Back to Journals » Journal of Multidisciplinary Healthcare » Volume 19
Physicians’ Knowledge and Practice Regarding Multiple Sclerosis (MS) in Saudi Arabia: A Cross-Sectional Study
Authors Abdallah MS ![]() , Mahafdeh R
, Mahafdeh R ![]() , Alrubayyi BZ, AlRasheed HA
, Alrubayyi BZ, AlRasheed HA ![]()
Received 6 February 2026
Accepted for publication 10 April 2026
Published 21 April 2026 Volume 2026:19 601699
DOI https://doi.org/10.2147/JMDH.S601699
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Charles V Pollack
Mahmoud S Abdallah,1 Rania Mahafdeh,2 Bayan Ziyad Alrubayyi,3,4 Hayam Ali AlRasheed5
1Department of PharmD, Faculty of Pharmacy, Jadara University, Irbid, Jordan; 2Department of Doctor of Pharmacy, Faculty of Pharmacy, Jadara University, Irbid, Jordan; 3Department of Pharmacy, Faculty of Pharmacy, Jadara University, Irbid, Jordan; 4Al-odah United Pharmacy for Medicines, Al-Jouf, Saudi Arabia; 5Department of Pharmacy Practice, College of Pharmacy, Princess Nourah bint Abdulrahman University, Riyadh, Saudi Arabia
Correspondence: Mahmoud S Abdallah, Department of PharmD, Faculty of Pharmacy, Jadara University, Irbid, Jordan, Email [email protected] Hayam Ali AlRasheed, Department of Pharmacy Practice, College of Pharmacy, Princess Nourah bint Abdulrahman University, Riyadh, Saudi Arabia, Email [email protected]
Background: Multiple sclerosis (MS) is a chronic central nervous system disorder induced by the immune system. It gets worse over time and is characterized by inflammation, demyelination, and marked disability.
Aim: To assess the knowledge and practices of physicians regarding MS care in Saudi Arabia.
Methods: This observational cross-sectional study included licensed physicians (neurologists, psychiatrists, neurosurgeons, and primary care physicians) practicing in Saudi Arabia. The data was collected using a content-validated questionnaire. Physicians were requested to answer from different locations, and a Google Form was used to collect the replies. Descriptive statistics and multivariate regression were performed to identify the factors affecting knowledge, practice and self-confidence among physicians.
Results: A total of 220 participants participated in the study. The knowledge score was 12.9 ± 4.05 out of 25, the practice score was 18.3 ± 5.84 out of 35, and the self-confidence score was 49.11 ± 13.99 out of 100. In multivariate analysis, possessing an MS-related certification emerged as the most significant predictor of increased knowledge (β = 6.324, p < 0.001). Having an MS specialization was second (β = 2.468, p = 0.021), and clinical experience was third (β = 2.180, p < 0.001). Having an MS subspecialization (β = 5.030, p = 0.002), an MS certification (β = 7.998, p < 0.001), or clinical experience (β = 3.447, p < 0.001) was also a good independent predictor of practice scores. The effects of MS subspecialization (β = 9.813, p = 0.020), MS certification (β = 14.863, p < 0.001), and years of experience (β = 8.493, p < 0.001) on confidence scores were statistically significant.
Conclusion: Physicians demonstrated moderate knowledge, practice but relatively low confidence regarding MS care, with significant gaps among non-specialists and less experienced clinicians. MS-specific certification, subspecialty training, and clinical practice are the key determinants for improved knowledge and practice.
Keywords: multiple sclerosis, physician knowledge, clinical practice, neurology training, Saudi Arabia
Introduction
Multiple sclerosis (MS) is a chronic autoimmune demyelinated disease of the central nervous system affecting brain, spinal cord, and optic nerves. Inflammation, demyelination, nerve loss and degeneration can all characterize the disease.1 MS primarily affects young adults, with a higher prevalence in females, and is a leading cause of non-traumatic neurological disability among this age group.2 Genetics and the environment are two of the many reasons it happens. But it grows worse at different speeds and varies for each person.3
Researchers believe that more than 2.8 million people around the world have MS.4 There have been a lot more patients with MS in the Middle East, especially in the Gulf area, in the past twenty years. More individuals are living in cities, healthcare professionals are learning more about illness, and more people are becoming aware of it.5 Previous reports from the Kashmir Valley of India demonstrated a lack of data on the prevalence rate of multiple sclerosis in this region, and more studies were needed among scientists and clinicians to investigate the pattern of prevalence of MS.6 A lack of specialists and diagnostic facilities led some physicians to claim MS was absent. However, after specialized neurology services were established, Zahoor et al demonstrated high prevalence of female patients and MS pattern in Kashmir was found to be relatively similar to West and rest of the Asia. However, larger comprehensive studies were needed to know the actual number of MS patients in India and Asia region.7
According to national records and regional research.5 MS is growing more widespread in Saudi Arabia, especially among young individuals. According to Saeedi et al,8 the rate is 62 per 100,000 people in KSA and 40 per 100,000 people in other regions. This shows how crucial it is to seek good medical care and take better care of sick people. Neurologists are highly crucial for determining what is wrong with patients who have MS and helping them get better. If they think, act, and treat patients well, they perform a terrific job. This is especially true when it comes to picking procedures, sticking to them, and developing long-term plans for treatment.9
Disease-modifying therapies (DMTs) are drugs that help people with MS avoid unexpected relapses, feel better, and reduce the disease’s progress. These drugs alter or impair the immune system. During the relapsing phase, their primary function is to reduce the frequency of relapses, inhibit the accumulation of magnetic resonance imaging (MRI) lesions, and stabilize or marginally enhance mobility.10 Interferons and glatiramer acetate were the first DMTs to be discovered by accident.11
Natalizumab (which stops adhesion) and S1P receptor modulators such fingolimod, siponimod, and ozanimod (which keep lymphocytes from getting into cells) fared better in MS.12,13 This led to the development of therapies that eliminate B lymphocytes. There have been many studies on rituximab, ocrelizumab, and ofatumumab. These are monoclonal antibodies that target CD20. They have been shown to reduce the frequency of relapses, decelerate the advancement of relapsing-remitting multiple sclerosis (RRMS), and diminish disability in primary progressive multiple sclerosis.1
