")
Back to Journals » Drug Design, Development and Therapy » Volume 17
Pharmacokinetics and Pharmacodynamics of Esomezol DR, a New Dual Delayed-Release Formulation of Esomeprazole 20 Mg or 40 Mg, in Healthy Subjects
Authors Kim HC , Yang E , Ban MS , Kim YK , Hong SH , Jung J , Jang IJ , Lee S
Received 14 November 2022
Accepted for publication 21 March 2023
Published 12 April 2023 Volume 2023:17 Pages 1115—1124
DOI https://doi.org/10.2147/DDDT.S392533
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Georgios Panos
Hyun Chul Kim,1,2 Eunsol Yang,1,3 Mu Seong Ban,1 Yu Kyong Kim,4 Sung Hee Hong,5 Jina Jung,5 In-Jin Jang,1 SeungHwan Lee1
1Department of Clinical Pharmacology and Therapeutics, Seoul National University College of Medicine and Hospital, Seoul, Republic of Korea; 2Integrated Major in Innovative Medical Science, Seoul National University Graduate School, Seoul, Republic of Korea; 3Kidney Research Institute, Seoul National University Medical Research Center, Seoul, Republic of Korea; 4Department of Clinical Pharmacology and Therapeutics, Chungbuk National University College of Medicine and Hospital, Cheongju, Republic of Korea; 5Hanmi Pharmaceutical Co., Ltd., Seoul, Republic of Korea
Correspondence: SeungHwan Lee, Department of Clinical Pharmacology and Therapeutics, Seoul National University College of Medicine and Hospital, Seoul, Republic of Korea, Tel +82-2-2072-2343, Fax +82-2-742-9252, Email [email protected]
Background: Esomeprazole, a proton pump inhibitor (PPI), is widely used to treat acid-related disorders, but it has short plasma half-life which can cause insufficient gastric acid suppression, such as nocturnal acid breakthrough. A new dual delayed-release (DR) formulation of esomeprazole (Esomezol DR), was developed to extend the duration of gastric acid suppression.
Purpose: This study aimed to evaluate the pharmacokinetics (PKs) and pharmacodynamics (PDs) of esomeprazole for the DR formulation compared to a conventional enteric-coated (EC) formulation (Nexium) in healthy male subjects.
Methods: Two randomized, open-label, multiple-dose, two-way crossover studies with esomeprazole 20 mg and 40 mg were conducted. Subjects received the DR formulation or the EC formulation once daily for 7 days in each period with a 7-day washout. Serial blood samples were collected up to 24 hours after the 1st dose, and 24-hour intragastric pH was continuously monitored before the 1st dose as baseline and after the 1st and the 7th dose.
Results: In 20 mg and 40 mg dose groups, 38 and 44 subjects completed the study, respectively. The DR formulation exhibited the dual-release pattern of esomeprazole, resulting in more sustained plasma concentration–time profiles compared to the EC formulation. The systemic exposure of esomeprazole for the DR formulation was comparable to that for the EC formulation, showing the similar area under the plasma concentration–time curve. The 24-hour gastric acid suppression was also similar between the two formulations, while the inhibition during night-time (22:00– 06:00) showed a better tendency in the DR formulation.
Conclusion: The sustained exposure of esomeprazole in the DR formulation led to well-maintained and higher acid inhibition compared to the EC formulation, especially during the night-time. These results suggest that the DR formulation can be an alternative formulation to the conventional EC formulation, expecting the potential of relieving nocturnal acid-related symptoms.
Keywords: proton pump inhibitors, esomeprazole, dual delayed-release formulation, gastro-esophageal reflux disease, GERD, nocturnal acid breakthrough
Introduction
Proton pump inhibitors (PPIs) are the most widely prescribed medication for controlling acid-related disorders based on their more profound gastric acid suppression compared to that of other acid reducing agents including antacids or histamine-2-receptor antagonists (H2RAs).1,2 PPIs inhibit H+/K+-ATPase (proton pump) irreversibly which is responsible for gastric acid secretion. However, the short plasma half-life in pharmacokinetic (PK) characteristics of PPIs and the natural recovery process of gastric acid secretion function can lead to the insufficient gastric acid suppression.2–6
Gastro-esophageal reflux disease (GERD) is one of the most common acid-related disorders in which gastric acid or contents refluxed into the esophagus or oropharynx result in troublesome symptoms including heartburn and acid regurgitation.7,8 Especially, the continued gastric acid secretion during the night-time, such as nocturnal acid breakthrough (NAB), may lead to the nocturnal GERD symptoms and additional mucosal injury in the most actively healing time of esophagitis.9,10 NAB is defined as the presence of intragastric pH <4 for at least continuous 60 minutes overnight during administrations of PPI therapy.10
In order to overcome the limitations of PPIs and improve gastric acid control, many methods have been proposed in terms of the PKs, formulations, or dosage regimens.11 Esomeprazole (S-enantiomer of omeprazole) and dexlansoprazole (R-enantiomer of lansoprazole), respectively, showed higher bioavailability and lower clearance than the racemic mixtures, omeprazole and lansoprazole.11–14 Enteric-coated (EC) delayed-release formulations are commonly used for acid-labile PPIs to prevent degradation by gastric acid, but there are still limitations regarding the PKs of the PPIs themselves or the physiology of the proton pump.2–6 Twice-daily PPI therapy is considered an option for some patients with GERD, but the frequency of doses may affect the patient compliance.1,11 Therefore, dexlansoprazole with dual delayed-release (DR) formulation was developed considering patient compliance.2,11
To prolong the anti-secretary effect of PPIs with extending the exposure in the recommended once-daily dosing regimen for the treatment of GERD, DR formulation has been developed for some PPIs. The DR formulation with additional drug release after the first drug release is expected to maintain systemic exposure longer than a conventional single-release formulation. The studies of dexlansoprazole modified release (MR) 30 and 60 mg (Dexilant, Takeda Pharmaceuticals) showed that the DR formulation maintained a higher mean intragastric pH and percentage of time with intragastric pH over 4 (%Time over pH 4) with a longer period of the plasma exposure when compared to the conventional formulation in a once-daily dosing regimen.14,15
A new DR formulation of esomeprazole (Esomezol DR) is under development by Hanmi Pharm. Co., Ltd. to extend duration of gastric acid suppression, especially during the night-time, with a once-daily dosing regimen. The DR formulation consists of 2 types of EC mini tablets designed to release esomeprazole at the different pH conditions and to reduce the breakdown of esomeprazole in the stomach. In the in vitro dissolution test, the enteric coatings prevented drug release from acid degradation (for 120 min in 0.1 N HCl), and esomeprazole was released immediately and slowly depending on the types of EC mini tablets in pH 6.8 phosphate buffer.16 In addition, in the in vivo evaluation of the DR formulation in beagle dogs pretreated with pentagastrin, the DR formulation exhibited the dual release pattern with the delayed absorption time, resulting in a longer half-life than the conventional formulation.16
Based on the in vitro and in vivo test results, this study aimed to evaluate the PKs and pharmacodynamics (PDs) for the newly developed DR formulation of esomeprazole compared to the conventional EC formulation (Nexium) in healthy male subjects. In addition, the gastric acid suppression of esomeprazole for the DR formulation during the night-time was explored compared to the EC formulation.
