Back to Journals » Patient Preference and Adherence » Volume 20
Perceived Barriers as Key Behavioral Predictors of Medication Adherence in Older Adults with Diabetes in Northern Iran: Insights from the Health Action Process Approach
Authors Dashteban Namaghi A ![]() , Bakhtiari A
, Bakhtiari A ![]() , Ghorbani S, Zeinali A
, Ghorbani S, Zeinali A ![]()
Received 28 July 2025
Accepted for publication 28 January 2026
Published 4 February 2026 Volume 2026:20 550698
DOI https://doi.org/10.2147/PPA.S550698
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Johnny Chen
Abouzar Dashteban Namaghi,1 Afsaneh Bakhtiari,2 Somayeh Ghorbani,3 Abolfazl Zeinali4
1Student Research Committee, Health Research Institute, Babol University of Medical Sciences, Babol, Iran; 2Social Determinants of Health Research Center, Health Research Institute, Babol University of Medical Sciences, Babol, Iran; 3Cancer Research Center, Golestan University of Medical Sciences, Gorgan, Iran; 4Department of Health Education and Health Promotion, Science and Research Branch, Islamic Azad University, Tehran, Iran
Correspondence: Afsaneh Bakhtiari, Email [email protected]
Background: Medication non-adherence remains a critical issue in older adults with type 2 diabetes. Understanding the behavioral determinants of adherence can help design more effective interventions.
Purpose: This study aimed to identify behavioral predictors of medication adherence among community-dwelling older adults with type 2 diabetes in Iran using the full Health Action Process Approach (HAPA) model.
Methods: In this cross-sectional study, 257 older adults were recruited from diabetes care centers in Gorgan, Golestan Province, Iran. Data were collected through structured interviews using a validated HAPA-based questionnaire and the 8-item Morisky Medication Adherence Scale (MMAS-8). Multiple linear and logistic regression models were used to evaluate associations between HAPA constructs and adherence.
Results: Overall, 52% of participants were non-adherent. In univariate analyses, intention, coping self-efficacy, and action planning showed some association with adherence. In the adjusted model, only perceived barriers remained significant (B = 0.034, p = 0.001; OR = 1.035, 95% CI: 1.015– 1.055), with higher scores, indicating fewer perceived barriers, linked to increased odds of adherence.
Conclusion: The findings highlight the dominant role of perceived barriers in shaping adherence behavior among older adults, overshadowing the effects of intention and planning. This suggests that interventions to improve adherence in this population should prioritize reducing contextual and psychological obstacles.
Keywords: medication adherence, aged, diabetes mellitus, type 2, health behavior, health promotion
Introduction
Medication adherence among older adults with Type 2 diabetes mellitus (T2DM) remains a substantial global challenge, especially in low- and middle-income countries (LMICs) like Iran, which are facing rapid demographic aging and rising multimorbidity.1,2 Poor adherence contributes to poor glycemic control, accelerated disease progression, increased hospitalizations, and reduced quality of life.3 Among older adults, this issue is further complicated by polypharmacy, cognitive decline, physical impairments, and economic vulnerability.4,5
Diabetes itself is becoming increasingly common in later life; in Iran, almost one-third of adults aged 60 years and older are estimated to have the disease.6 Alongside this demographic shift, evidence from urban Iranian populations indicates that more than half of patients with T2DM demonstrate low adherence to their medications.3 These patterns highlight the need for a deeper understanding of the behavioral mechanisms shaping adherence in ageing populations, particularly in settings where structural and socioeconomic constraints intersect with self-management demands.
The Health Action Process Approach (HAPA) offers a useful framework for examining how individuals form intentions and translate them into action, incorporating constructs such as self-efficacy, planning, and perceived barriers. Unlike models that focus mainly on motivation, HAPA distinguishes between a motivational phase (involving intention, outcome expectancies, and task self-efficacy) and a volitional phase (including planning, maintenance self-efficacy, and coping mechanisms).7 This two-phase structure makes it particularly suitable for investigating the complex journey from intention to action in sustained behaviors like medication adherence, especially when external barriers or internal doubts exist.8 Although HAPA has been applied in various health behaviors,9 its role in explaining medication adherence among older adults with diabetes in Iran has not been fully explored. To our knowledge, this study is the first comprehensive application of the HAPA model to investigate medication adherence among community-dwelling older adults with type 2 diabetes in Iran, aiming to generate insights needed for more context-appropriate and behaviorally informed interventions.
In recent years, several studies have applied the HAPA model to explain adherence behaviors in various populations. Wu et al10 found that both the intention to change and subsequent planning processes are shaped by perceived advantages, disadvantages, and self-efficacy, while sustained behavior is influenced by emotional and social support as well as environmental adjustments in Chinese adults with T2DM. Lu et al11 also demonstrated that HAPA-based multi-dimensional nursing interventions may enhance self-care capacity and cardiac function in patients with heart failure while also helping stabilize quality of life in the early post-discharge period. In Iran, HAPA-based research is growing but remains limited in scope. Ranjbaran et al12 applied the model in a sample of middle-aged patients with T2DM and demonstrated the relevance of planning and perceived barriers. Similarly, Mohammadi et al13 emphasized The HAPA framework has shown utility in explaining intention and behavior related to physical activity, accounting for substantial variance in hypertensive populations through constructs like self-efficacy and outcome expectancy.
Although many studies have explored behavioral determinants of treatment adherence, systematic reviews consistently show that older adults are often underrepresented, especially in theory-based research, including community-dwelling individuals with their unique cognitive, functional, and social characteristics.14,15 Given this gap, the present study seeks to explore behavioral predictors of medication adherence in community-dwelling older adults with T2DM in northern Iran using the full HAPA framework. By examining both motivational and volitional factors alongside the critical dimension of perceived barriers, the study offers insights into the complex interplay between individual beliefs, real-world constraints, and health behaviors in a vulnerable and understudied population.
