Back to Journals » Clinical Interventions in Aging » Volume 20
Development and Validation of Nomogram to Predict Frailty for Older Patients Undergoing Abdominal Surgery
Authors Zhang H, Xiao Y ![]() , Jin H, Wang X
, Jin H, Wang X ![]() , Wang J
, Wang J
Received 9 June 2025
Accepted for publication 1 December 2025
Published 6 December 2025 Volume 2025:20 Pages 2423—2435
DOI https://doi.org/10.2147/CIA.S545803
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Nandu Goswami
Honghui Zhang,1,2 Yuting Xiao,2 Huimin Jin,3 Xiaohui Wang,2 Jing Wang1
1Faculty of Nursing, Health Science Center, Xi’an Jiaotong University, Xi’an, Shaanxi, 710061, People’s Republic of China; 2Department of Hepatobiliary Diseases, Hunan Provincial People’s Hospital, The First-Affiliated Hospital of Hunan Normal University, Changsha, Hunan, 410005, People’s Republic of China; 3Department of General Surgery, The Second Xiangya Hospital, Central South University, Changsha, Hunan, 410000, People’s Republic of China
Correspondence: Jing Wang, Faculty of Nursing, Health Science Center, Xi’an Jiaotong University, 76 Yanta West Road, Xi’an, Shaanxi, 710061, People’s Republic of China, Tel +86 187 8940 0330, Email [email protected]
Background: Frailty is a critical geriatric syndrome associated with adverse surgical outcomes, yet preoperative risk prediction models for older adults undergoing abdominal surgery remain underdeveloped. This study aimed to identify frailty risk factors and establish a predictive nomogram in this population.
Methods: We enrolled 790 older patients undergoing abdominal surgery at Hunan Provincial People’s Hospital from February 2022 to September 2022. Frailty was assessed using the Tilburg Frailty Index. Univariate analysis, LASSO regression and multivariate analysis were used in turn to identify independent risk factors for frailty. The nomogram was developed based on the independent risk factors. The sample was randomly divided into a test group (75%) and a validation group (25%). The area under the curve (AUC) of the receiver operating characteristic (ROC) was calculated to assess the predictive performance of the nomogram.
Results: The prevalence of frailty among older patients undergoing abdominal surgery was 74.18%. Eight independent risk factors were identified: advanced age (OR=1.32), lower BMI (OR=1.28), limited education (OR=1.45), laparoscopy (OR=1.67), tumor comorbidity (OR=2.01), diabetes (OR=1.89), antihyperlipidemic drug use (OR=1.53), and elevated interleukin-6 (OR=1.76). The nomogram demonstrated acceptable discrimination, with AUCs of 0.748 (the test group) and 0.707 (the validation group).
Conclusion: Our findings demonstrate a nomogram to predict the probability of frailty for older patients undergoing abdominal with acceptable predictive performance. The nomogram is helpful in guiding further targeted and effective intervention and prevention efforts to decrease frailty and improve health outcomes.
Keywords: frailty assessment, risk assessment tool, older adults, abdominal surgery, China
Introduction
Frailty, an age-associated syndrome, is characterized by a multisystem (involving neurological, metabolic-endocrine, and immune systems) impairment of homeostasis, primarily manifesting as sarcopenia in older adults. This condition leads to reduced physiological reserve, diminished stress resilience, and a nonspecific vulnerability state, representing one of the most clinically significant geriatric syndromes. The prevalence of frailty is notably high among older populations. A global systematic review and meta-analysis1 reported a frailty prevalence of 13.60% in community-dwelling adults aged ≥60 years. In China, frailty affects 10.00% of community-dwelling adults aged ≥60 years.2–4 A study by Wei et al5 involving 279 hospitalized older patients in Shanghai tertiary hospitals (surgical, medical, and geriatric departments) revealed a frailty prevalence of 34.30%. These findings highlight that hospitalized older adults exhibit higher frailty rates than their community counterparts, underscoring the need for heightened clinical attention to frailty in hospitalized older adults.
Frailty arises from the cumulative decline of physiological and psychological functions, exacerbating vulnerability and impairing stress response. Minor stressors (eg, wound infections, falls, or minor surgeries) may trigger disproportionate health deterioration. Surgical interventions, inherently traumatic and stress-inducing,6 further amplify this risk. Research7 indicates that older surgical patients face elevated frailty risks, with prevalence reaching 30.00–50.00% in major surgeries. Frailty independently predicts postoperative complications and mortality, demonstrating high sensitivity and specificity, beyond age and the American Society of Anesthesiologists (ASA) physical status classification. Notably, abdominal surgeries—owing to the anatomical complexity of hepatobiliary and gastrointestinal systems, diverse pathophysiology, and significant surgical trauma—are associated with higher postoperative frailty rates (36.50%) compared to other procedures.8,9
Preoperative frailty prediction is thus critical for older patients undergoing abdominal surgery. Clinicians can leverage frailty screening to identify high-risk individuals, implement targeted interventions to mitigate or reverse frailty progression, and reduce adverse outcomes through primary, secondary, and tertiary prevention strategies. Establishing preoperative frailty risk models enables tailored interventions to improve clinical outcomes. However, no validated clinical models currently exist for predicting frailty in older abdominal surgery patients. This study aims to identify preoperative frailty risk factors and construct a predictive risk assessment nomogram, providing a scientific foundation for standardized frailty management protocols to optimize care for this vulnerable population.
