Back to Journals » Journal of Asthma and Allergy » Volume 19
Persistent Airflow Limitation in Asthma: Clinical Characteristics, Risk Factors, and Long−term Outcomes from a Multicenter Cohort Study
Authors Lee JK ![]() , Lee HW
, Lee HW ![]() , Lee CH
, Lee CH ![]() , Choi JY
, Choi JY ![]() , Jang JG
, Jang JG ![]() , Rhee CK
, Rhee CK ![]() , Park YB
, Park YB ![]() , Lim SY
, Lim SY ![]() , Yoo KH
, Yoo KH ![]() , Kim DK
, Kim DK ![]()
Received 19 March 2026
Accepted for publication 3 July 2026
Published 9 July 2026 Volume 2026:19 603856
DOI https://doi.org/10.2147/JAA.S603856
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Amrita Dosanjh
Jung-Kyu Lee,1 Hyun-Woo Lee,1 Chang Hoon Lee,2 Joon Young Choi,3 Jong Geol Jang,4 Chin Kook Rhee,5 Yong Bum Park,6 Seong Yong Lim,7 Kwang Ha Yoo,5 Deog Kyeom Kim1
1Division of Pulmonary and Critical Care Medicine, Department of Internal Medicine, Seoul Metropolitan Government-Seoul National University Boramae Medical Center, Seoul National University College of Medicine, Seoul, Republic of Korea; 2Division of Pulmonary and Critical Care Medicine, Department of Internal Medicine, Seoul National University Hospital, Seoul National University College of Medicine, Seoul, Republic of Korea; 3Division of Pulmonary and Critical Care Medicine, Department of Internal Medicine, Incheon St. Mary’s Hospital, The Catholic University of Korea College of Medicine, Seoul, Republic of Korea; 4Division of Pulmonology and Allergy, Department of Internal Medicine, Yeungnam University Medical Center, Yeungnam University College of Medicine, Daegu, Republic of Korea; 5Division of Pulmonary, Allergy and Critical Care Medicine, Department of Internal Medicine, Konkuk University School of Medicine, Seoul, Republic of Korea; 6Division of Pulmonary, Allergy and Critical Care Medicine, Department of Internal Medicine, Kangdong Sacred Heart Hospital, Hallym University, Seoul, Republic of Korea; 7Division of Pulmonary and Critical Care Medicine, Department of Medicine, Kangbuk Samsung Hospital, Sungkyunkwan University School of Medicine, Seoul, Republic of Korea
Correspondence: Deog Kyeom Kim, Division of Pulmonary and Critical Care Medicine, Department of Internal Medicine, Seoul Metropolitan Government-Seoul National University Boramae Medical Center, Seoul National University College of Medicine, 20 Boramaero-5-Gil, Dongjak-Gu, Seoul, 07061, Republic of Korea, Tel +82 2 870 2228, Email [email protected]
Background: Persistent airflow limitation (PAL) is an increasingly recognized asthma phenotype, but its prevalence, determinants, and prognostic significance in real-world settings remain unclear. This study evaluated the clinical characteristics and long-term outcomes associated with PAL and its severity in asthma.
Methods: Multicenter analysis of combined retrospective and prospective cohorts in South Korea. PAL was defined as post-bronchodilator FEV1/FVC < 0.70; severity was graded by STaging of Airflow obstruction by Ratio classification (STAR stage). Outcomes included subsequent exacerbations and longitudinal lung function change.
Results: Among 849 patients with asthma, 640 (75.4%) had PAL. PAL was associated with older age, male sex, lower body mass index, higher smoking intensity, lower FEV1, history of tuberculosis, and less frequent allergic rhinitis. Optimal predictors of PAL were FEV1 ≤ 83.7% predicted, age ≥ 63.5 years, and smoking intensity ≥ 9.5 pack-years. During follow-up, severe exacerbations occurred more frequently in the PAL group (13.0% vs 5.7%) with a 1.8-fold higher incidence (IRR 1.77, 95% CI 1.13– 2.79). Risk increased with PAL severity, particularly at STAR stage 4 vs stage 0 (aHR 3.32, 95% CI 1.60– 6.89). Longitudinally, annual FEV1 decline was slower in PAL than in non-PAL (− 28.1 vs − 42.5 mL/year, P = 0.028), but within PAL, STAR stage 4 showed relatively faster declines in both FEV1 and FVC.
Conclusion: PAL and its severity independently predict the risk of severe exacerbations and progressive lung function decline in asthma, underscoring PAL as a key marker of disease progression and a potential target for early intervention.
Keywords: asthma, persistent airflow limitation, exacerbation, lung function
Introduction
Asthma is a heterogeneous chronic airway disease characterized by variable respiratory symptoms and reversible airflow limitation. However, in a subset of patients, persistent airflow limitation (PAL) may develop despite appropriate treatment, reflecting disease progression and structural changes within the airways. PAL, also referred to as fixed or incompletely reversible airflow limitation, is defined as a reduced post-bronchodilator FEV1/FVC ratio that persists despite adequate therapy, and is commonly identified by a post-bronchodilator FEV1/FVC ratio below 0.70. PAL in asthma has been increasingly recognized as a clinically important phenotype, with evidence indicating its association with accelerated lung function decline and a more severe disease trajectory.1
The pathogenesis of PAL in asthma is believed to involve repeated airway inflammation leading to airway remodeling, including subepithelial fibrosis, smooth muscle hypertrophy, and mucus hypersecretion. These structural changes contribute to a fixed component of airflow obstruction that is not fully reversible with bronchodilator therapy.2,3 Patients with PAL often exhibit more frequent exacerbations, greater symptom burden, and poorer quality of life compared to those with fully reversible airflow limitation.4,5 Recent studies have also identified specific clinical and biological factors—such as male sex, older age at onset, type 2 inflammation, and small airway dysfunction—as being associated with the development of PAL.1,6
This study aimed to analyze the presence and severity of PAL in patients with asthma using real-world cohort data, with a focus on the clinical characteristics, associated factors, and long-term clinical outcomes. Accordingly, this study sought to characterize the phenotypic features and clinical trajectories of asthma patients with and without PAL, thereby enhancing the understanding of this phenotype and informing individualized management strategies to lessen its impact on disease progression and clinical outcomes.
