Back to Journals » Infection and Drug Resistance » Volume 16
Phenotypic Characterization and Antibiograms of Extended-Spectrum Beta-Lactamase-Producing Escherichia coli Isolated at the Human-Animal-Environment Interface Using a One Health Approach Among Households in Wakiso District, Uganda
Authors Muleme J, Kankya C, Munyeme M ![]() , Musoke D
, Musoke D ![]() , Ssempebwa JC, Isunju JB, Wambi R
, Ssempebwa JC, Isunju JB, Wambi R ![]() , Balugaba BE, Sekulima T
, Balugaba BE, Sekulima T ![]() , Mugambe RK, Cadmus S
, Mugambe RK, Cadmus S ![]() , Kajumbula HM
, Kajumbula HM
Received 18 January 2023
Accepted for publication 1 April 2023
Published 14 April 2023 Volume 2023:16 Pages 2203—2216
DOI https://doi.org/10.2147/IDR.S398951
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 6
Editor who approved publication: Professor Suresh Antony
James Muleme,1,2 Clovice Kankya,2 Musso Munyeme,3 David Musoke,1 John C Ssempebwa,1 John Bosco Isunju,1 Rogers Wambi,2,4 Bonny Enock Balugaba,1 Tahalu Sekulima,5 Richard K Mugambe,1 Simeon Cadmus,6 Henry M Kajumbula7
1Department of Disease Control and Environmental Health, Makerere University School of Public Health, Kampala, Uganda; 2Department of Biosecurity Ecosystems and Veterinary Public Health, Makerere University College of Veterinary Medicine Animal Resources and Biosecurity, Kampala, Uganda; 3Department of Disease Control, School of Veterinary Medicine, University of Zambia, Lusaka, Zambia; 4Department of Clinical Laboratory, Mulago National Referral Hospital, Kampala, Uganda; 5Department of Biotechnical and Diagnostic Sciences, Veterinary Microbiology Research Laboratory, College of Veterinary Medicine, Animal Resources and Biosecurity, Kampala, Uganda; 6Department of Veterinary Public Health and Preventive Medicine, Center for Control and Prevention of Zoonoses, Faculty of Veterinary Medicine, University of Ibadan, Ibadan, Nigeria; 7Department of Medical Microbiology, Makerere University College of Health Sciences, Kampala, Uganda
Correspondence: James Muleme, Email [email protected]
Background: The occurrence of extended spectrum beta-lactamase (ESBL) producing bacteria such as Escherichia coli has increasingly become recognized beyond hospital settings. Resistance to other types of antibiotics limits treatment options while the existence of such bacteria among humans, animals, and the environment is suggestive of potential zoonotic and reverse-zoonotic transmission. This study aimed to establish the antibiotic susceptibility profiles of the ESBL-producing Escherichia coli (ESBL-EC) from human, animal, and environmental isolates obtained among farming households within Wakiso district using a One Health approach.
Methods: A total of 100 ESBL-EC isolates from humans 35/100 (35%), animals 56/100 (56%), and the environment 9/100 (9%) were tested for susceptibility to 11 antibiotics. This was done using the Kirby-Bauer disk diffusion method according to Clinical and Laboratory Standards Institute (CLSI) guidelines. Data were analyzed in STATA ver. 16 and graphs were drawn in Microsoft excel ver. 10.
Results: Most of the ESBL-EC isolates (98%) were resistant to more than two antibiotics. ESBL-EC isolates were most susceptible to meropenem (MEM) (88.0%), and imipenem (82.0%) followed by gentamicin (72%). ESBL-EC isolates from humans were most susceptible to meropenem (MEM) followed by imipenem (IPM)> gentamicin (CN)> ciprofloxacin (CIP). Animal samples were more susceptible to MEM, IPM, and CN but were highly resistant to cefotaxime (CTX)> cefepime (FEP)>other antibiotics. Multidrug resistance (MDR) was mostly reported among households keeping goats under intensive husbandry practices. Seven percent of the isolates exhibited carbapenem resistance while 22% showed aminoglycoside resistance. Similar resistance patterns among humans, animals, and environmental samples were also reported.
Conclusion: Our study provides baseline information on non-hospital-based MDR caused by ESBL-EC using a One Health approach. ESBL-EC isolates were prevalent among apparently healthy community members, animals, and their environment. It is important to conduct more One Health approach studies to generate evidence on the drivers, resistance patterns, and transmission of ESBL-producing organisms at the human-animal-environmental interface.
Keywords: antibiogram, community, ESBL-producing, Escherichia coli, one health, Wakiso
Plain Language Summary
This study followed an earlier survey that assessed the presence of a “Superbug” called extended spectrum beta-lactamase producing Escherichia coli (ESBL-EC) among humans, animals, and the environment within farming households in central Uganda. This superbug is hard to treat using the commonly available and recommended antibiotic drugs. In the current study, we subjected the ESBL-EC bacteria to a panel of 11 drugs to check if any of these drugs are still effective on these bacteria.
Almost all of the bacteria were resistant to more than two of the 11 antibiotic drugs. The bacteria were not 100% susceptible to the reserved drugs (carbapenem drugs). Gentamicin was the only drug with a high efficacy after Carbapenems. Further analysis revealed that several bacteria from animals, humans, and the environment seem to be shared given the nature of the drug resistance profiles. For instance, bacteria from one animal had the same resistance profile as one from another animal of different species but within the same household. Animal-human spillovers were also reported in this article. It is important to note that the majority of the households with bacteria resistant to multiple drugs, practiced goat farming under the intensive animal husbandry system.
There is hardly any non-hospital-based study in Uganda that has checked the drug susceptibility profiles of ESBL-EC organisms. This implies we provide a baseline study to this effect, able to inform practice. Therefore, human and animal health professionals should continue to preserve the last resort drugs and gentamicin.
Background
Antibiotics have been used in the successful treatment of bacterial infections over the past decades even though, antimicrobial resistance (AMR) cases are increasingly being reported globally over time.1,2 If no appropriate actions are taken, AMR will affect more than 10 million lives with an economic loss of US$100 trillion per year by the year 2050.3,4 Unfortunately, the true burden of AMR in the African region especially in the East African sub-region, is poorly documented. Even though such estimates would provide useful information for public health decision-making by prioritizing interventions against infectious organisms.