Materials and Methods
The study was reviewed and approved by the Korean Ministry of Food and Drug Safety (MFDS) and the Institutional Review Board of Seoul National University Hospital (ClinicalTrials.gov: NCT03372850, study period: January 24th, 2018 – December 25th, 2019, first subject first visit: February 9th, 2018, last subject last visit: April 26th, 2019). This study was conducted in accordance with the Declaration of Helsinki and the Korean Good Clinical Practice. The written informed consents were obtained from all subjects prior to any study procedures.
Study Population
Healthy male subjects aged 19–50 years with 55–90 kg for weight and 18.0–27.0 kg/m2 for body mass index were enrolled in the study. Their eligibility for the study was evaluated based on health status including medical history, vital signs, physical examinations, and clinical laboratory tests. The subjects who were positive for Helicobacter pylori (H. pylori), who had history of clinically significant gastrointestinal diseases or gastrointestinal surgery, who had anatomical disabilities inserting and maintaining a pH-meter catheter, or whose aspartate aminotransferase or alanine aminotransferase was higher than 1.5 times of the upper normal limit were excluded.
Study Design
Two randomized, open-label, multiple-dose, two-way crossover studies with esomeprazole 20 mg and 40 mg were conducted, respectively. The enrolled subjects in each dose group were randomly assigned to one of two sequences (EC formulation → DR formulation or DR formulation → EC formulation) in a ratio of 1:1. According to their assigned sequence, the DR formulation as test formulation or the EC formulation as reference formulation were orally administered once daily for 7 days in each period under overnight fasting conditions (Figure 1). Considering the plasma half-life of esomeprazole and the recovery of gastric acid secretion, there was a 7-day washout period between the two administration periods.2–6 Meals were provided three times a day at the same time during the administration periods, but breakfast was not provided on the days for the 24-hour intragastric pH monitoring.
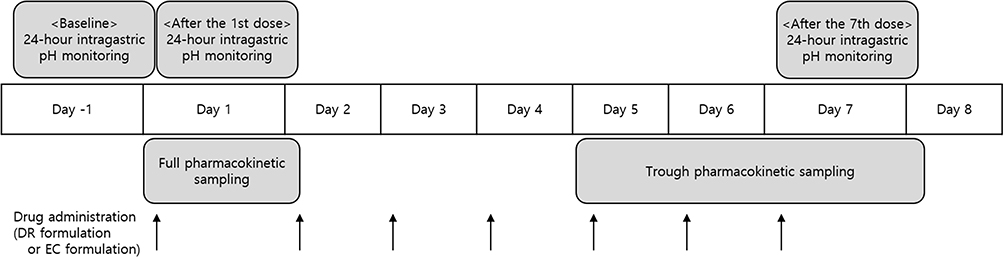 |
Figure 1 Study design in each period. Abbreviations: DR, dual delayed-release; EC, enteric-coated. Note: There was a 7-day washout period between the two administration (DR formulation or EC formulation) periods. |
The number of study subjects was calculated from the results of three different bioequivalence studies using Nexium 40 mg as a comparator.17–19 Assuming the maximum intra-subject coefficient of variation (CV) of 31.3% for PK parameters and the dropout rate of 10%, a total sample size of 48 subjects in each dose group was estimated to verify that the systemic exposure and acid suppressive effect for 24 hours between the DR formulation and the EC formulation are within the 20% difference with approximately 90% power at the significance level of 0.05.
Pharmacokinetic Assessment
Blood samples for PK assessment were collected at pre-dose and 0.25, 0.5, 0.75, 1, 1.5, 2, 2.5, 3, 3.5, 4, 4.5, 5, 5.5, 6, 8, 10, 12, 16, and 24 hours after the 1st dose of each study drug. Additional trough PK samples at each pre-dose of day 5 to 7 and at 24 hours after the last (the 7th) dose of the DR formulation or the EC formulation were obtained to check whether the plasma concentration of esomeprazole was reached at the steady-state (Figure 1).
The blood samples collected in K2-ethylenediaminetetraacetic acid (EDTA) vacutainer were centrifuged at 4°C and 3000 rpm for 10 minutes. The plasma was separated in the Eppendorf tubes and then stored at or below −70°C until analysis. The plasma concentrations of esomeprazole were determined by a validated ultra-performance liquid chromatography (UPLC; Waters ACQUITY UPLCTM System, Waters) with mass spectrometric (MS/MS; Micromass Quattro micro API, Waters) method. Esomeprazole as analyte and esomeprazole-d3 as internal standard were separated with a Waters ACQUITY UPLC BEH C18 column (1.7 μm, 2.1 mm I.D. × 50 mm L) and detected by positive ion electrospray ionization with multiple reaction monitoring at m/z 346 → 198 for esomeprazole and 349 → 198 for esomeprazole-d3.20,21 Calibration curve of esomeprazole was constructed in the range of 10 to 4000 ng/mL. For the calibration curve data and the quality control sample data of esomeprazole, the relative standard deviation and the deviation of the mean from theoretical were within 1.5–5.0% and −1.3–2.2%, respectively, in the 20 mg dose group, and within 2.0–4.6% and −4.4–3.3%, respectively, in the 40 mg dose group.
