Back to Journals » Journal of Asthma and Allergy » Volume 15
A Meta Analysis of Physical Exercise on Improving Lung Function and Quality of Life Among Asthma Patients
Authors Zhu Q ![]() , Zhu J
, Zhu J ![]() , Wang X
, Wang X ![]() , Xu Q
, Xu Q ![]()
Received 14 April 2022
Accepted for publication 26 June 2022
Published 13 July 2022 Volume 2022:15 Pages 939—955
DOI https://doi.org/10.2147/JAA.S369811
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Amrita Dosanjh
Qiaoyu Zhu,1 Jianming Zhu,2 Xing Wang,3 Qiong Xu4
1School of Physical Education, Shanghai University, Shanghai, 200444, People’s Republic of China; 2Sports Department, East China University of Political Science and Law, Shanghai, 200042, People’s Republic of China; 3School of Kinesiology, Shanghai University of Sport, Shanghai, 200438, People’s Republic of China; 4School of Physical Health, Shanghai Business School, Shanghai, 201400, People’s Republic of China
Correspondence: Qiong Xu, Email [email protected]
Objective: This paper aims to perform a systematic assessment of the influence of physical exercise on asthma patients and discuss the intervention effects of different exercises on the lung function FEV1 (%pred) and quality of life among asthma patients so as to lay a scientific foundation for improving asthma symptoms.
Methods: Both Chinese and English databases were retrieved, including PubMed, Web of Science, Embase, The Cochrane Library, CBM, CNKI, Wan Fang Data, and VIP, whose retrieval period started from the founding date of each database to 1st, November 2021. Randomized controlled trials (RCT) studying the symptom indicators of asthma patients were collected. Those collected papers were screened according to the Inclusion Criteria and Exclusion Criteria. Then, methodological quality assessments were conducted on the included papers, and combined effect sizes were analyzed by using software ReMan 5.3.5.
Results: The meta analysis showed that physical exercise could significantly improve lung function FEV1 (%pred) and quality of life score. Trails containing breathing exercise are the main source of heterogeneity, and the subgroup of breathing exercise may have better performance than the subgroup of aerobic exercise in improving FEV1 (%pred).
Conclusion: Physical exercise can significantly improve the symptoms and quality of life of asthma patients. Except the breathing exercise that showed heterogeneity, the subgroup of aerobic exercise could improve the capacity of FEV1 (%pred) more effectively, which led to a significant difference in the influence of quality of life. However, with regard to the gymnastic exercise including breathing exercise, there are limited same intervention methods and insufficient same outcome indicators. Therefore, more precise and high-quality researches are needed to make deeper verification in the future.
Keywords: physical exercise, asthma, lung function, quality of life, meta analysis
Introduction
Asthma is a heterogeneous disease which features chronic airway hyperresponsiveness with inflammation involving mast cells, T lymphocytes and eosinophils.1 It is reported that asthma has caused damage to around one-tenth of child health worldwide.2 The authoritative magazine The Lancet released a newly published major achievement regarding China Pulmonary Health Study (CPH Study) based on large-scale Chinese population, which shows that the prevalence rate of asthma among people aged 20 and over in China is 4.2%, the number of patients reaches 45.7 million, among which about 26.2% (13.1 million) patients suffer from pulmonary limited airflow function.
Asthma features limited reversible airflow, dyspnea caused by repeated wheezing, shortness of breath, and cough.3 There are many factors inducing asthma, and some studies have found that doing exercise can induce the onset of Exercise-induced Asthma (EIA), most patients of which do not receive reasonable anti-inflammatory treatment.4 As a result, most patients who only have partial understanding of sports reduce or even refuse to take part in physical exercise.5 However, it is clearly stated in the Global Initiative for Asthma (GINA) that the purpose of treating asthma is to achieve the normal level of physical activity and control the clinical symptoms of asthma.6 Only relying on glucocorticoids to control asthma, besides the toxic and side effects of drugs, the long-term state of not doing exercise will also impose adverse effects on body’s immunity and cardiopulmonary function.
Currently, asthma cannot be cured completely. But in recent years, increasingly literature shows that physical sports are able to improve the quality of life of asthma patients to a certain extent, including relieving the inflammation of asthma and improving physical exercise ability.7,8 There is enough evidence to prove that it is safe and effective for asthma patients to take part in sports with proper management and effective medical supervision,9 which makes more and more scholars begin to pay attention to the relationship between physical exercise and asthma. Scholar Moreira and Delgado put forward that there is a “U-shaped” dose-dependent relationship between exercise intensity and the incidence rate of EIA, which indicates that moderate-intensity exercise can minimize the incidence of asthma and the patient is safe during the exercise process.10 GINA mentions the normal physical activities of children with asthma, but does not give detailed exercise prescription, and the improvement mechanism of asthma remains unclear. Throughout previous literature, the research designs of sports explored by different scholars are not consistent, thus their results also vary due to various factors such as sports methods, sports intensity and outcome indicators. Therefore, it is still hard to determine the extent of improvement by different types of exercises as the intervention of asthma.
In light of the previous introduction, this paper used meta-analysis to conduct quantitative analyses on randomized controlled trials aimed at the physical exercise intervention on asthma patients. At the same time, the physical exercises written in the included literature were also conducted sub-group analyses in an effort to explore whether different types of exercise could improve the lung function and quality of life scores among asthma patients.
Research Method
This paper adheres to the guide of The PRISMA Statement for Reporting Systematic Reviews and Meta Analyses of Studies that Evaluate Health Care Interventions: Explanation and Elaboration when selecting and using research methods.11
Literature Inclusion and Exclusion Criteria
Research Method
The RCT of physical exercise intervention on the effects of improving the quality of life of asthma patients.
