Back to Journals » Drug Design, Development and Therapy » Volume 17
Phase I, Single-Dose Study to Assess the Pharmacokinetics and Safety of Suramin in Healthy Chinese Volunteers
Authors Wu G, Zhou H, Lv D, Zheng R, Wu L, Yu S, Kai J, Xu N, Gu L, Hong N, Shentu J
Received 10 April 2023
Accepted for publication 30 June 2023
Published 11 July 2023 Volume 2023:17 Pages 2051—2061
DOI https://doi.org/10.2147/DDDT.S416325
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Anastasios Lymperopoulos
Guolan Wu,1– 3 Huili Zhou,1,2 Duo Lv,1,2 Ruling Zheng,4 Lihua Wu,1 Songxia Yu,1,2 Jiejing Kai,1,2 Nana Xu,1,2 Lie Gu,5 Nanfang Hong,5 Jianzhong Shentu1,2
1Department of Clinical Pharmacy, The First Affiliated Hospital, Zhejiang University School of Medicine, Hangzhou, People’s Republic of China; 2Zhejiang Provincial Key Laboratory for Drug Evaluation and Clinical Research, The First Affiliated Hospital, Zhejiang University School of Medicine, Hangzhou, People’s Republic of China; 3Polytechnic Institute, Zhejiang University, Hangzhou, People’s Republic of China; 4The Fifth Affiliated Hospital, College of Medicine, Guangzhou Medical University, Guangzhou, People’s Republic of China; 5Hainan Honz Pharmaceutical Co. Ltd, Haikou, Hainan, People’s Republic of China
Correspondence: Jianzhong Shentu, Email [email protected]
Purpose: Suramin is a multifunctional molecule with a wide range of potential applications, including parasitic and viral diseases, as well as cancer.
Methods: A double-blinded, randomized, placebo-controlled single ascending dose study was conducted to investigate the safety, tolerability, and pharmacokinetics of suramin in healthy Chinese volunteers. A total of 36 healthy subjects were enrolled. All doses of suramin sodium and placebo were administered as a 30-minute infusion. Blood and urine samples were collected at the designated time points for pharmacokinetic analysis. Safety was assessed by clinical examinations and adverse events.
Results: After a single dose, suramin maximum plasma concentration (Cmax) and area under the plasma concentration–time curve from time zero to the time of the last measurable concentration (AUClast) increased in a dose-proportional manner. The plasma half-life (t1/2) was dose-independent, average 48 days (range 28– 105 days). The cumulative percentages of the dose excreted in urine over 7 days were less than 4%. Suramin can be detected in urine samples for longer periods (more than 140 days following infusion). Suramin was generally well tolerated. Treatment-emergent adverse events (TEAEs) were generally mild in severity.
Conclusion: The PK and safety profiles of suramin in Chinese subjects indicated that 10 mg/kg or 15 mg/kg could be an appropriate dose in a future multiple-dose study.
Keywords: suramin, clinical pharmacokinetics, antiviral, safety, drug repurposing
Introduction
Suramin is a drug that has been used to treat both children and adults with African sleeping sickness and river blindness for over a century.1 It has also been shown to inhibit the replication of a variety of viruses, including enteroviruses, Zika virus, Chikungunya, Ebola viruses, and SARS-CoV-2.2–8 Suramin’s viral inhibition mechanisms are diverse, including inhibition of viral attachment, entry, and release from host cells, which is accomplished in part through interactions with viral capsid proteins.3–5,7–9 Until now, suramin was only tested in a few clinical trials on cancer patients and children with an autism spectrum disorder.9–16 Suramin’s effectiveness in treating viral illnesses has not recently been validated by clinical research. However, suramin is expected to find a surprising variety of repurposing applications, particularly in anti-virus disease.
Suramin has poor oral absorption while being widely distributed to tissues, kidneys, and protein. This drug’s volume of distribution was 31–46 liters, with 80% excreted via the kidney.11,17 Suramin has an extremely long half-life (t1/2) of 50 days or more, resulting in drug accumulation with repeated dosing. Suramin levels above 350 μg/mL may increase the frequency of neurotoxicity and coagulopathy.18–21 The use of intermittent dosing schedules demonstrated that maintaining plasma suramin levels between 100 and 300 μg/mL significantly reduced suramin toxicities without compromising antineoplastic activity in prostate cancer patients.14,21–23
In China, enterovirus 71 (EV71) is the major etiological agent of hand foot mouth disease (HFMD) that poses severe risks to children’s health.24 To date, there are no specific treatment drugs for EV71-associated HFMD. Due to suramin’s preclinical effect for the EV-71 virus, injected suramin sodium was developed by Hainan Honz Pharmaceutical Co. Ltd for the treatment of HFMD. The salt form can improve the water solubility of suramin. Its long half-life and low therapeutic index make it difficult to design a regiment that would rapidly achieve concentrations in the range associated with biological effects. In addition, its pharmacokinetics in the Chinese population is poorly understood.
The aims of the study were to evaluate the safety, tolerability, and PK profile of suramin after single-dose in adult healthy Chinese subjects for the first time. The adult PK data would be applicable to modeling the PK/PD relationship in children with HFMD and provide dosing guidelines for further clinical trials in adults or children.