The World Health Organization (WHO) reports approximately 50% resistance to third-generation cephalosporins and fluoroquinolones among Escherichia coli (E. coli).5 Indeed, the occurrence of extended spectrum beta-lactamase (ESBL) producing bacteria such as E. coli has become increasingly recognized beyond hospital settings.6,7 E. coli has been implicated in both nosocomial and community-acquired infections, including respiratory tract infections, urinary tract infections, and enteric infections in Uganda and beyond.8,9 E. coli’s threat is mainly attributed to its ability to rapidly acquire antibiotic resistance through multiple mechanisms.10 Whereas evidence globally indicates the presence of E. coli in the environment and animals.11,12 Hospital-based studies constitute most of the current body of knowledge on AMR in low and middle-income countries (LMICs) such as Uganda.13
Globally, β-lactam drugs play an important role in the treatment of bacterial infection and account for almost 65% of antibiotic usage.14 Such antibiotics include penicillin, cephalosporins, cephamycin, carbapenems, monobactams, and β-lactamase inhibitors.15 These drugs target the cell wall synthesis that prevents perfect working of the penicillin-binding protein (PBP), which is responsible for cell wall synthesis in bacteria consequently leading to cellular death.13 Unfortunately, resistance to such important antibiotic classes is on the rise worldwide,16 perhaps these bacteria can produce extended-spectrum β-lactamase (ESBL) enzymes that render β-lactam drugs including 3rd generation cephalosporins, aztreonam, and some carbapenems ineffective. The subsequent resistance of ESBL-producing bacteria such as E. coli (ESBL-EC) to other antibiotics limits the treatment options for common bacterial infections while their existence among humans, animals, and the environment is suggestive of potential ESBL-related AMR transmission.17–19 Carbapenem drugs provide a broad-spectrum antibacterial activity against ESBL-producing organisms ranging from gram-negative to gram-positive.19,20 Despite this, there is an increasingly reported resistance of the ESBL-producing organisms to this critical class of antibiotics making them ineffective against hard-to-treat infections.21,22 Organisms such as ESBL-EC pose a major problem for clinical therapeutics in human and animal health thus undoing the progress made in achieving sustainable development goal 3.
Published studies have only focused on studying humans, animals, or the environment singly without the linkages leaving a gap in public health policy and practice.19,21–24 In this study, we examine the antibiotic susceptibility of ESBL-EC isolates from human (fecal and urine), animal (fecal), and environmental samples collected from farming households in a peri-urban community in Uganda. Therefore, this study sought to investigate Phenotypic characterization of ESBL producing organisms on the selected panel of antibiotics in the farming household setting.
Materials and Methods
Study Design
This cross-sectional laboratory-based study was conducted between June and July 2022 in Wakiso district central Uganda. Confirmed ESBL-producing E. coli (ESBL-EC) isolates were subjected to antibiotic susceptibility testing (AST). This analysis was conducted at the Makerere University, Veterinary Microbiology Research Laboratory.
Sample Collection, Transportation, and Preliminary Analysis
A total of 104 farming households were studied between March and July 2022. From these, 988 fresh samples were obtained from humans, animals, and the environment. Humans provided urine and or fecal, animals provided fecal samples per rectal, while environmental samples constituted soil, water for domestic use, swabs from animal feeding equipment, and doorknobs. The sample containers were labeled with a unique code that represented the household and the sample category. Within four hours of sample collection, samples were delivered to the Microbiology Laboratory in Ziploc bags under the ice.
ESBL chromogenic agar, CHROMID® ESBL (Condalab 2062, Madrid Spain) containing ESBL supplement (condalab6042, Madrid Spain) having inhibition and selective agents for detection of gram-negative bacteria producing extended-spectrum Beta lactamases. Presumptive ESBL-EC appeared as pink, medium-sized, raised, and moist colonies after 24 hours of incubation at 37°C (Figure 1). E. coli isolates were further confirmed by biochemical tests following standard operating procedures. Isolates with reduced susceptibility to cefotaxime (≤ 27 mm) and ceftazidime (≤ 22 mm) were confirmed for ESBL production using the modified double disk synergy (MDDS) method. The plates were then incubated at 35°C for 24 hours and examined for an enhancement of the inhibition zone of the β-lactam drugs caused by the synergy of the drugs and were interpreted as either being positive or negative for ESBL production (Figure 2).
 |
Figure 1 Primary cultures and subcultures. |
 |
Figure 2 Modified double disc diffusion test results. |
Approximately 25.4% (251/988) of the original samples were confirmed positive for ESBL-EC. Of these positives, 89, 139, and 23 isolates were from human, animal, and environmental samples respectively. During this study, 40% of each of the above positive categories was considered for AST. Therefore 100 ESBL-EC confirmed isolates were randomly selected for use in this study. This number agrees with the recommended sample size for the tricycle project for studying ESBL-EC in community settings.25
Antibiotic Sensitivity of E. coli Strains
The obtained 100 previously confirmed and cryopreserved ESBL-EC isolates were picked from the −80°C freezer and left to thaw in ice flakes. These were resuscitated by inoculating 100µL of broth in 1 mL of brain heart infusion broth and incubated overnight at 37°C. The broth cultures were then streaked onto freshly prepared MacConkey agar plates and incubated at 37°C for 24 hours in ambient air.26 Drug susceptibility testing was done following the Kirby Bauer disc diffusion method.27–29 Briefly, the 24-hour-old cultures were standardized by adjusting their turbidity to match the 0.5% McFarland standard. Using a sterile cotton-tipped swab, an inoculum was introduced onto freshly prepared Mueller Hinton agar plates and streaked to make a continuous lawn onto which antibiotic discs were added.
Eleven (11) different antibiotic discs were used for each isolate, these were Amoxicillin-clavulanic acid, AMC (30µg), Ciprofloxacin, CIP (5 µg), Gentamycin, CN (30 µg), Tetracycline, TE (30 µg), Sulfamethoxazole-Trimethoprim, SXT (25 µg), Cefotaxime, CTX (30 µg), Ceftazidime, CAZ (30 µg), Cefepime, FEP (30 µg), Aztreonam, ATM (30 µg), Imipenem, IPM (10 µg) and Meropenem, MEM (10 µg). Briefly, two plates were set for each isolate, one having 5 drugs and another plate having 6 drugs. The plates were then incubated at 37°C for 18 hours at ambient temperature and examined the following day for a confluence of growth and clearance around the drug discs. The diameters of the inhibition zones were measured to the nearest whole number in millimeters (mm) using a divider and a ruler. The results were interpreted according to breakpoints in the CLSI 2021 guidelines (Supplementary Table 1).