The PK parameters of esomeprazole were calculated with plasma concentration–time curves by a noncompartmental method using WinNonlin version 8.2 (Pharsight, CA, USA). The primary PK parameter was set as area under the plasma concentration–time curve (AUC) from time 0 to the last measurable time point (AUClast) to compare the systemic exposure of esomeprazole between two formulations. The secondary PK parameters included AUC from time 0 to infinity (AUCinf), maximum plasma concentration (Cmax), time to reach Cmax (Tmax), elimination half-life (t1/2), apparent total clearance (CL/F), and apparent volume of distribution (Vd/F).
Pharmacodynamic Assessment
The extent of gastric acid suppression has been measured using the surrogate markers, such as integrated gastric acidity and the duration of intragastric pH above 4,22–25 and the threshold of pH 4 has been proposed to discriminate the degree of GERD symptoms and the severity of mucosal injury.26–28
Continuous 24-hour intragastric pH monitoring with an ambulatory pH recorder, DigitrapperTM pH-Z system (Medtronic), was performed three times in each period, which were before the 1st dose as baseline, and after the 1st and the 7th dose (Figure 1).21 The primary PD parameter was set as the percentage decrease from baseline in integrated gastric acidity (ΔIntegrated gastric acidity) after the 7th dose.
The ΔIntegrated gastric acidity was calculated as follows:23
- Acid concentration (mmol/L) = 1000 × 10−pH.
- Acidity (mmol∙h/L) = (acid in mmol/L at time “t” + acid in mmol/L at time “t−1”)/2 × (t – t−1).
- Integrated acidity (mmol∙h/L) = ∑acidity in mmol/L × time in second.
- ΔIntegrated gastric acidity (%) = (Baseline – the 1st or the 7th dose)/Baseline × 100.
The secondary PD parameters included ΔIntegrated gastric acidity after the 1st dose, %Time over pH 4 after the 1st and the 7th dose, and median pH after the 1st and the 7th dose.
The exploratory PD parameters included the values during the night-time (22:00–06:00) after the 1st and the 7th dose as follows: the percentage of time with NAB (%Time with NAB), the percentage of subjects with at least one occasion of NAB (%Subjects with NAB), ΔIntegrated gastric acidity, %Time over pH 4, and median pH.
Safety Assessment
Safety was assessed by monitoring adverse events (AEs), physical examinations, vital signs, 12-lead electrocardiograms, and clinical laboratory tests.
Statistical Analysis
Statistics were analyzed by using SAS version 9.4 (SAS Institute Inc., Cary, NC, USA). The geometric mean ratios (GMRs) and its 90% confidence intervals (CIs) of the DR formulation to the EC formulation for AUClast and AUCinf after the 1st dose were estimated using a linear mixed effect model. The model contained period, sequence, formulation, and admission group as fixed effects, and subject nested within sequence and admission group as random effect. In the same manner as PK parameters, the corresponding values for ΔIntegrated gastric acidity after the 1st and the 7th dose were also estimated using the linear mixed effect model. It was concluded that the two formulations are bioequivalent in the systemic exposure and 24-hour acid suppressive effect if the 90% CIs of GMRs of the DR formulation to the EC formulation for the primary PK and PD parameters are within the conventional bioequivalence range of 0.80–1.25.
Results
Demographics
In the 20 mg dose group, 48 subjects were enrolled, and 38 participants completed the entire study schedule without major deviation. Six subjects withdrew the consent before the 1st dose, but four subjects withdrew after the 1st dose. The mean ± standard deviation values of 42 subjects who received study drug at least once were 28.5 ± 7.7 years for age, 173.1 ± 7.0 cm for height, 70.3 ± 8.6 kg for weight, and 23.4 ± 2.2 kg/m2 for body mass index.
In the 40 mg dose group, 48 subjects were enrolled, and 44 participants completed the entire study schedule without major deviation. Four subjects withdrew the consent, and two subjects each withdrew before and after the 1st dose. The mean ± standard deviation values of 46 subjects who received the study drug at least once were 31.2 ± 5.8 years for age, 172.7 ± 4.5 cm for height, 70.2 ± 8.0 kg for weight, and 23.5 ± 2.3 kg/m2 for body mass index.
In the demographics, there were no statistically significant differences between sequences of each dose group.
Pharmacokinetics
A total of 38 and 44 subjects who completed the study without major deviation were included in the PK analysis set for each of the 20 mg and 40 mg dose groups.
The DR formulation exhibited the dual-release pattern of esomeprazole, resulting in more sustained plasma concentration–time profiles compared to the EC formulation. The absorption of esomeprazole for the DR formulation was delayed with a prolonged Tmax compared to that for the EC formulation (Figure 2, Table 1). In the 20 mg dose group, the median Tmax of esomeprazole was 2.25 hours for the DR formulation and 2 hours for the EC formulation, and the corresponding values in the 40 mg dose group were 4 hours and 2 hours, respectively. However, the systemic exposure of esomeprazole for the DR formulation was comparable to that for the EC formulation in each dose group, showing the similar AUC values. The GMRs (90% CIs) of the AUClast of esomeprazole for the DR formulation to the EC formulation were 0.9577 (0.8791–1.0433) in the 20 mg dose group and 0.9479 (0.9056–0.9922) in the 40 mg dose group, which were both within the conventional bioequivalence range of 0.80–1.25 (Table 1).
