Back to Journals » Risk Management and Healthcare Policy » Volume 18
Physical Exercise, Sports Spectating, and Subjective Life Expectancy in Older Chinese Adults: A Chain Mediation Analysis
Received 3 September 2025
Accepted for publication 7 November 2025
Published 18 November 2025 Volume 2025:18 Pages 3675—3688
DOI https://doi.org/10.2147/RMHP.S565048
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Mecit Can Emre Simsekler
Longyin Chen,1 Jiru Guo,2 Xiya Han3
1Graduate School, Xi’an Physical Education University., Xi’an, People’s Republic of China; 2School of Economics and Management, Shanghai University of Sport., Shanghai, People’s Republic of China; 3Chemistry and Chemical Engineering, Ningxia Normal University., Guyuan, People’s Republic of China
Correspondence: Jiru Guo, Email [email protected]
Background: Participation in sports can influence subjective life expectancy (SLE) among older Chinese adults, yet differences between direct physical exercise and indirect engagement through spectating are not well understood. This study distinguishes the effects of physical exercise and sports spectating—further differentiating online from offline viewing—on older adults’ SLE, and examines the mediating roles of social integration and health status.
Methods: A cross-sectional survey of 693 Chinese adults aged 60 and above was analyzed using mediation models.
Results: Physical exercise was positively associated with SLE both directly (effect = 0.042, 95% CI [0.002, 0.081]) and indirectly through enhanced social integration and improved health (effect = 0.016, 95% CI [0.016, 0.038]). Offline sports viewing also produced indirect benefits via social interaction and health improvement, whereas online spectating influenced SLE mainly through health gains (effect = 0.013, 95% CI [0.004, 0.024]) with minimal impact on social integration (effect = 0.001, 95% CI [– 0.005, 0.006]).
Conclusion: This study demonstrates that direct and indirect forms of sports participation differentially shape older adults’ SLE, with offline engagement offering greater benefits through social pathways. These findings have implications for aging policy, suggesting that interventions promoting physically active and socially interactive sports engagement may support more positive life expectancy perceptions in later life.
Keywords: older adults, physical exercise, subjective life expectancy, chain mediation model, China
Introduction
The global population structure is undergoing profound demographic shifts. According to United Nations projections,1 the global population aged 60 years and above will exceed 2.2 billion by 2050, and this rapid aging trend is expected to pose persistent challenges to economic development, healthcare systems, and social security frameworks. Against this backdrop, subjective life expectancy (SLE)—a key psychological indicator measuring an individual’s perception of their remaining lifespan—has drawn growing attention from both scholars and policymakers. SLE not only reflects older adults’ subjective assessment of the aging process, but is also closely associated with health-related behaviors, resource allocation, and retirement decision-making.2 Moreover, it has demonstrated substantial consistency and reliability in predicting mortality.3,4 Therefore, in-depth research on SLE holds significant academic value and provides important empirical evidence for optimizing retirement, eldercare, and health policies. However, empirical studies in China show that SLE among adults aged 65 and older is generally low.5 Given China’s large elderly population, raising SLE levels could improve national well-being and generate spillover benefits for global aging strategies.
Among various intervention strategies, sports participation is particularly feasible due to its everyday applicability, operational simplicity, and low cost. It has been shown to benefit older adults by improving physical function, enhancing mental health, promoting social integration, and reducing medical expenses. Prior studies have identified a positive link between physical exercise and SLE.6,7 Longitudinal analysis also showed that physical activity was associated with a 30–50% higher likelihood of feeling younger 8 to 20 years later.8 Within the framework of the Health Belief Model, engaging in health-promoting behaviors—such as consistent exercise, moderate alcohol use, and balanced nutrition—strengthens individuals’ perceived control over their life trajectory, thereby lessening the influence of biological and genetic risk factors on SLE.9 Despite this, current research has yet to clearly explain the pathways through which physical exercise improves SLE.9 Many studies rely only on activity volume to define exercise levels, neglecting the significance of sports participation within a broader social context. Against this backdrop, the present study offers three main contributions: (1) distinguishing between direct sports participation (physical exercise) and indirect participation (sports spectating); (2) subdividing spectating into online and offline modes to compare their respective impacts on SLE; and (3) applying a chained mediation model to test the mediating roles of social integration and health status in these relationships.
Physical exercise is widely acknowledged as an economical, sustainable, and effective approach to health promotion. Its benefits are well-documented: regular activity can slow physical decline, lower the risk of chronic diseases, improve mental health, and enhance overall well-being.10–12Poor health status can make individuals feel older than their chronological age and foster negative attitudes toward aging.13,14 A similar effect pathway may be present in sports spectating.15–17 For example, Kawakami et al (2019), in a randomized controlled trial, reported that Japanese seniors who regularly attended professional baseball games experienced reduced depressive symptoms, which in turn improved their SLE.18
Beyond health status, social integration represents a key psychosocial pathway through which sports participation can influence SLE. It refers to the sustained, active, and meaningful involvement of older adults in society, which helps prevent isolation and marginalization arising from physical decline, psychological stress, changes in family roles, occupational loss, and social barriers such as the digital divide and ageism. Activity Theory emphasizes that engaging in social activities is central to healthy aging. Voluntary participation in such activities can mitigate the adverse effects of aging, physical deterioration, and shifts in social status. Within this perspective, physical exercise facilitates the formation of new social networks, strengthens social capital, and promotes broader community participation.19 Comprehensive social integration challenges stereotypes of “uselessness in old age”, enabling older adults to redefine their self-worth and cultivate a more positive outlook on aging.20 Sports spectating may similarly contributes to this process—particularly in-person attendance—which provides opportunities for direct interaction and emotional connection, supports the exchange of information and resources, and fosters a sense of belonging and social recognition.21,22 Ultimately, active social integration not only enriches older adults’ emotional experiences but also fosters more enduring and positive evaluations of SLE.
Drawing upon the preceding research background and theoretical framework, this study conducts a systematic comparison of the effects of physical exercise and sports spectating on the SLE of Chinese older adults. It further differentiates between online and offline spectating modes, and investigates the chained mediating roles of social integration and health status. The theoretical model developed for this study is presented in Figure 1, and the specific hypotheses are outlined as follows:
H1: Physical exercise and sports spectating have a significant positive effect on older adults’ SLE. H2: Both forms of sports participation enhance SLE by promoting social integration. H3: Both forms of sports participation improve SLE by enhancing health status. H4: Social integration and health status jointly mediate the relationship between sports participation and SLE in older adults.
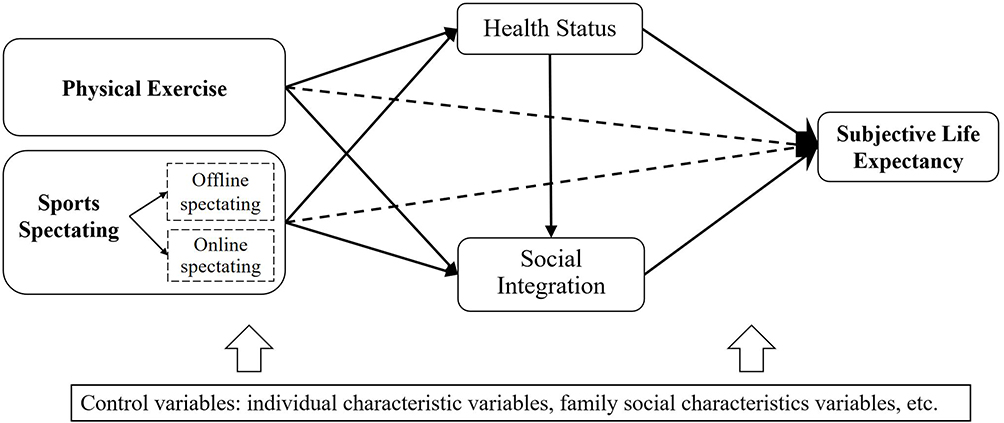 |
Figure 1 Theoretical Model Diagram. Note: “→” indicates directional relationships in the path analysis model, pointing from predictor variables to mediator variables or outcome variables. Solid lines represent indirect effect paths, while dashed lines represent direct effect paths. |
Methodology
Participants
This study focused on individuals aged 60 and above. A convenience sampling approach was used to conduct surveys between April and July 2025 across five Chinese cities: Shanghai, Wuhan, Xuzhou, Xi’an, and Ningxia. The selected locations encompass eastern, central, and western China, providing a degree of regional representativeness. Before the survey commenced, the research team contacted local community leaders to facilitate participant engagement. The purpose and significance of the study were clearly communicated to all prospective participants. Informed consent was obtained prior to data collection, and participants completed either electronic or paper-based questionnaires. A total of 764 questionnaires were distributed. Following the exclusion of cases with patterned responses, unusually short completion times, or incomplete participation, 693 valid questionnaires were obtained, yielding an effective response rate of 90.70%. The city-specific response rates were as follows: 93.75%, 91.61%, 89.33%, 90.00%, 88.59%, and 90.70%, respectively. The inclusion criteria for the participants were: (1) voluntary participation in this survey, (2) aged 60 years and above, (3) being able to read, write, and speak Chinese. The exclusion criteria were: (1) having a serious mental illness; (2) having cognitive disorders or dementia. For missing values in the recovered questionnaires, different treatments were applied depending on the variable type. When key variables—such as SLE scores or sports exercise—were missing, multiple regression imputation was used to estimate the missing data based on statistical relationships among observed variables. If the missing data involved only control variables, mean substitution was applied for continuous variables and mode substitution for categorical variables. These approaches were adopted to minimize sample attrition and preserve statistical power.
