Back to Journals » Patient Related Outcome Measures » Volume 13
Patients’ Experiences with Management of Benign Paroxysmal Positional Vertigo: Insights from the Vestibular Disorders Association Registry
Authors Grove CR ![]() , Souza WH, Gerend PL, Ryan CA, Schubert MC
, Souza WH, Gerend PL, Ryan CA, Schubert MC ![]()
Received 22 April 2022
Accepted for publication 24 June 2022
Published 6 July 2022 Volume 2022:13 Pages 157—168
DOI https://doi.org/10.2147/PROM.S370287
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Robert Howland
Colin R Grove,1 Wagner Henrique Souza,2 Patricia L Gerend,3 Cynthia A Ryan,3 Michael C Schubert1,4
1Department of Otolaryngology - Head and Neck Surgery, Laboratory for Vestibular NeuroAdaptation, Johns Hopkins University, Baltimore, MD, 21205, USA; 2KITE, Toronto Rehabilitation Institute – University Health Network, Toronto, ON M5G 2A2, Canada; 3Vestibular Disorders Association (VeDA), Portland, OR, 97211, USA; 4Department of Physical Medicine and Rehabilitation, Johns Hopkins University, Baltimore, MD, 21205, USA
Correspondence: Michael C Schubert, Department of Otolaryngology - Head and Neck Surgery, Johns Hopkins University, 601 N. Caroline Street, 6th Floor, Baltimore, MD, 21205, USA, Tel +1 410 955 7381, Email [email protected]
Introduction: Benign paroxysmal positional vertigo (BPPV) is the most frequently occurring peripheral vestibular disorder. Clinical practice guidelines (CPG) for BPPV exist; however, little is known about how affected patients perceive their condition is being managed. We aimed to leverage registry data to evaluate how adults who report BPPV are managed.
Material and Methods: We retrospectively analyzed of data from 1,262 adults (58.4 ± 12.6 years old, 81.1% female, 91.1% White) who were enrolled in the Vestibular Disorders Association Registry from 2014 to 2020. The following patient-reported outcomes were analyzed by proportions for those who did and did not report BPPV: symptoms experienced, falls reported, diagnostics undertaken, interventions received (eg, canalith repositioning maneuvers [CRMs], medications), and responses to interventions.
Results: Of the 1,262 adults included, 26% reported being diagnosed with BPPV. Many adults who reported BPPV (83%) also endorsed receiving additional vestibular diagnoses or may have had atypical BPPV. Those with BPPV underwent magnetic resonance imaging and were prescribed medications more frequently than those without BPPV (76% vs 57% [χ2=36.51, p< 0.001] and 85% vs 78% [χ2=5.60, p=0.018], respectively). Falls were experienced by similar proportions of adults with and without BPPV (55% vs 56% [χ2==11.26, p=0.59]). Adults with BPPV received CRMs more often than those without BPPV (86% vs 48%, χ2=127.23, p< 0.001). More registrants with BPPV also endorsed benefit from CRMs compared to those without BPPV (51% vs 12% [χ2=105.30, p< 0.001]).
Discussion: In this registry, BPPV was often reported with other vestibular disorders. Healthcare utilization was higher than would be expected with care based on the CPG. The rates of falls in those with and without BPPV are higher than previously reported. Adults with BPPV reported significant differences in how their care is managed and their overall outcomes compared to those without BPPV.
Conclusion: Patient-reported outcomes provide useful information regarding the lived experience of adults with BPPV.
Keywords: benign paroxysmal positional vertigo, vestibular disorders, falls, canalith repositioning maneuvers
Plain Language Abstract
This study investigated patient experiences in care received for their diagnosis of benign paroxysmal positional vertigo, which is the most frequent type of inner ear disorder. Although clinical practice guidelines exist that include specific directives for successful management of positional vertigo, results reveal these patients report both higher healthcare utilization and medication prescription, suggesting the guidelines have not been universally adopted.
Introduction
Benign paroxysmal positional vertigo (BPPV) is the most frequently occurring peripheral vestibular disorder in the general population.1 The incidence of BPPV is between 10.7 and 64.0 cases per 100,000 adults per year,2,3 and its lifetime prevalence is 3.2% in women, 1.6% in men, and 2.4% overall.1 The pathophysiology underlying BPPV involves otoconial debris that are either free-floating in one of the semicircular canals (canalithiasis)4 or adherent to a cupula (cupulolithiasis).5 Typical BPPV is characterized as involving the sudden onset of brief episodes of dizziness or vertigo that are provoked by changes in the position of the head relative to gravity, most frequently rolling over in bed, bending over, and looking upward, such as is common in persons with BPPV of the posterior semicircular canal.6
Several peripheral and central vestibular disorders either predispose adults to developing secondary BPPV7 or co-occur in not-insignificant proportions of specific populations. Reports indicate that 5.5%8 to 10%9 of adults with Ménière’s disease, 9.8% of those with a history of vestibular neuritis,10 and approximately 12% of persons with sudden sensorineural hearing loss develop BPPV.11,12 Additionally, BPPV has been reported in 8.5%13 and 21.4%14 of those who are status-post stapedotomy and cochlear implantation, respectively. Head trauma has been reported as the etiology for 9.4% of adults with BPPV.15 Also, those with BPPV of an unknown cause have been reported to be three times more likely to have migraine than those with BPPV secondary to a likely cause, eg, head trauma or surgery.16 In these cases, BPPV may have an atypical presentation.
