Back to Journals » Patient Related Outcome Measures » Volume 12
Pharmacotherapy Pattern and Treatment Outcomes of Stroke Patients Admitted to Jimma University Medical Center, Ethiopia
Authors Beyene N, Fanta K ![]() , Tatiparthi R
, Tatiparthi R ![]()
Received 22 February 2021
Accepted for publication 22 July 2021
Published 7 August 2021 Volume 2021:12 Pages 267—275
DOI https://doi.org/10.2147/PROM.S307291
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Robert Howland
Nigatu Beyene,1 Korinan Fanta,2 Ramanjireddy Tatiparthi3
1School of Pharmacy, Institute of Health, Jimma University, Jimma, Oromia, Ethiopia; 2Department of Clinical Pharmacy, Institute of Health, Jimma University, Jimma, Oromia, Ethiopia; 3Department of Pharmaceutics, Institute of Health, Jimma University, Jimma, Oromia, Ethiopia
Correspondence: Ramanjireddy Tatiparthi
Department of Pharmaceutics, Institute of Health, Jimma University, P.O.Box: 378, Jimma, Ethiopia
Tel +251931977170
Fax +251576617980
Email [email protected]
Korinan Fanta
Department of Clinical Pharmacy, Institute of Health, Jimma University, P.O.Box: 378, Jimma, Ethiopia
Tel +251911598485
Fax +251576617980
Email [email protected]
Background: Despite the fact that stroke has been reported as one of the top three leading causes of death and morbidity in Ethiopia, there are limited data regarding the management of stroke and clinical outcomes. Hence, the present study aimed to evaluate the pharmacotherapy of stroke and factors associated with poor treatment outcomes.
Methods: A retrospective cross-sectional study was conducted at Jimma University Medical Center (JUMC) among adult stroke patients managed from 2014 to 2017. Clinical characteristics, treatment, and outcomes data were analyzed by using SPSS version 21. Multivariable logistic regression was performed to identify the predictors of poor treatment outcomes. Two-sided P < 0.05 was accepted as statistically significant.
Results: A total of 153 illegible patient cases were included in this study. The majority, 111 (72.5%), were male and the mean age of the patients was 57± 13.7 years. Among 153 stroke patients, 112 (73.2%) patients presented with ischemic stroke. Aspirin and statins (78.6%) were the most commonly used treatment among ischemic stroke patients, whereas enalapril was used in about (43%) of stroke patients to treat high blood pressure. About 61 (40%) stroke patients had poor treatment outcomes; of this, 36 (23.5%) died in hospital. Older age (AOR = 1.034; 95% CI: 1.003– 1.069), history of heart failure (AOR = 4.26; 95% CI: 1.58– 11.48), loss of consciousness diabetes (AOR = 3.05 95% CI: 1.25– 7.44), and aspiration pneumonia (AOR = 5.94; 95% CI: 2.46– 14.32) were significantly associated with poor treatment outcomes.
Conclusion: Overall, treatment of stroke patients was sub-optimal and almost half of the patients had poor treatment outcomes. Availing of thrombolytic therapy, devising appropriate preventive measures of risk factors (hypertension), and decreasing preventable complication such as aspiration pneumonia could improve patient outcomes.
Keywords: stroke, poor outcome, treatment, resource limited-setting, Ethiopia
Introduction
Stroke is referred to as a focal or global neurological disorder as a result of disruption of cerebral blood flow lasting greater than 24 h and resulting in mortality in the absence of other causes.1 Stroke is the second most common cause of death next to heart disease and it is the leading cause of persistent disability worldwide.2,3 Despite the fact that stroke mortality and disability-adjusted life-years (DALY) rates have shown a downward trend since 1990, the absolute number of stroke deaths, number of patients remaining disabled, and new stroke cases have risen remarkably.3 About 70% of stroke cases worldwide and 87% of stroke-related mortality and DALY occur in low- and middle-income countries (LMIC).4 Although the number of total stroke deaths among younger adults in developed countries was declined, absolute numbers of stroke deaths among younger adults in LMIC were significantly increasing.5
It is highly recommended that patients suspected of acute stroke should undergo computed tomography (CT) scan on admission to the hospital to identify stroke subtypes and guide management decisions.6 However, in a resource-limited setting, access and affordability of a CT-scan is difficult and physicians depend on history and signs and symptoms for management without identifying the specific type of stroke.7 This shortcoming hinders the acute management of stroke and plays a significant role in poor treatment outcomes of stroke.