In the last ten years, it has been learned that B cells are just as important as T cells for the growth of MS. Despite significant advancements in RMS therapy, effective treatment for advanced MS remains elusive.3
Even while clinical practice has improved and there are new approaches to treat patients, it is still hard to make care more consistent and relate to patients in a way that is focused on them. The quality of care for individuals with MS may be influenced by the proficiency of neurologists in diagnosing the condition, identifying symptoms, and formulating tailored care plans.14 Neuropsychiatric cases require a multidisciplinary approach for effective management, so involving other specialists such as psychiatrists and neurosurgeons in addition to the neurologists in patients care is important for effective MS management.15 Özge et al demonstrated that collaborate between healthcare providers such as family medicine, neurology, and psychiatry can provide the best possible care for patients with complex neuropsychiatric cases.15 In Saudi Arabia, there is a lack of comprehensive data evaluating the current state of neurologists’ preparedness and approaches to MS care. In recent studies, the findings demonstrated minority of HCPs in Saudi Arabia, who have good knowledge and effective communication about the treatment management with patients diagnosed with MS especially that many patients have communication difficulties.16,17 Kadasah et al demonstrated that HCPs in Saudi Arabia should continuously educated about MS managements.17
The aim of this study is to evaluate physicians’ knowledge and practices related to multiple sclerosis (MS) in Saudi Arabia and to assess their preparedness for effective patient management. Specifically, the study examines physicians’ self-reported knowledge of MS diagnostic criteria, treatment sequencing, and symptom management; evaluates their clinical skills and routine MS care practices; assesses their confidence in discussing MS-related issues with patients; explores competencies in patient-centered care with an emphasis on quality-of-life considerations; and investigates the association between physicians’ demographic and professional characteristics and their levels of knowledge and practice.
Methods
Study Design
This study was an observational, cross-sectional study that targeted physicians practicing in Saudi Arabia. Data collection began in May 2025 and continued until the required sample size was achieved. The study received ethical approval from the Institutional Review Board (IRB) of the Faculty of Pharmacy, Jadara University, with IRB number (PHARM-JA-21/2025) and administration support from the research center and studies department in AL-Jouf health cluster via Email to facilitate the implementation of the study. Written informed consent was obtained from all participants prior to survey administration. All responses were anonymized and handled with strict confidentiality.
Population
The study population comprised licensed physicians practicing in Saudi Arabia, including neurologists, psychiatrists, neurosurgeons, and primary care physicians, who were actively involved in patient care with a clinical workload of at least 50% and were currently managing patients with multiple sclerosis (MS). Physicians who were retired, not actively practicing, or not involved in MS care were excluded. The sample size was calculated based on an assumed 50% prevalence of adequate knowledge, as reported by Péloquin, Schmierer, Leist, Oh, Murray and Lazure,14 with a 95% confidence level and a 7% margin of error, yielding a minimum required sample of 196 participants. To compensate for potential non-response, a 10% increment was applied, resulting in a final target sample size of approximately 220 physicians.

Data Collection Tool
Knowledge, practices, and confidence were assessed using a structured, peer-reviewed, and content-validated questionnaire adapted from previously published study (Péloquin et al, 2021, Multiple Sclerosis and Related Disorders) with permission from Elsevier (License No. 6236970732994) through the Copyright Clearance Center (RightsLink licensing system) and evaluated by an expert panel.14 The instrument demonstrated excellent reliability in a pilot study of 60 participants, with a Cronbach’s alpha of 0.946 for the overall scale, and 0.82, 0.89, and 0.97 for the knowledge, practice, and confidence domains, respectively. The questionnaire comprised five main sections:
- Sociodemographic questions include gender, age, specialty, subspeciality in MS, certification/training in MS, clinical care major, experience years, number of patients diagnosed, clinical practice place, working in academic setting major, and residence in either small cities (Taif, Abha, Khamis Mushait, Buraydah, Unayzah, Hail, Tabuk, Najran, Jazan, Sakaka, Arar) or major cities (Riyadh, Jeddah, Makkah Al-Mukarramah, Al-Madinah Al-Munawwarah, Al-Khobar, Dhahran).
- Questions 1–10 about the people who live there and their work history: It lists the country, the job title, the number of years of experience, the internship training, and the place of work.
- People who took the knowledge test (Q10) were asked to rate how much they knew about MS, how to use the McDonald criteria to identify it, the treatment plan, and how to spot symptoms that are not normal. The total score is 25; 5 points for each item of the Likert scale.
- Practice Domain (Q11–Q12): We asked the respondents how they could use diagnostic criteria, deal with symptoms, and understand clinical tools that were related to MS. The total score is 35; 5 points for each item of the Likert scale.
- Confidence in Patient Communication (Q13): We asked the respondents to rate themselves about their confidence levels using a scale of (0–100) regarding discussions of diagnosis, treatment, and psychosocial impacts. The total score is 100, calculated as the average score of all items; each item has a score of 100.
- MS Care and Quality of Life (Q14): Evaluated agreement with statements reflecting values toward holistic and patient-centered care.
As no validated cutoff values were available, no predefined categories (eg, low, moderate, high) were applied, and interpretation was based on proportional score distribution.
Recruitment
Physicians were invited to respond through via social media platforms, including WhatsApp groups, hospital networks, national conferences, professional societies, and online neurology forums across Saudi Arabia. A convenience sampling approach was used, whereby physicians who had access to these platforms and were willing to participate completed the survey voluntarily. Due to the open distribution of the survey link, the total number of physicians invited could not be determined, and therefore a response rate could not be calculated.
