Back to Journals » Patient Preference and Adherence » Volume 19
Patient Preferences for Low Back Pain Treatments in Iran: A Discrete Choice Experiment
Authors Soofi M ![]() , Karamimatin B, Alipoor Z, Kazemi-Karyani A
, Karamimatin B, Alipoor Z, Kazemi-Karyani A ![]()
Received 12 August 2025
Accepted for publication 6 December 2025
Published 12 December 2025 Volume 2025:19 Pages 4021—4032
DOI https://doi.org/10.2147/PPA.S560108
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Johnny Chen
Moslem Soofi,1 Behzad Karamimatin,2 Zahra Alipoor,1,3 Ali Kazemi-Karyani1
1Social Development and Health Promotion Research Center, Health Policy and Promotion Institute, Kermanshah University of Medical Sciences, Kermanshah, Iran; 2Research Center for Environmental Determinants of Health, Health Institute, Kermanshah University of Medical Sciences, Kermanshah, Iran; 3Department of Clinical Psychology, School of Medicine, Kermanshah University of Medical Sciences, Kermanshah, Iran
Correspondence: Ali Kazemi-Karyani, Social Development and Health Promotion Research Center, Health Policy and Promotion Institute, Kermanshah University of Medical Sciences, Kermanshah, Iran, Tel +98 833 822 0293, Fax +98 833 822 0293, Email [email protected]
Background: Low back pain (LBP) is a leading cause of disability worldwide, especially in LMICs like Iran, yet patient preferences for treatment remain unquantified, hindering patient-centered care. This study aimed to investigate and quantify Iranian patients’ preferences for LBP treatment attributes using a discrete choice experiment (DCE).
Methods: A cross-sectional DCE was conducted involving 331 adult patients in Kermanshah city, western Iran, between July and December 2024. The treatment attributes include pain reduction, risk of recurrence, treatment cost, time required for recovery, and type of treatment. A total of 24 treatment choice sets were developed using a D-efficient design and divided into four blocks. Patient preferences were analyzed using conditional and mixed logit regression models.
Results: The study population (N=331) had a mean age of 38.51 years and was 51.06% female. The conditional logit model identified pain reduction as the most influential attribute affecting patient preferences (coefficient = 0.836; 95% Confidence Interval(CI): 0.629 1.042; P< 0.001). A significant preference was observed for non-surgical treatments (coefficient = 0.665; 95% CI: 0.561– 0.767; P < 0.001), while higher treatment costs, particularly those exceeding 500 million IRR, were negatively associated with choice (coefficient = – 0.751; 95% CI:-0.905 − 0.595; P < 0.001). The mixed logit model revealed significant heterogeneity in preferences, especially for pain reduction (Standard Deviation(SD) up to 1.352; 95% CI: 0.634 − 2.071; P< 0.001), treatment type (SD = 1.827; 95% CI: 1.296– 2.358;P< 0.001), and high treatment costs (SD = 1.477; 95% CI: 0.928– 2.025; P< 0.001), indicating diverse patient valuations. In contrast, risk of recurrence and recovery time showed less variability across individuals.
Conclusion: This study showed strong preferences for pain reduction, affordability, and non-surgical treatments. Significant heterogeneity highlights diverse patient values and the need for individualized, patient-centered care. These findings inform clinical practice and health policy, supporting shared decision-making and improved access to effective, affordable, and non-invasive treatment options in low- and middle-income settings.
Keywords: low back pain, discrete choice experiment, patient preferences, health preferences, Iran
Introduction
Low back pain (LBP) is a leading global cause of disability, affecting approximately 619 million individuals worldwide in 2020 and projected to reach 843 million by 2050.1 It ranks among the top causes of years lived with disability (YLDs) worldwide and imposes a major burden on low- and middle-income countries (LMICs),1 including Iran, where prevalence among adults is estimated at 25.2%.2 LBP substantially reduces quality of life, work productivity, and imposes significant healthcare costs.3,4
A wide range of interventions is available for LBP management, including patient education and self-management, exercise and physiotherapy, behavioral and psychological therapies, pharmacological treatments, interventional procedures, surgical options, and complementary or traditional medicine approaches.5–9 However, treatment effectiveness often depends on how well clinical strategies align with patients’ preferences and expectations. Incorporating patient preferences into care decisions is an essential component of patient-centered practice and has been shown to improve adherence, satisfaction, and outcomes.10,11 Understanding these preferences is therefore crucial for designing effective and acceptable LBP management strategies.12–14
Discrete choice experiments (DCEs) are increasingly used to quantify patient preferences by how individuals value different attributes of healthcare interventions by assessing trade-offs among treatment attributes including effectiveness, side effects, cost, and etc.15 There is a limited body of research examining patient preferences for LBP treatments, with only a few studies conducted in high-income countries.16–18 In contrast, such preferences remain poorly understood in low- and middle-income settings.
To date, no DCE has investigated this topic in Iran, where distinct cultural norms, healthcare system structures, and patterns of service accessibility differ substantially from those in Western contexts. This gap in evidence constrains the development of evidence-based policies and the advancement of patient-centered approaches to LBP management in Iran. Several studies in high-income countries—such as Denmark,16 the USA,18 the Netherlands,19 and Canada20—have shown that patients value pain relief and functional improvement most, while preferring less invasive and affordable treatments. Despite these insights, there is limited evidence from LMICs, and no prior DCE study has explored this issue in Iran.
Given Iran’s distinctive healthcare and cultural context, patient preferences may differ substantially from those reported elsewhere. Addressing this evidence gap is essential for guiding both clinical practice and policy toward more patient-centered and equitable care. This study offers clinically relevant insights by highlighting patient preferences that can inform evidence-based decision-making, guide clinicians in tailoring LBP management to patient needs, and support researchers and policymakers in designing patient-centered interventions and policies. Therefore, this study aimed to identify and quantify Iranian patients’ preferences for LBP treatment attributes using a DCE to inform patient-centered clinical and policy decisions.
