Back to Journals » International Journal of General Medicine » Volume 19
Platelet Antigen Polymorphisms in Cirrhosis: Association with Esophageal Varices Development
Authors Abdallah HM, Osheba IS, Salman AA ![]() , Gaballa NK
, Gaballa NK ![]() , Helmi MO, Ibrahim AR, Atta ASS, Saad MG
, Helmi MO, Ibrahim AR, Atta ASS, Saad MG ![]() , Aboagiza SM, Abdel Hafez HS, El Helbawy MGED, GabAllah GMK, Elewa A, Salman MA
, Aboagiza SM, Abdel Hafez HS, El Helbawy MGED, GabAllah GMK, Elewa A, Salman MA ![]() , Abdelmegeed NA
, Abdelmegeed NA ![]()
Received 2 December 2025
Accepted for publication 23 April 2026
Published 29 April 2026 Volume 2026:19 581932
DOI https://doi.org/10.2147/IJGM.S581932
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Professor Hyam Leffert
Heba Mohamed Abdallah,1 Iman Shaban Osheba,1 Ahmed Abdallah Salman,2 Nahla K Gaballa,3 Merhan Osama Helmi,1 Amr Ragab Ibrahim,4 Asmaa Said Shahat Atta,1 Mohammed Gaber Saad,5 Sara Mohammed Aboagiza,1 Hanaa Saied Abdel Hafez,3 Mostafa Gamal El Din El Helbawy,4 Ghada M K GabAllah,6 Ahmed Elewa,7 Mohamed Abdalla Salman,8 Nashwa Abdelmotelb Abdelmegeed1
1Department of Clinical Pathology, National Liver Institute, Menoufia University, Shebin Elkom, Egypt; 2Department of Internal Medicine, Faculty of Medicine, Cairo University, Cairo, Egypt; 3Department of Anesthesiology and Intensive Care, National Liver Institute, Menoufia University, Shebin Elkom, Egypt; 4Department of Hepatology and Gastroenterology, National Liver Institute, Menoufia University, Shebin Elkom, Egypt; 5Department of Anesthesiology and Intensive Care and Pain Management, Faculty of Medicine, Al-Azhar University, Cairo, Egypt; 6Department of Medical Biochemistry, Faculty of Medicine, Menoufia University, Shebin Elkom, Egypt; 7General Surgery Department, National Hepatology and Tropical Medicine Research Institute, Cairo, Egypt; 8General Surgery Department, Faculty of Medicine, Cairo University, Cairo, Egypt
Correspondence: Ahmed Abdallah Salman, Department of Internal Medicine, Faculty of Medicine, Cairo University, Cairo, Egypt, Tel +201000468664, Email [email protected]; [email protected]
Background: Esophageal varices (EVs) are a serious consequence of portal hypertension in chronic liver disease, particularly in hepatitis C virus (HCV) infection. While endoscopy remains the gold standard for diagnosis, there is growing interest in human platelet antigen (HPA) polymorphisms as potential non-invasive markers associated with EV development.
Aim: To assess the association between HPA-1, HPA-2, and HPA-3 gene polymorphisms and the presence and severity of EVs in cirrhotic patients.
Methods: In this case-control study, 150 patients with HCV-related cirrhosis were enrolled and divided into two groups based on endoscopic findings: 75 with EVs and 75 without. HPA genotyping was performed using polymerase chain reaction with sequence-specific primers (PCR-SSP). Statistical analysis included univariate and multivariate logistic regression, with odds ratios (ORs) and 95% confidence intervals (CIs) calculated.
Results: The HPA-3 (ab + aa) genotypes were significantly associated with the presence of EVs in univariate analysis (OR: 2.244, 95% CI: 1.039– 4.847, p = 0.040), but this association was not maintained in multivariate analysis (OR: 0.679, 95% CI: 0.209– 2.211, p = 0.521). Higher grades of varices were significantly associated with HPA-1 (a), HPA-2 (b), and HPA-3 (a) alleles (p < 0.05). Platelet count and platelet count-to-spleen diameter (PC/SD) ratio were also significantly associated with EVs in univariate analysis (p < 0.001). In multivariate analysis, serum creatinine (OR: 0.234, 95% CI: 0.116– 0.473, p < 0.001) and portal vein diameter (OR: 1.542, 95% CI: 1.231– 1.930, p < 0.001) were identified as independent predictors of EVs.
Conclusion: HPA polymorphisms were associated with the presence and severity of esophageal varices but were not independent predictors. Further multicenter prospective studies are needed to clarify their clinical utility.