Data Management and Analysis
All data generated from the daily activities were regularly entered into a laboratory workbook. Descriptive statistical analysis was done using STATA version 16 and results were presented as frequencies, percentages, and graphs. Drug resistance profiles in this study mean the expression of the number of drugs to which isolates were resistant. These were presented as R1 for one drug, R2 for two drugs, and R9 for nine drugs respectively. Frequencies and Multiple antibiotic resistance index (MARI) numbers were then tabulated. MARI for all multidrug resistant (MDR) isolates was also calculated.30,31 MARI was determined by dividing the number of antibiotics to which an isolate is resistant by the total number of antibiotics to which each ESBL-EC isolate was subjected. Regarding relatedness, the sample sources ie, animals, humans, and or environment, and their respective types were noted. Unique identifiers ie A, B, C, and D were assigned to each of the samples as a prefix before the sample type name. Comparisons were then made across the panel of 11 drugs to check if any of the isolates from respective samples shared a similar antibiotic susceptibility profile.
Results
Characteristics of the ESBL-EC Isolates
Out of the 100 ESBL-EC isolates, 56%, 35%, and 9% belonged to animals, humans, and the environment respectively. Most, 37.5% (21/56) of the animal isolates were obtained from goat samples while 74.3% (26/35) of the human isolates were obtained from fecal samples. Swabs from the animal feeding equipment contributed the greatest number 55.6% (5/9) of environmental isolates (Table 1).
 |
Table 1 ESBL-EC Sample Characteristics |
Performance of Selected Antibiotics on ESBL-EC Isolates
Performance was measured based on the resistance and or susceptibility of the organism to the respective antibiotics. Of the 11 antibiotics tested, the ESBL-EC isolates were most susceptible to Carbapenems (meropenem and imipenem) at 88.0% and 82.0% respectively. Aminoglycoside (gentamicin) followed with 72% susceptibility while the rest of the antibiotics had susceptibilities below 50% (Table 2).
 |
Table 2 Antibiograms of Different Drugs on the ESBL-EC Isolates |
Antibiograms of Human, Animal, and Environmental ESBL-EC Isolates
Overall, ESBL-EC isolates from humans, animals, and the environment were more susceptible to Carbapenems (MEM and IPM) and Aminoglycosides (gentamicin). ESBL-EC isolates from humans and the environment were more susceptible to MEM than IPM. ESBL-EC isolates from humans were most susceptible to MEM followed by IPM> CN> CIP and were highly resistant to (FEP~CTX)> (TE~ATM)> SXT> CAZ among others (Figure 3). ESBL-EC isolates from the environment were most susceptible to MEM, followed by IPM, and were highly resistant to ATM, CTX, and FEP respectively. ESBL-EC isolates from the environment had similar susceptibility profiles to gentamycin and imipenem (Figure 4).
 |
Figure 3 Antibiograms of ESBL-EC Human isolates. |
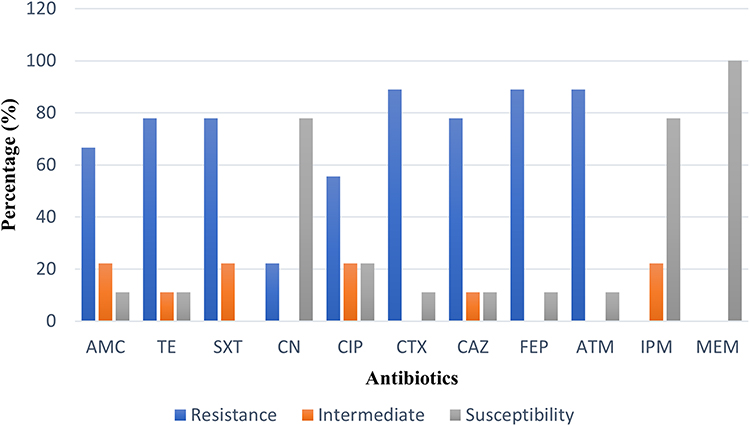 |
Figure 4 Antibiograms of ESBL-EC Environmental isolates. |
Animal isolates on the other hand were more susceptible to MEM, IPM, CN, and least for CAZ, CTX, and FEP. Animal isolates were highly resistant to CTX>FEP>other antibiotics. Animal ESBL-EC isolates had similar susceptibility to Carbapenems (MEM and IPM) (Figure 5).
 |
Figure 5 Antibiograms of ESBL-EC Animal isolates. |
Antibiotic Susceptibility Patterns for Individual ESBL-EC Isolates from Humans, Animals, and the Environment
ESBL-EC isolates from cows, ducks, and dogs had the lowest susceptibility (66.7%) to Carbapenems when compared to isolates from other domestic animals. ESBL-EC isolates from most animals were moderately susceptible to gentamicin (66.7–100) % except for isolates from dogs with the least susceptibility at 33.3%. Isolates from sheep and cats had the highest susceptibility (100%) to AMC while those from rabbits had the highest susceptibility (100%) to SXT. ESBL-EC from animals had a low susceptibility to other antibiotics such as tetracyclines and ciprofloxacin.
ESBL-EC isolates from human fecal samples were more susceptible to meropenem (92.3%) than those from urine samples (88.9%). ESBL-EC isolates from urine samples on the other hand were more susceptible to imipenem (88.9%) than those from fecal samples (76.9%). Human ESBL-EC isolates had low susceptibility to other antibiotics tested (<50%) however, those from fecal samples were still susceptible to gentamicin (69.2%).
ESBL-EC isolates from the environment were only susceptible to Carbapenems (75–100) % and gentamicin (75–80) %. These registered the lowest susceptibility to other classes of antibiotics among all isolates used in our study (40% and below) (Table 3).
 |
Table 3 Frequency and Proportion of Susceptibility for Individual ESBL-EC Isolates from Humans, Animal, and Environment |
Multidrug Resistance Among ESBL-EC Isolates
Two (2) percent of the organisms were resistant to at most 2 antibiotics with 1% being resistant to one drug (MARI = 0.09) and 1% being resistant to two drugs (MARI = 0.18). Up to 98% of the isolates were resistant to at least three antibiotics (Table 4). The different antibiotic resistance profiles are reported in Supplementary Table 2.
