Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 18
Perspectives and Attitudes of General Practitioners Towards Pharmacological and Non-Pharmacological COPD Management in a Belgian Primary Care Setting: A Qualitative Study
Authors Leemans G ![]() , Vissers D
, Vissers D ![]() , Ides K, Van Royen P
, Ides K, Van Royen P ![]()
Received 4 July 2023
Accepted for publication 16 August 2023
Published 25 September 2023 Volume 2023:18 Pages 2105—2115
DOI https://doi.org/10.2147/COPD.S423279
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Min Zhang
Glenn Leemans,1 Dirk Vissers,1 Kris Ides,2– 4 Paul Van Royen5
1Department of Rehabilitation Sciences and Physiotherapy, Faculty of Medicine and Health Sciences, University of Antwerp, Wilrijk, Belgium; 2Cosys-Lab, Flanders Make, University of Antwerp, Antwerp, Belgium; 3Laboratory of Experimental Medicine and Pediatrics, Faculty of Medicine and Health Sciences, University of Antwerp, Wilrijk, Belgium; 4Department of Pediatrics, Antwerp University Hospital, Edegem, Belgium; 5Department of Family Medicine and Population Health, University of Antwerp, Wilrijk, Belgium
Correspondence: Glenn Leemans, Department of Rehabilitation Sciences and Physiotherapy, Faculty of Medicine and Health Sciences, University of Antwerp, Universiteitsplein 1, Wilrijk, 2610, Belgium, Tel +32 495 34 84 59, Email [email protected]
Background: Chronic obstructive pulmonary disease (COPD) is a complex and heterogeneous condition that requires multidisciplinary management. In Belgium, the treatment of COPD is mainly managed by general practitioners (GPs). Several clinical practice guidelines (CPGs) recommend the use of non-pharmacological treatments, such as pulmonary rehabilitation, and interdisciplinary care for COPD patients. Although considerable research has been devoted to addressing the multitude of reasons for the lack of adherence to these aspects of the CPGs, less attention has been paid to understanding the perspectives and attitudes of GPs that lead to this suboptimal implementation.
Purpose: This study aimed to 1) explore Belgian GPs’ perceptions regarding COPD management in a primary care setting and 2) collect their views on the importance of pulmonary rehabilitation and interprofessional care in COPD management.
Methods: A descriptive study, conducted between August 2014 and May 2015, used interviews from a sample of 30 Flemish GPs. Data were analyzed following the principles of thematic analysis.
Results: COPD management was patient-centered, focusing on immediate symptom relief and reducing future risks through pharmacotherapy and proper patient education. Deviations from the CPGs were noted, with only a few GPs performing spirometry themselves. Conditions to prescribe respiratory physiotherapy were not well known. Some GPs remained unconvinced about the (cost-)effectiveness of respiratory physiotherapy despite the fast-expanding scientific evidence. Interprofessional care was limited to GP-respiratory physician (re)-referral and communication. GPs showed a reactive attitude towards interprofessional collaboration for non-pharmacological therapies, which is not in line with the proactive approach recommended in CPGs.
Conclusion: GPs managed COPD patients mainly by reducing symptoms with pharmacological therapy. Integrated care regarding non-pharmacological treatments was not well implemented due to the obstacles in interprofessional collaboration. Future care models incorporating personalized care planning could provide a solution to manage COPD’s complex healthcare demands.
Keywords: asthma/COPD management, family medicine, non-pharmacologic treatment, pulmonary rehabilitation, interdisciplinary care, thematic analysis
Introduction
Chronic obstructive pulmonary disease (COPD) is a highly prevalent chronic respiratory condition, defined by persistent airflow limitation. It constitutes a major public health problem and is currently the third leading cause of death worldwide.1 The most critical risk factor for COPD is tobacco smoking. Other risk factors include occupational exposures, chemical agents and fumes, and indoor and outdoor air pollutants. The patient’s genetic profile, asthma, malnutrition, aging, and low socioeconomic status also contribute to disease development.2 Clinical manifestations of COPD include persistent and progressive dyspnea, cough with sputum production, fatigue, and recurrent lower respiratory tract infections.3 COPD is associated with a significant reduction in physical activity and psychological problems, all of which contribute to the patient’s disability and poor health-related quality of life (QoL).4 In addition, COPD patients frequently experience exacerbations due to pulmonary infections. These exacerbations contribute to the worsening of their symptoms, and further loss of function, and often require hospital treatment or, in more severe cases, admission to intensive care units. For all these reasons, COPD is among the leading causes of disability-adjusted life years (DALYs) worldwide, imposing a substantial economic burden on healthcare systems.5,6
In Belgium, the majority of COPD management is provided by general practitioners (GPs) who focus on reducing the impact of chronic respiratory patients, both in terms of clinical burden and healthcare utilization, even in the early stage of the disease.7,8 GPs play a central role in the coordination and continuity of care, particularly in such patient-centered models.9 Furthermore, managing COPD requires a personalized and patient-centered approach, addressing the physical, emotional, and social functioning of each patient and empowering them and their families to actively collaborate with an interdisciplinary healthcare team.10–12
Since the late 1990s, evidence-based clinical practice guidelines (CPGs) have been developed to improve the diagnosis, management, and prevention of COPD, providing a comprehensive review of the diagnostic process and severity classification to start an effective pharmacological and/or non-pharmacological treatment.13 Pharmacological therapy accounts for a substantial portion of the resources used in the long-term management of COPD patients, increasing with disease severity, especially during acute exacerbations. However, non-pharmacological treatments such as smoking cessation, pulmonary rehabilitation (PR), and vaccination have been increasingly recommended as essential elements of therapy to promote self-efficacy and relieve symptoms. Such options also improve QoL and are cost-effective.14