Measurement
Dependent Variables
The core explanatory variable in this study is sports participation, which is divided into two categories: physical exercise (direct sports participation) and sports spectating (indirect sports participation). To measure physical exercise, we referred to the China General Social Survey (CGSS) and related literature. Participants were asked: “In the past year, how often have you participated in physical activity during your free time?” Responses were rated on a five-point scale: 0 = Never 1 = Several times a year or less 2 = Several times a month 3 = Several times a week 4 = Every day. A higher score indicates a higher frequency of physical exercise, reflecting greater engagement in direct sports participation.
Sports spectating was measured based on the framework proposed by Mehus (2005)23 and the International Physical Activity Scale (IPAS).24 Specific items used to assess this variable are detailed below: (1) How often do you watch sports competitions via media (eg, television, internet, smartphone, computer, tablet, etc).? Response options: 1 time or less per month 2–3 times per month 1–2 times per week 3–5 times per week About once per day. These were scored on a scale from 1 to 5, respectively. (2) How often do you attend live sports events? Response options mirrored the above and were similarly scored from 1 to 5. (3) How long do you typically spend sports spectating in a single session? Options included:10 minutes or less 11–20 minutes 21–30 minutes 31–59 minutes 60 minutes or more. Each was assigned a value from 1 to 5. To compute the sport event viewing index, the following formula was applied: (Live viewing frequency + Media viewing frequency) × (Viewing duration−1). For example, if a participant reports a media viewing frequency of 1–2 times per week (scored 3 points), a live attendance frequency of 2–3 times per month (scored 2 points), and a viewing duration of 31–59 minutes (scored 4 points), the sports viewing index is calculated as: (3+2) × (4−1) =15. A higher index value indicates more frequent and sustained exposure to sport events.
Dependent Variable
The dependent variable in this study is SLE. It is set according to the item DA029 in the China Health and Retirement Longitudinal Study (CHALRS),25 which asks respondents about the likelihood of living to a specific target age. Specifically, respondents were categorized into nine age groups, including: under 65, 65–69, 70–74, and other successive five-year brackets. Correspondingly, they were asked about their perceived probability of living to the ages of 75, 80, 85, 90, 95, 100, 105, 110, and 115. The study divided “probability” into five categories: “almost impossible”, “unlikely”, “probably”, “very likely”, and “almost certain”, and assigned a value of 1–5. Higher scores indicate a greater subjective expectation of longevity.
Mediating Variables
The mediating variables in this study are social inclusion and health status. The Social Network Index (SNI) in this study is adapted from the Berkman–Syme Social Network Index,26 which originally comprised four dimensions: marital status, religious or spiritual involvement, participation in social organizations, and number of close friends. To ensure cultural relevance within the context of Chinese society, the index was localized by preserving three original components—marital status, organizational participation, and number of friends—while substituting religious involvement with family connections. This modification better captures the central role of familial support within China’s social fabric. Scoring is structured as follows: marital status is assigned 3 points for individuals who are married or in a committed relationship, and 0 points for those who are divorced, widowed, separated, or single. The remaining three components—organizational participation, number of friends, and family connections—are each rated on a 0–3 scale, reflecting the degree of engagement. The cumulative score thus ranges from 0 to 12. To facilitate interpretation, total scores are categorized into five levels: Level I: 0–3 points Level II: 4–5 points Level III: 6–7 points Level IV: 8–9 points Level V: 10–12 points, Higher scores signify a more robust and developed social network.
The variable health status was measured using a widely adopted self-rated health indicator. Participants were asked: “In general, how do you feel about your health?” Responses were recorded on a five-point scale, ranging from 1 (very unhealthy) to 5 (very healthy). This subjective assessment is internationally recognized and frequently used in population health research.27 Self-rated health not only reflects an individual’ s current health status but also serves as a reliable predictor of future health outcomes.
Control Variables and Instrumental Variables
To mitigate potential omitted variable bias, this study incorporates a range of control variables informed by relevant literature. These variables include both individual characteristics—such as gender, age, education level, political affiliation, and employment status—and family and social characteristics, including marital status, total household income, and pension insurance. All of these factors have been shown to influence SLE among older adults and were therefore included in the regression model as covariates.
In addition, to address potential estimation bias arising from reverse causality and other endogeneity concerns, this study introduces two instrumental variables. Specifically, respondents were asked: (1) “What is the condition of fitness places or facilities in your neighborhood?” (2) “How many of your close friends and family members regularly watch sports (eg, soccer, basketball, the Olympics, etc).?” These two items serve as instrumental variables. They are significantly correlated with the endogenous variables—namely, physical exercise and sports spectating—yet they exhibit no direct association with the outcome variable, SLE. Theoretically, both instruments satisfy the essential requirements of relevance (strong correlation with the explanatory variables) and exogeneity (no correlation with the error term in the outcome equation).
Statistical Analysis
Data analysis was conducted using SPSS 26.0. First, descriptive statistics—including frequencies and percentages—were used to summarize the demographic and socioeconomic characteristics of older adults in China. Second, simple linear regression was employed to preliminarily assess the association between physical exercise and sports spectating with SLE. Third, to examine the hypothesized mediation effects, we applied PROCESS v4.1, developed by Hayes,28 within SPSS. An indirect effect was considered statistically significant if its 95% confidence interval (CI) did not include zero. Fourth, we further disaggregated the independent variable sports spectating into online and offline modalities. Their individual associations with SLE were then tested, alongside potential indirect pathways involving social integration and health status. All analyses controlled for a set of covariates: gender, age, marital status, education level, employment status, per capita household income, and so on. The bootstrap sample size was set to 5,000, with a 95% CI, and statistical significance was defined as P < 0.05.
Results
Test for Common Method Bias
To assess potential common method bias, we employed Harman’s one-factor test. The results indicated that the first factor accounted for 29.22% of the total variance, which is well below the critical threshold of 40%.29 This suggests that common method bias is not a serious concern in the present study.
Sample Description
The final sample comprised 693 elderly respondents. The mean score for physical exercise participation was 2.99, while the mean score for sports spectating reached 9.13. Both social integration and health status were reported at moderately high levels, with mean values of 3.08 and 3.09, respectively. The average score for SLE among participants was 3.03.
The mean age of the respondents was 71.03 ± 8.16, and 53.68% were male. Only 7.65% of respondents were members of the Communist Party of China (CPC). Two-thirds of the elderly had a primary education level. Furthermore, 56.13% of the respondents were unemployed, and 73.16% were married or in a relationship. A majority of respondents (63.92%) chose to live with their families. Regarding household income, 48.20% of the respondents reported a monthly income of less than 5,000 yuan. Additionally, 88.17% of the respondents had pension insurance (see Table 1).