Material and Methods
Study Design
This cross-sectional study was conducted between January 19 and June 19, 2024, to investigate the behavioral factors influencing medication adherence among older adults with T2DM, drawing upon the Health Action Process Approach (HAPA) as a theoretical framework. The study was grounded in the assumption that specific cognitive and motivational components, such as intention, self-efficacy, planning, and perceived barriers, may play a determining role in how consistently older adults follow their prescribed treatment regimens. The research also examined whether these behavioral constructs maintained their predictive value after adjusting for confounding influences. Participants were recruited through convenience sampling from diabetes care centers and health clinics located in Gorgan, the provincial capital of Golestan in northern Iran. All individuals had a confirmed diagnosis of T2DM, verified through clinical documentation and physician confirmation, and were actively receiving antidiabetic medications at the time of enrollment. Prior to data collection, the study received ethical approval from the Ethics Committee of Babol University of Medical Sciences (approval number: IR.MUBABOL.HRI.REC.1402.036). Informed written consent was obtained from all participants, who were informed of their right to withdraw at any stage of the study. All procedures adhered to the ethical principles set forth in the Declaration of Helsinki. The STROBE checklist was followed for observational studies.
Study Population and Sample Size
Participants were eligible if they were aged 60 or above, had been diagnosed with T2DM for over six months, were on medication, and had no major cognitive, visual, or hearing impairments, as assessed by standard screening tools (including Mini-Cog, the whisper test, and the WHO-recommended vision assessment). Those with severe physical or mental illness, recent bereavement (within six months), or incomplete responses were excluded.
The sample size was determined using G*Power 3.1 to detect a small-to-moderate correlation (r = 0.2) with a two-tailed test, α = 0.05, and 80% statistical power, resulting in a minimum of 191 participants. To ensure adequate power for multivariable regression analyses and account for potential nonresponse, the sample was increased to 257 participants. This sample size provided sufficient power to detect significant associations, including key predictors such as perceived barriers, as confirmed by our results.
Sampling Method and Data Collection
The participants were recruited via consecutive sampling from six diabetes care centers and comprehensive health care centers located in Gorgan to minimize selection bias. All eligible older adults visiting these centers during the study period were invited to participate. Of 315 individuals assessed for eligibility, 257 met the inclusion criteria and consented to participate (response rate: 81.6%). This high participation rate and detailed reporting of exclusion criteria help address concerns about selection bias. From 58 excluded people: 20 due to cognitive impairment (Mini-Cog score <3), 15 due to hearing impairment (<50% accuracy on the whisper test), 12 due to visual impairment (inability to read the 6/18 line on the WHO vision chart), and 11 due to other exclusion criteria (eg, severe physical/mental illness, recent bereavement, or declining participation). Data were gathered through in-person interviews. A single trained research team member conducted the interviews after explaining the study’s purpose and guiding participants on how to respond. Clarifications were offered as needed; no missing data were encountered in the dataset for the analyzed variables. Each session took approximately 20–30 minutes, and responses were recorded with care.
Measurements
General Information
Demographic and health-related information were collected using a standardized form, while clinical variables were cross-verified through medical record review. This instrument captured key demographic variables, including age, sex, marital status, education, occupation, retirement status, financial sufficiency, living arrangement, and self-rated health, as well as clinical variables such as polypharmacy (concurrent use of ≥5 prescribed medications for ≥1 month)., chronic conditions history, comorbidity (presence of ≥1 additional chronic condition besides type T2DM, each requiring ongoing management or lasting ≥1 year)., and past-year hospitalizations and diabetes complications.
Measurement Tool: HAPA-Based Questionnaire
The HAPA questionnaire used in this study was the Iranian version developed and validated by Ranjbaran et al (2020).12 The instrument was applied in its original form, and no further cultural adaptation was required. To ensure its suitability for our study population, we re-examined its performance in older adults with type 2 diabetes. Indices of internal consistency and test–retest stability for the eight HAPA subscales, together with the correlation matrix of the constructs, are presented in Supplementary Tables 1 and 2.
The instrument encompasses eight distinct subscales comprising a total of 38 items:
1. Intention to Adhere (2 items): evaluates the individual’s motivational readiness to initiate or maintain medication adherence.
2. Task Self-Efficacy (6 items): measures confidence in the ability to take diabetes medications under regular, routine circumstances.
3. Coping Self-Efficacy (7 items): assesses the perceived ability to manage obstacles or disruptions that might hinder adherence.
4. Recovery Self-Efficacy (3 items): evaluates one’s confidence in resuming adherence behaviors following a lapse or non-adherence event.
5. Action Planning (2 items): captures the extent to which individuals formulate concrete plans regarding the timing and manner of medication use.
6. Coping Planning (6 items): refers to the development of contingency strategies in anticipation of potential barriers.
7. Perceived Barriers (9 items): identifies psychological, contextual, or practical obstacles that may impede consistent medication intake.
8. Perceived Resources and Benefits (3 items): measures the degree to which individuals recognize facilitating factors and anticipated advantages of adherence.
Items within the subscales of medication adherence intention, perceived benefits and resources, and perceived barriers were rated on a 7-point Likert scale from “strongly agree” to “strongly disagree”. The remaining domains were assessed using a 4-point scale from “completely true” to “completely false”. In all subscales, higher scores reflect greater levels of the respective construct, such as stronger intention, greater perceived efficacy, more structured planning, increased recognition of barriers, or more acknowledged benefits, offering a multifaceted view of the behavioral mechanisms influencing adherence. Each subscale was scored and interpreted independently. A total score was calculated by summing the subscale scores. No cut-off values were defined for interpretation in this instrument. To standardize scores, all items were converted to a 0–100 scale using the following formula: Transformed score = 100 × (raw item score – minimum possible score) / possible score range. For each participant, the score for a given subscale was calculated as the mean of its respective transformed item scores.