Recommendations for the management of persons with BPPV are outlined in a recently updated clinical practice guideline (CPG).17 Diagnosis of BPPV by a healthcare provider requires the use of diagnostic positional maneuvers, eg, the Dix-Hallpike test (anterior or posterior canal BPPV) or supine roll test (lateral canal BPPV).17,18 Emerging evidence may support the inclusion of video head impulse testing for atypical presentations of BPPV.19,20 Though the natural course of BPPV is characterized by spontaneous remission for some,21 many patients benefit from canalith repositioning maneuvers (CRMs),22 Per the BPPV CPG, the use of CRMs is strongly recommended, and, although the provisional use of vestibular suppressants is acceptable in persons with BPPV, the routine use of these medications is discouraged.17 Additionally, providers may offer observation with follow-up as an initial management strategy or refer patients for vestibular rehabilitation.17,18
Gathering self-report data from persons with dizziness is essential to enhance the diagnostic process and assist clinical decision-making. The use of registries to obtain data from and about patients is increasing, and the value of these powerful tools to answer larger questions has been recognized by governments.23 Registries that focus on persons with vestibular dysfunction include the Registry to Evaluate the Burden of Disease in Vertigo (REVERT)24 and DizzyReg.25 These data sources have been utilized to examine the impact of vertigo on vocational performance and healthcare utilization,26 to develop classification systems for vertiginous patients,27 and to describe the demographic and clinical features of specific vestibular disorders.28
The purpose of this study was to leverage registry data to examine patients’ perceptions regarding: 1) how the management of adults who report being diagnosed with BPPV compares with the BPPV CPG, 2) whether those who report being diagnosed with BPPV are managed differently than those who report being diagnosed with other causes of vertigo or dizziness, and 3) whether the outcomes of common interventions differ between those who do and do not report being diagnosed with BPPV. We hypothesized that compared to those who report being diagnosed with other causes of vertigo or dizziness, adults who report being diagnosed with BPPV would endorse symptoms characteristic of BPPV more frequently, report falls less frequently, undergo advanced diagnostic testing less often, be offered CRMs more frequently, and achieve superior outcomes with CRMs.
Materials and Methods
We retrospectively analyzed data from 1,262 adults who reported receiving a vestibular diagnosis and who participated in a patient registry commissioned by the Vestibular Disorders Association (VeDA) from March 2014 to November 2020. Participants were included if they reported a vestibular diagnosis as the reason for registration. The registry was accessible through VeDA’s website,29 its list-serve, and its Facebook® page; it was also discoverable through internet search engines and was listed on fliers distributed by healthcare providers. The purpose of the registry and how the information would be used was disclosed on its internet landing page.30
Potential participants were advised regarding who would have access to their information, how their privacy would be protected, and whom to contact with questions. Participants, then, created an account with the Patient Insights Network® (PIN) developed by INVITAE™, an interactive, online, HIPAA-compliant, secure platform designed for surveying disease communities, uploading medical records, monitoring healthcare outcomes, and sharing de-identified data. All registrants provided basic health and demographic information. Informed consent was electronically obtained prior to the commencement of this study from all participants and included sharing their email address with non-profit advocacy organizations that support the PIN, sharing de-identified data with public databases, sharing de-identified data with researchers, as well as for completing questionnaires. The Advarra Institutional Review Board approved this protocol (Pro00015852).
Completion of the questionnaires was voluntary and partially completed questionnaires were accepted. The Dizziness Questionnaire consisted of 18 questions pertaining to symptoms, eg, history of dizziness, assessment of dizziness, and outcomes of the work-up. Questions related to specific diagnoses were structured to determine whether the participant’s vestibular dysfunction was self- or provider-diagnosed. The Diagnosis Questionnaire consisted of 13 questions pertaining to the work-up for dizziness, eg, healthcare provider involved in the diagnosis and testing that led to the diagnosis. The Medical Care Questionnaire was comprised of 13 questions relating to the healthcare received, eg, whether specific interventions were undertaken and the participant’s perceived response to these interventions.
The sample was divided into two groups, those who did (n=328) and did not (n=934) report being diagnosed with BPPV by a healthcare provider. In a critical review of the frequency of various causes of dizziness, Kroenke et al found that BPPV was diagnosed in 16% (range: 4% to 44%) of patients seeking care for vertigo or dizziness.31 Given that the proportion of participants in this study falls within this range, going forward we refer to participants as either being “with” or “without” BPPV. The diagnoses, other than BPPV, that participants reported being given were: acoustic neuroma (vestibular schwannoma) (n=19), auto-immune inner ear disease (n=25), bilateral vestibular hypofunction (n=100), central vestibulopathy (n=23), chronic subjective dizziness (persistent postural perceptual dizziness) (n=43), labyrinthitis (n=148), mal de debarquement syndrome (n=185), Ménière’s disease/endolymphatic hydrops (n=287), migraine associated vertigo (n=271), ototoxicity (n=29), perilymph fistula (n=24), superior canal dehiscence (n=23), vestibular neuritis (n=170), and not yet diagnosed (n=173). Participants could report multiple diagnoses. We excluded registrants if they resided outside the United States, were < age 18 years-old, or had missing data for a particular analysis.
