Back to Journals » Clinical Ophthalmology » Volume 20
Patients with Thyroid Eye Disease Initiating Teprotumumab: A Real-World Cohort Study Using the Linked IRIS-Komodo Database
Authors Mawn LA ![]() , Shriver EM, Tamhankar M, Yuan Y
, Shriver EM, Tamhankar M, Yuan Y ![]() , Xi A
, Xi A ![]() , Ayala-Haedo J, Patel H
, Ayala-Haedo J, Patel H
Received 10 February 2026
Accepted for publication 4 June 2026
Published 14 July 2026 Volume 2026:20 602582
DOI https://doi.org/10.2147/OPTH.S602582
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Sotiria Palioura
Video abstract of “Patients with Thyroid Eye Disease Initiating Teprotumumab” [602582].
Views: 5
Louise A Mawn,1 Erin Moore Shriver,2 Madhura Tamhankar,3 Yao Yuan,4 Ann Xi,4 Juan Ayala-Haedo,4 Haridarshan Patel4
1Department of Ophthalmology, Vanderbilt University Medical Center, Vanderbilt Eye Institute, Nashville, TN, USA; 2Department of Ophthalmology and Visual Sciences, University of Iowa, Iowa City, IA, USA; 3Department of Ophthalmology, Scheie Eye Institute, University of Pennsylvania, Philadelphia, PA, USA; 4Amgen Inc., Thousand Oaks, CA, USA
Correspondence: Louise A Mawn, Department of Ophthalmology, Vanderbilt University Medical Center, Vanderbilt Eye Institute, 2311 Pierce Avenue, Nashville, TN, 37232, USA, Tel +1-615-936-2020, Email [email protected]
Purpose: To describe patient characteristics and teprotumumab treatment patterns among patients with thyroid eye disease (TED), using large-scale, linked clinical and claims data.
Patients and Methods: This was an observational, retrospective cohort study using linked data from the American Academy of Ophthalmology IRIS® Registry (Intelligent Research in Sight) and Komodo Health Research Dataset (KRD; 2019– 2024). Adult (≥ 18 years) patients with a confirmed TED diagnosis in the IRIS Registry who initiated teprotumumab (ie, received ≥ 1 teprotumumab infusion in KRD) after its approval, and met continuous health plan enrollment requirements before and after treatment initiation were included. Outcomes were examined overall and stratified by TED duration at index (< 24 months vs ≥ 24 months). Outcomes included demographics (eg, age, sex at birth, race) and baseline disease burden (eg, clinical activity score [CAS], intraocular pressure, proptosis, eye signs and symptoms), as well as teprotumumab infusion patterns.
Results: A total of 2,886 patients were included (mean age: 59 years; 77% female). At baseline, 79% had ≥ 1 eye sign or symptom (proptosis: 45%; diplopia: 29%). Among 356 patients with CAS recorded, 91% had active disease (CAS ≥ 3/7 or 4/10). Teprotumumab was initiated within 12 months of TED diagnosis in 70% of patients. Among patients assessed for teprotumumab infusion patterns, 65% completed the 8-infusion course (median time to completion: 5 months); 35% discontinued (mean number of infusions received: 4); discontinuation peaked at the seventh infusion. Retreatment with teprotumumab occurred in 10% of patients completing the first course, 26% of whom completed the second course.
Conclusion: This large real-world analysis reveals high baseline TED burden, teprotumumab adoption within one year of diagnosis, and adherence to FDA-indicated dosing. The findings reflect evolving clinical practice in TED management and support the need for ongoing research to assess how teprotumumab may influence the natural history of disease over time.
Keywords: disease burden, treatment patterns, ophthalmology, TED duration, IRIS registry
Introduction
Thyroid eye disease (TED) is a chronic autoimmune condition characterized by inflammation and expansion of the extraocular muscles and orbital fat.1–3 Symptoms include proptosis, diplopia, eyelid retraction, and, in severe cases, optic nerve compression leading to vision loss.2,3 TED is commonly associated with Graves’ disease (GD), and even in mild forms, it can substantially impair quality of life.1
Historically, TED has been characterized by an active phase lasting up to 2 years, marked by inflammation and progressive tissue remodeling, followed by a chronic, inactive phase, in which proptosis and diplopia often persist.1,4,5
Until 2020, treatment options for TED were limited to systemic corticosteroids, orbital radiotherapy (ORT), non-specific immunosuppression, and off-label biologics.6 However, relapse requiring retreatment was common, underscoring the recurrent nature of TED despite standard therapies.7 Surgical interventions, including orbital decompression and strabismus surgery, are generally reserved for the inactive phase to correct persistent manifestations, such as proptosis and diplopia.8
In 2021, the European Group on Graves’ Orbitopathy (EUGOGO) introduced guidelines outlining a structured, stepwise approach to managing TED, based on disease activity and severity. For patients with active moderate-to-severe or sight-threatening disease, recommended first-line (1L) therapy includes high-dose glucocorticoids and mycophenolate sodium administered concomitantly, with escalation to second-line agents or urgent surgical intervention if response is inadequate.7,9 Similarly, the 2022 joint consensus statement from the American Thyroid Association and European Thyroid Association (ATA/ETA) recommend corticosteroids and/or ORT as 1L therapy for active TED, while reserving surgery for stable, moderate-to-severe disease.10
In the 2022 ATA/ETA statement, teprotumumab (Tepezza®) is listed as a preferred therapy (where available) for treatment of moderate-severe active TED when treatment goals are disease inactivation, reduction of diplopia and proptosis. Teprotumumab was approved in January 2020 by the US Food and Drug Administration (FDA) as the first targeted therapy for TED.1,9 As an insulin-like growth factor-1 receptor (IGF-1R) inhibitor, teprotumumab blocks dysregulated immune responses in TED by interfering with signaling through the IGF-1R and thyrotropin receptor (TSHR) complex in orbital fibroblasts and infiltrating immune cells.9,11
Teprotumumab was approved based on two randomized, double-blind, placebo-controlled clinical trials in patients with active, moderate TED.11,12 In Phase 2 (NCT01868997), 69% of patients on teprotumumab achieved the primary endpoint (≥2 mm reduction in proptosis), compared with 20% on placebo (P<0.001)12 and, in Phase 3 (NCT03298867), 83% of patients had ≥2 mm proptosis reduction versus 10% on placebo (P<0.001); benefits were also seen across other key outcomes, including clinical activity score (CAS), proptosis, diplopia, and quality of life.11