Materials and Methods
The clinical protocol and informed consent were reviewed and approved by the ethics committee of the First Affiliated Hospital, School of Medicine, Zhejiang University (approval No. 2018-EC-292). Clinical procedures were conducted in the Phase I clinical trial unit of the First Affiliated Hospital, School of Medicine, Zhejiang University. The study (NCT 03804749) was conducted in accordance with the Declaration of Helsinki and followed the principles of Good Clinical Practice. Written informed consent was obtained for all subjects prior to participating in any study procedures.
Study Participants
All healthy volunteers, aged 18–45 years, body weight of 45–75 kg (female) and 50–75 kg (male), and body mass index values of 18–26 kg/m2, were eligible to participate in the study. Subjects were required to be in good health, as determined by the absence of clinically significant findings from medical history, electrocardiogram, clinical laboratory assessments, vital sign measurements, and physical exams. Baseline laboratory test values for kidney and liver functions had to be within normal limits. The study candidates matched with the exclusion criteria in the study protocol will be excluded such as a history of heart, liver, lung, kidney, respiratory, nervous, skeletal muscle, endocrine, digestive system diseases or other serious diseases; clinical drug allergy history or specific allergic disease history, especially those who are allergic to any ingredient used in the investigational product. Individuals who screened positive for hepatitis B virus, HCV, or HIV were ineligible. Volunteers were also excluded from the study if they used tobacco or nicotine-containing products within 3 months of study initiation and had used any medications, vitamins, or herbal supplements within 2 weeks before study drug administration. Additional exclusion criteria were consumption of any caffeine-containing foods or beverages within 48 h and any alcohol or alcohol-containing drinks. Female subjects with childbearing potential needed to have a negative serum pregnancy test and use at least one acceptable form of contraception. Males had to agree to practice a reliable form of contraception or abstinence.
Study Design
The study was a double-blind, placebo-controlled, single-dose study conducted on healthy volunteers. Thirty-six participants were randomized to administer either injected suramin sodium or placebo (Figure 1). Each of the three dose escalation cohorts consisted of 12 healthy subjects. In the three dose escalation cohorts, ten subjects/cohort received 10, 15, or 20 mg/kg of suramin, respectively, and two subjects/cohort received placebo (ratio 5:1). Randomization was completed using a simple randomization schedule generated by SAS 9.4 (SAS Institute Inc., Cary, NC, USA). Volunteers were enrolled sequentially and assigned a random number in each dose group. All doses of injected suramin sodium and placebo calculated on the basis of the volunteer’s body weight were dissolved in 100 mL of 0.9% sodium chloride solution and injected intravenously at a consistent rate (infusion time was 30 min). Suramin dose escalation was only conducted after reviewing inpatient safety data (day 1 to day 8) from the previous cohort. Unblinding occurred after all subjects within each dose cohort had completed Day 28 visit. The study duration for each subject receiving injected suramin sodium (screening period, administration, and follow-up) was approximately 154 days. The median time to complete the study for placebo-treated subjects was approximately 32 days after their administration.
 |
Figure 1 Study design. Placebo-treated subjects were followed for at least 28 days until unblinding permits in each dose group. PK sampling time was up to 140 days for suramin treatment cohorts to better characterize the terminal phase, given the long elimination half-life based on emerging data. |
Sample Size
The sample size was based on the number of subjects that were feasible to evaluate the safety and the pharmacokinetic profile of suramin and not on any statistical hypothesis. According to Technical Guidelines for Clinical Pharmacokinetics Research on Chemical Drug, 8–12 subjects are generally required for each dose group. Considering the dropout rate, the sample size planned for our study was about 12 cases in each dose level.
Biological Sample Collection
Plasma and urine concentrations of suramin were measured in this study. Venous blood samples were collected into K2EDTA tubes at different time points: 0 (prior to the infusion), 10 min (during the infusion), 20 min (during the infusion), 30 min (immediately following completion of the infusion), and 35 min, 45 min, 1 h, 2 h, 3h, 4 h, 8 h, 12 h, 24 h, 48 h (day 3), 72 h (day 4), 96 h (day 5), 120 h (day 6), 144 h (day 7), 168 h (day 8), 336 h (day 14), 672 h (day 28), 1344 h (day 56), 2016 h (day 84), 2688 h (day 112), 3360 h (day 140) after the start of the infusion. After centrifugation at 1700 g for 10 min, the supernatant of each sample was collected and stored at −80 °C until analysis. 24-h urine samples were collected daily from day 1 to day 7 for measurement of urine volume and suramin concentration. Spot urine samples were collected on day 14, 28, 56, 84, 112, and 140 to obtain the suramin excretion. Two subjects receiving placebo in each cohort were discontinued after unblinding and no more PK samples need collecting.