Medication Adherence
Medication adherence was assessed using the 8-item Morisky Medication Adherence Scale (MMAS-8), a widely recognized tool in this field. The scale includes seven yes/no questions and one item rated on a 5-point scale, yielding a total score from 0 to 8. Based on established cut-offs, scores ≤5.9 indicate low adherence, 6–7.9 reflect moderate adherence, and a score of 8 denotes high adherence.16 The instrument’s psychometric properties have been validated in prior studies, including by Iranpour et al.17
Mini-Cog Test
Cognitive function was screened using the Mini-Cog, a brief and reliable tool for identifying cognitive impairment in older adults. It includes a three-word recall and a clock drawing task, with a total score ranging from 0 to 5. Participants scoring below 3 were excluded due to potential cognitive issues. The tool’s validity and reliability have been confirmed in Iranian populations.18
Whisper Test
Hearing was screened using the whisper test, a quick, low-cost method suited for older adults. From a distance of 60 cm, participants repeated whispered sequences (eg, “4-9-2”); less than 50% accuracy indicated possible hearing loss. The test has shown high sensitivity and is recommended for use in settings with limited resources.19
World Health Organization Vision Test
Vision was assessed using the World Health Organization (WHO) standard test, requiring participants to read symbols at a set distance. Those unable to read at least the 6/18 line in their better eye were excluded due to potential visual impairment affecting questionnaire completion.20
Statistical Analysis
Data were analyzed using IBM SPSS Statistics version 23. Categorical variables were summarized using frequencies and percentages, while continuous variables were described by means and standard deviations. The normality of quantitative data was evaluated through the Kolmogorov–Smirnov test and visual inspection of histogram plots. Krousel-Wood et al16 categorized MMAS-8 scores as high adherence (score = 8), moderate adherence (scores 6 to <8), and low adherence (score <6). However, to perform a binary logistic regression analysis, we divided these scores into two categories: favorable adherence, which combines both high and moderate adherence categories (MMAS-8 score ≥ 6), and unfavorable adherence, which is equivalent to the low adherence category (MMAS-8 score < 6). Independent samples t-tests were applied to compare mean scores of HAPA subscales and overall HAPA score between groups with favorable and unfavorable medication adherence. Pearson correlation coefficients were computed to explore the relationships among HAPA components. To assess the predictive effect of HAPA subscales on medication adherence scores, both simple and multiple linear regression analyses were conducted. Model assumptions were examined using residual plots and their distribution. Additionally, multivariable logistic regression (Enter method) was used to determine the association of demographic, socioeconomic, and occupational factors, along with HAPA components, with adherence status (favorable vs unfavorable). Due to the in-person interview method and immediate review of questionnaires, no missing data were encountered in the dataset for the analyzed variables.
Results
The participants had a mean age of 68.1 ± 4.7 years (range: 60–84). Most either were married (83%) and homemakers or retired without current employment (74%). Over half (53%) reported financial insufficiency. The mean duration of T2DM was 10.9 ± 4.5 years (range: 1–30). Polypharmacy affected 45% (mean number of medications: 4.6 ± 2.2), and 85% had comorbidity. Hypertension (69%) and hyperlipidemia (58%) were the most prevalent conditions (Table 1). Univariate analysis revealed several significant associations with medication adherence (p<0.05). Retirement status predicted adherence, with retirees showing lower favorable adherence (40.1%) than non-retired participants (62.2%; p=0.001). Occupation influenced adherence, lowest among working retirees (17.4%) and highest among homemakers (57.4%) and self-employed (64.3%; p=0.013). Perceived financial adequacy strongly correlated with adherence: 62.8% of those with adequate resources had favorable adherence versus 44.4% in the inadequate group (p=0.005). Hospitalization in the prior year increased adherence (56.5% vs 41.6%; p=0.018). Sex, marital status, education, living arrangement, polypharmacy, multimorbidity, and self-rated health showed no significant effect (Table 1).
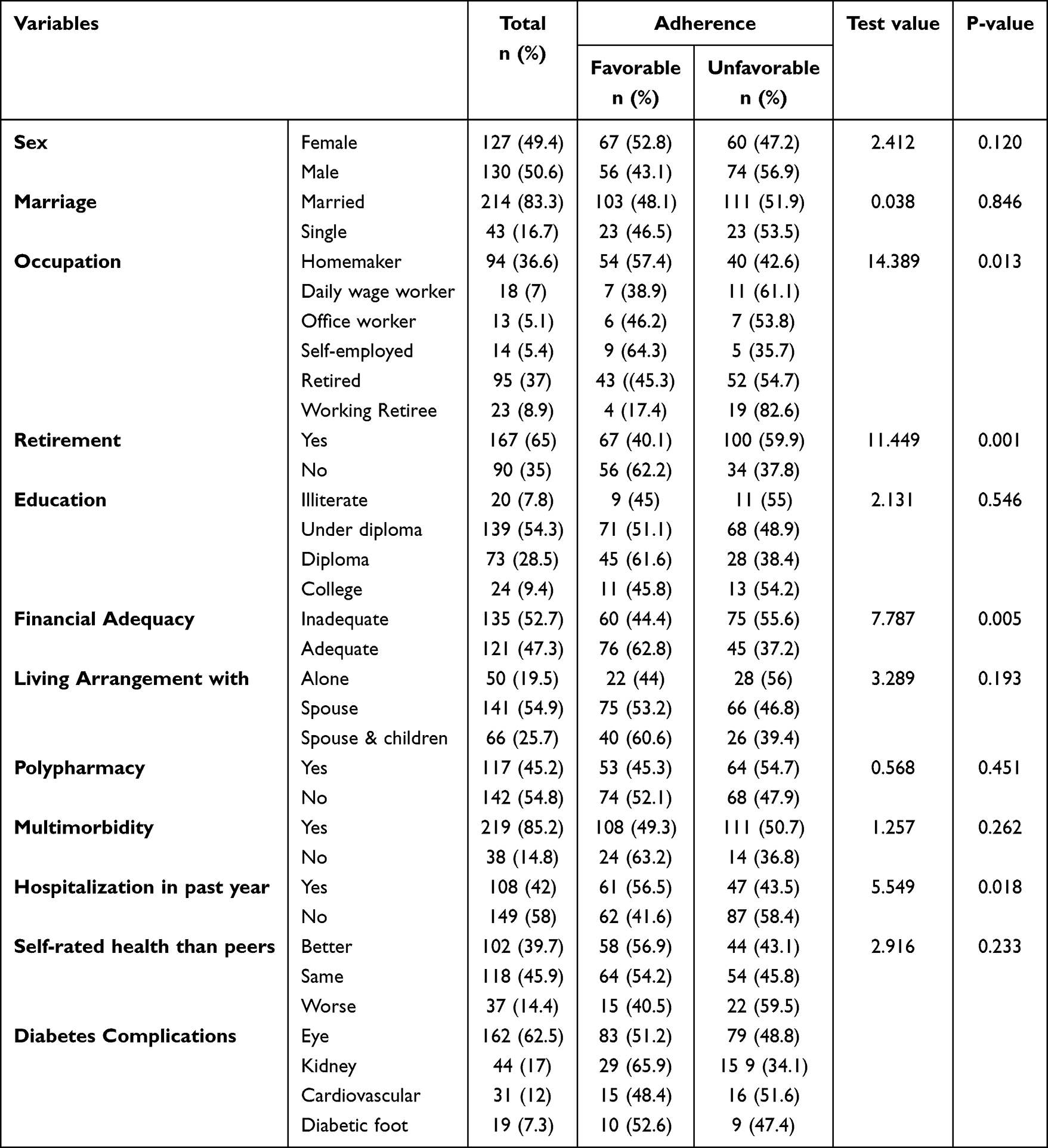 |
Table 1 Sociodemographic and Health-Related Characteristics by Medication Adherence Status (n=257) |
Medication non-adherence was observed in 52% of older adults with T2DM (Supplementary Table 3). Across HAPA constructs, only coping self-efficacy, action planning, and perceived barriers differed significantly between adherence groups. Coping self-efficacy was higher among participants with favorable adherence (69.9±17.6) compared with unfavorable adherence (65.9±15.0; t=2.000, p=0.047). Action planning showed a similar pattern (74.7±21.3 vs 67.9±20.6; t=2.609, p=0.010). Perceived barriers inversely related to adherence, with lower scores in the favorable group (46.9±18.1) versus unfavorable (58.4±17.6; t=–5.142, p<0.001), representing the largest statistical contrast in the table (t=–5.142, p < 0.001) (Table 2).