With further evidence in 2023 supporting efficacy in long-standing, and low activity TED (CAS ≤1), the FDA expanded teprotumumab’s indication in April 2023 to include all patients with TED, irrespective of disease activity level or duration.13
While clinical trials have demonstrated efficacy for teprotumumab in patients with TED, real-world evidence supporting its use remains scarce. Most studies to date have been conducted in single academic centers with small sample sizes.11,13–17 Although a small number of studies have leveraged the Academy IRIS (Intelligent Research in Sight) Registry data to provide valuable insights on patients with TED, no prior research has linked this large-scale, clinical data with administrative claims data to describe the real-world use of teprotumumab.18,19 The present study aimed to address these gaps and provide novel real-world evidence by leveraging large-scale, linked IRIS Registry data and Komodo Health’s Research Dataset (KRD) to describe the patient characteristics and teprotumumab infusion patterns among patients with TED in the US.
Materials and Methods
Data Source
This study used de-identified patient-level data from the IRIS Registry, developed by the American Academy of Ophthalmology (AAO),20 augmented with claims data from KRD21 (January 2019–December 2024). The IRIS Registry (IRIS Qdata Module dataset) is the largest, nationally representative ophthalmology registry in the US, integrating longitudinal electronic health record (EHR) data from 56 systems provided by approximately 15,000 clinicians. It includes over 11 years of data on more than 80 million unique patients and 805 million billed patient visits. KRD provides nationally representative longitudinal claims data, encompassing inpatient, outpatient, and pharmacy claims for over 330 million individuals across commercial and Medicare insurance plans.
Study Design and Population
This retrospective cohort study included adult (≥18 years) patients with a confirmed TED diagnosis in IRIS Registry data, identified using a validated algorithm developed by Verana Health.22 Eligible patients received ≥1 teprotumumab infusion on or after its approval (January 2020), as identified through KRD claims data. The index date was defined as the date of the first teprotumumab infusion (Supplemental Figure 1).
Patients were required to have continuous health plan enrollment for ≥12 months before and after the index date in the KRD claims data, defined as no gaps ≥45 days, as well as ≥3 months of clinical observation in the IRIS Registry prior to the index date. The baseline period was defined as the ≥12-month period preceding the index date, beginning at the start of continuous enrollment for the KRD claims data and the first record for the IRIS Registry EHR data. The follow-up period extended from the index date (ie, teprotumumab initiation) until the earliest of health plan disenrollment or the end of data availability.
The IRIS Registry and KRD are centralized, de-identified data repositories that can be used for research purposes. In accordance with the US Department of Health and Human Services regulations (45 CFR 46), this study did not involve human subjects as all data were de-identified and investigators had no access to patient identifiers. Therefore, institutional board review and informed consent were not required and this study adheres to the principles of the Declaration of Helsinki.
Outcomes, Measures, and Statistical Analyses
Outcomes were descriptively assessed to characterize real-world patients with TED initiating teprotumumab, including baseline demographic and clinical characteristics and infusion patterns during follow-up. Continuous variables were summarized using means with standard deviations (SDs) and medians with interquartile range (IQR), while categorical variables were reported as frequencies and percentages. Missing data were handled by excluding unknown values for continuous variables, whereas categorical variables comprised an “unknown” category.
Baseline characteristics and outcomes during follow-up were obtained from each data source as available. The IRIS Registry provided demographics (age, sex at birth, race), TED duration as of the index date, eye-related clinical measurements (CAS, intraocular pressure [IOP], visual acuity [VA], proptosis), eye signs and symptoms (assessed via diagnostic codes), and eye-related surgeries. KRD provided additional demographics (insurance type, geographic region), comorbidities, and use of TED-related treatments (eg., baseline treatments, teprotumumab infusions).
Eye-related characteristics assessed via clinical measurements were summarized among patients with available data in the IRIS Registry. Disease activity was defined using CAS measurements, with patients classified as having active disease (CAS ≥3 on a 7-point scale or ≥4 on a 10-point scale) or quiescent disease (CAS<3, CAS<4, respectively).23 Proptosis was assessed using oculus dexter (OD) and/or oculus sinister (OS) measurements, with the higher value reported when both were available. Disease activity and proptosis were assessed in the 60 days before and after the index date to account for real-world variability in measurement timing while ensuring values reflected patient status at teprotumumab initiation. IOP and VA were assessed during the baseline period, with the measurement closest to the index date retained for analysis.
During follow-up, infusion patterns were evaluated and categorized as full course completion (8 infusions) or discontinuation (received < 8 infusions). Full course completers were further stratified by the presence or absence of treatment gaps, defined as ≥90 days without an infusion based on teprotumumab’s recommended dosing schedule and clinician input. Additionally, teprotumumab retreatment was assessed as those who received ≥1 infusion following full course completion. Among discontinuers, teprotumumab reinitiation was assessed as those who received ≥1 infusion following a treatment gap.