It is well known that COPD patients demonstrate reduced levels of spontaneous physical activity when compared to healthy individuals. This difference is even more striking in patients receiving long-term oxygen therapy or with advanced stages of the disease. These patients would greatly benefit from PR: a multidisciplinary program that includes supervised exercise training, education, and psychological support, recommended by international CPGs to reduce COPD patients’ disabilities and improve their QoL.15 Indeed, PR is the most effective therapeutic strategy for improving shortness of breath, health status, and exercise tolerance.3 In addition, airway clearance techniques are recommended in several CPGs as a non-pharmacological treatment option performed by respiratory physiotherapists for patients with evidence of excessive sputum production.14,16–18 Despite all of this, there is significant variability in GPs’ adherence to these CPGs and their implementation in real-life clinical practice.19,20
Although considerable research has been devoted to addressing the multitude of reasons for the lack of adherence to these CPGs, less attention has been paid to understanding the perspectives and attitudes of GPs that lead to this suboptimal implementation.21
Therefore, the main aim of this qualitative study was to gain more insight into the perspectives and attitudes of GPs on the management of COPD in a primary care setting. Secondly, we proposed to collect their views on the importance of PR and interprofessional care in COPD management.
Materials and Methods
Study Setting
This study was conducted in the region of Antwerp, Flanders, Belgium. Here, the majority of COPD patients are monitored in primary care units, managed by a GP. GPs work primarily as independent, self-employed healthcare professionals in independent medical practices. The Belgian healthcare system is financed by social health insurance where patients pay a basic fee to healthcare professionals, and most costs are reimbursed by state-funded health insurers. Primary medical care is mainly private and based on the principles of independent medical practice. Independent GPs, and other healthcare professionals, including physiotherapists, are remunerated on a fee-for-service basis, with patients having a free choice of doctor. Every patient has free access to a medical specialist and hospital care, even as their first point of contact. There is no strict referral system between GPs and other specialists.22
Participant Recruitment
GPs were invited to participate in the study through the University of Antwerp network of GP practices, a symposium on multidisciplinary respiratory care, or the researchers’ local primary care networks. From this group of potential participants, a diverse purposeful sub-sample was selected: a mix of GPs based on gender, years of experience, and types of practice (solo, group, or multidisciplinary independent medical practice). Interested GPs were emailed the information leaflet explaining the reasons for the study and the potential uses of the results obtained from the study. All GPs provided written informed consent.
Study Design and Data Generation
A qualitative study with semi-structured interviews was conducted with the recruited GPs using a topic guide with prompts to answer the research questions (Supplementary Table 1). The topic guide consisted of seven major topics developed from the existing literature on COPD management.23–25 The interviews were carried out by two postgraduate medical students (L.T. and L.B.) and two undergraduate physiotherapy students (C.A. and B.B.) at the University of Antwerp, with close support and training from G.L. and P.V.R. Regular team meetings were held throughout the study to review transcripts and refine the interview technique. GPs were asked how they make a diagnosis and treat patients with COPD, including prescribed medication, vaccinations, patient education, smoking cessation, and the challenges they face in changing their patients’ health behavior to achieve treatment compliance. Specific questions about respiratory physiotherapy ranged from airway clearance techniques (ACT) to PR. In addition, GPs’ experiences with interprofessional care were explored. Finally, participants were asked to provide their insights on how to improve COPD management in the future. All interviews were digitally audio-recorded and transcribed verbatim. There was no repetition of interviews. Field notes taken after each interview were also used to record relevant contextual issues.
Data Analysis
All transcripts were analyzed using a thematic analysis approach.26 Firstly, each transcript was read to familiarize the research team with the data, and text sections were coded. In the initial stages of the analysis, a provisional coding framework was developed based on the issues addressed in the topic guide. Codes were then aggregated into major themes and subthemes using NVivo 10 (QSR international). Following regular discussions with the research team, the coding framework was continuously refined to include new themes and subthemes identified as the transcripts were reread to reflect the entire data set (see Supplementary Table 2 for the final coding framework). The consolidated criteria for reporting qualitative research (COREQ) were used to guide reporting (Supplementary Table 3).27
Ethics
The study was conducted in compliance with the approved protocol, the Declaration of Helsinki, and all applicable local regulatory requirements and was approved by the Ethics Committee of the Antwerp University Hospital with approval 14/21/232. All participants provided written informed consent before data collection, including using their anonymized responses to present the research findings.