Data Analysis
Frequencies, means, and standard deviations were used to describe the characteristics of the participants and their answers to the knowledge, skills, and practices questions. Discrete variables with many categories (+20) were treated as continuous. Normality of the numerical variables was assumed according to the central limit theory.18 Outcome variables were the knowledge score (score of 25), skills and practice score (score of 35), and self-confidence score (score of 100). In the inferential univariate analysis, to test the difference in knowledge, skills, and practices scores across demographic and baseline characteristics, the independent t-test was used for 2-category comparisons, or the ANOVA test followed by post hoc Tukey’s test was used for more than 2-category comparisons. Assumptions of ANOVA were checked for the validity of its results, including independence, normality, and homogeneity of variance. The Pearson correlation test was used to test the correlation between continuous demographic data and the outcome scores. Multivariate linear regression analyses to find independent variables while taking into account possible confounding factors. All linear regression assumptions were satisfied for knowledge, practice, and confidence scores. The models showed good fit, explaining 56.8% (R2=0.584; adj. R2=0.568; R=0.764), 53.1% (R2=0.550; adj. R2=0.531; R=0.742), and 43.2% (R2=0.455; adj. R2=0.432; R=0.675) of the variance, respectively. Durbin–Watson statistics (2.11, 2.08, and 2.15) indicated independence of residuals, and VIF values <3 confirmed absence of multicollinearity. A few outliers were detected (five in knowledge, one in practice, and one in confidence) but had no impact on estimates after sensitivity analysis. Residuals met homoscedasticity and normality assumptions based on visual inspection of histogram and normal probability (P-P) plots. A p-value of less than 0.05 was thought to be statistically significant. All of the studies were done with SPSS version 27 or a similar statistical program.