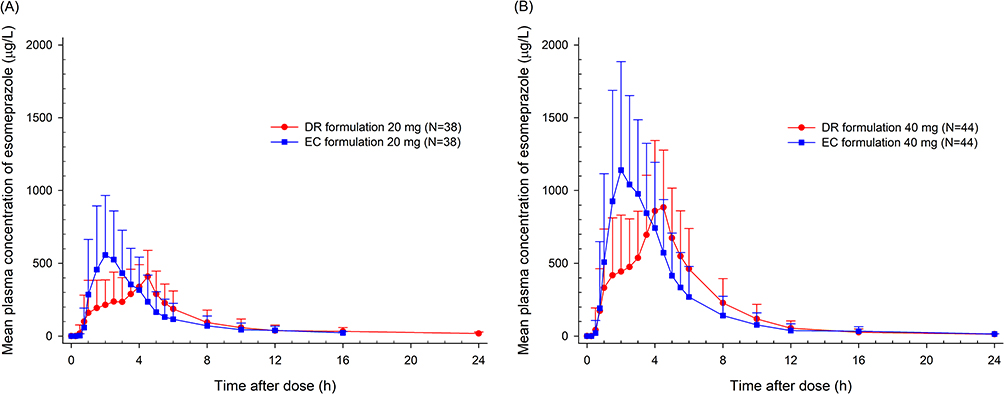 |
Figure 2 Mean plasma concentration-time profiles of esomeprazole for DR formulation or EC formulation after the 1st dose in (A) 20 mg and (B) 40 mg dose groups. Abbreviations: DR, dual delayed-release; EC, enteric-coated. Note: The vertical bars represent standard deviation. |
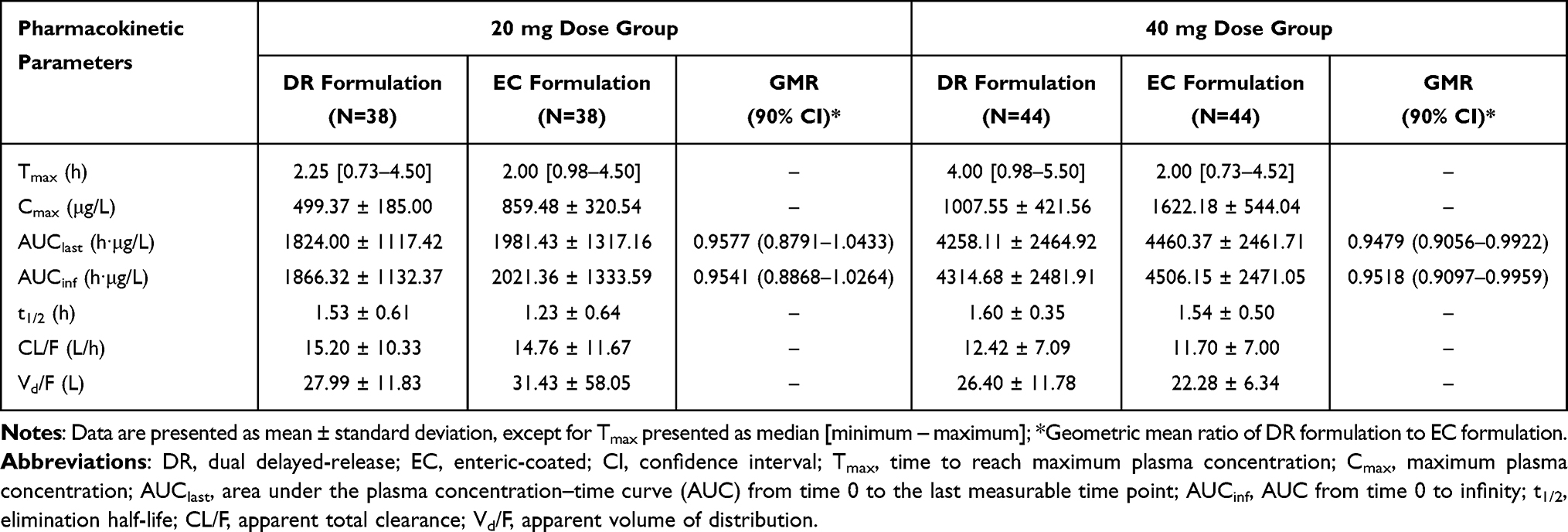 |
Table 1 Summary of Pharmacokinetic Parameters of Esomeprazole After the 1st Dose of DR Formulation or EC Formulation in 20 Mg and 40 Mg Dose Groups |
Pharmacodynamics
A total of 38 and 41 subjects who completed the study with sufficient intragastric pH data more than 95% of total pH monitoring time were included in the PD analysis set for each of the 20 mg and 40 mg dose groups.
The intragastric mean pH profiles of the DR formulation were similar to or lower than that of the EC formulation up to 4 hours after the 1st and the 7th dose, but showed a higher tendency thereafter (Figure 3). The 24-hour PD parameters between the two formulations were comparable in each dose group (Table 2). The GMRs (90% CIs) of the ΔIntegrated gastric acidity after the 7th dose for the DR formulation to the EC formulation were 1.0895 (1.0053–1.1808) in the 20 mg dose group and 1.0422 (0.9906–1.0964) in the 40 mg dose group (Table 2).
