Back to Journals » Cancer Management and Research » Volume 18

Perioperative Body Image Trajectories in Amputation Patients with Malignant Bone Tumors: A Latent Transition Analysis
Authors Li R ![]() , Wang Y, Mu D, Song H, Li YF, Zhao H
, Wang Y, Mu D, Song H, Li YF, Zhao H
Received 9 October 2025
Accepted for publication 30 December 2025
Published 7 January 2026 Volume 2026:18 573128
DOI https://doi.org/10.2147/CMAR.S573128
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Seema Singh
Rui Li,1,* Yao Wang,1,* Dandan Mu,1,* Hong Song,2 Yi-Fan Li,1 Huan Zhao1
1Department of Orthopaedic, The Second Affiliated Hospital of Xuzhou Medical University, Xuzhou, Jiangsu, People’s Republic of China; 2Department of Nursing, The Second Affiliated Hospital of Xuzhou Medical University, Xuzhou, Jiangsu, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Huan Zhao, Department of Orthopaedic, The Second Affiliated Hospital of Xuzhou Medical University, Xuzhou, Jiangsu, 221000, People’s Republic of China, Email [email protected]
Objective: To explore the changes in latent categories of body image among patients with malignant bone tumors before and after amputation surgery over time, and to analyze the influencing factors.
Methods: Between October 2021 and December 2024, 194 patients with malignant bone tumors were assessed before and after surgery using a general questionnaire and the Body Image Scale to analyze latent changes.
Results: Patients were categorized into two groups based on their body image before and after amputation: the high body image group and the low body image group. The high body image group exhibited strong stability, with a probability of 0.849 of maintaining their original group status. Patients with malignant bone tumors in the low body image group tended to transition to the high body image group over time, with a transition probability of 36.4%. Logistic regression analysis revealed that patients with low social support (OR=3.580), amputation sites on the thigh (OR=2.687), forearm (OR=1.568), and hemipelvis (OR=4.015) were more likely to shift from the low body image group to the high body image group (OR > 1). Conversely, patients aged 60 years or older (OR=0.697) had a lower probability of transitioning from the low body image group to the high body image group (OR < 1). When considering the change from the high body image group to the high body image group as the reference, the probability of patients with family residence (OR=1.582) and high social support (OR=2.567) transitioning from the high body image group to the low body image group increased (OR > 1).
Conclusion: Clinical medical staff should focus on high-risk groups and intensify perioperative psychological interventions for patients. This includes providing psychological counseling and enhancing social support to improve patients’ body image and enhance their quality of life and rehabilitation outcomes.
Keywords: malignant bone tumors, amputation, body image, latent profile analysis, latent transition analysis, influencing factors
Introduction
Primary malignant bone tumors constitute approximately 1% of all tumors.1 Radical resection, or amputation, is the preferred treatment for bone tumors, significantly improving survival rates.2,3
Body image is an individual’s subjective perception, emotion, and attitude towards their own body, encompassing appearance, function, and social perception.4 Patients with bone tumors who undergo limb amputation are susceptible to body image disorders due to physiological changes, psychological impacts,5 social pressures, and various other factors. Limb deformity not only compromises the body’s integrity but also leads to chronic pain, restricted movement, and phantom limb pain, further exacerbating physical discomfort.6 Additionally, patients may experience a self-identity crisis due to changes in appearance, resulting in a strong sense of stigma, social anxiety, and even depression, which severely affects their emotional regulation.7 Studies indicate that the incidence of psychological maladjustment in amputee patients is markedly higher than in the general population.8 Prolonged psychological imbalance can decrease treatment compliance and potentially impact survival rates.9
Latent transition analysis (LTA) is a statistical method used in longitudinal research. It employs latent class modeling to identify unobservable heterogeneous subgroups (ie, latent classes) to which individuals belong at different time points and further analyzes the dynamic transitions of these class states over time. The core principle involves utilizing multi - wave longitudinal data. First, conduct a latent class analysis (LCA) at each time point independently to determine the optimal number and characteristics of the classes, ensuring measurement invariance across time. Subsequently, estimate a transition probability matrix to quantify the likelihood of individuals moving from one specific class at a prior time point to another class at a subsequent time point. This reveals heterogeneous developmental patterns within the population. Unlike traditional methods that primarily focus on changes in variable means, LTA emphasizes capturing qualitative shifts in individuals’ class memberships.10
Body image is shaped by a complex interplay of multidimensional factors. Research indicates that demographic characteristics, such as age and occupation, serve as significant influencers, as variations in them may be linked to differences in social roles, life pressures, and accessible resources.11 Concurrently, clinical features—particularly treatment - related factors like amputation site—directly alter physical form and function, thereby profoundly affecting an individual’s perception of their body. Furthermore, psychosocial factors, with the level of social support acting as a crucial external buffer resource, play a moderating role in the psychological adaptation process to bodily changes.12 Together, these elements interact to shape the patient’s body image experience across different phases of illness and treatment.