Bioanalytical Procedures
Plasma and urine samples were analyzed for suramin concentrations using validated, sensitive, and specific liquid chromatography tandem mass spectrometric methods. The lower limit of quantification for suramin was 1.0 μg/mL for plasma concentrations and 0.2 μg/mL for urine concentrations. The system comprised an LC-20AD™ (Shimadzu System, Shimadzu, Japan) coupled with a mass spectrometry (Qtrap 5500, AB SCIEX, USA) to determine the suramin concentration in plasma and urine. Chromatography was performed with an ACE 3 C18-AR, 50 × 2.1 mm, equipped with a Phenomenex SecurityGuard Standard C18, 4 × 3.0 mm, and the mobile phase was water with 100 mM amine acetate (PH 7.6) (A)-acetonitrile (B) at a flow rate of 0.6 mL/min. The gradient elution program: 0–1.0 minutes, 20%A/80%B; 1.0–2.0 minutes, 95%A/5%B; 2.1–4.0 minutes, 20%A/80%B. The quantification was performed using multiple reaction monitoring of the transitions m/z 647→382 for suramin and m/z 651.1→382 for suramin-d8 (IS).
For plasma samples, the between-day assay accuracy, expressed as percent relative error, for quality control (QC) concentrations ranged from −4.60% to 2.00% for the low, medium, high, and diluted QC samples. Assay precision, expressed as the between-day percent coefficient of variation (%CV) of the mean estimated concentrations of QC samples, was ≤2.95% for low (3 μg/mL), medium 1 (25 μg/mL), medium 2 (200 μg/mL), high (400 μg/mL) and diluted (2000 μg/mL) concentrations. For urine samples, the accuracy, intra- and inter-day precisions were all required not to exceed 15%.
Pharmacokinetic Assessments
Pharmacokinetic parameters were estimated using noncompartmental methods (Phoenix WinNonlin version 8.0, Pharsight Corporation, Princeton, New Jersey). Cmax and time to Cmax (Tmax) were obtained from the observed data. The AUC for plasma concentration versus time from 0 to the last measurable time point (AUC0–t) was calculated using the linear trapezoidal rule. The AUC from 0 to infinity (AUC0-∞) was calculated as AUC0-t + Clast/λz, where Clast is the last measurable concentration and λz is the slope of the log-linear regression of the terminal concentration data points. Drug elimination half-life (t1/2) was then calculated as ln2/λz. The apparent clearance (CL) was calculated as the ratio of dose to AUC0-∞. The apparent volume of distribution (V) was calculated as the ratio of clearance to λz. The amount of drug excreted into the urine from time zero to time 7 days (Ae0–7d) was determined for each single-dose pharmacokinetic group from the urine drug concentration–time data.
Safety Assessments
We evaluated the safety by periodic physical examinations, including vital signs, assessment of 12-lead ECGs (PR, QRS, QT, QTcB [Bazett’s formula]), clinical laboratory tests (complete blood count [CBC] with differential, prothrombin time [PT], partial thromboplastin time [PTT], and sodium, potassium, calcium, glucose, creatinine, blood urea nitrogen [BUN], albumin, protein, bilirubin, aspartate aminotransferase [AST], alanine aminotransferase [ALT], triglycerides, total cholesterol, low-density lipoprotein, high-density lipoprotein, and alkaline phosphate levels) at baseline and at various time points during the studies, and examined the AEs and use of concomitant medications. AEs were evaluated according to National Cancer Institute Common Terminology Criteria for Adverse Events (CTCAE, version 5.0) and were managed and recorded promptly by qualified investigators according to relevant regulations.
The dose-escalation termination criteria in a single ascending-dose study were determined by AEs. The dose escalation was only conducted after reviewing impatient safety data (day 1 to day 8) from the previous cohort. Dose escalation should be terminated when 1) AEs related to study drug of CTCAE Grade 2 and above occur in ≥50% subjects of one dose group; 2) AEs related to the study drug of CTCAE Grade 3 and above occur in ≥25% subjects of one dose group. 3) SAE related to the study drug occurs in at least one subject, with the exception of controlled infusion reactions.
Statistical Analyses
Statistical analysis was performed using SAS Software version 9.4 (SAS Institute, Cary, NC, USA) or using Phoenix WinNonlin. AEs were coded using the MedDRA dictionary version 20.1. They were classified by System Organ Class (SOC) and Preferred Term (PT). Treatment-emergent AEs (TEAEs) were summarized and listed.
Suramin concentrations vs time were plotted on linear and semi-logarithmic scales. Plasma concentrations and PK parameters were listed. Summary statistics of PK parameters including means, geometric means and coefficients of variation were presented for each dose. The normal distribution test was conducted using one-sample Kolmogorov–Smirnov test within-group in pharmacokinetic variables of suramin except Tmax (using nonparametric tests). Before performing statistical comparison, non-normally distributed parameters were logarithmically transformed.
Pharmacokinetic parameters were compared among dose levels using analysis of variance (ANOVA). To confirm whether Cmax and AUC for suramin were dose-proportional over the 10–20 mg/kg dose range in healthy Chinese subjects, log-transformed pharmacokinetic parameters AUC and Cmax were analyzed using the power model, PK = A×(Dose)β, where PK is the pharmacokinetic parameter, A is the intercept, and β is the dose-proportionality coefficient. A 95% CI for the dose-proportionality parameter β was then calculated. Note that a slope of 1 would correspond to perfect dose proportionality. Body weight corrected PK parameter values of both sexes were compared using independent samples t-test to evaluate gender difference. P < 0.05 was considered significant.