Methods
Study Design and Setting
A cross-sectional DCE was conducted to elicit patients’ preferences for LBP treatment in Kermanshah city, western Iran, between July and December 2024. The DCE is a choice-based survey that quantifies preferences for attributes of goods, services or interventions. It assumes that goods or services (in this case LBP treatment) can be defined by two or more attributes and the levels of these attributes.21 For example, treatment for LBP can be characterized by certain features or attributes such as the type of treatment, treatment cost, effectiveness, time to full recovery, and so on. Each of these attributes has different levels (for instance, treatment cost may have three levels: lower than 200 million, 200 to 500 million, and more than 500 million Iranian Rials (IRR), while the type of treatment may have two levels: surgical and non-surgical). The combination of the different levels of these attributes produces various treatment alternatives for LBP. Patient preferences for LBP treatment are determined by the levels of these attributes. DCE allows researchers to understand how patients make trade-offs between these attributes when choosing treatments options, each with different combinations of attributes and their levels.22 In a DCE, each respondent faces a series of hypothetical choice sets composed of two or more alternatives, (two alternatives in present study) A choice set refers to the collection of alternatives presented to participants, in which they are asked to choose their preferred option. This approach is rooted in random utility theory, which assumes that individuals choose alternatives that maximize their utility.3 The study protocol was reviewed and approved by the Ethics Committee of Kermanshah University of Medical Sciences (Ethics code: IR.KUMS.REC.1402.591), and all participants provided written informed consent in accordance with the Declaration of Helsinki. The reporting of DCE in this study follows the DIscrete choice experiment REporting ChecklisT (DIRECT).23
Identification of Attribute and Levels
First, a list of attributes was extracted by literature review16–18,20,24 and expert opinions. The first list of attributes and levels included 13 attributes at different levels for the LBP treatments. Then, the final attributes were selected by a panel consisting of six experts from the fields of health economics, health policy, physiotherapist, neurosurgeon, and healthcare management, by ranking attributes, with five attributes were determined for the treatment of LBP. The five attributes related to preferences for LBP treatment included pain reduction, risk of recurrence, cost of treatment, type of treatment, and time needed for recovery. The levels of selected attributes were also chosen using relevant studies and the opinions of experts so that they could cover the essential dimensions of the LBP treatment. This selection aimed to capture the most important factors influencing patient preferences while maintaining a manageable cognitive burden for respondents. The final attributes and their levels are presented in Table 1.
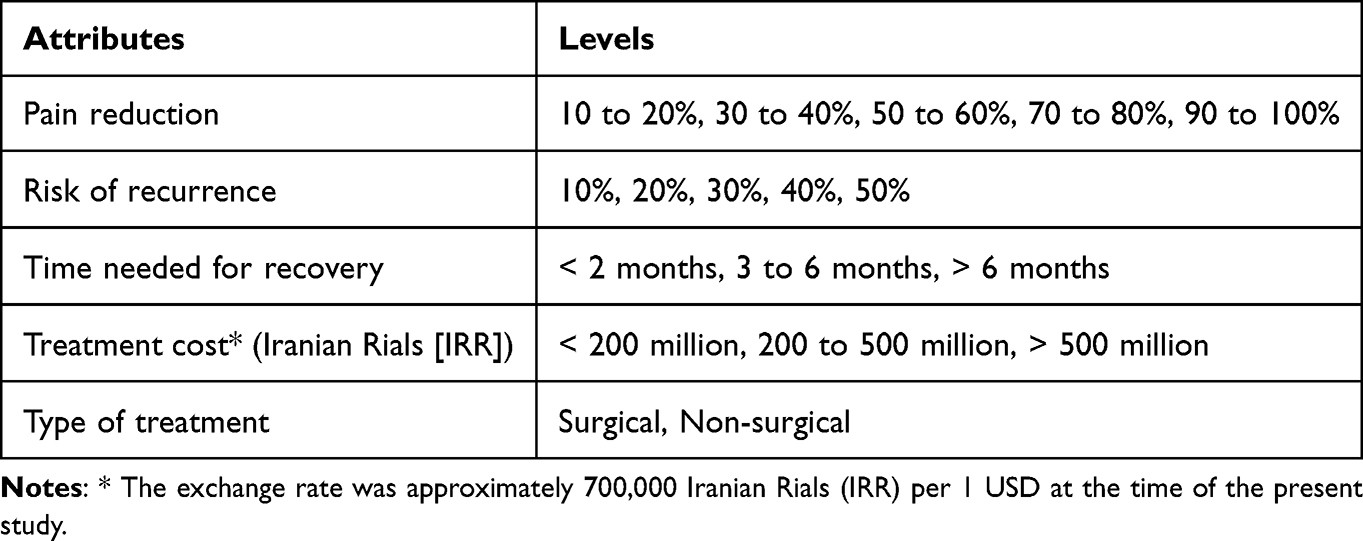 |
Table 1 Attributes of LBP Treatment and Their Levels Used in the Discrete Choice Experiment |
Experimental Design
The combination of attributes and attribute levels (two attributes with five levels, two attribute with three levels and one attribute with two levels) resulted in 450 hypothetical LBP treatment profiles (52 × 32×21).25 For obvious practical reasons, not all of these could be used in a questionnaire. Therefore, we generated a sample of hypothetical LBP treatment profiles (choice sets) from all these 450 treatment profiles for the questionnaire using a D-efficient fractional factorial design, which is considered optimal for maximizing statistical efficiency while minimizing the number of choice tasks required and respondent burden.26,27 The final experimental design consisted of 24 choice sets divided into 4 blocks, with each respondent completing 6 choice sets. Each choice set presented respondents with two hypothetical treatment scenarios (treatment A and treatment B) characterized by different levels of the five attributes.28
Following best practices in preference elicitation, a pre-test was conducted to evaluate understanding, respondent burden, timing, wording comprehension, task realism, and cognitive load. This pre-test included detailed discussions regarding the attributes and levels used in the DCE. While feedback from the pre-test confirmed that respondents clearly understood the scenarios and treatment options, minor modifications were made to the wording of the scenarios to improve task comprehension. Subsequently, a pilot test of the questionnaire was carried out to further assess understanding, respondent burden, timing, and wording. Incorporating feedback from the pilot test, slight adjustments were made to refine the instrument prior to its final implementation the pilot, slight modifications were made to improve the instrument before final implementation.27
To evaluate internal validity, we included a dominant choice set where one alternative was unambiguously superior across all attributes. This served as a rationality check to identify respondents who may not have understood the task or were not engaging meaningfully with the survey.29,30 The choice sets were designed using the Stata software version 17. One of the choice sets used in the study is displayed in Table 2.