Results
Sociodemographic and Response Data
The sociodemographic and occupational data for the 220 participants involved in the study are presented in Table 1. The responses to the knowledge, practice, and MS care domains are shown in Table 2, and the responses to the confidence domain are illustrated in Figure 1. The mean scores were 12.9 ± 4.053, 18.3 ± 5.84, and 49.11 ± 13.99 for knowledge, practice, and confidence, respectively.
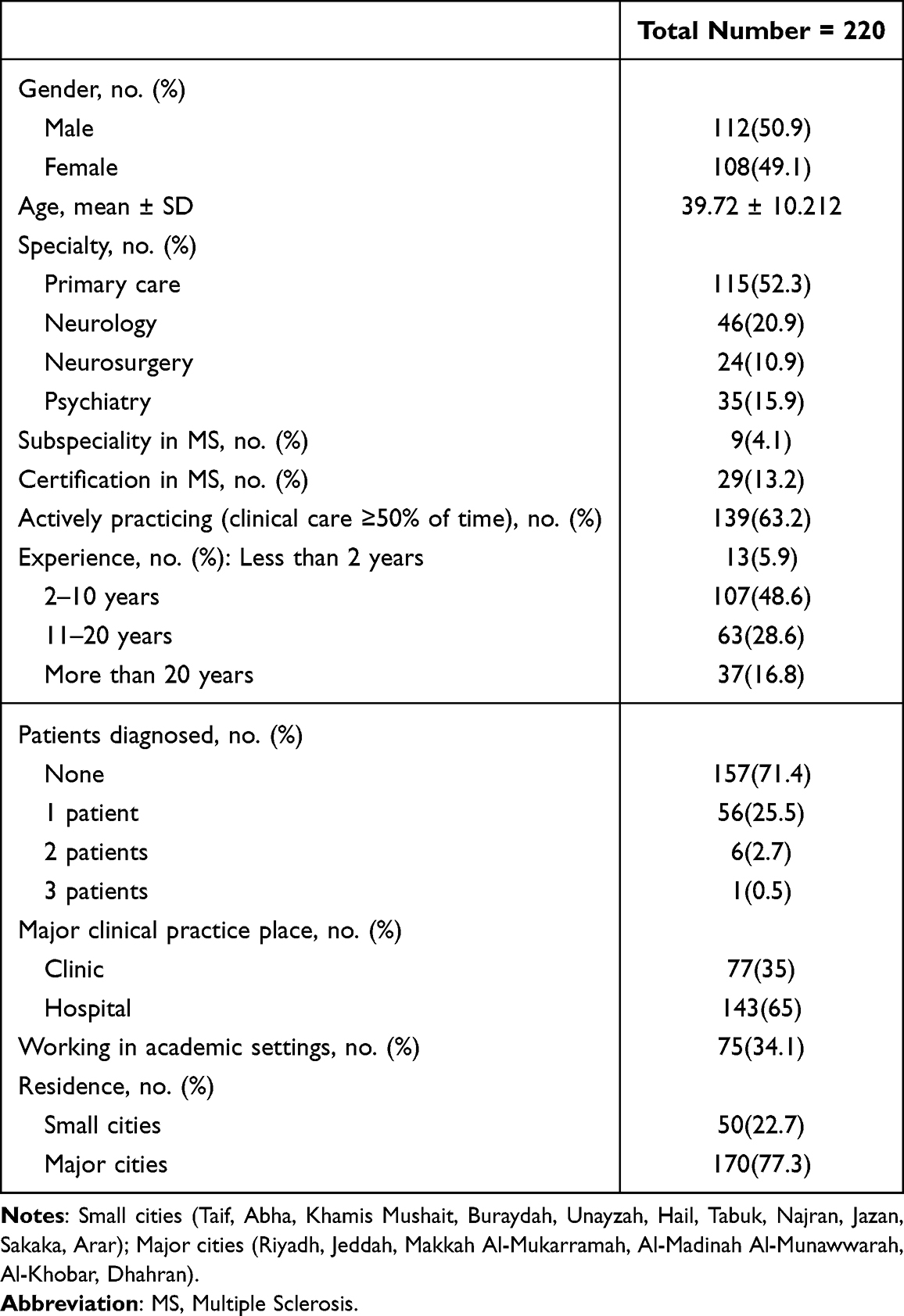 |
Table 1 Respondents Characteristics |
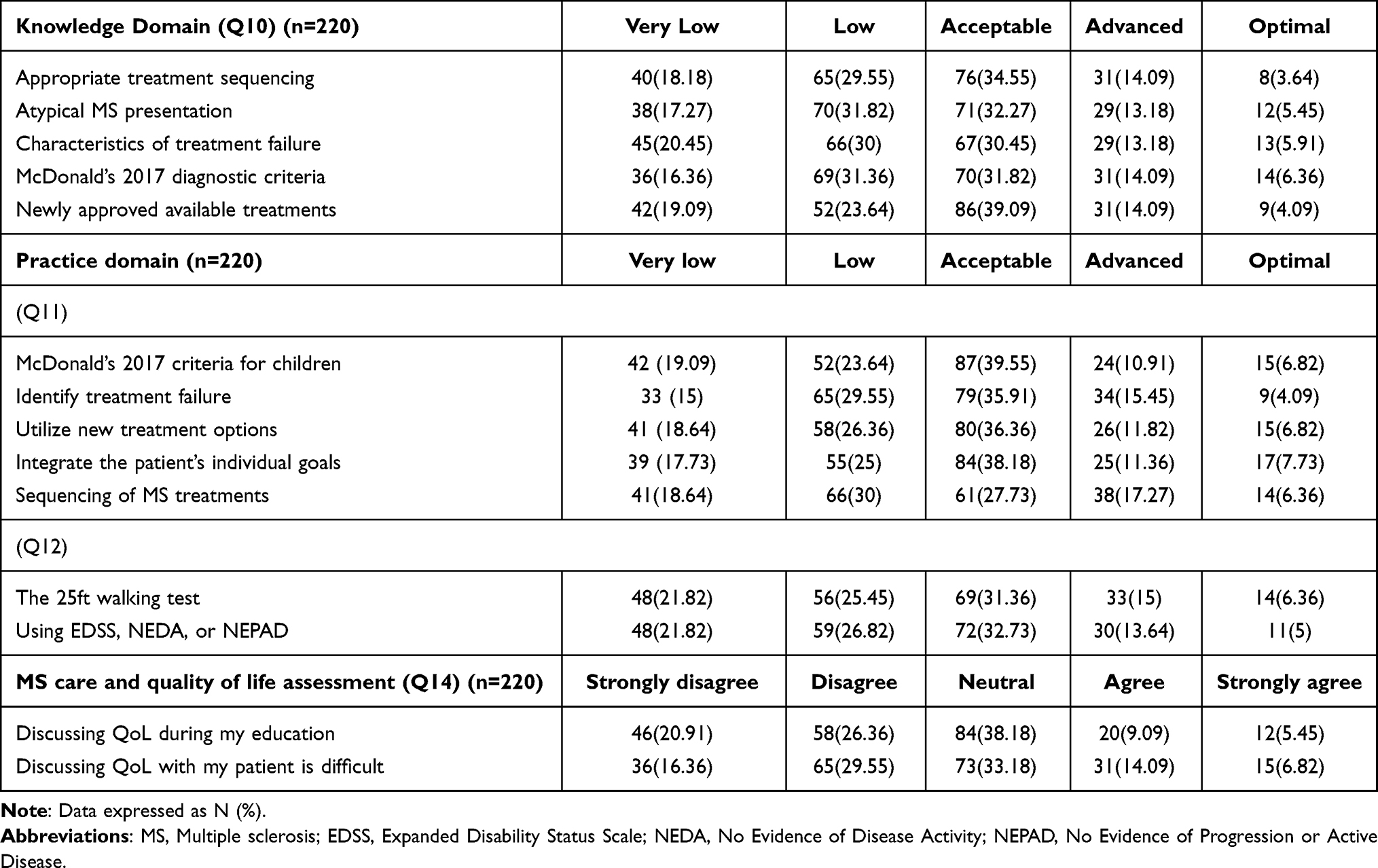 |
Table 2 Responses to the Questionnaire Domains |
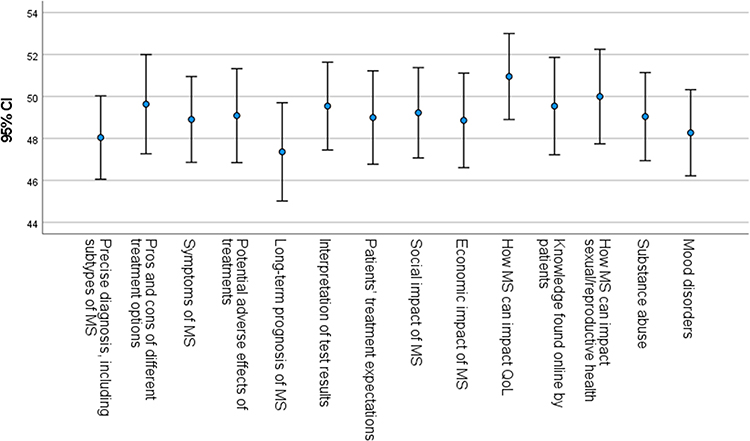 |
Figure 1 Confidence domain responses among all respondents. |
Knowledge-Associated Factors
Knowledge scores did not differ by gender (p = 0.939) or by city size (p = 0.329), but showed a strong positive correlation with age (r = 0.311, p < 0.001). Neurologists scored significantly higher than other specialties (15.80 ± 3.92, p < 0.001). Physicians with an MS subspecialty (19.33 ± 1.66) or MS certification (19.59 ± 1.27) also had higher knowledge scores than those without (p < 0.001). Direct patient care was associated with greater knowledge (p = 0.008). Experience positively influenced scores (p < 0.001), with physicians having 11–20 years (15.00 ± 3.86) or >20 years (15.38 ± 3.43) outperforming less experienced peers. Diagnosing ≥2 MS patients was linked to higher knowledge (p = 0.003), while non-academic physicians scored higher than academic physicians (p = 0.017).