Guidelines for the management of acute stroke advocate the use of tissue plasminogen activator (tPA), aspirins, anticoagulants (heparins or warfarin), antihypertensive medications, and lipid-lowering agents (statins) for the management of ischemic stroke.6,8,9 For hemorrhagic stroke guidelines recommend the use of osmotherapy, neuro-protection and neuro-restoration therapy, neuromuscular relaxants, and antihypertensive (calcium channel blockers) based on disease and patient-specific factors.10 However, it is challenging to apply those recommendations in resource-limited settings such as Ethiopia where there is limited access to neuroimaging and fibrinolytic therapy.11
In LMIC, the number of patients with acute stroke receiving recombinant-tPA (r-tPA) is very low. This is mostly due to prolonged pre-hospital delay, economic reasons, and lack of CT-scan capable centers and experienced physicians.12 Even if thrombolytic drugs are available low awareness of stroke symptoms by society and prolonged pre-hospital delay exclude most stroke patients from receiving r-tPA.13,14 This is due to the fact that fibrinolytic therapy has been proven to be beneficial if administered within 4.5 h after the onset of an ischemic stroke.15 Yet patients with large vessel occlusion will benefit from thrombolytic therapy beyond 6 h and up to 24 h since stroke onset.15,16 Initiation of aspirin in all patients presenting with acute stroke of undetermined etiology due to lack of neuroimaging (in a poor setting) resulted in a good prognosis at hospital discharge.4
Regarding Ethiopia, stroke is becoming one of the most common reasons for healthcare visits and it is a serious public health issue.17,18 On top of the increasing burden of stroke in the country, the prognosis of stroke patients was extremely poor.19,20 This is mostly due to a lack of important medications such as r-tPA and excessively prolonged pre-hospital delay.20,21 As a result stroke patients often receive sub-standard in-hospital management and are discharged from healthcare facilities without linking with rehabilitation centers. Despite the fact that stroke has been reported as one of the top three leading causes of death and morbidity in Ethiopia, there is limited data regarding the pharmacotherapy of stroke, and most of the studies were focused on clinical characteristics and risk factors of stroke.20 Hence, the present study is aimed at evaluating the pharmacotherapy of stroke and factors associated with poor treatment outcomes.
Methods and Materials
Study Design and Setting
A retrospective chart review of stroke cases managed at Jimma University Medical Center (JUMC), southwest Ethiopia was conducted from February 2014 to March 2017. JUMC is a public hospital that serves as a referral center for the southwestern part of the country and it serves more than 15,000,000 catchment population. It provides services for approximately 15,000 inpatient and 160,000 outpatient attendants, 11,000 emergency cases and 4500 deliveries in a year for clients coming to the hospital. The hospital has a stroke unit under the general medical ward. Currently, the hospital provides neuroimaging services with CT-scans and magnetic resonance imaging (MRI) although this service was not available during the data collection period of this study. In addition, there are no thrombolytic medications and endovascular treatment (thrombectomy) in the hospital.
Study Populations
The World Health Organization’s (WHO) definition of stroke as
A rapidly developed sign of focal or global impairment of cerebral functions, lasting longer than 24 h (or leading to death) without apparent cases other than vascular origin
was used for the diagnosis of stroke.22 Based on this definition, all adult stroke patients above 18 years having either a clinical diagnosis of stroke (without neuro-imaging but, treated as hemorrhagic or ischemic stroke) or confirmed diagnosis of stroke with CT-scan were included. Stroke cases (49 cases) with incomplete medical records (not including a patient demography, left against medical advice, and unidentified stroke sub-type clinically or by neuro-imaging), and patients with a diagnosis of transient ischemic attack or hematoma were excluded from this study.
Outcome and Validating Methods
Discharge treatment outcome was categorized into good treatment outcome or poor treatment outcome based on the treating physician's discharge summary notes or a record of physical disability measurement using the modified Rankin scale (mRs). Good treatment outcome/improvements were considered if a patient was discharged without significant disability (able to carry out all pre-stroke activities without assistance from other individuals) or a record of mRs ≤ 2. A poor treatment outcome was defined as a patient discharged with moderate to severe disability (bedridden, incontinent, requires continuous care or an mRs score = 3–5) or expired during their hospital stay (mRs score=6). Duration of hospital stay was calculated as a time gap between admission to JUMC until discharge or death (in hospital).
Data Collection Tool and Quality Management
The data collection tool was adapted after reviewing relevant literature in similar areas. A semi-structured questionnaire was developed to abstract data from eligible patient’s medical records. The data collection tool contains five parts (demographic characteristics, key medical history, clinical presentations, management, and in-hospital events). Data collection was conducted by two trained nurses. The data collection tool was cross-checked with patient medical charts to modify contents according to routine practice in the hospital. A pre-test was performed before initiating data collection on 5% of the sample population and relevant modifications were made accordingly.
Statistical Analysis
Data analysis was carried out by using a statistical package for social science (SPSS) version 20 (IBM, Armonk, NY, USA). Descriptive statistics such as proportions, means, and standard deviations were used to describe the socio-demographic characteristics and clinical findings between stroke subtypes. Categorical variables were compared by using the chi-square test or Fisher’s exact test and continuous variables were compared by using Student’s t-test. Variables that showed p-value < 0.25 on binary logistic regression analysis were considered for multivariate analysis. Multivariable logistic regression was used to determine independent predictors of in-hospital poor clinical outcomes. Confidence interval which does not contain 1 and predictors with probability value less than 0.05 was considered statistically significant.
Ethical Consideration
The present study protocol was approved by the Institutional Review Board (IRB) of Jimma University, Institute of Health before initiating data collection. A letter of the permission was obtained from responsible bodies of JUMC to abstract data from patient’s medical records. To maintain confidentiality all patient data were recorded by using codes and avoiding any identifier such as patient name and contact address.