Materials and Methods
Study Design and Participants
A multicenter cohort study was conducted using both retrospective and prospective data. The retrospective cohort enrolled adult patients with asthma from two tertiary hospitals in South Korea between January 2013 and December 2019. Inclusion criteria for this retrospective cohort were as follows: (1) a confirmed diagnosis of asthma based on variable expiratory airflow limitation demonstrated by pulmonary function tests (positive bronchodilator response, positive bronchial provocation test, or significant within-subject variability in lung function); (2) radiological evaluation with at least one chest computed tomography (CT) scan; and (3) availability of at least two spirometric assessments during follow-up. Asthma diagnosis was made according to the Global Initiative for Asthma (GINA) guidelines at the time of enrollment (Table S1).7 All patients fulfilled the GINA criteria for asthma on the basis of a history of characteristic respiratory symptoms together with objectively documented variable expiratory airflow limitation — a positive bronchodilator response, a positive bronchial provocation test, or significant within-subject variability in lung function — which represents the defining feature distinguishing asthma from COPD. All diagnoses were established and confirmed by respiratory specialists at tertiary referral centers. Patients with a follow-up period less than 12 months were excluded to ensure adequate evaluation of long-term outcomes. A portion of the retrospective cohort used in the present study was previously analyzed in a study evaluating the impact of coexisting bronchiectasis on asthma outcomes.8 In the present analysis, we incorporated updated and extended follow-up data, extending the observation period through December 2023. During preparation of the analytic dataset, the registry was systematically reviewed to improve data consistency and accuracy: continuous variables were screened for outliers and physiologically implausible values, missing data were identified and checked against the source records, and all spirometric measurements were re-verified. Discrepancies identified during this process were corrected by reference to the primary medical records.
In addition, data from an ongoing multicenter prospective cohort of patients with severe asthma were merged with the retrospective cohort to increase sample size and enhance the generalizability of the findings. This prospective cohort was derived from Korean participants of the International Severe Asthma Registry (ISAR) cohort, an ongoing global prospective observational cohort of patient s with severe asthma.9,10 Patients with severe asthma have been consecutively enrolled from 8 tertiary referral hospitals since April 2018, and data collected through August 2023 were included in the present analysis. Inclusion criteria for the ISAR cohort are detailed in Box S1, and has been published previously.9
PAL was defined as a post-bronchodilator forced expiratory volume in 1 second (FEV1)/ forced vital capacity (FVC) ratio less than 0.70 at baseline spirometry. Although PAL was classified at baseline spirometry, all patients with serial pulmonary function tests were assessed for the temporal stability of the FEV1/FVC ratio. The baseline classification was consistently maintained across up to five sequential tests over a mean follow-up of approximately four years (Table S2 and Figure S1), confirming that it reflected persistent rather than transient airflow limitation. To further stratify airflow obstruction severity, patients were categorized according to the STaging of Airflow obstruction by Ratio severity classification (STAR stage).11 STAR stage was originally developed as an index to evaluate the progression of obstructive ventilatory disorder in general population and patients with COPD, based on changes in the FEV1/FVC ratio.12 Previous studies have demonstrated that higher STAR stages are associated with increased lung hyperinflation and air trapping.11 In the present study, we assessed the severity of PAL using the STAR stage, which categorizes patients according to the FEV1/FVC ratio as follows: stage 1, ≥0.60 to <0.70; stage 2, ≥0.50 to <0.60; stage 3, ≥0.40 to <0.50; and stage 4, <0.40. Smoking intensity was expressed as pack-years, where one pack-year was defined as smoking 20 cigarettes (one standard cigarette pack) per day for one year. The Charlson comorbidity index was estimated to assess the burden of underlying comorbidities of participants.13 Baseline CT scans were reviewed to evaluate relevant structural abnormalities that could contribute to the progression of obstructive ventilatory disorder, with a particular focus on the presence and extent of bronchiectasis and tuberculosis (TB)-destroyed lung.14,15 TB-destroyed lung was defined as parenchymal destruction involving at least one lobe, presumed to be associated with a prior history of TB.16 A history of TB and TB-destroyed lung were reviewed and retained in the analysis, because prior TB is a recognized contributor to development of chronic airflow obstruction, and may therefore represent a clinically relevant determinant of PAL.16,17 Given that South Korea is a region of intermediate TB burden, in which prior TB and TB-destroyed lung are common among patients with asthma, these patients were retained to preserve the generalizability of the findings to the real-world asthma population.
Ethics Statement
All study procedures were approved by the Institutional Review Boards of the participating institutions. Written informed consent was obtained from all participants in the prospective cohort. For the retrospective cohort, written informed consent was waived because the analysis was based on anonymized retrospective data. The conduct of this study and the confidentiality of patient data were maintained in accordance with the Declaration of Helsinki.
Outcomes
The primary outcome was the annual incidence of subsequent moderate-to-severe acute exacerbations. Exacerbations were defined as an episode characterized by changes from the patient’s previous status, which required additional treatment.18 A moderate exacerbation was defined as a worsening of asthma symptoms requiring systemic corticosteroids, whereas a severe exacerbation was defined as an event necessitating hospitalization or emergency department visit. A frequent exacerbator was regarded as a patient with a history of two or more moderate-to-severe acute exacerbations per year.19 In addition, clinical courses after study enrollment were reviewed to assess the time-to-first exacerbation according to the presence and severity of PAL, stratified by exacerbation severity.
The secondary outcome was the longitudinal change in lung function. Repeated spirometric measurements after cohort enrollment were analyzed to evaluate lung function decline over time according to the presence and severity of PAL.
Statistical Analysis
Between-group differences were evaluated using the chi-square test or Fisher’s exact test for categorical variables and t-test or Wilcoxon rank-sum test for continuous variables. Associations between PAL and clinical variables were analyzed using binary logistic regression. Receiver operating characteristic (ROC) curve analysis was conducted to assess whether the identified variables could predict PAL and to determine the optimal cut-off values of each variable that maximized predictive accuracy. The associations between these variables, defined by their optimal cut-off values, and PAL were subsequently evaluated using multivariable binary logistic regression adjusted for other clinical factors. The annualized incidence rate of acute exacerbations during follow-up was analyzed using negative binomial regression. Time-to-first subsequent exacerbation after study enrollment was evaluated with Kaplan–Meier curves and Cox proportional hazards regression. A restricted cubic spline model was applied to explore the potential non-linear relationship between lung function index and the risk of subsequent severe exacerbations. The estimated hazard ratio was derived from a Cox proportional hazards regression model using a restricted cubic spline function. Longitudinal changes in lung function were assessed using linear mixed-effects models, adjusted for age, sex, and baseline lung function. A two-tailed P value <0.05 was considered statistically significant. Statistical analyses were performed using SPSS software (version 26.0; IBM Corp., Armonk, NY, USA) and R statistical software (version 4.4.2).
Results
Baseline Characteristics of Study Population
A total of 849 patients with asthma were included in this study, comprising 667 from the retrospective cohort and 182 from the prospective cohort. Of these, 640 patients (75.4%) had PAL at baseline, while 209 patients (24.6%) did not. Notably, the baseline PAL classification was temporally stable: in the PAL group, the FEV1/FVC ratio remained below 0.70 at every subsequent assessment across serial pulmonary function tests, and none reverted to a non-obstructive pattern, whereas it remained above 0.70 throughout in the non-PAL group (Table S2 and Figure S1). The distribution of the study population based on airflow limitation severity was further categorized using the STAR stage classification derived from baseline FEV1 and FEV1/FVC ratio (Figure S2). STAR 0 represented patients without PAL, whereas STAR stages 1 through 4 denoted increasing severity among those with PAL, demonstrating substantial heterogeneity in airflow limitation.
