Back to Journals » Journal of Pain Research » Volume 16
Patient-Reported Satisfaction with Using a Rechargeable 10 kHz Spinal Cord Stimulation Device
Authors Hagedorn JM ![]() , Tate J, Bharara M
, Tate J, Bharara M ![]()
Received 1 July 2022
Accepted for publication 8 October 2022
Published 5 January 2023 Volume 2023:16 Pages 47—53
DOI https://doi.org/10.2147/JPR.S374499
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Andrea Tinnirello
Jonathan M Hagedorn,1 Jordan Tate,2 Manish Bharara3
1iSpine Pain Physicians, Maple Grove, MN, USA; 2Southern Pain and Spine, Jasper, GA, USA; 3Clinical Affairs Department, Nevro Corp, Redwood City, CA, USA
Correspondence: Jonathan M Hagedorn, iSpine Pain Physicians, Maple Grove, MN, USA, Tel +1 763-201-8191, Fax +1 763-201-8192, Email [email protected]
Introduction: Chronic pain is a common clinical condition and is frequently treated with a variety of medications, but pharmacotherapy is oftentimes not the optimal long-term treatment option. Safe and effective long-term pain relief for trunk and limb pain is available using high-frequency spinal cord stimulation at 10 kHz (10 kHz SCS), which is delivered using a rechargeable implantable pulse generator (IPG). Although rechargeable devices have been shown to reduce patient risk and overall cost by eliminating the need for periodic surgeries to replace depleted non-rechargeable IPGs, there is little published evidence that rechargeable technology is practical and convenient for patients, especially in the context of 10 kHz SCS.
Objective: This analysis of real-world patients implanted with 10 kHz SCS devices was undertaken using patient data from an industry-maintained database to investigate whether there was a substantial burden associated with rechargeable SCS and the degree of patient satisfaction or dissatisfaction with 10 kHz SCS.
Results: This study included 10,391 men and women who were implanted with 10 kHz SCS devices to treat chronic pain of the trunk and/or limbs. They received stimulation for a median of 361 days (180– 1550 days), and 65.48% had previous spine surgery. In this patient sample, most patients were satisfied with the efficacy of 10 kHz SCS, including 77% who would repeat the procedure and 71% who would recommend it to other patients with similar pain. In regards to IPG recharging, 70% were satisfied or very satisfied and 19% were neutral, and a majority of patients recharged their device daily for 30 to 60 minutes.
Conclusion: These results indicate most patients do not find IPG recharging inconvenient or burdensome. In addition, IPG recharging is not a barrier to the majority of patients benefitting from 10 kHz SCS for long-term pain relief.
Keywords: SCS, spinal cord stimulation, satisfaction, real-world
Introduction
Chronic pain is a common clinical condition, which has been estimated to affect over 20% of the adult population in the United States, with 8% suffering with chronic pain that substantially impacts their quality of life, such as limiting daily or work activities.1 Pain is frequently treated with medications, including opioid analgesics, but such treatment has not been proven effective for long-term pain relief.2–4 Spinal cord stimulation (SCS) has been used clinically since the 1980s, and has been proven to provide long-term, non-pharmacologic pain relief for chronic intractable pain from a variety of etiologies.5 Conventional SCS involves programming frequencies of less than 1000 Hz, most commonly in the 40–60 Hz range, and produces the sensation of paresthesia, which must overlap the area of pain to provide analgesia; however, paresthesia can also cause discomfort that limits its use in some patients.6 High-frequency SCS, delivered at 10 kilohertz (10 kHz SCS), is an alternative form of SCS that functions in a paresthesia-free manner and has been shown to provide superior pain relief for low back and lower limb pain.7 SCS devices are powered by implantable pulse generators (IPGs) that generate the current delivered by the leads. Conventional, non-rechargeable (NRC) IPGs must be replaced periodically with a new device via surgery once its power reserve is depleted. In 2005, rechargeable (RC) IPGs were introduced, offering reduced risk by avoiding the requirement for additional surgery to replace a depleted IPG.8 Recharging is done via an external charger placed next to the skin, thus patients are limited in their activities during recharging periods. Conventional SCS can be provided by NRC or RC devices, while 10 kHz SCS is only available as an RC device.