Results
A total of 30 GPs participated in face-to-face interviews between August 2014 and May 2015, of whom 16 (53.0%) were female. The participants had a median working experience of 15.5 years, ranging from 2 to 39 years. All interviews lasted about 30 minutes and took place at the GPs workplace: 5 (16.7%) in a solo practice, 15 (50.0%) in a group practice, and 10 (33.3%) in a multidisciplinary medical center. As for the size of the GPs practice list (total number of registered patients), they were distributed as follows: 14 (46.7%) with <5000 patients, 6 (20%) with 5000–10,000 patients, and 3 (10%) with >10,000 patients (Table 1).
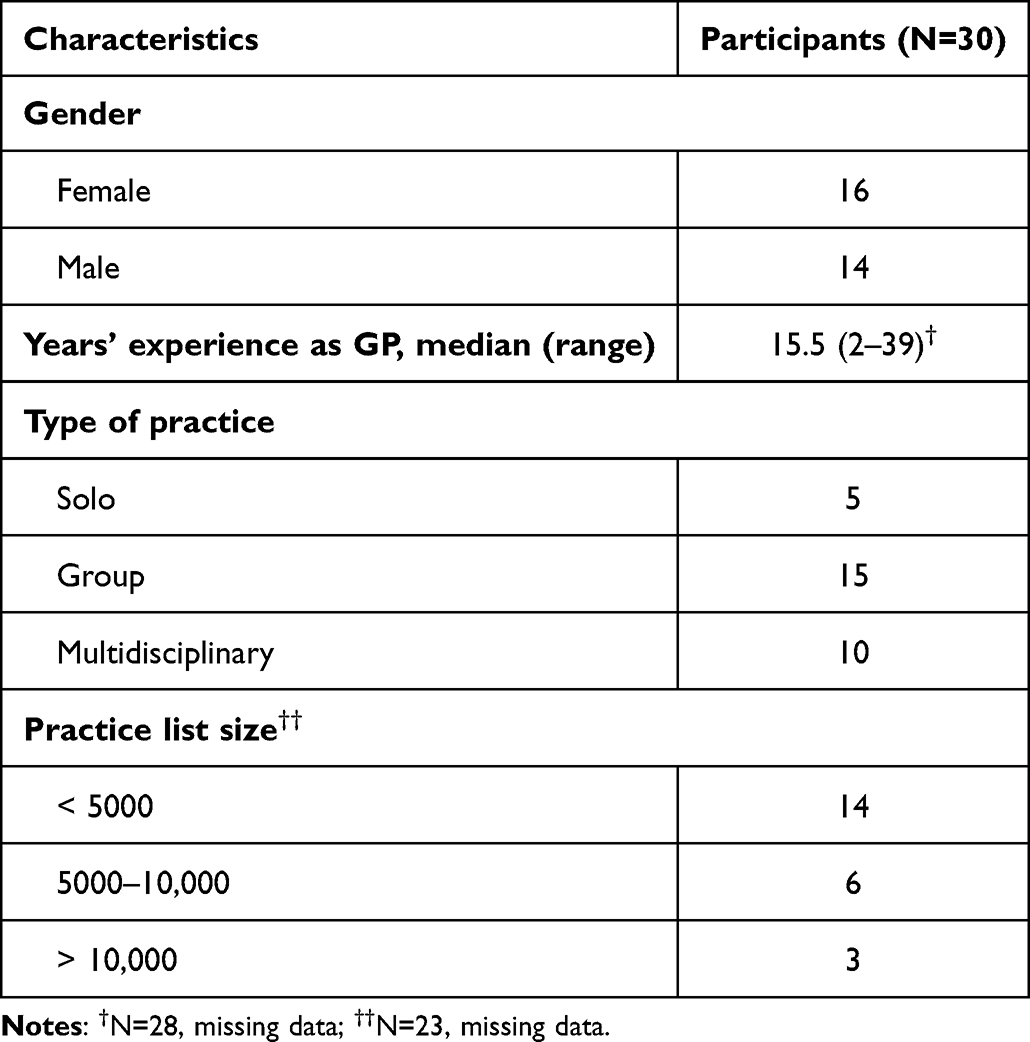 |
Table 1 Participants’ Characteristics |
Three major themes were developed during the thematic analysis (Figure 1) to fulfill the main goal of the study: 1) COPD management and challenges in primary care, 2) GPs’ experience and perspectives on respiratory physiotherapy and PR, and 3) GP’s view on interprofessional care.
 |
Figure 1 Main themes and subthemes. Abbreviation: GPs, general practitioners. |
COPD Management and Challenges in Primary Care
The participants guided their diagnostic approach based on the likelihood of the patient developing COPD, considering their clinical history. Patients with a high probability of COPD had a history of smoking, chronic cough, progressive dyspnea, and recurrent bronchitis. Although the guidelines prescribe spirometry as a first step to diagnose and classify the severity of COPD, disease management by GPs was initially driven by patients’ symptoms and clinical characteristics. Also, while performing spirometry is encouraged by Belgian health authorities with postgraduate training, most GPs did not regularly perform these technical examinations due to organizational problems.