However, there may be variations in the body image levels of patients with malignant bone tumors before and after amputation. Thus, understanding the body image levels of these patients before and after amputation surgery, and providing timely management and intervention during critical stages, is beneficial for maintaining their physical and mental health. This is crucial for their prognosis and overall well-being.13
Research on the body image of amputee patients with malignant bone tumors has been limited to analyzing the influencing factors of cross-sectional surveys, which cannot capture the heterogeneity among patients. There are also no reports on the evolution of body image over time before and after amputation surgery.
In light of this, this study utilized Latent Transition Analysis to explore the longitudinal trends in body image levels among patients with malignant bone tumors before and after amputation surgery, which aids healthcare professionals in early identification of individuals at high risk for body image disturbance and enables the implementation of targeted psychological interventions. Future research could further integrate biomarkers and longitudinal data to develop precise dynamic management models.
Study Subjects and Methods
Study Subjects
From October 2021 to December 2024, a convenience sampling method was employed to select 194 patients with malignant bone tumors who were admitted to the Department of Orthopedics at the Second Affiliated Hospital of Xuzhou Medical University as the subjects of the research. Inclusion criteria: patients met the diagnostic criteria14 over 18 years old, possessed a basic understanding and communication skills, and had all signed informed consent forms. Exclusion criteria: patients with a history of mental or psychological diseases; patients with a history of physical limb disability or activity disorders. Additional exclusion criteria: severe postoperative complications, death, and other reasons that led to incomplete participation in the two longitudinal measurements. The sample size15 was calculated using the following formula:

For the repeated measures longitudinal survey, in conjunction with the pilot study, the sample size required to be at least 156 cases. Considering the 10% dropout rate typical in longitudinal surveys, the minimum sample size for this study was determined as n = 156 / (1–0.10) = 174. The study protocol was approved by the institutional ethics committee (approval number: XKZY2021090016) and the study was performed in accordance with the ethical standards of the Declaration of Helsinki. All subjects volunteered to participate in this study and signed the informed consent form.
Survey Instrument
General Information Questionnaire
The general information questionnaire was self-compiled by the researchers. It included age, gender, education level, residence, lifestyle, economic income, marital status, self-rated social support system (low, medium, high), self-rated mental health status (healthy, sub-healthy, mentally imbalanced), presence of metastases, and amputation site.
Body Image Scale (BIS)
This scale was developed by Hopwood16 and Chinese scholar Cui Wanyu.17 It encompassed three dimensions: emotion, behavior, and cognition, with a total of 10 items. Each item was scored from 0 to 3, ranging from “not at all” to “very much”. The total score ranged from 0 to 30, with higher scores indicating greater disturbance from body image problems. The Cronbach’s α coefficient for the scale was 0.940. In this study, the Cronbach’s α coefficients were 0.824 and 0.815.
Data Collection Methods
To ensure the consistency of the questionnaire distribution process and maintain data quality, all nursing staff involved in the distribution were systematically trained before the study commenced. The survey was conducted in a relatively private environment. Nurses explained the purpose and content of the survey to patients in detail, and the questionnaire was distributed after obtaining the patients’ informed consent. A unified scale was used to measure the enrolled patients at two distinct stages: upon admission/before surgery (T1) and after surgery/before discharge (T2). Patients selected the questionnaire independently. The questionnaire was retrieved immediately after completion, and any with more than two missing items were verified promptly. Researchers then strictly reviewed the returned questionnaires, focusing on the authenticity of the responses, and eliminated those that were invalid and did not meet the requirements. Two independent input methods were used to ensure the accuracy of data entry and analysis.
Statistical Methods
The statistical packages SPSS 28.0 and Mplus 8.3 were utilized for data analysis. Measurement data were characterized by mean and standard deviation, while enumeration data were described by frequency and percentage (%). In this research, t-tests and chi-square tests were employed to examine the influence factors between groups, assessing the impact of various factors on different latent profiles, with the significance level set at P < 0.05. Mplus 8.3 software was utilized to conduct a latent profile category analysis of the body image of patients with malignant bone tumors. Initially, data model C1 was established, and the number of categories was incrementally increased. The optimal fitting model was selected by comparing the log-likelihood function value (Log(L)), Akaike information criterion (AIC), Bayesian information criterion (BIC), and sample size-adjusted BIC (aBIC) values. Furthermore, the Lo-Mendell-Rubin adjusted likelihood ratio test (LRT), bootstrap-based likelihood ratio test (BLRT), and P-value were commonly used to evaluate the model fit. The entropy value was used to assess the accuracy of classification, with values closer to 1 indicating higher classification accuracy. Latent transition analysis (LTA) was applied to uncover changes and transition patterns in latent category states over time, using transition probabilities. Univariate analysis was conducted through LTA, and statistically significant indicators were selected as independent variables, with LTA body image transition categories serving as dependent variables. Logistic regression was employed to analyze the factors influencing latent transition probabilities, with a P-value of less than 0.05 considered statistically significant.
Results
Basic Information and Body Image Scale Scores
A total of 194 questionnaires were distributed, and 2 invalid questionnaires were excluded, resulting in an effective recovery rate of 98.97%. The patient information is presented in Table 1.