Data regarding demographics, chronological factors, dizziness-related symptoms, history of falls, diagnostic testing performed, specific therapeutic interventions offered, and the response to interventions were analyzed using R for Statistical Computing (Version 4.1.0).32 Chronological data, which was initially reported as epochs of time, eg, 4 weeks, 6 months, etc., were re-coded as the corresponding number of weeks. The a priori alpha level for all analyses was 0.05. A two-tailed Student’s t-test was used to assess between-group differences in age. Wilcoxon rank sum tests were used to assess between-group differences in the time from onset of symptoms to the first healthcare visit, time from the first healthcare visit to final diagnosis, and the median numbers of diagnoses reported in addition to the primary diagnosis. Chi-squared tests were used to assess between-group differences in demographic count data. Fisher’s exact tests were used to assess between-group differences in the proportions of diagnoses count data. Point-biserial correlation was employed to assess the relationship between group assignment and the number of reported diagnoses received from a healthcare provider. Normally distributed data for age are presented as the mean (standard deviation [SD]), and skewed data for the time from symptom onset to first healthcare appointment, time from first healthcare appointment to final diagnosis, and number of diagnoses reported are represented by the median (inter-quartile range [IQR]). Proportions are given as n (%).
The authors were provided the raw data by an INVITAETM representative from the VeDA. Reporting conforms to the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) Statement33 and the REporting of studies Conducted using Observational Routinely-collected Data (RECORD).34
Results
Most demographic characteristics were similar across groups. The mean (SD) age of those with BPPV (59.9 [12.1] years old) was slightly higher than those without BPPV (57.9 [12.7] years old) (t=159.33, p=0.012) (Table 1). There was no significant between-group difference in sex (χ2=0.53, p=0.466) (Table 1). There were fewer Asian registrants with BPPV compared to those without BPPV (χ2=5.42, p=0.02), and more White registrants with BPPV comparedto those without BPPV (χ2=8.1, p=0.004 (Table 1). The ethnic composition was similar across groups (χ2=4.15, p=0.39) (Table 1). Those with and without BPPV waited a median of 1 month before seeking care (W=1298598, p=0.20) (Table 1). Also, those with BPPV and without BPPV waited a median of another 3 months to receive a final diagnosis (W=1147158, p=0.54) (Table 1).
 |
Table 1 Participant Characteristics |
Just 17% of those with BPPV reported that BPPV was the sole diagnosis given to them by a healthcare provider; thus, the majority (83%) of registrants with BPPV also endorsed receiving additional vestibular diagnoses. The median (IQR) for the number of diagnoses provided was 1 [2–4) for those with BPPV and 1 (0–2) for those without BPPV. An overall chi-squared test revealed that the distribution of the number of diagnoses received from a healthcare provider significantly differed between the groups (χ2=281.83, p<0.001. Additionally, group assignment was significantly correlated with the number of reported diagnoses (−0.45, t=−17.88, p<0.001), with a higher number of reported diagnoses being associated with inclusion in the group of those with BPPV.
Several co-morbid vestibular diagnoses were endorsed more often by those with BPPV compared to those without BPPV. A significantly greater proportion of adults with BPPV also endorsed being diagnosed with chronic subjective dizziness (p=0.001), central vestibulopathy (p=0.027), labyrinthitis (p<0.001], migraine associated vertigo (p<0.001), and vestibular neuritis (p<0.001) (Table 2).
 |
Table 2 Proportions of Adults with and without BPPV Who Reported Specific Co-Morbid Vestibular Diagnoses |
The symptom profile for those with BPPV differed from those without BPPV. A significantly greater proportion of those with BPPV endorsed that specific movements or positions triggered their dizziness (n=161/328 vs n=317/930, χ2=22.52, p<0.001) (Figure 1). Additionally, a significantly lower proportion of those with BPPV endorsed symptoms of room-spinning vertigo (n=133/328 vs n=469/934, χ2=8.71, p=0.001), head-spinning vertigo (n=160/328 vs n=567/934, χ2=13.65, p<0.001), feeling woozy while watching things move in the environment (n=161/328 vs n=535/934, χ2=6.26, p=0.012), and feeling woozy while being surrounded by people in a busy environment (n=116/328 vs n=428/934, χ2=10.41, p=0.001) (Figure 1).
 |
Figure 1 Black bar segments are the proportion adults with benign paroxysmal positional vertigo who reported the symptom. Gray bar segments are the proportion adults without benign paroxysmal positional vertigo who reported the symptom. *Indicate that p-values from chi-squared tests were < 0.05. The χ2 statistic and p-values are reported in the text. |
More than half of all participants reported falling due to dizziness in the 6 months prior to registration, and 1 to 2 out of 10 registrants reported that a fall resulted in seeking emergency care. The proportion of those with BPPV (55%) who acknowledged at least one fall due to dizziness was similar to that of those without BPPV (56%) (χ2=11.26, p=0.59) (Table 3). Additionally, the proportions of those with (15%) and without (12%) BPPV who indicated that at least one fall resulted in seeking emergency care were also similar (χ2=12.89, p=0.30) (Table 3).