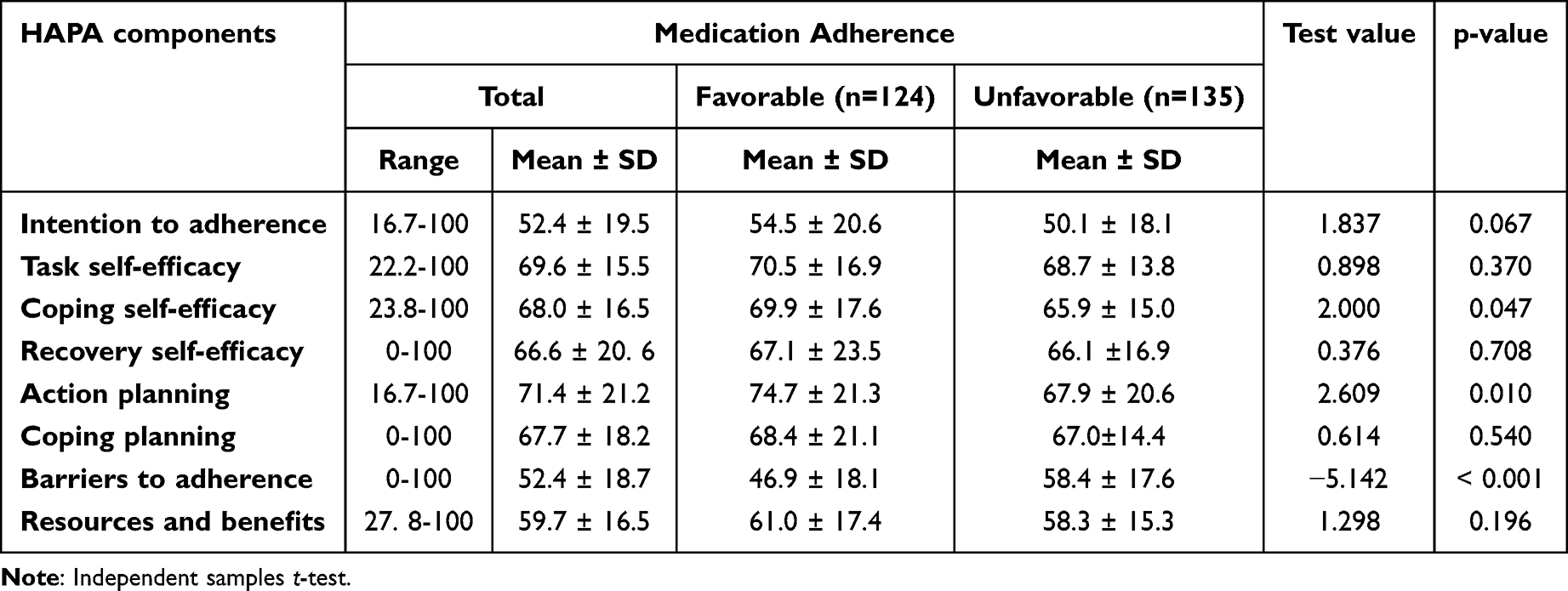 |
Table 2 Mean Score Comparison of the Health Action Process Approach Components Between Adherence Groups |
Perceived barriers to adherence were categorized into practical/logistical (Q1–2, Q7), financial (Q3), and psychosocial–emotional domains (Q4–6, Q8–9) (Figure 1). Financial barriers showed the highest overall endorsement (62.9%), followed by practical/logistical (≈42.6%) and psychosocial–emotional barriers (≈40.1%). The following results detail the distribution of responses for each of the nine items, with financial concerns most frequently reported (62.9%), travel-related insulin storage (55.6%) and forgetfulness (49.0%) also common, while psychosocial–emotional issues including stigma were less prevalent (30.9–38.2%) and injection/timing difficulties showed moderate agreement (Supplementary Table 4).
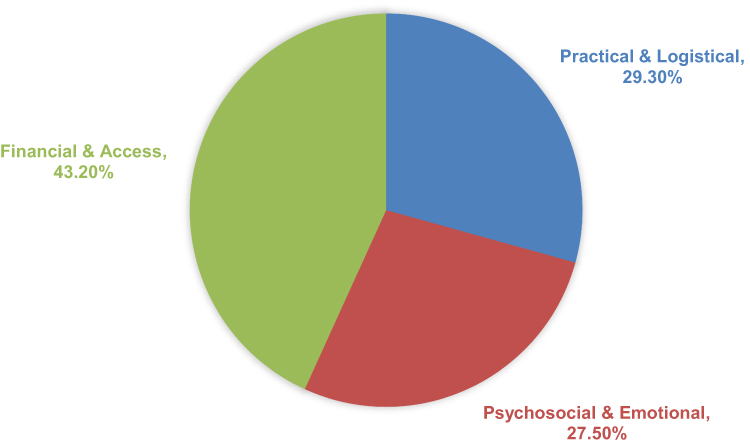 |
Figure 1 Mean Distribution of Medication Adherence Barrier Categories among Older Adults with Type 2 Diabetes. |
In the multivariable linear regression model, the barriers construct, coded such that higher values reflect fewer perceived obstacles, was the only factor that remained significantly associated with medication adherence (B=0.24, SE=0.006, p<0.001). Although intention, coping self-efficacy, action planning, and resources and benefits showed significant associations in unadjusted analyses, these relationships did not consistently hold once the model was adjusted for the full set of predictors. The remaining HAPA variables, including task self-efficacy, recovery self-efficacy, and coping planning, were not significant contributors. Overall, the model explained 14.6% of the variance in adherence (R2 = 0.146; F = 5.332; p < 0.001) (Table 3).