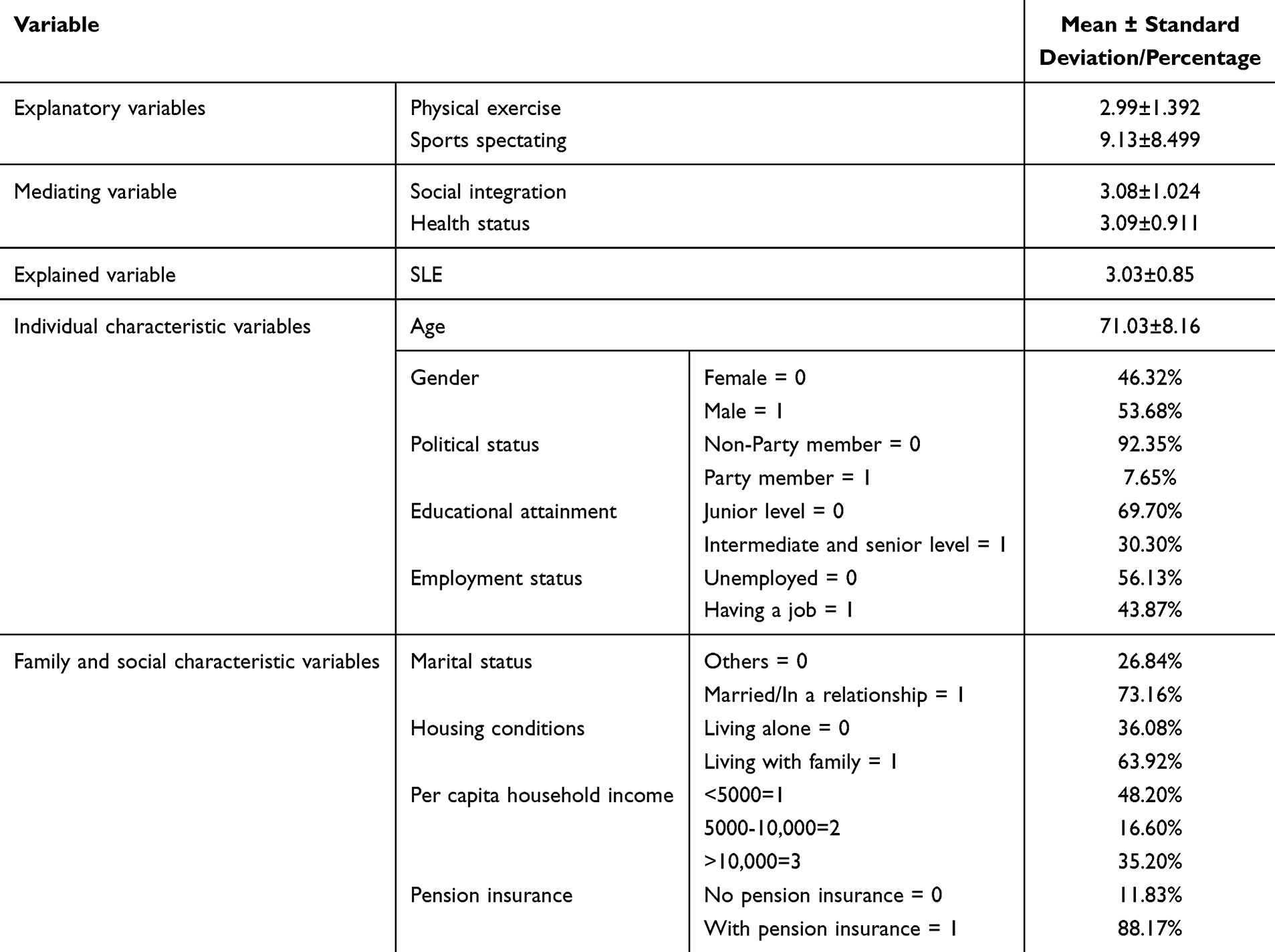 |
Table 1 Descriptive Statistics for Each Variable (N = 693) |
Benchmark Regression Tests
This section presents the regression analysis results of sports participation and older adults’ SLE through hierarchical regression analysis, as shown in Tables 2 and 3. Models 1 and 4 indicate that both physical exercise and sports spectating are positively and significantly related to SLE at the 1% significance level. Specifically, increased participation in sports is associated with higher SLE scores among older adults. For each 1-unit increase in physical exercise or sports spectating, SLE rises by 0.129 and 0.013 units, respectively. The coefficients for the core explanatory variables are 0.122 and 0.118 for physical exercise, and 0.013 and 0.012 for sports spectating. Although the regression coefficient declined, the positive correlation between physical exercise and sports spectating remained statistically significant at the 1% level. This suggests that a robust positive association continues to exist between overall sports participation and the SLE of older adults. Thus, hypothesis H1 is confirmed.
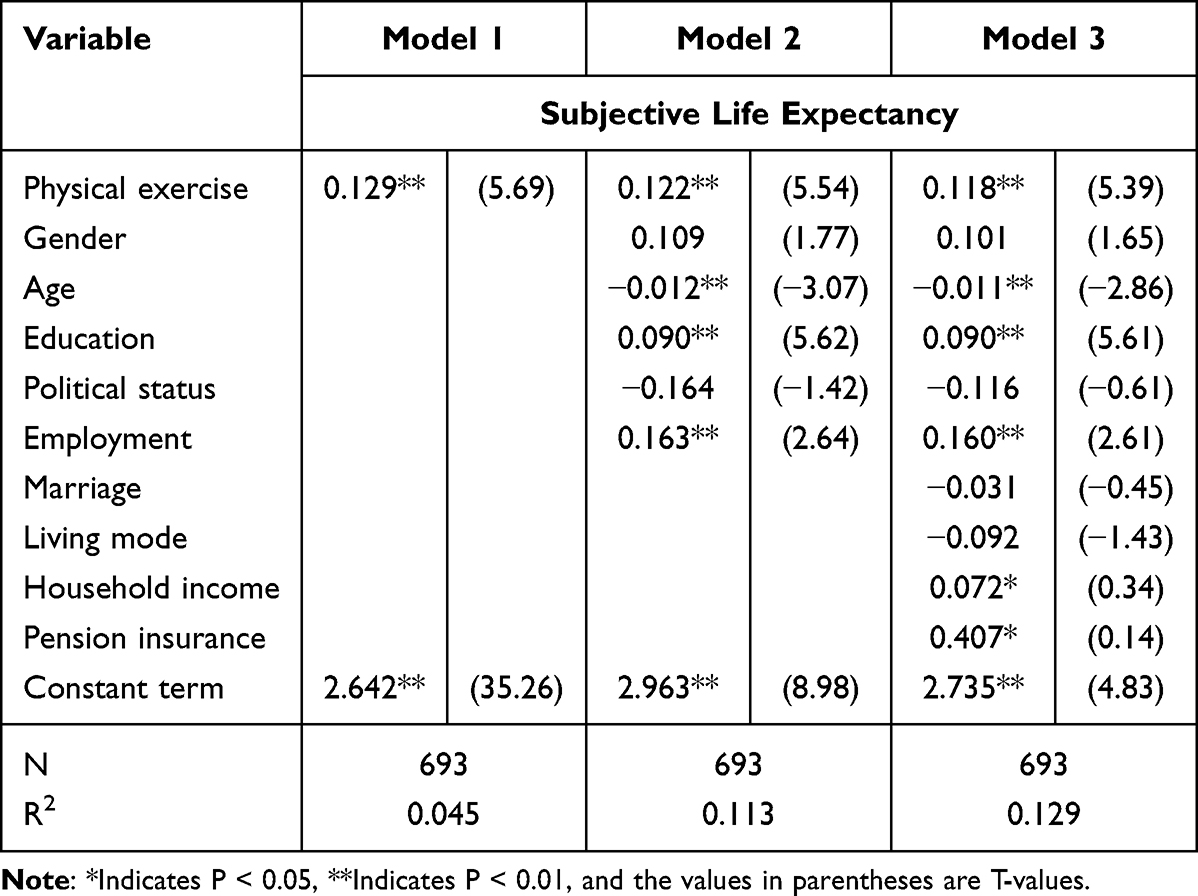 |
Table 2 Benchmark Regression Analysis (Physical Exercise) |
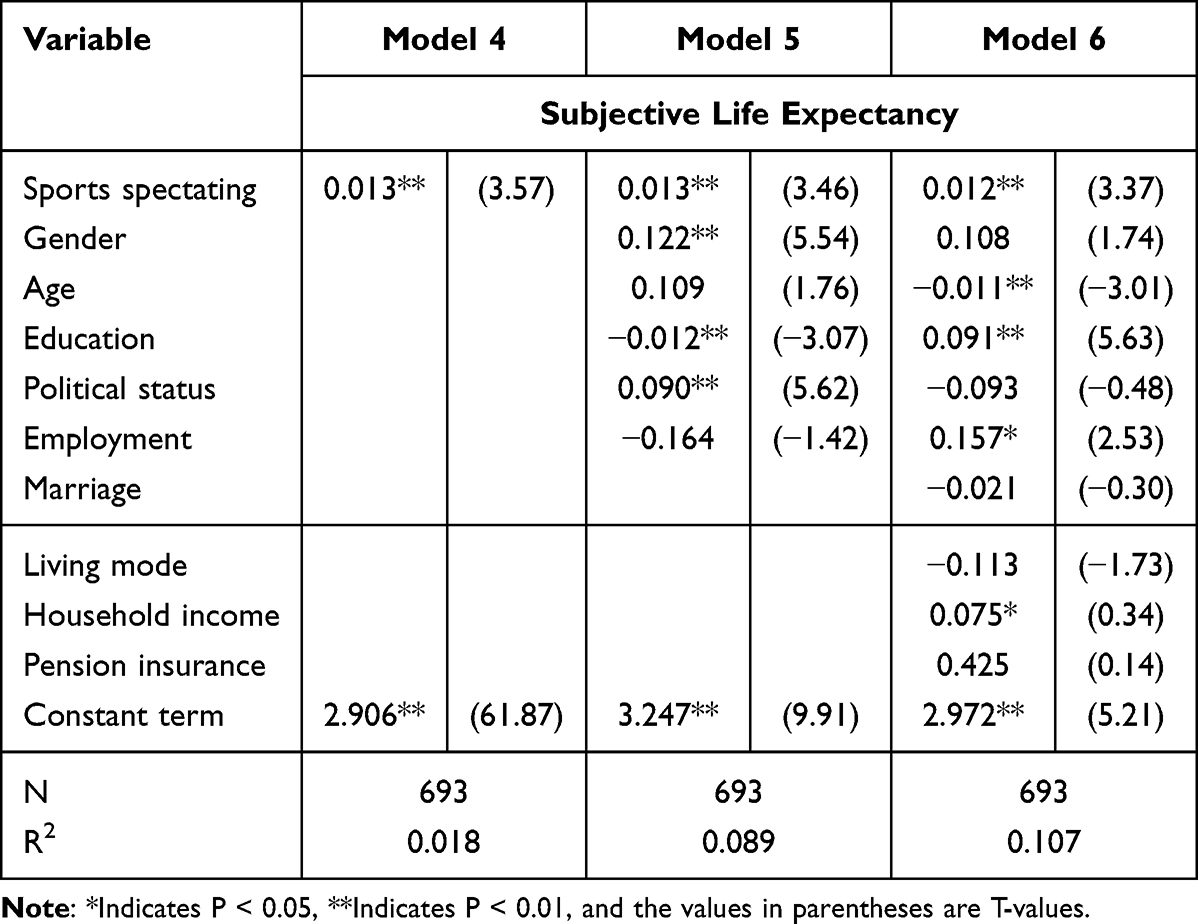 |
Table 3 Benchmark Regression Analysis (Sports Spectating) |