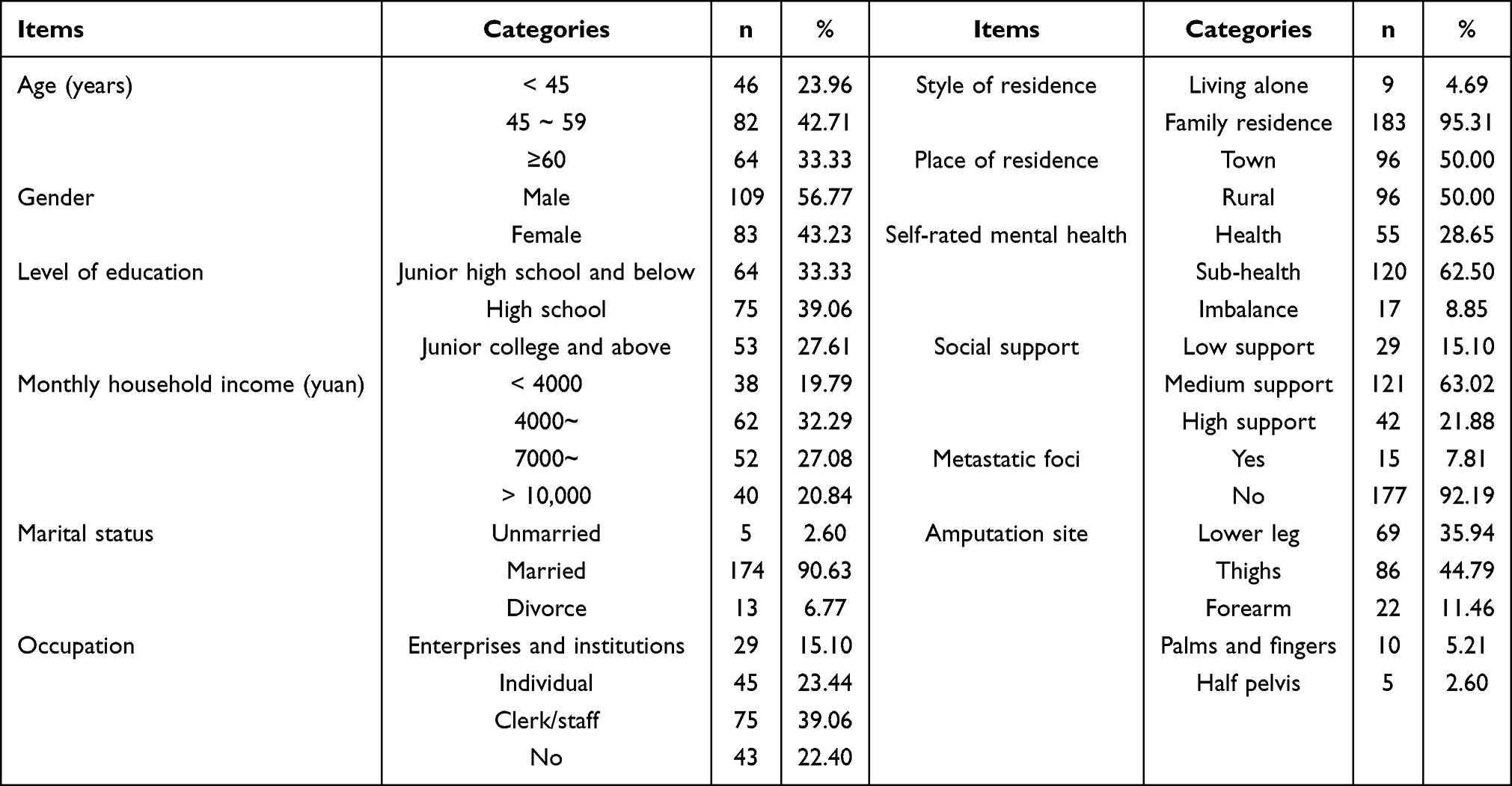 |
Table 1 General Information of the Participants (n=192) |
Latent Profile Analysis of Body Image in Patients with Malignant Bone Tumors
In this study, researchers selected scores from 10 items as the evaluation index for the body image score. Starting from the baseline model (with the number of categories set to 1), the researchers fitted models containing 1 to 4 latent profiles in sequence. The detailed data are presented in Table 2. For nodes T1 and T2, when LRT and BLRT are statistically significant, the smaller the AIC, BIC, and aBIC values are, the better the fit is. Moreover, an Entropy greater than 0.8 indicates higher credibility of the classification results. In this study, two category models were ultimately selected. Based on the distribution, the overall body image scores for category 1 were low, while those for category 2 were high. Consequently, this study named category 1 and category 2 as the pre-operation low body image group and the post-operation body image group, respectively, as depicted in Figure 1.
 |
Table 2 Comparison of Fitting Parameter Indexes for Various Latent Profile Models (n=192) |
 |
Figure 1 Latent profile line chart of body image in patients with malignant bone tumors before and after amputation surgery. |
The measurement invariance of the patient body image scale across time was evaluated by constructing a series of nested models: a configural invariance model, a weak invariance model (with factor loadings constrained equal), and a strong invariance model (with both factor loadings and item intercepts constrained equal). The model fit indices are presented in Table 3. The results indicated that the patient body image scores demonstrated configural, metric, and scalar invariance across time (as evidenced by ΔCFI ≤ 0.01), thus satisfying the necessary preconditions for conducting Latent Transition Analysis.