Subjects of the Study
Groups that have been diagnosed with asthma symptoms with no requirements on ethnicity, nationality or gender; have no other organ diseases; and have good control over the asthma symptoms.
Intervention Measures
(1). At least one experimental group employed physical exercise as intervention method, the type of which is unlimited. (2). Besides the differences of exercise intervention, the control group used the same intervention method as the experimental group. Both the experimental group and the control group received regular medicine treatment to ensure the safety of this experiment. (3). If there had been multiple groups of experimental data in one paper, those data would have been counted as multiple research results. The two groups highlighted exercise intervention.
Outcome Indicators
Main outcome indicators were selected according to the literature content and the main indicators of asthma: 1) Pulmonary function index: the ratio of forced expiratory volume in the first second (FEV1) to normal predicted value is analyzed; and the higher the ratio, the better the asthma control effect; 2) The total scores of asthma quality-of-life questionnaire (AQLQ) and pediatric asthma quality-of-life questionnaire (PAQLQ): the score range is 0–7, the higher the score, the lower the impact of asthma symptoms on daily life.
The Exclusion Criteria of Literature
(1) Papers recruiting non-asthma patients or patients with other pulmonary diseases; (2) Intervention involving factors other than exercise intervention; (3) Neither Chinese nor English literature; (4) Papers with poor quality evaluation that did not have detailed introduction to intervention measures and whose experimental data could not be extracted and calculated; (5) The baselines of research indicators in different groups have significant difference.
Retrieval Strategy
Two researchers joined in the retrieval of the literature, which contained eight databases (Chinese & English) including PubMed, Embase, The Cochrane Library, Web of Science, CBM, Wanfang, CNKI, and VIP. The retrieval period started from the founding date of each database to 1st, November, 2021. In addition, the retrieval method employed the method of “subject words+free words”, and the included papers were also conducted reference tracking. To be specific, English search terms used the PubMed format
Search (((((((Controlled Clinical Trials, Randomized) OR Trials, Randomized Clinical) OR Clinical Trials, Randomized) OR Randomized Controlled Trials as Topic) OR RCT) OR Randomized Controlled Trial)) AND ((((((((((((((((((((((((((((Trainings, Exercise) OR Training, Exercise) OR Exercise Trainings) OR Exercise Training) OR Exercises, Aerobic) OR Aerobic Exercises) OR Aerobic Exercise) OR Exercise, Aerobic) OR Isometric Exercise) OR Isometric Exercises) OR Exercises, Isometric) OR Exercise, Isometric) OR Exercises, Acute) OR Exercise, Acute) OR Acute Exercises) OR Acute Exercise) OR Physical Exercises) OR Physical Exercise) OR Exercises, Physical) OR Exercise, Physical) OR Physical Activities) OR Activity, Physical) OR Activities, Physical) OR Physical Activity) OR Exercises) OR Exercise)) AND ((((Asthma, Bronchial) OR Bronchial Asthma) OR Asthmas) OR Asthma))
as the retrieval strategy. Chinese search terms used asthma (哮喘, 哮病), physical exercise (运动), randomized controlled trial and RCT (随机对照试验, RCT).
Extraction and Screening of Literature
Papers that met the inclusion requirements were read and the relevant materials were extracted. First, the article titles and abstracts were screened, and relevant articles that did not meet the contents and methods of this study were excluded. Second, through reading the detailed information of the articles, we screened out the relevant articles with high quality and whose research data could be extracted. Finally, the contents of literature extraction were as follows: publication year of the literature, name of the author, age of study subjects, sample size, asthma disease severity, intervention measures (time, frequency, method, and intensity), and outcome indicators. If the literature did not contain this study indicator, the literature was excluded.
Then the papers retrieved from each database were imported into Endnote software for editing. Articles were screened by two researchers according to the inclusion and exclusion criteria in an independent, double-blind manner. After screening, the two researchers compared the extracted papers. If there was any disagreement, the inclusion of the article was decided through joint discussion by a third person.
Quality Assessment of Included Literature
Cochrane, a literature quality assessment tool, was used to evaluate the quality of included literature in seven aspects: random sequence generation, concealment of allocation, blinding of subjects and researchers, blinding of outcome evaluator, incomplete outcome data, selective reporting and other biases. For each indicator, “low risk of bias”, “uncertain risk of bias” and “high risk of bias” were used for judgment.
Data Processing
The research data were processed by Reviewer Manager 5.3.5 software, including effect size combination, heterogeneity test, sensitivity analysis, forest map drawing and so on. Since this study is a continuous variable, and the unit of measurement and scale span between each study are the same, the Mean Difference (MD) effect size was combined. And the 95% confidence interval was calculated. The P value and I2 were used for the heterogeneity test. If the combined result shows I2≥50%, it is considered that a great heterogeneity exists in the results, which needs sensitivity analysis and adopts combine data by using random effect; otherwise, fixed effect is used.