Keywords: platelet antigen polymorphisms, cirrhosis, esophageal varices
Introduction
Liver cirrhosis is characterized by progressive hepatic fibrosis and the formation of regenerative nodules, leading to increased intrahepatic resistance and the development of portal hypertension. One of the most clinically significant complications of portal hypertension is the formation of esophageal varices (EVs), which are dilated submucosal veins with a high risk of rupture and life-threatening bleeding. Clinically significant portal hypertension, defined as a hepatic venous pressure gradient (HVPG) ≥10 mmHg, is associated with the development of EVs, while HVPG >12 mmHg markedly increases the risk of variceal bleeding. Upper gastrointestinal endoscopy remains the gold standard for diagnosis.1 Early identification of high-risk patients and timely initiation of prophylactic therapies, including non-selective beta-blockers or transjugular intrahepatic portosystemic shunt (TIPS), are essential to reduce morbidity and mortality.2
Globally, liver cirrhosis represents a major health burden, with viral hepatitis being one of the leading causes. In particular, hepatitis C virus (HCV) infection remains highly prevalent in many regions, including the Middle East and Egypt, where it constitutes a major etiological factor for cirrhosis and its complications. The progression from chronic hepatitis to cirrhosis and portal hypertension is influenced not only by viral factors but also by host genetic variability.
Among host-related factors, human platelet antigens (HPAs), including HPA-1, HPA-2, and HPA-3, are encoded by single nucleotide polymorphisms (SNPs) that affect platelet membrane glycoproteins. These polymorphisms may influence platelet adhesion, aggregation, and interaction with the vascular endothelium. Mechanistically, altered platelet functions may contribute to hepatic fibrogenesis through modulation of inflammatory pathways, release of profibrotic mediators (such as transforming growth factor-β), and interactions with hepatic stellate cells, which play a central role in fibrosis development. In addition, platelet dysfunction and thrombocytopenia—common features in cirrhosis—may exacerbate portal hypertension by impairing vascular integrity and promoting microvascular changes within the hepatic and portal circulation.
Furthermore, HPA polymorphisms may indirectly influence the development of EVs by affecting the severity of fibrosis and portal pressure. For instance, genetic variations that alter platelet activation or endothelial interactions could contribute to increased intrahepatic resistance and collateral vessel formation, key processes in variceal development.
Although HPAs have been extensively studied in transfusion medicine, their role in liver disease and portal hypertension remains insufficiently explored.3 Emerging evidence, such as the association between HPA-15 polymorphism and reduced serum laminin levels in patients with chronic hepatitis C, suggests a potential role in fibrosis progression.4 Given that EVs are a major complication of portal hypertension, investigating HPA polymorphisms may provide insights into genetic susceptibility and disease progression.
Therefore, this study aims to evaluate the association between HPA-1, HPA-2, and HPA-3 polymorphisms and the development of esophageal varices in patients with liver cirrhosis.
Materials and Methods
Study Design, Setting, and Study Period
This case-control study was conducted at the National Liver Institute, Menoufia University, Egypt, between May and October 2024. A total of 150 patients with liver cirrhosis were enrolled and equally allocated into two groups: 75 cirrhotic patients with esophageal varices (EVs) and 75 cirrhotic patients without EVs. All clinical, laboratory, radiological, endoscopic, and molecular evaluations were performed during the study period.
Participants, Inclusion and Exclusion Criteria
Eligible participants were adult patients aged ≥18 years with HCV-related liver cirrhosis diagnosed on the basis of clinical, laboratory, and ultrasonographic findings. Patients were included if they had confirmed cirrhosis and underwent upper gastrointestinal endoscopy for assessment of esophageal varices.
Patients were excluded if they had hepatocellular carcinoma, any other malignancy, major comorbid conditions that could affect platelet parameters or portal hemodynamics, previous endoscopic or surgical treatment for varices, non-HCV-related cirrhosis, or incomplete clinical or laboratory data.
Written informed consent was obtained from all participants before enrollment in the study.
Sample Size Estimation
Sample size was estimated using Wan Nor Arifin’s online Sample Size Calculator. The minimum required sample size was calculated based on a case-control design, assuming a two-sided alpha error of 0.05, study power of 80%, and a moderate effect size. The calculation indicated that at least 30 participants were required in each group to detect a statistically meaningful difference between groups. To improve the robustness of the analysis and account for possible data variability, 75 patients were included in each group.