 |
Table 3 Model Fit Indices for the Measurement Invariance Models of the Patient Body Image Scale Across Two Time Points |
Analysis of Latent Changes in Body Image of Patients with Malignant Bone Tumors Before and After Amputation Surgery
Table 4 presents the results of latent changes in two body image categories before and after surgery in patients with malignant bone tumors. The diagonal elements of the transition matrix represent the probability that a subject remains in the original latent state at two adjacent time points. From pre-amputation to post-amputation, the probability of subjects in the low body image group and the high body image group remaining in their respective groups was higher, at 0.636 and 0.849, respectively. Patients with malignant bone tumors in the low body image group tended to transition to the high body image group over time, with a transition probability of 36.4%.
 |
Table 4 Latent State Probability and Latent Transition Probability of Body Image in Patients with Malignant Bone Tumors Before and After Amputation (n=192) |
Univariate Analysis of Latent Categories of Body Image in Patients with Malignant Bone Tumors Before and After Amputation
Univariate analysis revealed that the latent category of body image prior to surgery significantly differed by age (χ2=8.771, P=0.012) and occupation (χ2=10.904, P=0.012). The latent category of body image post-surgery also showed significant differences by age (χ2=11.741, P=0.003) and place of residence (χ2=4.099, P=0.012). There were significant variations between the two groups in terms of age (χ2=11.741, P=0.003), occupation (χ2=20.714, P<0.001), lifestyle (χ2=4.850, P=0.028), social support (χ2=6.830, P=0.033), and amputation site (χ2=18.947, P<0.001), as detailed in Table 5.
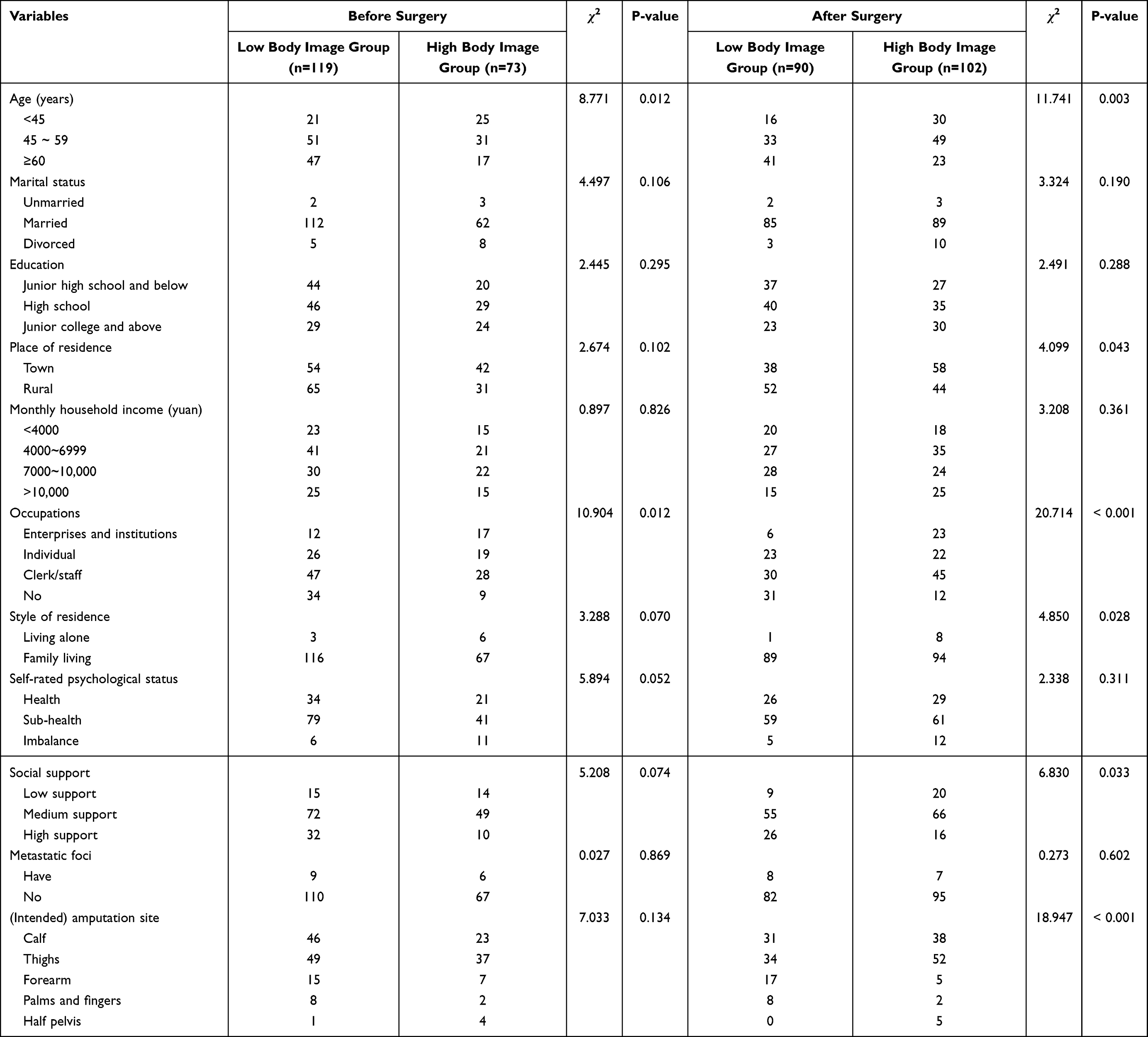 |
Table 5 Univariate Analysis of General Information and Latent Profile of Body Image (n=192) |
Influencing Factors of Latent Changes in Body Image Before and After Amputation in Patients with Malignant Bone Tumors
Taking the LTA symptom change category as the outcome variable, and the subjects who maintained the original group probability as the reference group, Logistic regression was used to explore the influence of statistically significant variables in univariate analysis on the changes of latent categories of body image in patients with malignant bone tumors before and after amputation surgery over time, and to obtain the odds ratio of subjects changing to other groups (odds ratio, P < 0.05). OR), as shown in Table 6. When the category of low body image group → low body image group was changed to the reference from pre-surgery to post-surgery, Patients with low social support (OR=3.580), amputation site of thigh (OR=2.687), forearm (OR=1.568), and hempelvis (OR=4.015) were more likely to change from low body image group to high body image group (OR > 1). However, patients aged ≥60 years (OR=0.697) were less likely to change from low body image group to high body image group (OR < 1). When taking the category change from high body image group to high body image group as the reference, the probability of patients with family residence (OR=1.582) and high social support (OR=2.567) to change from high body image group to low body image group increased (OR > 1).
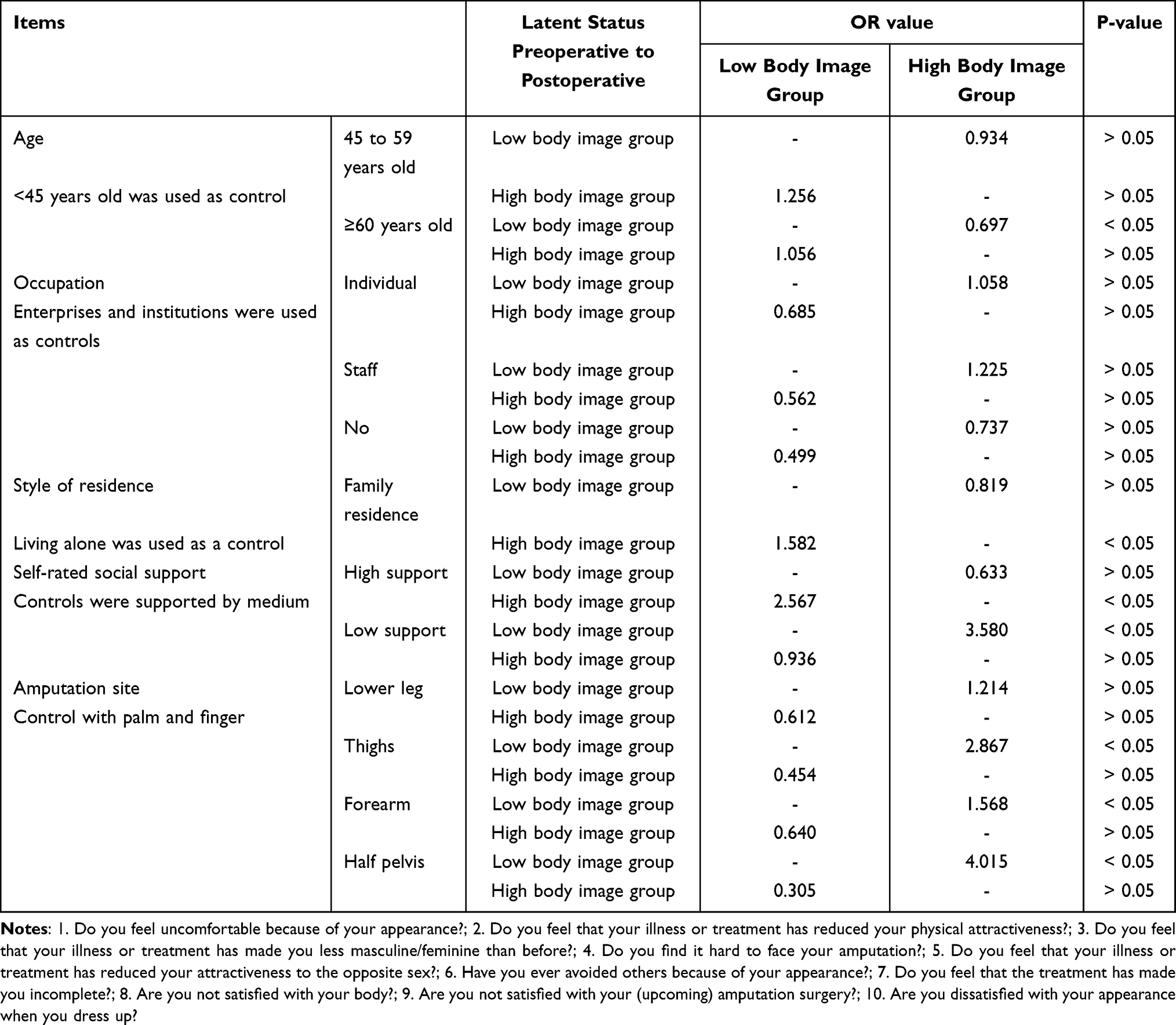 |
Table 6 Occurrence Ratio of Latent Category Transition Probability Influenced by Covariates of Body Image in Patients with Malignant Bone Tumors, Before and After Amputation (n=192) |
Discussion
The Body Image of Patients with Malignant Bone Tumors Before and After Amputation Showed Heterogeneity