Due to the COVID-19-related supply chain disruption, patients who initiated teprotumumab in the second half of 2020 and discontinued in the first half of 2021 were excluded from infusion pattern analyses to minimize potential bias.24
Outcomes were examined overall, as well as stratified by TED duration at index (<24 months [shorter] vs ≥24 months [longer]) to characterize patients at different disease phases. As there is no strict cut-off for the duration of active TED, with published reports ranging from 6–18 months to 3 years or more, a 24-month threshold was selected to reflect conventional definitions and align with pivotal teprotumumab trial criteria.4,5 Patients with unknown disease duration at index (N=338) were excluded from stratified analyses but included in descriptive summaries. All analyses were conducted in Databricks Runtime 11.3 LTS (Long-term Support) with Apache Spark 3.3.0 and Python 3.9.21.
Results
Study Population
Using clinical data from the IRIS Registry linked with KRD, a total of 2,886 eligible patients with TED who initiated teprotumumab were included. Of these, 2,161 had shorter (<24 months) and 387 had longer TED duration (≥24 months) at teprotumumab initiation (Supplemental Figure 2). A total of 2,637 patients were included in the infusion pattern analyses, after excluding 249 patients due to potential impact from the COVID-19-related supply chain disruption. Of these, 1,978 had shorter (<24 months) and 351 had longer TED duration (≥24 months) at teprotumumab initiation.
Baseline Demographics
In the overall population, the mean age was 59 years, and 77% were female. Most patients were of White race (70%) and 47% were from the South region. Commercial insurance was the predominant coverage type, reported in 48% of patients (Table 1).
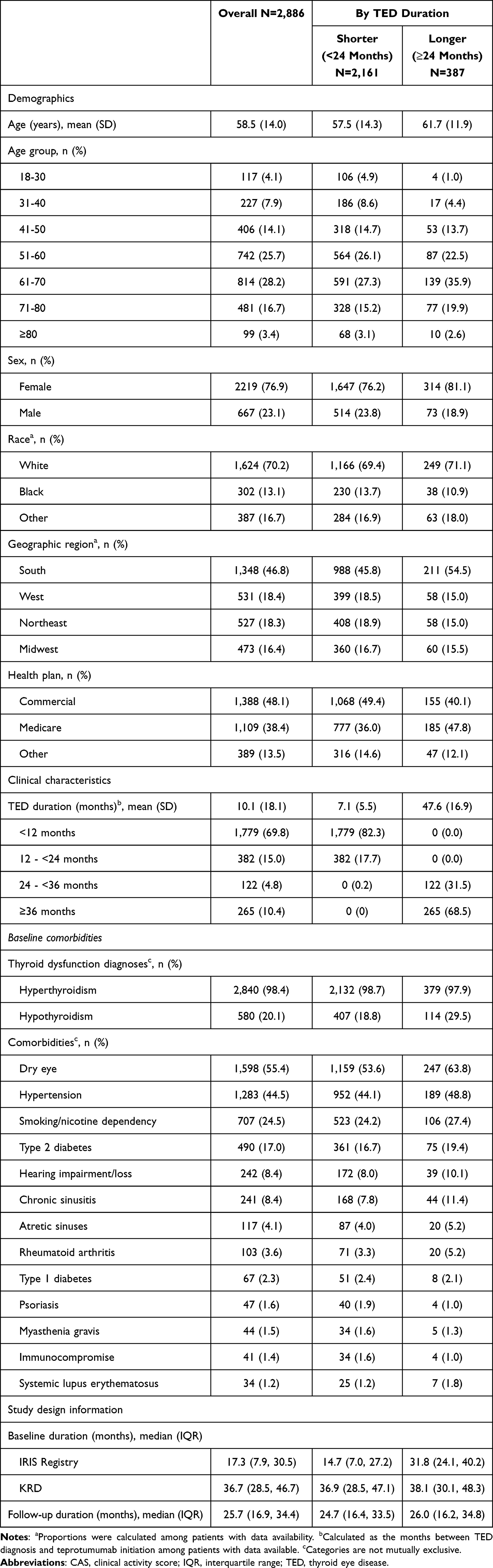 |
Table 1 Baseline Patient Demographics and Clinical Characteristics |
Clinical Burden at Baseline
Of 356 patients with available CAS measurements, 325 (91%) had active disease. Among patients with documented IOP, 16% (418/2,660) had values >21mmHg and among those with documented VA, 9% (167/1,967) had VA 20/50-20/160 and 2% (36/1,967) had VA ≤20/200, indicating impaired vision in 11% of patients overall. Of 511 patients with available proptosis measurements, 66% had proptosis >21mm.
Eye signs or symptoms (based on diagnostic codes) were present in 79% (2,291/2,886) of patients; the most common were proptosis (45%; 1,300/2,886), lid retraction (29%; 843/2,886), diplopia (29%; 841/2,886), strabismus (19%; 552/2,886), and keratoconjunctivitis (18%; 531/2,886).
Patients also demonstrated a high comorbidity burden, including dry eye (55%; 1,598/2,886), hypertension (45%; 1,283/2,886), smoking or nicotine dependence (25%; 707/2,886), and type 2 diabetes (17%; 490/2,886). Hearing impairment was documented in 8% (242/2,886) prior to teprotumumab initiation.
Overall, 5% (143/2,886) of patients had history of eye-related surgery, and the majority (89%; 2,581/2,886) did not receive high-dose corticosteroids, immunotherapy, surgery and/or ORT prior to teprotumumab (Table 2).