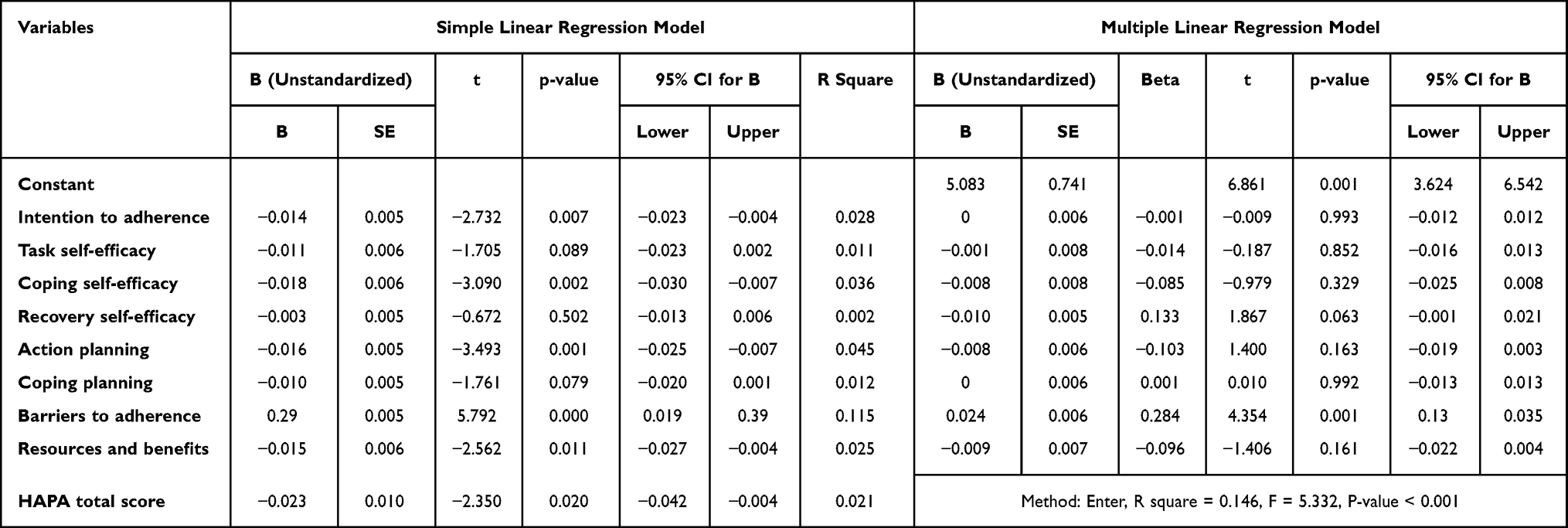 |
Table 3 Simple and Multiple Linear Regression Model to Predict Medication Adherence Behavior Score |
In the multivariable logistic regression model (Table 4), the barriers construct, reverse-coded such that higher scores indicate fewer perceived obstacles, was the only variable significantly associated with medication adherence (B=0.034, SE=0.010, p=0.001; Exp(B)=1.035, 95% CI:1.015–1.055). Retirement status was also significant, with retirees showing lower odds of adherence (B=−0.808, SE=0.319, p=0.011; Exp(B)=0.446). Other covariates, including sex, education, economic status, comorbidity, age, diabetes duration, and HAPA variables, were not significant predictors (p>0.05). The variables included in the regression models are presented in Supplementary Table 5.
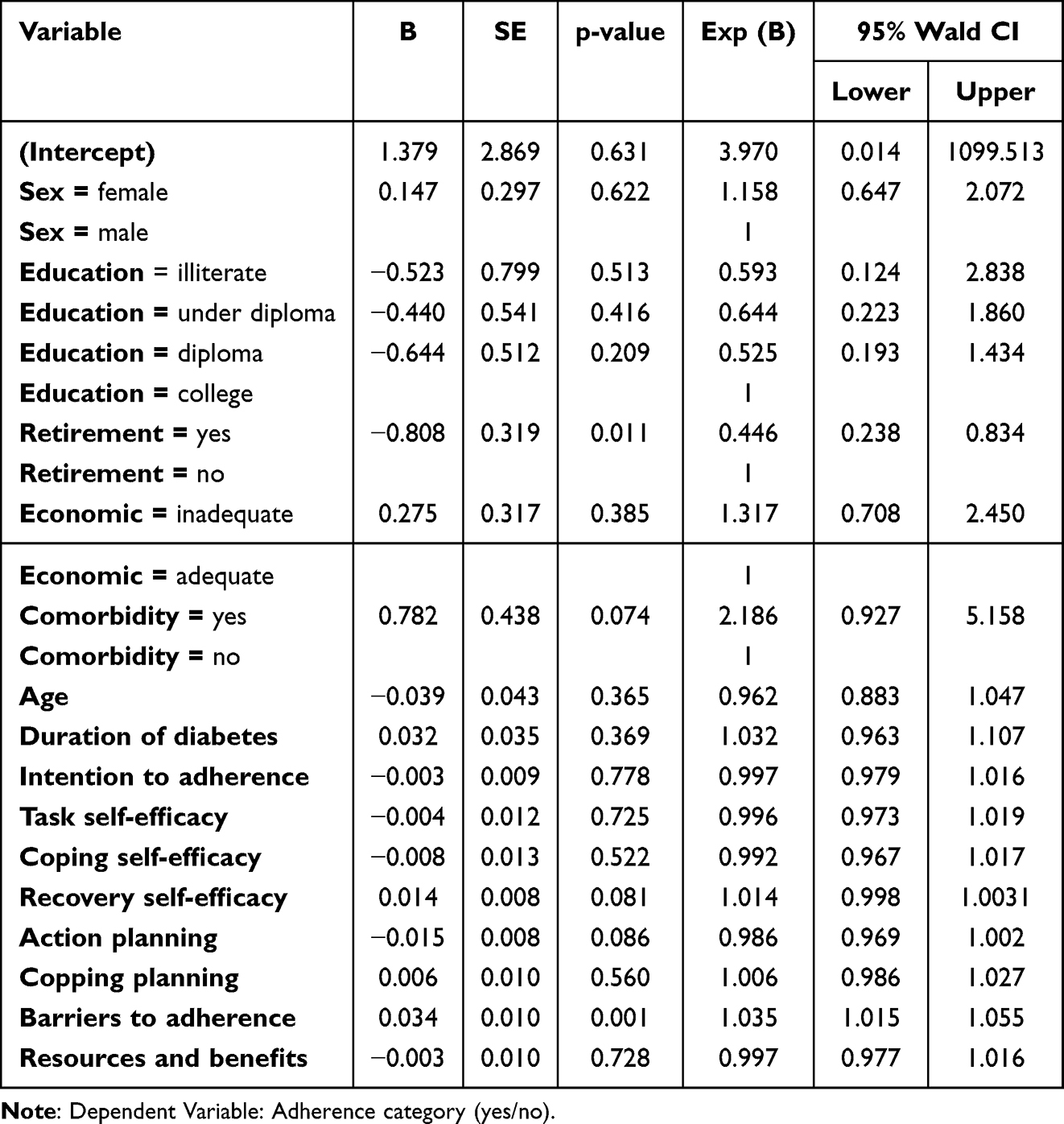 |
Table 4 Multiple Logistic Regression Analysis to Predict Adherence to Medication |
Discussion
This study aimed to investigate behavioral determinants of medication adherence among community dwelling older adults with T2DM in Iran, using the full HAPA framework. Our key finding is that perceived barriers, and not constructs like intention, coping self efficacy, or action planning, remained the only statistically significant independent predictor of non adherence in adjusted analyses (Table 4). While other constructs demonstrated associations in univariate models (Table 3), their effects dissipated when barriers were accounted for. This finding is particularly telling, considering that most HAPA-based research reports multiple significant predictors. What distinguishes our study is its focus on an older, community-based population in a LMICs, an underrepresented demographic in existing literature. By addressing this gap, we clarify how behavioral constructs operate differently in real-life, late-life contexts.
Compared to international studies, such as Rouvere et al on engagement with digital mental health platforms and by Paxton focusing on physical activity among breast cancer survivors in the US, researchers have found that volitional constructs, such as coping planning and self-efficacy, tend to reduce the negative influence of perceived barriers when it comes to predicting adherence-related behaviors.21,22 However, observational and interventional research frequently identifies barriers, complex regimens, cost, forgetfulness, as consistent suppressors of intention behavior pathways.23,24 Our results reinforce this pattern, suggesting that even well-formed intentions may fail to translate into action without addressing contextual impediments. This observed dominance of barriers provides empirical evidence for the intention-action gap, aligning with the WHO framework’s emphasis on socioeconomic and health system dimensions as critical determinants of adherence behavior.
Although our study was conducted in Northern Iran, the following comparisons are presented to provide contextual insight into adherence patterns across a range of countries from LMICs to high-income countries. Evidence from India, Brazil, and Malaysia indicates that practical and structural constraints, particularly medication cost, transportation difficulties, and limited continuity of care, often play a more decisive role in shaping adherence than motivational constructs or self-efficacy.25–27 These studies consistently show that when daily routines are disrupted by financial strain or health-system barriers, even individuals with strong motivation struggle to maintain regular medication use. In comparison, findings from high-income settings such as the United States, Canada, and several Western European countries suggest a different balance of determinants.28–30 In these regions, psychosocial factors, including confidence in self-management, coping strategies, and planning, tend to exert a stronger influence on adherence, largely because basic access, affordability, and medication supply are more reliably assured by the health system. Taken together, these cross-national patterns show that the central role of perceived barriers in our study reflects a broader trend within LMICs, where contextual constraints frequently overshadow motivational or volitional components of the HAPA model. This contrast underscores the need for adherence interventions that prioritize structural and environmental barrier reduction before attempting to strengthen self-efficacy or planning-based strategies.