The results of this study indicated that the proportion of patients with a low body image decreased from 83.2% before amputation to 55.7% post-amputation. Conversely, the proportion of patients with a high body image increased from 16.8% to 44.3%, signifying a significant shift in body image perception before and after the procedure. Patients with a lower preoperative body image may have been less affected by substantial changes in their body image. Despite the stress of disease diagnosis and impending surgery, these patients maintained hope for treatment and rehabilitation. Psychologically, they were more focused on the treatment of their disease than on changes in their physical appearance.18 In contrast, patients in the high body image group may have had preexisting psychological issues,19 such as anxiety, depression, or excessive concern about their disease prognosis, which could have led to a higher preoperative body image.20 The decrease in the proportion of patients with a low body image and the increase in those with a high body image after surgery might be attributed to changes in body image perception. Amputation disrupts patients’ original body image cognition, often resulting in a profound sense of self-rejection.21 Furthermore, postoperative challenges, including amputation care and managing complications, can limit patients’ quality of life and self-care abilities, fostering feelings of helplessness and defeat.22,23 Additionally, the ongoing impact of social stigma and discrimination can affect patients psychologically, leading them to avoid social interactions out of fear of others’ judgment. This avoidance can exacerbate feelings of loneliness and self-denial, causing more patients to transition from the low to the high body image group.24
The Latent Profile of Body Image of Patients with Malignant Bone Tumors Before and After Amputation Showed Dynamic and Stable Changes Over Time
The study’s findings indicated that from pre-amputation to post-surgery, the likelihood of subjects in the low body image group and the high body image group remaining in their respective groups was higher, at 0.636 and 0.849, respectively. Patients with malignant bone tumors in the low body image group tended to transition to the high body image group over time, with a transition probability of 36.4%. The patients with high body image before and after operation showed higher stability, and the patients with high body image before operation were more likely to have body image disorder after operation.25 Amputation, as a significant life event, directly impacts a patient’s body image and self-concept. The physical integrity of the self is compromised, making patients more susceptible to reviewing and feeling shame about their amputation, leading to continuous self-denial. This is also why patients in the high body image group have a higher probability of remaining in their original group.26 The preoperative low body image state is often based on a lack of understanding of the severity of the disease. With the realistic impact of surgical trauma and limb loss, the patient’s psychological defense mechanisms are broken, leading to an increase in body image levels. The dysfunction and social adaptation challenges faced by patients during the postoperative rehabilitation stage further exacerbate this transformation, and their original positive body perception is prone to decline. Developmental psychology theory emphasizes that psychological adaptation is a dynamic process.27 With postoperative discomfort, lifestyle changes, and economic pressures, such as chronic stressors, their psychological resources are depleted, leading to a decline in psychological adaptability. An excessive focus on the negative effects of amputation increases the body image issues for patients. Consequently, 36.4% of patients with malignant bone tumors transitioned from a low to a high level of body image after amputation.
The Latent Profile of Body Image of Patients with Malignant Bone Tumors Before and After Amputation is Affected by Many Factors