Path Analysis of the Mediation Model
The results of the mediation analysis are presented in Tables 4 and 5. Physical exercise showed significant positive correlations with both social integration (β = 0.172, P < 0.01) and health status (β = 0.089, P < 0.01). Social integration was positively associated with health status (β = 0.355, P < 0.01) and with SLE (β = 0.211, P < 0.01). Health status also demonstrated a significant positive relationship with SLE (β = 0.269, P < 0.01). In contrast, sports spectating does exhibit a modest but statistically significant relationship with both health status (β = 0.019, P < 0.01) and SLE (β = 0.007, P < 0.05). This implies that the influence of sports spectating on SLE may operate primarily through the intermediary of improved health status, rather than through social engagement.
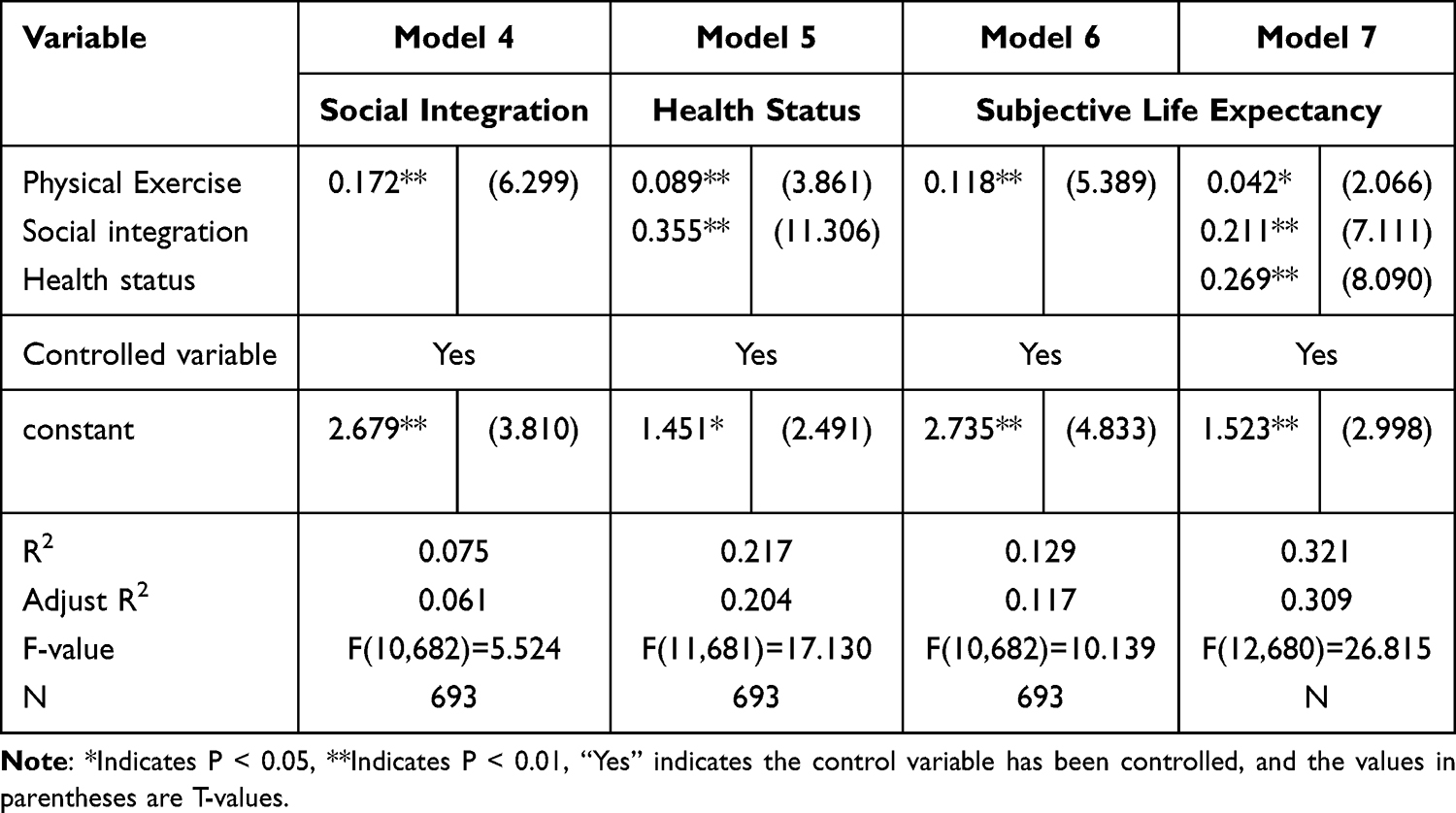 |
Table 4 Mediation Effects Model Test (Sports Spectating) |
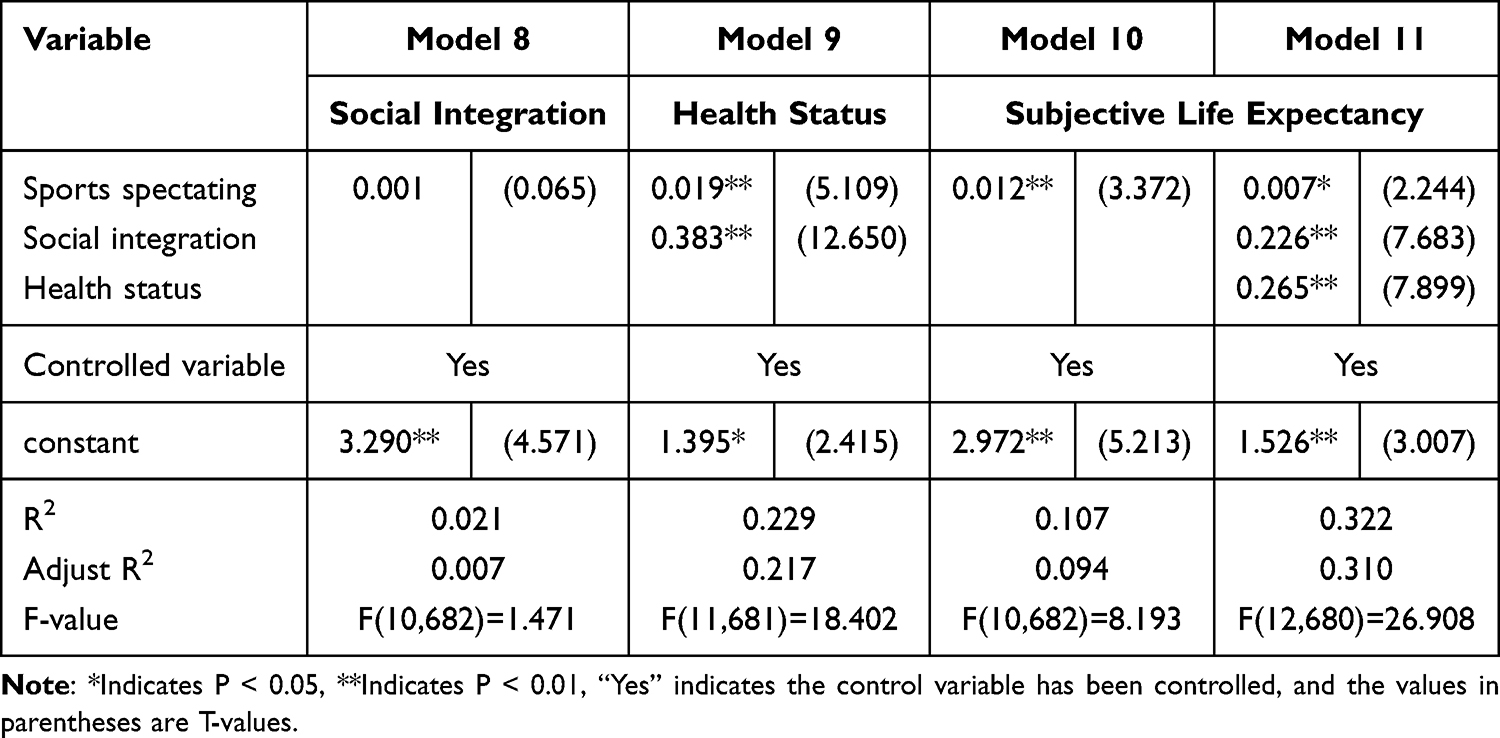 |
Table 5 Mediation Effects Model Test (Physical Exercise) |
The Bootstrap method (with 5,000 repetitions) was employed to further test the significance of the multiple mediating effects in the model. The results are presented in Table 6. For physical exercise, the overall regression equation was significant, with R2 = 0.1311, F (10, 682) = 10.286, and P < 0.01.