Results
Participant Demographics
In total, 113 healthy Chinese subjects were recruited for the study, of whom 36 were randomized. Thirty subjects received injected suramin sodium 10–20 mg/kg and 6 subjects received placebo. Two subjects (No.1007 in 10 mg/kg cohort and No.3006 in 20 mg/kg cohort) were lost to follow-up on day 84 and considered not to have completed the study. One female subject (No.2010) was withdrawn from the 15 mg/kg suramin-treated cohort on day 28 because of a pregnancy event. All subjects were included in the safety analysis, while 26 subjects treated with suramin sodium were included in the PK analysis.
Baseline demographic characteristics were generally comparable across treatment groups (Table 1).
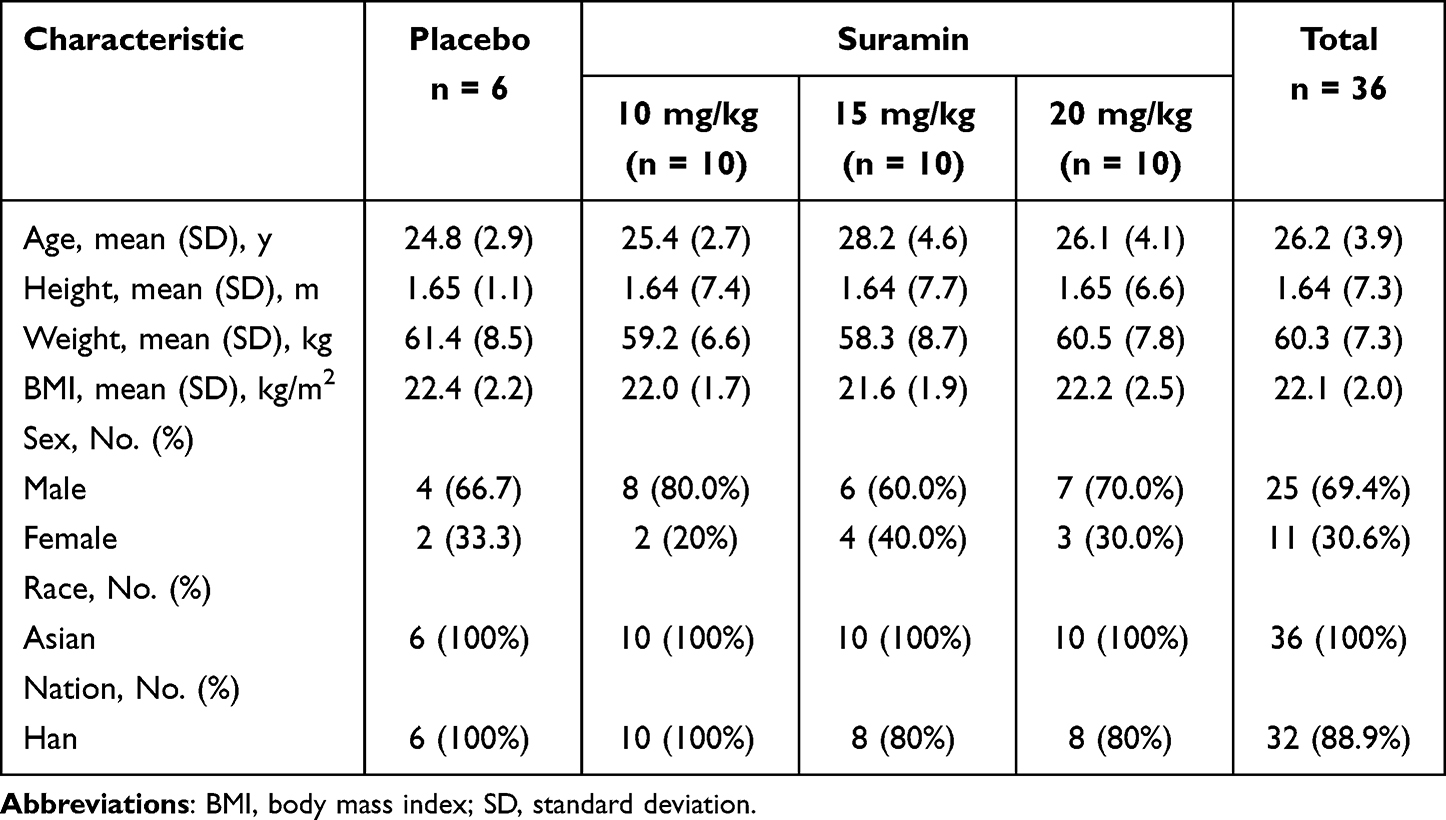 |
Table 1 Baseline Characteristics of the Randomized Study Population (n = 36) |
Pharmacokinetics Results
The mean plasma concentration–time profile of suramin following single IV infusion dosing of 10–20 mg/kg is shown in Figure 2. Pharmacokinetic parameters are enlisted in Table 2. The PK characteristics of suramin indicated by the parameters of Tmax, t1/2, V, and CL were similar in the three dose groups (P > 0.05). Plasma t1/2 was independent of the dose, averaging 48 days (range 28–105 days). V and CL ranged between 31.5 and 109 L and 18.7 and 51.5 mL/h, respectively, over the entire dose range. AUC0-140d was 13.7 ± 2.7, 24.2 ± 4.7, and 33.8 ±3.1 h·mg/mL for 10 mg/kg, 15 mg/kg, and 20 mg/kg dose groups, respectively. AUC0-∞ was 16.1 ± 4.5, 26.8 ± 5.2, and 38.5 ± 5.6 h·mg/mL for the three dose groups. Cmax was 161 ± 15.4, 254 ± 27.6, and 328 ± 21.2 μg/mL for the three dose groups. According to ANOVA, there was a dose-proportional increase in Cmax, AUC0-140d, and AUC0-∞ with the dose (P < 0.0001), with a slope of 1.040 (90% CI 0.908–1.171) for Cmax, 1.334 (90% CI 0.908–1.171) for AUC0-140d and 1.228 (90% CI 1.004–1.573) for AUC0-∞. This indicated that AUC parameters and Cmax were linearly related to dose within 10–20 mg/kg dose range. The dose linearity plots are demonstrated in Figure 3. Gender differences of pharmacokinetics were evaluated in 18 males and 8 females for single-dose study. There were no statistically significant differences in single-dose pharmacokinetic parameters between female and male subjects (P > 0.05, Table S1).