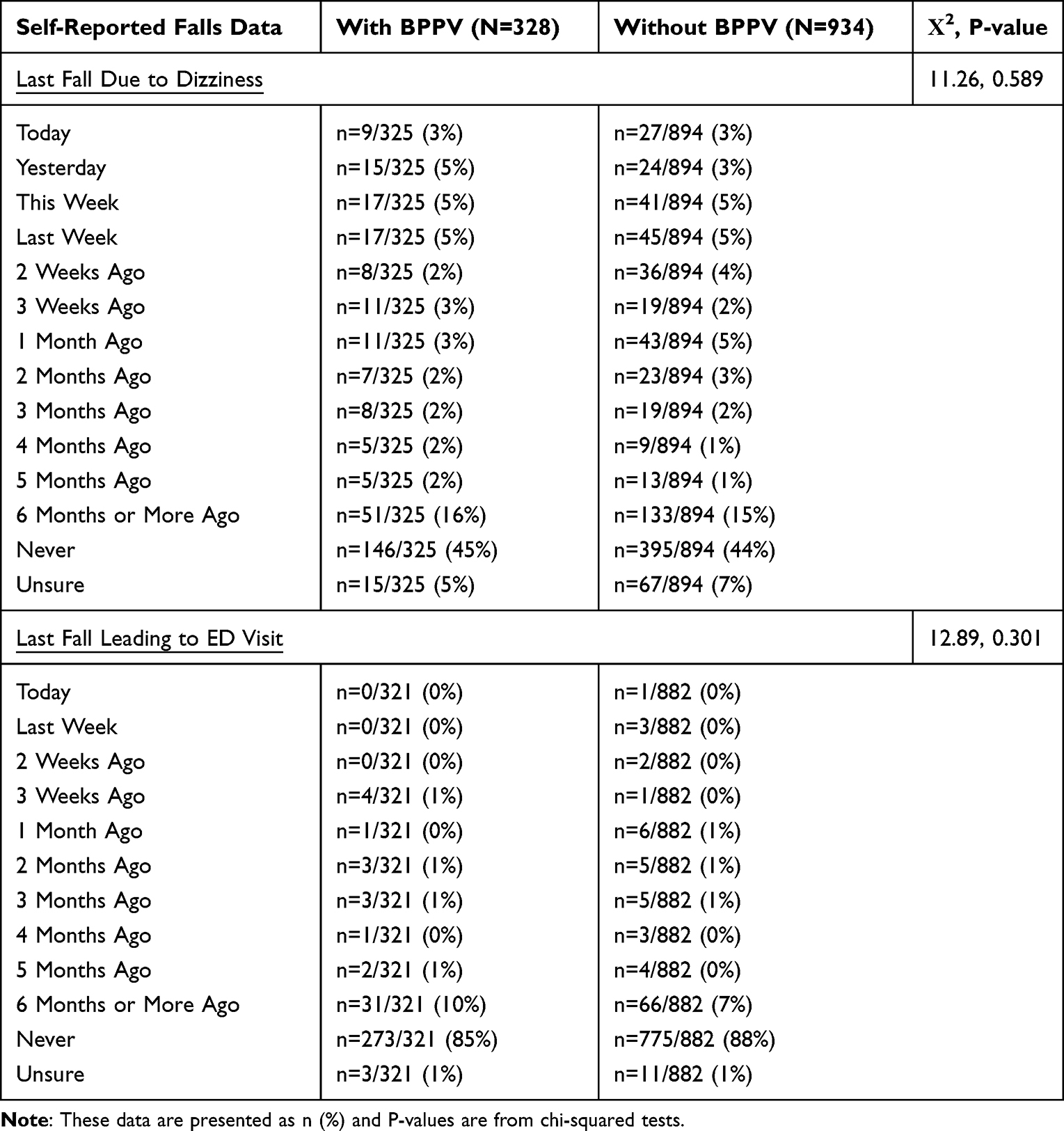 |
Table 3 Self-Reported Falls Data |
Participants with BPPV indicated having more diagnostics than those without BPPV. A significantly greater proportion of those with BPPV indicated having blood tests (n=181/328 vs n=410/934, χ2=11.97, p=0.001), an audiogram (n=272/328 vs n=608/934, χ2=35.73, p<0.001), electronystagmography (n=122/328 vs n=246/934, χ2=13.33, p<0.001), videonystagmography (n=166/328 vs n=333/934, χ2=22.09, p<0.001), computerized dynamic visual acuity testing (n=87/328 vs n=158/934, χ2=13.72, p<0.001), computerized dynamic posturography (n=62/328 vs n=127/934, χ2=4.96, p=0.03), Gans sensory organization performance testing (n=43/328 vs n=70/934, χ2=8.71, p=0.003), a computed tomography (CT) scan (n=175/328 vs n=371/934, χ2=17.83, p<0.001), and magnetic resonance imaging (MRI) (n=248/328 vs n=528/934, χ2=36.51, p<0.001) (Figure 2). The same proportion of those with (n=15/328) and without (n=45/934) BPPV indicated having no specific diagnostic work-up (χ2=0.001, p=0.98) (Figure 2).
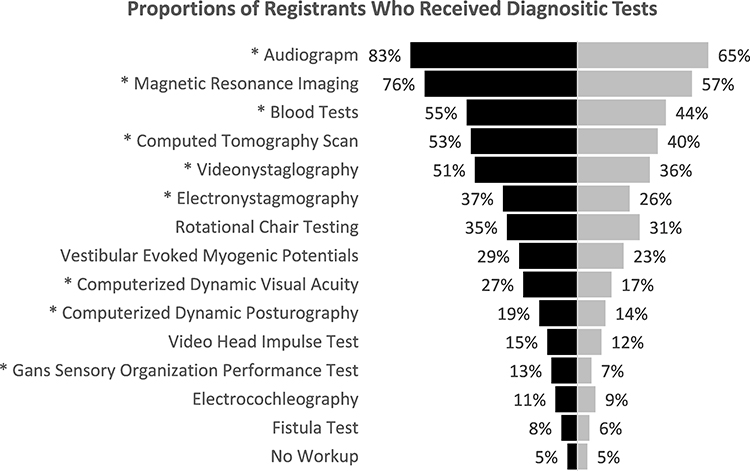 |
Figure 2 Black bar segments are the proportion adults with benign paroxysmal positional vertigo who reported receiving the test. Gray bar segments are the proportion adults without benign paroxysmal positional vertigo who reported receiving the test. *Indicate that p-values from chi-squared tests were < 0.05. The χ2 statistic and p-values are reported in the text. |
Between-group differences were found for the types of interventions offered. A significantly greater proportion of those with BPPV indicated having CRMs at least once, currently or in the past, (n=269/312 vs n=290/609, χ2=127.23, p<0.001) and being prescribed medication to relieve symptoms of dizziness (n=268/315 vs n=497/634, χ2=5.6, p=0.018) (Figure 3).