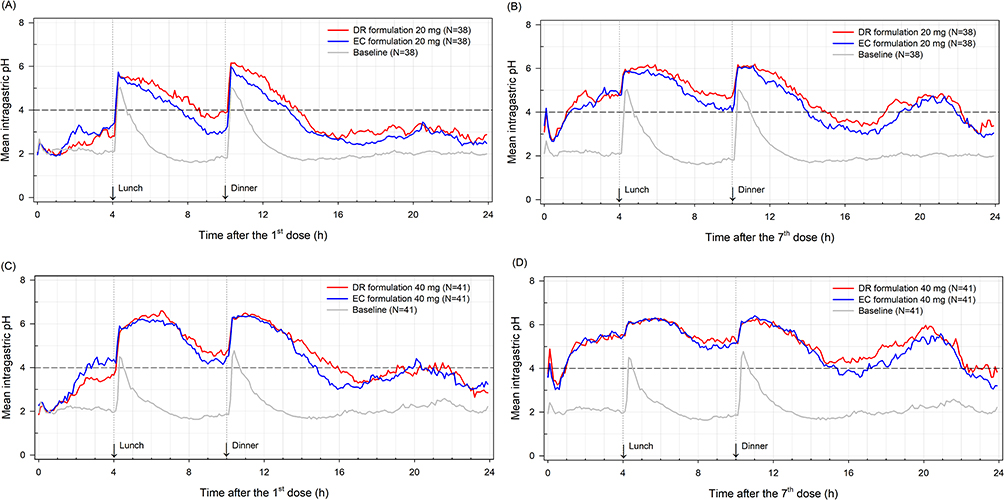 |
Figure 3 Mean intragastric pH-time profiles for DR formulation or EC formulation after (A) the 1st and (B) the 7th dose in 20 mg dose group and after (C) the 1st and (D) the 7th dose in 40 mg dose group. Abbreviations: DR, dual delayed-release; EC, enteric-coated. Note: The gray line represents mean intragastric pH before the 1st dose of DR formulation or EC formulation as baseline. |
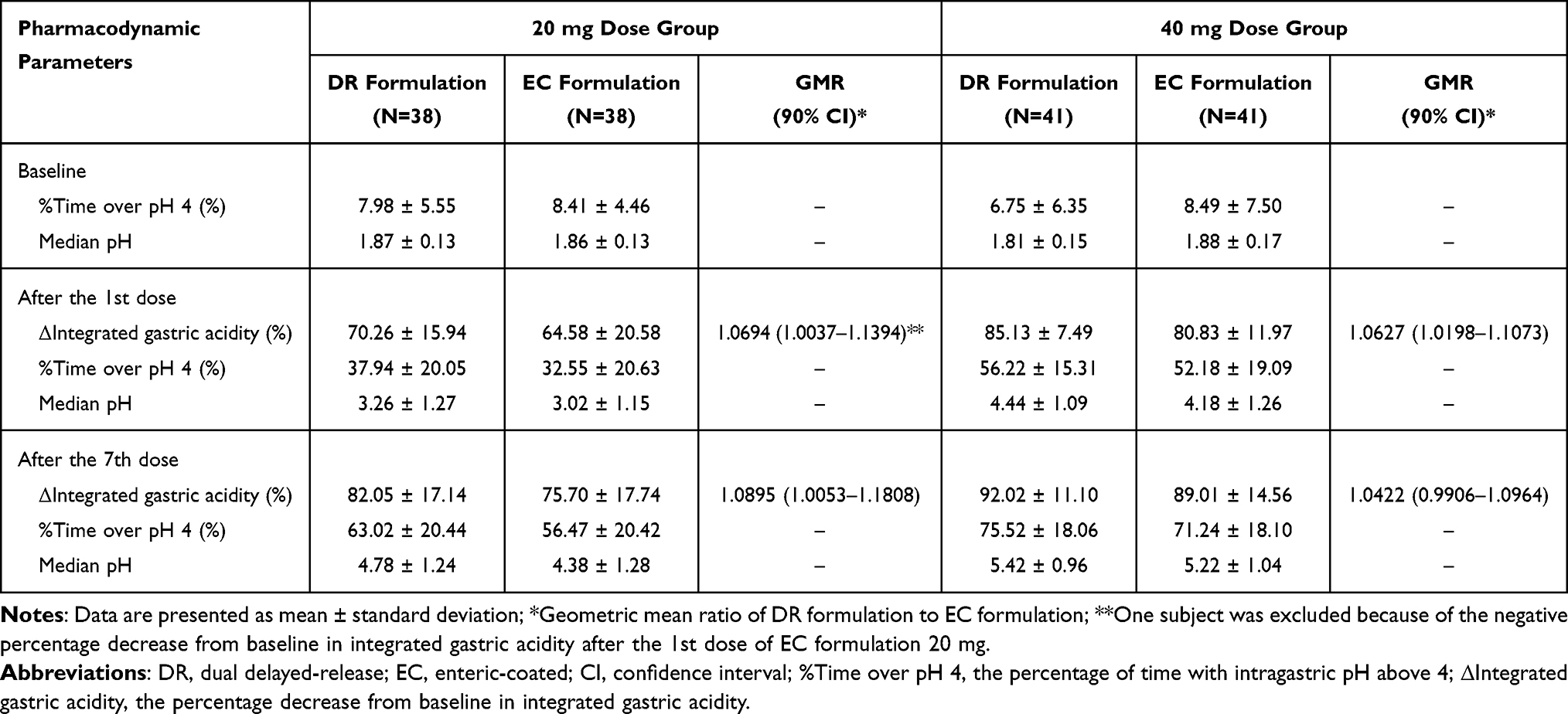 |
Table 2 Summary of 24-Hour Pharmacodynamic Parameters of Esomeprazole at Baseline and After the 1st and the 7th Dose of DR Formulation or EC Formulation in 20 Mg and 40 Mg Dose Groups |
During the night-time (22:00–06:00), the %Time with NAB and %Subjects with NAB after the 7th dose tended to be lower for the DR formulation than for the EC formulation. The mean %Time with NAB after the 7th dose was 33.95% for the DR formulation and 41.81% for the EC formulation in the 20 mg dose group, and the corresponding values in the 40 mg dose group were 14.95% and 22.09%, respectively. The ΔIntegrated gastric acidity, %Time over pH 4, and median pH of the DR formulation had a higher tendency than each corresponding value of the EC formulation (Table 3).