Literature Retrieval Result
Overall 5485 papers were left for the first retrieval after examining eight databases including PubMed, Embase, The Cochrane Library, Web of Science, CBM, Wanfang, CNKI, and VIP. No papers were gotten through other resources. There were 2331 repeated papers after checking; 2787 unqualified papers after reading their titles and abstracts; and 349 papers that could not extract data or were irreverent with this research content were excluded after manual review. To sum up, 18 papers were left that could be included in this study (see Figure 1).
 |
Figure 1 Literature screening process. # PubMed=908, EMbase=1090, The Cochrane Library=1742, Web of Science=519, CBM=151, Wan Fang=315, VIP=141, CNKI=199. |
Basic Information of Included Literature
Table 1 is the included literature information. A total of 1021 subjects were included in the 18 articles, including 530 subjects in the experimental group and 491 subjects in the control group. All the sample sizes adopted the outcome indicator values after trials on the condition that their baselines showed no significant difference. One paper covered subjects who were over 60-year-old, four papers covered subjects between 20–40-year-old, and the remaining 13 papers covered subjects under 15-year-old.. Theresearch intervention method mainly adopted aerobic exercise,12–14,21 free-choice exercise by patients,22–24 combined exercise,25 resistive exercise,26 and breathing exercise.27–29 Seven papers are from China, and eleven from other countries, among which one is a master’s thesis, and the rest are journal papers. See Table 1
 |
Table 1 Basic Features of the Included Literature |
Assessment of Bias Risks
Figures 2 and 3 present the bias of included papers. The 18 included papers were all RCTs, all the subjects of which had signed informed consent forms. Therefore, there was no double-blind trial. There were three papers showing relatively high quality, which clearly described the random allocation method and the process of allocation concealment;14,16,18 one paper did not adopt the random generation process;27 another one paper lost the track of follow-up patients and did not report the treatment of those lost subjects.14 Overall, there is a certain bias in the included papers, but the overall outcome indicators are relatively complete.
 |
Figure 2 Risk of bias summary. |
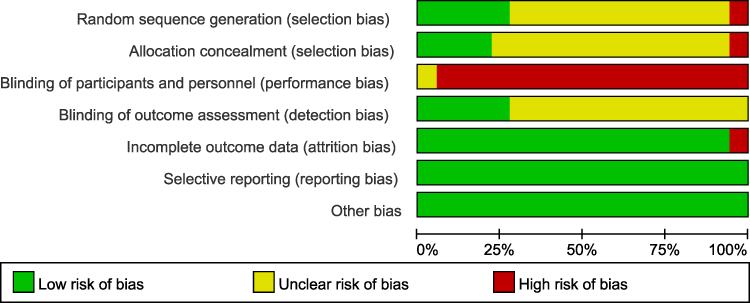 |
Figure 3 Risk of bias graph. |
Meta-Analysis Results
Effects of Physical Exercise on Lung Function of Patients with Asthma
Finally, 16 articles (a total of 18 studies) with FEV1 (%pred) indicators were included in the 18 papers, and the total number of subjects was 966, including 506 in the experimental group and 460 in the control group. As shown in Figure 4, the results of heterogeneity test showed that I2=81%, and P < 0.01, indicating that there was high heterogeneity in each study, thus random effect was adopted for analyzing. The results of combined meta-analysis showed that the combined effect amounted MD=4.81, and the CI was [1.57,8.05], P < 0.05. It indicated that physical exercise intervention could significantly improve the pulmonary function of patients with asthma.
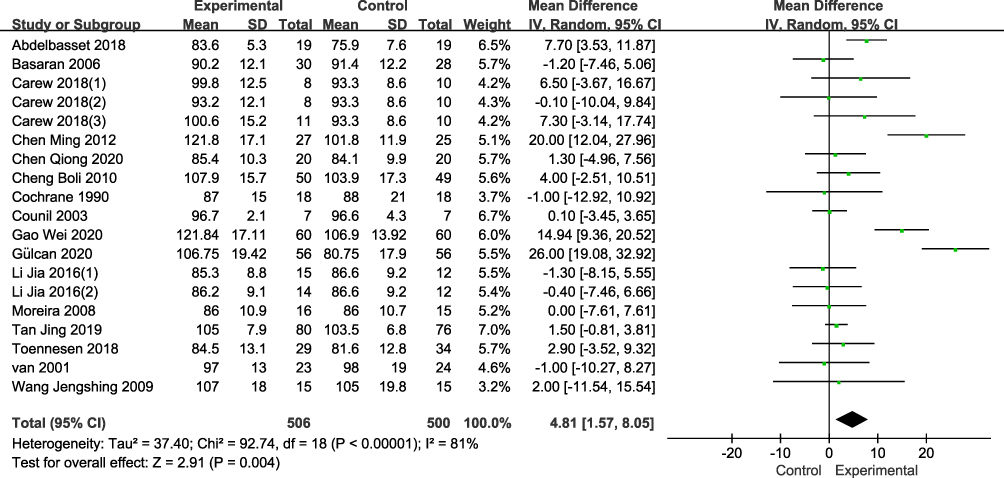 |
Figure 4 Improvements of physical exercise to lung function FEV1(%pred). |
Effects of Physical Exercise on Quality of Life of Patients with Asthma
At last, nine papers recording the quality of life questionnaire of asthma patients were collected from the results, which recorded and compared the effect of exercise on life improvement among 642 subjects with 323 in the experimental group and 319 in the control group. As shown in Figure 5, the heterogeneity test results showed I2=100%, P > 0.05, indicating that there was great heterogeneity in various studies of this result. Therefore, random effect was adopted for analysis. The results of the combined meta-analysis showed that the combined effect was MD=0.84, and the CI was [−0.29,1.97], P > 0.05. The results showed that physical exercise could improve the quality of life of patients with asthma, but there was no statistical significance.
 |
Figure 5 Effect of Physical Exercise on quality of life Scale. |
Subgroup Analyses of the Effects of Physical Exercise on Lung Function of Asthma Patients
To explore the possible factors for the heterogeneity of lung function in asthmatic patients caused by physical exercise, a subgroup analysis was performed on 18 included studies. The exercise influence on asthma patients mainly lies in the following aspects: different age groups, exercise cycles, exercise duration, exercise frequency, exercise intensity and different types of exercise. In the included literature, symptom reports of asthma patients were mostly mild and moderate, and the overall symptoms were similar. Therefore, this paper mainly performed subgroup analyses on six aspects, including exercise style, exercise intensity, subject age, exercise frequency, exercise duration and exercise cycle.