Methods
Study Design, Participants, and Procedure
We have investigated 790 older patients with abdominal surgery at Hunan Provincial People’s Hospital from February 2022 to September 2022. A convenience sampling method was employed to recruit eligible patients who satisfied the following inclusion criteria: (1) age ≥ 60 years; (2) undergoing abdominal surgery; (3) in stable disease condition; (4) with sufficient literacy to understand and complete the survey. Following patients were excluded: (1) severe and irreversible diseases of vital organs, such as the heart, kidneys, and gastrointestinal systems, leading to complete dependency in daily activities; (2) Alzheimer’s disease or other types of dementia; (3) other severe physical or mental illness leading to inability to complete the survey.
The sample size was calculated according to the calculation method of modeling sample size.10 The risk assessment model includes a total of 26 risk factors, each requiring 5 to 10 participants. The incidence of frailty in older patients undergoing abdominal surgery was reported as 36.5% based on previous literature. Considering an attrition rate of 15%, the sample size required for this study was calculated as 820 cases (26 × 10 × (1 + 15%) ÷ 36.5%). Therefore, a total of 820 participants were recruited for the study, 790 valid responses were obtained, yielding an impressive response rate of 96.3%. Finally, 790 responses were included and randomly distributed to a testing group (n = 592) for modeling fitting and a validation group (n = 198) for model validation with the ratio 3:1.
The study was approved by the Ethics Committee of Hunan Provincial People’s Hospital (No.: [2022]-13) and was carried out in accordance with the guidelines outlined in the Declaration of Helsinki. All participants provided written informed consent before participating in the study. Eligible participants were approached and recruited by the ward nurses, who explained the study’s purpose and procedures to the patients. Patients who were interested in participating in the survey were then referred to our research team, who received standard and uniform training on research conduct and data collection. All participants were fully informed about the study and assured that their participation was entirely voluntary, with the understanding that refusal or withdrawal from the study would not affect their hospital treatment. After providing written informed consent, participants were invited to complete a series of questionnaires based on face-to-face interviews conducted by the research team to collect basic information and assess their frailty and other health statuses. In addition, data on participants’ demographic characteristics and laboratory-related clinical indicators were collected through the hospital’s electronic medical record system.
Measurement
Patients’ socio-demographic and clinical characteristics were collected through a researcher-designed questionnaire, and their laboratory-related indicators were retrieved from the electronic medical record system. Standard scales were used to assess frailty, psychological distress, cognitive impairment, and disability.
A researcher-designed questionnaire was used to collect participants’ basic information, including gender, age, education level, marital status, surgical method, BMI, comorbidities, polypharmacy, etc. In addition, laboratory-related indicators were collected through the electronic medical record system, which included hemoglobin, albumin, and inflammatory factors such as IL-6, procalcitonin, white blood cells, and TNF-ɑ.
Frailty was assessed using the Tilburg Frailty Index (TFI), a self-report standardized questionnaire developed by Gobbens.11 The TFI comprises three domains: physical frailty (8 items), psychological frailty (4 items), and social frailty (3 items), totaling 15 items. Items 9–11 and 14 employ a three-category response format (“Yes”, “Sometimes”, “No”), which were subsequently dichotomized according to standardized conversion criteria. Items 1, 12, and 15 are reverse-scored. The total score ranges from 0 to 15, with scores ≥5 indicating frailty status, where higher scores reflect greater severity of frailty. The scale demonstrates excellent psychometric properties, with a Cronbach’s α coefficient of 0.880, confirming strong reliability and validity.
Psychological distress was assessed using the self-administered Hospital Anxiety and Depression Scale (HADS) compiled by Snaith and Zigmond.12 It is a 14-item scale under two subscales: anxiety (7 items) and depression (7 items). Each item is rated on a four-point Likert scale ranging from 0 to 3. The total score for each subscale ranges from 0 to 21, with a score >8 indicating the presence of anxiety or depression. The HADS showed good internal consistency with a Cronbach’s α coefficient of 0.879.
Cognitive impairment was assessed using the Mini-Mental State Examination (MMSE) developed by Folstein et al.13 It is the most widely used and well-known short screening tool for measuring cognitive impairment in clinical, research, and community settings. The MMSE includes 11 items covering time orientation, place orientation, immediate memory, attention and calculation, recall, naming, retelling, 3-level instruction, reading, writing, and tracing. The total score ranges from 0 to 30 points, with a score of 28 to 30 indicating normal cognitive function, and a score below 27 indicating cognitive impairment. The MMSE showed good internal consistency in the current study, with a Cronbach’s coefficient of 0.833.