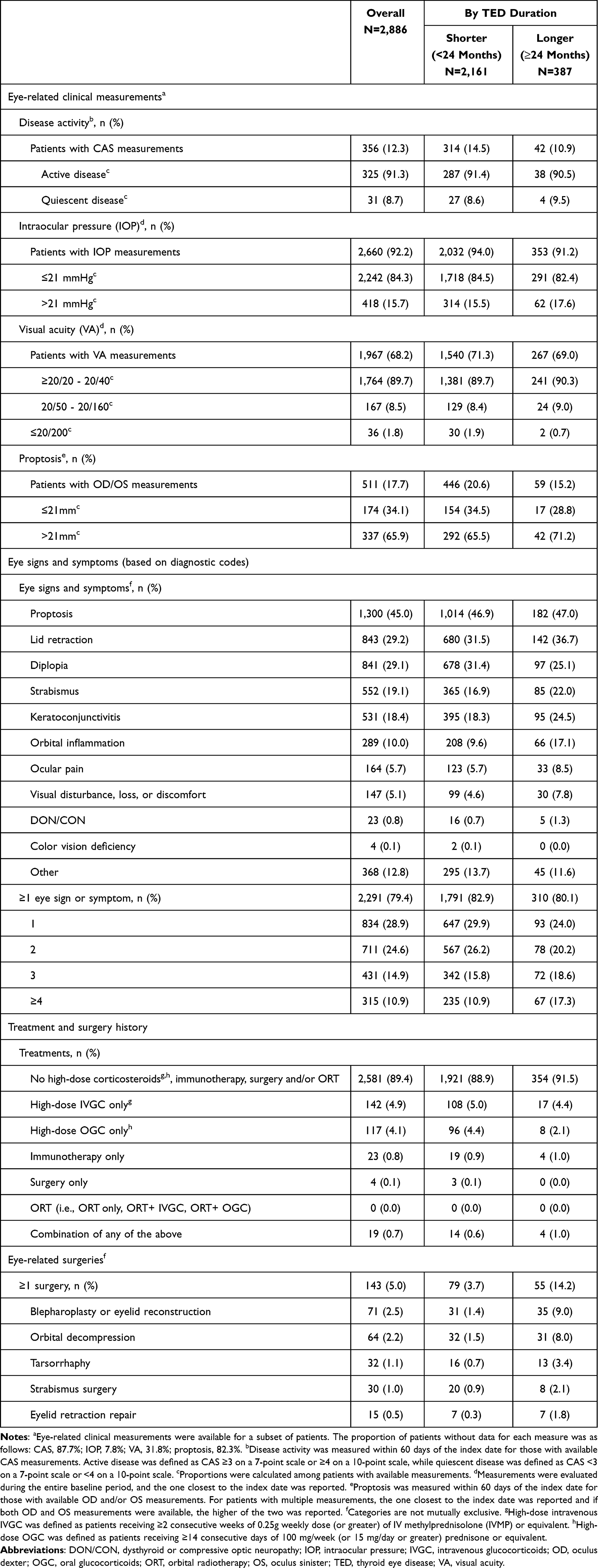 |
Table 2 Baseline Clinical Burden |
Teprotumumab Infusion Patterns
Among 2,637 patients who initiated teprotumumab, 65% (1,712/2,637) completed the full first course of treatment (8 infusions); 63% (1,654/2,637) completed without treatment gaps, while 2% (58/2,637) completed with a treatment gap.
Among patients who completed the full first course without treatment gaps, the median time to completion was 5 months (IQR: 5, 5). For those who completed the first course with treatment gaps, the median time to completion was 13 months (IQR: 10, 19).
Among patients who completed the full first course regardless of treatment gaps, 10% (174/1,712) were retreated with teprotumumab, with a median time from first course completion to retreatment of 9 months (IQR: 1, 15); of these, 26% (46/174) completed the full second course.
The remaining patients who initiated teprotumumab (35%; 925/2,637) discontinued before completing the full course, with a median time to discontinuation of 3 months (IQR: 1, 4) and a mean (SD) of 4 (2) total infusions. Among those who discontinued teprotumumab, 5% (46/925) reinitiated treatment after a treatment gap (Figure 1). Among the 925 patients who discontinued teprotumumab during the first course, discontinuation was observed at all infusion points, most frequently at the seventh (21%) or sixth (16%) infusions (Figure 2).