 |
Figure 3 Black bar segments are the proportion adults with benign paroxysmal positional vertigo who reported receiving the intervention. Gray bar segments are the proportion adults without benign paroxysmal positional vertigo who reported the intervention. *Indicate that p-values from chi-squared tests were < 0.05. The χ2 statistic and p-values are reported in the text. |
Finally, between-group differences were found related to responses to interventions. Overall chi-squared tests revealed that, compared to adults without BPPV, those with BPPV responded more favorably to CRMs (χ2=105.3, p<0.001), the use of medications to relieve dizziness (χ2=7.12, p=0.028), and vestibular rehabilitation (χ2=10.04, p=0.007) (Table 4). Though 51% of adults with BPPV indicated that CRMs relieved or eliminated their dizziness symptoms, 43% reported their symptoms were unchanged afterwards. Interestingly, 12% of those without BPPV indicated that CRMs reduced their dizziness symptoms and 79% reported their symptoms were unchanged following treatment (Table 4).
 |
Table 4 Response to Interventions |
Discussion
This study highlights several interesting findings. The most frequently reported symptom of those with BPPV was a falling sensation, even while sitting or lying down, and, though the proportions of symptoms reported by those with and without BPPV differed, there was considerable overlap. Thus, the presentation of BPPV was atypical for many registrants. Those with BPPV underwent an array of resource-intensive diagnostic tests more frequently than did those without BPPV. A large percentage of participants reported falling due to dizziness, and a not-insignificant proportion of participants reported that a fall prompted emergency care. The frequency with which specific interventions were received differed based on whether or not a diagnosis of BPPV was reported. Finally, whether or not participants perceived benefit from specific interventions, eg, CRMs, differed based on the condition they reported.
One explanation for why participants with BPPV often endorsed an atypical symptom profile may relate to the finding that 83% of these participants reported receiving at least one additional vestibular diagnosis. This is consistent with the literature on BPPV being prevalent in several populations of those with other peripheral and central vestibular disorders.8–16 In a critical review related to the association of BPPV with other vestibular conditions,7 it was concluded that BPPV is under-diagnosed in these cases because dizziness may be attributed to the primary pathology alone; affected persons may present with dizziness atypical of BPPV and, thus, are not exposed to diagnostic positioning maneuvers; or persons with dizziness may receive an initial diagnosis of BPPV and further work-up is not undertaken. Our findings suggest that diagnostic positioning maneuvers should be conducted in patients who report dizziness during position changes, even if the symptom profile is not typical for BPPV. Additionally, our data regarding the prolonged times to seek care and to receive a final diagnosis, as well as the lower rate of favorable outcomes after CRMs in those with BPPV compared to previous studies of those with typical BPPV,35 further support the conclusion that many registrants may have had atypical BPPV that was either secondary to or co-morbid with other vestibular disorders.
Audiometric testing, vestibular function tests, and advanced imaging are commonly ordered for persons with vestibular dizziness; however, the use of these resource-intensive diagnostic tests to evaluate persons suspected to have typical BPPV is not encouraged.17,18 Still, participants with BPPV in this study indicated more often undergoing advanced diagnostic testing than those who reported being diagnosed with other causes for vestibular dizziness and at rates much higher than prior reports on healthcare utilization for the BPPV population in the United States36 but similar to those reported in Europe.37 For example, Dunlap et al reported that imaging was recommended during 4.3% of physician visits coded for BPPV and 5.3% of physician visits coded for all other vestibular diagnoses.36 However, Grill et al found that, prior to being referred to a specialized tertiary balance clinic, 71% and 45% of those diagnosed with BPPV had undergone MRI and CT imaging, respectively.37 Advanced testing is recommended for those with signs and symptoms atypical for BPPV;17 thus, one might expect higher healthcare utilization in this study’s sample.
Experiencing ongoing dizziness and having impaired balance confers a 12-fold increase in the odds of falling.38 Our finding of a history of falls in 55% of persons with BPPV is higher than the 39% reported by Oghalai et al who investigated cases of unrecognized BPPV in older adults.39 This discrepancy may be related to the fact that our data were obtained through a questionnaire, whereas Oghalai et al gathered information about falls from health records. The higher incidence of falls in this sample may suggest that persons with atypical BPPV may have greater risk of falling compared to those with typical BPPV.40
Population-based data indicates that the emergency department visit rate for falls and fall-related injuries increased between 2003 and 201041 a period when considerable effort was devoted to falls prevention.42,43 Our findings of falls resulting in emergency care for 15% of participants with BPPV suggests that BPPV is not entirely benign and that additional efforts towards injury prevention in adults with BPPV are needed. Compared to the 12-months prior to treatment, the incidence of falls in adults with BPPV can be reduced by 65% in the 12 months following treatment with CRMs.44 Such a dramatic reduction in fall rates provides a benchmark against which falls prevention programs for adults with BPPV can be measured. Additionally, we recommend that future studies include fall rates as a factor in determining whether interventions for BPPV are successful.