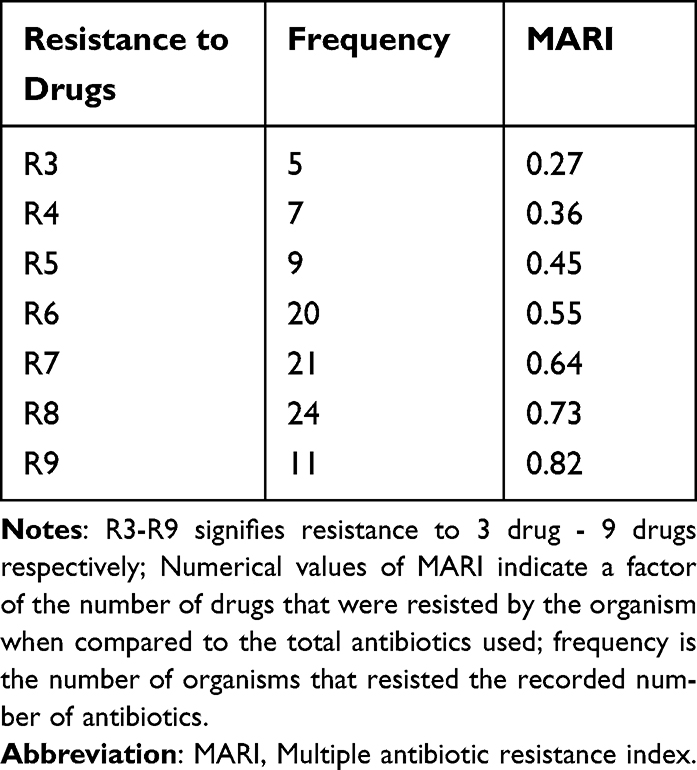 |
Table 4 Drug Resistance Profile of ESBL-EC Isolates |
Relatedness in Drug Sensitivity Profiles Among ESBL-EC Isolates from Unique Households
Out of the sampled households, only 4 showed similarities in resistance to over 10 out of the 11 drugs used. From household A, the chicken and the cat had similar antibiotic resistance profiles across all eleven drugs. From household D, the humans (fecal isolate) shared a resistance profile as environmental soil isolate for all drugs apart from AMC. In household B, the pig and goats shared the same resistance profile for all drugs. For household C, humans shared similar resistance with animals (goats) for ten drugs apart from gentamycin where the human sample was resistant while the animal (goat) sample was susceptible (Figure 6).
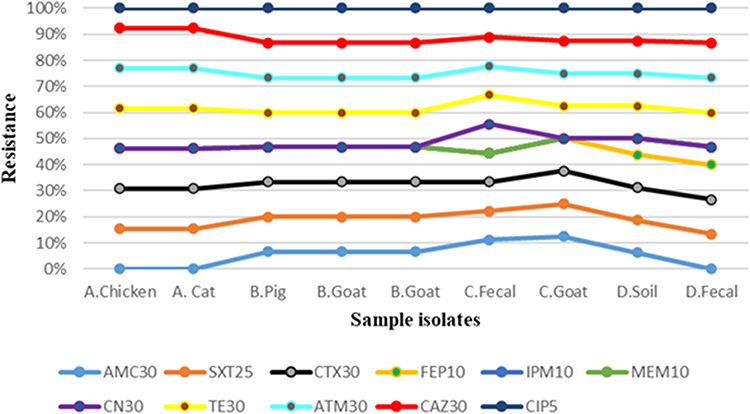 |
Figure 6 Antibiotic sensitivity profiles for isolates from four unique households. |
Matrix of Factors Linked to the Highest and Lowest Resistance
For this matrix, we considered 8 households with ESBL-EC isolates showing resistance to a high number of antibiotics (>8). These households were practicing an intensive animal husbandry system, obtained water from a protected water source, had heads having attained “primary and above” education level, and reared mainly goats (Table 5). On the other hand, households with the least (n=3) number of MDR ESBL-EC isolates were characterized by a free-ranging animal husbandry system, headed by elderly (>50 years) females who had no formal education record, negotiated with health professionals on dosage due to financial constraints, and was in a rural setting (Supplementary Table 3).
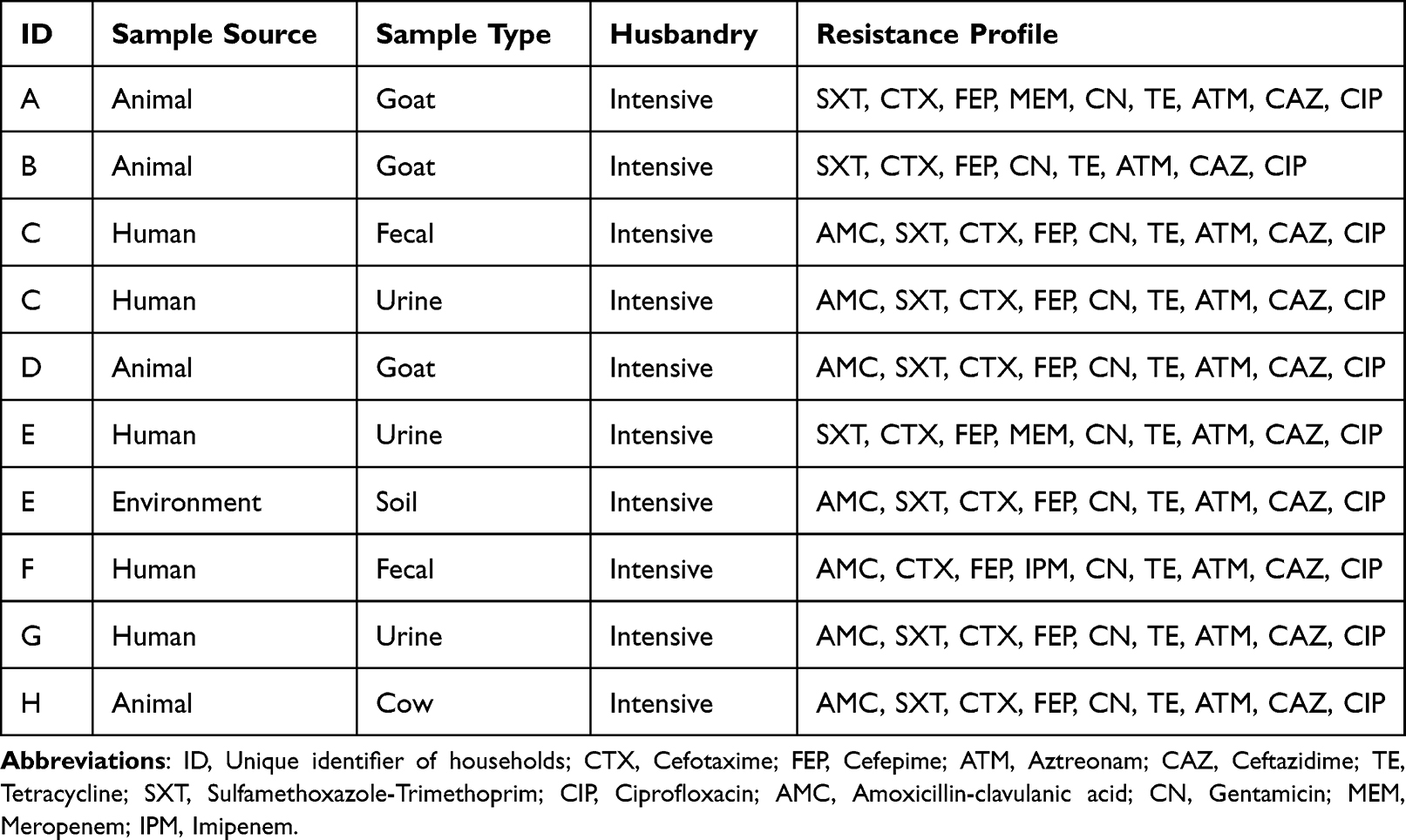 |
Table 5 Matrix for the Highest Resistance Among Households |
Discussion
Since the early 2000s, ESBL-producing organisms have been greatly recognized and implicated in several hospital and community-acquired infections around the world.32 Understanding the resistance patterns exhibited by ESBL-producing organisms such as E. coli is paramount in choosing the available effective antibiotic therapy to be adopted during human and animal treatment. This also provides evidence-based advice for good agricultural practices to regulate the use of antibiotic agents to prevent and control AMR development. Our study details the antibiotic sensitivity profiles of the increasingly recognized ESBL-EC organisms at the human-animal-environmental interface using a One Health paradigm as earlier used.33
Up to 98% of the ESBL-EC isolates in this study were resistant to at least three antibiotics. We, therefore, report a low percentage (2%) of non-MDR ESBL-EC isolates ie, 1% being resistant to one drug and 1% being resistant to two drugs. ESBL-EC isolates were more susceptible to meropenem (MEM), and imipenem followed by gentamicin. ESBL-EC isolates from humans and animals were most susceptible to MEM followed by imipenem (IPM)> gentamicin (CN)> ciprofloxacin (CIP). ESBL-EC isolates from the environment were most susceptible to MEM, followed by IPM, and were highly resistant to other antibiotics. ESBL-EC isolates from the environment had similar susceptibility profiles for gentamicin and imipenem. Importantly, our results reveal some degree of similarity in the phenotypic antibiograms of the different samples from humans, animals, and the environment which is indicative of potential transmission at the household interface. Such observed resistance profiles of the ESBL-EC isolates obtained from community settings are worrying and warrant urgent attention.
Out of the 11 antibiotics used in our study, carbapenems ie, meropenem and imipenem had the highest activity against the ESBL-EC isolates from humans, animals, and the environment. Despite this, only 88% and 82% of the isolates were susceptible with about 5% and 2% being resistant to MEM and IPM respectively. Reporting carbapenem resistance in community settings presents a worrying situation since this class of drugs is the last resort beta-lactam and is considered the safest and most effective antibiotic for the treatment of bacterial infections. Carbapenems have also been reported in several other studies to still be effective on ESBL-producing organisms.34,35 A study conducted in rural Tanzania among scavenging local chickens also revealed that the ESBL-EC isolates were 100% susceptible to Carbapenems and gentamicin.36 Presentation of carbapenem resistance in our study could potentially be linked to exposures from hospital