Disability was assessed using the Barthel activities of daily living (ADL) index, a widely used standardized scale in clinical, research, and community settings.14 The Barthel ADL index comprises ten items: feeding, grooming, bathing, dressing, bowel and bladder care, toileting, ambulation, transfers, and stair climbing. The total score ranges from 0 to 100 points, with a higher score indicating lower dependency and higher ADL abilities. Based on the total score, participants are divided into the following four groups: severe dependence (≤40 points), moderate dependence (41~60 points), mild dependence (61~99 points), and no dependence (100 points). Since most participants had no dependence, participants with mild to severe dependence were combined into the disability group. ADL demonstrated good internal consistency in the current study with a Cronbach’s α coefficient of 0.929.
Statistical Analysis
The data distribution of continuous variables was assessed using the Shapiro–Wilk test and presented as means ± standard deviations for normally distributed data or medians and interquartile ranges (IQRs) for data with non-normal distributions. Categorical variables were presented as numbers and percentages. Univariate logistic regression analysis, LASSO regression analysis and multivariate logistic regression analysis were used to identified the independent risk factors for frailty. The nomogram to predict the probability of frailty was developed based on the risk factors in multivariate logistic regression analysis and performed by the “rms” R package. The “ROC package” was employed to draw the Receiver Operating Characteristic curve (ROC) and calculate the area under the curve (AUC) to evaluate the predicting ability of the nomogram, with an AUC of ≥0.8 indicating good predicting performance.15 All statistical analyses were performed using R version 4.2.2.
Results
Patients Demographics and Characteristics
Of the 820 older patients undergoing abdominal surgery approached for participation, 790 (96.3%) completed the survey and were included in this study. The average age of the participants was 68.77 (standard deviation [SD], 5.78) years, with a balanced gender distribution (397 males, 50.25%). Most participants were married (721, 91.27%) and had attained primary school education or below (343, 43.42%), while 83 patients (10.51%) reported college-level education or higher. The average body mass index (BMI) was 22.44 kg/m2 (SD, 3.31).
Gallstone/cholecystitis constituted the predominant diagnosis (333, 42.15%), followed by intrahepatic bile duct stones (95, 12.03%), colorectal cancer (80, 10.13%), and pancreatic cancer (45, 5.70%). Minimally invasive approaches were favored, with laparoscopy being the most common surgical intervention (561, 71.01%), followed by cholecystectomy (373, 47.22%) and liver resection (165, 20.89%). Hypertension emerged as the most prevalent comorbidity (320, 40.51%), followed by diabetes (153, 19.37%) and coronary heart disease (97, 12.28%). Pharmacological management included antihypertensive drugs (167, 21.14%), antihyperglycemic agents (97, 12.28%), Antihyperlipidemic drugs (59, 7.47%) and so on. Psychological distress was reported in 9.87% (depression, n=78) and 11.27% (anxiety, n=89) of participants, while cognitive impairment and disability each affected 36 patients (4.56%). Laboratory indicators such as interleukin-6, procalcitonin and other details were described in Table 1.
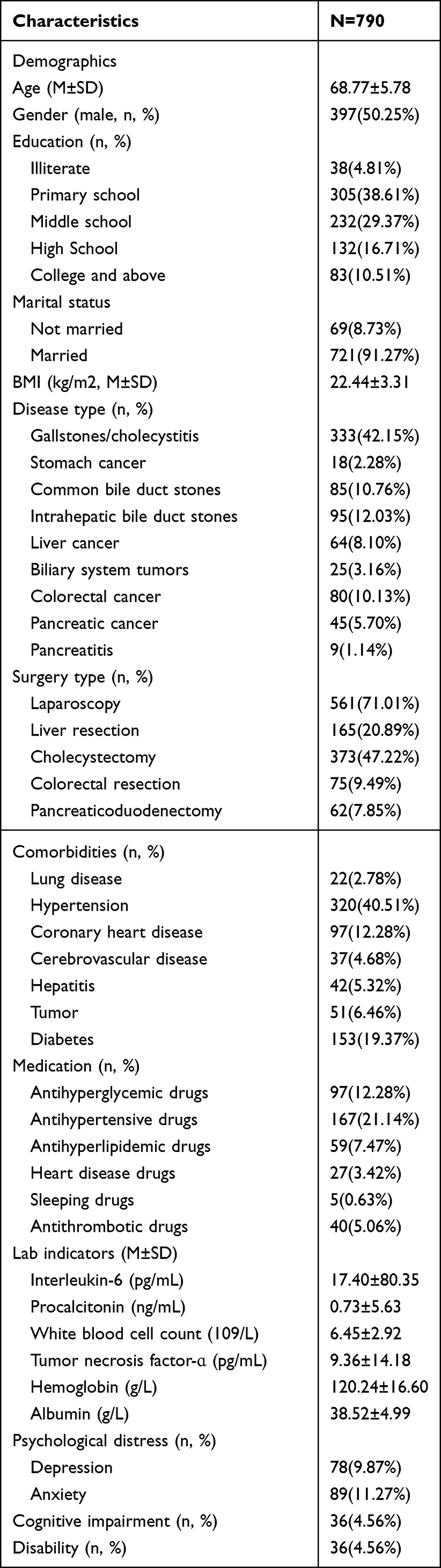 |
Table 1 Patient Demographics and Characteristics |
Independent Factors for Frailty
Of all patients, 586 (74.18%) patients were assessed as frailty. First, we performed univariate analysis and found that age, education, marital status, BMI, disease type, surgery type, tumor, diabetes, antithrombotic drugs, interleukin-6, hemoglobin, albumin, depression, anxiety, cognitive impairment, and disability were associated with frailty (Table 2). All risk factors identified in the univariate analysis were included in the LASSO logistic regression model.