Clinical and Endoscopic Assessment
Detailed demographic and clinical data were recorded for all participants, including age, sex, presenting symptoms, and relevant family history. Liver status was evaluated by duplex ultrasonography. Upper gastrointestinal endoscopy was performed for all patients, and esophageal varices were graded according to the Paquet classification system.5
Procedures and Anesthetic Technique
Endoscopy was performed under conscious sedation using propofol and dexmedetomidine administered via a target-controlled infusion (TCI) technique. Patients with ASA physical status II or III were monitored with supplemental oxygen, intravenous access, and SedLine monitoring, with a target sedation index of 25–50. Hemodynamic parameters were continuously monitored using the ICON monitor (Osypka Medical, USA).5 Propofol and dexmedetomidine doses were titrated according to patient age, clinical response, and hemodynamic stability. The TCI pump (Injectomat TIVA Agilia, Fresenius Kabi) was operated according to the Marsh pharmacokinetic model.6
Laboratory Investigations
All participants underwent comprehensive laboratory evaluation. Complete blood count with differential was performed using the Sysmex XN1000 analyzer. Liver and renal function tests, including alanine aminotransferase (ALT), aspartate aminotransferase (AST), total bilirubin, serum albumin, creatinine, and blood urea nitrogen (BUN), were measured using the Cobas 6000 analyzer (Roche Diagnostics). Coagulation profile, including international normalized ratio (INR), was assessed using the Sysmex CS-1600 system. The platelet count/spleen diameter ratio was also calculated as a non-invasive parameter related to portal hypertension. In addition, molecular genotyping of HPA-1, HPA-2, and HPA-3 polymorphisms were performed to investigate their possible association with the presence of esophageal varices.
Molecular Testing for HPA-1, HPA-2, and HPA-3 Polymorphisms
Genomic DNA was extracted from peripheral EDTA-anticoagulated blood using the Genomic DNA Purification Mini Kit (Thermo Fisher Scientific, Cat. No. K0781), according to the manufacturer’s instructions. Briefly, samples were digested with proteinase K at 55 °C, lysed using binding buffer and ethanol, and then processed through silica-based spin columns. After washing, DNA was eluted and quantified using a NanoDrop spectrophotometer to assess DNA concentration and purity.
Genotyping of HPA-1, HPA-2, and HPA-3 polymorphisms were performed using polymerase chain reaction with sequence-specific primers (PCR-SSP). This technique allows allele discrimination based on primer-template mismatch at the 3′ end, which prevents extension by Taq DNA polymerase in the presence of a noncomplementary nucleotide. For each polymorphism, two allele-specific forward primers (for allele “a” and allele “b”) and one common reverse primer were used.
The primer sequences were as follows: HPA-1a: 5′-ACT TAC AGG CCC TGC CTC T-3′, HPA-1b: 5′-ACT TAC AGG CCC TGC CTC C-3′, and common reverse primer: 5′-AGC CGG AGT GCA ATC CTC TG-3′; HPA-2a: 5′-CCC CCA GGG CTC CTG AC-3′, HPA-2b: 5′-GCC CCC AGG GCT CCT GAT-3′, and common reverse primer: 5′-GCC AGC GAC GAA AAT AGA GG-3′; HPA-3a: 5′-GGG GGA GGG GCT GGG GA-3′, HPA-3b: 5′-GGG GGA GGG GCT GGG GC-3′, and common reverse primer: 5′-GAC CTG CTC TAC ATC CTG GA-3′.
Each 25 µL PCR reaction contained 12.5 µL TaqMan Universal PCR Master Mix, 6.5 µL DNase-free water, 0.5 µL of each primer, and 5 µL genomic DNA. The thermal cycling conditions consisted of an initial denaturation at 94 °C for 10 minutes, followed by 35 cycles of denaturation at 94 °C, annealing at 60 °C, and extension at 72 °C for 50 seconds each, with a final extension at 72 °C for 10 minutes. PCR products were separated on 2.5% agarose gel stained with ethidium bromide and visualized under ultraviolet illumination (Figure 1).
 |
Figure 1 Representative agarose gel electrophoresis of PCR-SSP products for HPA genotyping. (a) HPA-1 showing a 196 bp band. (b) HPA-2 showing a 241 bp band. (c) HPA-3 showing a 230 bp band. Lanes 1–6 represent analyzed samples with allele-specific amplification (a/b). Bands correspond to allele-specific amplification products. A 100–1000 bp DNA ladder is shown on the left. |
PCR Quality Control
To ensure the reliability of genotyping results, standard quality-control measures were applied throughout the molecular procedures. DNA concentration and purity were checked before amplification. Negative control reactions without template DNA were included to exclude contamination. A subset of samples was re-genotyped in duplicate to confirm reproducibility, and genotype calls were interpreted independently after gel visualization. Only clear and concordant banding patterns were accepted for final analysis.