First of all, the exercise styles in the literature on lung function indicators were grouped, which could be divided into four subgroups: aerobic exercise (incremental or intermittent), combined exercise, free-choice exercise, and breathing exercise. To facilitate grouping of exercise intensity, Turner et al16 used Borg scale 6–20 RPE subjective measurement scale, and the maximum heart rate amounted to approximately 120 to 140 beats/min by multiplying the outcome indicator by 10.30 According to the maximum heart rate calculator: actual heart rate/(220-age) equals that the exercise intensity was about 80%~90%. van et al22 reported in the previous literature that the exercise level of the experimental group was increased to the anaerobic threshold, and it was also reported in the previous literature that the anaerobic threshold corresponded to its maximum intensity was about 86.3%.31 Therefore, the exercise intensity could be divided into four groups: 60% ~80%, more than 80% ~ 90%, individualized intensity, and unreported intensity; The age of the subjects could be divided into two subgroups: those under 20 years old and those over 20 years old. The exercise duration was mainly divided into three groups for subgroup analyses: 20min~40min, greater than 40 min~60min, and more than 60min.
The results of subgroup analyses in Table 2 show that all the I2 values of three groups out of four subgroups (except breathing exercise) divided by exercise type were less than 50%, which indicated that breathing exercise might be the source of heterogeneity. The results of subgroup analysis divided by exercise intensity showed that except for individualized intensity (I2=0), the I2 values of the rest three subgroups were all >50%, so it was suggested that exercise intensity was not the source of heterogeneity. Likewise, there were two groups of I2 values >50% in the age subgroup, so age factor might not be the source of heterogeneity. In addition, in the exercise duration subgroup, except that the exercise duration ≥60min showed heterogeneity (I2=67), the I2 values of the other two groups were <50%, suggesting that exercise duration might also be a factor contributing to heterogeneity. In conclusion, it could be concluded from Table 2 that exercise type and duration may be the source of heterogeneity.
 |
Table 2 Subgroup Analyses of the Effect of Physical Exercise on Lung Function FEV1 (%) Among Asthma Patients |
A Sensitivity Analysis of Physical Exercise on Life of Asthma Patients
Since the overall number of included papers concerning the quality of life of asthma patients was limited, subgroup analysis method for classifying possible factors was not suitable. Instead, the sensitivity analysis was adopted to eliminate individual studies from the included literature one by one to find the source of heterogeneity (as shown in Table 3).
 |
Table 3 A Sensitivity Analysis of Physical Exercise on Quality of Life of Asthma Patients |
It can be clearly seen from Figure 5 that only after excluding the article Gülcan 2020 and combining the rest data, the heterogeneity was significantly reduced to 18%, so it can be considered that this paper is the main cause of heterogeneity. After removing Gülcan 2020, the effect size plot showed MD=0.41, the 95% CI was [0.32, 0.51], and P < 0.01, I2=18% in Table 3.
Combined Results After Eliminating Heterogeneous Indicators
Figure 6 shows that the combined results of subgroup analysis of FEV1 (%pred) were MD=1.84, and the 95% CI was [0.47, 3.21], P < 0.01, and I2=0%. There was no heterogeneity between the papers, so the data results were reliable.
 |
Figure 6 Improvements on lung function FEV1(%pred) after eliminating heterogeneous papers. |
Figure 7 shows the combined results of MD=0.41, 95% CI was [0.32, 0.51], and P < 0.001 I2=18% for the subgroup analysis of quality of life scores. The heterogeneity between the articles is small, thus the data results are reliable.
 |
Figure 7 Improvements on quality of life after eliminating heterogeneous papers. |
Effects of Breathing Exercise on Lung Function FEV1(%pred)
There was significant heterogeneity when the breathing exercise combined with other types of exercise to conduct sub-analyses. Thus, the breathing exercise was singled out for an independent sub-analysis. The combined results of the sub-group analysis of FEV1(%pred) in Figure 8 show that MD=20.08, the 95% CI was [13.33, 26.83], P < 0.001, and I2=67%, indicating heterogeneity between the three papers, and requiring further sensitivity analysis.
 |
Figure 8 Subgroup analyses of the effect of physical exercise on lung function FEV1 (%) among asthma patients. |
Discussion and Analysis
Improvements in Asthma Patient Symptoms Through Physical Exercise
The aim of this study is to analyze the improvement condition of asthma symptoms after doing different types and features of exercise in an effort to find the best exercise in relieving the symptoms. However, a large number of previous studies showed that asthma patients were prone to the onset of exercise-induced bronchoconstriction/bronchialspasm (EIB), which could easily induce the occurrence of EIA in patients.32 Some studies have pointed out that exercise can induce asthma symptoms in most patients who do not have reasonable anti-inflammatory therapy. The type and intensity of exercise can contribute to respiratory depression caused by increased airway resistance after exercise.33 However, previous studies used one-time experimental sampling with medium or above intensity and immediate after exercise,34,35 which made the long-term recovery of airway function and lung function after regular exercise to be unknown. The current study believes that exercise can reduce asthma symptoms and improve the quality of life, which has been a consensus among researchers. Exercise can not only improve lung function of patients with asthma FEV1 (%pred) but also reduce the symptoms of patients. Meta-analysis on the effect of exercise on asthma confirms that exercise has a positive effect on improving the asthma symptoms. Swiss scholar Eichenberger et al36 included 17 studies in a meta-analysis in 2013, containing a total of 599 subjects. By measuring the indicators such as Forced Expiratory Volume in 1 Second (FEV1), peak expiratory volume, and maximum oxygen uptake, his study found that exercise can significantly improve lung function indicators and the quality of life has significantly improved. Scholar Avallone et al37 pointed out in their research that asthmatic patients have lower physical activity levels than normal people, and the long-term lack of exercise makes the symptoms of asthma appear more negative. Regular aerobic training can improve the management of asthma symptoms and lung function. The results of the quantitative meta-analysis of the effect of different types of exercise on improving asthma symptoms in this paper are basically consistent with previous studies.37 However, the relationships among exercise types, exercise intensity, and exercise duration had not been discussed in the previous literature, so this paper analyzed exercise effects based on the previous literature in a more precise manner.