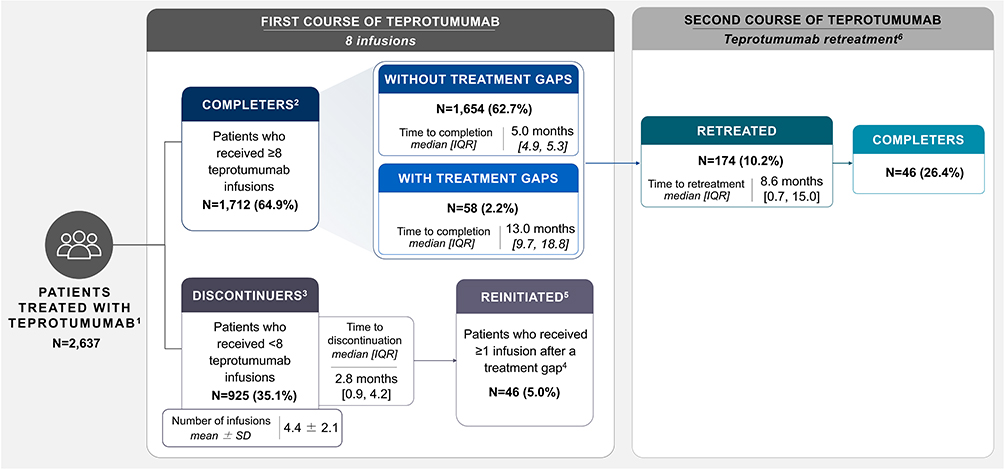 |
Figure 1 Teprotumumab infusion patterns. Abbreviations: IQR, interquartile range; SD, standard deviation. Note: 1Infusion patterns were reported based on all teprotumumab claims (which were required to be ≥10 days apart to be considered separate claims) observed between the index date and the end of follow-up. Patients who were potentially impacted by the COVID-19 supply chain disruption (ie, patients who initiated teprotumumab in the second half of 2020 and discontinued in the first half of 2021; n=249) were excluded from the infusion pattern analyses. 2First course completers were defined as patients who received ≥8 teprotumumab infusions. 3Discontinuers were defined as patients who received <8 teprotumumab infusions. 4Treatment gaps were defined as a period of ≥90 days between two consecutive teprotumumab infusions. 5Among discontinuers, reinitiation was defined as receiving a subsequent infusion after a treatment gap (≥90 days), while still receiving <8 overall. 6Among completers, retreatment was defined as receiving at least one subsequent infusion after completion of a course (ie, ≥9 infusions), with second course completers defined as patients who received ≥16 teprotumumab infusions. Patients who did not complete a second course were either censored due to insufficient follow-up or discontinued retreatment prior to completing 16 infusions. |
 |
Figure 2 Discontinuation timing within the first course of teprotumumab. |
Subgroup Analysis by TED Duration
Baseline demographic and clinical characteristics by TED duration are summarized in Table 1. Profiles were generally comparable across subgroups, although descriptively, patients with longer TED duration were slightly older (mean age: 62 vs 58), more frequently female (81% vs 76%), more often covered by Medicare (48% vs 36%), and had a greater prevalence of comorbidities (eg, dry eye: 64% vs 54%; hypertension: 49% vs 44%). Baseline clinical burden, shown in Table 2, was likewise generally similar, though patients with longer TED duration exhibited descriptively higher burden (eg, 36% with ≥3 eye signs or symptoms vs 27%).
Among 1,978 patients with shorter TED duration (<24 months) who initiated teprotumumab, 65% (1,287/1,978) completed the full first course (8 infusions); 63% (1,245/1,978) without a treatment gap (median time to completion: 5 months, IQR: 5, 5) and 2% (42/1,978) with a gap (median time to completion: 12 months, IQR: 10, 19). Among those who completed the full first course, with or without treatment gaps, retreatment occurred in 10% of patients (127/1,287; median time to retreatment: 9 months, IQR: 1, 15), with 27% (34/127) completing the full second course.
A total of 691 patients (35%) with shorter TED duration discontinued treatment (median time to discontinuation: 3 months, IQR: 1, 4; mean [SD] number of infusions: 4 [2]). Reinitiation after a treatment gap occurred in 5% of patients (33/691) (Supplemental Figure 3).
In the subgroup of 351 patients with longer TED duration (≥24 months), 63% (220/351) completed the first full course of teprotumumab, including 61% (213/351) without a treatment gap (median time to completion: 5 months, IQR: 5, 5) and 2% (7/351) with a gap (median time to completion: 12 months, IQR: 9, 18). Among those who completed the full first course regardless of treatment gaps, retreatment with teprotumumab occurred in 10% of patients (22/220; median time to retreatment: 1 month, IQR: 1, 19), of whom 18% (4/22) completed the second course.
A total of 131 patients (37%) discontinued, with a median time to discontinuation of 3 months (IQR: 1, 4) and a mean (SD) of 4 (2) infusions. Teprotumumab reinitiation after a treatment gap occurred in 5% of patients (7/131; Supplemental Figure 3).
Discussion
This large-scale, population-based study provides one of the most comprehensive real-world assessments of teprotumumab use in TED to date, capturing demographic and clinical characteristics and infusion patterns among nearly 2,900 patients in routine clinical settings. Unlike prior small, single-center studies focused on specific outcomes such as diplopia recurrence or surgical interventions,14–17 this analysis leverages linked ophthalmology IRIS Registry and US claims data to comprehensively characterize patients and their teprotumumab treatment course.
At the time of teprotumumab initiation, patients exhibited substantial disease burden, irrespective of TED duration. Compared with clinical trials where proptosis is often the primary efficacy endpoint, patients in this real-world setting presented with a broad spectrum of symptoms. Most patients had at least one sign or symptom at baseline, highlighting the heterogeneity of TED manifestations and the broader applicability of teprotumumab beyond those with proptosis.
Both shorter- and longer-duration subgroups demonstrated substantial baseline disease burden. Patients with longer TED duration showed greater overall burden, consistent with cumulative effects of longstanding disease. Approximately two-thirds of patients presented with proptosis >21 mm, and among those with available CAS data, the majority had active disease. These findings underscore persistent unmet clinical needs across the disease course. In addition, the high observed rates of active disease and proptosis at treatment initiation were comparable to those reported in pivotal trials, reinforcing the relevance of these findings.11,12
Baseline comorbidity burden was also notable Dry eye and type 2 diabetes were especially common, both of which are clinically relevant in TED management, alongside hypertension and smoking or nicotine dependence. Importantly, pre-existing hearing impairment was documented in 8% of patients prior to initiating teprotumumab, consistent with prior evidence of increased hearing loss risk in TED compared with both GD and the general US population (adjusted hazard ratio [TED vs. GP]: 1.6, p<0.01).25 Although the pathophysiology is not well understood, autoimmune and inflammatory mechanisms implicated in TED, including immune-mediated inflammation and vascular changes affecting the cochlea, may contribute to auditory dysfunction,26,27 suggesting TED itself may be an independent risk factor for hearing impairment.25 These findings highlight the importance of routine hearing assessment and monitoring in patients with TED.