settings where significant resistance to this class of antibiotics has been reported. It is important to note that despite being a beta-lactam antibiotic, carbapenem efficacy has been attributed to their stability against beta-lactamase enzymes produced by the ESBL bacteria, rendering them the treatment of choice against ESBL infections.37 Infection prevention and control, as well as hygiene measures, need to be promoted to make hospital environments safe and ensure the protection of humans (patients and caretakers) respectively. A limitation of this study is that we did not screen for carbapenemase-producers among the isolates, which could potentially cause an overestimate in ESBL-EC prevalence.
More than 60% of the ESBL-EC in this study were still susceptible to these aminoglycosides (gentamicin), which is quite useful. On the contrary, a study conducted in Thailand revealed a high degree of ESBL-EC resistance to gentamicin among cows even though the calves were susceptible to the same antibiotic.38 The difference in the ESBL-EC sensitivity to gentamicin could be because of the routine use of aminoglycosides on cattle farms in Thailand thus creating selective pressure for the antibiotic. It is important to note that studies conducted on bacterial sensitivity to aminoglycosides within hospital settings have reported a slightly higher resistance.39,40 On the other hand, the mechanism of action (creating fissures in the outer membrane of the bacterial cell and inhibiting bacterial polyprotein synthesis) for Aminoglycosides such as gentamicin makes them still effective at treating these ESBL infections.39 Such action is however interrupted by the co-existence of aminoglycoside and carbapenem resistance. In Uganda, there is currently limited use of gentamicin in the treatment of microbial infections due to the feared nephrotoxicity and need for multiple daily dosing, unlike ceftriaxone which is perceived safe and taken in a single daily dose. Like it is for carbapenems, the source of gentamicin resistance in community bacterial samples remains largely unclear even though links can be made to hospital settings or previous admission to hospital and veterinary practice.
The ESBL-EC isolates registered a high resistance to fluoroquinolones, cephalosporins, and penicillin within the study population in Wakiso district. These results are similar to those of a study in Morocco which reported a high resistance (100%) of ESBL-EC urinary tract infections to cephalosporins and penicillin with inhibitors such as Amoxicillin/ clavulanate.41 Similar antibiotic resistance patterns have been reported in other studies elsewhere.30,42 The clear cause of ESBL-EC community occurrence and their corresponding high resistance to most antibiotics remains complex and under-studied. However, the reported irrational use of antibiotics among humans and animals, the presence of resistant organisms in the environment coupled with the high degree of interaction at the human-animal-environment interface could potentially contribute to this problem. Other studies back up this argument by demonstrating that antibiotic-resistant organisms have a set of mechanisms for transferring drug resistance genes from one bacteria to another via plasmids, and transposons among others thus limiting the therapeutic choice and increasing treatment failure.43,44
Based on the MARI values reported in our study, most of the ESBL-EC isolates belonged to the MDR class. Previous studies have shown that all ESBL-producing E. coli isolates belong to MDR.45,46 These results are contrary to those reported in a study conducted among livestock in Malaysia that indicated a very low prevalence of MDR ESBL-EC.47 The difference in the MARI could be attributed to the variations in the regulation of antibiotic use in the two countries. This high degree of resistance in almost all the drug combinations in this study could be associated with epidemiological and practice factors. Studies have reported several factors that include availability and accessibility without a doctor’s prescription from a pharmacy and relatively cheap.48–50 In addition, self-prescription, antibiotic drug leftovers, and subsequent use of antibiotics for all types of infection by patients, animal health workers, quacks, and doctors these actions expose pathogens to low or high doses of antibiotics leading to AMR development.51–53 Low- and middle-income countries such as Uganda need to enhance the regulation of antibiotic use among humans, animals, and crops.