Baseline demographic and clinical characteristics of the study population are presented in Table 1. Patients in PAL group was significantly older, predominantly male, had a lower body mass index (BMI), and demonstrated a higher prevalence of ever-smokers and greater smoking intensity compared with non-PAL group. The comorbidity index was similar between the groups; however, PAL group had a significantly higher prevalence of prior TB and a lower prevalence of allergic rhinitis. Compared with non-PAL group, PAL group exhibited significantly lower FEV1 and FEV1/FVC ratio, but higher FVC, and tended to have lower fractional exhaled nitrogen oxide (FeNO) levels, although the difference was not statistically significance. On baseline CT, the prevalence of bronchiectasis was similar, but TB-destroyed lung, although present in only a small proportion of patients, was significantly more frequent in PAL group (28 (5.3%) vs 1 (0.7%); P=0.017). Asthma medication uses according to PAL status is presented in Table S3. Patients with PAL more frequently received long-acting muscarinic antagonist (LAMA) (41.4% vs 9.6%) and LAMA–LABA (long-acting β2-agonist) (25.0% vs 5.9%), whereas the use of any inhaled corticosteroid (ICS) (68.0% vs 80.0%), ICS monotherapy (18.6% vs 30.4%), and leukotriene receptor antagonist (LTRA) (17.7% vs 34.1%) was less frequent, and the ICS medication possession ratio was lower (0.49 vs 0.58) in the PAL group.
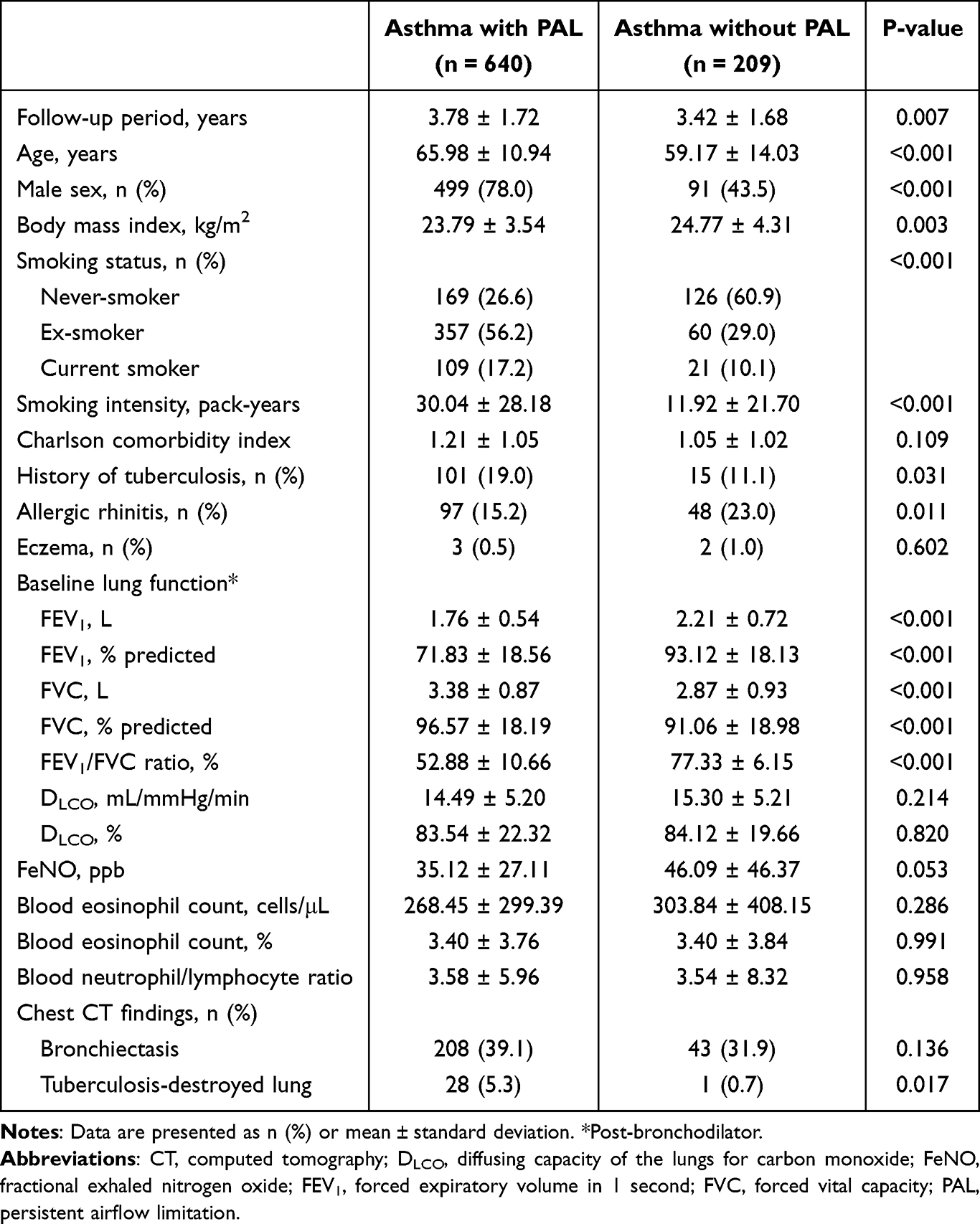 |
Table 1 Baseline and Clinical Characteristics of the Study Population |
Baseline characteristics of the study population stratified by STAR stage are presented in Table S4. As STAR stage increased, patients tended to be older with lower BMI, while the proportions of ever-smokers, smoking intensity, prior TB, and TB-destroyed lung progressively increased. In contrast, the prevalence of allergic rhinitis decreased, and pulmonary function showed lower FEV1 and higher FVC. These trends indicate that the clinical features associated with PAL became progressively more pronounced according to airflow limitation.
Clinical Factors Associated with PAL
We analyzed clinical factors associated with PAL in patients with asthma (Table 2). In univariable analyses, older age, male sex, smoking intensity, and a history of TB had significantly positive association with PAL, whereas BMI, allergic rhinitis, FEV1, and FeNO showed negative associations. In the multivariable analysis adjusted for relevant clinical factors, PAL remained independently associated with male sex, lower BMI, higher smoking intensity, lower FEV1, and absence of allergic rhinitis.