Results
Out of 179 cirrhotic patients screened at the National Liver Institute, 29 were excluded (12 declined participation and 17 did not meet the inclusion criteria). A total of 150 eligible patients were enrolled and equally divided into two groups: 75 patients with esophageal varices (EVs) and 75 without EVs.
Baseline Clinical Characteristics
The majority of patients had HCV-related cirrhosis. Detailed data regarding HCV genotype, viral load, treatment history, and duration of liver disease were not available and are acknowledged as a limitation of the study. Comorbid conditions and beta-blocker use were comparable between the two groups (p > 0.05).
Laboratory and Radiological Findings
Patients with EVs demonstrated significantly lower platelet count, alkaline phosphatase (ALP), serum creatinine, and platelet count-to-spleen diameter (PC/SD) ratio. In contrast, they showed significantly higher mean platelet volume (MPV), platelet large cell ratio (P-LCR), splenic diameter, and portal vein diameter (PVD) (p < 0.05).
No statistically significant differences were observed between the two groups in hemoglobin (Hb), red blood cell count (RBCs), white blood cell count (WBCs), hematocrit (HCT), mean corpuscular volume (MCV), platelet distribution width (PDW), liver enzymes (AST, ALT), serum albumin, total bilirubin, blood urea, and international normalized ratio (INR) (p > 0.05) (Tables 1 and 2).
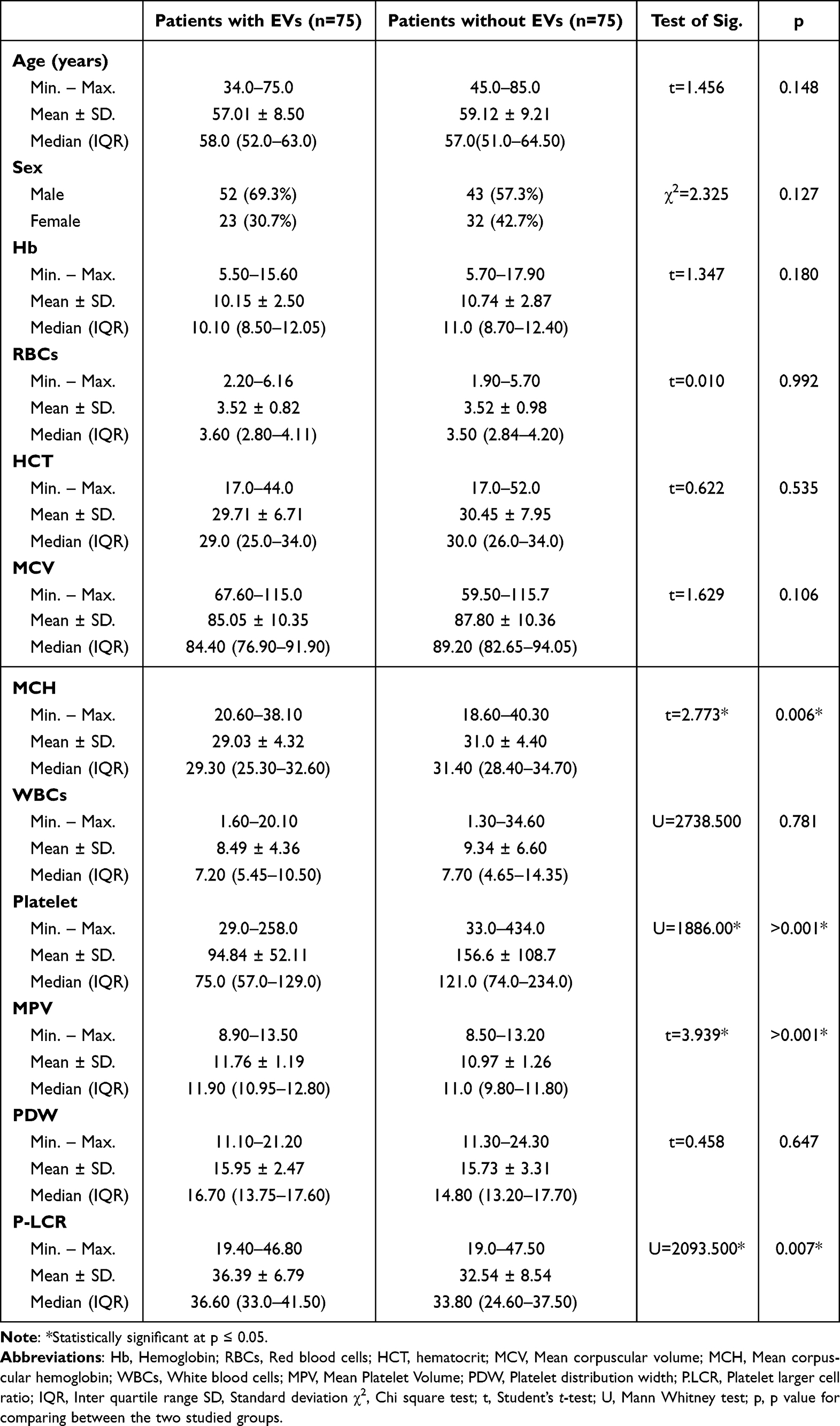 |
Table 1 Comparison of Demographic and CBC Parameters Between Cirrhotic Patients with and without Esophageal Varices |
 |
Table 2 Comparison of Different Parameters Between Cirrhotic Patients with and without Esophageal Varices |
Genotype and Allele Distribution