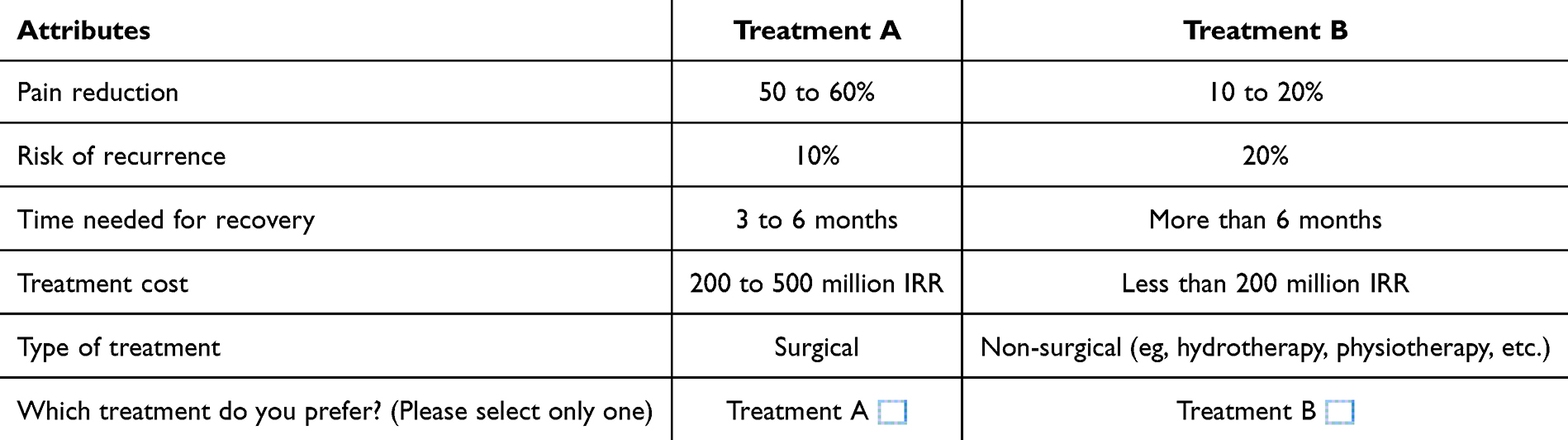 |
Table 2 One of the Choice Sets Used in the Study |
Sampling
We followed a commonly used rule-of-thumb to determine sample size:

where n was the number of respondents, c was the largest number of levels for any attributes, a was the number of alternatives, and s was the number of choice sets each respondent receive. This formula indicated a minimum sample size of 208 respondents. However, to ensure robust statistical analysis and to account for potential heterogeneity in preferences, a larger sample of 362 patients was recruited. This number of individuals was calculated to be sufficiently large for reliable statistical analyses for our study.31–33 A convenience sample of adult participants (≥18 years) with a self-reported or clinically documented diagnosis of LBP (ICD-10: M54.5) was recruited. All enrolled individuals provided informed consent prior to inclusion. The sole exclusion criterion was an inability to understand the survey questions during the initial explanation, which was assessed before consent was sought.
Data Collection
Each respondent was randomly assigned to one of the four blocks of choice sets. Sociodemographic and clinical information were collected to describe the study population and to explore potential differences in preferences across different patient subgroups. Each participant completed a series of 6-choice tasks presented on a paper-based questionnaire, with responses recorded by the interviewer. Data collection was conducted through face-to-face interviews conducted by trained interviewers by visiting relevant hospital centers and specialists’ clinics in Kermanshah city, Western Iran. Although face-to-face administration facilitated participant comprehension and completion of the DCE survey, it may have introduced potential biases, including social desirability and interviewer effects. Before completing the DCE tasks, participants received detailed explanations about the purpose of the study and the nature of the choice tasks. The trained interviewers ensured that the respondents understood the attributes during the interview.
Data Analysis
Of the 362 participants who completed the survey, 31 failed the rationality check (did not choose the dominant alternative) and were excluded from the analysis to ensure data quality. The final sample used in the analysis comprised 331 respondents, each providing responses to 6 completed choices and resulting in 3972 observations (331 individuals × 6 choices × 2 options for each choice). We used a conditional logit regression model to analyze patients’ preferences as a commonly used method for analyzing DCE data.16 We used a fixed-effects conditional logit model for the analysis. Utility function were specified as follows:
Uij= β1×Pain reduction: 30–40%+β2×Pain reduction: 50 −60%+β3×Pain reduction: 70–80% +β4×Pain reduction: 90 −100%+β5×Risk of recurrence: 20% +β6×Risk of recurrence: 30%+β7×Risk of recurrence: 40%+β8×Risk of recurrence: 50% +β9×Time needed for recovery: 3–6 months+β10×Time needed for recovery: > 6 months+β11×Treatment cost: 200–500 million+β12×Treatment cost: > 500 million+β13×Type of treatment: nonsurgical + εij
Where:
Uij represents the utility derived from a treatment alternative, each β represents the preference weight (coefficient) for the corresponding attribute level relative to the reference category, indicating the relative importance (value) that individuals place on attribute levels. In this model, more preferred levels have higher coefficient value, and its sign indicates whether the attribute level has a positive or negative effect on participants’ utility. A statistically significant coefficient indicates that the respondents considered the attribute important in their choices. Also, εij is a random error term that represents the unmeasured effects in participants’ preferences.25,34,35 The mixed logit model also was employed to capture individual preference heterogeneity by allowing random variation in parameters. This approach relaxes the assumption of uniform preferences typical in traditional models. Using both mixed and conditional logit models provides a more flexible and comprehensive analysis. Together, they enhance the robustness and validity of the study’s findings.35–37
Results
Sample Characteristics
A total of 362 patients with LBP participated in the study and met the inclusion criteria. Of which, 31 (8%) were excluded because of irrational response to dominant choice set, indicating a lack of engagement. Thus, data from 331 patients, with a mean age of 38.51 years (SD 11.56 years),were analyzed. Sex was evenly distributed (48.94% male, 51.06% female), with the largest age group being 31–40 years (38.37%). Most participants were married (67.67%), held postgraduate degrees (55.29%), and belonged to middle socioeconomic status (49.85%). While 91.24% had basic insurance, only 41.39% reported complementary coverage (Table 3).