Practice-Associated Factors
Practice scores did not differ by gender (p = 0.677), city versus rural location (p = 0.247), academic involvement (p = 0.192), or primary clinical setting (clinic vs. hospital, p = 0.218), but were positively correlated with age (r = 0.308, p < 0.001). Neurologists had the highest practice scores (22.17 ± 6.14), significantly exceeding general care physicians (17.07 ± 6.08), neurosurgeons (17.50 ± 3.32), and psychiatrists (17.77 ± 3.49; p < 0.001). Physicians with an MS subspecialty (27.89 ± 3.26) or MS certification (27.21 ± 3.03) also scored higher than those without (p < 0.001). Practice improved with experience (p < 0.001), with clinicians having 11–20 years (21.13 ± 5.65) or >20 years (22.22 ± 5.08) outperforming less experienced peers. Additionally, physicians who had diagnosed ≥2 MS patients had the highest practice scores (27.17 ± 3.49; p < 0.001).
Confidence-Associated Factors
There was no significant difference in confidence between males and females (p = 0.837) or among physicians based on clinical setting—clinical care (p = 0.394), academic institutions (p = 0.753), or clinics/hospitals (p = 0.339). Confidence, however, showed a strong positive correlation with age (r = 0.327, p < 0.001). Neurologists were the most confident (57.31 ± 13.43), compared to general care physicians (45.55 ± 14.40), neurosurgeons (49.05 ± 12.38), and psychiatrists (50.04 ± 9.35; p < 0.001), reflecting their extensive experience with MS patients. Physicians with an MS subspecialty (66.98 ± 5.01) or MS license (66.13 ± 5.56) were also significantly more confident than those without (p < 0.001).
Confidence increased with clinical experience (p < 0.001), with physicians having 11–20 years (55.07 ± 13.21) or >20 years (59.19 ± 9.23) of experience scoring higher. It also rose with the number of MS cases diagnosed (p = 0.012), peaking at 64.88 ± 5.12 for those with ≥2 cases. Additionally, physicians residing in towns reported higher confidence (50.45 ± 12.89) than those in smaller cities (44.54 ± 16.53; p = 0.008).
Multivariate Analysis
Higher knowledge scores were independently associated with having a subspecialty in multiple sclerosis (β = 2.47, p = 0.020), holding MS-related certification (β = 6.32, p < 0.001), and greater clinical experience (β = 2.17, p < 0.001). In contrast, age, sex, active clinical practice status, primary practice setting, and city size were not significant predictors of knowledge score (p > 0.05). Moreover, higher practice scores were significantly predicted by having an MS subspecialty (β = 5.03, p = 0.002), MS-related certification (β = 8.00, p < 0.001), and greater clinical experience (β = 3.45, p < 0.001). Conversely, age, sex, active clinical practice status, primary practice setting, and city size were not significantly associated with practice scores (p > 0.05). Additionally, higher confidence scores were independently associated with having an MS subspecialty (β = 9.81, p = 0.020), MS-related certification (β = 14.87, p < 0.001), greater clinical experience (β = 8.51, p < 0.001), and practicing in major cities (β = 4.98, p = 0.004). In contrast, age, sex, active clinical practice status, and primary practice setting were not significant predictors of confidence (p > 0.05).
Discussion
This study aimed to assess the knowledge, skills, practice, and confidence of physicians regarding MS in Saudi Arabia. The findings reveal insufficient knowledge and skills among physicians who are non-neurologists compared to neurologists, highlighting the importance of subspecialized training and targeted education programs in improving MS knowledge.19
This study is significant due to its extensive data collection and its status as one of the initial investigations into MS-related skills among a multidisciplinary group of physicians in Saudi Arabia. This study provides crucial insights into the knowledge, practice, and levels of trust that influence evaluations of healthcare policy, changes in medical education, and targeted professional development programs.20
The findings of this study are crucial for comprehending the treatment of MS in Saudi Arabia. While all items included in knowledge and practice scores were rated as “moderate” on average, there was a notable lack of “advanced” or “optimal” proficiency across the board. In addition, the average confidence score was 49.11 out of 100, which is relatively low. This interpretation is based on the percentages rather than fixed categories. This suggests that while many physicians have a foundational understanding of MS, they lack the deep expertise required for nuanced clinical decision-making.
Specifically, the study pinpointed weaknesses in critical areas such as the application of the McDonald 2017 diagnostic criteria (especially in pediatric populations), sequencing of MS treatments, and familiarity with newly approved therapies. These gaps are concerning, as they can lead to diagnostic delays and suboptimal treatment choices. Furthermore, a low level of proficiency in using standardized neurological assessments like the EDSS indicates a potential disconnect between clinical practice and evidence-based standards for monitoring disease progression.21,22
The present study demonstrates that the respondents had greater knowledge and better practice if they got training/certification in MS, specialized in MS care, and had more years of experience. The present study demonstrates that the respondents were quite sure of themselves when they talked about different MS issues. The regression analysis, on the other hand, indicated that this trust is not spread out evenly. If respondents have an MS subspeciality, specific training/certification, clinical experience, and major city residence, they can make a more trusting decision. Some small city physicians may have lower confidence because they cannot easily get to the tools and knowledge they need.
Lastly, the present study shows that physicians who learned more about the QoL parts of MS care are missing out. QoL was something that physicians said they felt was not difficult to talk about with their patients, but almost half of them said that it was not something that they learned enough about in medical school. Because of this difference, physicians’ responses may be accepted with their answers, but they may not be based on official, scientific ways to measure QoL. As can be seen, this shows how important structured teaching is for patient-centered care.