Results
Baseline Clinical Characteristics
Among a total of 153 stroke patients included in this study, 111 (72.5%) were male and the mean age of the patients was 57.3±13.7 years. More than half of the patients, 65 (58%), were from rural areas and about one in five were smokers. Alcohol use was more common among hemorrhagic stroke patients compared to those who presented with ischemic stroke.
Regarding co-morbid diseases, hypertension 64 (41.8%) was the most common risk factor identified among enrolled stroke cases. Other common risk factors identified were atrial fibrillation 35 (22.9%), diabetes mellitus 34 (22.2%), and a history of heart failure 31 (20.3%). Other less prevalent co-morbid conditions were chronic kidney disease 15 (9.8%) and coronary heart disease 12 (7.8%), and a previous history of stroke 10 (6.5%) (Table 1).
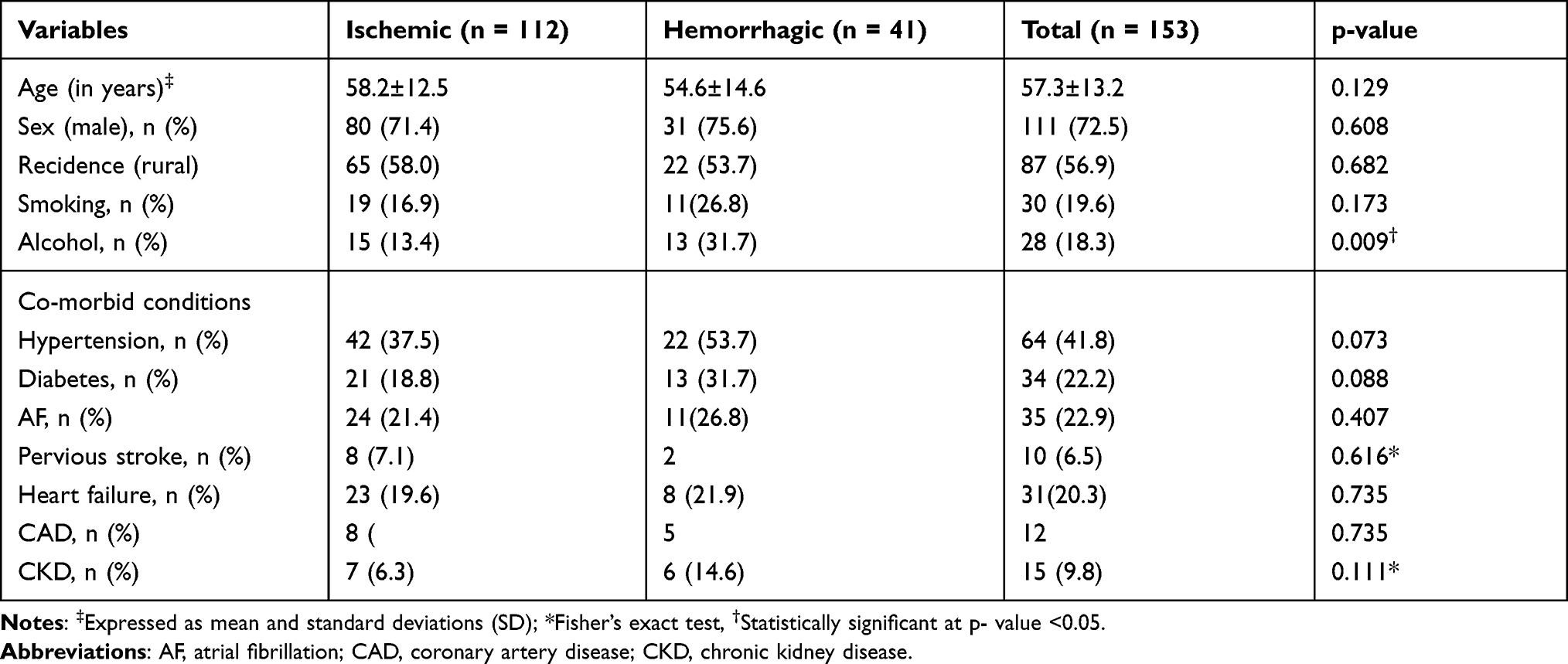 |
Table 1 Demographic Characteristics and Common Co-morbid Conditions Among Adult Stroke Patients Admitted to JUMC, Ethiopia |
Clinical Presentation and In-Hospital Complications
The majority of stroke patients presented with hemiparesis/hemiplegia, 83 (54.21%), followed by aphasia, 62 (40.5%), and headache, 60 (39.2%). Ischemic stroke patients were more likely to present with hemiparesis than hemorrhagic stroke patients (p = 0.008). Whereas, headache (p = 0.010) and a decreased level of consciousness (p = 0.006) were more common among hemorrhagic stroke patients. (Table 2).