Lung function is an important objective indicator for detecting respiratory diseases. Observation of pulmonary function can effectively assess the severity of asthma symptoms after exercise. There were two main presentations in the included literature: FEV1 (%pred) and FEV1/FVC. It is generally believed that the ratio of FEV1 to its expected value is a reliable indicator of the severity of airflow obstruction, while FEV1/FVC is a sensitive indicator of obstructive ventilatory dysfunction.38 Therefore, FEV1 (%pred) was used as the observation indicator in this study. It is also controversial whether exercise can significantly improve FEV1 (%pred) in the included literature. Among the 18 included literature, only four studies showed that exercise significantly improved FEV1 (%pred). The results of the other six studies favored the experimental group but showed no significant difference. The results in Figure 4 show that exercise can significantly affect lung function FEV1 (%pred). But as 50% < I2 = 81% indicates a high heterogeneity of the results, the conclusions obtained are not reliable and require further subgroup analysis.
Asthma causes damage to the physiological health of patients. Besides, children with asthma feel disturbed in their daily life from sleeping, learning ability, social communication, exercise, entertainment to leisure activities, which could severely decrease the life of quality of them. Nonetheless, all included papers showed significant differences in quality of life scores, which may preliminarily indicate a common understanding that exercise can reduce asthma symptoms. Extreme heterogeneity in QOL score I2=100% as shown in Figure 5 also led to unstable analysis results, thus further sensitivity analysis is required to reach a final conclusion.
Effects of Physical Exercise on Lung Function FEV1(%pred) of Patients with Asthma
There is great heterogeneity among the included literature after performing combined effects. The subgroup analyses combined with Table 2 and Figure 6 show that: 1) Physical exercise can improve FEV1 (%pred) of patients with asthma by 0.05 > P = 0.008; 2) There is currently insufficient evidence to prove whether the age and the intensity of exercise can significantly affect the performance of lung function; 3) Aerobic exercise had a significantly greater effect on FEV1 (%pred) than combined exercise and free-choice exercise 0.05 > P = 0.04; 4) The source of heterogeneity was most likely from exercise containing breathing exercise or intervention method lasting ≥60min each time,27–29 When groups with heterogeneity were excluded, the rest 15 included studies were highly homogeneous (I2=0%) and significantly different overall. It had been found in clinical trials that regular exercise can reduce the risk of asthma in children. A RCT study by Min et al39 showed that after three months of treatment with high-intensity exercise combined with drugs, the levels of lung function parameters—FVC (forced vital capacity), FEV1 and PEF (peak expiratory flow) in the exercise group—were higher than those in the control group, and the serum contents of inflammatory factors—IL-1, IL-2, HMGB1 and TNF-α—were lower than those in the control group, which indicated that exercise could reduce the symptoms of asthma to a certain extent. Another study showed that regular exercise played a role of resisting Immunoglobulin E (IgE),14 thus reducing the level of antigen-specific IgE in the blood of patients, which are the main mechanisms for improving lung function.
In this study, the subgroup of Table 2 (Figure 8) shows that aerobic exercise had shown significant differences compared with other intervention methods in the subgroup. So it is feasible to improve lung function parameters by exercise, and aerobic exercise may have a better effect on lung function than other types of exercise. In an RCT study of adult asthmatic patients, Mends et al40 found that the total number of cells and eosinophils in induced sputum (P = 0.004) and the level of Fractional Exhaled Nitric Oxide (FeNO) (P = 0.009) were decreased in the experimental group after three months of aerobic exercise. The days of asymptomatic asthma and VO2max were also significantly improved (P < 0.001), and the exacerbation of asthma in the experimental group was reduced (P < 0.01). In addition, there was a strong positive correlation between the baselines—FeNO and eosinophil counts—and improvement after training. Regular aerobic exercise also affects airway remodeling. In the asthma mouse model, aerobic exercise increases glucocorticoid receptor and anti-inflammatory cytokines, reduces the expression of inflammatory mediators and restores airway remodeling.41 At the same time, aerobic exercises such as swimming and jogging can improve the exercise tolerance of the body, enhance the respiratory muscle strength, improve the thoracic volume, and promote the air exchange in the lung so as to effectively increase the rate and function of lung ventilation.42
The Influences of Quality of Life on Patients with Asthma
Individual paper was gradually examined one by one through the sensitivity analysis. Finally, after one article with high heterogeneity was excluded, seven articles containing quality of life scoring parameters were included for comprehensive analysis, whose results showed that there was a high degree of homogeneity among the seven studies and had significant difference from the control group. A comparative study of patients with bronchiectasis found that sedentary behaviour was the only factor leading to hospitalization, and the sedentary group was 5.91 times the hospitalization rate of the exercise group.43 The sensitivity analysis showed that all exercises could significantly improve the quality of life scoring of patients with asthma. Long-term lack of exercise resulting in decreased physical activity is an important factor affecting the treatment effect and quality of life of patients with asthma.44 Most of the body functions of asthma patients in daily life belong to the sub-health level, so physical exercise can improve their bodies’ ability to adapt to the environment. Studies have found that the diversity of intestinal microorganisms in athletes is higher than that in normal people by comparing the composition of microbial communities of them, which has also produced the view of “biodiversity hypothesis”.45 Metagenomics and other studies focusing on healthy and diseased individuals have shown that decreased biodiversity and altered microbiota composition in the gut and skin are associated with a variety of inflammatory states including asthma, allergy, inflammatory bowel disease, type I diabetes and obesity.46 Mancuso et al47 made an assessment of longitudinal asthma status in 256 patients in New York who joined in increased physical activity in life, the results of which showed significant improvement in AQLQ scores as exercise cycle increased. Therefore, forming regular exercise habits is a scientific method to reduce and control the incidence of asthma. Although the mean difference of 0.41 (Figure 7) was statistically significant, it was slightly less than the minimal clinically significant difference (0.5) reported in the study of Juniper et al48.Therefore, overall speaking, disease symptoms may not improve significantly among patients. But Figure 9 aerobic exercise subgroup shows high homogeneity and statistical significance and achieves the minimal clinically significant difference (0.52). It also showed that aerobic exercise could provide minimal improvement in patients’ quality of life.