The primary findings of this study align with those of other global research, indicating that non-specialist physicians lack sufficient knowledge on MS. Research conducted in Europe and North America indicates that primary care physicians frequently lack confidence in their diagnostic capabilities for MS and their understanding of the complex treatments that can alter the disease’s trajectory. Specializing is a well-known way to learn a lot about long-term disorders that are challenging to treat. Our discovery that neurologists possess much superior scores in knowledge and practice corroborates this assertion.23
The Multiple Sclerosis International Federation (MSIF) affirmed the same thing in the third version of the Atlas of MS: trends are the same all over the world. The respondents who filled out the survey were from 107 different nations and made up 83% of the world’s population. They all agreed that there was at least one key difficulty that made it tougher to find MS early on. The biggest concerns were that 68% of the general public and 59% of healthcare professionals did not know what MS indicators were and that 44% of healthcare professionals did not know enough to recognize MS. A third of the respondents who answered also stated they could not get to medical tests or instruments used by professionals. About 79% of respondents who answered stated the 2017 McDonald criteria were the most common technique to diagnose, although only 34% said they only utilized that version. But 66% of them claimed that at least one obstacle prohibited them from using it. The primary cause was that neurologists either lacked sufficient knowledge or adequate training.24
This study revealed that Saudi physicians have a limited comprehension of critical aspects related to the diagnosis and treatment of MS, achieving moderate knowledge score, in contrast to earlier research. Some of the items that were spoken about were the McDonald 2017 diagnostic criteria, how to pick the best treatment, and when treatment has not worked. The findings indicate that the MS misdiagnosis is not limited to Saudi Arabia. Medical professionals worldwide agreed with the significant challenge of ensuring an adequate number of trained specialists and maintaining current diagnostic standards.25
Our study mirrors prior findings, indicating that non-specialist clinicians possess insufficient knowledge and skills, particularly in areas such as treatment sequencing, identifying treatment failures, and understanding the McDonald 2017 criteria.26
These similarities indicate that the issues related to MS care are not confined to a single area. This is particularly important when it involves prioritizing the patient, disseminating your knowledge, and making informed decisions as a professional. They demonstrate that MS education and practice are ineffective in many regions worldwide.27 The linear regression models show that this is true with strong statistical evidence. This agrees with earlier studies that showed that certification programs can help enhance therapeutic results.
Physicians do not know as much about the McDonald 2017 criteria when the rules for diagnosis change, according to another study. Physicians who are not experts may require some time to become used to new norms and make them a part of their daily life.22 It’s the same thing that’s happening throughout the world that makes practitioners in small cities feel like they do not have confidence. This is because healthcare providers who work outside of cities often have challenges, like being alone at work and not being able to easily get specialized continuing medical education.28 This study is significant since it demonstrates that these issues also exist within the Kingdom’s healthcare system and provide a Saudi perspective on the worldwide discourse.
A comparable cross-sectional study methodology was employed to distribute a pre-existing online survey to 222 neurologists. Everyone filled out the poll. About 14% of participants properly named “periventricular” and “juxtacortical” cancers, and 2% accurately named these terms in 9 out of 10 photographs. Twenty-four percent of participants correctly named all four CNS sites where MRI can spread in space. In two instances, 61% and 71% of individuals accurately indicated that DIT had not been accomplished; yet, 85% and 86% thereafter subscribed to ambiguous historical symptoms lacking objective evidence for DIT fulfillment.29 This study, however, demonstrated that physicians did not possess uniform levels of skill. In this instance, neurologists had a superior average knowledge score (15.8) compared to general practitioners (12.13). This comparison demonstrates that, even within highly specialized domains, standardized diagnostic variables are nonetheless employed in a diverse range of methods. This underscores the significance of continuously engaging in systematic, evidence-based training for the diagnosis and management of MS.19
Consistent with the findings of the present study, a mixed-methods investigation was conducted across Canada, France, Germany, Italy, Spain, the United Kingdom, and the United States. The study included 333 neurologists and 135 nurses with a minimum of two years of experience in caring for individuals with MS. More than one-third of neurologists reported having no or only basic knowledge regarding the characteristics of treatment failure (35%), while 32% indicated limited skills in identifying such failure. Additionally, nearly 39% of neurologists reported low proficiency in integrating patients’ individual goals into treatment recommendations. The study also found significant differences based on years of professional experience in the majority of the 14 assessed confidence domains, particularly in discussions of MS-specific issues with patients. These findings align with the present study’s findings, which demonstrated that physicians’ knowledge, practice, and confidence in managing MS were strongly influenced by their clinical experience and specialized training.14
A cross-sectional study was performed to evaluate the utilization and comprehension of McDonald criteria among German neurologists through a previously created survey instrument that was updated and disseminated to neurology residents and specialists (general neurology, excluding MS subspecialists). Sixty-eight neurologists, comprising forty-two neurology residents and twenty-six neurology specialists, completed the survey. A recurrent misapplication of McDonald’s criteria was identified by the researchers. Thirty-one percent of individuals misidentified unusual symptoms as typical for MS. The comprehension of MRI distribution criteria in space was inadequate. Periventricular and juxtacortical lesions were misidentified by 46% and 55%, respectively. The majority of participants regarded solely anamnestic accounts of prior neurological symptoms, devoid of objective clinical data, as adequate to demonstrate dispersion across time.30
These findings are consistent with our findings, whereas the present study sample showed moderate knowledge about the McDonald’s 2017 diagnostic criteria, emphasizing the importance of incorporating the items in the targeted training program for primary care physicians. Moreover, we found that non-neurologists, particularly those with less experience, showed lower knowledge, providing a chance for more targeted and greater cost-effective educational interventions.