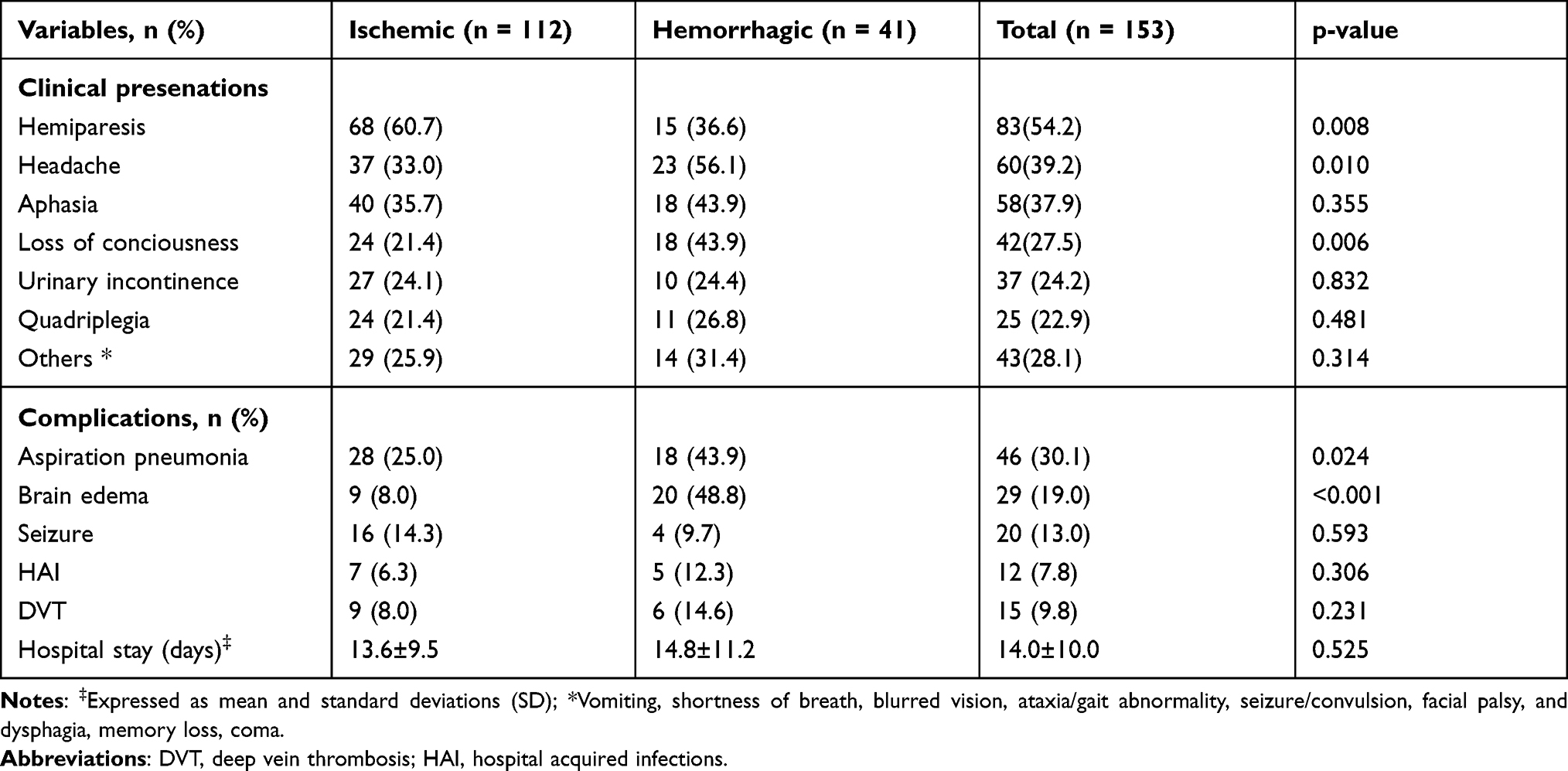 |
Table 2 Presentations and In-hospital Complications Among Adult Stroke Patients Admitted to JUMC, Ethiopia |
A common complication that developed during hospital stay was aspiration pneumonia which occurred in about 30% of stroke patients. Brain edema (increased intracranial pressure) was the most common neurological complication detected in about 19% of the patients. Another neurological complication recorded during hospitalization was seizure which occurred in 13% of stroke patients. Aspiration pneumonia and brain edema had a statistically significant association with hemorrhagic stroke compared to ischemic stroke (p-value < 0.001 and p-value = 0.024 respectively). There was no significant association between other complications such as seizure, deep vein thrombosis, hospital acquired infections, and heart failure with stroke subtypes. The mean hospital stay was 14±10 days (Table 2).
Stroke Management
During hospitalization the most commonly used antiplatelet and lip-lowering agents were aspirin and atorvastatin which were administered in about 44% of the patients. A small number of hemorrhagic stroke patients (5) also received antiplatelets before identifying the stroke subtypes by CT-scanner. The most commonly used antihypertensive medication among stroke patients was enalapril, which was used in about 43%, followed by hydrochlorothiazide, which was given to around 27% of stroke patients. Other concomitant medications used for management of stroke complications and comorbid conditions were antibiotics (ceftriaxone and metronidazole) in 35.3% of hospitalized stroke patients, mainly for treatment of aspiration pneumonia and other hospital-acquired infections. Similarly, phenytoin was used in 14.4%, anti-pain 23%, and antidiabetes was used in 22% of admitted stroke patients (Table 3). None of the patients had received tPA during hospital admission because of the unavailability of the medications and prolonged pre-hospital delay.
 |
Table 3 Medications Administered During Hospital Stay Among Stroke Patients |
Treatment Outcomes and Associated Factors
Among 153 stroke patients, about 117 (76.5%) were discharged alive from the hospital, and 36 (23.5%) died during a hospital stay. From those patients who were discharged alive 25 (21.4%) were discharged with a significant disability. Overall 61 (40%) of the patients had poor treatment outcomes while 92 (60%) were discharged with improvement and without any significant disability.