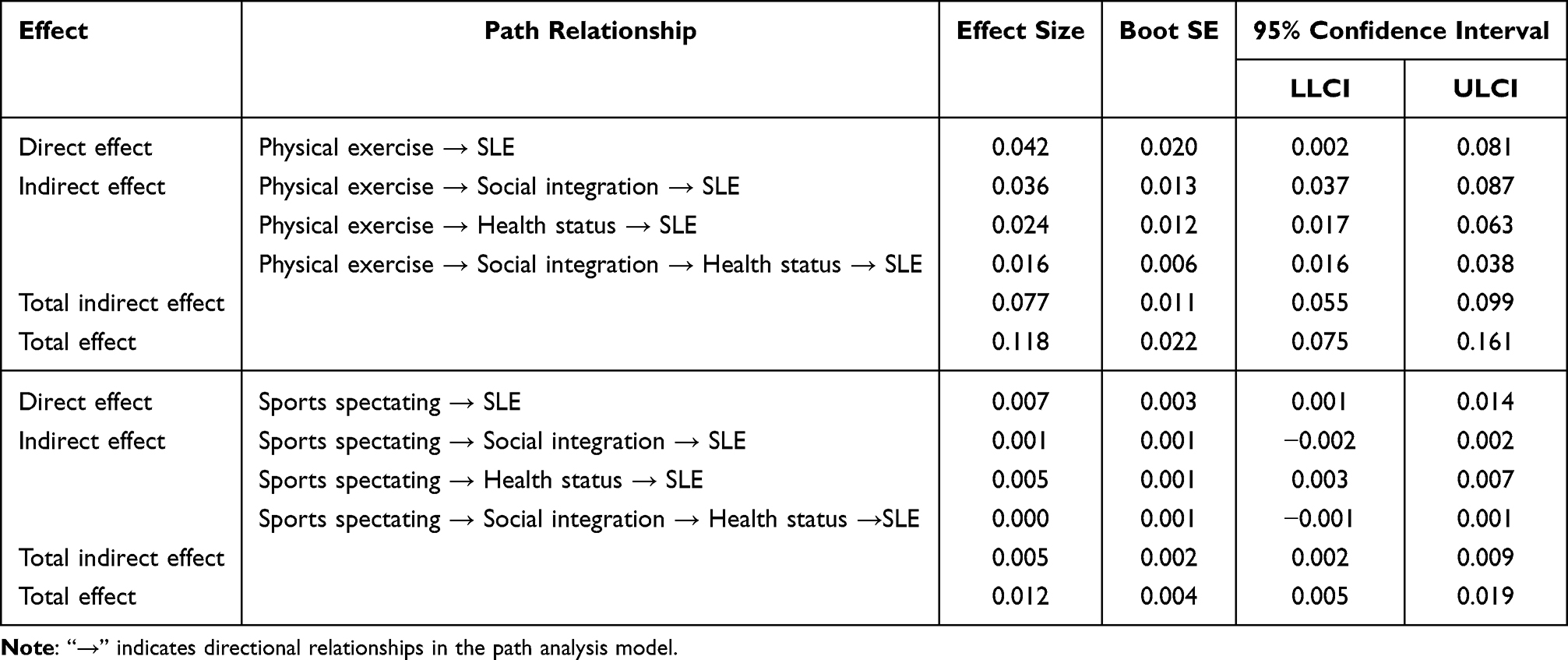 |
Table 6 Bootstrap Analysis of Mediation Effect Significance Test |
The single mediating effect of physical exercise through social integration was 0.036 (95% CI = [0.037, 0.087]). When health status served as the sole mediator, the indirect effect was 0.024 (95% CI = [0.017, 0.063]). The chained mediating effect through both social integration and health status was 0.016 (95% CI = [0.016, 0.038]). The total indirect effect amounted to 0.077 (95% CI = [0.055, 0.099]), and the total effect was 0.118. This means that approximately 65% of the statistical relationship between physical exercise and SLE can be attributed to the combined mediating roles of social integration and health status.
Regarding sports spectating, there exists a significant association between sports spectating and health status in SLE (β=0.005, 95% CI [−0.003, 0.007]). However, the single mediation pathway through social integration (X→M1→Y) and the chain mediation pathway involving both social integration and health status (X→M1→M2→Y) did not achieve significance, with corresponding confidence intervals of [−0.002, 0.002] and [−0.001, 0.001], respectively. These results indicate that, although sports spectating did not indirectly enhance older adults’ SLE by fostering social integration, it did contribute positively to health status. This, in turn, significantly improved their SLE. In other words, the association between sports spectating and SLE is predominantly mediated by health status, whereas social integration does not contribute significantly to this pathway. Regarding the effect size, both the direct effect (0.007) and the total indirect effect (0.005) are minimal, representing less than 1% of the scale range. This indicates that sports spectating has a weak overall relationship with SLE, with its influence arising mainly from a modest mediated link through health status. From a practical perspective, initiatives aimed at promoting sports spectating may need to be integrated with other health-focused interventions to produce more substantial improvements in life expectancy among older adults.
Chain Mediation Model Analysis of Different Forms of Sports Spectating
The previous analysis revealed that H2 and H4 were not fully supported. To examine in greater detail the relationship between sports spectating and SLE among older adults, this study subdivided sports spectating into two categories: online attendance (“offline attendance frequency = 0” ∧ “online attendance frequency > 0”) and offline attendance (“online attendance frequency = 0” ∧ “offline attendance frequency > 0”). The chained mediating effects for each category were analyzed separately, and the results are presented in Table 7.The results presented in Table 7 indicate that the effect of online sports spectating on SLE mirrors the findings for overall sports viewing. Specifically, the correlation between sports spectating and social integration did not reach statistical significance, and the Bootstrap mediation analysis failed to identify a significant chain mediation effect. Regarding effect size, the total effect of online sports spectating was 0.039, representing approximately 0.78% of the possible range (1–5) on the SLE scale. Most of this effect arose from an indirect pathway through health status (indirect effect = 0.013), which accounted for about 33% of the total effect. In contrast, offline sports spectating demonstrated a significant positive correlation with social integration, and both social integration and health status were significantly associated with higher SLE scores (β = 0.022, 95% CI = [0.010, 0.038]). The total effect of offline spectating was 0.096, corresponding to approximately 1.92% of the scale’s range. The total indirect effect reached 0.070, representing about 73% of the total effect. Overall, these findings suggest that offline spectating is linked to greater social participation and improved health status, which together contribute to higher SLE scores among older adults.