Although several HAPA-based studies, especially those conducted in younger or clinical populations have reported significant effects for intention, planning, and self-efficacy, these constructs often lose their predictive power in more complex, barrier-heavy settings. For instance, Our findings align with this pattern, as even action planning lost its predictive power when contextual barriers were accounted for. Ranjbaran et al12 found that intention, planning, and perceived barriers each independently contributed to medication and dietary adherence in adults with T2DM in Tehran. Lu et al11 and Pan et al30 similarly observed that coping planning and self-efficacy significantly predicted adherence in older cardiac patients and hypertensive in China. However, our findings align with qualitative and quantitative data from elderly cohorts: factors that amplify barrier perception and diminish the unique influence of motivation or planning. For example, qualitative work by Iranian researchers (eg, interviews with cardiovascular diseases patients) consistently highlights limited access to healthcare, misunderstanding of disease, and cultural beliefs as pervasive barriers.31 Quantitative studies in Tehran, Iran show high rates of limited health literacy and renal dysfunction that independently associate with poor adherence.32 The contrast suggests that as individuals age and face compounded vulnerabilities (eg, financial constraints, polypharmacy, cognitive decline), perceived barriers become disproportionately influential, overshadowing the capacity of motivational and volitional skills (Tables 2–4). In such contexts, even individuals with good intention and self-efficacy cannot adhere unless these barriers are reduced. This pattern aligns with the WHO’s five-dimensional model of adherence, which emphasizes the interplay of patient-related and system-related factors.33
In aging populations, perceived barriers function as gatekeepers of behavior. Economic hardship, cognitive decline, complex medication regimens, and lack of support increase cognitive and logistical burden, undermining the salience of intention and reducing the efficacy of planning. Barriers elevate the perceived effort and risk of adherence actions, essentially “locking out” further behavioral processes unless mitigated. Thus, perceived barriers function as a foundational constraint in this population. Their dominant statistical association, overshadowing motivational and volitional constructs, suggests that the effectiveness of intention and planning may be conditional upon first addressing these contextual obstacles. Consequently, barrier reduction should be a primary or parallel focus alongside self-efficacy or planning interventions, making practical support a critical prerequisite for success. The modest explained variance (R2 = 0.146) is consistent with the application of psychosocial models to complex health behaviors in heterogeneous, real-world elderly populations. It underscores that while perceived barriers are a dominant and statistically robust predictor, adherence is a multifactorial phenomenon. Clinical variables, polypharmacy, health system factors, and socioeconomic constraints, not fully captured by the HAPA model, likely account for additional variance. Consequently, the primary strength and clinical relevance of our finding lies not in the quantity of variance explained, but in the qualitative identification of a specific, dominant, and actionable target for intervention: the reduction of perceived barriers.