All GPs stated that their COPD management strategy consists of improving quality of life and functional status by reducing immediate symptoms, to improve long-term outcomes and reduce further risks.
The main goal is that the disease doesn’t get any worse and that the patient can go through life comfortably [GP 26]
The aim of improving long-term outcomes was achieved through various treatment modalities, whether in combination or not. Many GPs started their initial pharmaceutical treatment in accordance with the existing CPGs, starting with short-acting bronchodilators and adding long-acting muscarinic (LAMA), long-acting β2-agonist (LABA), or combination inhalers, according to the patient’s needs. Corticosteroids were prescribed during exacerbations, with or without the use of antibiotics.
The participants believed that therapy compliance was related to the severity of COPD and the experienced symptoms. Several GPs declared that treatment compliance would temporarily increase during exacerbations, but subsequently decline during recovery. On the contrary, some GPs found greater compliance in less severe COPD patients, as this subpopulation experienced an enhanced positive effect of their inhaled medications due to a larger preserved bronchodilator reversibility.
In addition to pharmacological therapy, multiple GPs believed that proper patient education is the driving force for behavioral change, a crucial factor in COPD management. However, despite all efforts, GPs found it difficult to motivate patients.
The better informed you are as a patient, the more you understand the problem and the more you can act on it. [GP 30]
Educational topics included smoking as a causative factor for developing COPD, and the pathophysiology of COPD and its related symptoms. Another important educational topic was related to the correct use of inhalation devices.
Regarding future risk reduction, participants focused on smoking cessation, vaccination, and general health promotion, such as encouraging daily physical activity.
All GPs believed smoking cessation is a vital disease modifier for slowing the progression of the disease and improving its prognosis.
That is the only thing that can stop the progress of the disease! [GP 23]
The cheapest medicine is to quit smoking. [GP 20]
Smoking cessation counseling provided by GPs was accomplished through a combination of cognitive behavioral therapies and pharmacological support.
Other challenges perceived by GPs that influenced disease management were patients’ financial status, social background, health literacy, and reimbursement strategies for prescribed therapies. Some participants expressed concern that patients’ financial ability influenced compliance, such as the cost of the inhaled medications, while others disagreed since many medicines were reimbursed. Some participants felt that the current reimbursement strategies were too focused on spirometry alone and, therefore, not aligned with the complex clinical presentation of patients.
…and that is one of the big problems, no two COPD patients are the same, of course. If a patient says: ‘I have an exacerbation three times a week’, even though he has a wonderful spirometry report, you have to act accordingly. [GP 8]
GP’s Experiences and Perspectives on Respiratory Physiotherapy and Pulmonary Rehabilitation
First, it is important to mention that only a minority of the participants were aware of the benefits of respiratory physiotherapy in COPD, having previously prescribed it based on the patient’s symptoms or disease severity. Moreover, several GPs believed that there is a lack of scientific evidence to support its use and thus did not prescribe it.
I have the impression that the scientific evidence is not very strong for physical therapy for exercises, breathing exercises, asthma exercises. [GP 8]
Other barriers to why most interviewees rarely prescribed respiratory physiotherapy were related to patient motivation, organizational aspects such as transportation to the private practice or hospital, often linked to patients’ financial status, and reimbursement policies. One aspect mentioned by several GPs is that the relationship between physiotherapy and the expected benefits was difficult for patients to understand, as respiratory physiotherapy does not provide immediate symptom relief like pharmacological treatments.
…and there is often no direct link. If they take a puff, yes. But after the physiotherapy treatment, they often say: I do not feel better, I do not feel worse, but I do feel worse because I had to take a taxi and I lost a lot of money. [GP 8]
Nevertheless, various GPs believe that their patients have improved with physiotherapy in the long-term, clearly objectified by improving their exercise tolerance. Therefore, multiple GPs stated that they prescribe physiotherapy in the context of COPD treatment, now more than before.
As for the benefits of PR, opinions were divided. While some recognize the value of PR, for other GPs, this treatment modality does not offer more benefits than unsupervised training.
I think that PR has no more effect than saying, for example, go outside for some cycling. [GP 4]
Some GPs also believe that prescribing non-pharmacological treatment options like PR is the responsibility of the respiratory physician.
I only start respiratory physiotherapy during an exacerbation, like chest percussion, to improve the comfort of the patient. But I do not think I have ever really started rehabilitation myself. The respiratory physician always starts that. [GP 18]
GP’s Views on Interprofessional Care and Future Perspectives on COPD Management
In general, all participating GPs believed that in an interdisciplinary setting, they play a central role in the coordination and continuity of care for COPD patients. Hence, GPs perceived themselves as the leading primary care providers with a distinct view of a patient’s health care. However, they did not want to be responsible for implementing all interprofessional decisions and related actions.
I think the GP should be aware of everything and be able to follow everything, but that doesn’t mean he should do everything. [GP 1]
Several GPs indicated that they would only refer to other healthcare professionals when their current management strategies cannot improve patients’ symptoms or prevent further disease progression. Despite being satisfied with the current interprofessional care, mainly focused on re-referral between the GP and respiratory physician, some participants admitted that communication and cooperation with other healthcare professionals were not frequent and should be optimized.