 |
Table 2 The Univariate Logistic Regression Analysis of Frailty |
Ten factors (age, BMI, education, marital status, surgical method, tumor, diabetes, antihyperlipidemic drugs, interleukin-6, and hemoglobin) with nonzero coefficients were retained in the LASSO analysis (Figure 1) and were included in the further multivariate regression analyses (Figures 2 and 3). Finally, eight variables were identified as independent risk factors for frailty: age, BMI, education, surgical method, tumor, diabetes, antihyperlipidemic drugs and interleukin-6 (Table 3).
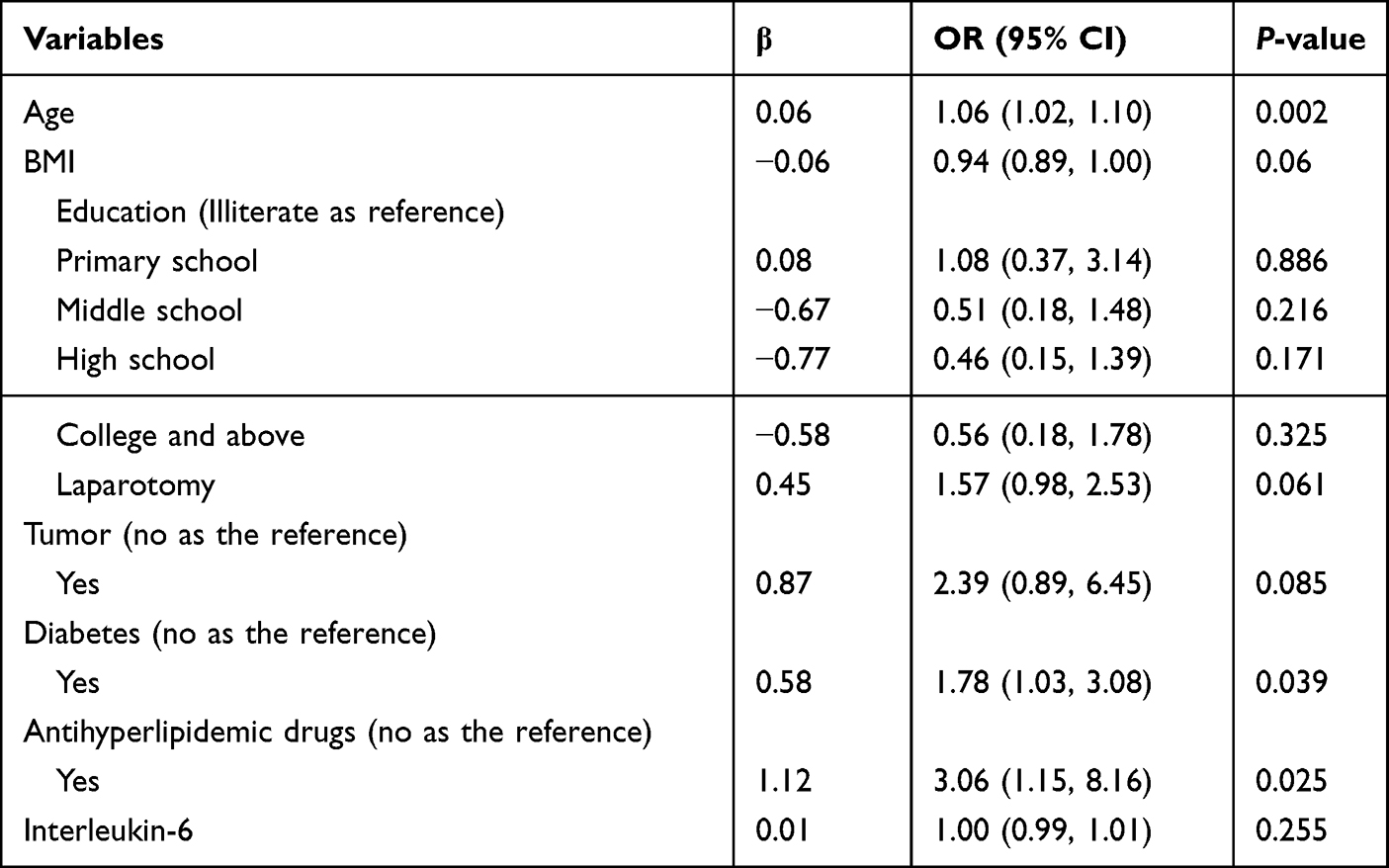 |
Table 3 The Multivariate Logistic Regression Analysis of Frailty |
 |
Figure 1 Cross-validation plot of LASSO regression analysis. |
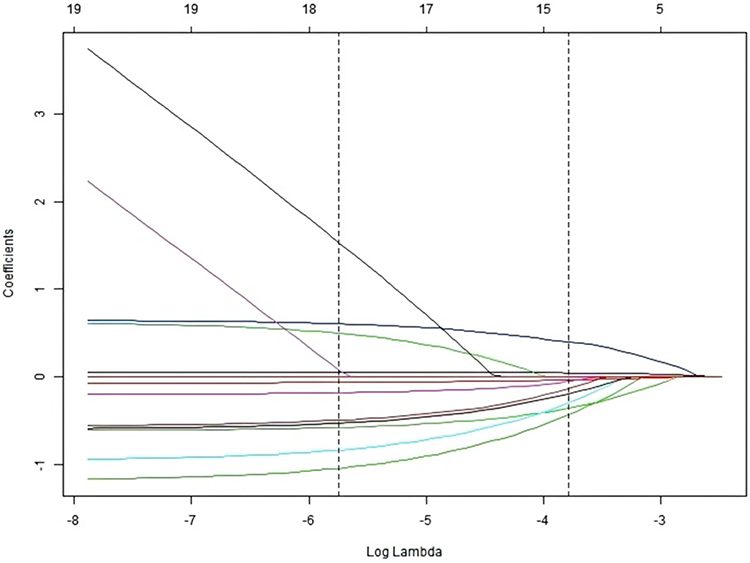 |
Figure 2 LASSO coefficient regularization path plot. |
 |
Figure 3 Nomogram of frailty risk. |
Predictive Nomogram for Frailty
We developed a nomogram to predict the frailty probability of older patients with abdominal surgery based on independent risk factors for frailty, the nomogram is illustrated in Figure 3. For example, a 70 years old patients with BMI 22kg/m2, college education, antihyperlipidemic drugs, non-laparotomy, non-tumor, non-diabetes and Interleukin-6 0 pg/mL would score of 92.5 points (22 points for 70 years old, 30 points for BMI 22kg/m2, 0 point for college education, 40.5 points for antihyperlipidemic drugs, 0 point for non-laparotomy, non-tumor, non-diabetes and Interleukin-6 0 pg/mL), which corresponded to 83.5% probability of frailty.
We randomly selected 75% of the total sample as the test group and the remaining 25% as the validation group. The AUC of the nomogram for predicting the probability of frailty was 0.748 in the test group and 0.707 in the validation group, indicating acceptable predictive performance (Figure 4).
 |
Figure 4 Receiver operating characteristic (ROC) curves show the predictive ability of the risk assessment model for frailty. |
Discussion