The findings of this study indicated that patients with thigh (OR=2.687), forearm (OR=1.568), and hemipelvis (OR=4.015) amputations were more likely to transition from a low to a high body image group (OR > 1). The substantial rise in the risk of a high body image following thigh amputation is attributed to its severe impact on basic walking abilities and the difficulty in fitting a prosthesis. Persistent movement disorders can lead to frustration, which in turn triggers body image issues.28 The impact of forearm amputation, while less severe, remains significant. As the most intricate operational organ of the human body, the loss of hand function irreversibly affects daily life independence and career progression. The ongoing disruption of frequent daily activities, such as writing and eating, gradually diminishes patients’ self-acceptance, thereby exacerbating their body image issues. The detrimental effects of hemipelvic amputation are not only marked by significant physical deformities but also by multi-system problems, including excrement dysfunction and sitting balance disorders, which inflict considerable physical and mental distress on patients and greatly elevate their body image levels. Furthermore, the study revealed that patients aged ≥60 years (OR=0.697) were less inclined to shift from the low to the high body image group (OR < 1). This may be because older patients tend to prioritize medical interventions focused on life support, and the relatively lower social role expectations for the elderly act as a protective factor for body image. Considering the transition from a high body image to a low body image group, family living (OR = 1.582) and high social support (OR = 2.567) increased the likelihood of patients moving from a high to a low body image group (OR > 1). Patients residing at home can restore their sense of security and self-worth through daily emotional interactions and practical life assistance. A stable family environment can mitigate the psychological impact of the adaptation period. The understanding and encouragement from family members can effectively alleviate the stigma experienced by patients and reduce their body image issues. A robust social support network not only provides practical assistance but also offers emotional acceptance and affirmation of value, thereby alleviating patient stigma, enhancing social identity, and consequently increasing the likelihood of patients transitioning from the low to the high body image group.29
Conclusions
There were two distinct categories of body image among patients with malignant bone tumors before and after amputation surgery: the high body image group and the low body image group. The likelihood of patients transitioning from the low to the high body image group increased during the perioperative period, whereas the high body image group remained relatively stable Based on the dynamic changes in body image among patients with malignant bone tumors during the perioperative period of amputation, clinical departments should implement systematic psychological care measures. Preoperatively, it is essential to conduct thorough communication and education, explaining the necessity of the surgery, expected outcomes, and the rehabilitation pathway. Inviting patients who have successfully recovered to share their experiences can help establish realistic psychological expectations and alleviate the fear that “amputation equals death”. Postoperatively, a multidisciplinary psychological support team should be established. Utilizing mindfulness-based therapies could guide patients to consciously and non-judgmentally perceive and accept changes in their body. Simultaneously, in collaboration with rehabilitation therapists, a gradual adaptive training plan should be developed to help patients regain a sense of control in their lives through functional recovery. Family members should provide ample care and encouragement, assisting patients in participating in appropriate social activities to gradually resume normal daily life.