I do think that more could be achieved through good cooperation between the pneumologist, the general practitioner and the physiotherapist. [GP 30]
Concerning referral to a physiotherapist, only a minority of the GPs knew to whom they must refer. Others believed that every physiotherapist could provide respiratory physiotherapy, so it did not matter to whom they referred.
But I think most physiotherapists know the basics of that, right? I hope! [GP 19]
Concerning interprofessional care for non-pharmacological treatments, some GPs believed that this is only needed when problems arise in the current management of COPD patients. However, they also stated that this belief is a possible reason why interprofessional care often starts too late.
Several topics were discussed regarding the participants’ opinions on how to improve COPD chronic management in the future. Firstly, most GPs believed that the Belgian government should be more focused on preventing smoking-related diseases like COPD. Secondly, GPs would like to improve their practice management, including having dedicated healthcare professionals perform technical assessments such as spirometry. Thirdly, participants would like to gain more scientific evidence within CPGs concerning respiratory physiotherapy and have more information on the non-pharmacological therapy’s indications and reimbursement modalities.
I have no idea how many physiotherapy sessions for COPD are allowed, what is reimbursed and the frequency of therapy. For example: does it have to be every day, does it have to be once a week? I have no idea! [GP 10]
Some even believed that more positive experiences with physiotherapy would lead to more referrals in the future.
[…] because if our experience shows that it actually does help, then I think that is the best incentive. [GP 7]
Lastly, all GPs believed that the existing healthcare system should change to improve interprofessional care. One recommendation was to develop a chronic care plan for COPD due to the complex nature of the disease. Another recommendation was to establish agreements with other healthcare providers to achieve interprofessional collaboration and improve communication between different healthcare professionals.
Discussion
The main goal of this qualitative study was to explore the perceptions and attitudes of Belgian GPs regarding COPD management in a primary care setting. Other underlying objectives included the collection of GPs’ views on the importance of PR and interprofessional care, to identify shortfalls in current primary care practice and find opportunities for more targeted interventions. Our main findings were that GPs report their COPD management as patient-centered, focusing on immediate symptom relief to improve patients’ QoL. Although well-educated in spirometry, GPs did not manage to perform these tests due to organizational challenges. The participating GPs most often choose a pharmacological approach for COPD management. Non-pharmacological treatments, such as respiratory physiotherapy or PR, were hardly known by GPs. Although physiotherapy is only reimbursed in Belgium when prescribed by a GP or a specialist clinician, there seem to be several reasons why GPs did not include respiratory physiotherapy in their chronic care management. Interprofessional care was limited to (re)-referral and communication between GPs and respiratory physicians. GPs generally showed a reactive approach to PR, respiratory physiotherapy and interprofessional collaboration. This attitude is not in line with the proactive approach recommended in CPGs, which aims not only to determine the level of airflow limitation and its impact on the patient’s health status, but also to reduce extrapulmonary symptoms and, just as importantly, to reduce the risk of future events (such as exacerbations, hospital admissions or death). For this, it should be actively sought to appropriately treat concomitant comorbidities, including cardiovascular diseases, skeletal muscle dysfunctions and/or depression/anxiety, among others, as they can influence mortality and the risk for hospitalization independently.16,28,29
Among the main barriers to the implementation of PR in COPD management is the lack of awareness and familiarity with international CPGs. In line with our data, a Swedish study from 2020 highlighted that there is still a considerable gap between treatment guidelines and the actual management of COPD in municipal healthcare,30 confirming the validity of our findings today.
A main recurrent issue in primary care is the lack of spirometry performed by GPs to detect and diagnose COPD,31 contributing to it remaining largely undiagnosed or being diagnosed late in the course of the disease.32 A telephone survey conducted on 197 Flemish GPs in 2006 showed an undoubted interest among GPs in office spirometry; however, they needed educational and financial support to overcome the prevailing barriers in establishing office spirometry on a routine basis.33 Despite national initiatives in Belgium, such as postgraduate spirometry courses and reimbursement of GPs spirometry assessments, our participants still experienced time constraints in performing office spirometry. As indicated by the participants, further financial incentives to have trained staff to assist in practice management would help continue the implementation of office spirometry.
In recent years, the diagnostic focus has been revised to account for COPD’s heterogeneous and complex nature, enabling a more personalized treatment.8,28,34 The results of our study confirm that all interviewed GPs strove to achieve this goal in primary care. Although their focus was primarily on symptom reduction through pharmacological treatments to improve patient’s QoL, they also combined this with general health promotion, education for smoking cessation, and vaccinations as long-term strategies to prevent disease progression. When their current individualized management strategies cannot improve their patients’ symptoms or prevent further disease progression, some GPs have started to provide interprofessional care mainly focused on re-referral between GP and respiratory physician, with satisfying results in the interviewees’ opinions. Nevertheless, current strategies neglect the potential of other personalized measures, such as physical therapy or PR, to prevent and/or treat the disease progression, reducing symptoms, and future risks.