Published estimates of the comparative costs of NRC versus RC devices delivering conventional, low-frequency SCS for chronic pain have predominantly found the longer lifespan of the RC devices makes them more cost-effective overall.9–14 A longer lifespan for RC devices results in fewer surgeries, such as those to replace depleted IPGs. Undergoing multiple revision surgeries is known to increase the risk of infection, particularly among patients with other risk factors such as uncontrolled diabetes mellitus,15 and studies examining the effect of different IPGs on outcomes have found RC devices are indeed associated with lower rates of complications than NRC devices.11 A recent comparative study by Luecke et al showed patients treated with RC devices have reduced pain diagnoses, hospitalizations, physician visits, and use of pain medications compared to patients treated with NRC devices.16
In addition to costs and objective outcomes, patient satisfaction with the use of RC or NRC devices is critical for determining how broadly useful these therapies can be for treating patients with chronic pain; however, there has been little published research on this topic. Previous, small surveys of real-world patient cohorts revealed most individuals preferred RC to NRC devices, and the biggest patient-perceived downside to NRC devices was the possibility there could be an extended period without pain relief if implantation of the new IPG was delayed.17 Finally, a minority of real-world patients reported that lifestyle costs outweighed the benefits of RC devices, particularly among those individuals who were older and those who recharged more often.18 Although the published literature supports the use of RC IPGs from a cost and longevity standpoint, concern exists regarding patient dissatisfaction with this IPG option given the “burden” of necessary recharge for on-going device use. Our objective was to evaluate patient dissatisfaction with IPG recharge requirement following implantation of a RC IPG for various chronic pain indications.
Methods
This real-world, retrospective study included patients implanted with a 10 kHz SCS system (Nevro Corp, Redwood City, California) to treat chronic refractory pain of the trunk and/or limbs. Patient data from October 2, 2016 through January 29, 2020 was obtained from an industry-maintained registry, HFX CloudTM (Nevro Corp).
Procedures
Trial stimulation and implant procedures for 10 kHz SCS have been previously described.19 Briefly, patients underwent implantation of octapolar leads in the epidural space at locations determined by the area of the patient’s pain. The patients first underwent a trial of 10 kHz stimulation for up to 14 days, and those who had pain relief of ≥50% were eligible for a permanent implant. Stimulation was delivered at a frequency of 10 kHz, pulse width of 30 μs, and amplitudes adjusted to maximize each individual patient’s pain relief.
Patient-Reported Outcomes
Patient-reported outcomes (PROs) were collected when patients were contacted by telephone at 3, 6, 12, and 24 months after implant. The only criterion for inclusion was being previously implanted with a 10 kHz SCS device, and no specific exclusion criteria were used. Responses from all patients who were successfully contacted within 2 weeks of the relevant timepoint (3, 6, 12, or 24 months) were included, and no responses were excluded. Some of the responses were obtained over the telephone by a therapy support specialist employed by Nevro Corp, while other data were collected with a survey administered via text messaging, which the patient filled out independently, without any direct human involvement. Individual patients may have provided multiple responses over time; if so, the reported data is the most recent patient response available. Given the nature of this data, results are reported descriptively, and median values are reported where appropriate.
Ethics Consideration
All data were collected independent of the centers in which patients were implanted and were obtained fully deidentified, thereby obviating the need for ethics board review approval of this evaluation per United States 45 Code of Federal Regulations (CFR) § 46.104(d)(2)(i).
Results
Patient Demographics
The study population had more women (56.12%) than men and included a mix of patients with and without previous spine surgery (Table 1). The median follow-up was one year, and the majority of patients had no previous experience with neuromodulation. All patients in this study received 10 kHz SCS to treat chronic pain of the trunk and/or limbs, and most had pain in the lower back and lower limbs.