The allelic and genotypic distributions of HPA-1, HPA-2, and HPA-3 were consistent with Hardy–Weinberg equilibrium, and no linkage disequilibrium was observed (p > 0.05).
A borderline difference was observed in the allelic and genotypic frequencies of HPA-3 between patients with and without EVs (p = 0.051), which did not reach statistical significance. However, the HPA-3 a/a genotype appeared more frequent among patients with EVs (Table 3).
 |
Table 3 Comparison of Genotypic and Allelic Frequencies of HPA-1, HPA-2, and HPA-3 Between Cirrhotic Patients with and without Esophageal Varices |
Genotype and EV Severity
A statistically significant association was observed between HPA genotypes and EV grades (p < 0.001). The a/a and a/b genotypes, as well as allele “a” of HPA-1 and HPA-3, were more frequently observed in patients with higher-grade varices (grade III/IV). In addition, the HPA-2 “b” allele showed a significant association with grade IV EVs (p = 0.002) (Table 4).
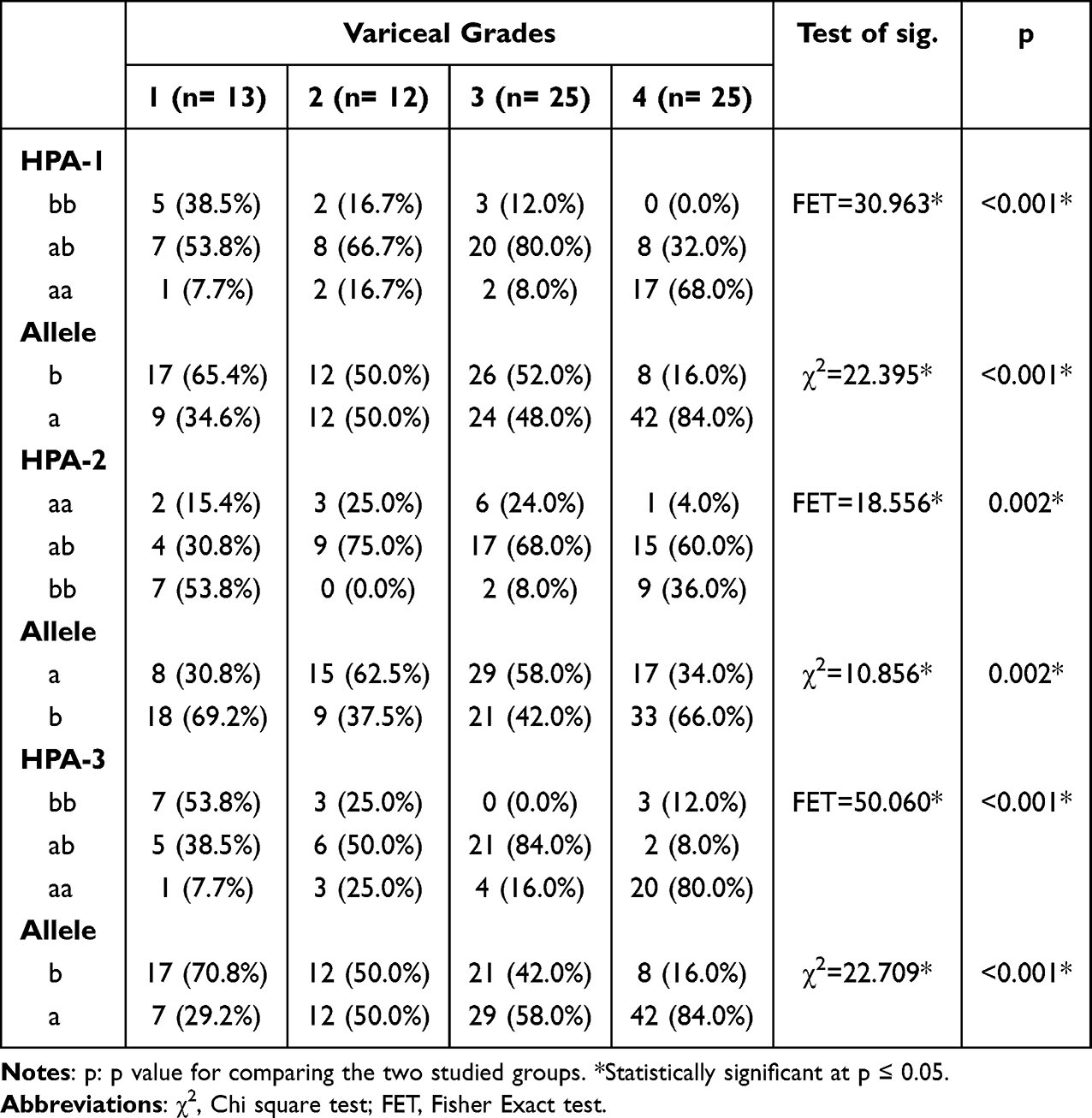 |
Table 4 Association Between Esophageal Variceal Grades and HPA-1, HPA-2, and HPA-3 Genotypes in Cirrhotic Patients with Esophageal Varices (n = 75) |
Genotype and Platelet Parameters
Patients carrying the HPA-1 a/a and HPA-3 a/a genotypes tended to have lower platelet counts and reduced platelet count-to-spleen diameter ratios compared to other genotypes. However, these differences were not statistically significant (p > 0.05).
Multivariate Analysis
Multivariate logistic regression analysis identified serum creatinine and portal vein diameter as independent predictors of the presence of esophageal varices (p < 0.05), while HPA polymorphisms were not independent predictors after adjustment for clinical and hemodynamic variables (Table 5).
 |
Table 5 Univariate and Multivariate Logistic Regression Analysis of Factors Associated with the Presence of Esophageal Varices in Cirrhotic Patients |