Considering the participants that were familiar with the strong evidence on the advantages of PR in COPD management, some of them believed that this type of treatment does not offer more benefits than unsupervised patient training. Another barrier to prescribing non-pharmacological treatments as part of interprofessional care is the participants’ perception that these therapies are only needed when problems arise in the current management of COPD patients. If the benefit of non-pharmacological treatment, for example respiratory physiotherapy, was not leading to an immediate reduction in symptoms, GPs trusted that COPD patients would often not be motivated to pursue this therapy. In a qualitative study by Molin et al in Denmark, GPs reported similar beliefs about unmotivated patients for non-pharmacological treatments, specifically PR. Molin et al concluded that this perception led to a more reactive approach by the GPs rather than a proactive management to avoid systemic consequences of the disease.35 Finally, the GPs in our study did not know to whom they should refer patients for respiratory physiotherapy, nor what reimbursement modalities were possible in this socio-economic deprived population. These observations are in line with previous reports. A qualitative study conducted in Australia found that 83% of the interviewed GPs had not directly referred COPD patients to PR,36 and the participants identified as the main barriers to referral their low knowledge of PR in the management of COPD, lack of perceived benefit, low comprehension of the referral process, difficulties with access to PR by their patients and questions about the need to educate patients to further promote exercise behavior change. Altogether, these obstacles in the referral process need to be tackled to properly implement respiratory physiotherapy and PR as part of the ideal integrated care described in the CPGs for COPD.
Regarding recommendations to improve the chronic management of COPD, the participating GPs described the need for a chronic care plan that captures the complexity of COPD with its multi-comorbidities. Interprofessional collaboration and the use of shared care plans between all team members and the patient, support the effective management of patients with complex chronic conditions with high demands for care.37 This shared care also provides a possible solution to our participants’ reported frustration with the low compliance of their COPD patients to certain therapies. A systematic review found that personalized care planning improves certain indicators of the patients’ physical and psychological health status and people’s ability to self-manage their condition compared to usual care. While the effects were not significant, they appear to be greater when the intervention is more comprehensive, more intensive, and better integrated into routine care.38 Therefore, it is essential that healthcare systems invest in solutions for chronic disease management in primary care, such as facilitating the provision of adequate interdisciplinary guidelines, education, and resources.21
Strengths and Limitations
Qualitative research enables the exploration of the GPs’ perspectives related to the challenges they experience.39 By using a qualitative approach, this study has provided insights into GPs’ perspectives, attitudes, challenges, and ideas for improvement in the management of COPD. To the extent of our knowledge, this is the first qualitative study on COPD management through the eyes of GPs, including respiratory physiotherapy and interprofessional care, in Belgium. Our study gathered the views of 30 primary care practitioners. This was sufficient to reach data saturation concerning the current management of COPD. Our participants represented a range of experience and practice demography, but all worked in Antwerp, Belgium. The transferability of our findings in the present study is challenged by the context of the study, which may affect its applicability to other healthcare systems. However, the credibility of this study was supported by the high consistency in some of the findings across this wide variety of GPs. Furthermore, the influence of all interviewers in this qualitative study must be considered. Concerning consistency, all interviews were conducted similarly through training in interviewing techniques by the researchers. There was a risk of informant bias, as recruitment was performed through the Antwerp University network of GP practices and at a symposium about multidisciplinary respiratory care. For future research, the experience of GPs with the promising role of technology in chronic disease care should be investigated.40 Remote respiratory assessments in people with COPD are feasible and can improve health-related outcomes when well-integrated with existing healthcare services.41 eHealth technology could also help support self-management by engaging patients in their health and changing health behaviors.42 Koff et al demonstrated that a healthcare delivery model, coupling integrated care with remote monitoring, improved quality of life, exercise capacity, identification of unreported exacerbations, and reduced urgent office visits for people with advanced COPD.43
Conclusion
As described by GPs in this qualitative study, COPD management was mainly focused on improving the functional status of COPD patients through short-term symptomatic relief and reducing the patients’ risk status through pharmacological treatments. Interprofessional care was limited to GP-respiratory physician (re)-referral and communication. Conditions to prescribe respiratory physiotherapy were not well-known by GPs. Furthermore, some GPs remained unconvinced about respiratory physiotherapy’s (cost-)effectiveness, despite the fast-expanding scientific evidence and the recommendations in CPGs. Future research should focus on chronic models of care incorporating personal care planning and new technologies to address COPD’s complex healthcare demands.
Acknowledgments
The authors would like to acknowledge the undergraduate medical students (L.T., L.B) and two undergraduate physiotherapy students (C.A., B.B.) at the University of Antwerp for their help in this qualitative research. The authors thank Carla Gomes (W4Research) for providing medical writing support in accordance with Good Publication Practice (GPP3) guidelines (http://www.ismpp.org/gpp3).
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was not funded.
Disclosure
All authors report no conflicts of interest in this work.