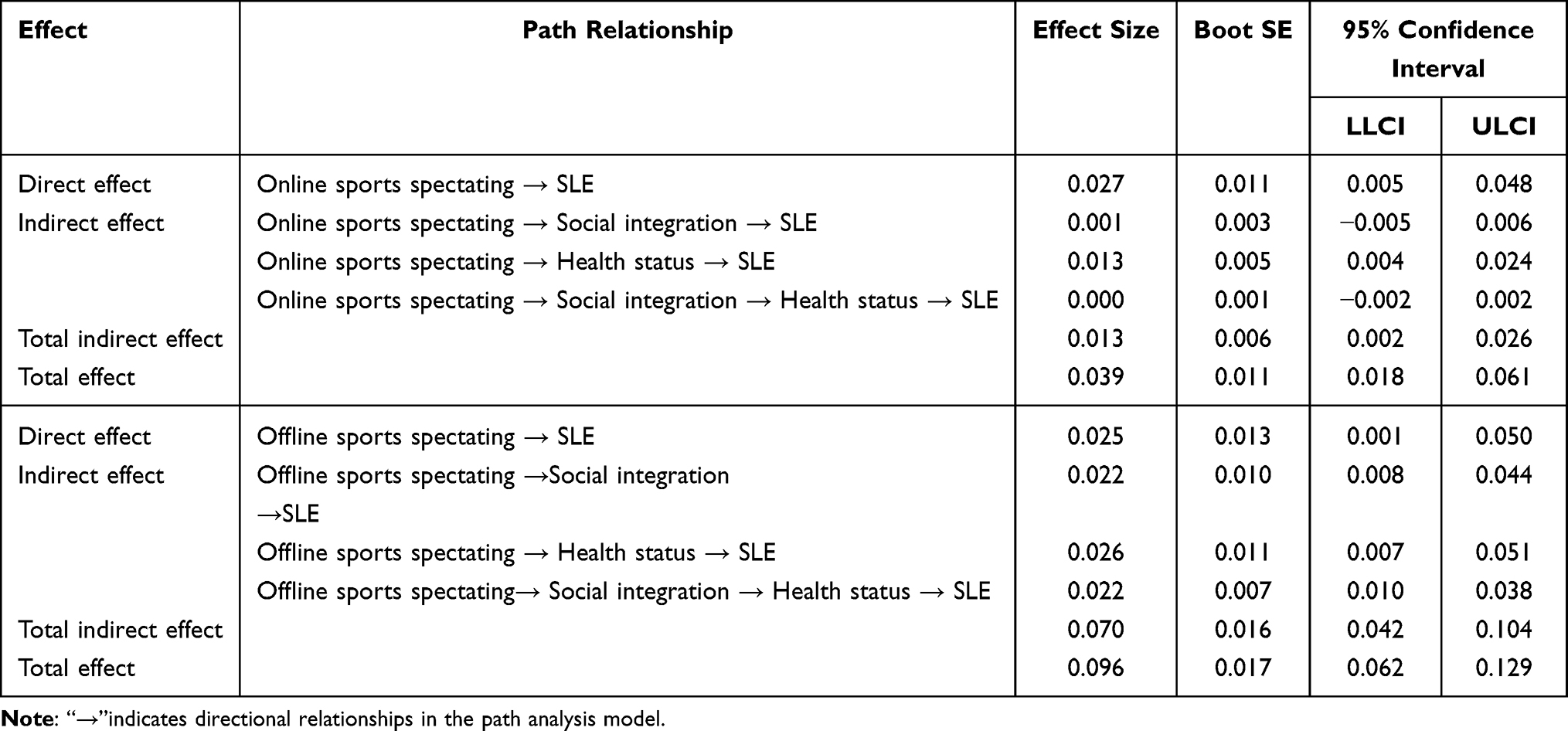 |
Table 7 Results of Chain Mediation Effect Test for Different Forms of Sports Spectating in Predicting SLE |
Robustness Tests
To strengthen the robustness of the findings, this study conducted two robustness tests for the benchmark model. First, the regression model was replaced. Specifically, the OLS model was substituted with an ordered logit model, while maintaining the same procedures as in the benchmark regression. Second, a full model estimation was performed. Both health status and social integration were introduced as control variables in the benchmark model, creating a comprehensive model to examine the effects of physical exercise and sports spectating on the SLE of older adults. The results, presented in Table 8, demonstrate that the regression outcomes remain highly robust, whether through the replacement of the regression model or the full model estimation. These findings further confirm the previous conclusions.
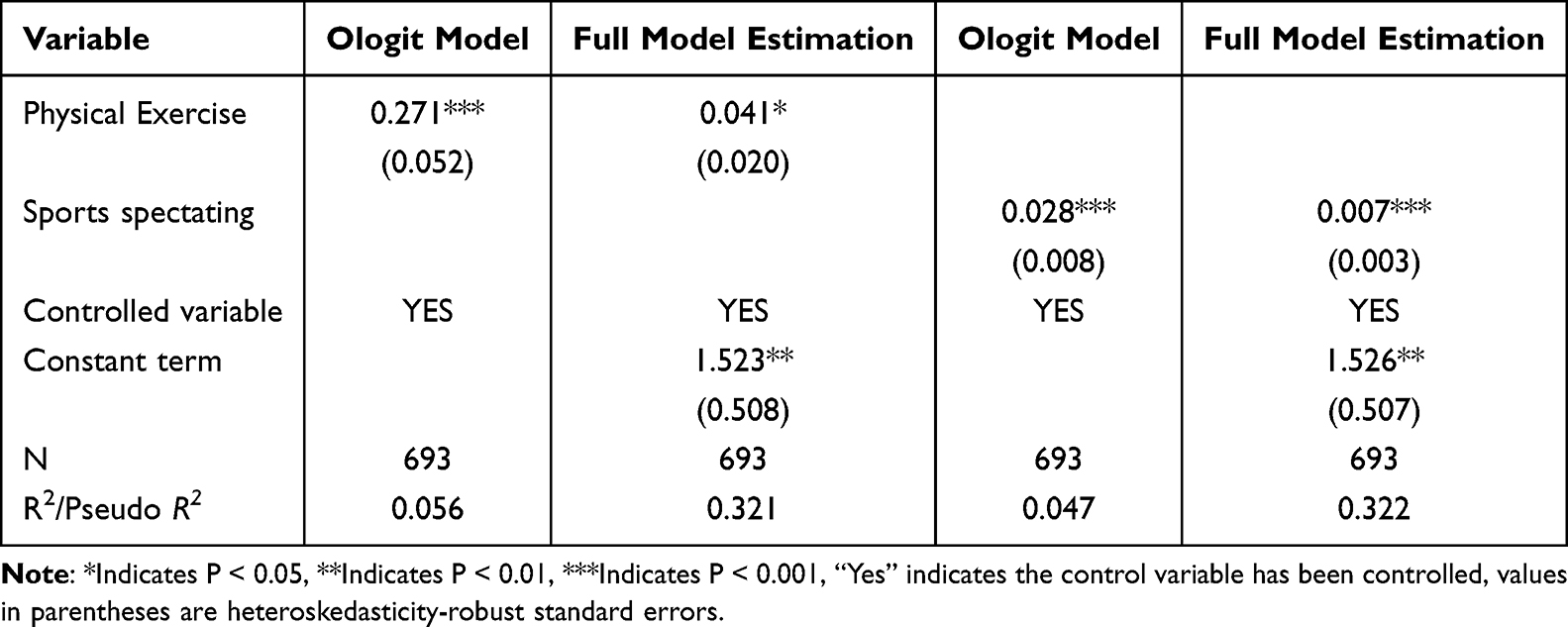 |
Table 8 Robustness Test Results |
Endogenous Problems
Considering the potential reverse causality between older adults’ sports participation and their SLE—ie, individuals with higher SLE may be more likely to engage in physical activity—endogeneity arising from bidirectional causality and omitted variables may bias the estimates. To address this, two instrumental variables were introduced based on prior studies and available survey data: (1) “What is the situation of fitness places or facilities in your community?” and (2) “How many of your friends and family regularly watch sports (eg, soccer, basketball, the Olympics)?” Community fitness facilities affect exercise behavior by reducing time and access costs, satisfying the relevance criterion. To mitigate endogeneity problems in the model as much as possible.30 Since their construction depends on municipal planning rather than personal traits, the exogeneity condition is also met. Likewise, the sports-viewing behavior of friends and relatives influences older adults through social interaction but does not directly affect their health or longevity.
To test for endogeneity, the Durbin and Wu-Hausman tests were applied. For physical exercise, the Durbin test (χ2 = 1.64, P = 0.200) and the Wu-Hausman test (F = 1.64, P = 0.201) yielded results that were not significant enough to reject the null hypothesis of exogeneity, confirming the robustness of the previous results. In contrast, sports spectating showed significant endogeneity (Durbin χ2 = 24.49; Wu-Hausman F = 25.49; P < 0.01), prompting the use of two-stage least squares (2SLS) for further analysis (results in Table 9). The F-statistic for the first stage was 114, well above the threshold of 10, indicating strong instruments with no weak instrument problem. Second-stage regression results confirmed that sports spectating significantly promotes older adults’ attitudes toward SLE, reaffirming the robustness of the main findings.