When transitioning from the physician level to the patient level, consider that general knowledge and practice, as well as confidence, are highly correlated with and influence population health, particularly in how MS patients care for themselves and cope with their disorder.31
Beyond physicians, parallel studies among MS patients and the general population in Saudi Arabia and other regions reveal substantial knowledge gaps regarding MS diagnosis, disease course, and treatment. These patient-level deficiencies likely reflect, in part, gaps in physician knowledge and counseling, underscoring the interdependence between provider competence and patient health literacy.32,33
Overall, the present findings reinforce global evidence that structured, continuous, and multidisciplinary MS education is urgently needed. Targeted training programs for non-neurologists, improved dissemination of updated diagnostic criteria, and enhanced access to specialist education, particularly outside major cities, are essential to improve MS care and patient outcomes in Saudi Arabia and beyond.
Limitations
This study has several limitations. First, its cross-sectional design cannot prove causality, precluding any inference of causality. Second, the use of self-reported questionnaires may introduce reporting bias by the respondents themself. Third, the relatively small sample size may limit the generalizability of the findings. Finally, the response rate could not be calculated due to using the convenience sampling approach and open distribution networks such as institutional emails, and social media platforms such as professional WhatsApp groups, which may introduce selection bias and limit the generalizability of the findings. Nonetheless, the findings provide important insights into current gaps in MS-related physician education and practice.
Conclusion
This study concludes that while physicians in Saudi Arabia possess moderate levels of knowledge, practice, and relatively low confidence regarding multiple sclerosis care. It showed that significant and clinically relevant gaps exist, particularly among non-neurologists, those who do not get training or certification in MS care, those who have less clinical care and more academic settings, those who have fewer years of experience, or those who diagnosed fewer patients with MS. In the multivariate regression analysis, neurologists with a subspecialty in MS, certification/training in MS, and years of experience are the significant predictors of knowledge score. Practice scores focusing on proficiency in applying current diagnostic criteria, sequencing advanced treatments, and utilizing standardized assessment tools might be suboptimal, especially among those who are not neurologists, lack a subspecialty in MS care, are not trained or certified in MS, have fewer years of experience, are younger, and diagnose fewer MS patients. In the multivariate regression analysis, neurologists with a subspecialty in MS, certification/training in MS, and years of experience are the significant predictors of practice score. Confidence score is also affected by age, experience, specialty in neurology, subspecialty in MS, certification/training in MS, number of patients diagnosed, and, moreover, residence in a major city. The most powerful predictors of higher knowledge, superior practice skills, and greater confidence are MS-specific training/certification, subspecialty in MS, and extensive clinical experience. These findings underscore that general medical training is insufficient for the complexities of modern MS management. Furthermore, a disparity in confidence between major and small cities suggests a need to address geographical inequities in professional support and education. Given the study’s limitations (cross-sectional design, self-reported data, small sample size, and convenience sampling approach), future research should employ longitudinal designs and larger representative samples to confirm these findings.
Data Sharing Statement
The raw data supporting the conclusion of this article will be made available from the corresponding author upon request.
Acknowledgment
The authors would like to thank Princess Nourah bint Abdulrahman University Researchers Supporting Project number (PNURSP2026R485), Princess Nourah bint Abdulrahman University, Riyadh, Saudi Arabia.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The authors declare no conflicts of interest in this work.
References
1. Florou D, Katsara M, Feehan J, Dardiotis E, Apostolopoulos V. Anti-CD20 agents for multiple sclerosis: spotlight on ocrelizumab and ofatumumab. Brain Sci. 2020;10(10):758. doi:10.3390/brainsci10100758
2. Wallin MT, Culpepper WJ, Campbell JD, et al. The prevalence of MS in the United States: a population-based estimate using health claims data. Neurology. 2019;92(10):e1029–11. doi:10.1212/wnl.0000000000007035
3. Dobson R, Giovannoni G. Multiple sclerosis - a review. Eur J Neurol. 2019;26(1):27–40. doi:10.1111/ene.13819
4. Coetzee T, Thompson AJ. Atlas of ms 2020: Informing Global Policy Change. London, England: SAGE Publications Sage UK; 2020:1807–1808.
5. AlJumah M, Otaibi HA, Al Towaijri G, et al. Familial aggregation of multiple sclerosis: results from the national registry of the disease in Saudi Arabia. Mult Scler J. 2020;6(4):1–7. doi:10.1177/2055217320960499
6. Zahoor I, Haq E, Asimi R. Multiple sclerosis in Kashmir: where we stand. J Neurol Sci. 2017;373:129–133. doi:10.1016/j.jns.2016.12.042
7. Zahoor I, Asimi R, Haq E, Yousuf Wani I. Demographic and clinical profile of multiple sclerosis in Kashmir: a short report. Mult Scler Relat Disord. 2017;13:103–106. doi:10.1016/j.msard.2017.02.018
8. Saeedi JA, AlYafeai RH, AlAbdulSalam AM, et al. Saudi consensus recommendations on the management of multiple sclerosis: diagnosis and radiology/imaging. Clin Transl Neurosci. 2023;7(1):5. doi:10.3390/ctn7010005