Summary of the Findings
This study represents the first effort to develop and validate a frailty risk assessment model tailored to older Chinese adults undergoing abdominal surgery. We identified a striking frailty prevalence of 74.18% in this population, substantially higher than rates reported in prior Chinese and international cohorts. Through univariate logistic regression, LASSO logistic regression and multivariate logistic regression, eight independent predictors of frailty were established: age, BMI, education, surgical method, tumor comorbidity, diabetes, antihyperlipidemic drug use, and interleukin-6 elevation. The nomogram demonstrated clinically acceptable predictive performance, with AUC values of 0.748 (test group) and 0.707 (validation group). This model provides clinicians with a practical tool to stratify perioperative risks, optimize surgical decision-making, and implement targeted interventions to mitigate postoperative complications and mortality.
Prevalence of Frailty
The frailty prevalence of 74.18% observed in our cohort markedly exceeds rates from comparable studies. For instance, Liang et al16 reported frailty rates of 19.2–35.1% in mixed surgical and non-surgical hospitalized older adults, while Han et al17 and Cao18 documented rates of 26.12% and 36.50%, respectively, in thoracic/abdominal surgery populations. Globally, frailty prevalence in non-cardiac surgical patients ranges from 10.60% (US)19 to 25.70% (UK emergency surgeries).20 This discrepancy likely stems from two key factors: (1) our cohort had a higher mean age (68.77 years vs 60–65 years in prior studies) and included a substantial proportion of cancer patients (10.13% colorectal cancer, 5.70% pancreatic cancer), both recognized frailty accelerators; (2) unlike studies using generic frailty tools (eg, Fried phenotype), the TFI’s multidimensional design (physical, psychological, social domains) may capture subtler deficits prevalent in abdominal surgery candidates.