 |
Figure 9 Improvement of quality of life by aerobic exercise. |
Scholar Sanz‐Santiago et al26 adopted the 60min-resistance exercise test in studying patients’ quality of life score scale, and the result is not significantly heterogeneous with other studies, which may also indicate that exercise duration is not a factor causing heterogeneity. As shown in Figure 8, FEV1 (%pred) lung function was significantly improved by Yoga and Tai Chi, which emphasized breath training. Breath training mainly included abdominal breathing exercise and chest expansion exercise. The combination of chest breathing and abdominal breathing could effectively increase thoracic movement, promote gas exchange in the lung and improve lung function.49 Compared with other exercises, the exercise containing respiratory training might show more significant improvement in lung function. There is a study that selected 92 cases of asthma patients who were admitted to a hospital and those cases were randomly divided into experimental group and control group. The intervention measures were lip-abdominal breathing and vertical breathing exercise. After three months of intervention training, lung function recovery was promoted and exercise tolerance and quality of life were improved as well.50 In the included papers, the author Gülcan adopted yoga intervention in his study, while yoga exercises mainly emphasized the body posture and breath method for breathing adjustment. And Gao Wei, Chen Ming and other authors adopted the combination of Tai Chi breathing exercise and other conventional interventions. As a result, the sensitivity analysis in Table 4 shows that the results of the studies by Gao Wei and Chen Ming have relatively high homogeneity, which can significantly improve lung function FEV1 (%pred).
 |
Table 4 Sensitivity Analysis of FEV1 (%pred) in Respiratory Exercise Group |
Limitations and Inadequacies
1) This study merely focuses on two indicators, pulmonary function FEV1 (%pred) and quality of life score. Therefore, to some extent, the study is not comprehensive. 2) Exercise that includes respiratory training can promote FEV1 (%pred). However, due to the limited amount of included literature and relatively high heterogeneity, the experimental conclusion needs to be further improved. 3) All the subjects had signed the informed consent form in the 17 included articles, leading to a non-double-blind trial. The lack of blinding may make the measurement and study results, such as quality of life evaluation, deviate from the reality, showing a certain degree of subjectivity.
Conclusion
Current evidence from the included literature suggests that physical exercise interventions positively improve lung function FEV1 (%pred) and quality of life scores in asthma patients. Different types of exercise have different effects on patients with asthma as well. Exercises that contain respiratory training and aerobic exercise have a greater effect on FEV1 (%pred). These interventions may serve as a method that is cost-effective and easy to have feasible adjunctive therapy. There were certain limitations in terms of research methods, such as limited observation indicator, small amount of literature on certain exercises, and not having blinding method. However, this paper still sheds lights on improving asthma patient symptoms by exercise and offers references on future research on asthma by exercise for medical staff.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Beck KC, Hyatt RE, Mpougas P, et al. Evaluation of pulmonary resistance and maximal expiratory flow measurements during exercise in humans. J Appl Physiol. 1999;86(4):1388–1395. doi:10.1152/jappl.1999.86.4.1388
2. Puranitee P, Kamchaisatian W, Manuyakorn W, et al. Direct medical cost of Thai pediatric asthma management: a pilot study. Asian Pac J Allergy Immunol. 2015;33(4):296–300.
3. Huang K, Yang T, Xu J, et al. Prevalence, risk factors, and management of asthma in China: a national cross-sectional study. Lancet. 2019;394(10196):407–418. doi:10.1016/S0140-6736(19)31147-X
4. Crimi E, Bartalucci C, Brusasco V. Asthma, exercise, and the immune system. Exerc Immunol Rev. 1996;2:45–64.
5. Mainardi TR, Mellins RB, Miller RL, et al. Exercise-induced wheeze, urgent medical visits, and neighborhood asthma prevalence. Pediatrics. 2013;131(1):127–135. doi:10.1542/peds.2012-1072
6. Sullivan PW, Campbell JD, Ghushchyan VH, et al. Outcomes before and after treatment escalation to global initiative for asthma steps 4 and 5 in severe asthma. Ann Allergy Asthma Immunol. 2015;114(6):462–469.e6. doi:10.1016/j.anai.2015.03.019
7. Jaakkola JJK, Aalto SAM, Hernberg S, et al. Regular exercise improves asthma control in adults: a randomized controlled trial. Sci Rep. 2019;9(1):20188. doi:10.1038/s41598-019-48484-8
8. Efaat A, Gawish M. Effect of physical training on health-related quality of life in patients with moderate and severe asthma. Egypt J Chest Dis Tuberc. 2015;64(4):761–766. doi:10.1016/j.ejcdt.2015.07.004
9. Lucas S, Plattsmills T. Physical activity and exercise in asthma: relevance to etiology and treatment. J Allergy Clin Immunol. 2005;115(5):928–934.