References
1. Adeloye D, Song P, Zhu Y, et al. Global, regional, and national prevalence of, and risk factors for, chronic obstructive pulmonary disease (COPD) in 2019: a systematic review and modelling analysis. Lancet Respir Med. 2022;10(5):447–458. doi:10.1016/S2213-2600(21)00511-7
2. Safiri S, Carson-Chahhoud K, Noori M, et al. Burden of chronic obstructive pulmonary disease and its attributable risk factors in 204 countries and territories, 1990–2019: results from the global burden of disease study 2019. BMJ. 2022:e069679. doi:10.1136/bmj-2021-069679
3. Mccarthy B, Casey D, Devane D, Murphy K, Murphy E, Lacasse Y. Pulmonary rehabilitation for chronic obstructive pulmonary disease. Cochrane Database Syst Rev. 2015;2015(2). doi:10.1002/14651858.CD003793.pub3
4. Corhay JL, Dang DN, Van Cauwenberge H, Louis R. Pulmonary rehabilitation and COPD: providing patients a good environment for optimizing therapy. Int J Chron Obstruct Pulmon Dis. 2013;9:27–39. doi:10.2147/COPD.S52012
5. Martí D, Gimeno-Santos Elena JDM, Gimeno-Santos E. Physical therapy and rehabilitation in chronic obstructive pulmonary disease patients admitted to the intensive care unit. Semin Respir Crit Care Med. 2020;41(06):886–898. doi:10.1055/s-0040-1709139
6. GBD 2017 DALYs and HALE Collaborators. Global, regional, and national disability-adjusted life-years (DALYs) for 359 diseases and injuries and healthy life expectancy (HALE) for 195 countries and territories, 1990–2017: a systematic analysis for the global burden of disease study 2017. Lancet. 2018;392(10159):1859–1922. doi:10.1016/S0140-6736(18)32335-3
7. Clini E, Castaniere I, Tonelli R. Looking for a chronic care model in COPD patients. Eur Respir J. 2018;51(1):1702087. doi:10.1183/13993003.02087-2017
8. Yawn BP, Mintz ML, Doherty DE. GOLD in practice: chronic obstructive pulmonary disease treatment and management in the primary care setting. Int J Chron Obstruct Pulmon Dis. 2021;16:289–299. doi:10.2147/COPD.S222664
9. Valentijn PP, Schepman SM, Opheij W, Bruijnzeels MA. Understanding integrated care: a comprehensive conceptual framework based on the integrative functions of primary care. Int J Integr Care. 2013;13(1):e010. doi:10.5334/ijic.886
10. Franssen FME, Alter P, Bar N, et al. Personalized medicine for patients with COPD: where are we? Int J Chron Obstruct Pulmon Dis. 2019;14:1465–1484. doi:10.2147/COPD.S175706
11. Houben-Wilke S, Augustin IM, Vercoulen JH, et al. COPD stands for complex obstructive pulmonary disease. Eur Respir Rev. 2018;27(148):180027. doi:10.1183/16000617.0027-2018
12. Bodenheimer T, Wagner EH, Grumbach K. Improving primary care for patients with chronic illness. JAMA. 2002;288(15):1909. doi:10.1001/jama.288.15.1909
13. Rodriguez-Roisin R. Twenty Years of GOLD (1997–2017). The Origins; 2019.
14. Clini EM, Ambrosino N. Nonpharmacological treatment and relief of symptoms in COPD. Eur Respir J. 2008;32(1):218–228. doi:10.1183/09031936.00134007
15. Spruit M, Singh SJ, Garvey C, et al. An official American Thoracic Society/European Respiratory Society statement: key concepts and advances in pulmonary rehabilitation. Am J Respir Crit Care Med. 2013;188(8):e13–64. doi:10.1164/rccm.201309-1634ST
16. NICE. Chronic obstructive pulmonary disease in over 16s: diagnosis and management; 2019. Available from: https://www.nice.org.uk/guidance/ng115/chapter/recommendations#physiotherapy.
17. NHG. NHG-Standaard COPD; 2021.
18. Lung Foundation Australia. Australian and New Zealand guidelines for the management of chronic obstruction pulmonary diseases: O6.8 Chest physiotherapy (Airway clearance techniques); 2020. Available from: https://copdx.org.au/copd-x-plan/o-optimise-function/o6-non-pharmacological-interventions/o67-chest-physiotherapy-airway-clearance-techniques/.
19. Albitar HAH, Iyer VN. Adherence to global initiative for chronic obstructive lung disease guidelines in the real world: current understanding, barriers, and solutions. Curr Opin Pulm Med. 2020;26(2):149–154. doi:10.1097/MCP.0000000000000655
20. Miravitlles M, Roche N, Cardoso J, et al. Chronic obstructive pulmonary disease guidelines in Europe: a look into the future. Respir Res. 2018;19(1):1–9. doi:10.1186/s12931-018-0715-1
21. Sehl J, O’Doherty J, O’Connor R, O’Sullivan B, O’Regan A. Adherence to COPD management guidelines in general practice? A review of the literature. Ir J Med Sci. 2018;187(2):403–407. doi:10.1007/s11845-017-1651-7
22. World Health Organization Regional Office for Europe. Creating 21st century primary care in Flanders and beyond; 2019.