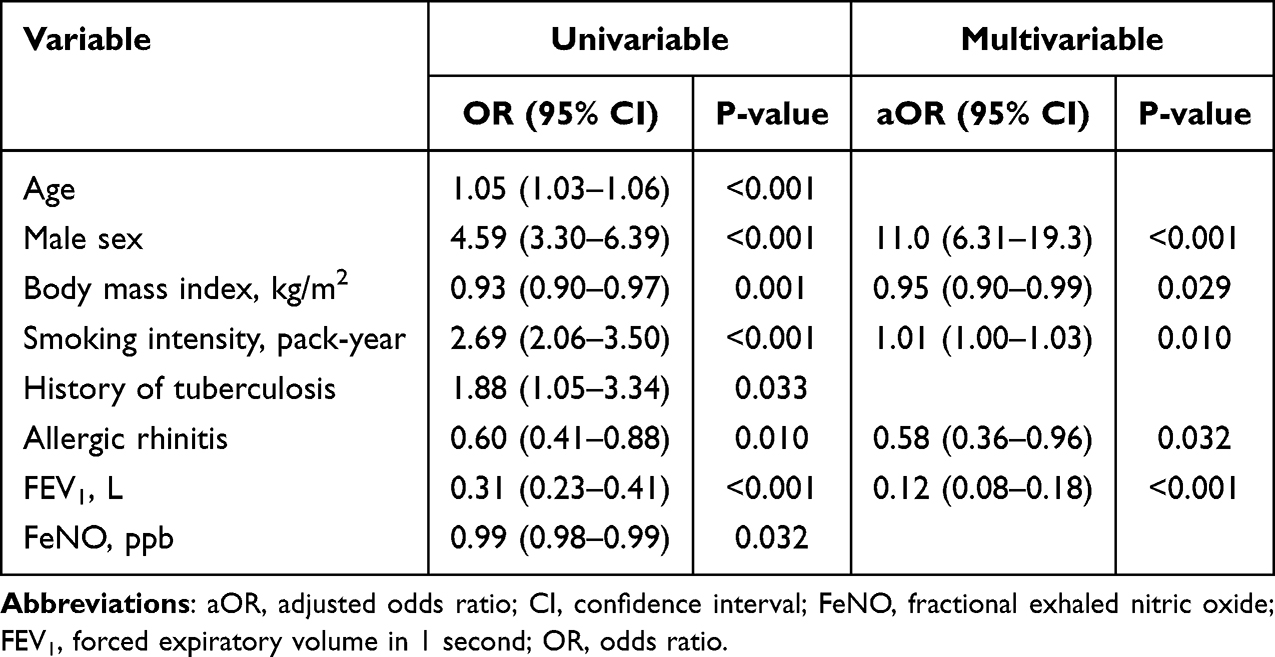 |
Table 2 Factors Associated with PAL Among Patients with Asthma |
To evaluate the predictive performance of clinical factors associated with PAL, ROC curve analyses were conducted using age, smoking intensity, and the inverse of FEV1% predicted (Figure 1). Among these variables, the inverse of FEV1% predicted demonstrated the highest predictive ability (AUC, 0.80; 95% CI, 0.76–0.83; P<0.001), followed by smoking intensity (AUC, 0.71; 95% CI, 0.67–0.75; P<0.001) and age (AUC, 0.65; 95% CI, 0.60–0.69, P<0.001).
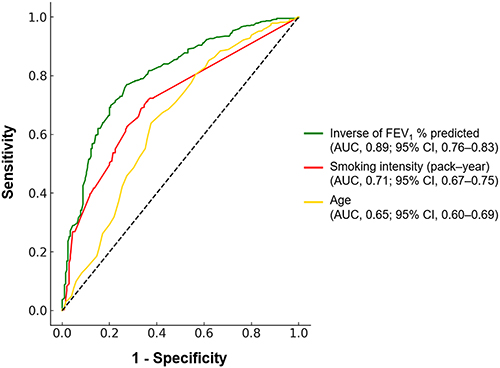 |
Figure 1 Receiver operating characteristic curves for predicting PAL in asthma patients using age, smoking intensity (pack-year), and inverse of FEV1% predicted. Among the three variables, the inverse of FEV1% predicted showed the highest discriminatory ability (AUC 0.80, 95% CI 0.76–0.83, P<0.001), followed by smoking intensity (AUC 0.71, 95% CI 0.67–0.75, P<0.001) and age (AUC 0.65, 95% CI 0.60–0.69, P<0.001). |
Based on these results, we estimated the optimal cut-off values that maximized predictive accuracy and calculated the corresponding sensitivity and specificity (Table S5). In the multivariable analysis, age ≥ 63.5 years, smoking intensity ≥ 9.5 pack-years, and FEV1% predicted ≤ 83.7% were each significantly associated with an increased risk of PAL, with adjusted odds ratios of 3.91 (95% CI, 2.63–5.81), 3.16 (95% CI, 2.16–4.62), and 10.59 (95% CI, 7.10–15.79), respectively.
Risk of Subsequent Acute Exacerbations According to PAL Status and Severity
The history of acute exacerbations by PAL status is summarized in Table 3. No significant differences were found between groups in the occurrence, annual incidence rate of moderate or overall acute exacerbations and proportion of frequent exacerbator according to PAL status. However, during follow-up, PAL group had significantly more severe exacerbations than non-PAL group (13.0% vs 5.7%; P=0.046) and a higher annual incidence rate of severe exacerbations (0.10 ± 0.31 events/year vs 0.05 ± 0.21 events/year; P=0.041). These findings were consistent when stratified by STAR stage, showing significant differences in both the occurrence and annual incidence rate of severe exacerbations (Table S6). Notably, STAR stage 4 patients had the highest occurrence and annual frequency of severe exacerbations across all other stages.
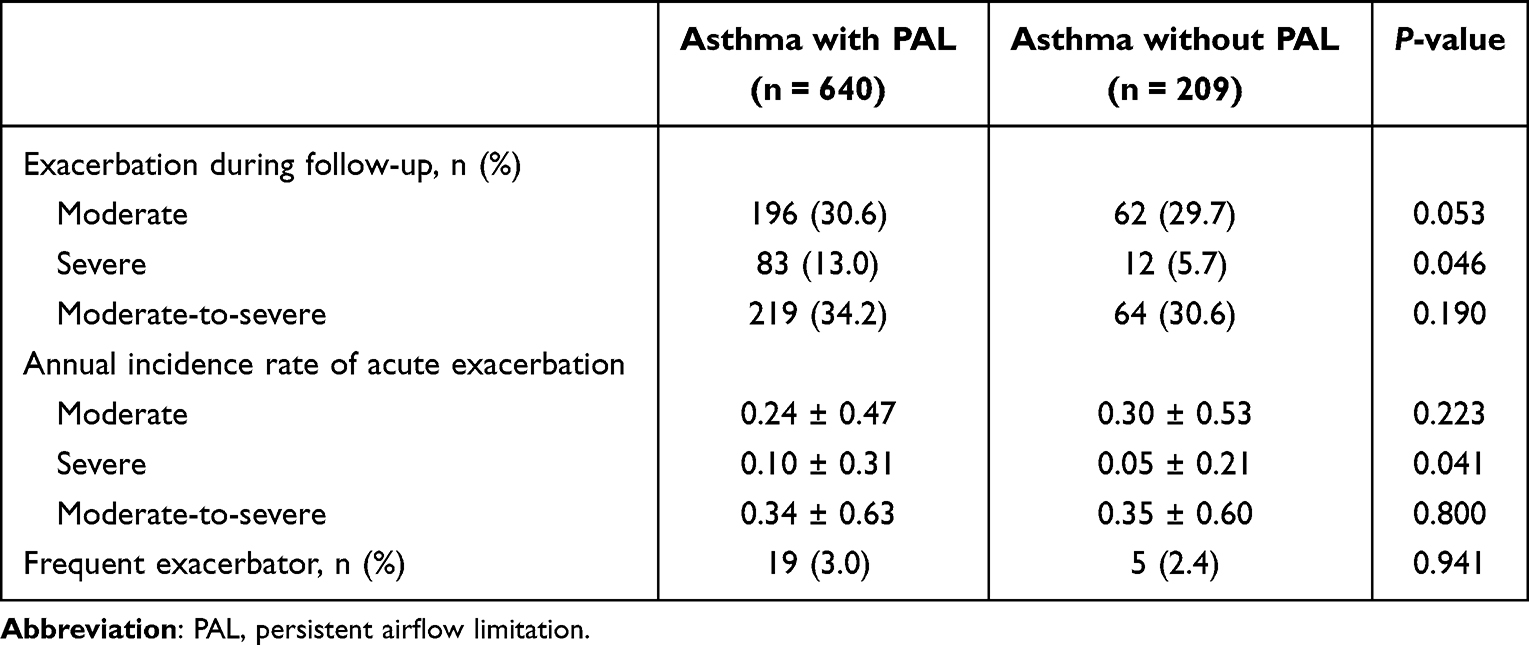 |
Table 3 Classification and History of Subsequent Exacerbation According to PAL |
Associations of PAL status and severity (STAR stage) with annual acute exacerbation rates were evaluated using negative binomial regression (Table 4). PAL was not associated with the incidence of moderate or overall acute exacerbations, but was significantly associated with a higher incidence of severe exacerbations (IRR, 1.77; 95% CI, 1.13–2.79; P=0.014). When stratified by STAR stage, stage 1, 2, and 4 were significantly associated with approximately 1.8-fold, 1.7-fold, and 2.4-fold higher risks of severe exacerbations, respectively, compared with stage 0. The risk of moderate or overall exacerbations was not significantly associated with STAR stage. Across STAR stages, the risk of severe exacerbations increased progressively with advancing severity of airflow limitation, with the highest risk observed at STAR stage 4.