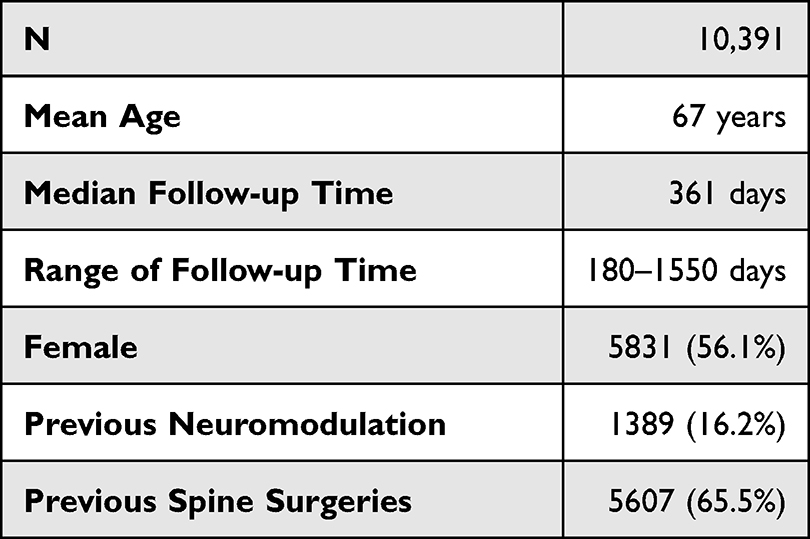 |
Table 1 Patient Demographics |
Patient Satisfaction
Over 80% of the patients in this study rated their activity limitations, symptoms, emotions, and overall quality of life as “a great deal better” or “moderately better” since initiating 10 kHz SCS, while only 5% reported a worsening of these same outcomes (Figure 1).
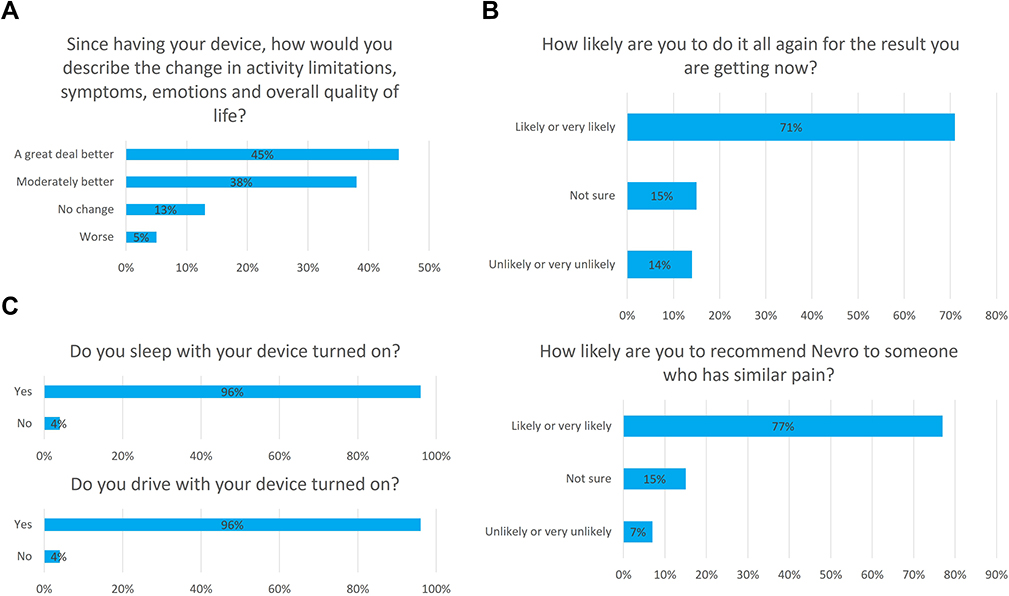 |
Figure 1 Most patients were satisfied with the efficacy and tolerability of 10 kHz SCS. The graphs show (A) the change in patients’ activity limitations, symptoms, emotions, and overall quality of life since initiating 10 kHz SCS treatment (n = 10,390), (B) patients’ willingness to repeat the process of receiving SCS therapy again to achieve the same results (n = 10,391) and the likelihood they would recommend 10 kHz SCS to someone with similar pain (n = 10,369), and (C) whether patients slept (n = 10,388) or drove (n = 10,035) with their SCS device powered on. |
More than 70% reported being “likely” or “very likely” to repeat the procedure again to get the same results or to recommend 10 kHz SCS to another individual with a similar pain experience. Finally, 96% of patients reported sleeping with the 10 kHz SCS device powered on. Of the subgroup of patients who had prior experience with SCS (N = 1205), three-fourths rated 10 kHz SCS a “great deal better” or “moderately better” than conventional SCS (Figure 2).