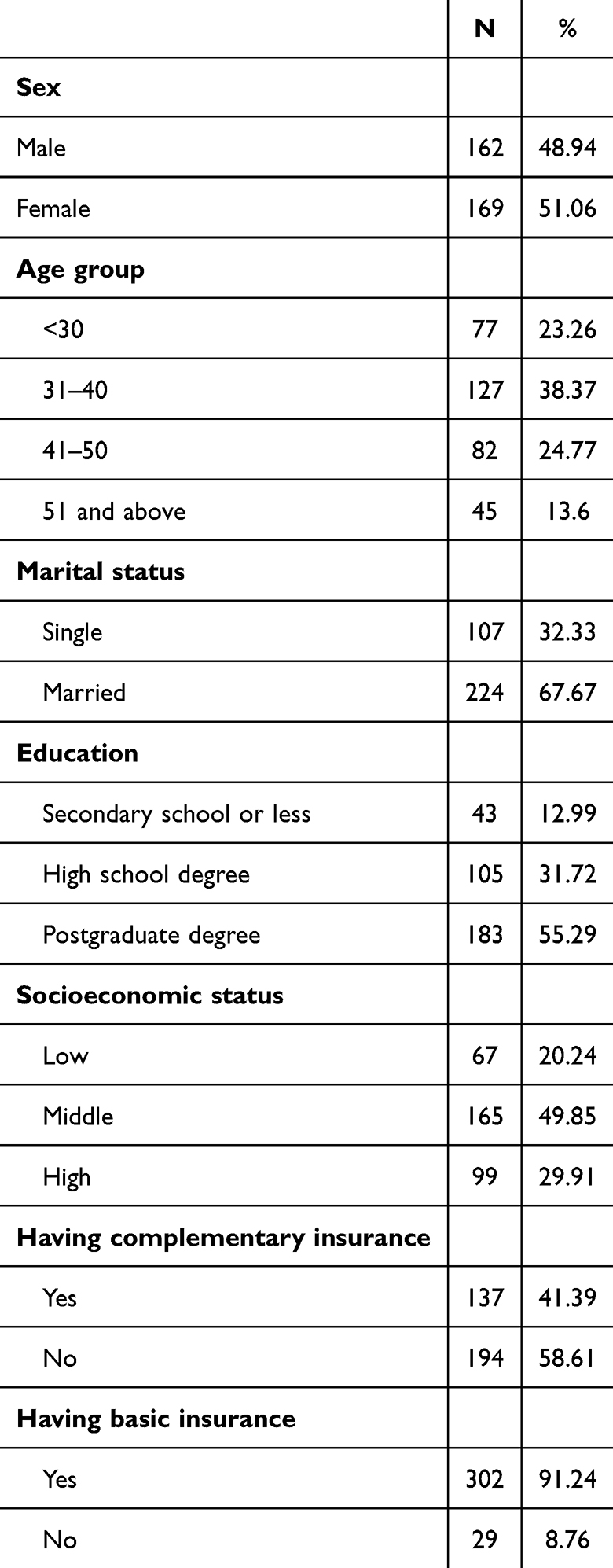 |
Table 3 Demographic Characteristics of Study Participants |
Among the participants, 36.56% reported experiencing LBP for less than three months, followed by 29.31% who had symptoms persisting for more than two years. In the week before the study, 63.75% of participants experienced pain on two days or fewer. Prior to participation, various treatment modalities had been utilized, with painkillers and rest being the most commonly reported (60.73%). Only 4.53% had undergone surgery for LBP (Table 4).
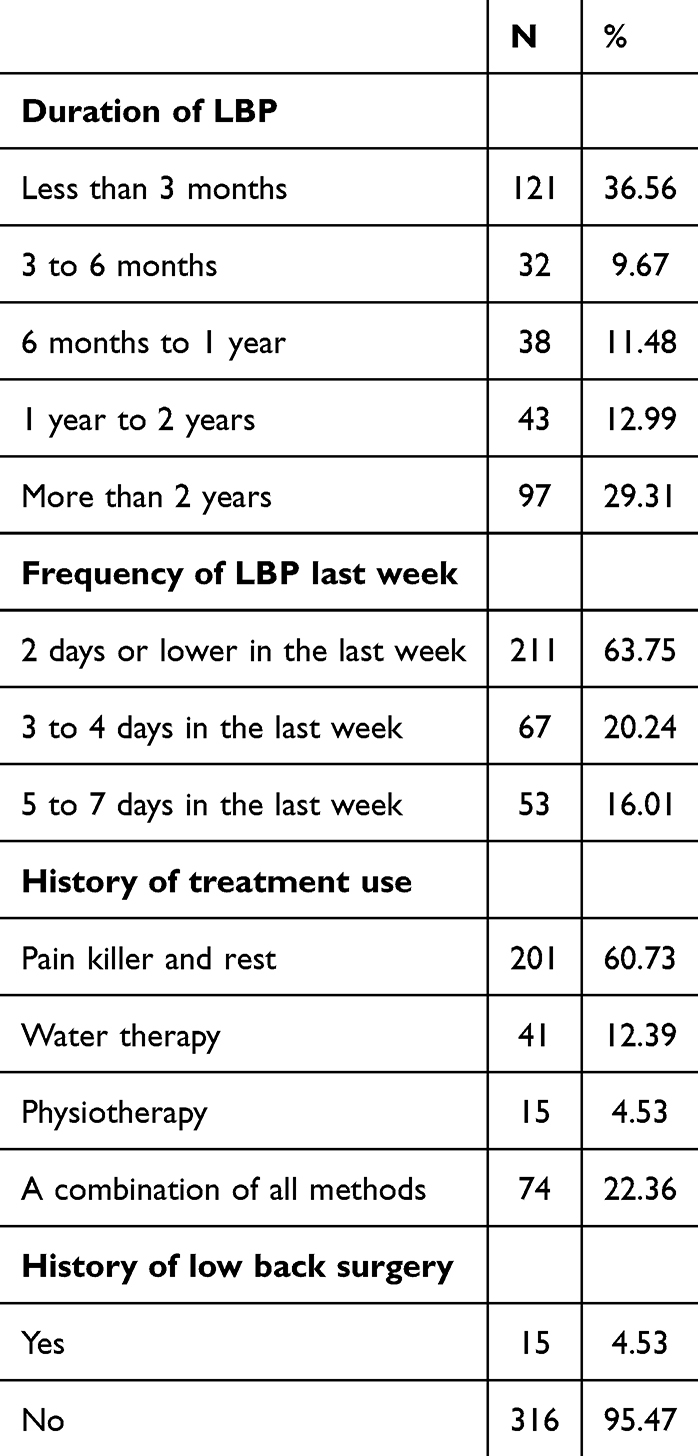 |
Table 4 Clinical Characteristics of Participants |
The conditional logit model identified pain reduction as the most influential factor in patient preferences for LBP treatments, with very high pain relief significantly increasing treatment selection (coefficient = 0.836; 95% CI: 0.6290–1.0420; OR = 2.30; P <0.001). Treatment cost negatively impacted preferences, especially above 50 million IRR (coefficient = –0.751; 95% CI: −0.905 −0.595; OR = 0.47; P < 0.001). Patients strongly preferred non-surgical over surgical treatments (coefficient = 0.665; 95% CI: 0.5610–0.767; OR = 1.94; P < 0.001). Higher risk of recurrence reduced treatment likelihood (coefficient = –0.512; 95% CI: −0.711 −0.311; OR = 0.59; P < 0.001), and recovery time only influenced choices when exceeding six months (coefficient = –0.345; 95% CI: −0.490 −0.200; OR = 0.71; P <0.001) (Table 5).