Our research strengths include the use of a validated theoretical model in a vulnerable, understudied population and precise quantification of barrier effects. Several limitations should be noted. The cross-sectional design and reliance on self-reported data, particularly in older adults, limit causal inference and may introduce recall bias. Some potentially important influences, such as health literacy or other contextual factors, were not formally measured. Recruitment from urban diabetes care centers may also introduce selection bias, limiting generalizability to rural or culturally diverse settings. These issues highlight the need for future multi-site, longitudinal studies incorporating barrier-focused interventions and long-term assessment of adherence and glycemic control.
Conclusion
Our results show that perceived barriers, particularly financial constraints, were the most influential independent predictors of medication adherence, whereas motivational and planning-related HAPA constructs were not significant. Despite the modest explanatory power (R2 = 0.146), perceived barriers, particularly those affecting treatment access or affordability, remain important targets for intervention. The cross-sectional design and non-significant HAPA constructs limit causal inference and generalizability, yet the results provide actionable guidance for targeted interventions in resource-limited settings. Within the Iranian context, effective measures could include reducing financial burdens, simplifying treatment regimens, assisting with injection-related tasks, strengthening social support, training community health workers (Behvarz) to aid medication management in rural areas, developing community-based pick-up or home delivery systems, and incorporating brief barrier-screening questions into routine primary care. While these strategies may improve adherence, their generalizability beyond similar settings requires further study.
Data Sharing Statement
The datasets generated and analyzed during the current study are not publicly available due to privacy and ethical restrictions involving older adult participants. However, anonymized data may be made available from the corresponding author upon reasonable request and with approval from the relevant ethics committee.
Ethical Approval and Informed Consent
This study was conducted in accordance with the ethical standards of the institutional and national research committee and with the 1964 Helsinki Declaration and its later amendments. Written informed consent was obtained from all participants prior to data collection. Ethical approval was granted by the [National System of Ethics in Biomedical Research] (Approval code: IR.MUBABOL.HRI.REC.1402.036).
Acknowledgments
We would like to thank Babol University of Medical Sciences for their invaluable feedback and support throughout this study. Their contributions helped enhance the quality of the research and facilitated meaningful, informative discussions. MMAS® 2006 used with permission https://www.moriskyscale.com
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was partially supported by Babol University of Medical Sciences, Iran. The support was limited and did not cover publication or open-access fees. No other external funding was received.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Magliano DJ, Boyko EJ. IDF Diabetes Atlas 10th edition scientific committee. In: IDF DIABETES ATLAS [Internet]. 10th Ed. Brussels: International Diabetes Federation; 2021:35914061.
2. ElSayed NA, Aleppo G, Aroda VR, et al. 13. Older adults: standards of care in diabetes—2023. Diabetes Care. 2023;46(Supplement_1):S216–11. doi:10.2337/dc23-S013
3. Pourhabibi N, Mohebbi B, Sadeghi R, et al. Determinants of poor treatment adherence among patients with type 2 diabetes and limited health literacy: a scoping review. J Diabetes Res. 2022;2022:2980250. doi:10.1155/2022/2980250
4. Punnapurath S, Vijayakumar P, Platty PL, Krishna S, Thomas T. A study of medication compliance in geriatric patients with chronic illness. J Family Med Prim Care. 2021;10(4):1644–1648. doi:10.4103/jfmpc.jfmpc_1302_20
5. Amerzadeh M, Shafiei Kisomi Z, Senmar M, Khatooni M, Hosseinkhani Z, Bahrami M. Self-care behaviors, medication adherence status, and associated factors among elderly individuals with type 2 diabetes. Sci Rep. 2024;14(1):19118. doi:10.1038/s41598-024-70000-w
6. Fotouhi F, Rezvan F, Hashemi H, et al. High prevalence of diabetes in elderly of Iran: an urgent public health issue. J Diabetes Metab Disord. 2022;21(1):777–784. doi:10.1007/s40200-022-01051-x
7. Sahmad S, Abdullah AZ, Syafar M, Sidin I, Mallongi A. Health action process approach in non-communicable diseases: a systematic review. Pharmacogn J. 2025;17(1):107–116. doi:10.5530/pj.2024.17.15
8. Lim D, Woo K. Medication adherence and related factors among older adults with type 2 diabetes who use home health care. Geriatric Nurs. 2025;61:270–277. doi:10.1016/j.gerinurse.2024.11.014
9. Schwarzer R. Health action process approach (HAPA) as a theoretical framework to understand behavior change. Actualidades en Psicología. 2016;30(121):119–130. doi:10.15517/ap.v30i121.23458
10. Wu Y, Yu Z, Yin X, et al. Explain the behavior change and maintenance in diabetic patients using MTM-HAPA framework. Front. Psychiatry. 2024;15:1497872. doi:10.3389/fpsyt.2024.1497872
11. Lu F, Zhang L, Xu X, et al. Effects of multi-dimensional nursing based on HAPA theory on self-care ability and cardiac function in patients with coronary heart failure and heart failure. Altern Ther Health Med. 2023;29(8):601–607.
12. Ranjbaran S, Shojaeizadeh D, Dehdari T, Yaseri M, Shakibazadeh E. Determinants of medication adherence among Iranian patients with type 2 diabetes: an application of health action process approach. Heliyon. 2020;6(7):e04442. doi:10.1016/j.heliyon.2020.e04442
13. Mohammadi Zeidi I, Morshedi H, Shokohi A. Predicting psychological factors affecting regular physical activity in hypertensive patients: application of health action process approach model. Nursing Open. 2021;8(1):442–452. doi:10.1002/nop2.645
14. Gellad WF, Grenard JL, Marcum ZA. A systematic review of barriers to medication adherence in the elderly. Am J Geriatr Pharmacother. 2011;9(4):318–327. doi:10.1016/j.amjopharm.2011.02.004
15. Barry HE, McCartin M, Patterson SM. An update on medication use in older adults: a narrative review. Drugs Aging. 2021;38(2):147–168. doi:10.1007/s40266-020-00824-4
16. Krousel-Wood M, Islam T, Webber LS, Re R, Morisky DE, Muntner P. New medication adherence scale versus pharmacy fill rates in hypertensive seniors. Am J Manag Care. 2009;15(1):59. PMID: 19146365; PMCID: PMC2728593.