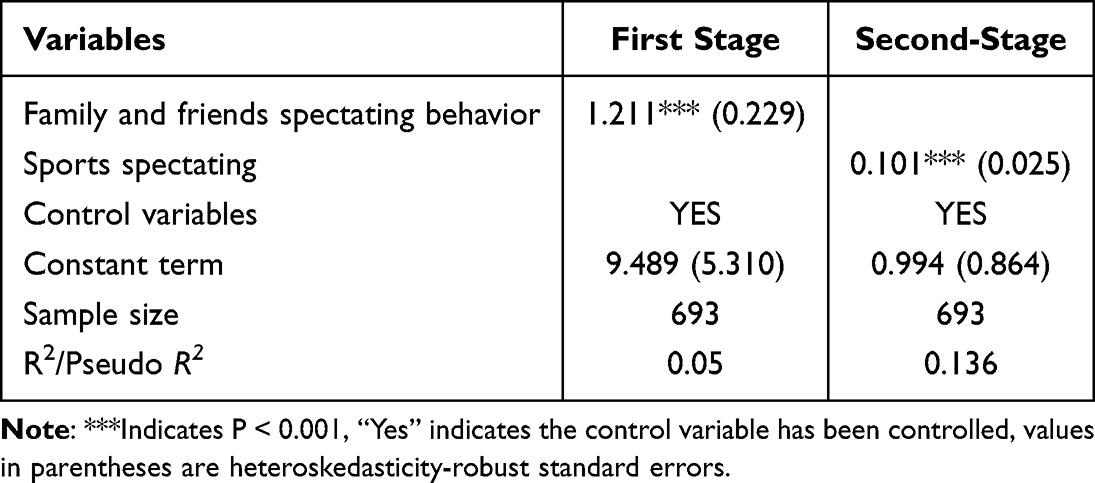 |
Table 9 Regression Results of Instrumental Variable Method |
Discussion
Sports participation, as an active lifestyle choice, has long been acknowledged for its significant impact on older adults’ subjective health and life expectancy. The empirical findings of this study indicate that, while both physical exercise and sports spectating are forms of sports participation, they differ in their effects on SLE.
In terms of physical exercise, as an important lifestyle for healthy aging,31 it has a significant positive predictive effect on the SLE of older adults, this finding echoes previous research. For example, Li et al (2024) contend that regular physical activity not only delays the aging process and lowers the risk of chronic diseases, but also indirectly influences individuals’ perceived life expectancy by improving subjective health perceptions, enhancing life meaning, and fostering more positive expectations for the future.6 Similarly, Griffin et al (2013) proposed a bio-psycho-social model suggesting that physical exercise, as a proactive health behavior, can indirectly shape subjective perceptions of lifespan through improvements in health status and psychological self-regulation.9 Building on previous research, this study demonstrates that sports participation not only directly enhances SLE but also establishes a significant chain-mediated pathway by improving social integration and health status. On one hand, regular physical exercise promotes community engagement, broadens social networks, and strengthens social integration.32 On the other hand, enhanced social integration further improves individual health status, both in terms of better subjective health and more positive perceptions of future life expectancy.33
Compared to physical exercise, sports spectating —a more passive form of sport culture consumption—demonstrates distinct pathways to SLE. The overall analysis indicated no statistically significant association between sports spectating and social integration. This result contrasts with the conclusion of Inoue et al (2017), who argued that “spectating at sporting events is not only an emotional consumption process but also a social interaction arena”.16 Further examination showed that the positive correlation between spectating and SLE is highly audience-specific: it emerges only among live spectators and is absent in online viewing contexts, such as television or internet streaming. This audience-specific effect is consistent with findings from a study on professional baseball, which reported that viewing frequency was positively associated with life satisfaction only in offline settings, with no comparable impact in online environments.34
Possible explanations are as follows. First, online sports spectating is less effective in promoting social integration because it lacks face-to-face interaction. This aligns with Wheatley and Bickerton’s (2017) view that the “social dimension” of cultural and sporting activities is central to enhancing subjective well-being and fostering social support.35 From a theoretical perspective, face-to-face interactions offer a media richness advantage in building social capital and a sense of belonging. Consistent with social capital theory and media richness theory, the multidimensional nature of interactive information—verbal, nonverbal, and contextual cues—facilitates the formation of emotional bonds and trust. Offline spectator events provide such high-richness contexts, enabling participants to forge close social ties within shared physical spaces. In contrast, online spectating functions as a largely one-way flow of information, without immediate feedback or an empathetic atmosphere. Consequently, its capacity to expand social networks and enhance social capital is limited—a constraint that may be especially pronounced among older adults. Second, while online sports spectating offers temporary emotional pleasure and informational satisfaction, live sports viewing provides an opportunity to escape daily life, appreciate athletic aesthetics, and socialize with friends or family, making the experience more immersive.36 Such immersive, shared live experiences are more likely to evoke an “ageless” mindset in older adults. Third, among older adults, socio-demographic factors—such as digital literacy and the extent of social isolation—may intensify the limitations of online sports viewing. For those with strong digital skills, online spectating can partly maintain social connections through interactions on social media.37 In contrast, for individuals with limited digital literacy or inadequate internet access, this pathway is largely obstructed, reducing the potential link between online viewing and social integration. Social isolation further differentiates these effects. Seniors who already experience high levels of isolation may benefit substantially from in-person attendance, which not only allows them to watch the games but also provides a crucial opportunity for face-to-face contact and rebuilding social ties. Conversely, online viewing—lacking the interpersonal extension of offline activities—has little capacity to disrupt entrenched patterns of isolation.
Although this study aims for rigor, it is subject to several methodological and data-related limitations. First, due to its cross-sectional design, the findings reflect only correlations between variables and cannot establish causal pathways. Future research could examine the temporal effects of chained mediation mechanisms by employing longitudinal tracking or experimental interventions. Second, the measures of social integration and health status are based on self-reports, which may introduce subjective bias and common method bias, potentially leading to an overestimation of the associations observed. Incorporating objective health indicators—such as medical examinations, physiological measurements—and behavioral records would help verify the robustness of these results. Third, the analysis does not account for potential sample heterogeneity, including factors such as gender, family structure, urban–rural differences, and variations in educational or cultural backgrounds. Future studies should consider stratified analyses or interaction tests based on these variables to develop a more nuanced explanatory framework.
Conclusions
Using data from Chinese older adults, this study examined how two forms of sports participation—physical exercise and sports spectating—affect SLE and the mechanisms underlying these associations. Physical exercise showed a consistent positive correlation with SLE, operating through a sequential mediation pathway involving social integration and health status. In contrast, sports spectating had a weaker overall effect, driven mainly by health status. Within this category, offline spectating was more strongly linked to both social integration and health status than online spectating. These results underscore the potential role of physical exercise in promoting active aging, demonstrate how participation format and social context shape underlying pathways, and offer empirical insights for health promotion strategies in an aging society.
At both policy and practice levels, governments should integrate physical exercise and suitable in-person sports spectating into healthy aging policy frameworks. By harnessing public funding and optimizing venue allocation, they can reduce barriers to participation and improve accessibility. Community organizations, drawing on their social networks and spatial resources, can regularly host outdoor fitness sessions, group sports activities, and facilitate older adults’ attendance at local sporting events. Such initiatives create opportunities for face-to-face interaction and foster a sense of belonging, thereby strengthening social capital. Healthcare and public health institutions can embed sports participation into chronic disease management and rehabilitation programs. Through tailored health education and personalized guidance, they can raise older adults’ awareness of and capacity for regular exercise and active community engagement. Where necessary, these institutions can coordinate community resources to support chronically isolated or digitally underserved older adults in gaining access to offline participation opportunities. Collaboration across government, community, and healthcare sectors can not only amplify the health benefits of physical exercise but also enhance social integration, leading to a more positive perception of life expectancy. Such integrated efforts can promote physical, mental, and social well-being as part of comprehensive healthy aging strategies. Nevertheless, the applicability of these conclusions may be constrained by cultural and regional contexts. The social functions of sports participation, as well as its influence on life expectancy, can vary according to differences in cultural values, community structures, and levels of social capital. Future studies should assess the robustness of these findings using cross-cultural and multi-regional samples, and design localized health interventions tailored to diverse social environments, thereby improving the global relevance and effectiveness of such policies.
Abbreviation
SEL, subjective life expectancy.
Data Sharing Statement
The datasets used and/or analysed during the current study are available from the corresponding author on reasonable request.
Ethics Approval and Consent to Participate
This research has been performed in accordance with the Declaration of Helsinki and were approved by the Ethics Committee of Xi’an Physical Education University (protocol code 2024031). Written informed consent was obtained from all participants included in the study.