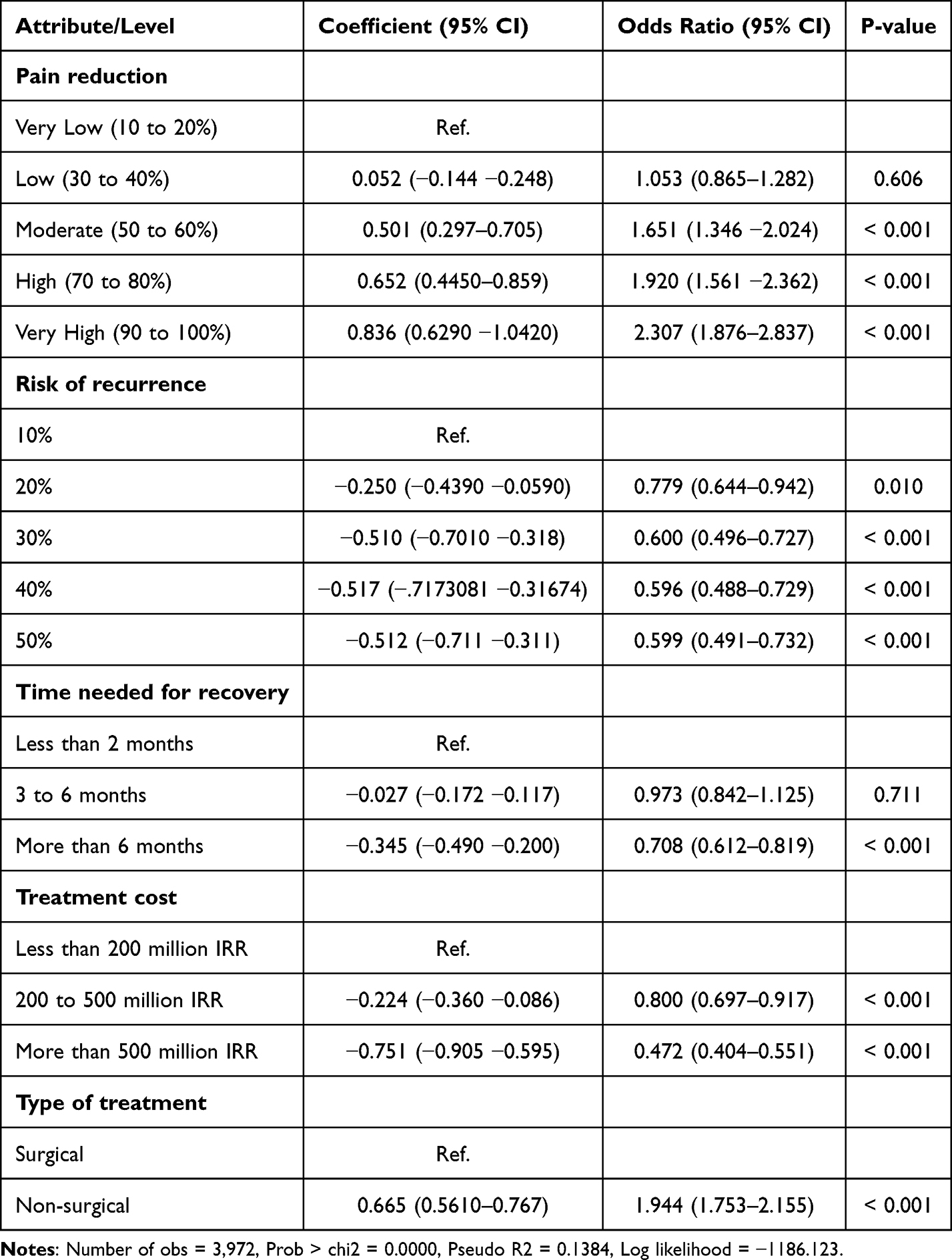 |
Table 5 Conditional Logit Model of the Patients’ Preferences for the Attributes of LBP Treatments |
The mixed logit model results confirm the key findings of the conditional logit model, reinforcing that pain reduction, treatment type, cost, risk of recurrence, and recovery time significantly influence patient preferences for LBP treatments. The mixed logit model extends these insights by accounting for preference heterogeneity among patients, as indicated by statistically significant standard deviations for several key attributes. Notably, substantial variability exists in how patients value pain reduction, particularly at high (SD = 0.941, 95% CI: p = 0.023) and very high levels (SD = 1.352, 95% CI: 0.634 −2.071; p < 0.001). Preference heterogeneity is also pronounced for treatment type, with non-surgical options showing a large standard deviation (SD = 1.827, 95% CI: 1.296–2.358; p < 0.001), reflecting diverse patient attitudes toward surgical versus non-surgical interventions. Additionally, treatment cost above 500 million IRR exhibits significant variability in patient sensitivity (SD = 1.477, 95% CI: 0.928–2.025; p < 0.001). Some attributes, such as risk of recurrence and recovery time, show less consistent heterogeneity (Table 6).