 |
Table 2 Pharmacokinetic Parameters of Suramin After Single-Dose Administration of Injected Suramin Sodium in Healthy Subjects |
 |
Figure 2 Mean concentration–time curve with standard deviation for suramin in healthy human subjects after a single dose. |
 |
Figure 3 Dose linearity plots of Cmax and AUC parameters in a single ascending-dose study. |
The rates of drug excreted 7 days after administration of the three doses were 3.95%, 3.57%, and 3.81%, respectively. In urine samples, suramin can be detected up to 140 days. The mean urine concentrations on day 140 were 1.22, 1.81, and 2.76 μg/mL after 10, 15, and 20 mg/kg doses, respectively.
Safety and Tolerability
A total of 58 clinical treatment related adverse events (TEAEs) were reported in 69.4% (25/36) of the randomized subjects, and eight clinical TEAEs were reported in 66.7% (4/6) of the placebo subjects. There were no deaths due to TEAEs. No subjects were withdrawn from the study due to drug-related TEAEs. The incidence of TEAEs by treatment group is shown in Table 3.
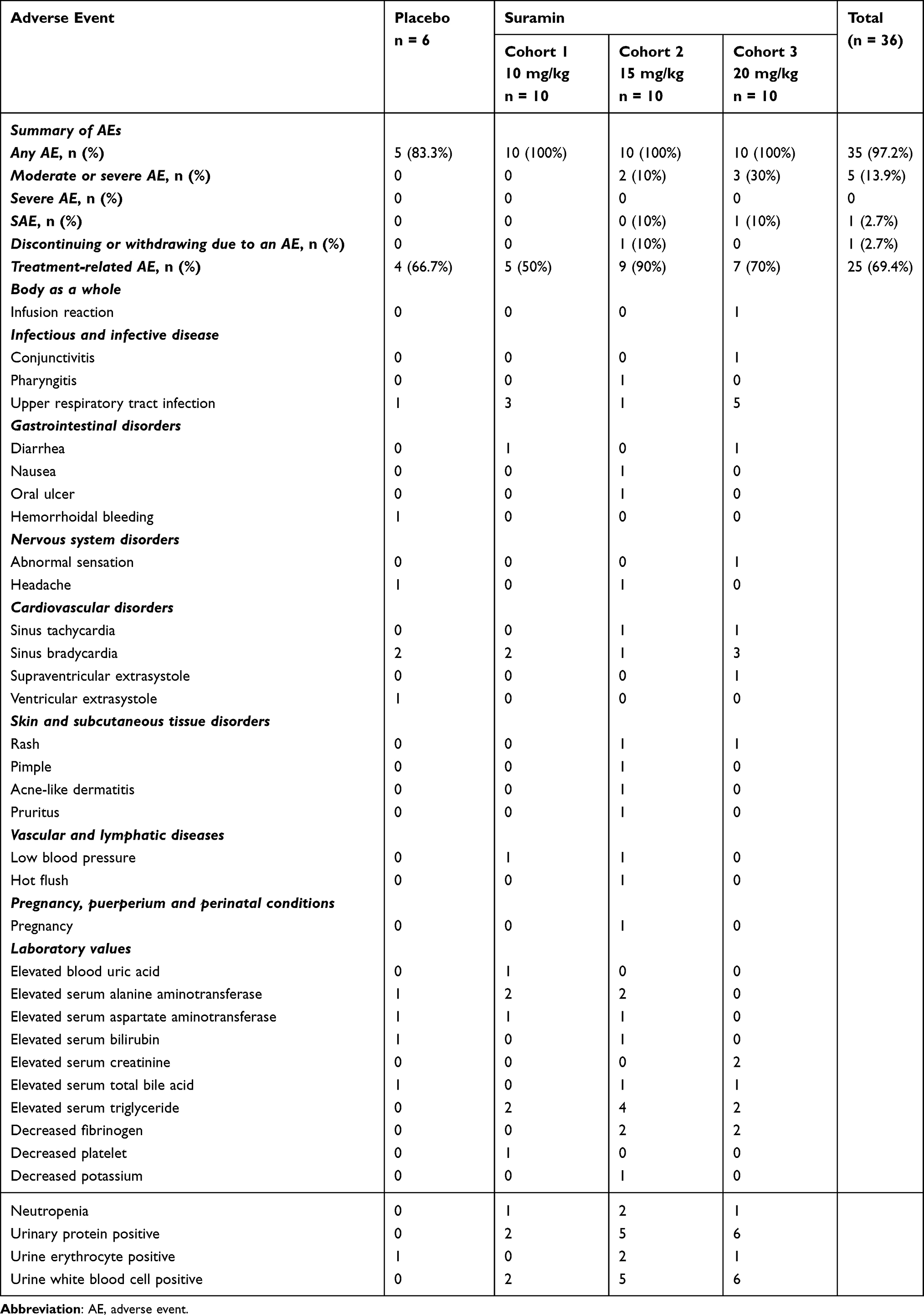 |
Table 3 Summary of Adverse Events |
The number (incidence) of subjects experiencing AEs for 10 mg/kg, 15 mg/kg, 20 mg/kg dose group and placebo group was 5 (83.3%), 10 (100%), 10 (100%) and 10 (100%), respectively. Among the reported AEs after suramin administration, 44 cases (19/30, 63.3%) were deemed to be related to study drug with CTCAE Grade 1. The most frequently reported laboratory abnormalities were positive urine protein tests (n = 12), increase in serum triglyceride (n = 6), increase in ALT (n = 4), positive urine blood tests (n = 3).
Throughout the study, one serious adverse event (infusion reaction) occurred in the 20 mg/kg dose group, which did not meet the protocol’s dose-escalation termination criteria. After 10 minutes of infusion at a rate of 40 mg/kg/h, the subject (No.3009) developed flushing, conjunctival hyperemia, and shortness of breath. At times, he was in mild abdominal pain with the following vital signs: heart rate 120 beats per minute, respiratory rate 20 breaths per min, blood pressure 117/71 mmHg, temperature 36.5°C, arterial oxygen saturation (SpO2) when breathing room air was 98%. The symptoms disappeared by themselves immediately after the infusion was interrupted. We resumed administration at 20 mg/kg/h (half the prior dose/rate) about 20 minutes later. He completed administration successfully at 9:51 AM but developed a fever at 10:25 AM with a temperature of 38.0°C, with the highest temperature reached being 39.7°C. The therapeutic measures, which including intravenous pulse of methylprednisolone, indomethacin, and rehydration support therapy, resulted in temperature normalization in 48 hours. Details of this adverse reaction and treatment process were reported to the ethics committee, and the adverse reactions were assessed as moderate in severity. The subject was followed up to 140 days and remained in the safety analysis set but was excluded from PK analysis due to protocol deviation.
All AEs in the study were resolved by last contact, except for 5 cases. Among the cases, serum triglyceride was increased in 1 case, fibrinogen was decreased in 1 case, urine protein was positive in 1 case, and serum creatine was slightly increased in 1 case.