Variables with a p-value < 0.25 on bivariate logistic regression analysis were considered as a candidate for multivariable logistic regression analysis. Accordingly, sociodemographic characteristics (age, sex, and residence), smoking, alcohol, key medical history (hypertension, diabetes, atrial fibrillation, heart failure, and stroke), stroke subtypes, and duration of hospital stay were included in the final multivariate logistic regression. Upon multivariable analysis older age (adjusted odd ratio (HR) = 1.034, 95% confidence interval (CI) =1.003–1.069), history of heart failure (AOR = 4.26, 95% CI = 1.58–11.48), loss of consciousness diabetes (AOR = 3.05 95% CI = 1.25–7.44), and aspiration pneumonia (AOR = 5.94 95% CI = 2.46–14.32) were significantly associated with poor treatment outcomes (Table 4).
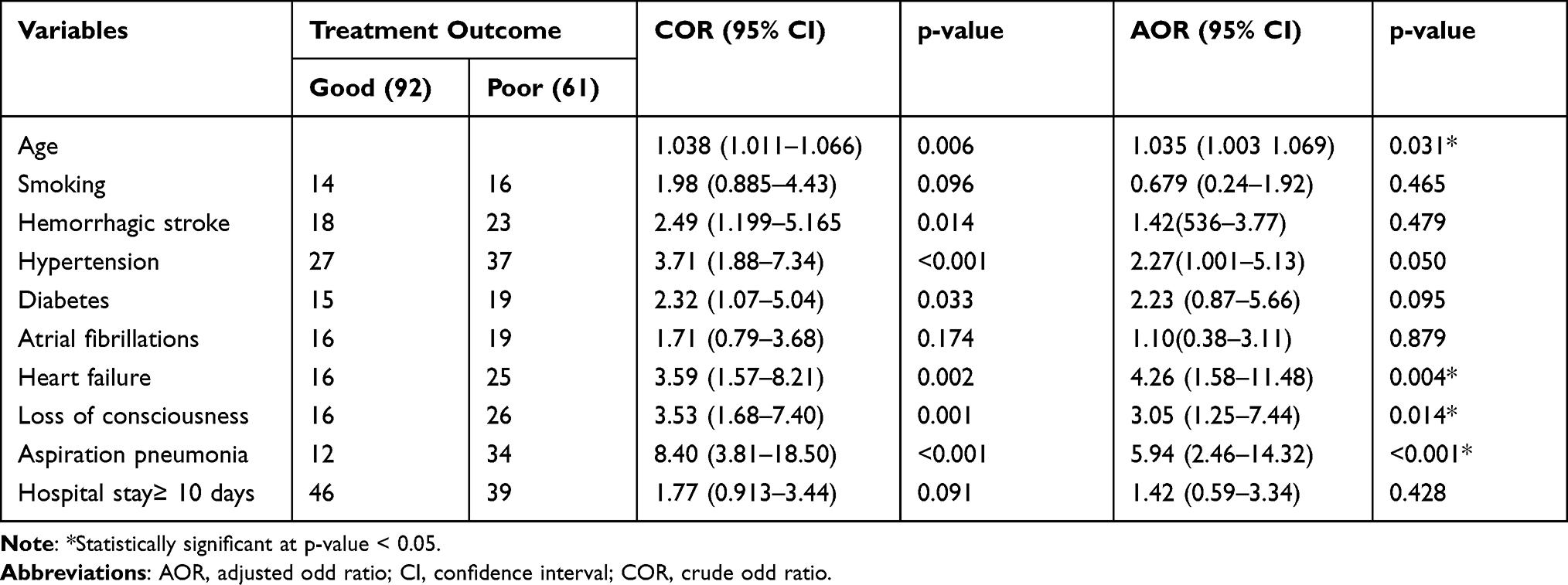 |
Table 4 Predictors of Poor Treatment Outcomes Among Adult Stroke Patients Admitted to JUMC, Ethiopa |
Discussion
A three years retrospective analysis of stroke cases on pharmacotherapy patterns and treatment outcomes among adult patients admitted to the stroke unit of JUMC was carried out. The result of the present study indicated that stroke cases were more common in males than females. The finding of this study also indicates that stroke occurs a decade earlier in Ethiopia compared to Western data. The majority of stroke patients presented with ischemic stroke compared to hemorrhagic stroke. The most common risk factor identified in the present study was high pretension. Antiplatelets (aspirin) and lipid-lowering agents (statins) were the most commonly used medications among ischemic stroke patients. ACEIs (enalapril) were the most commonly used antihypertensive medication among hypertensive stroke patients. None of the study patients received thrombolytic medications due to the unavailability of the medications. About 40% of stroke patients had poor treatment outcomes. Older age, altered level of consciousness on admission, comorbid heart failure, and complication with aspiration pneumonia were significantly associated with poor treatment outcome.