The presence of similar resistance profiles among humans, animals, and the environment at the household level in our study area is suggestive of both horizontal zoonotic and reverse zoonotic transmission. This study reports relatedness in the resistance profiles exhibited at the household level ie, cats and chickens; pigs and goats; humans and goats; soil and humans. This could be explained by the potential ESBL-EC transmission at the human-animal-environment interface since some antibiotics have not been reported to be used in animal treatment. For instance, in Uganda, there is currently no reported use of carbapenems in the treatment of animals, especially livestock, therefore, the presence of carbapenem resistance could also imply potential transmission from either hospital settings, household, and or farm environments. Similarly, despite the prohibited use of carbapenems in livestock production in Germany, studies have reported high carbapenem resistance among dogs.54 This can be suggestive of human-to-animal transmission of the resistance genes. It is therefore important to promote improved infection prevention and control as well as biosecurity measures at the farming household level to intercept the transmission pathway of the resistant organisms. In addition, public health interventions should be designed to break the chain of interactions and reduce the burden of ESBL-EC and associated consequences.
Based on the epidemiological factors reported, households that had the highest number of MDR ESBL-EC isolates were practicing intensive animal husbandry systems and mainly reared goats. Studies conducted in both LMICs and developed countries to ascertain the burden of antibiotic residues have reported goats’ meat to have a lot of drug residues.55 Several other studies also report that under the intensive animal husbandry system, there is wide use of antimicrobial agents for disease prevention, treatment, and growth promotion.56,57 There is a need for the creation of specific diagnostic and treatment protocols for small ruminants such as goats to minimize irrational use and subsequent resistance development and its socio-economic outcomes. It is no doubt that the intensive usage of antimicrobials in livestock production and human health may cause selection for resistance among microorganisms. Therefore, veterinary authorities, farmers, and human medical practitioners should be sensitized and alerted to rationalize the usage of antimicrobials to reduce the AMR burden and preserve the efficacy of the treatment options.
Conclusion
Our study provides baseline information on the multi-drug resistance nature of ESBL-EC at the human-animal-environment interface. ESBL-EC isolates were prevalent among apparently healthy community members, animals, and their environment in Wakiso district, central Uganda. Our study provides baseline information on non-hospital-based MDR caused by ESBL-EC using a One Health approach. Routine monitoring of ESBL producers, and improved regulation of antibiotic use, alongside increased antibiogram testing may greatly reduce the burden of resistant bacteria in community settings and subsequent disease outbreaks. More studies using a One Health approach are needed to generate more evidence on the drivers, resistance patterns, and transmission of ESBL-producing organisms at the human-animal-environmental interface.
Abbreviations
AMR, Antimicrobial Resistance; AST, Antibiotic Susceptibility Testing; CLSI, Clinical and Laboratory standards Institute; ESBL, Extended Spectrum Beta-Lactamase; ESBL-EC, ESBL-producing Escherichia coli; I, Intermediate; LMICs, low and middle-income countries; MARI, Multiple antibiotic resistance index; MDR, Multidrug resistance; R, Resistant; S, Susceptible; WHO, World Health Organization.
Ethical Considerations
The study was approved by the Makerere University School of Public Health Higher Degrees Research and Ethics Committee (HDREC), protocol number SPH-2021-167 and registered with the Uganda National Council for Science and Technology (UNCST) registration number HS1919ES. The participants consented to using their samples for further analysis within the same approved study.
Acknowledgment
The authors acknowledge the work of all farmers, village health team members, district officials, and research assistants in Wakiso district to the support rendered in the study process until completion.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This research was supported by the Consortium for Advanced Research Training in Africa (CARTA). CARTA is jointly led by the African Population and Health Research Center and the University of the Witwatersrand and funded by the Carnegie Corporation of New York (Grant No–B 8606.R02), Sida (Grant No:54100113), the DELTAS Africa Initiative (Grant No: 107768/Z/15/Z) and Deutscher Akademischer Austauschdienst (DAAD). The DELTAS Africa Initiative is an independent funding scheme of the African Academy of Sciences (AAS)’s Alliance for Accelerating Excellence in Science in Africa (AESA) and supported by the New Partnership for Africa’s Development Planning and Coordinating Agency (NEPAD Agency) with funding from the Wellcome Trust (UK) and the UK government. James Muleme is a CARTA PhD fellow. The statements made and views expressed are solely the responsibility of the Fellow. The funders had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Ferri M, Ranucci E, Romagnoli P, Giaccone V. Antimicrobial resistance: a global emerging threat to public health systems. Crit Rev Food Sci Nutr. 2017;57:2857–2876. doi:10.1080/10408398.2015.1077192
2. Bassetti M, Poulakou G, Ruppe E, et al. Antimicrobial resistance in the next 30 years, humankind, bugs and drugs: a visionary approach. Intensive Care Med. 2017;43:1464–1475. doi:10.1007/s00134-017-4878-x
3. Patel A. Tackling antimicrobial resistance in the shadow of covid-19. MBio. 2021;12. doi:10.1128/mBio.00473-21
4. Cassini A, Högberg LD, Plachouras D, et al. Attributable deaths and disability-adjusted life-years caused by infections with antibiotic-resistant bacteria in the EU and the European Economic Area in 2015: a population-level modelling analysis. Lancet Infect Dis. 2019;19:56–66. doi:10.1016/S1473-3099(18)30605-4
5. World Health Organization. WHO Report on Surveillance of Antibiotic Consumption: 2016–2018 Early Implementation. Geneva: World Health Organization; 2018.