In the present study, the use of the established TFI cutoff (≥5) for defining frailty resulted in a high prevalence rate of 47.1% among community-dwelling older adults. This high rate may reflect the inherent design of the TFI as a multidimensional screening instrument aimed at maximizing sensitivity rather than specificity. A high sensitivity is desirable in community and primary care settings to ensure that the majority of at-risk individuals are identified early, thereby allowing for timely interventions to prevent or delay adverse outcomes such as disability, increased healthcare use, and reduced quality of life. However, the trade-off for high sensitivity is often a lower specificity, which may lead to overidentification of individuals as “frail” who might not experience the outcome of interest (eg, mortality). This is supported by our findings, where the AUC values for mortality prediction using the TFI cutoff, though significant, were moderate (eg, unadjusted AUC = 0.627 for total frailty), indicating limited discriminatory accuracy.21 Therefore, while the TFI is a valuable tool for initial screening and comprehensive frailty assessment, clinicians and researchers should be aware of its operational characteristics—prioritizing broad detection over precise prognostic stratification—when implementing it in practice or interpreting results in relation to specific outcomes like mortality.
Risk Factors of Frailty
Frailty is a geriatric syndrome resulting from multiple interacting factors that collectively influence its development. Therefore, the risk prediction of frailty should be based on multiple factors rather than a single factor. In this study, we developed a predictive nomogram for frailty based on eight independent risk factors including demographic characteristics, disease, treatment, and laboratory indicators, thereby further corroborating the multidimensional concept of frailty.
Demographic and physiological factors:
Consistent with previous researches,22–24 advancing age and low BMI (a proxy for sarcopenia and malnutrition25,26) emerged as central frailty drivers. The protective effect of higher education aligns with Huibregtse et al’s27 observations, likely mediated by enhanced health literacy and proactive self-management behaviors in educated populations.
Surgical and comorbidity profiles:
Our study found that the surgical procedure was associated with frailty status, with patients undergoing laparoscopy being less likely to be frail compared to those undergoing open surgery. This finding was consistent with Sioutas et al’s28 literature review and Mosquera et al’s29 study, which showed a higher prevalence of frailty among patients undergoing open surgery compared to those undergoing laparoscopy. Compared to traditional open surgeries, laparotomy has multiple advantages, such as smaller surgical incisions, more rapid postoperative recovery, and fewer complications related to the internal organs, leading to a lower risk of frailty.30,31
The strong frailty association with tumors and diabetes corroborates mechanistic links between chronic metabolic stress (eg, insulin resistance, cachexia) and accelerated functional decline.32,33 Notably, 42.15% of our cohort had gallstone/cholecystitis—a condition often accompanied by chronic inflammation and nutritional malabsorption—potentially synergizing with comorbidities to amplify frailty.
Pharmacological and inflammatory mediators:
The use of antihyperlipidemic drugs was shown to be associated with an increased risk of frailty in our study, which may be related to the adverse effects of these drugs, especially statin-associated muscle symptoms (SAMS). SAMS often manifests as fatigue, muscle pain, cramps, or muscle weakness, with or without an increase in creatine kinase (CK).34 In severe cases, rhabdomyolysis may occur, causing severe skeletal muscle damage.34 Studies show that the use of antihyperlipidemic drugs may exacerbate age-related loss of muscle function and muscle weakness, leading to frailty.35,36
Finally, the results of this study showed that elevated interleukin-6 was associated with an increased risk of preoperative frailty. The inflammatory response is a potential pathophysiological change closely related to the occurrence and development of frailty. Interleukin-6 is an important pro-inflammatory cytokine that can lead to muscle atrophy by promoting skeletal muscle proteolysis, inducing insulin resistance, and promoting phosphorylation of myocyte growth factor.37 Xu et al38 conducted a systematic review and meta-analysis of 53 cross-sectional studies on the relationship between chronic inflammation and frailty, showing that the peripheral blood inflammatory marker interleukin-6 was related to frailty.
Limitations
The study has several limitations. First, the cross-sectional study design cannot verify the causal relationships between risk factors and frailty. Although the nomogram demonstrated good diagnostic performance in this study, its predictive ability requires further validation in longitudinal study designs. Second, this was a single-center study, which may lack representativeness for a broader population. Although we had a large sample size of 790 older patients undergoing abdominal surgery, further multicenter studies are needed to obtain a more representative sample and enhance the external validity of our model. Third, the model only collects data within a fixed period of time, and its long-term prediction effect needs to be confirmed by further research. In subsequent studies, time periods can be added for follow-up, and the nomogram can be compared with other frailty assessment scales to explore its clinical adaptability.
Conclusions
This study establishes that 74.18% of older adults undergoing abdominal surgery exhibit frailty, driven by a confluence of demographic, surgical, metabolic, and inflammatory factors. The nomogram showed good performance in predicting the probability of frailty. The nomogram can help clinicians to identify patients at high risk of frailty and make informed and effective decisions on further management, such as targeted and effective intervention and prevention efforts which can decrease frailty and improve patients’ outcomes. In addition, the nomogram can guide shared decision-making in borderline surgical candidates. Prior to any clinical application, our findings necessitate external validation and further investigation in higher-level clinical studies to assess their impact.