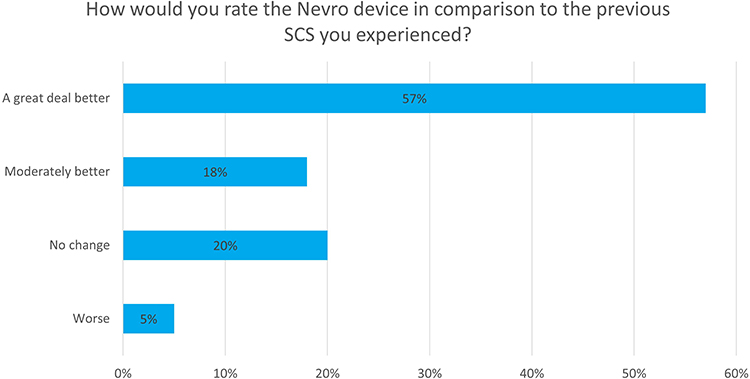 |
Figure 2 Patients with previous experience with neuromodulation preferred 10 kHz SCS to conventional SCS (n = 1205). |
IPG Charging
Most patients surveyed did not individually adjust the therapy settings of their 10 kHz SCS device. About half reported never using their remote to adjust therapy settings, and an additional one-third adjusted it once per week or less (Figure 3).
 |
Figure 3 Most patients were satisfied with the recharging demands of their device. The graphs show (A) the frequency with which patients needed to adjust the settings of their device using the remote (n = 10,387), (B) patients’ satisfaction with the convenience of recharging the device (n = 10,387), and (C) the frequency (n = 10,385) and time (n = 10,386) needed for IPG recharging. |
Seventy percent were “satisfied” or “very satisfied” and 19% were “neutral” with the convenience of recharging requirements for their 10 kHz SCS device. Of the 11% who were “dissatisfied” or “very dissatisfied”, 64% reported “a great deal better” or “moderately better” overall quality of life since initiating 10 kHz SCS. More than 50% of these patients who were dissatisfied with recharging requirements also responded that they would recommend the same therapy to friends or family members with similar pain. About two-thirds of the survey population reported recharging their device daily, and a similar proportion reported a recharging time of 30 to 60 minutes.
Discussion
The efficacy of 10 kHz SCS for relieving chronic pain has been documented in many clinical trials,7,19–24 but there is a paucity of data assessing patient perceptions and benefits of RC IPGs. This study of over 10,000 patients demonstrates high satisfaction rates amongst patients that use 10 kHz SCS for chronic pain, in addition to other benefits including patients’ functioning and quality of life. A large majority of patients in our sample indicated that their activity, limitations, symptoms, emotions, and overall quality of life was “better” or “a great deal better” than before beginning 10 kHz SCS, would be willing to undergo the same process again to achieve the same result, and would recommend it to friends or family members with similar pain. These results are in line with previous studies of low-frequency SCS with RC IPGs,25 suggesting that for most patients the benefits of stimulation were of a large enough magnitude to be worth the risks, costs, and any perceived inconveniences associated with testing and implanting a SCS device, including necessary recharging of the IPG.
Paresthesia-free pain relief is one of the primary advantages of 10 kHz SCS over low-frequency modalities, since paresthesia can be uncomfortable, or even intolerable to some patients, and paresthesia-based stimulation cannot be used during certain activities such as driving.6 Our results also confirm that in these patients 10 kHz SCS provided effective pain relief without paresthesia, and nearly all patients slept and drove with their device powered on, activities which are not usually possible or permitted when using low-frequency SCS. Previous research has also reported that pain relief from 10 kHz SCS is durable over time,26–28 and our results showed that pain relief from 10 kHz SCS was, likewise, consistent and stable over time. Nearly half of the respondents never adjusted the therapy settings of their device, and a large majority adjusted their pain relief settings once per week or less. This is vastly different than prior reports, which suggested that patients make approximately 18 to 31 adjustments per day.29 This durability and consistency in pain relief is essential for any treatment for chronic pain. Finally, a subset of the patient sample had previous experience with low-frequency SCS, allowing an indirect comparison of that modality with 10 kHz stimulation. Among these patients, the majority responded that 10 kHz SCS was “a great deal better” than their previous SCS experience, and only 1 in 20 perceived 10 kHz SCS as worse.