Most patients initiated teprotumumab within 12 months of diagnosis, with limited use of prior TED-related interventions. The early use in this cohort likely reflects teprotumumab’s initial FDA approval in 2020, for patients with active, moderate-to-severe disease, as well as growing clinical confidence in IGF-1R-targeted biologics and the later label expansion in 2023 to all patients regardless of disease activity or duration.
These patterns reflect a shift in the treatment paradigm, with corticosteroid-based approaches increasingly replaced by targeted therapy.7,10 Post-approval, a multicenter study found that teprotumumab was used as first-line therapy in 60% of patients with active, moderate-to-severe TED.28 However, access varies across the US, as some insurers require corticosteroid step therapy, potentially limiting first-line use and warranting further large-scale assessment.
Recent evidence has highlighted the benefits of early initiation; a meta-analysis demonstrated greater efficacy when teprotumumab was started within the first 6 months of diagnosis (the “critical window”) compared with later initiation, underscoring the value of early intervention.29 However, an orbital MRI study in patients with TED showed improvements in proptosis with teprotumumab, regardless of disease duration or CAS.30 Together, these data support the role of teprotumumab across the disease continuum, with particular benefit from early initiation.
Adherence was notable: nearly two-thirds of patients completed the full 8-infusion course of teprotumumab, with a median time to completion of 5 months, closely aligned with the recommended dosing schedule. Only a minority experienced treatment gaps ≥90 days, likely reflecting flexible dosing strategies, patient-specific factors, or logistical barriers such as travel, scheduling difficulties, or insurance delays. Among course completers, few underwent retreatment, with a median time to retreatment of 8 months. This pattern is consistent with the relapsing nature of TED, in which disease activity may flare over time and necessitate additional therapy.7
Nevertheless, discontinuation of the initial 8-infusion course of teprotumumab occurred in approximately one-third of patients, with rates peaking near the seventh infusion. This pattern suggests potential heterogeneity in treatment duration in real-world practice, which may reflect differences in patient characteristics, treatment response, or access-related factors. Discontinuation was more frequent in this study than in clinical trials, potentially reflecting real-world challenges such as comorbidities, tolerability, payer decisions, interruptions in continued access, differences in perceived treatment benefit, or clinician- and patient-driven treatment decisions. Although the dataset does not capture specific reasons, discontinuation later in the course may also represent patients achieving an adequate therapeutic response and no longer requiring further treatment. Conversely, tolerability issues or logistical barriers could also be contributing factors. Further research is warranted to evaluate patient- and system-level factors associated with discontinuation, including baseline disease characteristics and access-related factors.
Reinitiation was uncommon, with only 5% of discontinuers restarting treatment after a gap, suggesting that most patients did not resume therapy once interrupted. The clustering of discontinuation near the seventh infusion highlights the need for further investigation into the drivers of treatment interruption, including both clinical and nonclinical factors. The low rates of reinitiation among discontinuers, together with the relatively infrequent retreatment observed among course completers, support the possibility of treatment durability in some patients, though adverse events remain a possibility.
While clinical outcomes following discontinuation were not assessed in this study, prior evidence indicates that even partial treatment courses may yield meaningful benefits. In a multicenter cohort of 74 patients with active or minimally active TED who experienced COVID-related treatment interruptions, teprotumumab was still associated with significant improvements in proptosis, CAS, and motility restriction, which were maintained throughout the interruption period.24
Real-world access issues remain a concern. In a recent study, approximately one-quarter of patients recommended for teprotumumab did not initiate treatment, primarily owing to insurance denial (36%) or patient refusal (64%) over side effect concerns.28 These findings underscore the need for patient education and comprehensive healthcare system support to ensure adherence and optimize outcomes.
This analysis has limitations common to retrospective claims-based studies, including potential coding errors, missing data, and variability in clinical documentation. CAS and proptosis clinical measurements were available for only a small subset of patients, reflecting limited capture of certain clinical measures in the IRIS Registry; therefore, estimates of disease activity and measurement-based proptosis are based on a subset of patients and may not be fully representative of the overall cohort. Because teprotumumab is administered on a 21-day schedule, some infusions may not have been captured due to the continuous enrollment criterion, which allowed gaps of <45 days. Although using linked IRIS Registry and KRD claims data provides a more comprehensive dataset than either source alone, underreporting of clinical characteristics and treatments remains likely. In addition, the TED diagnosis date was determined by the first documented mention of relevant terms in clinical notes, which may not reflect true disease onset, particularly for diagnoses before 2019. For the infusion pattern analyses, which focused exclusively on teprotumumab, the potential influence of other interim interventions (eg, TED-related treatments or surgeries) is unknown, and limited follow-up may have reduced the ability to fully capture retreatment events Further studies with longer follow-up and more complete and systematically captured clinical data, including standardized clinical outcome measurements, are needed to better characterize disease activity, treatment patterns, retreatment needs, and real-world dosing practices in representative patient populations.
Key strengths of this study include its large sample size, national representativeness, and the use of integrated real-world data sources to evaluate infusion patterns. The study design captured a diverse patient population across a wide spectrum of disease severity, care settings, and insurance types. Importantly, the analysis captured real-world adherence and teprotumumab treatment patterns using infusion-level data, including timing, gaps, and retreatment, which are rarely available metrics in traditional EHR studies. The stratification by disease duration and linkage of claims with structured clinical data allowed for a more comprehensive characterization of patient profiles and treatment journeys than prior single-source datasets.