Several authors report that atypical BPPV is less responsive to CRMs.45–47 Thus, the fact that a large number of participants in this study may have had BPPV that was secondary to or co-morbid with other vestibular disorders may explain why only 51% of those with BPPV indicated that CRMs either eliminated their dizziness or improved its frequency and/or severity. Interestingly, 12% of those without BPPV endorsed that CRMs resulted in improvement of their dizziness. This raises the question of whether so-called “type 2 BPPV”48 was present in these cases. The fact that many registrants without BPPV endorsed receiving CRMs may suggest that this intervention was administered successfully in cases of undiagnosed BPPV, that it is frequently inappropriately implemented, and/or that some registrants may have misunderstood or were unable to accurately recall their diagnosis. Although the questions posed in the registry regarding treatment outcomes were specific to each intervention that a participant reported receiving, our analysis cannot rule out the possibility of an interaction effect between multiple interventions. Further research regarding mono-therapy and multi-therapy outcomes in adults with and without BPPV is needed to better assess overall care.
A large proportion of registrants with (85%) and without (78%) BPPV indicated being prescribed medication to relieve dizziness. This is in contrast with a prior report that revealed, across all specialties, anti-vertigo medications were recommended during 16% of physician visits coded for BPPV and 22% of physician visits coded for all other vestibular disorders.36 In this analysis of a nation-wide dataset, Dunlap and colleagues showed that primary care physicians more frequently prescribed anti-vertigo medications compared to specialists such as otolaryngologists and neurologists.36 One reason for this discrepancy may be that, compared to those analyzed by Dunlap and colleagues, registrants in this study may have had more chronic, unrelenting symptoms and, thus, may have been more likely to be offered medications. In the study by Dunlap and colleagues, 50% of those whose care was coded as being for BPPV and 46% of those whose care was coded as being for other vestibular diagnoses were seen for acute symptoms; whereas, the times to seek care and to receive a final diagnosis in our analysis suggest that the majority of registrants had chronic dizziness.
Clinical Take-Aways
Based on our findings, we recommend that clinicians who evaluate and treat persons with BPPV consider the following:
- Atypical BPPV may be more common that previously known49
- Persons with atypical BPPV may require specific management that is provisionally acceptable per the current BPPV CPG but is not necessarily encouraged49
- Adults with BPPV who are at increased risk for falling should be started on a comprehensive fall prevention program
Limitations
Though a large amount of data is gathered through the VeDA registry, the self-reported nature of this information is a primary limitation of our analyses. Related to this is that the registry questionnaires are not administered at the point of care, and, thus, lack details related to the chronology of specific data points. Unlike the data gathered for other vestibular registries, the information we analyzed cannot be corroborated with health records. Even so, cross-referencing with health records may be insufficient as the diagnosis of BPPV is often mistakenly utilized. It is optimal for BPPV to be confirmed by a specialist; thus, we cannot be certain that our group assignment is entirely accurate. Also, it may be more likely that persons with chronic and/or severe symptoms were attracted to the VeDA registry; therefore, our findings may not be generalizable to the overall population of adults with dizziness. Ultimately, population-based, prospective studies of unselected adults who develop vestibular dizziness that augments self-reported data with confirmation of the diagnosis by vestibular specialists are needed to clarify relationships between the perception and reality of healthcare for persons with dizziness.
Conclusions
Our findings support several overarching conclusions. Atypical BPPV may be more common than previously recognized. Though diagnostics and medications have roles in the management of vestibular dizziness, advanced tests and anti-vertigo medications are reported to continue to be used at high rates, particularly for those who may have atypical BPPV. The high rates of falls in those with and without BPPV suggest that falls prevention should be a top priority in the management of persons with vestibular dizziness. The specific patient-reported outcomes data analyzed herein suggests that adults with BPPV also report significant differences in how their care is managed and their overall outcomes compared to the recommendations in the BPPV CPG and to those without BPPV. More broadly, the mounting evidence related to atypical BPPV must be considered further when the BPPV CPG is revised. Finally, perceptions regarding the effectiveness of interventions such as CRMs may differ between patients and providers; thus, providers should consider a patient’s diagnostic test results and the patient’s self-reported assessment of the effectiveness of interventions when evaluating outcomes for those with BPPV.
Abbreviations
BPPV, Benign Paroxysmal Positional Vertigo; CRM, canalith repositioning maneuver; CT, computed tomography; IQR, inter-quartile range; MRI, magnetic resonance imaging; PIN, Patient Insights Network; VeDA, Vestibular Disorders Association.
Data Sharing Statement
The dataset supporting the conclusions of this article is available from the authors upon written request.
Ethics Approval and Consent to Participate
The Advarra Institutional Review Board approved this research. All participants gave written consent.
Acknowledgment
We thank Habib Risk, MD for reviewing the manuscript prior to its submission and for providing thoughtful suggestions to enhance its content.
Author Contributions
CRG and MCS are responsible for the study design. PLG and CR are responsible for the design of the registry and assisted with acquisition of the registry data. CRG performed all analyses and wrote the original draft of the manuscript. All authors contributed to preparing the manuscript for publication through its writing and/or revision, have reviewed the versions of this manuscript that were submitted for publication, agree with the submission of this manuscript to this journal, and agree to take responsibility and be accountable for the contents of the manuscript.
Funding
There is no funding to report.
Disclosure
Dr. Schubert is a member of the medical advisory board for the Vestibular Disorders Association. The authors report no other conflicts of interest in this work.