23. Billion L, Timmerman L. Description of Primary Care in Non-Hospitalised Patients with COPD in the Province of Antwerp. University of Antwerp; 2016.
24. Global Initiative for Chronic Obstructive Lung Disease. Pocket guide to COPD diagnosis, management, and prevention – a guide for healthcare professionals; 2015.
25. Postma D, Anzueto A, Calverley P, et al. A new perspective on optimal care for patients with COPD. Prim Care Respir J. 2011;20(2):205–209. doi:10.4104/pcrj.2011.00041
26. Braun V, Clarke V. Using thematic analysis in psychology. Qual Res Psychol. 2006;3(2):77–101. doi:10.1191/1478088706qp063oa
27. O’Brien BC, Harris IB, Beckman TJ, Reed DA, Cook DA. Standards for reporting qualitative research: a synthesis of recommendations. Acad Med. 2014;89(9):1245–1251. doi:10.1097/ACM.0000000000000388
28. Global Initiative for Chronic Obstructive Lung Disease. Global strategy for the diagnosis, management and prevention of COPD; 2022.
29. Gupta D, Agarwal R, Aggarwal AN, et al. Guidelines for diagnosis and management of chronic obstructive pulmonary disease: joint ICS/NCCP (I) recommendations. Lung India. 2013;30(3):228–267. doi:10.4103/0970-2113.116248
30. Lundell S, Pesola UM, Nyberg A, Wadell K. Groping around in the dark for adequate COPD management: a qualitative study on experiences in long-term care. BMC Health Serv Res. 2020;20(1). doi:10.1186/s12913-020-05875-2
31. Rose D, Ray E, Summers RH, et al. Case-finding for COPD clinic acceptability to patients in GPs across Hampshire: a qualitative study. NPJ Prim Care Respir Med. 2021;31(1):1–8. doi:10.1038/s41533-021-00216-0
32. Lindberg A, Bjerg-Bäcklund A, Rönmark E, Larsson LG, Lundbäck B. Prevalence and underdiagnosis of COPD by disease severity and the attributable fraction of smoking: report from the obstructive lung disease in Northern Sweden Studies. Respir Med. 2006;100(2):264–272. doi:10.1016/j.rmed.2005.04.029
33. Boffin N, Van der Stighelen V, Paulus D, Van Royen P. Use of office spirometers in Flemish general practice: results of a telephone survey. Monaldi Arch Chest Dis. 2006;65(3):128–132. doi:10.4081/monaldi.2006.557
34. Agustí A, Bafadhel M, Beasley R, et al. Precision medicine in airway diseases: moving to clinical practice. Eur Respir J. 2017;50(4):1701655. doi:10.1183/13993003.01655-2017
35. Molin KR, Egerod I, Valentiner LS, Lange P, Langberg H. General practitioners’ perceptions of COPD treatment: thematic analysis of qualitative interviews. Int J Chron Obstruct Pulmon Dis. 2016;11:1929–1937. doi:10.2147/COPD.S108611
36. Johnston KN, Young M, Grimmer KA, Antic R, Frith PA. Barriers to, and facilitators for, referral to pulmonary rehabilitation in COPD patients from the perspective of Australian general practitioners: a qualitative study. Prim Care Respir J. 2013;22(3):319–324. doi:10.4104/pcrj.2013.00062
37. Van Dongen JJJ, Van Bokhoven MA, Daniëls R, Van Der Weijden T, Emonts WW, Beurskens A. Developing interprofessional care plans in chronic care: a scoping review. BMC Fam Pract. 2016;17(1):1–9. doi:10.1186/s12875-016-0535-7
38. Coulter A, Entwistle VA, Eccles A, Ryan S, Shepperd S, Perera R. Personalised care planning for adults with chronic or long-term health conditions. In: Coulter A, editor. Cochrane Database of Systematic Reviews. John Wiley & Sons, Ltd;2013.
39. Pope C, Van Royen P, Baker R. Qualitative methods in research on healthcare quality. Qual Saf Health Care. 2002;11(2):148–152. doi:10.1136/qhc.11.2.148
40. Milani RV, Bober RM, Lavie CJ. The role of technology in chronic disease care. Prog Cardiovasc Dis. 2016;58(6):579–583. doi:10.1016/j.pcad.2016.01.001
41. Baroi S, McNamara RJ, McKenzie DK, Gandevia S, Brodie MA. Advances in remote respiratory assessments for people with chronic obstructive pulmonary disease: a systematic review. Telemed E Health. 2018;24(6):415–424. doi:10.1089/tmj.2017.0160
42. Schnall R, Rojas M, Bakken S, et al. A user-centered model for designing consumer mobile health (mHealth) applications (apps). J Biomed Inform. 2016;60:243–251. doi:10.1016/j.jbi.2016.02.002
43. Koff PB, Min SJ, Diaz DLP, et al. Impact of proactive integrated care on chronic obstructive pulmonary disease. Chron Obstruct Pulmon Dis. 2020;8(1). doi:10.15326/JCOPDF.2020.0139
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.