Discussion
This project was a randomized, double-blind, placebo-controlled, dose-escalation, phase I study to determine the safety, tolerability, and PK profiles of suramin after administration of single IV doses in healthy Chinese adult subjects. Suramin was safe and well tolerated in our study, with no evidence of serious adverse events and no discontinued use because of drug-related TEAEs. Most reported TEAEs were mild or moderate and were spontaneously relieved without any treatment intervention.
The TEAEs possibly related to drug administration were skin and subcutaneous tissue disorders, gastrointestinal disorders, and significant changes in laboratory values, such as elevated activity of ALT and AST, as well as the appearance of urinary erythrocytes and protein. Among them, the frequency of urinary protein and white blood cell positivity increased with dose (20%, 50%, and 60%). Other TEAEs were considered accidental, as neither frequency nor severity increased with dose.
Suramin’s most common side effects include nephrotoxicity, hypersensitivity reactions, dermatitis, anemia, peripheral neuropathy, and bone marrow toxicity.10 In our study, we found infusion reactions, dermatologic disorders (rash, dermatitis, and pruritus), neutropenia, and increased ALT and AST levels, but the frequency is much lower. The reason for fewer AEs in our study is that only a single dose was administered, and the number of subjects enrolled in this phase I clinical trial was limited; further research in larger populations will provide a more precise safety profile of suramin. It was also demonstrated that slow infusion, along with the administration of antihistamines and corticosteroids, can control the infusion reaction.
Following a single 30-minute intravenous infusion of 10, 15, or 20 mg/kg injected suramin sodium, Cmax and AUC increased proportionally with suramin dose. The Cmax mean values were 160 μg/mL, 253 μg/mL, and 328 μg/mL, respectively. Previous studies suggested an increased incidence of neurotoxicity at suramin concentrations greater than 300 μg/mL.10 In the present study, the peaks on seven subjects in 20 mg/kg cohort were greater than 300 μg/mL. Then, we should choose a lower dose or prolonged infusion time for further trials to avoid such off-limit peaks. CL and V did not vary significantly with dosage. The elimination t1/2 proved to be independent of the dose, with values of 28–105 days, which was close to the values reported in previous studies.21 Suramin was eliminated in the kidney via slow urinary excretion; this observation suggests a need for dosage adjustment in patients with the most severe degrees of renal impairment. There are fewer data on the clinical pharmacokinetics of suramin in women. In the present study, there were no statistically significant differences in pharmacokinetic parameters between female and male subjects. However, its pharmacokinetics may vary between younger and older subjects, so further investigation of suramin pharmacokinetics was required for these different subgroups.