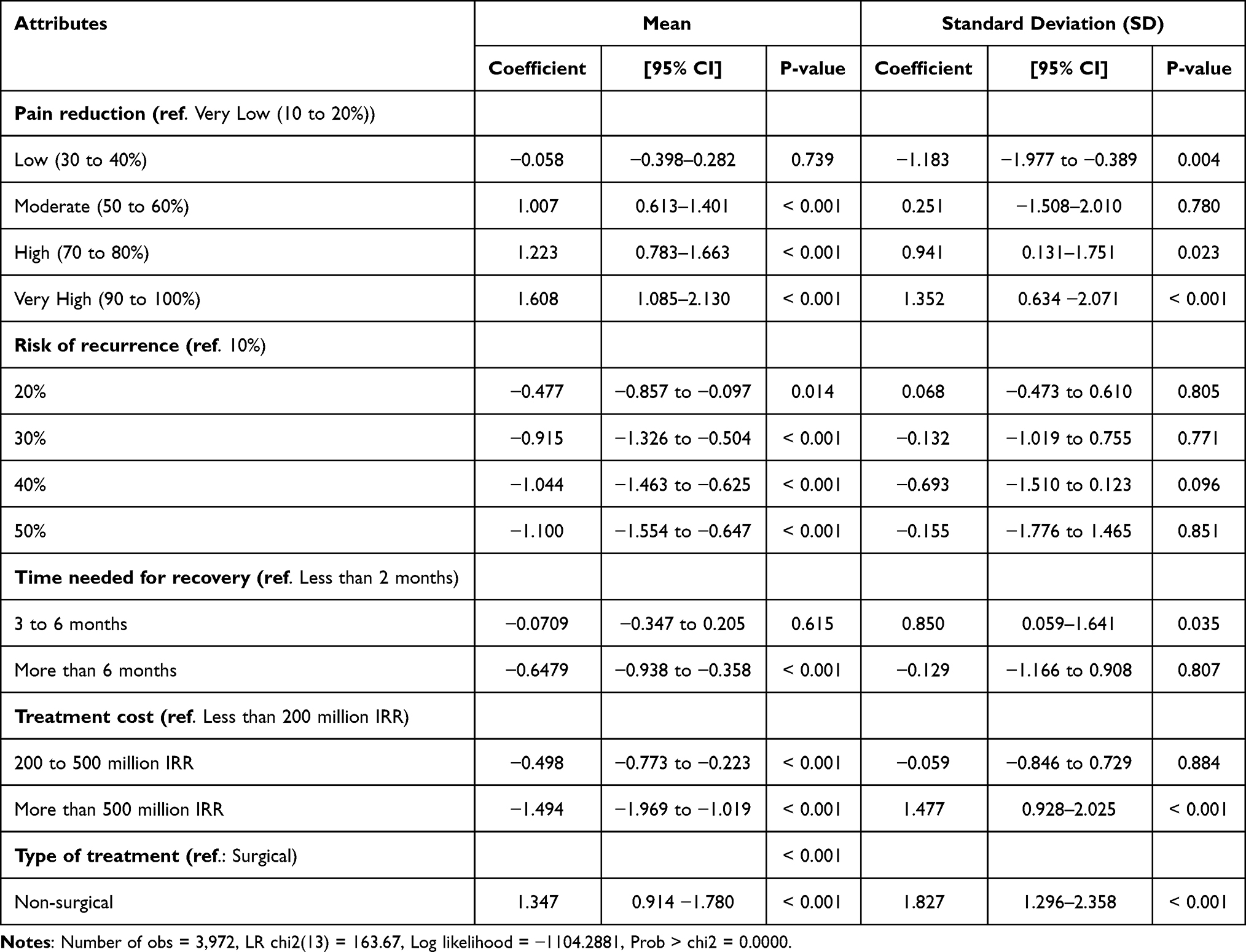 |
Table 6 Mixed Logit Model of the Patients’ Preferences for the Attributes of LBP Treatments |
Discussion
This study explored Iranian patients’ preferences for LBP treatments using a DCE, the first of its kind conducted in Iran. The findings highlight critical insights into patient preferences for LBP treatment in Iran, revealing that pain reduction is the dominant attribute influencing treatment choices, followed by a preference for non-surgical treatment options, cost considerations, risk of recurrence, and recovery duration. These findings reveal a strong desire for effective symptom relief and affordable, minimally invasive care, underscoring the need for patient-centered and economically sensitive management strategies in Iran’s healthcare system.
Consistent with previous research,16,18 pain reduction was the dominant attribute shaping treatment decisions. They similarly identified pain relief and functional improvements (eg, ability to perform daily activities) as central drivers of patient preferences. This consistency across diverse populations suggests the universal prioritization of symptom alleviation in LBP management. The contrast with Morillon et al (2023),20 who found treatment modality (eg, preference for physical manipulations) more influential than pain reduction, may reflect contextual differences. In Iran, where access to advanced non-surgical options is limited, patients may value treatment outcomes over modality choice.
Economic factors also significantly influenced preferences. Higher treatment costs significantly reduced the likelihood of treatment selection, consistent with findings from Gadjradj et al (2021),19 where out-of-pocket costs significantly influenced preferences for lumbar disc herniation surgery, and Wilson et al (2023),18 who highlighted socioeconomic disparities in treatment accessibility. The pronounced cost sensitivity underscores the importance of enhancing financial protection such as expanding insurance coverage for effective non-surgical interventions to improve treatment accessibility and adherence in LBP management. This finding is particularly salient in the Iranian context, where high out-of-pocket expenditures and limited insurance coverage constrain access to care.38 Comparable studies in other settings have identified cost as a critical determinant of treatment choice.
Patients expressed a clear preference for non-surgical treatments, aligning with prior studies indicating caution toward invasive procedures.16,19 The aversion to surgery likely reflect concerns about surgical risks, long recovery, and long-term outcomes.19 These results highlight the need for clinicians to engage patients in shared decision-making and consider non-surgical options where clinically appropriate.
Consistent with previous research,16,17 risk of recurrence and recovery time also influenced treatment preferences, although to a lesser degree. Patients appeared willing to tolerate moderate recovery periods if outcomes were favorable, but treatments associated with extended recovery or higher recurrence risk were viewed less favorably. These findings highlight the multifaceted nature of patient decision-making, where both short-term symptom relief and long-term health prospects are weighed in evaluating treatment choices.16,20
The mixed logit model confirmed significant heterogeneity in patient preferences, particularly regarding pain reduction, treatment type, and cost. This heterogeneity indicates that while average trends can guide clinical practice, individualized approaches remain essential. For instance, the heterogeneity for “non-surgical treatment” implies that while the average preference was positive, a meaningful segment of patients may actually prefer surgical options, highlighting the need for personalized care. This is in line with the study by Kløjgaard et al that revealed preferences heterogeneity in treatment modality and the level of pain reduction in LBP care.16 While average trends offer useful guidance, this variability highlights that patients weigh treatment attributes differently, reflecting diverse priorities and trade-offs in LBP management. Recognizing this heterogeneity is essential for personalized medicine, as it supports tailoring treatments to align with individual values and expectations, ultimately enhancing patient satisfaction and outcomes. The mixed logit model’s ability to reveal such nuanced preference patterns enhances the relevance of results for clinical decision-making and health policy development.35
From a policy perspective, translating these insights into practice requires multi-level action. Clinicians could use structured patient preference checklist to facilitate shared decision-making; policymakers might revise insurance reimbursement schemes to favor high-value, non-surgical treatments and mitigate cost barriers; and healthcare administrators could design culturally adapted patient decision aids informed by the attributes and levels valued by patients in this study.
This study contributes novel evidence from a middle-income setting, contextualizing patient preferences within Iran’s distinct cultural and economic environment. Unlike many DCEs conducted in high-income countries, our findings reflect the interplay of cultural, economic, and systemic factors shaping treatment choices in an LMIC. For example, the observed cost sensitivity and preference for non-invasive treatments may be amplified by limited healthcare resources and cultural attitudes toward traditional and conservative care. Such findings reinforce the importance of locally grounded preference studies to inform patient-centered care and health policy effectively.