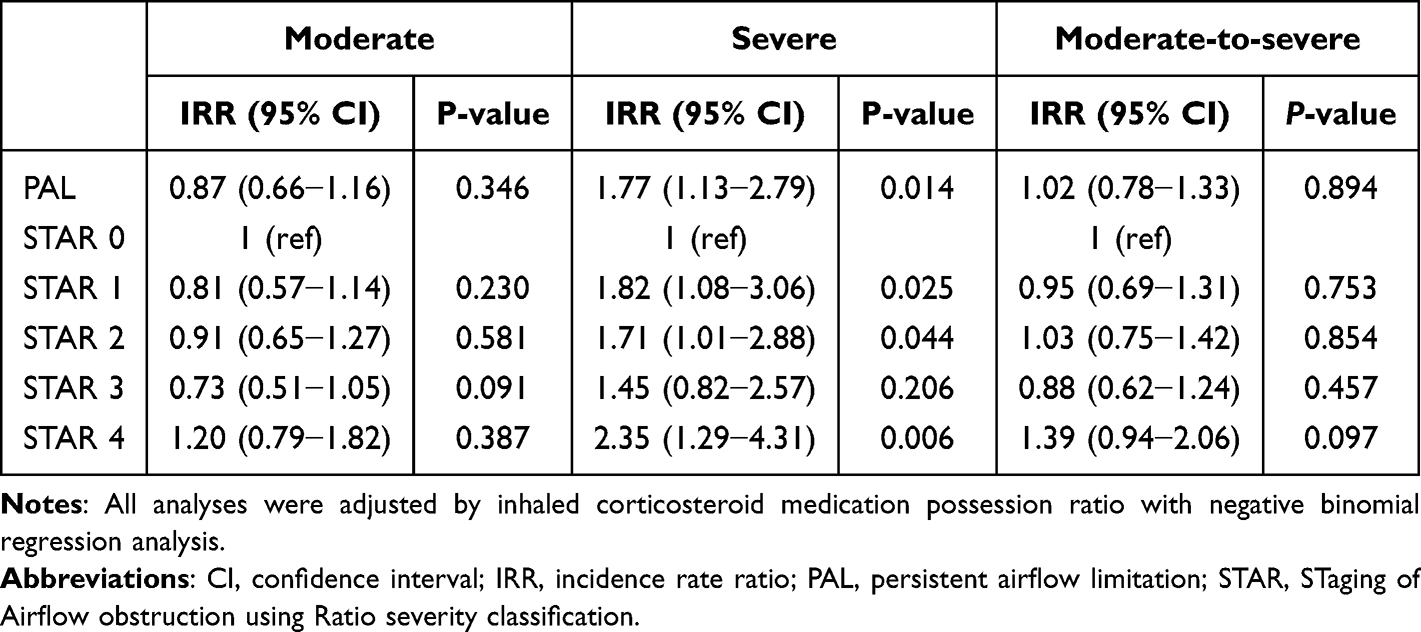 |
Table 4 Association of PAL and Its Severity with Annualized Rate of Subsequent Acute Exacerbation Among Asthma Patients |
To further evaluate the association of PAL status and its severity with severe exacerbations, we analyzed time to first severe exacerbation during follow-up (Figure 2). Kaplan–Meier analysis for time to severe exacerbation demonstrated a non-significant trend toward higher cumulative hazard in PAL group compared with non-PAL group (P=0.090). When stratified by STAR stage, significant differences were observed across the stages (P=0.006). In the multivariable Cox regression analysis, PAL showed a trend toward an increased risk of severe exacerbations (adjusted hazard ratio (aHR), 1.81; 95% CI, 0.99–3.32), although this did not reach statistical significance (Table S7). Among STAR stages, stage 4 was significantly associated with a more than threefold higher risk of severe exacerbations compared with stage 0 (aHR, 3.32; 95% CI, 1.60–6.89), whereas stages 1–3 did not show significant associations.
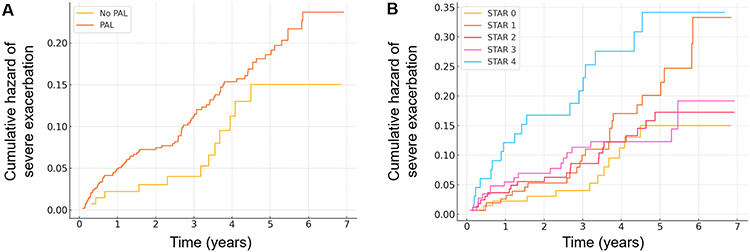 |
Figure 2 Risk of severe exacerbations according to PAL status and severity (STAR stage). (A) Cumulative hazard curves for severe exacerbation comparing patients with and without PAL (log-rank P=0.090). (B) Cumulative hazard curves according to STAR stage (log-rank P=0.006). Abbreviations: PAL, persistent airflow limitation; STAR, STaging of Airflow obstruction using Ratio severity classification. |
We further analyzed the associations between major lung function indices and severe exacerbation risk, stratified by PAL status (Figure 3). The risk of severe exacerbations increased with decreasing FEV1 and FVC. Within the range of FEV1 and FVC values below 100% predicted, PAL group consistently exhibited a higher risk of severe exacerbations compared with non-PAL group, with the differences progressively widening as FEV1 and FVC declined. Restricted cubic spline modeling revealed a non-linear association between FEV1/FVC ratio and the risk of severe exacerbations, with a marked increase in risk at lower ratios, and disproportionate increase in risk below a ratio of approximately 0.70, indicating that the degree of airflow limitation carries graded prognostic significance.
