associated pseudomembranous colitis, particularly when diarrhea occurs after antibiotic exposure. However, repeated negative assays for C. difficile toxins A/B, lack of response to empiric antimicrobial therapy, and the rapid cessation of pseudomembranous discharge with marked clinical improvement after glucocorticoid pulse therapy collectively support immune-mediated vasculitis rather than infection as the primary driver. In addition, inflammatory bowel disease (IBD) and mesenteric ischemia should be considered and excluded.18 IBD typically follows a chronic course and is supported by characteristic endoscopic findings, whereas mesenteric ischemia is more common in older patients or those with cardiovascular risk factors. In this patient, young age and the absence of evidence for thrombosis argued against these diagnoses. Moreover, contrast-enhanced CT demonstrated the classic target sign and comb sign, which resolved rapidly after immunosuppressive treatment, further supporting the diagnosis of LE.
Treatment of LE
The main therapeutic goals in LE are rapid control of vasculitic inflammation, reversal of bowel-wall edema, and prevention of severe complications (eg., bowel necrosis and perforation). High-dose glucocorticoid pulse therapy is the first-line treatment, and most patients achieve substantial clinical improvement with radiographic resolution within 72 hours.19 With increasing recognition of relapse and refractory disease, early adjunctive immunosuppressants (eg., cyclophosphamide) and biologic agents have been increasingly used in relapsed or steroid-refractory LE.20 Emerging evidence suggests that biologics may be effective options; for example, belimumab can reduce overall SLE activity in patients at high risk of LE relapse,21 whereas rituximab has been reported to be effective in severe LE through B-cell depletion.22 Intravenous immunoglobulin (IVIg) is not usually considered a first-line treatment for LE, but it can serve as adjunctive therapy in severe cases, especially when systemic activity or hematologic involvement is present.16 In this case, IVIg was introduced early as part of an intensive combination regimen because the patient had active SLE with progressive gastrointestinal symptoms and hematologic involvement. After methylprednisolone pulse therapy plus IVIg, followed by cyclophosphamide, her condition improved rapidly within 48–72 hours. Radiologic abnormalities resolved markedly, and complement levels returned to normal. This early combined approach may therefore be helpful in selected patients with severe disease.
Limitations of This Case
This case has several limitations. Endoscopic evaluation and histopathological confirmation were not obtained, which should be acknowledged as a diagnostic limitation. In the acute phase, however, the patient had ongoing passage of clear gelatinous pseudomembrane-like stool and marked bowel-wall edema on CT, raising concern about procedure-related intestinal injury. After discussion of the potential risks and benefits, the patient’s family declined endoscopic evaluation. Although endoscopy might have provided additional mucosal and pathological information, the diagnosis of LE was supported by the patient’s established history of SLE, active serologic and hematologic abnormalities, characteristic contrast-enhanced CT findings, negative microbiological studies, exclusion of major alternative diagnoses, and rapid clinical and radiologic response to glucocorticoid-based immunosuppressive therapy.
Another limitation is related to the early use of empirical antibiotics. Ceftriaxone plus ornidazole was administered at admission because infectious enterocolitis or intra-abdominal infection could not be excluded during the initial presentation. Repeated Clostridioides difficile toxin assays and stool cultures were negative, and antibiotics were discontinued once infection was considered unlikely. This reflects the practical difficulty of distinguishing LE from infectious enterocolitis in the early phase, especially when abdominal pain, diarrhea, low-grade fever, and suspected contaminated food exposure coexist.
Finally, as this is a single case report, the relationship between transparent gelatinous pseudomembrane-like stool and the underlying pathological process of LE cannot be definitively established. Nevertheless, this unusual stool manifestation occurred in parallel with active SLE, characteristic CT findings, negative microbiological studies, and rapid improvement after immunosuppressive therapy. Therefore, it may represent a clinically relevant clue to severe mucosal edema and exudation in LE. Further reports, particularly those with endoscopic or histopathological evidence when clinically feasible, are needed to better characterize this rare manifestation.
Conclusion
In patients with SLE who present with an acute abdomen, LE should be considered, particularly when contrast-enhanced CT shows characteristic findings such as the target sign or comb sign. The present case adds to the literature by showing that large amounts of clear, gelatinous, pseudomembrane-like stool material, although suggestive of infectious or pseudomembranous colitis, may also occur as an unusual manifestation of active LE. Clinicians should therefore integrate immune activity markers, imaging findings, microbiological results, and treatment response rather than attributing such stool findings to infection alone. Early multidisciplinary assessment involving rheumatologists, gastroenterologists, radiologists, infectious disease specialists, and surgeons may help distinguish LE from infectious enterocolitis, inflammatory bowel disease, mesenteric ischemia, and surgical emergencies, while facilitating timely glucocorticoid-based immunosuppressive therapy and monitoring for severe complications such as bowel necrosis and perforation.