Although RC devices have been used clinically for some time with all SCS modalities, few studies have assessed patients’ recharging behavior or determining whether patients are comfortable and satisfied with the recharging process. Patients with chronic pain may have difficulties with the recharging process, and it has been shown that for low-frequency SCS, NRC devices may be the best treatment option.18 To our knowledge, no assessment of patients’ recharging experience has yet been published for 10 kHz SCS.
In this sample of over 10,000 patients, a large majority reported being either “very satisfied”, “satisfied”, or “neutral” with the convenience of the recharging process, which is reflective of results in patients with RC devices for low-frequency SCS.17,18,25 The frequency of recharging and length of individual recharge sessions can impact the convenience of the recharging process as well as the amount of time the device is available to provide pain relief. Our results showed that two-thirds of respondents charged their device daily and that the majority spent 30 to 60 minutes in each charging session, and nearly one-quarter of respondents charged for less than 30 minutes at each recharge session. These data suggest that although daily charging is often needed for 10 kHz SCS, the aggregate time spent in charging is comparable to those for low-frequency stimulation.18
There are several limitations within this study that must be addressed. Because only a single SCS technology was used in this survey, it is not known if these results are broadly applicable. However, the programming variations used in this sample affect the amount of time that is required to charge the IPG, consistent with previously published literature.30 Provenzano et al, (2021) reported that patients using pulse dosing of 10kHz SCS reported similar pain relief and satisfaction to those on standard dosage.30 This variation in the individual charging experience of each patient suggests responses on charging satisfaction are broadly applicable. Another limitation concerns the reliability of comparisons of RC IPGs with NRC IPGs due to the relatively small number of patients with a previous history using NRC systems (a subset of N=1205 patients). The rest of the results, in comparison, were derived from a pool of over 10,000 patients. Additionally, using data obtained from an industry-maintained registry may have introduced bias into the results, but industry involvement in the database is restricted to maintaining the data and making the data available. The patient survey was administered partially by text message, minimizing possible influence on the data. Finally, not all implanted patients responded to all questionnaire requests and data on how many patients were initially contacted with the questionnaire are unavailable, however, the percentage change between responses was relatively small due to the large number of patients, minimizing resulting gaps in the data.
Conclusion
Within this large patient dataset of over 10,000 individuals, 70% of implanted patients were “satisfied” or “very satisfied”, 19% were “neutral”, and 11% were “dissatisfied” or “very dissatisfied” with the convenience of the IPG recharging process. It does not appear that IPG recharging detrimentally affects therapy outcome or patient satisfaction following 10 kHz SCS implantation.
Acknowledgments
The authors thank Erik MacLaren, PhD, from Galen Medical Writing, LLC for medical writing assistance in the preparation of this manuscript.
Funding
There is no funding to report.
Disclosure
JMH is a consultant for Abbott, Boston Scientific, Nevro Corp, and Saluda. He has funded research with Abbott, Medtronic, and Saluda. JLT is a consultant for Nevro Corp. MB is an employee of Nevro Corp. The authors report no other conflicts of interest in this work.