Statement
An unauthorized version of the Chinese MMSE was used by the study team without permission, however this has now been rectified with PAR. The MMSE is a copyrighted instrument and may not be used or reproduced in whole or in part, in any form or language, or by any means without written permission of PAR (www.parinc.com).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Ofori-Asenso R, Chin KL, Mazidi M, et al. Global incidence of frailty and prefrailty among community-dwelling older adults: a systematic review and meta-analysis. JAMA Network Open. 2019;2(8):e198398. doi:10.1001/jamanetworkopen.2019.8398
2. Ma L, Tang Z, Zhang L, et al. Prevalence of frailty and associated factors in the community-dwelling population of China. J Am Geriatr Soc. 2018;66(3):559–564. doi:10.1111/jgs.15214
3. He B, Ma Y, Wang C, et al. Prevalence and risk factors for frailty among community-dwelling older people in China: a systematic review and meta-analysis. J Nutr Health Aging. 2019;23(5):442–450. doi:10.1007/s12603-019-1179-9
4. Wu C, Smit E, Xue QL, et al. Prevalence and correlates of frailty among community-dwelling Chinese older adults: the China health and retirement longitudinal study. J Gerontol a Biol Sci Med Sci. 2017;73(1):102–108. doi:10.1093/gerona/glx098
5. Wei Y, Cao YP, Yang XL, Xu Y. Frailty syndrome in hospitalized geriatric patients and its risk factors. Fudan Univ J Med Sci. 2018;45(04):496.
6. Moldovan F, Ivanescu AD, Fodor P, et al. Correlation between inflammatory systemic biomarkers and surgical trauma in elderly patients with hip fractures. J Clin Med. 2023;12(15):5147. doi:10.3390/jcm12155147
7. Ondeck NT, Bohl DD, Bovonratwet P, et al. Discriminative ability of commonly used indices to predict adverse outcomes after poster lumbar fusion: a comparison of demographics, ASA, the modified Charlson comorbidity index, and the modified frailty index. Spine J. 2018;18(1):44–52. doi:10.1016/j.spinee.2017.05.028
8. Zhang Q, Zhang M, Hu S, et al. Prevalence and risk factors of preoperative frailty in Chinese elderly inpatients with gastric and colorectal cancer undergoing surgery: a single-center cross-sectional study using the Groningen frailty indicator. Support Care Cancer. 2022;30(1):677–686. doi:10.1007/s00520-021-06483-4
9. Richards SJG, Cherry TJ, Frizelle FA, et al. Pre-operative frailty is predictive of adverse post-operative outcomes in colorectal cancer patients. ANZ J Surg. 2021;91(3):379–386. doi:10.1111/ans.16319
10. Chen Y, Du H, Wei BH, et al. Development and validation of risk-stratification delirium prediction model for critically ill patients: a prospective, observational, single-center study. Medicine. 2017;96(29):e7543. doi:10.1097/MD.0000000000007543
11. Gobbens RJ, van Assen MA, Luijkx KG, et al. The Tilburg frailty indicator: psychometric properties. J Am Med Dir Assoc. 2010;11(5):344–355. doi:10.1016/j.jamda.2009.11.003
12. Zigmond AS, Snaith RP. The Hospital Anxiety and Depression Scale. Acta psychiatrica scandinavica. 1983;67(6):361–370. doi:10.1111/j.1600-0447.1983.tb09716.x
13. Folstein MF, Folstein SE, McHugh PR. “Mini-mental state”: a practical method for grading the cognitive state of patients for the clinician. J Psychiatr Res. 1975;12(3):189–198. doi:10.1016/0022-3956(75)90026-6
14. Mahoney FI, Barthel DW. Functional evaluation: the Barthel index. Md State Med J. 1965;14:61–65.
15. Nahm FS. Receiver operating characteristic curve: overview and practical use for clinicians. Korean J Anesthesiol. 2022;75(1):25–36. doi:10.4097/kja.21209
16. Liang YD, Zhang YN, Li YM, et al. Identification of frailty and its risk factors in elderly hospitalized patients from different wards: a cross-sectional study in China. Clin Interv Aging. 2019;14:2249–2259. doi:10.2147/CIA.S225149
17. Han B, Li Q, Chen X. Frailty and postoperative complications in older Chinese adults undergoing major thoracic and abdominal surgery. Clin Interv Aging. 2019;14:947–957. doi:10.2147/CIA.S201062
18. Cao T. Influencing factors and predictive performance of preoperative frailty in elderly patients undergoing elective abdominal surgery. Tianjin Medical University. 2019.