10. Del Giacco SR, Firinu D, Bjermer L, et al. Exercise and asthma: an overview. Eur Clin Respir J. 2015;2(1):27984. doi:10.3402/ecrj.v2.27984
11. Liberati A, Altman DG, Tetzlaff J, et al. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: explanation and elaboration. Epidemiol Biostat Public Health. 2009;6(10):e1–e34.
12. Cochrane LM, Clark CJ. Benefits and problems of a physical training programme for asthmatic patients. J Cardiopulm Rehabil Prev. 1992;12(5):345–351.
13. Counil FP, Varray A, Matecki S, et al. Training of aerobic and anaerobic fitness in children with asthma. J Pediatr. 2003;142(2):179–184. doi:10.1067/mpd.2003.83
14. Moreira A, Delgado L, Haahtela T, et al. Physical training does not increase allergic inflammation in asthmatic children. Eur Respir J. 2008;32(6):
15. Wang JS, Hung WP. The effects of a swimming intervention for children with asthma. Respirology. 2010;14(6):838–842. doi:10.1111/j.1440-1843.2009.01567.x
16. Turner S, Eastwood P, Cook A, et al. Improvements in symptoms and quality of life following exercise training in older adults with moderate/severe persistent asthma. Respiration. 2010;81(4):302–310. doi:10.1159/000315142
17. Jia L, Xingqiao W, Army B, et al. The role of high-intensity intermittent exercise and medium intensity continuous exercise in the management of childhood asthma . J Beijing Sport Univ. 2016;39(10):58–64.
18. Abdelbasset WK, Alsubaie SF, Tantawy SA, et al. Evaluating pulmonary function, aerobic capacity, and pediatric quality of life following a 10-week aerobic exercise training in school-aged asthmatics: a randomized controlled trial. Patient Prefer Adherence. 2018;12:1015–1023. doi:10.2147/PPA.S159622
19. Carew C, Cox DW. Laps or lengths? The effects of different exercise programs on asthma control in children. J Asthma. 2017;55:881–887.
20. Toennesen LL, Meteran H, Hostrup M, et al. Effects of exercise and diet in nonobese asthma patients—A randomized controlled trial. J Allergy Clin Immunol Pract. 2017;2017:
21. Qiong C, Fengqin W, Sun X. Experimental study on aerobic exercise improving exercise ability and quality of life of asthmatic children . Guangzhou Sports Institute Daily. 2020;40(5):125–128.
22. Van Veldhoven NHMJ, Vermeer A, Bogaard JM, et al. Children with asthma and physical exercise: effects of an exercise programme. Clin Rehabil. 2001;15(4):360–370. doi:10.1191/026921501678310162
23. Boli C, Study on the role of exercise in the prevention and management of childhood asthma [D] Chongqing Medical University, 2010.
24. Jing T, Chengjun L, Junming H, et al. Application of exercise prescription in condition control of children with asthma. Chin J Child Health. 2019;27(12):1331.
25. Basaran SS, Guleruysal FF, Ergen NN, et al. Effects of physical exercise on quality of life, exercise capacity and pulmonary function in children with asthma. J Rehabil Med. 2006;38(2):130–135. doi:10.1080/16501970500476142
26. Sanz‐Santiago V, Diez‐Vega I, Santana‐Sosa E, et al. Effect of a combined exercise program on physical fitness, lung function, and quality of life in patients with controlled asthma and exercise symptoms: a randomized controlled trial. Pediatr Pulmonol. 2020;55:1608–1616.
27. Ming C, Yang G. Effect of exercise on rehabilitation treatment of patients with bronchial asthma . J Wannan Med Coll. 2012;1(6):458–461.
28. Turan GB, Tan M. The effect of yoga on respiratory functions, symptom control and quality of life of asthma patients: a randomized controlled study. Complement Ther Clin Pract. 2020;38(1):101070. doi:10.1016/j.ctcp.2019.101070
29. Wei G. Effectiveness analysis of respiratory training combined with exercise therapy in patients with asthma in remission . China Pract Med. 2020;15(24):154–156.
30. Williams N. The Borg Rating of Perceived Exertion (RPE) scale. Occup Med (Chic Ill). 2017;67(5):404–405. doi:10.1093/occmed/kqx063