Discussion
The risk of variceal development and bleeding closely correlates with the severity of liver disease and remains a significant cause of mortality among cirrhotic patients.7 This is supported by recent studies demonstrating that the progression of portal hypertension and hepatic structural changes directly influences the occurrence of esophageal varices and related complications.
Thrombocytopenia is a well-established hematological abnormality linked to portal hypertension and EV development in cirrhotic patients. Platelet counts often fall below 150,000/μL due to hypersplenism, reduced thrombopoietin production, bone marrow suppression, and increased peripheral destruction.7
In the present study, patients with EVs showed significantly lower platelet count and PC/SD ratio, consistent with findings by Mostafa et al,8 Hayashi et al,9 and Nouh et al10 Previous studies have demonstrated that combining platelet count, spleen diameter, and Doppler ultrasound parameters improves diagnostic accuracy for EVs.11 A platelet count ≤121,000/μL and splenic diameter >145 mm were reported as strong indicators of EV presence.7 Similarly, the PC/SD ratio, with a proposed cutoff ≤818, has been validated as a cost-effective and non-invasive screening tool.12,13 Shear wave elastography has also shown correlation with variceal development.14
In agreement with these findings, splenic diameter and portal vein diameter (PVD) were significantly higher in patients with EVs in our study. Bhattarai et al reported a PVD cutoff of 12.25 mm with high predictive accuracy,15 whereas Mathur et al found no significant association,16 which may reflect differences in study populations, disease stages, or portal hemodynamics.