Conclusion
This large, real-world analysis using IRIS Registry data linked with KRD claims data provides insight into teprotumumab use in routine clinical practice, highlighting its early adoption and alignment with treatment guidelines across patients with both recent-onset and longstanding TED. Patients initiating teprotumumab exhibited substantial overall disease burden, not only in terms of TED-related signs and symptoms, but also comorbidities and broader clinical complexity, underscoring the multifaceted impact of TED on patient health.
The findings suggest a shift in practice toward earlier use of targeted therapy and point to the importance of addressing treatment adherence and discontinuation in real-world settings. As the first and only approved targeted therapy for TED, teprotumumab represents an important therapeutic advancement that may influence the natural disease course. Ongoing research will be critical to understanding its long-term role in shaping TED outcomes.
Abbreviations
1L, first-line; AAO, American Academy of Ophthalmology; CAS, clinical activity score; CFR, Code of Federal Regulations; COVID-19, coronavirus disease 2019; EHR, electronic health record; ETA, European Thyroid Association; EUGOGO, European Group on Graves’ Orbitopathy; FDA, Food and Drug Administration; GD, Graves’ disease; GP, general population; IGF-1R, insulin-like growth factor-1 receptor; IOP, intraocular pressure; IRB, Institutional Review Board; IRIS, Intelligent Research in Sight; IQR, interquartile range; KRD, Komodo Health Research Dataset; LTS, Long-term Support; MRI, magnetic resonance imaging; NCT, National Clinical Trial; OD, oculus dexter; ORT, orbital radiotherapy; OS, oculus sinister; SD, standard deviation; TED, thyroid eye disease; TSHR, thyrotropin receptor; US, United States; VA, visual acuity; WCG, Western Copernicus Group.
Data Sharing Statement
The data that support the findings of this study were used under license for this study from Verana Health and Komodo Research Dataset. Restrictions apply to the availability of these data. Due to the sensitivity and privacy around the IRIS Registry, raw data must remain confidential and cannot be shared. Aggregated data are available upon reasonable request. Requests should be directed to Ann Xi ([email protected]).
Ethics Statement
The IRIS Registry and KRD are centralized, de-identified data repositories that can be used for research purposes. In accordance with the US Department of Health and Human Services regulations (45 CFR 46), this study did not involve human subjects, as all data were de-identified and investigators had no access to patient identifiers. Therefore, institutional board review and informed consent are not required. This study adheres to the principles of the Declaration of Helsinki.
Acknowledgments
Medical writing and editorial assistance was provided by Lorena Tonarelli, MSc, of LT Medical & Value Communications Ltd, and funded by Amgen Inc., USA.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by Research to Prevent Blindness Unrestricted Grant to the Department of Ophthalmology Vanderbilt University Medical Center and Amgen Inc., USA. The sponsor, Amgen, participated in the design of the study, conducting the study, interpretation of the data, and review or approval of the manuscript.
Disclosure
Louise A. Mawn: Amgen (consultant, research), Genentech (consultant), Genentech (clinical research). Erin M. Shriver: Amgen (consultant), Genentech (consultant), Immunovant (clinical research). Madhura Tamhankar: Amgen (consulting, honoraria, advisory board), Viridian (advisory board), Genentech (advisory board), Argenx (consulting, advisory board). Yao Yuan: Amgen (contractor). Ann Xi: Amgen (employment and stock ownership). Juan Ayala-Haedo: Amgen (employment and stock ownership). Haridarshan Patel: Amgen (employment and stock ownership). The authors report no other conflicts of interest in this work.
References
1. Nie T, Lamb YN. Teprotumumab: a review in thyroid eye disease. Drugs. 2022;82(17):1663–14. doi:10.1007/s40265-022-01804-1
2. Park K, Li J, Wen J, et al. Extraocular muscle enlargement in thyroid eye disease using volumetric analysis. Cureus. 2024;16(7):e63843. doi:10.7759/cureus.63843
3. Gupta V, Hammond CL, Roztocil E, Gonzalez MO, Feldon SE, Woeller CF. Thinking inside the box: current insights into targeting orbital tissue remodeling and inflammation in thyroid eye disease. Surv Ophthalmol. 2022;67(3):858–874. doi:10.1016/j.survophthal.2021.08.010
4. Verity DH, Rose GE. Acute thyroid eye disease (TED): principles of medical and surgical management. Eye. 2013;27(3):308–319. doi:10.1038/eye.2012.284
5. Gillespie EF, Smith TJ, Douglas RS. Thyroid eye disease: towards an evidence base for treatment in the 21st century. Curr Neurol Neurosci Rep. 2012;12(3):318–324. doi:10.1007/s11910-012-0256-9
6. Dosiou C, Kossler AL. Thyroid eye disease: navigating the new treatment landscape. J Endocr Soc. 2021;5(5):bvab034. doi:10.1210/jendso/bvab034
7. Bartalena L, Kahaly GJ, Baldeschi L, et al. The 2021 European Group on Graves’ orbitopathy (EUGOGO) clinical practice guidelines for the medical management of Graves’ orbitopathy. Eur J Endocrinol. 2021;185(4):G43–G67. doi:10.1530/EJE-21-0479
8. Couch SM. Teprotumumab (Tepezza) for thyroid eye disease. Mo Med. 2022;119(1):36.
9. Moledina M, Damato EM, Lee V. The changing landscape of thyroid eye disease: current clinical advances and future outlook. Eye (Lond). 2024;38(8):1425–1437. doi:10.1038/s41433-024-02967-9
10. Burch HB, Perros P, Bednarczuk T, et al. Management of thyroid eye disease: a consensus statement by the American Thyroid Association and the European Thyroid Association. Eur Thyroid J. 2022;11(6). doi:10.1530/ETJ-22-0189.