31. J Dwyer, R Bybee. Heart rate index of anaerobic threshold . China Sports Sci Technol. 1984:Z3:46–47.
32. Carlsen KCL, Haland G, Devulapalli CS, et al. Asthma in every fifth child in Oslo, Norway: a 10‐year follow up of a birth cohort study*. Allergy. 2010;61(4):454–460. doi:10.1111/j.1398-9995.2005.00938.x
33. Suman OE, Beck KC, Babcock MA, et al. Airway obstruction during exercise and isocapnic hyperventilation in asthmatic subjects. J Appl Physiol. 1999;87(3):1107–1113. doi:10.1152/jappl.1999.87.3.1107
34. Stirling DR, Cotton DJ, Graham BL, et al. Characteristics of airway tone during exercise in patients with asthma. J Appl Physiol. 1983;54(4):934–942. doi:10.1152/jappl.1983.54.4.934
35. Beck KC, Offord KP, Scanlon PD. Bronchoconstriction occurring during exercise in asthmatic subjects. Am J Respir Crit Care Med. 1994;149(2 Pt 1):352–357. doi:10.1164/ajrccm.149.2.8306029
36. Eichenberger PA, Diener SN, Kofmehl R, et al. Effects of exercise training on airway hyperreactivity in asthma: a systematic review and meta-analysis. Sports Med. 2013;43(11):1157–1170. doi:10.1007/s40279-013-0077-2
37. Avallone KM, Mcleish AC. Asthma and aerobic exercise: a review of the empirical literature. J Asthma Res. 2013;50(2):109–116. doi:10.3109/02770903.2012.759963
38. Shaofu Z. It is suggested that forced vital capacity / vital capacity should be used as a routine measure of pulmonary function to judge airflow obstruction in chronic obstructive pulmonary disease . Chin J Tuberc Respir. 2001;024(004):235.
39. Min L, Guoping Y, Liang Z. Effects of high intensity intermittent exercise combined with drug therapy on airway function and inflammatory factor secretion in asthmatic children . J Hainan Med Coll. 2018;24(3):331–334.
40. Mendes FAR, Almeida FM, Cukier A, et al. Effects of aerobic training on airway inflammation in asthmatic patients. Ed Sci Sports Exerc. 2011;43(2):197–203. doi:10.1249/MSS.0b013e3181ed0ea3
41. Silva RA, Almeida FM, Olivo CR, et al. Exercise reverses OVA-induced inhibition of glucocorticoid receptor and increases anti-inflammatory cytokines in asthma. Scand J Med Sci Sports. 2016;26(1):82–92. doi:10.1111/sms.12411
42. Liu N, Caixia L, Xu L, et al. Effects of respiratory function training on pulmonary function and quality of life in children with stable asthma . Gen Nurs. 2015;000(033):3362–3364.
43. Alcarazserrano V, Gimenosantos E, Scioscia G, et al. Association between physical activity and risk of hospitalisation in bronchiectasis. Eur Respir J. 2020;55(6):1902138. doi:10.1183/13993003.02138-2019
44. Santos-Silva R, Melo C, Gonçalves D, et al. Comparison between exercise performance in asthmatic children and healthy controls – physical Activity Questionnaire application. Rev Port Pneumol. 2014;20(3):138–145. doi:10.1016/j.rppneu.2013.11.005
45. Clarke SF, Murphy EF, O’Sullivan O, et al. Exercise and associated dietary extremes impact on gut microbial diversity. Gut. 2014;63(12):1913–1920. doi:10.1136/gutjnl-2013-306541
46. Haahtela T, Holgate S, Pawankar R. The biodiversity hypothesis and allergic disease: world allergy organization position statement. World Allergy Organ J. 2013;6(1):3. doi:10.1186/1939-4551-6-3
47. Mancuso CA, Choi TN, Westermann H, et al. Improvement in asthma quality of life in patients enrolled in a prospective study to increase lifestyle physical activity. J Asthma. 2012;50:103–107.
48. Juniper EF, Guyatt GH, Willan A, Griffith LE. Determining a minimal important change in a disease-specific quality of life questionnaire. J Clin Epidemiol. 1994;47(1):81–87. doi:10.1016/0895-4356(94)90036-1
49. Yi D. Effect of balloon breathing training on respiratory function of asthmatic patients . Lab Med Clinic. 2016;13(014):2032–2034.
50. Weiwe Z. Effects of vertical breathing gymnastics combined with lip abdominal breathing on exercise tolerance and quality of life in patients with asthma . Nurs Pract Res. 2019;16(23):77–79.
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Impact of Baseline Lung Function on Future Exacerbations in Patients with Moderate-to-Severe Asthma
Khan AH, Gray C, Eckert L, Amand C, Maroni J, Wang Z, Jones B, Berni T, Morgan CL, Rowe PJ
Journal of Asthma and Allergy 2022, 15:1639-1644
Published Date: 11 November 2022
Mometasone/Indacaterol/Glycopyrronium (MF/IND/GLY) and MF/IND at Different MF Strengths versus Fluticasone Propionate/Salmeterol Xinafoate (FLU/SAL) and FLU/SAL+ Tiotropium in Patients with Asthma
van Zyl-Smit RN, Chapman KR, Kerstjens HAM, Gessner C, Sagara H, Tanase AM, Hosoe M, Pethe A, Lawrence D, Tillmann HC, D'Andrea P
Journal of Asthma and Allergy 2023, 16:123-134
Published Date: 20 January 2023
Impact of Lung Function on Asthma Exacerbation Rates in Children Treated with Dupilumab: The VOYAGE Study
Guilbert TW, Murphy KR, Hamelmann E, Ross KR, Gupta A, Fiocchi A, Xia C, Gall R, Ledanois O, Radwan A, Jacob-Nara JA, Rowe PJ, Deniz Y
Journal of Asthma and Allergy 2024, 17:81-87
Published Date: 8 February 2024
Characteristics of Older Individuals with Asthma Being Treated with Biologics
Aetou M, Kiskinov Y, Ratsimba SFN, Barth M, Pizarro C, Bergs I, Spiesshoefer J, Skowasch D, Dreher M
Journal of Asthma and Allergy 2025, 18:993-1002
Published Date: 11 June 2025
The Effects of Obesity on Lung Physiology, the Prevalence and Severity of Chronic Pulmonary Diseases, and Inhalation Treatment
Fröhlich E
Drug Design, Development and Therapy 2025, 19:11885-11900
Published Date: 30 December 2025