Ethics Approval and Consent to Participate
Written informed consent was obtained from the patient for publication of this case report and any accompanying clinical information or images. According to the policy of The Affiliated Hospital of Chengde Medical College, institutional approval was not required for publication of this single case report.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Fanouriakis A, Kostopoulou M, Alunno A, et al. 2019 update of the EULAR recommendations for the management of systemic lupus erythematosus. Ann Rheumatic Dis. 2019;78(6):736–11
2. Siegel CH, Sammaritano LR. Systemic lupus erythematosus: a review. JAMA. 2024;331(17):1480–1491. doi:10.1001/jama.2024.2315
3. Frittoli RB, Vivaldo JF, Costallat LTL, Appenzeller S. Gastrointestinal involvement in systemic lupus erythematosus: a systematic review. J Trans Autoimmun. 2021;4:100106. doi:10.1016/j.jtauto.2021.100106
4. Alharbi S. Gastrointestinal manifestations in patients with systemic lupus erythematosus. Open Access Rheumatol. 2022;14:243–253. doi:10.2147/OARRR.S384256
5. Muñoz-Urbano M, Sangle S, D’Cruz DP. Lupus enteritis: a narrative review. Rheumatology. 2024;63(6):1494–1501. doi:10.1093/rheumatology/kead689
6. Ko SF, Lee TY, Cheng TT, et al. CT findings at lupus mesenteric vasculitis. Acta Radiol. 1997;38(1):115–120. doi:10.1080/02841859709171253
7. Aringer M, Costenbader K, Daikh D, et al. European League Against Rheumatism/American College of Rheumatology classification criteria for systemic lupus erythematosus. Ann Rheumatic Dis. 2019;78(9):1151–1159. doi:10.1136/annrheumdis-2018-214819
8. Yavari T, Alikhani M, Alikhani M, Bijani F, Moghtadaie A. Pos1163 lupus mesenteric vasculitis as life-threatening etiology of acute abdominal pain in lupus patients. Ann Rheumatic Dis. 2025;84:1234–1235. doi:10.1016/j.ard.2025.06.513
9. Leone P, Prete M, Malerba E, et al. Lupus vasculitis: an overview. Biomedicines. 2021;9(11):1626. doi:10.3390/biomedicines9111626
10. Carlé C, Mas E, Barreau F. Intestinal involvement in lupus: from pathophysiology to therapeutic perspectives. Lupus. 2023;32(4):461–470. doi:10.1177/09612033231155840
11. Wang Y, Zhou Y. Pediatric-onset lupus mesenteric vasculitis. Radiology. 2026;318(1):e252508. doi:10.1148/radiol.252508
12. Zhou L, Cai SZ, Dong LL. Recent advances in pathogenesis, diagnosis, and therapeutic approaches for digestive system involvement in systemic lupus erythematosus. J Dig Dis. 2024;25(7):
13. Louthrenoo W, Gumtorntip W, Thanunchai P, Amantakul A, Kasitanon N, Pojchamarnwiputh S. Clinical features, imaging findings, and outcomes of acute abdominal pain in systemic lupus erythematosus: comparing mesenteric vasculitis, non-mesenteric vasculitis, and surgical conditions. Clin Rheumatol. 2024;43(12):3699–3712. doi:10.1007/s10067-024-07189-8
14. Mai Thanh C, Nguyen Trong P, Nguyen Thanh N. Protein-losing enteropathy as initial presentation of pediatric systemic lupus erythematosus: a rare case report from Vietnam and literature review. Inter J Immuno Pharmacol. 2025;39. doi:10.1177/03946320251358304
15. Gan H, Wang F, Gan Y, Wen L. Rare case of lupus enteritis presenting as colorectum involvement: a case report and review of literature. World J Clin Case. 2023;11(34):
16. Thomas A, Smithhart C, Chopra M, et al. Severe Lupus Enteritis Complicated by Intractable Gastrointestinal Hemorrhage. ACG Case Rep. J. 2023;10(11):e01188. doi:10.14309/crj.0000000000001188
17. Zhu J, Lai J, Liu X, et al. Clinical characteristics and prognosis of childhood-onset lupus mesenteric vasculitis as the initial presentation-a case-control study. Arthritis Res Ther. 2023;25(1). doi:10.1186/s13075-023-03237-x.
18. Faraji M, Gutierrez E, Glotser A, Thaker J, Gammarano C. Targets and combs: a case of lupus enteritis. Cureus. 2020;12(4).
19. Williamson L, Hao Y, Basnayake C, Oon S, Nikpour M. Systematic review of treatments for the gastrointestinal manifestations of systemic lupus erythematosus. Semin. Arthritis Rheum. 2024;69:152567. doi:10.1016/j.semarthrit.2024.152567
20. Chen L, He Q, Luo M, et al. Clinical features of lupus enteritis: a single-center retrospective study. Orphanet J Rare Dis. 2021;16(1):396. doi:10.1186/s13023-021-02044-4
21. Almutairi R, Alkhudair D, Aldei A. Lupus enteritis as the early manifestation of systemic lupus erythematosus successfully managed with belimumab: a case report. Cureus. 2025;17(1).
22. Kenar G, Atay K, Yüksek GE, Öz B, Koca SS. Gastrointestinal vasculitis due to systemic lupus erythematosus treated with rituximab: a case report. Lupus. 2020;29(6):640–643. doi:10.1177/0961203320910803
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
From Nerve to Autoimmunity: Acute Guillain-Barré Syndrome in a 4-Year-Old with Early-Onset Pediatric Systemic Lupus Erythematosus
Kanan M, Hasan HA, Hassan AM, Sbitan L
Open Access Rheumatology: Research and Reviews 2026, 18:578137
Published Date: 8 February 2026
Pleural Effusion and Neuropsychiatric Involvement in a Patient with SLE: A Report from a Resource-Limited, Tuberculosis-Endemic Country
Hersi AA, Ahmed SI, Adam AM, Ibrahim KJ
International Medical Case Reports Journal 2026, 19:584784
Published Date: 22 June 2026