This study has certain limitations. The use of a convenience sampling method at a single center may diminish the representativeness and universality of the sample. Additionally, reliance on patient-reported outcomes may increase the risk of reporting bias. Future efforts will aim to address these issues to optimize results. Simultaneously, focusing on the psychological issues of patients post-amputation, subsequent stages will concentrate on the formulation and implementation of intervention measures, thereby facilitating better social and life integration for patients post-amputation.
Ethics Statement
Informed consent was obtained from all patients in this study.
This study was finally approved by the Ethics Committee of the Second Affiliated Hospital of Xuzhou.
Funding
The study was supported by Project of Xuzhou Science and Technology Bureau Social Development General (KC23213 and KC23214).
Disclosure
The authors have no conflicts of interest to disclose.
References
1. Keil L. Bone tumors: primary bone cancers. FP Essent. 2020;493:22–12.
2. Huang B, Yin Z, Zhou F, Su J. Functional anti-bone tumor biomaterial scaffold: construction and application. J Mater Chem B. 2023;11(36):8565–8585. doi:10.1039/D3TB00925D
3. Manabe J. Treatment modalities for metastatic bone tumors and associated issues: focusing on surgical indications and techniques for metastatic lesions in limb bones. J Orthop Sci. 2000;5(5):524–531. doi:10.1007/s007760070034
4. Cash TF. Body Image: a joyous journey. Body Image. 2017;23:A1–A2. doi:10.1016/j.bodyim.2017.11.001
5. Xin L, Shu L, Fangyi Z, Dongmiao L. Investigation and research on the current situation of body image and coping strategies of amputees due to accidental trauma. J Continuing Educ Nurs. 2022;37(19):1810–1813.
6. Ohenewa E, Yendork JS, Amponsah B, Owusu-Ansah FE. “After cutting it, things have never remained the same”: a qualitative study of the perspectives of amputees and their caregivers. Health Expect. 2025;28(1):e70148. doi:10.1111/hex.70148
7. Wang G, Liu X, Zhu S, Lei J. Regulatory emotional self-efficacy and self-compassion mediate anxiety, depression, body image distress and subjective well-being in women with polycystic ovary syndrome: a cross-sectional study. J Adv Nurs. 2024;81(1):286–299. doi:10.1111/jan.16220
8. Bin PI, Ningxi Y. Psychosocial needs and clinical humanistic intervention of amputation patients in orthopedic accidents during the perioperative period: from the perspective of narrative medicine. Chin Med Ethics. 2019;32(2):177–181.
9. Kar Z, Kutlu A. Investigation of body image and quality of life of patients with lower limb amputation: problems experienced of patients. Niger J Clin Pract. 2023;26(11):1685–1695. doi:10.4103/njcp.njcp_307_23
10. Lanza ST, Bray BC. Transitions in drug use among high-risk women: an application of latent class and latent transition analysis. Adv App Stat Sci. 2010;3(2):203–235.
11. Frederick DA, Crerand CE, Brown TA, et al. Demographic predictors of body image satisfaction: the US body project I. Body Image. 2022;41:17–31. doi:10.1016/j.bodyim.2022.01.011
12. Almeida M, Griff MI, Brandão T. Coping and positive body image in young women with breast cancer: the buffering role of social support. Healthcare. 2025;13(3):346. doi:10.3390/healthcare13030346
13. Aydin T, Sen EI, Kesiktas N, et al. The effect of postamputation pain and phantom sensations on prosthesis use, body image, and quality of life in patients with lower-extremity amputation. Agri. 2021;33(3):183–189. doi:10.14744/agri.2020.83798
14. Fei F, Hai Z, Lili Q. The latest interpretation of the 2015 evidence-based clinical diagnosis and treatment guidelines for bone tumors in China. Chin Med Sci. 2016;2:5–6.