Ischemic stroke was the most common stroke subtype diagnosed in the present study. This finding is in line with several prior studies which reported that ischemic stroke was more prevalent than hemorrhagic strokes.13,18,19 On the other hand, there are studies from Ethiopia that reported equal prevalence of both stroke subtypes or high prevalence of hemorrhagic stroke.23–25 This discrepancy could be due to differences in stroke diagnosis (clinical vs neuroimaging), population-level socio-economics and risk factors. Despite the fact that ischemic stroke is still the commonest form of stroke presentation in sub-Saharan Africa, the prevalence of hemorrhagic stroke is increasing and it is associated with a high risk of mortality.26,27 This difference could be a result of differences in risk factors (such as the high prevalence of hypertension), environmental factors, study design (community vs facility-based), and clinical diagnosis of stroke in most sub-Saharan Africa.
The most common comorbid disease identified among stroke cases in the present study was hypertension (42%). This result was comparable to other studies which showed that hypertension is the common risk factor for stroke worldwide.20,28,29 In sub-Saharan Africa, hypertension is still underdiagnosed or poorly controlled among those who are on treatments which further contribute to poor treatment outcomes in stroke patients.30 This trend might be due to low awareness, limited access to healthcare, and a lack of a healthy lifestyle. Preventing, timely diagnosing, and treating hypertension as well as promoting public awareness can help to decrease the burden of cerebrovascular disease.
The outcome of stroke management depends on how fast the treatment is initiated, the earlier the treatment is initiated then the better the outcome.6 Although IV tPA is recommended in all eligible acute stroke patients presented within 4.5 hours of last known normal15 none of our study participants received thrombolytic medications due to a lack of coordinated emergency medical service and unavailability of tPA. In the present study, antiplatelet (aspirin) in combination with lipid-lowering agents (statins) were the most commonly administered medications during hospitalization. This finding is consistent with prior studies which reported that antiplatelet and lipid-lowering agents were the commonly prescribed medications among hospitalized stroke patients.11,24 ACEIs were the most commonly used antihypertensive medications among ischemic stroke and hemorrhagic stroke patients. This result is consistent with the study conducted by Fikadu et al11 in Ethiopia which also reported ACEIs as the commonest antihypertensive medications used among acute stroke patients.
About 40% of stroke patients had poor treatment outcomes (died in-hospital or discharged with significant disability). This finding was low compared to studies done in Ethiopia which reported that 55–65.4% of stroke patients had poor treatment outcomes.19,21,31 This difference might be due to due to differences in study design, stroke diagnosis (clinical vs brain imaging), standard of care, and prevalence of in-hospital complications.
In the present study, older age, altered level of consciousness on admission, comorbid heart failure, and complication with aspiration pneumonia significantly associated with poor treatment outcomes. Previous studies also indicated that advanced age, presence of comorbidity, and complications (aspiration pneumonia) were significantly associated with a poor prognosis.32–35 However, a study done by Fikadu et al in Ethiopia showed that level of education and duration of hospital stay was an independent predictor of poor treatment outcomes. Other studies done by Alemayehu et al23 and Gebreyohannes et al36 reported that hemorrhagic stroke and elevated serum creatinine were the only variables significantly associated with poor treatment outcomes, respectively. This variation in predictors of poor treatment outcomes could be due to differences in sample size, duration of follow-up, risk factors, and difference in assessment and detection of complications and outcomes.
Limitations of the Study
The present study has several limitations. First, it included small case numbers which decrease its power to identify potential independent predictors. Second, it was conducted by retrospective chart review and suffered from the exclusion of many patient cases due to the incompleteness of the medical record. Third, patients diagnosed without neuro-imaging were still included in the study because not all suspected stroke patients get CT-scans due to economic or other reasons. Fourth, the present study is a single-center study and cannot be generalized to all hospitals in Ethiopia. Finally, it was a retrospective observational study that cannot provide cause-and-effect relationships. So, this study should be used in light of its limitations and strengths.
Conclusions
The most common subtype of stroke encountered in the present study was an ischemic stroke. Stroke patients were presented in their mid-50s with male predominance. The most common comorbid condition identified was hypertension. Aspirin and atorvastatin were the most commonly used medications among ischemic stroke patients while ACEIs were the most commonly used antihypertensive medication in both stroke subtypes. A significant number of stroke patients had poor treatment outcomes. Older age, heart failure, decreased level of consciousness on admission, and aspiration pneumonia were significantly associated with poor prognosis. Availing thrombolytic therapy, devising appropriate preventive measures of risk factors (hypertension), and decreasing preventable complications such as aspiration pneumonia could improve patient outcomes.
Abbreviations
DALY, disability-adjusted life years; JUMC, Jimma University Medical Center; LMIC, low and middle-income countries; MRI, magnetic resonance imaging; CT, computed tomography; mRs, modified Rankin scale; r-tPA, recombinant tissue plasminogen activators.
Data Sharing Statement
The data used for this study will be made available by the corresponding author (RT) upon reasonable request.