References
1. Dahlhamer J, Lucas J, Zelaya C, et al. Prevalence of chronic pain and high-impact chronic pain among adults - United States, 2016. MMWR Morb Mortal Wkly Rep. 2018;67(36):1001–1006. doi:10.15585/mmwr.mm6736a2
2. Dowell D, Haegerich TM, Chou R. CDC guideline for prescribing opioids for chronic pain--United States, 2016. JAMA. 2016;315(15):1624–1645. doi:10.1001/jama.2016.1464
3. Gupta M, Abd-Elsayed A, Knezevic NN. Improving care of chronic pain patients with spinal cord stimulator therapy amidst the opioid epidemic. Neurol Sci. 2020;41(10):2703–2710. doi:10.1007/s10072-020-04435-0
4. Hylands-White N, Duarte RV, Raphael JH. An overview of treatment approaches for chronic pain management. Rheumatol Int. 2017;37(1):29–42. doi:10.1007/s00296-016-3481-8
5. Wolter T. Spinal cord stimulation for neuropathic pain: current perspectives. J Pain Res. 2014;7:651–663. doi:10.2147/JPR.S37589
6. De Carolis G, Paroli M, Tollapi L, et al. Paresthesia-independence: an assessment of technical factors related to 10 kHz paresthesia-free spinal cord stimulation. Pain Physician. 2017;20(4):331–341.
7. Kapural L, Yu C, Doust MW, et al. Novel 10-kHz High-frequency Therapy (HF10 Therapy) is superior to traditional low-frequency spinal cord stimulation for the treatment of chronic back and leg pain: the SENZA-RCT randomized controlled trial. Anesthesiology. 2015;123(4):851–860. doi:10.1097/ALN.0000000000000774
8. Boston Scientific. Revolutionary technology offers new hope for treating chronic pain [press release], March 29, 2005. Available from: https://news.bostonscientific.com/news-releases?item=58694.
9. Abejon D, Vancamp T, Monzon EM, Cost-Consequence Analysis A. Examining the differences between non-rechargeable and rechargeable systems. Anesth Pain Med. 2020;10(1):e100308. doi:10.5812/aapm.100308
10. Annemans L, Van Buyten JP, Smith T, Al-Kaisy A. Cost effectiveness of a novel 10 kHz high-frequency spinal cord stimulation system in patients with failed back surgery syndrome (FBSS). J Long Term Eff Med Implants. 2014;24(2–3):173–183. doi:10.1615/JLongTermEffMedImplants.2014011685
11. Hornberger J, Kumar K, Verhulst E, Clark MA, Hernandez J. Rechargeable spinal cord stimulation versus non-rechargeable system for patients with failed back surgery syndrome: a cost-consequences analysis. Clin J Pain. 2008;24(3):244–252. doi:10.1097/AJP.0b013e318160216a
12. Thomson SJ, Kruglov D, Duarte RV. A spinal cord stimulation service review from a single centre using a single manufacturer over a 7.5 year follow-up period. Neuromodulation. 2017;20(6):589–599. doi:10.1111/ner.12587
13. Kumar K, Rizvi S. Cost-effectiveness of spinal cord stimulation therapy in management of chronic pain. Pain Med. 2013;14(11):1631–1649. doi:10.1111/pme.12146
14. Costandi S, Mekhail N, Azer G, et al. Longevity and utilization cost of rechargeable and non-rechargeable spinal cord stimulation implants: a comparative study. Pain Pract. 2020;20(8):937–945. doi:10.1111/papr.12926
15. Follett KA, Boortz-Marx RL, Drake JM, et al. Prevention and management of intrathecal drug delivery and spinal cord stimulation system infections. Anesthesiology. 2004;100(6):1582–1594. doi:10.1097/00000542-200406000-00034
16. Luecke T, Kuhlmann H, May M, Petermann M, Libutzki B, Jaehnichen G. Spinal cord stimulation: a real-world data analysis on outcomes and differences between rechargeable and non-rechargeable implantable pulse generators. J Int Med Res. 2021;49(8):3000605211038457. doi:10.1177/03000605211038457
17. McAuley J, Farah N, Van groningen R, Green C. A questionnaire-based study on patients’ experiences with rechargeable implanted programmable generators for spinal cord stimulation to treat chronic lumbar spondylosis pain. Neuromodulation. 2013;16(2):142–146. doi:10.1111/j.1525-1403.2012.00456.x