15. Xian L, Guifen L, Dawei H, Yangfeng W. Sample size estimation of repeated measurement design. Chin Health Stat. 2001;18(4):204–206.
16. Hopwood P, Fletcher I, Lee A, Al GS. A body image scale for use with cancer patients. Eur J Cancer. 2001;37(2):189–197. doi:10.1016/S0959-8049(00)00353-1
17. Rui L, Hong S, Chunyan Z, Yifan L, Haitang L. Analysis of the effect path of uncertainty on depressive symptoms in the main caregivers of patients with malignant bone tumors. China Med Guide. 2024;21(23):81–86.
18. Demirdel S, Ulger O. Body image disturbance, psychosocial adjustment and quality of life in adolescents with amputation. Disabil Health J. 2021;14(3):101068. doi:10.1016/j.dhjo.2021.101068
19. Miller MJ, Cook PF, Magnusson DM, et al. Self-efficacy and social support are associated with disability for ambulatory prosthesis users after lower-limb amputation. PM R. 2021;13(5):453–460. doi:10.1002/pmrj.12464
20. Ward KY, O’Keeffe F, Nolan M, Stow J, Davenport J. “Not a whole woman”: an interpretative phenomenological analysis of the lived experience of women’s body image and sexuality following amputation. Disabil Rehabil. 2021;43(2):251–261. doi:10.1080/09638288.2019.1622797
21. Imeni M, Sabouhi F, Abazari P, Iraj B. The effect of spiritual care on the body image of patients undergoing amputation due to type 2 diabetes: a randomized clinical trial. Iran J Nurs Midwifery Res. 2018;23(4):322–326. doi:10.4103/ijnmr.IJNMR_113_15
22. Chenguang C, Panjie L, Zimeng W. The impact of acceptance and commitment therapy on stigma, acceptance of disability and post-traumatic growth level in patients with lower limb amputation. Int J Transplantation Blood Purification. 2023;21(4):13–17.
23. Meng L, Sijian L. Study on common complications of amputees with different characteristics after discharge. Nurs Res. 2021;35(6):1109–1113.
24. Huizhen Y, Bo L, Xinxin Z, et al. A prospective longitudinal study on the changes in positive psychological capital levels in patients after traumatic lower extremity amputation. Chin J Modern Nurs. 2025;31(6):784–790.
25. Byrne E, Gaffey J, Hayden L, et al. Body image and cancer-related lymphoedema: a systematic review. Psychooncology. 2023;32(10):1528–1538. doi:10.1002/pon.6215
26. Bowie J, Brunckhorst O, Stewart R, Dasgupta P, Ahmed K. Body image, self-esteem, and sense of masculinity in patients with prostate cancer: a qualitative meta-synthesis. J Cancer Surviv. 2022;16(1):95–110. doi:10.1007/s11764-021-01007-9
27. Klaver P, Rohlfing KJ. Challenges in developmental psychology, a focus on sustainable development. Front Psychol. 2022;13:1086458. doi:10.3389/fpsyg.2022.1086458
28. Zhang Q, Liyan C, Yuanyuan L, Aihua Z, Lijuan Y. Meta-integration of qualitative studies on the life experiences of patients with non-traumatic lower limb amputation. Chin J Nurs. 2023;58(9):1112–1119.
29. Dongmiao L, Xin L, Shu L, Qiaomei C. A longitudinal study on post-traumatic stress disorder and social support in Amputees. Chin J Nurs. 2019;54(7):965–969.
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Changes in Depression Among Adolescents: A Multiple-Group Latent Profile Transition Analysis
Li G, Liu J, Wen H, Shen Q
Psychology Research and Behavior Management 2023, 16:319-332
Published Date: 8 February 2023
Latent Profile Analysis of Medication Beliefs in Patients with Type 2 Diabetes in the Hospital-Home Transition and Comparison with Medication Adherence
Jiang S, Luo T, Zhu Z, Huang Y, Liu H, Li B, Feng S, Zeng K
Patient Preference and Adherence 2024, 18:839-853
Published Date: 16 April 2024
Latent Profile Analysis and Determinants of Marital Adjustment in Patients with Breast Cancer
Chen XF, Shen C, Gu ZF, Dong C, Zhuang Y, Lu LH, Lu P, Li YJ
Journal of Multidisciplinary Healthcare 2024, 17:5799-5809
Published Date: 5 December 2024
Heterogeneity in Health-Related Quality of Life of Patients with Aplastic Anemia: A Latent Profile Analysis
Wu G, Li X, Ren X, Huang J, Zhang X, Liang T, Sun L, Hao M, Kuang Z, Li X, Zhang Q, Xu L, Zheng Y, Xie W
Patient Preference and Adherence 2025, 19:673-684
Published Date: 19 March 2025
The Sleep Patterns and Influencing Factors of Chronic Heart Failure Patients in China: A Latent Profile Analysis
Li Y, Li J, Qin J, Zhou S, Gong K
Nature and Science of Sleep 2025, 17:571-581
Published Date: 8 April 2025