Suramin has been shown to prevent SARS-CoV-2 infection in cell culture since 2020, with half-maximal inhibition concentration (IC50) values in the low micromolar range.7,8 Suramin is a highly effective inhibitor of the SARS-CoV-2 RNA-dependent RNA polymerase (IC50, 0.26 μM)7 and SARS-CoV-2 3CLpro (IC50, 6.3 μM).25 Suramin provided full protection against SARS-CoV-2- induced cell death in Vero E6 cells and inhibited the virus with an EC50 of 20 μM,8 which is less than one-tenth of the maximum attainable level in human plasma. Due to its powerful influence in preclinical evidence and the PK findings from this study, we initiated a study of a 60-minute intravenous 15 mg/kg on day 1 and day 5 in China for coronavirus disease 2019 (COVID-19) patients. Based on the raw data from the current study, a three-compartment PK model adequately captured suramin pharmacokinetics in healthy individuals. Suramin concentrations in adult COVID-19 patients were found to be consistent with the PK model prediction (Figure S1). These findings will help future research into suramin as a possible therapy option for RNA virus infection, particularly enterovirus 71.26 Furthermore, we sought to recreate concentrations in children aged 5–14 years after a single intravenous infusion of 20 mg/kg suramin for 1 hour using the PK model. Table S2 indicated that anticipated plasma concentrations in children were comparable to observed data.16 As discussed above, we propose a day 1, day 3 or day 1, day 5 dosing regimen, a prolonged infusion time (over 60 min), as well as a lower starting dosage at 10 mg/kg of suramin for the multiple-dose study in healthy volunteers or patients with RNA virus infection.
This study had some limitations that should be considered. First, although a modest number of subjects per treatment group are usually acceptable for Phase I trial, the sample size of the present study was relatively small. Second, all participants were young, healthy Chinese volunteers; the results cannot be extrapolated to an older population or children with infection. Third, fewer AEs in our study lie in the fact that only a single dose was taken, and further evaluation in larger populations will provide a more exact safety profile of suramin.
Conclusion
In conclusion, following 30-minute infusion administration, suramin was relatively well tolerated and demonstrated a large apparent distribution volume and extremely long elimination half-life. These characteristics were similar to those observed in patients. Suramin was generally safe and well tolerated in healthy Chinese volunteers. The PK and safety profiles of suramin in Chinese subjects indicated that 10 mg/kg or 15 mg/kg could be an appropriate dose in a future multiple-dose study.
Data Sharing Statement
The original contributions presented in the study are included in the article, and further inquiries can be directed to the corresponding author.
Acknowledgments
The authors thank the clinical site staff for their contributions. The authors also would like to thank Dr. Y.Y. Jiang for her assistance in safety monitoring. The author expressed gratitude to nurses Y.L. Yang and Y. Yu for their assistance with drug allocation and blindness maintenance. The authors thank Jiangsu Value Pharmaceutical Services CO., Ltd for the bioanalytical analysis. The authors would also like to thank the contributions from the study sponsor Hainan Honz Pharmaceutical Co., Ltd.
Funding
This work was funded by Hainan Honz Pharmaceutical Co., Ltd. This work was also supported by Zhejiang Provincial Science and Technology Department Key R & D Plan Emergency Project (No. 2020c03123-8).
Disclosure
Lie Gu and Nanfang Hong are employed by Hainan Honz Pharmaceutical Co., Ltd. who funded the study. Jianzhong Shentu, as the principal investigator, received funding from Hainan Honz Pharmaceutical Co., Ltd. All other authors declare no competing interests.