17. Iranpour A, Sarmadi V, Alian Mofrad A, et al. The Persian version of the 8-item Morisky Medication Adherence Scale (MMAS-8): can we trust it? J Diabetes Metab Disord. 2022;21(1):835–840. doi:10.1007/s40200-022-01047-7
18. Rezaei M, Rashedi V, Lotfi G, Shirinbayan P, Foroughan M. Psychometric properties of the Persian adaptation of mini-cog test in Iranian older adults. Int. J. Aging Hum. Dev. 2018;86(3):266–280. doi:10.1177/0091415017724547
19. Ting H-C, Huang -Y-Y. Sensitivity and specificity of hearing tests for screening hearing loss in older adults. J Otol. 2023;18(1):1–6. doi:10.1016/j.joto.2022.11.003
20. Sum G, Lau LK, Jabbar KA, et al. The World Health Organization (WHO) Integrated Care for Older People (ICOPE) framework: a narrative review on its adoption worldwide and lessons learnt. Int J Environ Res Public Health. 2022;20(1):154. doi:10.3390/ijerph20010154
21. Rouvere J, Blanchard BE, Johnson M, et al. Application of an adapted health action process approach model to predict engagement with a digital mental health website: cross-sectional study. JMIR Human Factors. 2024;11(1):e57082. doi:10.2196/57082
22. Paxton RJ. The health action process approach applied to African American breast cancer survivors. Psycho‐oncology. 2016;25(6):648–655. doi:10.1002/pon.3866
23. Chantzaras A, Yfantopoulos J. Determinants of medication adherence in patients with diabetes, hypertension, and hyperlipidemia. Hormones. 2025:1–17.
24. Mei J, Xie Y, Huang P, Jin Y, Wang X, Chen Y. The effects of HAPA theory-based case management in patients with metabolic dysfunction-associated steatotic liver disease. Ann. Hepatol. 2025;30(2):101790. doi:10.1016/j.aohep.2025.101790
25. Joshi SR, Das AK, Vijay VJ, Mohan V. Challenges in diabetes care in India: sheer numbers, lack of awareness and inadequate control. J Assoc Physicians India. 2008;56:443–450.
26. Costa FA, Guerreiro JP. Duggan C. The problematic nature of medication adherence in elderly patients with chronic conditions: a Brazilian perspective. Int J Clin Pharm. 2015;37(1):1–3.
27. Ramli A, Ahmad NS, Paraidathathu T. Medication adherence among hypertensive patients of primary health clinics in Malaysia. Patient Prefer Adherence. 2012;6:613–622. doi:10.2147/PPA.S34704
28. García-Pérez LE, Álvarez M, Dilla T, Gil-Guillén V, Orozco-Beltrán D. Adherence to therapies in patients with type 2 diabetes: a review of international literature. Patient Prefer Adherence. 2013;7:53–64.
29. Jimmy B, Jose J. Patient medication adherence: measures in daily practice. Oman Med J. 2011;26(3):155–159. doi:10.5001/omj.2011.38
30. Insel KC, Morrow DG, Brewer BB, Figueredo AJ. Executive function, working memory, and medication adherence among older adults. J Gerontol B Psychol Sci Soc Sci. 2006;61(2):P102–P107. doi:10.1093/geronb/61.2.P102
31. Kalantarzadeh M, Yousefi H, Alavi M, Maghsoudi J. Adherence barriers to treatment of patients with cardiovascular diseases: a qualitative study. Iranian J Nurs Midwifery Res. 2022;27(4):317–324. doi:10.4103/ijnmr.ijnmr_307_21
32. Bahadori M, Najari F, Alimohammadzadeh K. The relationship between health literacy and general health level of hemodialysis patients: a case study in Iran. Nephrourol Mon. 2018;10(3). doi:10.5812/numonthly.66034
33. Alvi Y, Khalique N, Ahmad A, Khan HS, Faizi N. World Health Organization dimensions of adherence to antiretroviral therapy: a study at antiretroviral therapy centre, Aligarh. Indian J Community Med. 2019;44(2):118–124. doi:10.4103/ijcm.IJCM_164_18
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Exercise Adherence and Compliance and Its Related Factors Among Elderly Patients with Type 2 Diabetes in China: A Cross-Sectional Study
Zhu Y, Cheng K, Wang H, Xu Z, Zhang R, Cheng W, Wang Y, Lyu W
Patient Preference and Adherence 2022, 16:3329-3339
Published Date: 19 December 2022
Diabetes Mellitus and Its Therapy in Brunei Darussalam – A Critical Revisit
Muhammad Haskani NH, Ming LC, Dhaliwal JS, Wee DVT, Goh BH, Ali M, Shaharuddin S, Goh KW, Goh HP
Patient Preference and Adherence 2023, 17:1131-1136
Published Date: 22 April 2023
Evaluating Strategies for Enhancing Medication Adherence in the Kingdom of Saudi Arabia (KSA): A Cross-Sectional Study
Alhomoud FK, Alwohaibi LW, Aljarrash K, Alhomoud F, Alamer K, Alsultan MM, Alqarni Y, Alotaibi N, Alsaad AK, Alqahtani AD, Alkhnbashi RS
Patient Preference and Adherence 2024, 18:2469-2480
Published Date: 8 December 2024
Development and Psychometric Validation of the ASMA Medication Adherence Questionnaire for Adults with Type 2 Diabetes in Saudi Arabia: A Cross-Sectional Study
Aloudah N
Patient Preference and Adherence 2026, 20:603658
Published Date: 19 March 2026
The Impact of the Multidisciplinary Team on Medication Adherence in Type 2 Diabetes: A Narrative Review
Kacha G, Highton PJ, Funnell MP, Seidu S, Khunti K
Journal of Multidisciplinary Healthcare 2026, 19:571581
Published Date: 18 June 2026