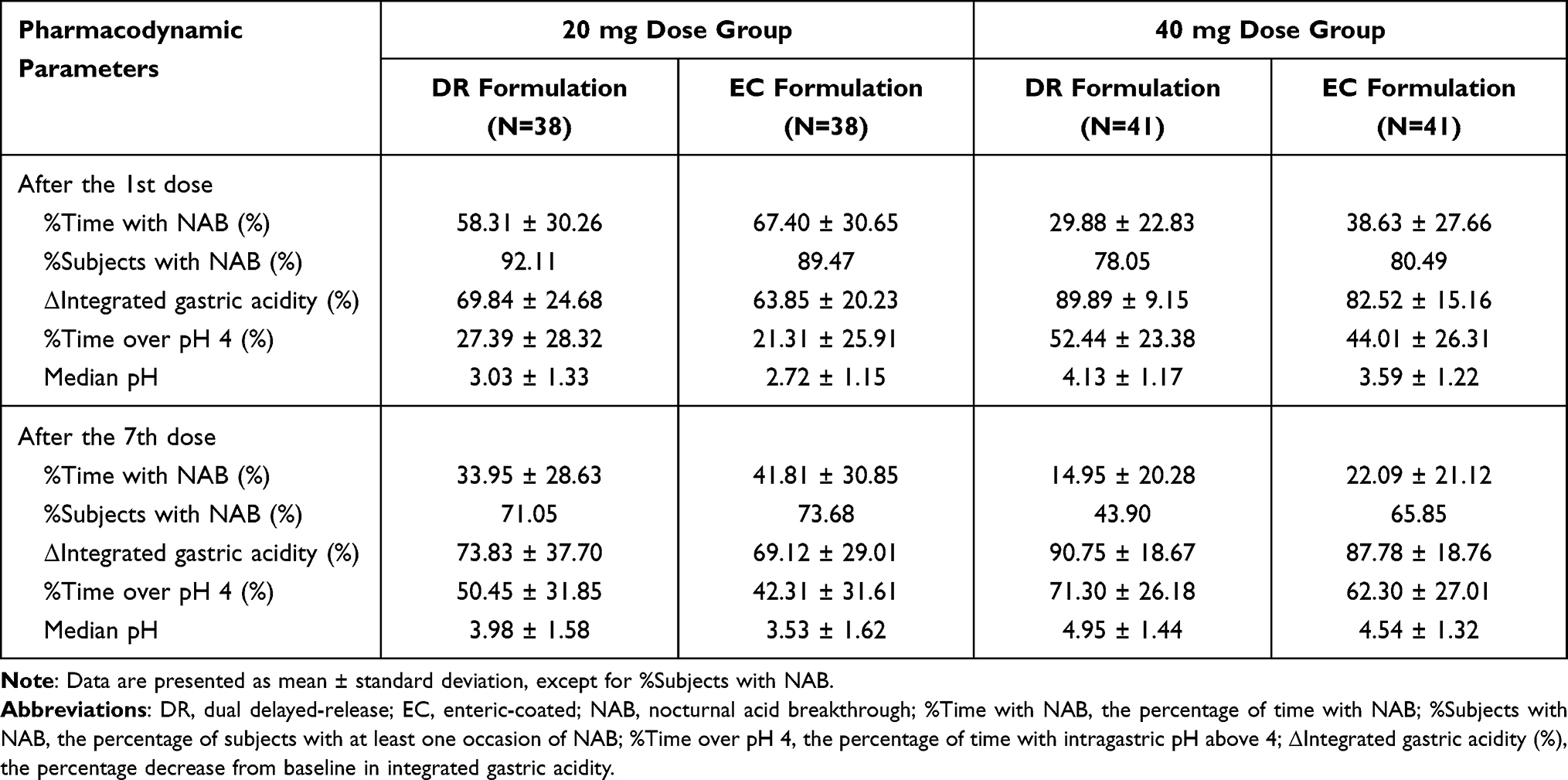 |
Table 3 Summary of Night-Time (22:00–06:00) Pharmacodynamic Parameters of Esomeprazole After the 1st and the 7th Dose of DR Formulation or EC Formulation in 20 Mg and 40 Mg Dose Groups |
Safety
A total of 42 and 46 subjects who received the study drug at least once were included in the safety analysis set for each of the 20 mg and 40 mg dose groups.
The incidence of adverse drug reactions (ADRs) was similar between the two formulations in each dose group (Table S1). Three ADRs in three subjects for the DR formulation and two ADRs in one subject for the EC formulation occurred in the 20 mg dose group, and ten ADRs in six subjects for the DR formulation and eight ADRs in five subjects for the EC formulation occurred in the 40 mg dose group. All ADRs were mild, and there was no serious AE (Table S1).
There were no clinically significant changes in physical examinations, vital signs, 12-lead electrocardiograms, and clinical laboratory tests.
Discussion
This study was conducted to evaluate the PKs and PDs of the newly developed DR formulation of esomeprazole compared to the conventional EC formulation. The systemic exposure and the 24-hour acid suppressive effect of esomeprazole for the DR formulation were comparable to those for the EC formulation. However, the DR formulation with more sustained exposure of esomeprazole than the EC formulation tended to be better in intragastric acid suppression during the night-time (22:00–06:00).
The DR formulation consists of 2 types of enteric-coated mini tablets, which were designed to release immediately in around 5–10 minutes above pH 5.5 and slowly in around 15–90 minutes above pH 6 to 7.16 The 1st and the 2nd peaks of esomeprazole in the individual PK profiles of the DR formulation appeared in approximately 1.75 hours and 3–6 hours after administration, respectively (Figure S1). The dual-release pattern of esomeprazole after administration of the DR formulation shows that esomeprazole in the DR formulation was released as expected depending on gastric emptying time, acidity of the proximal (pH 6.6) or distal (pH 7.5) small intestine,29 and migrating motor complex pattern (85 to 120 minutes).30 The characteristics of the DR formulation with this dual-release pattern allowed the plasma concentration of esomeprazole to be sustained.
In the PK-PD relationship for any PPI, AUC is well known as the best predictor of acid suppressive effects.3 In consistency with this, the similar AUC values between two formulations, despite the different absorption profiles, resulted in the comparable 24-hour acid suppressive effects, suggesting the clinical efficacy for the DR formulation may be similar to the EC formulation. Meanwhile, the sustained exposure of esomeprazole in the DR formulation, indicated by the delayed absorption with a dual peak, led to maintaining the higher mean pH and %Time over pH 4 from 4 hours post-dose compared to the EC formulation (Figure S2). Especially during the night-time, the median pH of the DR formulation was close to or higher than pH 4 in both dose groups. These results indicate the substitutability of the DR formulation with the conventional EC formulation, expecting the favorable properties in terms of the relieve of nocturnal acid-related symptoms.