Ethics Approval and Consent to Participate
The present study protocol was approved by the Institutional Review Board (IRB) of Jimma University, Institute of Health before starting data collection. The ethical committee reviewed the study protocol and approved verbal informed consent received from patients before reviewing their medical records. In addition, permission was obtained from the hospital chief medical director and the process was approved. The patient’s data from the medical records were handled with strong confidentiality. Neither the medical records nor the data extracted was used for any other purpose. Participants privacy and confidentiality was kept throughout the study process by using codes and removing identifiers such as patient name and contact address from the data collection tool. All the study protocols were conducted in line with the ethical principle of the Declaration of Helsinki.37
Acknowledgments
We would like to thank the data collectors and stroke unit staff members for their strong dedication toward the success of this study. We are also grateful to Eshetu Mulisa for language edition support and proofreading and Jimma University community based education coordinators for logistic support of the study.
Author Contributions
All authors made substantial contributions to conception and design, acquisition of data, or analysis and interpretation of data; took part in drafting the article or revising it critically for important intellectual content; agreed to submit to the current journal; gave final approval of the version to be published; and agree to be accountable for all aspects of the work.
Disclosure
The authors declare that there is no conflicts of interest regarding this work.
References
1. Abbott AL, Silvestrini M, Topakian R, et al. Optimizing the definitions of stroke, transient ischemic attack, and infarction for research and application in clinical practice. Front Neurol. 2017;8:1–14. doi:10.3389/fneur.2017.00537
2. Mozaffarian D, Benjamin EJ, Go AS, et al. Heart disease and stroke statistics-2016 update a report from the American Heart Association. Circulation. 2016;133:e38–e360. doi:10.1161/CIR.0000000000000350
3. Feigin VL, Norrving B, Mensah GA. Global burden of stroke. Circ Res. 2017;120(3):439–448. doi:10.1161/CIRCRESAHA.116.308413
4. Berkowitz AL. Managing acute stroke in low-resource settings. Bull World Health Organ. 2016;94(7):554–556. doi:10.2471/BLT.15.162610
5. Feigin V, Krishnamurthi R, Parmar P, et al. Update on the global burden of ischaemic and hemorrhagic stroke in 1990–2013: the GBD 2013 Study. Neuroepidemiology. 2016;45(3):161–176. doi:10.1159/000441085.UPDATE
6. Powers WJ, Derdeyn CP, Biller J, et al. 2015 American Heart Association/American stroke association focused update of the 2013 guidelines for the early management of patients with acute ischemic stroke regarding endovascular treatment: a guideline for healthcare professionals from the American. Stroke. 2015;46(10):3020–3035. doi:10.1161/STR.0000000000000074
7. Baatiema L, Chan CKY, Sav A, Somerset S. Interventions for acute stroke management in Africa: a systematic review of the evidence. Syst Rev. 2017;6(1):213. doi:10.1186/s13643-017-0594-4
8. Powers WJ, Rabinstein AA, Ackerson T, et al. Guidelines for the early management of patients with acute ischemic stroke: 2019 update to the 2018 guidelines for the early management of acute ischemic stroke a guideline for healthcare professionals from the American Heart Association/American Stroke A. Stroke. 2019;50(12):e344–e418. doi:10.1161/STR.0000000000000211
9. Lin MP, Sanossian N. Reperfusion therapy in the acute management of ischemic stroke. Cardiol Clin. 2015;33(1):99–109. doi:10.1016/j.ccl.2014.09.009
10. Powers WJ, Rabinstein AA, Ackerson T, et al. 2018 Guidelines for the early management of patients with acute ischemic stroke: a guideline for healthcare professionals from the American Heart Association/American Stroke Association. Stroke. 2018;49(3):870–947. doi:10.1161/STR.0000000000000158
11. Fekadu G, Chelkeba L, Melaku T, et al. Management protocols and encountered complications among stroke patients admitted to stroke unit of Jimma university medical center, Southwest Ethiopia: Prospective Observational Study. Ann Med Surg. 2019;48:135–143. doi:10.1016/j.amsu.2019.11.003
12. Johnson W, Onuma O, Owolabi M, Sachdev S. Stroke: a global response is needed. Bull World Health Organ. 2016;94(9):634A–635A. doi:10.2471/BLT.16.181636
13. Fekadu G, Chelkeba L, Melaku T, Tegene E, Kebede A. 30-Day and 60-day rates and predictors of mortality among adult stroke patients: Prospective Cohort Study. Ann Med Surg. 2020;53:1–11. doi:10.1016/j.amsu.2020.03.001
14. Nicks B, Henley J, Mfinanga J, Manthey D. Neurologic emergencies in resource-limited settings: a review of stroke care considerations. Afr J Emerg Med. 2015;5(1):37–44. doi:10.1016/j.afjem.2014.06.002
15. Berge E, Whiteley W, Audebert H, et al. European Stroke Organisation (ESO) guidelines on intravenous thrombolysis for acute ischaemic stroke. Eur Stroke J. 2021;6(1):I–LXII. doi:10.1177/2396987321989865
16. Norrving B. Stroke management – recent advances and residual challenges. Nat Rev Neurol. 2019;15(2):69–71. doi:10.1038/s41582-018-0129-1
17. Fekadu G, Chelkeba L, Kebede A. Burden, clinical outcomes and predictors of time to in hospital mortality among adult patients admitted to stroke unit of Jimma university medical center: a Prospective Cohort Study. BMC Neurol. 2019;19:1–11. doi:10.1186/s12883-019-1439-7
18. Shenkutie Greffie E. Risk factors, clinical pattern and outcome of stroke in a Referral Hospital, Northwest Ethiopia. Clin Med Res. 2015;4(6):182. doi:10.11648/j.cmr.20150406.13
19. Fekadu G, Adola B, Mosisa G, Shibiru T, Chelkeba L. Clinical characteristics and treatment outcomes among stroke patients hospitalized to Nekemte referral hospital, western Ethiopia. J Clin Neurosci. 2020;71:170–176. doi:10.1016/j.jocn.2019.08.075
20. Alene M, Assemie MA, Yismaw L, Ketema DB. Magnitude of risk factors and in-hospital mortality of stroke in Ethiopia: a systematic review and meta-analysis. BMC Neurol. 2020;20(1):1–10. doi:10.1186/s12883-020-01870-6
21. Gedefa B, Menna T, Berhe T, Abera H. Assessment of risk factors and treatment outcome of stroke admissions at St. Paul’s Teaching Hospital, Addis Ababa, Ethiopia. J Neurol Neurophysiol. 2017;08(03):6–11. doi:10.4172/2155-9562.1000431
22. Diseases WHON, Cluster MH. WHO STEPS Stroke Manual: The WHO STEP Wise Approach to Stroke Surveillance/Noncommunicable Diseases and Mental Health. World Health Organization;2005:8 sections.