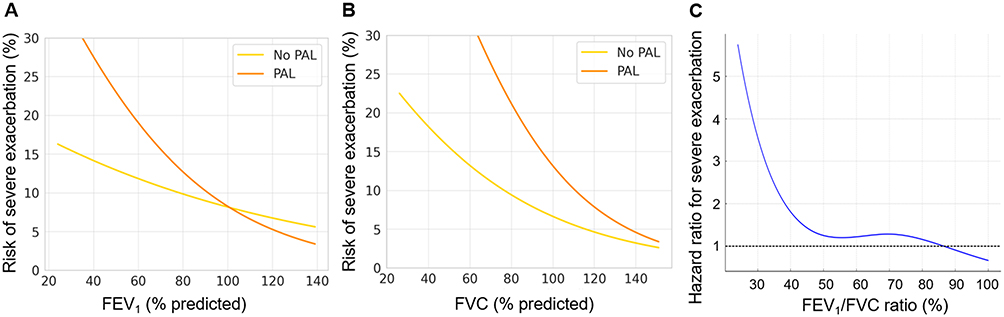 |
Figure 3 Associations between lung function indices and the risk of severe exacerbations. (A) Predicted risk of severe exacerbations according to FEV1% predicted, stratified by PAL status. (B) Predicted risk of severe exacerbations according to FVC % predicted, stratified by PAL status. (C) Restricted cubic spline model demonstrating the non-linear association between FEV1/FVC ratio and the risk of severe exacerbations. The solid blue line represents the estimated hazard ratio derived from a Cox proportional hazards model, and the horizontal dashed line indicates the reference level of risk. |
Longitudinal Changes in Lung Function According to PAL Status and Severity
Longitudinal lung function trajectories \stratified by PAL status and STAR stage were evaluated with linear mixed-effects models adjusted for age, sex, and baseline lung function (Figure 4). The annual decline in FEV1 was significantly slower in PAL group than in non-PAL group, both in absolute volume (−28.1 ± 2.9 mL/year vs −42.5 ± 6.4 mL/year; P=0.028) and % predicted (−0.04 ± 0.14%/year vs −0.68 ± 0.33%/year; P=0.035) (Table S8). In contrast, annual changes in FVC, FEV1/FVC ratio, and DLCO did not differ significantly between groups.
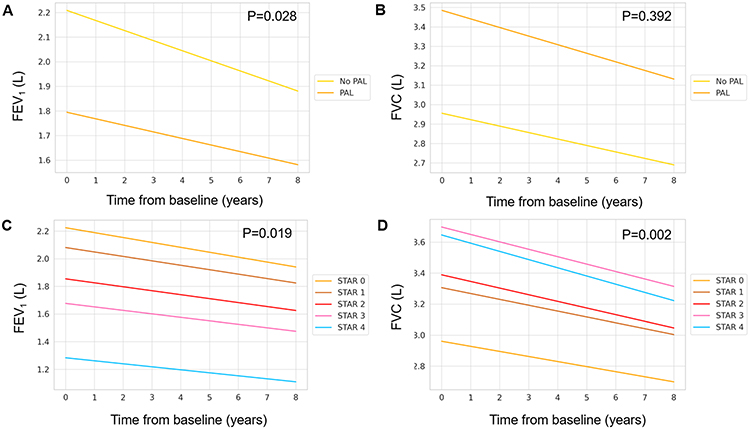 |
Figure 4 Longitudinal trajectories of lung function according to the presence of PAL and STAR stage classification in patients with asthma. Predicted lung function over time was estimated using linear mixed-effects models adjusted for age, sex, and baseline lung function. (A) Annual decline in FEV1 stratified by PAL status. (B) Annual decline in FVC stratified by PAL status. (C) Annual decline in FEV1 stratified by STAR stage. (D) Annual decline in FVC stratified by STAR stage. |
Changes by STAR stage revealed more heterogeneous patterns with increasing PAL severity (Table S9). Patients in STAR 0 and STAR 4 exhibited the most pronounced annual declines in FEV1, whereas intermediate stages showed more modest reductions. FVC decline was most pronounced in STAR 4, while reduction in FEV1/FVC ratio, as an indicator of obstructive ventilatory disorder, was greatest in STAR 0. DLCO changes did not differ significantly across STAR stages.
Discussion
In this multicenter cohort of asthma patients, incorporating both retrospective and prospective data, PAL was a common feature encompassing a wide range of airflow limitation. At baseline, approximately three-quarters of patients exhibited PAL. Previous studies reported that the prevalence of PAL is approximately 20% in general asthma populations and up to 60% among those with severe or refractory disease.20 The reported prevalences of PAL in asthma patients vary depending on the study population, the definition applied, and disease severity.21 The relatively high prevalence in our study likely reflects the inclusion of patients treated at tertiary referral centers, who typically have more severe disease than the broader asthma population. Moreover, PAL in our cohort was a temporally consistent phenotype rather than a cross-sectional finding: serial pulmonary function tests confirmed that the baseline classification remained stable over a mean follow-up of approximately four years, with the PAL group consistently maintaining an FEV1/FVC ratio below 0.70 and none reverting to a non-obstructive pattern, reinforcing its relevance as a stable clinical phenotype in a real-world asthma population.
Patients with PAL were characterized by older age, male sex, lower BMI, greater smoking exposure, and lower FEV1, whereas type 2 inflammation–related features, including allergic rhinitis and FeNO, showed negative associations with PAL. The pattern of medication use was consistent with the clinical profile of PAL. The greater use of long-acting bronchodilators (LAMA and LAMA–LABA), together with lower use of ICS and LTRA and lower ICS adherence, accords with a phenotype characterized by fixed airflow limitation and a predominantly non–type 2 inflammatory background. Dominant eosinophilic inflammation in asthma reflects increased disease activity and uncontrolled airway inflammation, and may accelerate airway remodeling leading to PAL.22 However, a neutrophilic inflammation–dominant endotype may also contribute, particularly in populations characterized by smoking, advanced age, and infection-related factors, which are linked to a neutrophil-predominance and reduced FEV1 reversibility.23,24 Factors associated with PAL in this study—including smoking intensity, older age, prior TB, and TB-destroyed lung—suggest that the development of PAL in this cohort may be predominantly driven by non–type 2 and neutrophilic inflammatory pathways. Collectively, these findings suggest that recurrent and chronic airway inflammation across diverse endotypes in asthma may result in PAL development. Even among patients with similar PAL severity, therapeutic strategies may need to be individualized according to the underlying endotype, underscoring the need for further research.