Human platelet antigens (HPAs) are polymorphic glycoproteins that influence platelet immunogenicity and function. Their relevance is particularly evident in HCV-related cirrhosis, where immune-mediated cytopenias are common. Abd El Aal et al reported that the HPA-3ab genotype may have a protective effect against advanced fibrosis in HCV patients,17 while El Sayed et al linked the HPA-3a allele to extrahepatic manifestations in HCV-infected individuals.18
In the present study, the HPA-3 a/a genotype and allele “a” were more frequently observed among cirrhotic patients with EVs. However, this finding requires cautious interpretation. Previous reports have associated the HPA-3b allele with thrombocytopenia in conditions such as COVID-19,19 creating an apparent discrepancy. This inconsistency may be explained by differences in disease context, underlying mechanisms, and study endpoints. While earlier studies focused primarily on platelet count and immune-mediated destruction, our study assessed portal hypertension-related complications. It is therefore plausible that the HPA-3 “a” allele may be linked to pathways influencing fibrosis progression or vascular remodeling rather than directly affecting platelet count.
Although our findings suggest an association between HPA polymorphisms and EV presence and severity, these polymorphisms did not remain independent predictors after multivariate analysis. This indicates that HPA variants may reflect disease severity rather than serve as standalone predictive markers.
The association between HPA genotypes and EV severity observed in this study, particularly the higher frequency of HPA-1 and HPA-3 a/a genotypes in grade III/IV EVs, further supports the potential role of genetic factors in disease progression. However, this association should be interpreted as contributory rather than causative.
In addition, cirrhotic patients with EVs carrying HPA-1 (a/a), HPA-2 (b/b), and HPA-3 (a/a) genotypes demonstrated lower platelet counts and PC/SD ratios, along with higher MPV, PDW, and P-LCR values. These findings suggest a potential link between HPA polymorphisms and altered platelet morphology and function, which may indirectly contribute to portal hypertension and variceal formation.
From a clinical perspective, the identification of HPA polymorphisms may provide additional insight into individual susceptibility to EV development. However, these findings do not support the use of HPA genotyping as a standalone screening or predictive tool in routine clinical practice. Established parameters such as platelet count, spleen size, and portal vein diameter remain more practical and clinically validated.
Moreover, although PCR-based genotyping is technically feasible, its cost, limited availability, and lack of standardized clinical utility restrict its application in routine settings, particularly when compared with widely available and cost-effective non-invasive tools such as PC/SD ratio and ultrasonography.
This study has several limitations. It was conducted at a single center, which may limit generalizability. The cross-sectional design precludes establishing causal relationships. No functional studies were performed to directly assess the biological impact of HPA polymorphisms. Additionally, the absence of an external validation or replication cohort limits the strength of the conclusions.
Future multicenter studies with larger sample sizes and longitudinal follow-up are needed to validate these findings and further clarify the role of HPA polymorphisms in liver disease progression and portal hypertension.
In conclusion, the HPA-3 a/a genotype was associated with esophageal varices in cirrhotic patients but was not an independent predictor. Further studies are needed to confirm its clinical relevance.
Ethical Standards
The study was approved by the IRB of the National Liver Institute, Menoufia University (Protocol No: 00569/2024), and conducted in accordance with ethical standards, including the Declaration of Helsinki and its amendments.
Informed Consent
Informed Consent was obtained from all participants included in the study.
Acknowledgments
The authors would like to express their sincere gratitude to Dr. Sally Waheed Elkhadry - Department of Epidemiology and Community Medicine, National Liver Institute, Menoufia University, Shebin Elkom, Egypt - for her valuable contribution to the statistical analysis of this study.
Funding
There is no funding to report.
Disclosure
The authors declare that there is no conflict of interest in this study.
References
1. Gralnek IM, Dumonceau JM, Kuipers EJ, et al. Diagnosis and management of acute esophageal variceal hemorrhage: ESGE guideline. Endoscopy. 2022;54(11):1094–11. doi:10.1055/a-1939-4887
2. de Franchis R, Bosch J, Garcia-Tsao G, et al. Baveno VII - Renewing consensus in portal hypertension. J Hepatol. 2022;76(4):959–974. doi:10.1016/j.jhep.2021.12.022
3. Curtis BR, McFarland JG . Human platelet antigens and their role in platelet transfusion therapy. Transfus Med Rev. 2013;27(4):207–214.
4. Zhou Y, Liu D, Chen J, et al. Association between HPA-15 polymorphism and serum laminin levels in chronic hepatitis C patients. Hepatol Res. 2021;51(2):134–141.
5. Ding DF, Wu LF, Wang P, et al. Target-controlled infusion of propofol and remifentanil combined with dexmedetomidine reduces functional endoscopic sinus surgery bleeding. Exp Ther Med. 2017;14(5):4526–4531.