Strengths and Limitations
Several limitations should be acknowledged. The use of a non-probability, convenience sample from a single geographic location (Kermanshah) may introduce selection bias and likely does not capture the full spectrum of cultural, socioeconomic, and healthcare-access variations present across Iran, limiting the generalizability of results to the national population with LBP. Future research employing a probability-based sampling design from a wider range of regions is warranted to enhance the external validity and national representativeness. Preferences were assessed at a single point in time, whereas they may evolve with experience or changes in health status. Longitudinal studies could provide insights into the dynamics of patient preferences. Additionally, participants’ previous experiences with different treatment modalities may have influenced their preferences in ways that are difficult to quantify. Finally, the hypothetical nature of the choices made by respondents may not fully reflect real-world clinical decision-making.
Despite these limitations, the study followed established DCE methodological standards,23,27,39 and provides robust, context-specific evidence to guide patient-centered practice and policy in Iran. Future research exploring subgroup variations such as gender, income, and prior treatment experience would further enhance understanding of patient heterogeneity in LBP management.
Conclusion
This study provides the first quantitative evidence of Iranian patients’ preferences for LBP management, highlighting that treatment decisions are primarily influenced by pain reduction, affordability, and non-surgic al options. The significant heterogeneity in preferences underscores the need to move beyond standardized protocols toward individualized, patient-centered care. These findings contribute to the growing literature on patient preference studies in low- and middle-income contexts and offer a practical foundation for policy and clinical decision-making. Integrating these insights into clinical practice can guide the development of shared decision-making tools and individualized treatment plans. From a policy perspective, the results support revising insurance coverage and resource allocation strategies to enhance access to high-value, non-surgical, and cost-effective LBP treatments. Future research should replicate these methods across diverse Iranian populations and clinical subgroups in different regions to further inform equitable, evidence-based LBP health policy.
Code Availability
We used STATA SE software version 17 codes for our analyses. The codes are available on the STATA Corp website.
Data Sharing Statement
The data collected and/or analyzed during the current study are not publicly available due the terms of consent to which the participants agreed but are available from the corresponding author on reasonable request.
Ethics Approval
This study was approved by the Ethics Committee of KUMS. (Ethics code: IR.KUMS.REC.1402.591).
Consent to Participate
Informed consent was obtained from all the respondents included in the study.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was funded by Kermanshah University of Medical Sciences (KUMS) under grant No. 4020936.
Disclosure
The authors have no competing interests to declare that are relevant to the content of this article.
References
1. Ferreira ML, de Luca K, Haile LM. et al. Global, regional, and national burden of low back pain, 1990–2020, its attributable risk factors, and projections to 2050: a systematic analysis of the Global Burden of Disease Study 2021. Lancet Rheumatol. 2023;5(6):e316–e329. doi:10.1016/S2665-9913(23)00098-X
2. Ghafouri M, Teymourzadeh A, Nakhostin-Ansari A, et al. Prevalence and predictors of low back pain among the Iranian population: results from the Persian cohort study. Ann Med Surg. 2022;74:103243. doi:10.1016/j.amsu.2022.103243
3. Alfalogy E, Mahfouz S, Elmedany S, et al. Chronic low back pain: prevalence, impact on quality of life, and predictors of future disability. Cureus. 2023;15(9). doi:10.7759/cureus.45760
4. Fatoye F, Gebrye T, Ryan CG, et al. Global and regional estimates of clinical and economic burden of low back pain in high-income countries: a systematic review and meta-analysis. Front Public Health. 2023;11:1098100. doi:10.3389/fpubh.2023.1098100
5. Qaseem A, Wilt TJ, McLean RM, et al. Noninvasive treatments for acute, subacute, and chronic low back pain: a clinical practice guideline from the American College of Physicians. Ann Internal Med. 2017;166(7):514–530. doi:10.7326/M16-2367
6. Kuzu Ş, Canli M, Valamur İ, et al. Effects of aerobic exercise in addition to core stabilization exercises on functional capacity, physical performance and fall risk in geriatric individuals with chronic non-specific low back pain. BMC Sports Sci Med Rehabil. 2025;17(1):218. doi:10.1186/s13102-025-01271-7
7. Özüdoğru A, Canlı M, Ceylan İ, et al. Five Times Sit-to-Stand Test in people with non-specific chronic low back pain—a cross-sectional test–retest reliability study. Irish J Med Sci. 2023;192(4):1903–1908. doi:10.1007/s11845-022-03223-3
8. Zhou T, Salman D, McGregor AH. Recent clinical practice guidelines for the management of low back pain: a global comparison. BMC Musculoskelet Disorders. 2024;25(1):344. doi:10.1186/s12891-024-07468-0
9. Seyed MA, Mohamed SHP. Low back pain: a comprehensive review on the diagnosis, treatment options, and the role of other contributing factors. Open Access Maced J Med Sci. 2021;9(F):347–359. doi:10.3889/oamjms.2021.6877
10. Ostermann J, Brown DS, de Bekker-Grob EW, et al. Preferences for health interventions: improving uptake, adherence, and efficiency. Patient-Patient-Centered Outcomes Res. 2017;10:511–514. doi:10.1007/s40271-017-0251-y
11. Whitty JA, Fraenkel L, Saigal CS, et al. Assessment of individual patient preferences to inform clinical practice. Patient-Patient-Centered Outcomes Res. 2017;10:519–521. doi:10.1007/s40271-017-0254-8
12. Soroceanu A, Ching A, Abdu W, et al. Relationship between preoperative expectations, satisfaction, and functional outcomes in patients undergoing lumbar and cervical spine surgery: a multicenter study. Spine. 2012;37(2):E103–E108. doi:10.1097/BRS.0b013e3182245c1f
13. Yee A, Adjei N, Do J, et al. Do patient expectations of spinal surgery relate to functional outcome? Clin Orthop Related Res. 2008;466:1154–1161. doi:10.1007/s11999-008-0194-7
14. Stewart MJ, Maher CG, Refshauge KM, et al. Patient and clinician treatment preferences do not moderate the effect of exercise treatment in chronic whiplash-associated disorders. Eur J Pain. 2008;12(7):879–885. doi:10.1016/j.ejpain.2007.12.009
15. Ryan M, Bate A, Eastmond CJ, et al. Use of discrete choice experiments to elicit preferences. BMJ Qual Saf. 2001;10(suppl 1):i55–i60. doi:10.1136/qhc.0100055
16. Kløjgaard ME, Manniche C, Pedersen LB, et al. Patient preferences for treatment of low back pain—a discrete choice experiment. Value Health. 2014;17(4):390–396. doi:10.1016/j.jval.2014.01.005
17. Turk D, Boeri M, Abraham L, et al. Patient preferences for osteoarthritis pain and chronic low back pain treatments in the United States: a discrete-choice experiment. Osteoarthritis Cartilage. 2020;28(9):1202–1213. doi:10.1016/j.joca.2020.06.006
18. Wilson L, Zheng P, Ionova Y, et al. CAPER: patient preferences to inform nonsurgical treatment of chronic low back pain: a discrete-choice experiment. Pain Med. 2023;24(8):963–973. doi:10.1093/pm/pnad038
19. Gadjradj PS, Smeele NVR, de Jong M, et al. Patient preferences for treatment of lumbar disc herniation: a discrete choice experiment. J Neurosurg Spine. 2021;36(5):704–712. doi:10.3171/2021.8.SPINE21995
20. Morillon GF, Benkhalti M, Dagenais P, et al. Preferences of patients with chronic low back pain about nonsurgical treatments: results of a discrete choice experiment. Health Expectations. 2023;26(1):510–530. doi:10.1111/hex.13685
21. Ryan M. Discrete choice experiments in health care. BMJ. 2004;328:360–361. doi:10.1136/bmj.328.7436.360
22. Soekhai V, de Bekker-Grob EW, Ellis AR, et al. Discrete choice experiments in health economics: past, present and future. Pharmacoeconomics. 2019;37:201–226. doi:10.1007/s40273-018-0734-2
23. Ride J, Goranitis I, Meng Y, et al. A reporting checklist for discrete choice experiments in health: the DIRECT checklist. Pharmacoeconomics. 2024;42(10):1161–1175. doi:10.1007/s40273-024-01431-6
24. Gadjradj PS, Harhangi BS, van Tulder MW, et al. Surgeons preference for lumbar disk surgery: a discrete choice experiment. Eur Spine J. 2021;1–9.