References
1. Brun R, Blum J, Chappuis F, Burri C. Human African trypanosomiasis. Lancet. 2010;375(9709):148–159. doi:10.1016/S0140-6736(09)60829-1
2. Ren P, Zou G, Bailly B, et al. The approved pediatric drug suramin identified as a clinical candidate for the treatment of EV71 infection-suramin inhibits EV71 infection in vitro and in vivo. Emerg Microbes Infect. 2014;3(9):e62. doi:10.1038/emi.2014.60
3. Albulescu IC, Kovacikova K, Tas A, Snijder EJ, van Hemert MJ. Suramin inhibits Zika virus replication by interfering with virus attachment and release of infectious particles. Antiviral Res. 2017;143:230–236. doi:10.1016/j.antiviral.2017.04.016
4. Albulescu IC, van Hoolwerff M, Wolters LA, et al. Suramin inhibits chikungunya virus replication through multiple mechanisms. Antiviral Res. 2015;121:39–46. doi:10.1016/j.antiviral.2015.06.013
5. Albulescu IC, White-Scholten L, Tas A, et al. Suramin inhibits chikungunya virus replication by interacting with virions and blocking the early steps of infection. Viruses. 2020;12(3):314. doi:10.3390/v12030314
6. Henss L, Beck S, Weidner T, et al. Suramin is a potent inhibitor of Chikungunya and Ebola virus cell entry. Virol J. 2016;13(1):149. doi:10.1186/s12985-016-0607-2
7. Yin W, Luan X, Li Z, et al. Structural basis for inhibition of the SARS-CoV-2 RNA polymerase by suramin. Nat Struct Mol Biol. 2021;28(3):319–325. doi:10.1038/s41594-021-00570-0
8. Salgado-Benvindo C, Thaler M, Tas A, et al. Suramin inhibits SARS-CoV-2 infection in cell culture by interfering with early steps of the replication cycle. Antimicrob Agents Chemother. 2020;64(8). doi:10.1128/AAC.00900-20
9. Wiedemar N, Hauser DA, Mäser P. 100 Years of Suramin. Antimicrob Agents Chemother. 2020;64(3). doi:10.1128/AAC.01168-19
10. Ryan C, Vokes E, Vogelzang N, Janisch L, Kobayashi K, Ratain M. A phase I study of suramin with once- or twice-monthly dosing in patients with advanced cancer. Cancer Chemother Pharmacol. 2002;50(1):1–5. doi:10.1007/s00280-002-0458-y
11. Kaur M, Reed E, Sartor O, Dahut W, Figg WD. Suramin’s development: what did we learn? Invest New Drugs. 2002;20(2):209–219. doi:10.1023/a:1015666024386
12. Small EJ, Meyer M, Marshall ME, et al. Suramin therapy for patients with symptomatic hormone-refractory prostate cancer: results of a randomized Phase III trial comparing suramin plus hydrocortisone to placebo plus hydrocortisone. J Clin Oncol. 2000;18(7):1440–1450. doi:10.1200/JCO.2000.18.7.1440
13. Garcia-Schurmann JM, Schulze H, Haupt G, et al. Suramin treatment in hormone- and chemotherapy-refractory prostate cancer. Urology. 1999;53(3):535–541. doi:10.1016/s0090-4295(98)00544-5
14. Eisenberger MA, Sinibaldi VJ, Reyno LM, et al. Phase I and clinical evaluation of a pharmacologically guided regimen of suramin in patients with hormone-refractory prostate cancer. J Clin Oncol. 1995;13(9):2174–2186. doi:10.1200/JCO.1995.13.9.2174
15. Grossman SA, Phuphanich S, Lesser G, et al. Toxicity, efficacy, and pharmacology of suramin in adults with recurrent high-grade gliomas. J Clin Oncol. 2001;19(13):3260–3266. doi:10.1200/JCO.2001.19.13.3260
16. Naviaux RK, Curtis B, Li K, et al. Low-dose suramin in autism spectrum disorder: a small, phase I/II, randomized clinical trial. Ann Clin Transl Neurol. 2017;4(7):491–505. doi:10.1002/acn3.424
17. Kobayashi K, Vokes EE, Vogelzang NJ, et al. Phase I study of suramin given by intermittent infusion without adaptive control in patients with advanced cancer. J Clin Oncol. 1995;13(9):2196–2207. doi:10.1200/JCO.1995.13.9.2196
18. Stein CA, LaRocca RV, Thomas R, McAtee N, Myers CE. Suramin: an anticancer drug with a unique mechanism of action. J Clin Oncol. 1989;7(4):499–508. doi:10.1200/JCO.1989.7.4.499
19. La Rocca RV, Meer J, Gilliatt RW, et al. Suramin-induced polyneuropathy. Neurology. 1990;40(6):954–960. doi:10.1212/wnl.40.6.954
20. Horne MK, Stein CA, La Rocca RV, Myers CE. Circulating glycosaminoglycan anticoagulants associated with suramin treatment. Blood. 1988;71(2):273–279.
21. Eisenberger MA, Reyno LM. Suramin. Cancer Treat Rev. 1994;20(3):259–273. doi:10.1016/0305-7372(94)90003-5
22. Scher HI, Jodrell DI, Iversen JM, et al. Use of adaptive control with feedback to individualize suramin dosing. Cancer Res. 1992;52(1):64–70.
23. Jodrell DI, Reyno LM, Sridhara R, et al. Suramin: development of a population pharmacokinetic model and its use with intermittent short infusions to control plasma drug concentration in patients with prostate cancer. J Clin Oncol. 1994;12(1):166–175. doi:10.1200/JCO.1994.12.1.166
24. Ye L, Chen J, Fang T, et al. Vaccination coverage estimates and utilization patterns of inactivated enterovirus 71 vaccine post vaccine introduction in Ningbo, China. BMC Public Health. 2021;21(1):1118. doi:10.1186/s12889-021-11198-6
25. Eberle RJ, Olivier DS, Amaral MS, et al. The repurposed drugs suramin and quinacrine cooperatively inhibit SARS-CoV-2 3CL(pro) in vitro. Viruses. 2021;13(5):873. doi:10.3390/v13050873
26. Wang Y, Qing J, Sun Y, Rao Z. Suramin inhibits EV71 infection. Antiviral Res. 2014;103:1–6. doi:10.1016/j.antiviral.2013.12.008
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.