References
1. von Brevern M, Radtke A, Lezius F, et al. Epidemiology of benign paroxysmal positional vertigo: a population based study. J Neurol Neurosurg Psychiatry. 2007;78(7):710–715. doi:10.1136/jnnp.2006.100420
2. Mizukoshi K, Watanabe Y, Shojaku H, Okubo J, Watanabe I. Epidemiological studies on benign paroxysmal positional vertigo in Japan. Acta Otolaryngol Suppl. 1988;105(sup447):67–72. doi:10.3109/00016488809102859
3. Froehling DA, Silverstein MD, Mohr DN, Beatty CW, Offord KP, Ballard DJ. Benign positional vertigo: incidence and prognosis in a population-based study in Olmsted County, Minnesota. Mayo Clin Proc. 1991;66(6):596–601. doi:10.1016/S0025-6196(12)60518-7
4. Hall SF, Ruby RR, McClure JA. The mechanics of benign paroxysmal vertigo. J Otolaryngol. 1979;8(2):151–158.
5. Schuknecht HF. Cupulolithiasis. Arch Otolaryngol. 1969;90(6):765–778. doi:10.1001/archotol.1969.00770030767020
6. Furman JM, Cass SP. Benign paroxysmal positional vertigo. N Engl J Med. 1999;341(21):1590–1596. doi:10.1056/NEJM199911183412107
7. Riga M, Bibas A, Xenellis J, Korres S. Inner ear disease and benign paroxysmal positional vertigo: a critical review of incidence, clinical characteristics, and management. Int J Otolaryngol. 2011;2011:709469. doi:10.1155/2011/709469
8. Gross EM, Ress BD, Viirre ES, Nelson JR, Harris JP. Intractable benign paroxysmal positional vertigo in patients with Meniere’s disease. Laryngoscope. 2000;110(4):655–659. doi:10.1097/00005537-200004000-00022
9. Perez N, Martin E, Zubieta JL, Romero MD, Garcia-Tapia R. Benign paroxysmal positional vertigo in patients with Meniere’s disease treated with intratympanic gentamycin. Laryngoscope. 2002;112(6):1104–1109. doi:10.1097/00005537-200206000-00031
10. Mandalà M, Santoro GP, Awrey J, Nuti D. Vestibular neuritis: recurrence and incidence of secondary benign paroxysmal positional vertigo. Acta Otolaryngol. 2010;130(5):565–567. doi:10.3109/00016480903311278
11. Kim MB, Ban JH. Benign paroxysmal positional vertigo accompanied by sudden sensorineural hearing loss: a comparative study with idiopathic benign paroxysmal positional vertigo. Laryngoscope. 2012;122(12):2832–2836. doi:10.1002/lary.23607
12. Lee NH, Ban JH, Lee KC, Kim SM. Benign paroxysmal positional vertigo secondary to inner ear disease. Otolaryngol Head Neck Surg. 2010;143(3):413–417. doi:10.1016/j.otohns.2010.06.905
13. Magliulo G, Gagliardi M, Cuiuli G, Celebrini A, Parrotto D, D’Amico R. Stapedotomy and post-operative benign paroxysmal positional vertigo. J Vestib Res. 2005;15(3):169–172. doi:10.3233/VES-2005-15305
14. Viccaro M, Mancini P, La Gamma R, De Seta E, Covelli E, Filipo R. Positional vertigo and cochlear implantation. Otol Neurotol. 2007;28(6):764–767. doi:10.1097/MAO.0b013e318064e8d4
15. Katsarkas A. Benign paroxysmal positional vertigo (BPPV): idiopathic versus post-traumatic. Acta Otolaryngol. 1999;119(7):745–749. doi:10.1080/00016489950180360
16. Ishiyama A, Jacobson KM, Baloh RW. Migraine and benign positional vertigo. Ann Otol Rhinol Laryngol. 2000;109(4):377–380. doi:10.1177/000348940010900407
17. Bhattacharyya N, Gubbels SP, Schwartz SR, et al. Clinical practice guideline: benign paroxysmal positional vertigo (Update). Otolaryngol Head Neck Surg. 2017;156(3_suppl):S1–S47. doi:10.1177/0194599816689667
18. Rizk H, Wal Y, Barthel S, et al. Quality improvement in neurology: neurotology quality measurement set. Otolaryngol Head Neck Surg. 2018;159(4):603–607. doi:10.1177/0194599818790947
19. Castellucci A, Malara P, Martellucci S, Delmonte S, Ghidini A. Fluctuating posterior canal function in benign paroxysmal positional vertigo depending on how and where otoconia are disposed. Otol Neurotol. 2021;42(2):e193–e198. doi:10.1097/MAO.0000000000002913
20. Castellucci A, Botti C, Martellucci S, et al. Spontaneous upbeat nystagmus and selective anterior semicircular canal hypofunction on video head impulse test: a new variant of Canalith Jam? J Audiol Otol. 2021. doi:10.7874/jao.2021.00297
21. Imai T, Ito M, Takeda N, et al. Natural course of the remission of vertigo in patients with benign paroxysmal positional vertigo. Neurology. 2005;64(5):920–921. doi:10.1212/01.WNL.0000152890.00170.DA
22. McDonnell MN, Hillier SL. Vestibular rehabilitation for unilateral peripheral vestibular dysfunction. Cochrane Database Syst Rev. 2015;1:CD005397. doi:10.1002/14651858.CD005397.pub4
23. Heger M. A registry of registries? The US backs the idea for patients. Nat Med. 2011;17(1):4–4a. doi:10.1038/nm0111-4a
24. Agus S, Benecke H, Thum C, Strupp M. Clinical and demographic features of vertigo: findings from the REVERT registry. Front Neurol. 2013;4:48. doi:10.3389/fneur.2013.00048
25. Grill E, Muller T, Becker-Bense S, et al. DizzyReg: the prospective patient registry of the German center for vertigo and balance disorders. J Neurol. 2017;264(Suppl1):34–36. doi:10.1007/s00415-017-8438-7
26. Benecke H, Agus S, Kuessner D, Goodall G, Strupp M. The burden and impact of vertigo: findings from the REVERT patient registry. Front Neurol. 2013;4:136. doi:10.3389/fneur.2013.00136
27. Strobl R, Grozinger M, Zwergal A, Huppert D, Filippopulos F, Grill E. A set of eight key questions helps to classify common vestibular disorders-results from the DizzyReg patient registry. Front Neurol. 2021;12:670944. doi:10.3389/fneur.2021.670944
28. Habs M, Strobl R, Grill E, Dieterich M, Becker-Bense S. Primary or secondary chronic functional dizziness: does it make a difference? A DizzyReg study in 356 patients. J Neurol. 2020;267(Suppl1):212–222. doi:10.1007/s00415-020-10150-9