Notably, PAL was significantly associated with an increased risk of subsequent severe exacerbations in asthma. Previous asthma cohort studies showed that severe exacerbations accelerate FEV1 decline and promote future exacerbations, thereby worsening long-term disease trajectories.25,26 Especially, STAR stage 4 group, representing the most advanced PAL, had a higher risk of severe acute exacerbations and a shorter time to first severe exacerbation compared with non-PAL group. These findings align with previous studies showing that PAL, even at comparable disease control, may contribute to increase risk of acute exacerbations,1 supporting the concept that PAL reflects cumulative airway remodeling in asthma. As structural changes progress—airway wall thickening, smooth muscle hypertrophy, and parenchymal destruction—airflow obstruction becomes less reversible and more impactful on long-term clinical outcomes.2
The difference in severe exacerbation risk between PAL and non-PAL groups widened as FEV1 and FVC declined, suggesting that PAL itself may serve as a prognostic factor, and its prognostic value becomes increasingly independent as the disease advances. The sharp rise in severe exacerbation risk with decreasing FEV1/FVC ratio indicates that both the presence and severity of PAL have prognostic importance. Accordingly, the FEV1/FVC ratio may be a practical marker for monitoring disease progression and guiding therapeutic decisions in asthma. These findings highlight the need for early detection and intervention to prevent the development and progression of PAL in the asthma management.
In longitudinal analysis, lung function trajectories differed by PAL status and severity. Paradoxically, PAL group exhibited a significantly slower annual decline in FEV1 than non-PAL group, which may be attributable to their substantially lower baseline FEV1. Consistent with COPD cohort studies, faster annual FEV1 decline is typically observed in mild-to-moderate disease, whereas the decline attenuates in more advanced stages—likely reflecting diminishing physiological reserve for further loss and reduced reversibility as disease progresses.27 Long-term follow-up studies in asthma, extending over a 10-year observation period, similarly show a steep early decline in FEV1 that subsequently decelerates, aligning with the pattern observed in our cohort.28 However, when lung function trajectories were stratified by STAR stage, patients in STAR 4 demonstrated a distinct pattern, showing significantly faster declines in both FEV1 and FVC compared with the other stages. This finding may be explained by the higher proportion of ever-smokers, greater smoking intensity, and higher frequency of severe acute exacerbations observed in the STAR 4 group. Smoking can accelerate lung-function decline by inducing recurrent and persistent airway inflammation,29 while severe and frequent exacerbations contribute to cumulative airway and parenchymal injury, thereby being linked to excess short- and long-term FEV1 decline.25,30
The clinical course observed in the STAR 4 group suggests that PAL represents a difficult-to-treat phenotype associated with airway remodeling and adverse outcomes, including accelerated lung-function decline and increased morbidity. These findings indicate that PAL may not simply serve as a cross-sectional descriptor but rather as a longitudinal risk phenotype, with its presence and severity conveying important information about future airflow trajectories and exacerbation risk.
This study has several limitations. First, the study population comprised a mixture of retrospective and prospective cohorts that differed in enrollment criteria, data collection, and follow-up, which may have introduced heterogeneity within these cohorts. Second, because participants were recruited from tertiary referral hospitals, selection bias cannot be excluded, and the generalizability of these findings to the general asthma population may be limited. Third, given the inherent nature of an observational study design, our analysis cannot establish definitive causal relationships between PAL and clinical outcomes. Fourth, a substantial proportion of patients with PAL were ever-smokers, a concomitant COPD component or asthma–COPD overlap cannot be entirely excluded. Nonetheless, all patients met objective GINA criteria for asthma with documented variable expiratory airflow limitation, and diagnoses were confirmed by respiratory specialists; accordingly, our analysis focused on PAL as a phenotype within physician-diagnosed asthma.
In conclusion, our study demonstrates that PAL is highly prevalent among patients with asthma and represents a clinically meaningful phenotype characterized by distinct inflammatory pathways, increased risk of severe exacerbations, and heterogeneous patterns of lung-function decline. The presence and severity of PAL convey important prognostic information beyond cross-sectional lung function, underscoring its role as a longitudinal risk phenotype. Assessing PAL and its severity may therefore aid risk stratification and prognostication in clinical practice. Further studies are warranted to determine whether earlier identification of PAL or endotype-based management strategies can improve long-term outcomes.
AI Use Statement
Artificial intelligence tools were not used in the conception, design, analysis, or original drafting of this manuscript. ChatGPT was used solely for English language editing. All scientific content, interpretations, and conclusions were developed and written exclusively by the author.
Data Sharing Statement
All data generated or analyzed during this study are included in this published article and its Supplementary Information Files.
Ethics Approval and Consent to Participate
The retrospective cohort of this study was approved by the Institutional Review Board of Seoul National University Hospital (No:2004-089-1117) and Seoul Metropolitan Government–Seoul National University Boramae Medical Center (No: 30-2020-7). The informed consent of subjects was waived due to retrospective design of this study under approval of the institutional review board of all participating institutions. The prospective cohort of this study was approved by the Institutional Review Boards of the participating institutions (No: 10-2021-5) and written informed consent was obtained from all participants in this prospective cohort. The conduct of this study and the confidentiality of patient data were maintained in accordance with the Declaration of Helsinki.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
No funding was reported.
Disclosure
The authors declare no competing interests in this work.
References
1. Kole TM, Vanden Berghe E, Kraft M, et al. Predictors and associations of the persistent airflow limitation phenotype in asthma: a post-hoc analysis of the ATLANTIS study. Lancet Respir Med. 2023;11(1):55–12. doi:10.1016/S2213-2600(22)00185-0
2. Hsieh A, Assadinia N, Hackett TL. Airway remodeling heterogeneity in asthma and its relationship to disease outcomes. Front Physiol. 2023;14:1113100. doi:10.3389/fphys.2023.1113100
3. Elliot JG, Jones RL, Abramson MJ, et al. Distribution of airway smooth muscle remodelling in asthma: relation to airway inflammation. Respirology. 2015;20(1):66–72. doi:10.1111/resp.12384
4. Mindus S, Gislason T, Benediktsdottir B, et al. Respiratory symptoms, exacerbations and sleep disturbances are more common among participants with asthma and chronic airflow limitation: an epidemiological study in Estonia, Iceland and Sweden. BMJ Open Respir Res. 2024;11(1). doi:10.1136/bmjresp-2023-002063
5. Van Zyl-Smit RN, Kerstjens HA, Maspero JF, et al. Efficacy of once-daily, single-inhaler, fixed-dose combination of mometasone/indacaterol/glycopyrronium in patients with asthma with or without persistent airflow limitation: post hoc analysis from the IRIDIUM study. Respir Med. 2023;211:107172. doi:10.1016/j.rmed.2023.107172
6. Colak Y, Afzal S, Marott JL, et al. Type-2 inflammation and lung function decline in chronic airway disease in the general population. Thorax. 2024;79(4):349–358. doi:10.1136/thorax-2023-220972