6. Fang L, Wang Q, Xu Y. Postoperative discharge scoring criteria after outpatient anesthesia: a review of the literature. J Perianesth Nurs. 2023;38(4):642–649.e641. doi:10.1016/j.jopan.2022.11.008
7. Mohsen W, Elhady M, Ahmed R, et al. Noninvasive predictors of esophageal varices in cirrhotic patients. Clin Exp Hepatol. 2023;9(1):15–23. PMID: PMC10750066.
8. Mostafa M, Hassouna M, Abou El-Magd A, et al. The use of platelet count/spleen diameter ratio as a non-invasive predictor of esophageal varices in cirrhotic patients. J Gastroenterol Hepatol Res. 2020;9(3):3096–3102.
9. Hayashi H, Beppu T, Masuda T, et al. Platelet count/spleen diameter ratio as a predictor of esophageal varices in patients with liver cirrhosis. J Gastroenterol Hepatol. 2014;29(2):324–330.
10. Nouh A, Eissa M, Ahmed A. Platelet count and spleen size as predictors of esophageal varices in cirrhotic patients. Egypt J Intern Med. 2018;30(2):66–71.
11. Charoenchue R, Suksamai W, Sornkayasit K, Akkarachaneeyakorn S, Li D, Yan -L-L. Non-invasive predictors of esophageal varices in hepatitis C-related liver cirrhosis. BMC Gastroenterol. 2023;23(1):48. doi:10.1186/s12876-023-02633-9
12. Hassouna MG, El-Amir MI, El-Mohamady AM, El-Sayed GG. Clinical value of platelet count/spleen diameter ratio in the prediction of esophageal varices in cirrhotic patients. Int J Trop Dis Health. 2022;43(23):10–20.
13. Bangaru SS, Reddy SK, Jonnalagadda SR, Rao GV. Platelet count/spleen diameter ratio as a non-invasive predictor of esophageal varices in liver cirrhosis. Hepatol Int. 2020;14(2):307–314.
14. Abdelwahab MA, El-Gharabawy RM, Ghonimy NE, Shaltout MB. Role of portal vein velocity and transient elastography in the prediction of esophageal varices in cirrhotic patients. Egypt Liver J. 2024;14(1):1–8. doi:10.1186/s43162-024-00311-x
15. Bhattarai B, Rijal S, Bansal R, et al. Correlation of portal vein diameter and splenic size with presence of esophageal varices in cirrhosis of liver: a prospective study in tertiary care center. Kathmandu Univ Med J. 2014;12(47):181–185. PMID: 25799857.
16. Mathur A, Elhence A, Aggarwal R, et al. Noninvasive prediction of large esophageal varices in cirrhosis: is there still a role for ultrasonography? Saudi J Gastroenterol. 2020;26(1):20–25. doi:10.4103/sjg.SJG_370_18
17. Abd El Aal DE, Amer HE, El Sayed M, et al. Association between human platelet antigen (HPA)-3 polymorphism and hepatic fibrosis in Egyptian patients with chronic hepatitis C. Egypt J Med Hum Genet. 2019;20(1):4. doi:10.1186/s43042-019-0008-1
18. El Sayed M, Abd El Aal DE, El Ashry H, et al. Human platelet antigen-3 polymorphism and its association with rheumatologic manifestations in females with chronic hepatitis C virus infection. Clin Exp Hepatol. 2020;6(1):25–30. doi:10.5114/ceh.2020.93671
19. Ghaffari S, Amiri MM, Jafarzadeh A, et al. Association of HPA-3 polymorphism with thrombocytopenia in COVID-19 patients. Platelets. 2023;34(5):624–633.
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Prediction of High-Risk Varices in Patients with Compensated Advanced Chronic Liver Disease in Saudi Arabia
Ismail M
Clinical and Experimental Gastroenterology 2023, 16:117-127
Published Date: 19 July 2023
Clinical Audit of Non-Selective Beta Blockers Titration in the Management of Portal Hypertension at a National Hospital in Tanzania
Pazi SK, Mwanga AH, Lyuu TA, Ng’wanasayi M, Rwegasha J, Komba EV, Nkandala I
Clinical Audit 2024, 16:39-44
Published Date: 18 April 2024
The Adjunctive Efficacy of Fuzheng Huayu Tablet on Portal Hypertension with HBV Related Cirrhosis: A Protocol for a Multicenter Randomized Controlled Trial
Li Z, Guo Y, Huang J, Lv J, Liu C
Open Access Journal of Clinical Trials 2025, 17:51-61
Published Date: 3 June 2025