Acknowledgments
We sincerely thank all the older people who participated in this study.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
There is no funding to report.
Disclosure
The authors declare no competing interests.
References
1. World Health Organization. Ageing and Health. 2024. Available from: https://www.who.int/zh/news-room/fact-sheets/detail/ageing-and-health/.
2. Wang XF, Diao H. The impact of social activities on the subjective life expectancy of the elderly. Lanzhou Acad J. 2025;02:195–205.
3. Van Doorn C, Kasl SV. Can parental longevity and self-rated life expectancy predict mortality among older persons? Results from an Australian cohort. J Gerontol B Psychol Sci Soc Sci. 1998;53(1):S28–S34. doi:10.1093/geronb/53B.1.S28
4. Hurd MD, McGarry K. Evaluation of the subjective probabilities of survival in the health and retirement study. J Hum Resour. 1995;30(34):268–292. doi:10.2307/146285
5. Wang JW. The subjective life expectancy of the Chinese middle-aged and older adults and its socio-economic disparity. Population Econom. 2021;04:51–66.
6. Li Z, Zhang Y, Wu M, Yang J. Is subjective life expectancy stronger in older adults with more physical activity? Evidence from China. Geriatric Nurs. 2024;59:646–652. doi:10.1016/j.gerinurse.2024.08.035
7. Zaccardi F, Rowlands AV, Dempsey PC, et al. Interplay between physical activity volume and intensity with modeled life expectancy in women and men: a prospective cohort analysis. J Sport Health Sci. 2025;14:100970. doi:10.1016/j.jshs.2024.100970
8. Stephan Y, Sutin AR, Terracciano A. Physical activity and subjective age across adulthood in four samples. Eur J Ageing. 2020;17(4):469–476. doi:10.1007/s10433-019-00537-7
9. Griffin B, Loh V, Hesketh B. A mental model of factors associated with subjective life expectancy. Soc Sci Med. 2013;82:79–86. doi:10.1016/j.socscimed.2013.01.026
10. Gómez-Redondo P, Valenzuela PL, Martínez-de-Quel Ó, et al. The role of supervision and motivation during exercise on physical and mental health in older adults: a study protocol for a randomized controlled trial (PRO-Training project). BMC. Geriatrics. 2024;24(1):274. doi:10.1186/s12877-024-04868-8
11. Wang H, Liu YY, Pei Z, Liang JF, Ding XS. The influence of Tai Chi exercise on the subjective well-being in the aged: the mediating role of physical fitness and cognitive function. BMC Geriatr. 2023;23(1):636. doi:10.1186/s12877-023-04366-3
12. Oduro JK, Oduro MA. Well-being: pathway to life satisfaction among older persons in Ghana. BMC Geriatr. 2025;25(1):1–12. doi:10.1186/s12877-025-06036-y
13. Demakakos P, Gjonca E, Nazroo J. Age identity, age perceptions, and health: evidence from the English longitudinal study of aging. Ann New York Acad Sci. 2007;1114(1):279–287. doi:10.1196/annals.1396.021
14. Ron P. Elderly people’s attitudes and perceptions of aging and old age: the role of cognitive dissonance? Int J Geriatric Psychiatry. 2007;22(7):656–662. doi:10.1002/gps.1726
15. Jang W, Ko YJ, Wann DL, Kim D. Does spectatorship increase happiness? The energy perspective. J Sport Manage. 2017;31(4):333–344. doi:10.1123/jsm.2016-0113
16. Inoue Y, Sato M, Filo K, Du J, Funk DC. Sport spectatorship and life satisfaction: a multicountry investigation. J Sport Manage. 2017;31(4):419–432. doi:10.1123/jsm.2016-0295
17. Jang W, Wann DL, Ko YJ. Influence of team identification, game outcome, and game process on sport consumers’ happiness. Sport Manage Rev. 2018;21(1):63–71. doi:10.1016/j.smr.2017.03.002
18. Kawakami R, Sawada SS, Ito T, et al. Effect of watching professional baseball at a stadium on health‐related outcomes among Japanese older adults: a randomized controlled trial. Geriatrics Gerontol Int. 2019;19(8):717–722. doi:10.1111/ggi.13687
19. Yang F, Huang YJ, Wang FBH. Physical exercises of Chinese older adults and social participation: health promotion and network expansion. Population Res. 2021;45(03):97–113.
20. Guo K, Huang Q. Where does the spirit of “refusing to age” come from? Exploring the pathways of physical exercise’s impact on aging identity among Chinese elderly. J Sports Res. 2025;06:1–23.
21. Zhong HM, Xu WX. Research on subjective well-being effects of physical exercise participation:—An empirical analysis based on China family panel studies survey data. J Xi’an Phys Educ Univ. 2024;41(1):62–75.
22. Zhang XL. Collective effervescence: generation mechanism and empirical test of how watching sports events enhances Chinese residents’ happiness. J Wuhan Sports Univ. 2025;59(05):19–26.
23. Mehus I. Distinction through sport consumption: spectators of soc-cer, basketball, and ski-jumping. Int Rev Sociol Sport. 2005;40(3):321–333. doi:10.1177/1012690205060159
24. Craig CL, Marshall AL, Sjöström M, et al. International physical activity questionnaire: 12-country reliability and validity. Med Sci Sports Exercise. 2003;35(8):1381–1395. doi:10.1249/01.MSS.0000078924.61453.FB
25. Zhao Y, Hu Y, Smith JP, Strauss J, Yang G. Cohort profile: the China health and retirement longitudinal study (CHARLS). Int J Epidemiol. 2014;43(1):61–68. doi:10.1093/ije/dys203
26. Berkman L, Breslow L. Health and ways of living: the Alameda County Study. Ann Internal Med. 1985;102(1):146.
27. Bowling A. Measuring health: a review of subjective health, well-being and quality of life measurement scales; 2017.
28. Hayes AF. Introduction to Mediation, Moderation, and Conditional Process Analysis: A Regression-Based Approach. Guilford publications; 2017.
29. Podsakoff PM, MacKenzie SB, Lee JY, Podsakoff NP. Common method biases in behavioral research: a critical review of the literature and recommended remedies. J Appl Psychol. 2003;88(5):879–903. doi:10.1037/0021-9010.88.5.879
30. Bian YJ, Zhang YX, Lu XL. Theory-oriented quantitative research in the sociology of sport: problems, solutions, and prospects. J Shanghai Univ Sport. 2024;48(1):1–13.
31. Ojijieme NG, Feng T, Chui CM, Qi X, Liu Y. Physical activity dynamically moderates the impact of multimorbidity on the trajectory of healthy aging over sixteen years. BMC Geriatr. 2024;24(1):565. doi:10.1186/s12877-024-05067-1
32. Downward P, Dawson P, Mills TC. Sports participation as an investment in (subjective) health: a time series analysis of the life course. J Public Health. 2016;38(4):e504–e510. doi:10.1093/pubmed/fdv164
33. Blake HT, Buckley JD, Stenner BJ, O’Connor EJ, Burgess SA, Crozier AJ. Sport participation and subjective outcomes of health in middle-aged men: a scoping review. Am J Men’s Health. 2022;16(2):15579883221084493. doi:10.1177/15579883221084493
34. Watanabe Y, Qian TY, Wang JJ, Pifer ND, Zhang JJ. Sport spectatorship and health benefits: a case of a Japanese professional golf tournament. Front Psychol. 2020;11:1494. doi:10.3389/fpsyg.2020.01494
35. Wheatley D, Bickerton C. Subjective well-being and engagement in arts, culture and sport. J Cultural Econ. 2017;41:23–45. doi:10.1007/s10824-016-9270-0
36. Kawaguchi K, Ide K, Kanamori S, Tsuji T, Kondo K. Watching sports and happiness among older adults in Japan: the JAGES cohort study. PLoS One. 2025;20(4):e0320213. doi:10.1371/journal.pone.0320213
37. Liu L, Wu F, Tong H, Hao C, Xie T. The digital divide and active aging in China. Int J Environ Res Public Health. 2021;18(23):12675. doi:10.3390/ijerph182312675
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Development and Validation of Nomogram to Predict Frailty for Older Patients Undergoing Abdominal Surgery
Zhang H, Xiao Y, Jin H, Wang X, Wang J
Clinical Interventions in Aging 2025, 20:2423-2435
Published Date: 6 December 2025
Factors Influencing Physical Activity Participation Among Older Adults: A Social Ecological Analysis of Sports-Medical Integration
Chen Y, Bin Abdullah MF, Li F, Zainal Abidin NE, Sha S, Wang H, Yang C
Journal of Multidisciplinary Healthcare 2026, 19:600190
Published Date: 15 May 2026