A twice-daily PPI therapy is considered for patients who have both extraesophageal and typical GERD, and the addition of H2RA at bedtime or baclofen is suggested for patients on PPIs with persistent nocturnal symptoms.1 In the study on the effect of splitting the dose of esomeprazole, esomeprazole 20 mg twice daily was not different in 24-hour PD parameters at steady-state (on day 6) from esomeprazole 40 mg once daily, but it showed the significant improvement in night-time (22:00–07:00) gastric acid suppression.31 It might be attributed to the sustained systemic exposure of esomeprazole in a 20 mg twice-daily regimen as observed with the DR formulation. Meanwhile, dexlansoprazole MR 30 mg once daily was a successful alternative to twice-daily PPI with well-controlled GERD-related symptoms even after step-down management in the GERD patients.32 Therefore, the DR formulation of esomeprazole once-daily regimen with the more sustained acid suppression may control nocturnal GERD symptoms as an alternative to twice-daily regimen of conventional delayed-release PPI formulation or use of the concomitant drugs.
The studies comparing intragastric pH before and after eradication of H. pylori have reported that the profiles of gastric acid secretion and NAB are different in H. pylori-positive patients.33–36 Further studies are needed to evaluate whether the DR formulation of esomeprazole is effective in improving NAB in this patient group.
Conclusion
The DR formulation exhibited the dual-release pattern of esomeprazole, resulting in more sustained plasma concentration–time profiles compared to the EC formulation. Consistent with the well-known PK-PD relationship for PPIs, the sustained exposure of esomeprazole in the DR formulation led to well-maintained and higher acid inhibition compared to the EC formulation, especially during the night-time. These results suggest that the DR formulation can be an alternative formulation to the conventional EC formulation, expecting the potential of relieving nocturnal acid-related symptoms. In addition, our findings can be widely used to understand the PKs and PDs of DR formulations for their appropriate clinical use or the further studies.
Acknowledgments
We would like to thank the staff at Seoul National University Hospital Clinical Trials Center. This study was sponsored by Hanmi Pharm. Co., Ltd.
Disclosure
Sunghee Hong and Jina Jung are employees of Hanmi Pharmaceutical Co. Ltd. The other authors do not have any conflicts of interest for this study.
References
1. Katz PO, Dunbar KB, Schnoll-Sussman FH, Greer KB, Yadlapati R, Spechler SJ. ACG clinical guideline for the diagnosis and management of gastroesophageal reflux disease. Am J Gastroenterol. 2022;117(1):27–56. doi:10.14309/ajg.0000000000001538
2. Strand DS, Kim D, Peura DA. 25 years of proton pump inhibitors: a comprehensive review. Gut Liver. 2017;11(1):27–37. doi:10.5009/gnl15502
3. Sachs G, Shin JM, Howden CW. Review article: the clinical pharmacology of proton pump inhibitors. Aliment Pharmacol Ther. 2006;23(Suppl 2):2–8. doi:10.1111/j.1365-2036.2006.02943.x
4. Gedda K, Scott D, Besancon M, Lorentzon P, Sachs G. Turnover of the gastric H+,K+-Adenosine triphosphatase alpha subunit and its effect on inhibition of rat gastric acid secretion. Gastroenterology. 1995;109(4):1134–1141. doi:10.1016/0016-5085(95)90571-5
5. Shin JM, Sachs G. Pharmacology of proton pump inhibitors. Curr Gastroenterol Rep. 2008;10(6):528–534. doi:10.1007/s11894-008-0098-4
6. Lind T, Cederberg C, Ekenved G, Haglund U, Olbe L. Effect of omeprazole--A gastric proton pump inhibitor--on pentagastrin stimulated acid secretion in man. Gut. 1983;24(4):270. doi:10.1136/gut.24.4.270
7. Kahrilas PJ. GERD pathogenesis, pathophysiology, and clinical manifestations. Cleve Clin J Med. 2003;70(Suppl 5):S4–S19. doi:10.3949/ccjm.70.Suppl_5.S4
8. Gyawali CP, Kahrilas PJ, Savarino E, et al. Modern diagnosis of GERD: the Lyon Consensus. Gut. 2018;67(7):1351–1362. doi:10.1136/gutjnl-2017-314722
9. Fouad Y, Katz P, Castell D. Oesophageal motility defects associated with nocturnal gastro-oesophageal reflux on proton pump inhibitors. Aliment Pharmacol Ther. 1999;13(11):1467–1472. doi:10.1046/j.1365-2036.1999.00641.x
10. Peghini PL, Katz PO, Bracy NA, Castell DO. Nocturnal recovery of gastric acid secretion with twice-daily dosing of proton pump inhibitors. Am J Gastroenterol. 1998;93(5):763–767. doi:10.1111/j.1572-0241.1998.221_a.x
11. Metz DC, Vakily M, Dixit T, Mulford D. Review article: dual delayed release formulation of dexlansoprazole MR, a novel approach to overcome the limitations of conventional single release proton pump inhibitor therapy. Aliment Pharmacol Ther. 2009;29(9):928–937. doi:10.1111/j.1365-2036.2009.03984.x
12. Olbe L, Carlsson E, Lindberg P. A proton-pump inhibitor expedition: the case histories of omeprazole and esomeprazole. Nat Rev Drug Discov. 2003;2(2):132–139. doi:10.1038/nrd1010
13. Novotna A, Srovnalova A, Svecarova M, Korhonova M, Bartonkova I, Dvorak Z. Differential effects of omeprazole and lansoprazole enantiomers on aryl hydrocarbon receptor in human hepatocytes and cell lines. PLoS One. 2014;9(6):e98711. doi:10.1371/journal.pone.0098711
14. Grady H, Murakawa Y, Mulford D, Kukulka M. Development of dexlansoprazole delayed-release capsules, a dual delayed-release proton pump inhibitor. J Pharm Sci. 2019;108(11):3496–3501. doi:10.1016/j.xphs.2019.07.023
15. Vakily M, Zhang W, Wu J, Atkinson SN, Mulford D. Pharmacokinetics and pharmacodynamics of a known active PPI with a novel Dual Delayed Release technology, dexlansoprazole MR: a combined analysis of randomized controlled clinical trials. Curr Med Res Opin. 2009;25(3):627–638. doi:10.1185/03007990802693883
16. Kwon TK, Kang J-H, Na S-B, et al. Novel esomeprazole magnesium-loaded dual-release mini-tablet polycap: formulation, optimization, characterization, and in vivo evaluation in beagle dogs. Pharmaceutics. 2022;14(7):1411. doi:10.3390/pharmaceutics14071411