23. Alemayehu CM. Assessment of stoke patients: occurrence of unusually high number of haemorrhagic stroke casesin Tikur Anbessa Specialized Hospital, Addis Ababa, Ethiopia. Clin Med Res. 2013;2(5):94. doi:10.11648/j.cmr.20130205.11
24. Deresse B, Shaweno D. Epidemiology and in-hospital outcome of stroke in South Ethiopia. J Neurol Sci. 2015;355(1–2):138–142. doi:10.1016/j.jns.2015.06.001
25. Zewdie A, Debebe F, Kebede S, et al. Prospective assessment of patients with stroke in Tikur Anbessa Specialised Hospital, Addis Ababa, Ethiopia. Afr J Emerg Med. 2018;8(1):21–24. doi:10.1016/j.afjem.2017.11.001
26. Adoukonou T, Kossi O, Fotso Mefo P, et al. Stroke case fatality in sub-Saharan Africa: systematic review and meta-analysis. Int J Stroke. 2021:1747493021990945. Available from: https://journals.sagepub.com/doi/abs/10.1177/1747493021990945?journalCode=wsoaII.
27. O’Donnell S, Tirschwell D, Kalani R, Feigin V, Johnson C, Roth G. Global variation and burden of hemorrhagic stroke (S10.004). Neurology. 2018;90:
28. Fekadu G, Chelkeba L, Kebede A. Retraction note: risk factors, clinical presentations and predictors of stroke among adult patients admitted to stroke unit of Jimma university medical center, south west Ethiopia: Prospective Observational Study. BMC Neurol. 2019;19(183):1–12.
29. Alloubani A, Saleh A, Abdelhafiz I. Hypertension and diabetes mellitus as a predictive risk factors for stroke. Diabetes Metab Syndr Clin Res Rev. 2018;12(4):577–584. doi:10.1016/j.dsx.2018.03.009
30. Mohamed SF, Uthman OA, Caleyachetty R, et al. Uncontrolled hypertension among patients with comorbidities in sub-Saharan Africa: protocol for a systematic review and meta-analysis. Syst Rev. 2020;9(1):1–5. doi:10.1186/s13643-020-1270-7
31. Temesgen TG, Teshome B, Njogu P. Treatment outcomes and associated factors among hospitalized stroke patients at Shashemene Referral Hospital, Ethiopia. Stroke Res Treat. 2018;2018. Available from: https://www.hindawi.com/journals/srt/2018/8079578/III.
32. Rønning OM, Stavem K. Predictors of mortality following acute stroke: a cohort study with 12 years of follow-up. J Stroke Cerebrovasc Dis. 2012;21(5):369–372. doi:10.1016/j.jstrokecerebrovasdis.2010.09.012
33. Abdo R, Abboud H, Salameh P, El Hajj T, Hosseini H. Mortality and predictors of death poststroke: data from a multicenter prospective cohort of Lebanese stroke patients. J Stroke Cerebrovasc Dis. 2019;28(4):859–868. doi:10.1016/j.jstrokecerebrovasdis.2018.11.033
34. Tinker RJ, Smith CJ, Heal C, et al. Predictors of mortality and disability in stroke-associated pneumonia. Acta Neurol Belg. 2021;121(2):379–385. doi:10.1007/s13760-019-01148-w
35. Femi O, Mansur N. Factors associated with death and predictors of one-month mortality from stroke in Kano, Northwestern Nigeria. J Neurosci Rural Pract. 2013;4:S56–61. doi:10.4103/0976-3147.116460
36. Gebreyohannes EA, Bhagavathula AS, Abebe TB, Seid MA, Haile KT. In-hospital mortality among ischemic stroke patients in Gondar University Hospital: a Retrospective Cohort Study. Stroke Res Treat. 2019;2019. Available from: https://www.hindawi.com/journals/srt/2019/7275063/.
37. World Medical Association. World medical association declaration of Helsinki: ethical principles for medical research involving human subjects. JAMA. 2013;310(20):2191–2194. doi:10.1001/jama.2013.281053
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.