18. Lam CK, Rosenow JM. Patient perspectives on the efficacy and ergonomics of rechargeable spinal cord stimulators. Neuromodulation. 2010;13(3):218–223. doi:10.1111/j.1525-1403.2009.00269.x
19. Gupta M, Scowcroft J, Kloster D, et al. 10-kHz spinal cord stimulation for chronic postsurgical pain: results from a 12-month prospective, multicenter study. Pain Pract. 2020;20(8):908–918. doi:10.1111/papr.12929
20. Al-Kaisy A, Van Buyten JP, Kapural L, et al. 10 kHz spinal cord stimulation for the treatment of non-surgical refractory back pain: subanalysis of pooled data from two prospective studies. Anaesthesia. 2020;75(6):775–784. doi:10.1111/anae.15036
21. Al-Kaisy A, Palmisani S, Smith TE, et al. 10 kHz high-frequency spinal cord stimulation for chronic axial low back pain in patients with no history of spinal surgery: a preliminary, prospective, open label and proof-of-concept study. Neuromodulation. 2017;20(1):63–70. doi:10.1111/ner.12563
22. Galan V, Scowcroft J, Chang P, et al. 10-kHz spinal cord stimulation treatment for painful diabetic neuropathy: results from post-hoc analysis of the SENZA-PPN study. Pain Manag. 2020;10(5):291–300. doi:10.2217/pmt-2020-0033
23. Kapural L, Gupta M, Paicius R, et al. Treatment of chronic abdominal pain with 10-kHz spinal cord stimulation: safety and efficacy results from a 12-month prospective, multicenter, feasibility study. Clin Transl Gastroenterol. 2020;11(2):e00133. doi:10.14309/ctg.0000000000000133
24. Van Buyten JP, Al-Kaisy A, Smet I, Palmisani S, Smith T. High-frequency spinal cord stimulation for the treatment of chronic back pain patients: results of a prospective multicenter European clinical study. Neuromodulation. 2013;16(1):59–65; discussion 65–56. doi:10.1111/ner.12006
25. Van Buyten JP, Fowo S, Spincemaille GH, et al. The restore rechargeable, implantable neurostimulator: handling and clinical results of a multicenter study. Clin J Pain. 2008;24(4):325–334. doi:10.1097/AJP.0b013e31816216a9
26. Al-Kaisy A, Van Buyten JP, Smet I, Palmisani S, Pang D, Smith T. Sustained effectiveness of 10 kHz high-frequency spinal cord stimulation for patients with chronic, low back pain: 24-month results of a prospective multicenter study. Pain Med. 2014;15(3):347–354. doi:10.1111/pme.12294
27. Kapural L, Yu C, Doust MW, et al. Comparison of 10-kHz high-frequency and traditional low-frequency spinal cord stimulation for the treatment of chronic back and leg pain: 24-month results from a multicenter, randomized, controlled pivotal trial. Neurosurgery. 2016;79(5):667–677. doi:10.1227/NEU.0000000000001418
28. Al-Kaisy A, Palmisani S, Smith TE, et al. Long-term improvements in chronic axial low back pain patients without previous spinal surgery: a cohort analysis of 10-kHz high-frequency spinal cord stimulation over 36 months. Pain Med. 2018;19(6):1219–1226. doi:10.1093/pm/pnx237
29. Schultz DM, Webster L, Kosek P, Dar U, Tan Y, Sun M. Sensor-driven position-adaptive spinal cord stimulation for chronic pain. Pain Physician. 2012;15(1):1–12. doi:10.36076/ppj.2012/15/1
30. Provenzano D, Tate K, Gupta M, et al. Pulse dosing of 10-kHz paresthesia-independent spinal cord stimulation provides the same efficacy with substantial reduction of device recharge time. Pain Med. 2021;22(1):1–12. doi:10.1093/pm/pnaa413
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Migration of Epidural Leads During Spinal Cord Stimulator Trials
Jenkinson RH, Wendahl A, Zhang Y, Sindt JE
Journal of Pain Research 2022, 15:2999-3005
Published Date: 24 September 2022
Spinal Cord Stimulation for Intractable Visceral Pain Originating from the Pelvic and Abdominal Region: A Narrative Review on a Possible New Indication for Patients with Therapy-Resistant Pain
Bieze M, van Haaps AP, Kapural L, Li S, Ferguson K, de Vries R, Schatman ME, Mijatovic V, Kallewaard JW
Journal of Pain Research 2024, 17:691-736
Published Date: 19 February 2024