9. Marrie RA, Donkers SJ, Jichici D, et al. Models of care in multiple sclerosis: a survey of Canadian health providers. Front Neurol. 2022;13:1–12. doi:10.3389/fneur.2022.904757
10. McGinley MP, Goldschmidt CH, Rae-Grant AD. Diagnosis and treatment of multiple sclerosis: a review. JAMA. 2021;325(8):765–779. doi:10.1001/jama.2020.26858
11. Prod’homme T, Zamvil SS. The evolving mechanisms of action of glatiramer acetate. Cold Spring Harbor Perspect Med. 2019;9(2):1–15. doi:10.1101/cshperspect.a029249
12. McGinley MP, Cohen JA. Sphingosine 1-phosphate receptor modulators in multiple sclerosis and other conditions. Lancet. 2021;398(10306):1184–1194. doi:10.1016/S0140-6736(21)00244-0
13. Khoy K, Mariotte D, Defer G, Petit G, Toutirais O, Le Mauff B. Natalizumab in multiple sclerosis treatment: from biological effects to immune monitoring. Front Immunol. 2020;11:1–7. doi:10.3389/fimmu.2020.549842
14. Péloquin S, Schmierer K, Leist TP, Oh J, Murray S, Lazure P. Challenges in multiple sclerosis care: results from an international mixed-methods study. Mult Scler Relat Disord. 2021;50:1–8. doi:10.1016/j.msard.2021.102854
15. Özge A, Domaç FM, Tekin N, et al. One patient, three providers: a multidisciplinary approach to managing common neuropsychiatric cases. J Clin Med. 2023;12(17):5754. doi:10.3390/jcm12175754
16. Makkawi S, Abulaban A, Al Malik Y, et al. Administration and monitoring burden of high-efficacy disease-modifying therapies for multiple sclerosis: a delphi consensus of clinical experts from Saudi Arabia. Neurol Ther. 2025;14(1):413–427. doi:10.1007/s40120-024-00707-5
17. Kadasah SF, Ishaqui AA, Alshahrani SM. Evaluating healthcare professionals’ knowledge, attitudes, and barriers toward complementary and alternative medicine in managing multiple sclerosis in Saudi Arabia. J Disability Res. 2025;4(3). doi:10.57197/JDR-2025-0010
18. Zhang X, Astivia OLO, Kroc E, Zumbo BD. How to think clearly about the central limit theorem. Psychological Methods. 2023;28(6):1427. doi:10.1037/met0000448
19. Filippi M, Preziosa P, Arnold DL, et al. Present and future of the diagnostic work-up of multiple sclerosis: the imaging perspective. J Neurol. 2023;270(3):1286–1299. doi:10.1007/s00415-022-11488-y
20. Langer-Gould A, Cheng SC, Li BH, Kanter MH. The multiple sclerosis treatment optimization program. Ann Clin Transl Neurol. 2021;8(11):2146–2154. doi:10.1002/acn3.51472
21. Montalban X, Lebrun-Frénay C, Oh J, et al. Diagnosis of multiple sclerosis: 2024 revisions of the McDonald criteria. Lancet Neurol. 2025;24(10):850–865. doi:10.1016/S1474-4422(25)00270-4
22. Rovira À, Auger C. Beyond McDonald: updated perspectives on MRI diagnosis of multiple sclerosis. Expert Rev Neurotherapeutics. 2021;21(8):895–911. doi:10.1080/14737175.2021.1957832
23. Sandroff BM, Richardson EV, Motl RW. The neurologist as an agent of exercise rehabilitation in multiple sclerosis. Exer Sport Sci Rev. 2021;49(4):260–266. doi:10.1249/JES.0000000000000262
24. Solomon AJ, Marrie RA, Viswanathan S, et al. Global barriers to the diagnosis of multiple sclerosis: data from the Multiple Sclerosis International Federation Atlas of MS. Neurology. 2023;101(6):e624–e635. doi:10.1212/WNL.0000000000207481
25. Marin CE, Kfouri PP, Callegaro D, et al. Patients and neurologists have different perceptions of multiple sclerosis symptoms, care and challenges. Mult Scler Relat Disord. 2021;50:1–6. doi:10.1016/j.msard.2021.102806
26. Travers BS, Tsang BK, Barton JL. Multiple sclerosis: diagnosis, disease-modifying therapy and prognosis. Austr J General Pract. 2022;51(4):199–206. doi:10.31128/AJGP-07-21-6103
27. Mohammed Aarif K, Alam A, Pakruddin, Riyazulla Rahman J. Exploring challenges and opportunities for the early detection of multiple sclerosis using deep learning. In: Artificial Intelligence and Autoimmune Diseases: Applications in the Diagnosis, Prognosis, and Therapeutics. Springer; 2024:151–178.
28. Fifield KE, Fudge NJ, Arsenault ST, et al. An overview of multiple sclerosis care in rural and urban Newfoundland and Labrador. In: Canadian Journal of Neurological Sciences. Cambridge University Press; 2025:1–25.
29. Solomon AJ, Kaisey M, Krieger SC, et al. Multiple sclerosis diagnosis: knowledge gaps and opportunities for educational intervention in neurologists in the United States. Mult Scler J. 2022;28(8):1248–1256. doi:10.1177/13524585211048401
30. Heinemann J, Yankov D, Solomon AJ, Rauer S, Wiendl H, Dersch R. McDonald criteria application by German neurologists suggests a need for further training. Mult Scler Relat Disord. 2025;94:1–5. doi:10.1016/j.msard.2025.106304
31. Smith E, Langdon D. A systematic review to explore patients’ MS knowledge and MS risk knowledge. Neurol Sci. 2024;45(9):4185–4195. doi:10.1007/s10072-024-07541-5
32. Farran EK, Waggas DS, Alkhunani TA, Almuwallad SA, Aljohani RA. Assessment of multiple sclerosis awareness and knowledge among the community of Jeddah, Saudi Arabia. J Neurosci Rural Pract. 2021;12(4):733–738. doi:10.1055/s-0041-1734009
33. El-Tantawy NL, Alzahrani SA, Alzahrani RM, Alghamdi RA, Alghamdi AS, Abouhussien RM. Assessment of Multiple Sclerosis Patients’ awareness and knowledge about their illness in KSA: a cross-sectional study. Al-Azhar Int Med J. 2024;5(4):8. doi:10.58675/2682-339X.2352
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
The Epidemiology, Treatment Patterns and Economic Burden of Different Phenotypes of Multiple Sclerosis in Italy: Relapsing-Remitting Multiple Sclerosis and Secondary Progressive Multiple Sclerosis
Perrone V, Veronesi C, Giacomini E, Citraro R, Dell'Orco S, Lena F, Paciello A, Resta AM, Nica M, Ritrovato D, Degli Esposti L
Clinical Epidemiology 2022, 14:1327-1337
Published Date: 6 November 2022