17. The Korean Ministry of Food and Drug Safety (MFDS). Bioequivalence test review results of Hanxium®; 2014.
18. The Korean Ministry of Food and Drug Safety (MFDS). Bioequivalence test review results of Esora®; 2016.
19. The Korean Ministry of Food and Drug Safety (MFDS). Bioequivalence test review results of S-Empra®; 2016.
20. Choi Y, Han H, Shin D, Lim KS, Yu KS. Comparison of the pharmacokinetics and tolerability of HCP1004 (a fixed-dose combination of naproxen and esomeprazole strontium) and VIMOVO® (a marketed fixed-dose combination of naproxen and esomeprazole magnesium) in healthy volunteers. Drug Des Devel Ther. 2015;9:4127–4135. doi:10.2147/DDDT.S86725
21. Bae S, Kwon J, Lee SB, Jang IJ, Yu KS, Lee S. Comparative pharmacokinetics/pharmacodynamics of fixed-dose combination of esomeprazole and calcium carbonate (AD-206) to the Conventional esomeprazole. Drug Des Devel Ther. 2021;15:5099–5108. doi:10.2147/DDDT.S341271
22. Bell N, Burget D, Howden C, Wilkinson J, Hunt R. Appropriate acid suppression for the management of gastro-oesophageal reflux disease. Digestion. 1992;51(Suppl. 1):59–67. doi:10.1159/000200917
23. Gardner JD, Rodriguez-Stanley S, Robinson M. Integrated acidity and the pathophysiology of gastroesophageal reflux disease. Am J Gastroenterol. 2001;96(5):1363–1370. doi:10.1111/j.1572-0241.2001.03790.x
24. Graham DY, Tansel A. Interchangeable use of proton pump inhibitors based on relative potency. Clin Gastroenterol Hepatol. 2018;16(6):800–808 e807. doi:10.1016/j.cgh.2017.09.033
25. Gardner J, Perdomo C, Sloan S, et al. Integrated acidity and rabeprazole pharmacology. Aliment Pharmacol Ther. 2002;16(3):455–464. doi:10.1046/j.1365-2036.2002.01158.x
26. Schindlbeck NE, Heinrich C, König A, Dendorfer A, Pace F, Müller-Lissner SA. Optimal thresholds, sensitivity, and specificity of long-term pH-metry for the detection of gastroesophageal reflux disease. Gastroenterology. 1987;93(1):85–90. doi:10.1016/0016-5085(87)90318-0
27. Smith JL, Opekun AR, Larkai E, Graham DY. Sensitivity of the esophageal mucosa to pH in gastroesophageal reflux disease. Gastroenterology. 1989;96(2):683–689. doi:10.1016/S0016-5085(89)80065-4
28. Hunt RH. Importance of pH control in the management of GERD. Arch Intern Med. 1999;159(7):649–657. doi:10.1001/archinte.159.7.649
29. Evans D, Pye G, Bramley R, Clark A, Dyson T, Hardcastle J. Measurement of gastrointestinal pH profiles in normal ambulant human subjects. Gut. 1988;29(8):1035–1041. doi:10.1136/gut.29.8.1035
30. Hellstrom PM, Gryback P, Jacobsson H. The physiology of gastric emptying. Best Pract Res Clin Anaesthesiol. 2006;20(3):397–407. doi:10.1016/j.bpa.2006.02.002
31. Hammer J, Schmidt B. Effect of splitting the dose of esomeprazole on gastric acidity and nocturnal acid breakthrough. Aliment Pharmacol Ther. 2004;19(10):1105–1110. doi:10.1111/j.1365-2036.2004.01949.x
32. Fass R, Inadomi J, Han C, Mody R, O’Neil J, Perez MC. Maintenance of heartburn relief after step-down from twice-daily proton pump inhibitor to once-daily dexlansoprazole modified release. Clin Gastroenterol Hepatol. 2012;10(3):247–253. doi:10.1016/j.cgh.2011.11.021
33. Katsube T, Adachi K, Kawamura A, et al. Helicobacter pylori infection influences nocturnal gastric acid breakthrough. Aliment Pharmacol Ther. 2000;14(8):1049–1056. doi:10.1046/j.1365-2036.2000.00799.x
34. Verdu E, Armstrong D, Fraser R, et al. Effect of Helicobacter pylori status on intragastric pH during treatment with omeprazole. Gut. 1995;36(4):539–543. doi:10.1136/gut.36.4.539
35. Fukuchi T, Ashida K, Yamashita H, et al. Influence of cure of Helicobacter pylori infection on gastric acidity and gastroesophageal reflux: study by 24-h pH monitoring in patients with gastric or duodenal ulcer. J Gastroenterol. 2005;40:350–360. doi:10.1007/s00535-004-1552-1
36. Haruma K, Mihara M, Okamoto E, Kusunoki H, Hananoki M, Tanaka S. Eradication of Helicobacter pylori increases gastric acidity in patients with atrophic gastritis of the corpus—evaluation of 24-h pH monitoring. Aliment Pharmacol Ther. 1999;13:155–162. doi:10.1046/j.1365-2036.1999.00459.x
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.