11. Douglas RS, Kahaly GJ, Patel A, et al. Teprotumumab for the treatment of active thyroid eye disease. N Engl J Med. 2020;382(4):341–352. doi:10.1056/NEJMoa1910434
12. Smith TJ, Kahaly GJ, Ezra DG, et al. Teprotumumab for thyroid-associated ophthalmopathy. N Engl J Med. 2017;376(18):1748–1761. doi:10.1056/NEJMoa1614949
13. Douglas RS, Couch S, Wester ST, et al. Efficacy and safety of teprotumumab in patients with thyroid eye disease of long duration and low disease activity. J Clin Endocrinol Metab. 2023;109(1):25–35. doi:10.1210/clinem/dgad637
14. Davis JB, Mudalegundi S, Henderson AD, Carey AR. Stability of ocular alignment after teprotumumab therapy in a cohort of patients with thyroid eye disease and baseline diplopia. J Neuro Ophthalmol. 2024;44(4):527–532. doi:10.1097/WNO.0000000000002066
15. Chen Y, Linaburg T, Wang S, et al. Observational characterization of the retreatment course of patients with thyroid eye disease. J Neuro Ophthal. 2025;10:1097.
16. Ting MA, Topilow NJ, Ediriwickrema LS, et al. A comparison of proptosis reduction with teprotumumab versus surgical decompression based on fat-to-muscle ratio in thyroid eye disease. Orbit. 2024;43(2):222–230. doi:10.1080/01676830.2023.2282509
17. Mudalegundi S, Huang P, Henderson AD, Carey AR. Objective diplopia outcomes for patients treated with teprotumumab for thyroid eye disease. J Neuro Ophthalmol. 2024;44(1):80–86. doi:10.1097/WNO.0000000000002001
18. Ramesh S, Zhang QE, Sharpe J, et al. Thyroid eye disease and its vision-threatening manifestations in the academy IRIS registry: 2014-2018. Am J Ophthalmol. 2023;253:74–85. doi:10.1016/j.ajo.2023.04.013
19. Oke I, Reshef ER, Elze T, et al. Smoking is associated with a higher risk of surgical intervention for thyroid eye disease in the IRIS registry. Am J Ophthalmol. 2023;249:174–182. doi:10.1016/j.ajo.2023.01.020
20. AAO. Data from: IRIS® (Intelligent Research in Sight) Registry. American Academy of Ophthalmology. 2025.
21. Komodo Health Inc. Explore the healthcare map: the most complete View of the patient journey. 2025, Available from: https://www.komodohealth.com/solutions/healthcare-map/.
22. Torres A, Lien A, Shekhar Sahoo H, Moss H. Using natural language processing to identify and characterize patients with TED in the IRIS registry. American Academy of Ophthalmology. 2025;2025.
23. Mourits MP, Koornneef L, Wiersinga WM, Prummel MF, Berghout A, van der Gaag R. Clinical criteria for the assessment of disease activity in Graves’ ophthalmopathy: a novel approach. Br J Ophthalmol. 1989;73(8):639–644. doi:10.1136/bjo.73.8.639
24. Ho TC, Maamari RN, Kossler AL, et al. Outcomes of patients with thyroid eye disease partially treated with teprotumumab. Ophthalmic Plast Reconstr Surg. 2023;39(2):150–155. doi:10.1097/IOP.0000000000002267
25. Brant JA, Manchaiah V, Ma J, Chauchan D, Franco P, Patel H. Epidemiology and risk factors of hearing loss in thyroid eye disease in the United States. Manuscript submitted for publication.
26. Berker D, Karabulut H, Isik S, et al. Evaluation of hearing loss in patients with Graves’ disease. Endocrine. 2012;41(1):116–121. doi:10.1007/s12020-011-9515-9
27. Tsai YT, Chang IJ, Hsu CM, et al. Association between sudden sensorineural hearing loss and preexisting thyroid diseases: a nationwide case-control study in Taiwan. Int J Environ Res Public Health. 2020;17(3):834. doi:10.3390/ijerph17030834
28. Rachmasari KN, Toro-Tobon D, Wagner LH, Tooley AA, Bradley EA, Stan MN. Impact of teprotumumab on clinical practice in thyroid eye disease. Endocr Pract. 2024;30(10):937–942. doi:10.1016/j.eprac.2024.06.010
29. Alves Junior JM, Bernardo W, Villagelin D. Effectiveness of different treatment modalities in initial and chronic phases of thyroid eye disease: a systematic review with meta-analysis. J Clin Endocrinol Metab. 2024;109(11):2997–3009. doi:10.1210/clinem/dgae526
30. Ugradar S, Parunakian E, Zimmerman E, et al. Clinical and radiologic predictors of response to teprotumumab: a 3D volumetric analysis of 35 patients. Ophthalmic Plast Reconstr Surg. 2025;41(4):408–414. doi:10.1097/IOP.0000000000002867
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Clinical Burden and Costs of Anti-Neutrophil Cytoplasmic Antibody-ANCA-Associated Vasculitis: Main Findings from REDCap Registry of a University Hospital in Spain
Draibe J, Martinez Valenzuela L, Gomez-Preciado F, Anton-Pampols P, Rau AM, Díaz-Cuervo H, Crespo C, Cuervo J, Ramirez de Arellano A
ClinicoEconomics and Outcomes Research 2025, 17:537-546
Published Date: 1 August 2025