6. Adekanmbi AO, Akinpelu MO, Olaposi AV, Oyelade AA. Extended spectrum beta-lactamase encoding gene-fingerprints in multidrug resistant Escherichia coli isolated from wastewater and sludge of a hospital treatment plant in Nigeria. Int J Environmental Stud. 2020;140–150. doi:10.1080/00207233.2020.1778271
7. Gekenidis MT, Qi W, Hummerjohann J, et al. Antibiotic-resistant indicator bacteria in irrigation water: high prevalence of extended-spectrum beta-lactamase (ESBL)-producing Escherichia coli. PLoS One. 2018;13:e0207857. doi:10.1371/journal.pone.0207857
8. Mbyemeire H, Ssekatawa K, Kato CD, Wampande EM. Molecular characterization and distribution of cephalosporin resistance determinants in Escherichia coli and Klebsiella pneumoniae isolated from patients attending Kampala International University Teaching Hospital in Bushenyi, Western Uganda. Alexandria J Med. 2021;57:205–214. doi:10.1080/20905068.2021.1952821
9. Odongo I, Ssemambo R, Kungu JM. Prevalence of Escherichia coli and its antimicrobial susceptibility profiles among patients with UTI at Mulago Hospital, Kampala, Uganda. Interdiscip Perspect Infect Dis. 2020;2020. doi:10.1155/2020/8042540
10. Dunn SJ, Connor C, McNally A. The evolution and transmission of multi-drug resistant Escherichia coli and Klebsiella pneumoniae: the complexity of clones and plasmids. Curr Opin Microbiol. 2019;51:51–56. doi:10.1016/j.mib.2019.06.004
11. Thanner S, Drissner D, Walsh F. Antimicrobial resistance in agriculture. MBio. 2016;7. doi:10.1128/mBio.02227-15
12. Gwenzi W, Musiyiwa K, Mangori L. Sources, behaviour and health risks of antimicrobial resistance genes in wastewaters: a hotspot reservoir. J Environ Chem Eng. 2020;8:102220. doi:10.1016/j.jece.2018.02.028
13. Musoke D, Kitutu FE, Mugisha L, et al. A one health approach to strengthening antimicrobial stewardship in Wakiso District, Uganda. Antibiot. 2020;9:764. doi:10.3390/antibiotics9110764
14. Patel MP, Hu L, Brown CA, et al. Synergistic effects of functionally distinct substitutions in Î2-lactamase variants shed light on the evolution of bacterial drug resistance. J Biol Chem. 2018. doi:10.1074/jbc.RA118.003792
15. Bush K, Bradford PA. Interplay between β-lactamases and new β-lactamase inhibitors. Nat Rev Microbiol. 2019;17:295–306. doi:10.1038/s41579-019-0159-8
16. Sonda T, Kumburu H, van Zwetselaar M, et al. Meta-analysis of proportion estimates of extended-spectrum-beta-lactamase-producing Enterobacteriaceae in East Africa hospitals. Antimicrob Resist Infect Control. 2016;5:18. doi:10.1186/s13756-016-0117-4
17. Bader MS, Loeb M, Brooks AA. An update on the management of urinary tract infections in the era of antimicrobial resistance. Postgrad Med. 2016;129:242–258. doi:10.1080/00325481.2017.1246055
18. Mazzariol A, Bazaj A, Cornaglia G. Multi-drug-resistant Gram-negative bacteria causing urinary tract infections: a review. J Chemother. 2017;29:2–9. doi:10.1080/1120009X.2017.1380395
19. Shnaiderman-Torban A, Navon-Venezia S, Baron H, et al. Prevalence and molecular characterization of extended-spectrum β-lactamase producing enterobacterales in healthy community dogs in Israel. Antibiotics. 2022;11:1069. doi:10.3390/antibiotics11081069
20. Kakooza S, Munyiirwa D, Ssajjakambwe P, et al. Epidemiological dynamics of extended-spectrum β -lactamase- or AmpC β -lactamase-producing Escherichia coli screened in apparently healthy chickens in Uganda. Scientifica. 2021;2021:1–6. doi:10.1155/2021/3258059
21. Seni J, Najjuka CF, Kateete DP, et al. Antimicrobial resistance in hospitalized surgical patients: a silently emerging public health concern in Uganda. BMC Res Notes. 2013;6:1–7. doi:10.1186/1756-0500-6-298
22. Kateregga JN, Kantume R, Atuhaire C, Lubowa MN, Ndukui JG. Phenotypic expression and prevalence of ESBL-producing Enterobacteriaceae in samples collected from patients in various wards of Mulago Hospital, Uganda. BMC Pharmacol Toxicol. 2015;16:1–6. doi:10.1186/s40360-015-0013-1
23. Ball T, Monte D, Aidara-Kane A, et al. International lineages of Salmonella enterica serovars isolated from chicken farms, Wakiso District, Uganda. PLoS One. 2020;15:e0220484. doi:10.1371/journal.pone.0220484
24. Kivumbi MT, Standley CJ. Efforts to identify and combat antimicrobial resistance in Uganda: a systematic review. Trop Med Infect Dis. 2021;6:86. doi:10.3390/tropicalmed6020086
25. World Health Organization. Global Antimicrobial Resistance and Use Surveillance System (GLASS): Early Implementation 2020. Available from: https://www.who.int/publications/i/item/9789240005587.
26. Babalola TO. Utilization of microbial consortia as biofertilizers and biopesticides for the production of feasible agricultural product. Int J Life Sci. 2021;57:57–66.
27. Dégi J, Moțco O-A, Dégi DM, et al. Antibiotic susceptibility profile of Pseudomonas aeruginosa canine isolates from a multicentric study in Romania. Antibiotics (Basel, Switzerland). 2021;10:846. doi:10.3390/antibiotics10070846
28. Gaire U, Thapa Shrestha U, Adhikari S, et al. Antibiotic susceptibility, biofilm production, and detection of mecA gene among Staphylococcus aureus isolates from different clinical specimens. Diseases. 2021;9:80. doi:10.3390/diseases9040080
29. Aksel H, Küçükkaya Eren S, Çakar A, et al. Effect of instrumentation techniques and preparation taper on apical extrusion of bacteria. J Endod. 2017;43:1008–1010. doi:10.1016/j.joen.2017.01.014
30. Gekenidis M-T, Kläui A, Smalla K, Drissner D. Transferable extended-spectrum β-lactamase (ESBL) plasmids in Enterobacteriaceae from irrigation water. Microorganisms. 2020;8:978. doi:10.3390/microorganisms8070978
31. Elbehiry A, Marzouk E, Moussa IM, et al. Acinetobacter baumannii as a community foodborne pathogen: peptide mass fingerprinting analysis, genotypic of biofilm formation and phenotypic pattern of antimicrobial resistance. Saudi J Biol Sci. 2021;28:1158–1166. doi:10.1016/j.sjbs.2020.11.052
32. Shakya P, Shrestha D, Maharjan E, Sharma VK, Paudyal R. ESBL Production among E. coli and Klebsiella spp. causing urinary tract infection: a hospital based study. Open Microbiol J. 2017;11:23. doi:10.2174/1874285801711010023
33. Subramanya SH, Bairy I, Metok Y, Baral BP, Gautam D, Nayak N. Detection and characterization of ESBL-producing Enterobacteriaceae from the gut of subsistence farmers, their livestock, and the surrounding environment in rural Nepal. Sci Rep. 2021;11:1–13.