25. Hensher DA, Rose JM, Greene WH. Applied Choice Analysis, 2nd ed. Cambridge: Cambridge University Press; 2015.
26. Jonker MF, Donkers B, de Bekker‐Grob E, et al. Attribute level overlap (and color coding) can reduce task complexity, improve choice consistency, and decrease the dropout rate in discrete choice experiments. Health Econ. 2019;28(3):350–363. doi:10.1002/hec.3846
27. Johnson FR, Lancsar E, Marshall D, et al. Constructing experimental designs for discrete-choice experiments: report of the ISPOR conjoint analysis experimental design good research practices task force. Value Health. 2013;16(1):3–13. doi:10.1016/j.jval.2012.08.2223
28. Lancsar E, Fiebig DG, Hole AR. Discrete choice experiments: a guide to model specification, estimation and software. Pharmacoeconomics. 2017;35:697–716. doi:10.1007/s40273-017-0506-4
29. Johnson FR, Yang J-C, Reed SD. The internal validity of discrete choice experiment data: a testing tool for quantitative assessments. Value Health. 2019;22(2):157–160. doi:10.1016/j.jval.2018.07.876
30. Lancsar E, Louviere J. Conducting discrete choice experiments to inform healthcare decision making: a user’s guide. Pharmacoeconomics. 2008;26:661–677. doi:10.2165/00019053-200826080-00004
31. Assele SY, Meulders M, Vandebroek M. Sample size selection for discrete choice experiments using design features. J Choice Model. 2023;49:100436. doi:10.1016/j.jocm.2023.100436
32. de Bekker-Grob EW, Donkers B, Jonker MF, et al. Sample size requirements for discrete-choice experiments in healthcare: a practical guide. Patient-Patient-Centered Outcomes Res. 2015;8:373–384. doi:10.1007/s40271-015-0118-z
33. Orme B. Sample size issues for conjoint analysis studies. Sequim: Sawtooth software technical paper, 1998.
34. McFadden D. Conditional logit analysis of qualitative choice behavior. In: Zarembka P, editor. Frontiers in Econometrics New York. New York, NY, USA: Academic Press; 1974:104–142.
35. Hauber AB, González JM, Groothuis-Oudshoorn CGM, et al. Statistical methods for the analysis of discrete choice experiments: a report of the ISPOR conjoint analysis good research practices task force. Value Health. 2016;19(4):300–315. doi:10.1016/j.jval.2016.04.004
36. Karim S, Craig BM, Vass C, et al. Current practices for accounting for preference heterogeneity in health-related discrete choice experiments: a systematic review. Pharmacoeconomics. 2022;40(10):943–956. doi:10.1007/s40273-022-01178-y
37. Vass C, Boeri M, Karim S, et al. Accounting for preference heterogeneity in discrete-choice experiments: an ISPOR special interest group report. Value Health. 2022;25(5):685–694. doi:10.1016/j.jval.2022.01.012
38. Soofi M, Arab‐Zozani M, Kazemi‐Karyani A, et al. Can Health insurance protect against catastrophic health expenditures in Iran? A systematic review and meta‐analysis. World Med Health Policy. 2021;13(4):695–714. doi:10.1002/wmh3.425
39. Bridges JF, Hauber AB, Marshall D, et al. Conjoint analysis applications in health—a checklist: a report of the ISPOR Good Research Practices for Conjoint Analysis Task Force. Value Health. 2011;14(4):403–413. doi:10.1016/j.jval.2010.11.013
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Patient Preference for Self-Injection Devices in Rheumatoid Arthritis: A Discrete Choice Experiment in China
Wei Y, Zhao J, Ming J, Zhang X, Chen Y
Patient Preference and Adherence 2022, 16:2387-2398
Published Date: 31 August 2022
Willingness to Pay and Preferences Among Patients Undergoing Cystoscopies: Results from a Large Survey-Based Study in Spain
Borja Brugés CN, Rindorf DK, Cepeda M, Schultz Hansen K
Research and Reports in Urology 2022, 14:359-367
Published Date: 18 October 2022
The Impact of Substantial Improvements in HbA1c and Weight Loss on the Medication Preferences of People with Type 2 Diabetes
Gelhorn HL, Osumili B, Brown K, Ross MM, Schulz A, Fernandez G, Boye KS
Patient Preference and Adherence 2023, 17:793-805
Published Date: 22 March 2023
Understanding Treatment Preferences Among People Living with HIV in Australia: A Discrete Choice Experiment
Fifer S, Kularatne T, Tan M, Drummond F, Rule J
Patient Preference and Adherence 2023, 17:1825-1843
Published Date: 26 July 2023
Eliciting Depression Patients’ Preferences for Medication Management: A Protocol for Discrete Choice Experiment
Xie P, Li HQ, Peng WL, Yang H
Patient Preference and Adherence 2024, 18:289-300
Published Date: 2 February 2024