19. Shinall MC Jr, Arya S, Youk A, et al. Association of preoperative patient frailty and operative stress with postoperative mortality. JAMA Surg. 2020;155(1):e194620. doi:10.1001/jamasurg.2019.4620
20. Tan HL, Chia STX, Nadkarni NV, et al. Frailty and functional decline after emergency abdominal surgery in the elderly: a prospective cohort study. World J Emerg Surg. 2019;14:62. doi:10.1186/s13017-019-0280-z
21. Gobbens RJJ, van Assen M, Augustijn H, et al. Prediction of mortality by the Tilburg Frailty Indicator (TFI). J Am Med Dir Assoc. 2021;22(3):
22. Howlett SE, Rutenberg AD, Rockwood K. The degree of frailty as a translational measure of health in aging. Nat Aging. 2021;1(8):651–665. doi:10.1038/s43587-021-00099-3
23. O’Caoimh R, Galluzzo L, Rodríguez-Laso Á. Prevalence of frailty at population level in European advantage joint action member states: a systematic review and meta-analysis. Ann Ist Super Sanita. 2018;54(3):226–238. doi:10.4415/ANN_18_03_10
24. Qin Y, Hao X, Lv M, et al. A global perspective on risk factors for frailty in community-dwelling older adults: a systematic review and meta-analysis. Arch Gerontol Geriatr. 2023;105:104844. doi:10.1016/j.archger.2022.104844
25. Mustaffa M, Hairi NN, Majid HA, et al. Prevalence of co-occurrence of physical frailty and malnutrition and its associated factors among community-dwelling older adults in a Rural District, Malaysia. Asia Pac J Public Health. 2024;36(2–3):210–218. doi:10.1177/10105395241238092
26. McLean C, Randall AM, Ryan M, et al. The association of frailty and malnutrition with dietary intake and gastrointestinal symptoms in people with kidney failure: 2-year prospective study. J Ren Nutr. 2024;34(2):177–184. doi:10.1053/j.jrn.2023.10.006
27. Huibregtse BM, Newell-Stamper BL, Domingue BW, et al. Genes related to education predict frailty among older adults in the United States. J Gerontol B Psychol Sci Soc Sci. 2021;76(1):173–183. doi:10.1093/geronb/gbz092
28. Sioutas G, Tsoulfas G. Frailty assessment and postoperative outcomes among patients undergoing general surgery. Surgeon. 2020;18(6):e55–e66. doi:10.1016/j.surge.2020.04.004
29. Mosquera C, Spaniolas K, Fitzgerald TL. Impact of frailty on approach to colonic resection: laparoscopy vs open surgery. World J Gastroenterol. 2016;22(43):9544–9553. doi:10.3748/wjg.v22.i43.9544
30. Lee B, Youn SI, Lee K, et al. Comparing the short-term outcomes and cost between solo single-incision distal gastrectomy and conventional multiport totally laparoscopic distal gastrectomy for early gastric cancer: a propensity score-matched analysis. Ann Surg Treat Res. 2021;100(2):67–75. doi:10.4174/astr.2021.100.2.67
31. Xinhua C, Tian L, Huilin H, et al. Application value of overlap guiding tube (OGT) in assisting overlap esophagojejunostomy during laparoscopic total gastrectomy for gastric/gastroesophageal junction (G/GEJ) tumors. Gastric Cancer. 2022;25(4):827–836. doi:10.1007/s10120-022-01296-8
32. Guo Y, Miao X, Jiang X, Xu T, Xu Q. Associated factors of frailty in cancer patients: a meta-analysis. Chin Gen Med. 2023;26(08):989–996.
33. Yanagita I, Fujihara Y, Eda T, et al. Low glycated hemoglobin level is associated with severity of frailty in Japanese elderly diabetes patients. J Diabetes Investig. 2018;9(2):419–425. doi:10.1111/jdi.12698
34. Grundy SM, Stone NJ, Bailey AL. Guideline on the management of blood cholesterol: a report of the American college of cardiology/American heart association task force on clinical practice guidelines. Circulation. 2019;139(25):e1082–1143. doi:10.1161/CIR.0000000000000625
35. Lopez D, Nedkoff L, Briffa T, et al. Effect of frailty on initiation of statins following incident acute coronary syndromes in patients aged >/=75 years. Maturitas. 2021;153:13–18. doi:10.1016/j.maturitas.2021.07.006
36. Hale M, Zaman H, Mehdizadeh D, et al. Association between statins prescribed for primary and secondary prevention and major adverse cardiac events among older adults with frailty: a systematic review. Drugs Aging. 2020;37(11):787–799. doi:10.1007/s40266-020-00798-3
37. Lin B, Bai L, Wang S, et al. The association of systemic interleukin 6 and interleukin 10 levels with sarcopenia in elderly patients with chronic obstructive pulmonary disease. Int J Gen Med. 2021;14:5893–5902. doi:10.2147/IJGM.S321229
38. Xu Y, Wang M, Chen D, et al. Inflammatory biomarkers in older adults with frailty: a systematic review and meta-analysis of cross-sectional studies. Aging Clin Exp Res. 2022;34(5):971–987. doi:10.1007/s40520-021-02022-7
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Physical Exercise, Sports Spectating, and Subjective Life Expectancy in Older Chinese Adults: A Chain Mediation Analysis
Chen L, Guo J, Han X
Risk Management and Healthcare Policy 2025, 18:3675-3688
Published Date: 18 November 2025