34. D’Angelo RG, Johnson JK, Bork JT, Heil EL. Treatment options for extended-spectrum beta-lactamase (ESBL) and AmpC-producing bacteria. Expert Opin Pharmacother. 2016;17:953–967. doi:10.1517/14656566.2016.1154538
35. Abalkhail A, AlYami AS, Alrashedi SF, et al. The prevalence of multidrug-resistant Escherichia coli producing ESBL among male and female patients with urinary tract infections in Riyadh Region, Saudi Arabia. Healthc. 2022;10:1778. doi:10.3390/healthcare10091778
36. Armah EO, Tuntufye HN. Antibiogram and diversity of extended-spectrum beta-lactamase genes in scavenging local chicken in Morogoro Municipality, Tanzania. Int J Curr Microbiol Appl Sci. 2020;9:2699–2709. doi:10.20546/ijcmas.2020.903.308
37. El-Gamal MI, Brahim I, Hisham N, et al. Recent updates of carbapenem antibiotics. Eur J Med Chem. 2017;131:185–195. doi:10.1016/j.ejmech.2017.03.022
38. Vannakovida C, Lampang KN, Chuammitri P, et al. Comparative occurrence and antibiogram of extended-spectrum β-lactamase-producing Escherichia coli among post-weaned calves and lactating cows from smallholder dairy farms in a parallel animal husbandry area. Vet World. 2021;14:1311. doi:10.14202/vetworld.2021.1311-1318
39. Ojdana D, Sieńko A, Sacha P, et al. Genetic basis of enzymatic resistance of E. coli to aminoglycosides. Adv Med Sci. 2018;63:9–13. doi:10.1016/j.advms.2017.05.004
40. Alyamani EJ, Khiyami AM, Booq RY, et al. The occurrence of ESBL-producing Escherichia coli carrying aminoglycoside resistance genes in urinary tract infections in Saudi Arabia. Ann Clin Microbiol Antimicrob. 2017;16:1–13. doi:10.1186/s12941-016-0177-6
41. Kettani Halabi M, Lahlou FA, Diawara I, et al. Antibiotic resistance pattern of extended spectrum beta lactamase producing Escherichia coli isolated from patients with urinary tract infection in Morocco. Front Cell Infect Microbiol. 2021;11:720701. doi:10.3389/fcimb.2021.720701
42. Somily AM, Habib HA, Absar MM, et al. ESBL-producing Escherichia coli and Klebsiella pneumoniae at a tertiary care hospital in Saudi Arabia. J Infect Dev Ctries. 2014;8:1129–1136. doi:10.3855/jidc.4292
43. Preena PG, Swaminathan TR, Kumar VJR, Singh ISB. Antimicrobial resistance in aquaculture: a crisis for concern. Biologia. 2020;75:1497–1517. doi:10.2478/s11756-020-00456-4
44. Mutuku C, Gazdag Z, Melegh S. Occurrence of antibiotics and bacterial resistance genes in wastewater: resistance mechanisms and antimicrobial resistance control approaches. World J Microbiol Biotechnol. 2022;38:152. doi:10.1007/s11274-022-03334-0
45. Sivakumar M, Abass G, Vivekanandhan R, et al. Extended-spectrum beta-lactamase (ESBL) producing and multidrug-resistant Escherichia coli in street foods: a public health concern. J Food Sci Technol. 2020;58:1247–1261. doi:10.1007/s13197-020-04634-9
46. Naziri Z, Derakhshandeh A, Borchaloee AS, Poormaleknia M, Azimzadeh N. Treatment failure in urinary tract infections: a warning witness for virulent multi-drug resistant ESBL-producing Escherichia coli. Infect Drug Resist. 2020;13:1839. doi:10.2147/IDR.S256131
47. Chai MH, Sukiman MZ, Jasmy N, et al. Molecular detection and antibiogram of ESBL-producing and carbapenem-resistant Escherichia coli from rabbit, swine, and poultry in Malaysia. Trop Anim Sci J. 2022;45:16–23. doi:10.5398/tasj.2022.45.1.16
48. Dheda K, Gumbo T, Maartens G, et al. The Lancet Respiratory Medicine Commission: 2019 update: epidemiology, pathogenesis, transmission, diagnosis, and management of multidrug-resistant and incurable tuberculosis. Lancet Respir Med. 2019;7:820–826. doi:10.1016/S2213-2600(19)30263-2
49. Wall BA, Mateus AL, Marshall L, et al. Drivers, Dynamics and Epidemiology of Antimicrobial Resistance in Animal Production. Food and Agriculture Organization of the United Nations; 2016.
50. Birgand G, Zahar J-R, Lucet J-C. Insight into the complex epidemiology of multidrug-resistant Enterobacteriaceae. Clin Infect Dis. 2018;66:494–496. doi:10.1093/cid/cix826
51. Aarestrup FM, Wegener HC, Collignon P. Resistance in bacteria of the food chain: epidemiology and control strategies. Expert Rev Anti Infect Ther. 2008;6:733–750. doi:10.1586/14787210.6.5.733
52. Haque KJ. Knowledge, attitude, and practices on antimicrobial use in broiler and layer farms at Cumilla District, Bangladesh. 2021.
53. Lim C, Takahashi E, Hongsuwan M, et al. Epidemiology and burden of multidrug-resistant bacterial infection in a developing country. Elife. 2016;5:e18082. doi:10.7554/eLife.18082
54. Boehmer T, Vogler AJ, Thomas A, et al. Phenotypic characterization and whole genome analysis of extended-spectrum beta-lactamase-producing bacteria isolated from dogs in Germany. PLoS One. 2018;13:e0206252. doi:10.1371/journal.pone.0206252
55. Landfried K, Barnidge E, Pithua P, et al. Antibiotic use on goat farms: an investigation of knowledge, attitudes, and behaviors of missouri goat farmers. Animals. 2018;8:198. doi:10.3390/ani8110198
56. Clement M, Olabisi M, David E, Issa M. Veterinary pharmaceuticals and antimicrobial resistance in developing countries. In: Veterinary Medicine and Pharmaceuticals. IntechOpen; 2019.
57. Manyi-Loh C, Mamphweli S, Meyer E, Okoh A. Antibiotic Use in Agriculture and Its Consequential Resistance in Environmental Sources: potential Public Health Implications. Mol AJ Synth Chem Nat Prod Chem. 2018;23:54.
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Extended-Spectrum Beta-Lactamases Producing Escherichia coli in South America: A Systematic Review with a One Health Perspective
Bastidas-Caldes C, Romero-Alvarez D, Valdez-Vélez V, Morales RD, Montalvo-Hernández A, Gomes-Dias C, Calvopiña M
Infection and Drug Resistance 2022, 15:5759-5779
Published Date: 30 September 2022