29. Vestibular Disorders Association. Available from: www.vestibular.org.
30. INVITAE. Available from: https://connect.invitae.com/org/veda.
31. Kroenke K, Hoffman RM, Einstadter D. How common are various causes of dizziness? A critical review. South Med J. 2000;93(2):
32. R Core Team. R: a language and environment for statistical computing. R Foundation for Statistical Computing; 2021.
33. von Elm E, Altman DG, Egger M, et al. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: guidelines for reporting observational studies. PLoS Med. 2007;4(10):e296. doi:10.1371/journal.pmed.0040296
34. Benchimol EI, Smeeth L, Guttmann A, et al. The REporting of studies Conducted using Observational Routinely-collected health Data (RECORD) statement. PLoS Med. 2015;12(10):e1001885. doi:10.1371/journal.pmed.1001885
35. Gordon CR, Gadoth N. Repeated vs single physical maneuver in benign paroxysmal positional vertigo. Acta Neurol Scand. 2004;110(3):166–169. doi:10.1111/j.1600-0404.2004.00296.x
36. Dunlap PM, Khoja SS, Whitney SL, Freburger JK. Assessment of health care utilization for dizziness in ambulatory care settings in the United States. Otol Neurotol. 2019;40(9):e918–e924. doi:10.1097/MAO.0000000000002359
37. Grill E, Strupp M, Müller M, Jahn K. Health services utilization of patients with vertigo in primary care: a retrospective cohort study. J Neurol. 2014;261(8):1492–1498. doi:10.1007/s00415-014-7367-y
38. Agrawal Y, Carey JP, Della Santina CC, Schubert MC, Minor LB. Disorders of balance and vestibular function in US adults: data from the National Health and Nutrition Examination Survey, 2001–2004. Arch Intern Med. 2009;169(10):938–944. doi:10.1001/archinternmed.2009.66
39. Oghalai JS, Manolidis S, Barth JL, Stewart MG, Jenkins HA. Unrecognized benign paroxysmal positional vertigo in elderly patients. Otolaryngol Head Neck Surg. 2000;122(5):630–634. doi:10.1016/S0194-5998(00)70187-2
40. Herdman SJ, Blatt P, Schubert MC, Tusa RJ. Falls in patients with vestibular deficits. Am J Otol. 2000;21(6):847–851.
41. Shankar KN, Liu SW, Ganz DA. Trends and characteristics of emergency department visits for fall-related injuries in older adults, 2003–2010. West J Emerg Med. 2017;18(5):785–793. doi:10.5811/westjem.2017.5.33615
42. Guideline for the prevention of falls in older persons. American Geriatrics Society, British Geriatrics Society, and American Academy of Orthopaedic Surgeons Panel on Falls Prevention. J Am Geriatr Soc. 2001;49(5):664–672.
43. Panel on Prevention of Falls in Older Persons, American Geriatrics Society and British Geriatrics Society. Summary of the Updated American Geriatrics Society/British Geriatrics Society clinical practice guideline for prevention of falls in older persons. J Am Geriatr Soc. 2011;59(1):148–157. doi:10.1111/j.1532-5415.2010.03234.x.
44. Gananca FF, Gazzola JM, Gananca CF, Caovilla HH, Gananca MM, Cruz OL. Elderly falls associated with benign paroxysmal positional vertigo. Braz J Otorhinolaryngol. 2010;76(1):113–120.
45. Monobe H, Sugasawa K, Murofushi T. The outcome of the canalith repositioning procedure for benign paroxysmal positional vertigo: are there any characteristic features of treatment failure cases? Acta Otolaryngol Suppl. 2001;545:38–40. doi:10.1080/000164801750388081
46. Del Rio M, Arriaga MA. Benign positional vertigo: prognostic factors. Otolaryngol Head Neck Surg. 2004;130(4):426–429. doi:10.1016/j.otohns.2003.12.015
47. Korres S, Balatsouras DG, Ferekidis E. Prognosis of patients with benign paroxysmal positional vertigo treated with repositioning manoeuvres. J Laryngol Otol. 2006;120(7):528–533. doi:10.1017/S0022215106000958
48. Buki B, Simon L, Garab S, Lundberg YW, Junger H, Straumann D. Sitting-up vertigo and trunk retropulsion in patients with benign positional vertigo but without positional nystagmus. J Neurol Neurosurg Psychiatry. 2011;82(1):98–104. doi:10.1136/jnnp.2009.199208
49. Harmat K, Tamás LT, Schubert MC, Gerlinger I, Komoly S, Büki B. Prevalence of and theoretical explanation for type 2 benign paroxysmal positional vertigo. J Neurol Phys Ther. 2022;46(2):88–95. doi:10.1097/NPT.0000000000000383
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.