7. Global Initiative for Asthma. Global strategy for asthma management and prevention; 2019.
8. Kim NY, Lee CH, Jin KN, et al. Clinical deterioration and lung function change in patients with concomitant asthma and bronchiectasis. J Allergy Clin Immunol Pract. 2022;10(10):2607–2613e2604. doi:10.1016/j.jaip.2022.05.026
9. FitzGerald JM, Tran TN, Alacqua M, et al. International severe asthma registry (ISAR): protocol for a global registry. BMC Med Res Methodol. 2020;20(1):212. doi:10.1186/s12874-020-01065-0
10. Larenas-Linnemann D, Rhee CK, Altraja A, et al. International Severe Asthma Registry (ISAR): 2017-2024 status and progress update. Tuberc Respir Dis. 2025;88(2):193–215. doi:10.4046/trd.2024.0198
11. Bhatt SP, Nakhmani A, Fortis S, et al. FEV(1)/FVC severity stages for chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 2023;208(6):676–684. doi:10.1164/rccm.202303-0450OC
12. Bhatt SP, Balte PP, Schwartz JE, et al. Discriminative accuracy of FEV1:FVC thresholds for COPD-related hospitalization and mortality. JAMA. 2019;321(24):2438–2447. doi:10.1001/jama.2019.7233
13. Charlson ME, Pompei P, Ales KL, et al. A new method of classifying prognostic comorbidity in longitudinal studies: development and validation. J Chronic Dis. 1987;40(5):373–383. doi:10.1016/0021-9681(87)90171-8
14. Radovanovic D, Santus P, Blasi F, et al. A comprehensive approach to lung function in bronchiectasis. Respir Med. 2018;145:120–129. doi:10.1016/j.rmed.2018.10.031
15. Yang B, Choi H, Shin SH, et al. Association of ventilatory disorders with respiratory symptoms, physical activity, and quality of life in subjects with prior tuberculosis: a National Database Study in Korea. J Pers Med. 2021;11(7):678. doi:10.3390/jpm11070678
16. Rhee CK, Yoo KH, Lee JH, et al. Clinical characteristics of patients with tuberculosis-destroyed lung. Int J Tuberc Lung Dis. 2013;17(1):67–75. doi:10.5588/ijtld.12.0351
17. Kamenar K, Hossen S, Gupte AN, et al. Previous tuberculosis disease as a risk factor for chronic obstructive pulmonary disease: a cross-sectional analysis of multicountry, population-based studies. Thorax. 2022;77(11):1088–1097. doi:10.1136/thoraxjnl-2020-216500
18. Reddel HK, Taylor DR, Bateman ED, et al. An official American Thoracic Society/European Respiratory Society statement: asthma control and exacerbations: standardizing endpoints for clinical asthma trials and clinical practice. Am J Respir Crit Care Med. 2009;180(1):59–99. doi:10.1164/rccm.200801-060ST
19. Sprio AE, Carriero V, Levra S, et al. Clinical characterization of the frequent exacerbator phenotype in Asthma. J Clin Med. 2020;9(7):2226. doi:10.3390/jcm9072226
20. Bertels X, Edris A, Garcia-Aymerich J, et al. Phenotyping asthma with airflow obstruction in middle-aged and older adults: a CADSET clinical research collaboration. BMJ Open Respir Res. 2023;10(1). doi:10.1136/bmjresp-2023-001760
21. Bakakos A, Vogli S, Dimakou K, et al. Asthma with fixed airflow obstruction: from fixed to personalized approach. J Pers Med. 2022;12(3):333. doi:10.3390/jpm12030333
22. Mogensen I, Alving K, Dahlen SE, et al. Fixed airflow obstruction relates to eosinophil activation in asthmatics. Clin Exp Allergy. 2019;49(2):155–162. doi:10.1111/cea.13302
23. Smith BM, Zhao N, Olivenstein R, et al. Asthma and fixed airflow obstruction: long-term trajectories suggest distinct endotypes. Clin Exp Allergy. 2021;51(1):39–48. doi:10.1111/cea.13714
24. Ray A, Kolls JK. Neutrophilic Inflammation in Asthma and Association with Disease Severity. Trends Immunol. 2017;38(12):942–954. doi:10.1016/j.it.2017.07.003
25. O’Byrne PM, Pedersen S, Lamm CJ, et al. Severe exacerbations and decline in lung function in asthma. Am J Respir Crit Care Med. 2009;179(1):19–24. doi:10.1164/rccm.200807-1126OC
26. Tomisa G, Santa B, Horvath A, et al. Risk of exacerbation and mortality in asthma: a 10-year retrospective financial database analysis of the Hungarian Health Insurance Fund. BMJ Open Respir Res. 2024;11(1). doi:10.1136/bmjresp-2023-002006
27. Kirkby J, Nenna R, McGowan A. Changes in FEV(1) over time in COPD and the importance of spirometry reference ranges: the devil is in the detail. Breathe. 2019;15(4):337–339. doi:10.1183/20734735.0252-2019
28. Bucchieri S, Alfano P, Audino P, et al. Lung function decline in adult Asthmatics–A 10-year follow-up retrospective and prospective study. Diagnostics. 2021;11(9):1637. doi:10.3390/diagnostics11091637
29. Ilmarinen P, Tuomisto LE, Kankaanranta H. Phenotypes, risk factors, and mechanisms of adult-onset asthma. Mediators Inflamm. 2015;2015:514868. doi:10.1155/2015/514868
30. Bai TR, Vonk JM, Postma DS, et al. Severe exacerbations predict excess lung function decline in asthma. Eur Respir J. 2007;30(3):452–456. doi:10.1183/09031936.00165106
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
A Meta Analysis of Physical Exercise on Improving Lung Function and Quality of Life Among Asthma Patients
Zhu Q, Zhu J, Wang X, Xu Q
Journal of Asthma and Allergy 2022, 15:939-955
Published Date: 13 July 2022
A Comparison of the Effectiveness of Asthma Medications on Asthma Exacerbations in Real World National Cohort
Park HJ, Jeon S, Lee HS, Kim BY, Chae YJ, Kim GO, Park JW, Lee JH
Journal of Asthma and Allergy 2022, 15:1155-1165
Published Date: 24 August 2022
Relationship Between Asthma Control as Measured by the Asthma Impairment and Risk Questionnaire (AIRQ) and Patient Perception of Disease Status, Health-Related Quality of Life, and Treatment Adherence
Reibman J, Chipps BE, Zeiger RS, Beuther DA, Wise RA, McCann W, Gilbert I, Eudicone JM, Gandhi HN, Harding G, Cutts K, Coyne KS, Murphy KR, George M
Journal of Asthma and Allergy 2023, 16:59-72
Published Date: 5 January 2023
Mometasone/Indacaterol/Glycopyrronium (MF/IND/GLY) and MF/IND at Different MF Strengths versus Fluticasone Propionate/Salmeterol Xinafoate (FLU/SAL) and FLU/SAL+ Tiotropium in Patients with Asthma
van Zyl-Smit RN, Chapman KR, Kerstjens HAM, Gessner C, Sagara H, Tanase AM, Hosoe M, Pethe A, Lawrence D, Tillmann HC, D'Andrea P
Journal of Asthma and Allergy 2023, 16:123-134
Published Date: 20 January 2023
Effects of ICS + LABA Combination Therapy on Asthma Control: An Observational Study in Real-World Settings
Han P, Wang L
Therapeutics and Clinical Risk Management 2026, 22:547261
Published Date: 7 February 2026